Embed Size (px)
Citation preview

HeadachesHeadaches

CONTINUITY CLINIC
ObjectivesObjectives Recognize and differentiate the elements Recognize and differentiate the elements
of history and physical findings of history and physical findings associated with the following headache associated with the following headache types:types: MigraineMigraine Tension headacheTension headache Increased Intracranial PressureIncreased Intracranial Pressure
Know which signs and symptoms Know which signs and symptoms mandate imagingmandate imaging
Be familiar with the treatment options for Be familiar with the treatment options for HAHA

CONTINUITY CLINIC
BackgroundBackground Recurrent headache is a common complaint in
pediatric clinics; studies indicate that it affects: almost 40% of kids by 7 years of age 75% of children by 15years of age.
Important causes: Migraine Psychogenic factors Increased intracranial pressure Depression may present as headache Toxins (carbon monoxide) Sinusitis Eye issues: refractive errors,strabismus Bruxism.

MigrainesMigraines
CONTINUITY CLINIC
MigrainesMigraines Migraine headaches are the most common Migraine headaches are the most common
cause of intermittent headache in children.cause of intermittent headache in children. They are defined as a recurrent headache They are defined as a recurrent headache
with symptom-free intervals and at least with symptom-free intervals and at least three of the following (Prensky criteria):three of the following (Prensky criteria): Hemi cranial painHemi cranial pain Throbbing/pulsatile character of painThrobbing/pulsatile character of pain Associated with abdominal pain, nausea, OR Associated with abdominal pain, nausea, OR
vomitingvomiting Relieved by rest/sleepRelieved by rest/sleep Visual, sensory or motor auraVisual, sensory or motor aura Family history in first-degree relativeFamily history in first-degree relative

CONTINUITY CLINIC
HistoryHistory Location of pain – usually bifrontal or temporal regionsLocation of pain – usually bifrontal or temporal regions Photophobia, phonophobia or lightheadedness Photophobia, phonophobia or lightheadedness Limitation of daily activities? – often nausea and vomiting cause Limitation of daily activities? – often nausea and vomiting cause
the greatest limitationthe greatest limitation SchoolSchool SportsSports
How long? - often last 1-3 hours (longest is up to 24 hours)How long? - often last 1-3 hours (longest is up to 24 hours) Focal neurologic symptoms? – before, during, or afterFocal neurologic symptoms? – before, during, or after
Visual disturbancesVisual disturbances WeaknessWeakness Paresthesia Paresthesia
Precipitating causes including:Precipitating causes including: Emotional stressEmotional stress Changes in sleep patternsChanges in sleep patterns MenstruationMenstruation Weather changesWeather changes Foods - chocolate, cola, nuts, MSG and meats Foods - chocolate, cola, nuts, MSG and meats Relief from analgesicsRelief from analgesics
Family history is very important: an estimated 80-90% of children Family history is very important: an estimated 80-90% of children with migraine have an affected relative.with migraine have an affected relative.

CONTINUITY CLINIC
Classification of Classification of MigrainesMigraines
Migraine with aura begins with an aura, usually visual, that lasts 5-20 minutes prior to the headache. Visual phenomenon may include photopsia (flashing lights), fortification spectra (zigzags), black dots, colored lights, scotomata, or distortions of size. It may be the only manifestation of the headache, and children are often distressed by this symptom and have difficulty describing it.
Migraine without aura is usually diagnosed with the help of family history and the character of the headache.
Complicated migraine is migraine associated with a transient, focal neurologic abnormality, most commonly hemiparesis, hemianesthesia, visual field deficits and cranial nerve palsies (oculomotor). It is the most common cause of third cranial nerve palsy in children. Note that because of these associated deficits, evaluation of the first episode should include a CT or MRI brain scan.

CONTINUITY CLINIC
TreatmentTreatment For an acute episode, sleep is very effective in curing the pain. Non-prescription analgesics such as acetaminophen, ibuprofen or
naproxen are usually effective. Others may require combinations of metaclopramide plus
analgesics. Note that once an attack begins, the effectiveness of oral agents is reduced by decreased gastric motility and absorption.
Ergotamines (dihydroergotamine mesylate) have long been effective in the treatment of severe migraine. Sumatriptan, subcutaneously, has been proven effective in children, but the oral forms have been much less successful, and it is an expensive drug.
Deal with precipitating factors! Stress management techniques are important, as difficulty dealing with
stress is the most common precipitating factor. Biofeedback and relaxation techniques have demonstrated efficacy in
several studies, and should be a part of the treatment regimen. Prophylaxis is appropriate when the headaches interfere with the
child’s ability participate in school or activities. Some neurologists would consider prophylaxis reasonable when children suffer more than two incapacitating headaches per month or those who have recurrent complicated migraine.
Medications used for prophylaxis include amitryptiline, propranolol and cyproheptadine.
CONTINUITY CLINIC
Medication ReviewMedication Review MetoclopramideMetoclopramide - enhances GI motility and is an - enhances GI motility and is an
effective antinauseant effective antinauseant Ergotamines - administered to relieve migraine
headaches; the drug is roughly 70% effective in controlling acute migraine attacks
Sumatriptan - very specific for one subtype of serotonin receptors. It is approved for the treatment of migraine with or without aura, but not for long-term migraine prophylaxis or for the management of hemiplegic or basilar migraine. Although the efficacy of subcutaneous sumatriptan as an abortive agent in the treatment of migraine has been demonstrated, headache recurrence is a frequent problem.

