Embed Size (px)
Citation preview

Treatment of vertebral hemangioma : what the
interventional radiologist can do ? Hatem Rajhi .MD
Department of Radiology and Interventional Radiology- Charles Nicolle Hospital
Tunis -Tunisia

PURPOSE
To illustrate through a series of
observations documented therapeutic
methods in the interventional treatment
of vertebral hemangiomas

INTRODUCTION
Vertebral Hémangioma (VH) • The most common benign tumor of the spine
• Multiple in 25% of cases
• Peak incidence: 40-60 years
• Slow-growing lesion
• benign vascular dysplasia
capillary
Cavernous (most common)
or Venous(Picture taken from website:www.back.com/causes-tumors-benign.html)

INTRODUCTION
When to treat a spinal hemangioma?
Usually asymptomatic, discovered incidentally.
Only 0.9% to 1.2% of cases become symptomatic:
Aggressive Hemangioma
Local pain,
Radiological aggressiveness
Neurologic deficit

Background: Semiology of vertebral HemangiomaRadiographic findings
Vertical striations and trabeculations“Honeycomb” appearence.
MRIincreased signal on T1- and T2 weighted images (intralesional fat)
CT axial image
“Polka dot” appearance of the involved vertebra

Signs of aggressiveness on imaging of Vertebral Hemangioma
• Spine level between T3 to T10
• Involvement of the entire vertebral body
• Extension to the posterior arch
• Discontinuous cortical bone
• Lytic appearence
• Paraspinal or intra ductal expansion
• Low signal intensity on T1-weighted images
• Intense enhancement after contrast injection

CASE N°1
A 18 years old patient
09/08/2007 Neurological dysfunction due to spinal cord
compression.
Radiographic findings: aggressive vertebral hemangioma T3
10/08/2007 bilateral T3 laminectomy
Follow-up: worsening paraparesis
Immediate revision surgery: epidural hematoma evacuation

• Significant improvement of motor deficit.• Histologic diagnose: capillary hemangioma

• April 2009 (20 months later)• High back pain• Spastic paraparesis • Bilateral Babinski signs

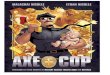
a b c d e
MRI sequencesa,b,c sagittale T2-weighted imagesd : sagittale T1 weighted images with contrast injectione : axial T1 weighted image with contrast injection
Is there an explanation for the current neurological symptoms ?

What could be proposed?
A. Reoperation
B. Transarterial Embolization
C. Surgery with preoperative embolization
D. vertebroplasty
E. Radiotherapy

What could be proposed?
A. Reoperation
B. Transarterial EmbolizationC. Surgery with preoperative embolization
D. vertebroplasty
E. Radiotherapy

What arterial branches to explore?
A. The celiac trunk and superior mesenteric artery
B. The dorsal intercostal arteriesC. The lumbar arteriesD. The thoracic and abdominal aorta

What arterial branches to explore?
A. The celiac trunk and superior
mesenteric artery B. The dorsal intercostal arteries
C. The lumbar arteries
D. The thoracic and abdominal aorta

Which embolic agent to use ?
A. Coils
B. Embospheres
C. Curaspon
D. Ethanol
E. Biological Glue

Which embolic agent to use ?
A. Coils
B. Embospheres
C. Curaspon
D. Ethanol
E. Biological Glue

Which embolic agent to use ?
A. Coils
B. Embospheres
C. Curaspon
D. Ethanol
E. Biological Glue

Which embolic agent to use ?
A. Coils
B. Embospheres
C. Curaspon
D. Ethanol
E. Biological Glue

Which embolic agent to use ?
A. Coils
B. Embospheres
C. Curaspon
D. Ethanol
E. Biological Glue

Which embolic agent to use ?
A. CoilsB. Embospheres
C. Curaspon
D. Ethanol
E. Biological Glue

The anterior spinal artery was identified in T10 left. Is there a risk of embolization of T3.
A. yesB. noC. Distrust

The anterior spinal artery was identified in T10 left. Is there a risk of
embolization of T3.
A. Yes
B. NoC. Distrust

Embolization
Right T4
Right T5

Selective angiography of the pedicle of the left T3 intercostal artery
We can embolize at this level?
A. Yes
B. No

Selective angiography of the pedicle of the left T3 intercostal artery
We can embolize at this level?
A. YesB. No

Surgical resection is limited because of:
A. The involvement of the anterior archB. The epidural extensionC. The involvement of the posterior arch

Surgical resection is limited because of:
A. The involvement of the anterior archB. The epidural extensionC. The involvement of the posterior
arch

What can we do ?
A. Surgery as part of the angioma was embolized
B. Vertebroplasty
C. Sclerotherapy with Absolute ethanol
D. There is no other treatment
E. There is another alternative ?

What can we do ?
A. Surgery as part of the angioma was embolized
B. Vertebroplasty
C. Sclerotherapy with Absolute ethanol
D. There is no other treatment
E. There is another alternative?