Tension Tension HeadachesHeadaches

CONTINUITY CLINIC
Tension Headache - Tension Headache - HistoryHistory
Chronic stress or tension-type headaches are not very Chronic stress or tension-type headaches are not very common in the pediatric population before puberty and common in the pediatric population before puberty and represent a diagnosis of exclusion. represent a diagnosis of exclusion.
These headaches are characterized by a diffuse, symmetric These headaches are characterized by a diffuse, symmetric distribution in the frontal or occipital areas, often described distribution in the frontal or occipital areas, often described as bandlike.as bandlike.
The pain may be described as constant and aching, as The pain may be described as constant and aching, as opposed to the throbbing of migraineopposed to the throbbing of migraine
HA is usually accompanied by fatigue but not the nausea HA is usually accompanied by fatigue but not the nausea and vomiting of migraine or increased intracranial pressure. and vomiting of migraine or increased intracranial pressure.
Activities are usually not limited, although most occur Activities are usually not limited, although most occur during the school day and may be related to activities such during the school day and may be related to activities such as tests. as tests.
It is important to give the child the opportunity to share It is important to give the child the opportunity to share concerns and conflicts, as most can provide insight into the concerns and conflicts, as most can provide insight into the cause of the headache. One must also screen for depression cause of the headache. One must also screen for depression by asking about changes in mood, behavior, appetite, sleep by asking about changes in mood, behavior, appetite, sleep and withdrawl.and withdrawl.

CONTINUITY CLINIC
Tension Headache - Tension Headache - TreatmentTreatment
Education about how stress can cause headaches leads to a discussion about how to reduce anxiety or remove anxiety- producing situations
Biofeedback and self-relaxation techniques have a significant role in symptom management, and are most effective for a chronic headache
Analgesics such as acetaminophen and ibuprofen usually provide relief for acute headache

Increased Increased Intracranial Intracranial
PressurePressure

CONTINUITY CLINIC
Increased ICP - HistoryIncreased ICP - History Headache initially sporadic and occurs in the early hours of the
morning; it may also awaken the child. Pain is diffuse and generalized, usually in frontal or occipital
regions. It is exacerbated by movements that increase ICP (coughing, sneezing, straining and lying flat) and may be temporarily relieved by vomiting.
As ICP increases, the child may become more irritable or lethargic Physical exam with special attention to the neurologic exam
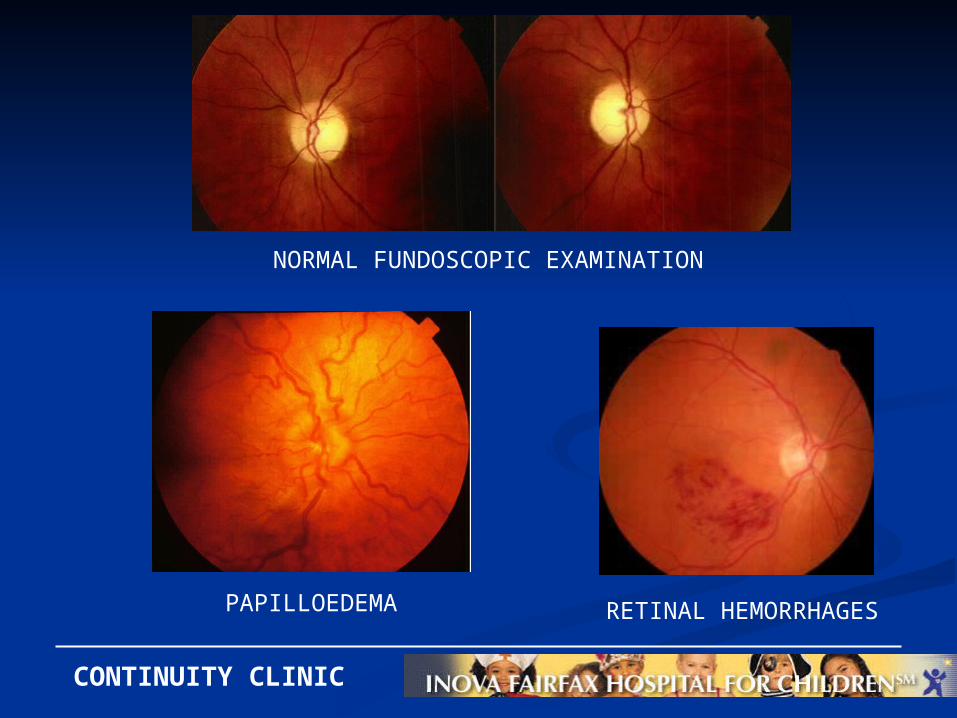
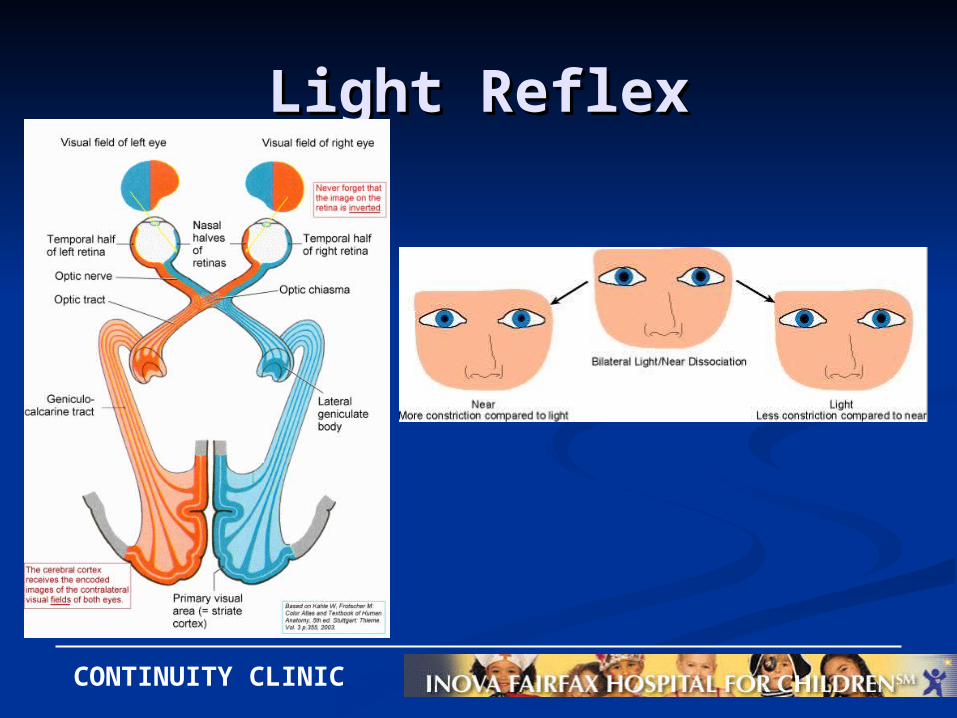
Cranial nerve abnormalities Defects in visual fields or acuity Changes in DTR or muscle strength Fundoscopic exam may reveal papilledema or retinal hemorrhage Check the pupillary exam for asymmetry of the light reflexes. Cranial bruit on exam may represent an arteriovenous malformation,
especially when asymmetric or eliminated by compression of the ipsilateral carotid artery.
Other important components of the physical include growth parameters (chronic illness, hypothalamopituitary dysfunction), head circumference, blood pressure and skin (trauma or neurocutaneous disorder).
CONTINUITY CLINIC
NORMAL FUNDOSCOPIC EXAMINATION
PAPILLOEDEMA RETINAL HEMORRHAGES
CONTINUITY CLINIC
Light ReflexLight Reflex

WARNINGWARNING
Cushing’s Triad (hypertension, Cushing’s Triad (hypertension, bradycardia and irregular bradycardia and irregular
respirations) is a late finding! respirations) is a late finding! Absence of these symptoms does Absence of these symptoms does
not eliminate the possibility of not eliminate the possibility of increased ICP.increased ICP.

CONTINUITY CLINIC
Increased ICPIncreased ICP
The most common causes of elevated ICP in children include hydrocephalus, brain tumors (esp. posterior fossa), subdural hematoma, cerebral abscess, meningitis/encephalitis, pseudotumor cerebri and chronic lead poisoning.
If elevated ICP is suspected, it is implicit that imaging is done before lumbar puncture.

ImagingImaging

CONTINUITY CLINIC
When to order?When to order? Abnormal neurologic signs on physical exam Acute increased frequency or severity of headache; overall
change in pattern Focal neurologic signs/symptoms during HA (complicated
migraine) Recent school failure, behavior change, fall-off in linear
growth rate HA awakens child during sleep, occurs in early morning with
increasing frequency or severity Brief cough HA in child or adolescent Visual graying out occurs at the peak of HA instead of at the
aura Cluster HA in a child; any child less than 5 years whose
primary complaint is HA Focal neuro signs/symptoms develop during the aura with
fixed laterality or occur at the peak of HA instead of during the aura
CONTINUITY CLINIC