What does this alternative ?
A. radiofrequency ablation
B. direct embolization ?

What does this alternative ?
A. Radiofrequency ablation
B. Direct embolization ?

Which embolic agent to use ?
A. Ethanol
B. Coils
C. Embospheres
D. Biological Glue

Which embolic agent to use ?
A. Ethanol
B. Coils
C. EmbospheresD. Biological glue

Which type of radiographic guidance ?
A. Fluoroscopy
B. CT scanner
C. Ultrasonography

Which type of radiographic guidance ?
A. FluoroscopyB. CT scanner
C. Ultrasonography

Sclerotherapy with Glubran 2 by direct puncture under CT guidance

Sclerotherapy with Glubran 2 by direct puncture under CT guidance

Sclerotherapy with Glubran 2 by direct puncture under CT guidance

Sclerotherapy with Glubran 2 by direct puncture under CT guidance

Sclerotherapy with Glubran 2 by direct puncture under CT guidance

Is surgery indicated ?
A. Yes
B. No

Is surgery indicated ?
A. Yes
B. No

What time limits ?
A. In 7 days so that the inflammation decreases
B. In one month
C. Within 48 hours of embolization
D. The time limits is not important

What time limits ?
A. In 7 days so that the inflammation decreases
B. In one month
C. Within 48 hours of embolization
D. The time limits is not important

Surgery should include :
A. T 3 Laminectomy
B. T 3 Vertebrectomy
C. Laminectomy and osteosynthesis
D. Osteosynthesis

Surgery should include:
A. T 3 Laminectomy
B. T 3 VertebrectomyC. Laminectomy and osteosynthesis
D. Osteosynthesis

Osteosynthesis T1 to T6

• Favorable evolution with recovery of motor function of lower extremities.
• Is the treatment achieved ?
A . Yes
B . No

• Favorable evolution with recovery of motor function of lower extremities.
• Is the treatment achieved?
A . YesB . No

To treat vertebral body of T3 must be
associate :
A. Surgery by anterior approach
B. Percutaneous Vertebroplasty
C. Sclerotherapy with Glubran 2 under CT guidance

To treat vertebral body of T3 must be
associate :
A. Surgery by anterior approach
B. Percutaneous Vertebroplasty
C. Sclerotherapy with Glubran 2 under CT guidance

Percutaneous Vertebroplasty

Significant improvement with gait recoveryactually walking without cane

PERCUTANEOUS VERTEBROPLASTY

•Percutaneous injection of acrylic cement in
a pathologic vertebral body
•Double effet:
Pain relief
Vertebral stabilization
PERCUTANEOUS VERTEBROPLASTY

Patient preparation
Systematic radiological assessment: X-ray + CT + MRI
• Anesthesia consultation before the procedure.
• Informed consent obtained from the patient
• Search for contraindications
PERCUTANEOUS VERTEBROPLASTY

Absolute Contraindications
- Pregnancy;
- coagulation disorders;
- Contraindications to anesthesia and prolonged
prone position;
- Allergy to PMMA;
- Systemic or local infections;
- Spinal cord compression with neurological
deficit

- Pedicles fracture
- Vertebral body collapse with retropulsion of
fracture fragment causing spinal canal compromise
- Severe vertebral body collapse
Relative Contraindications

• Fluoroscopic C-arm• Guidance
• CT guidance
• General anesthesia or local analgesia with or without conscious sedation
Technique

Bone cement :PMMA
Bone Needles 11 G 10 cm (thoracic spine) 15 cm (lumbar spine)
Surgical hammerCombination pliers
Equipment

Methylmethacrylate powder is mixed with methylmethacrylate monomer liquid.
Metallic powder is added to PMMA in order to enhance the visibility of the cement.
The preparation is mixed until it becomes like toothpaste
Cement volume vary between 2 and 10 ml
Cement preparation

• Transpedicular approach Unipedicular or Bipedicular
Cement injection

Postero lateral approach - pedicular lysis - osteosynthesis
Cement injection

• Vascular leakage of cement - the operator should adjust the needle direction - or stop the injection immediately.
Risk of Pulmonary embolism
Incidents

Incidents
Spinal canal and epidural extravasation of cement- Low risk < 1 %
- Associated with vertebral fracture:
Pedicles posterior wall posterior arch

Incidents
Foraminal leakage of ciment
Risk of compression of the nerve root

Incidents
Paravertebral cement leakage
Intervertebral disc cement leakage
Without major complications

The analgesic effect is immediate and complete
in the vast majority of cases according to various
studies.
The frequency of complications is highly variable
depending on the series (1% to 13.5%)
It's mostly technical incidents without major
consequences
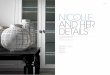
Vertebroplasty Results

H Rajhi and al in 2011: 100% improvement
at least partially in the short and medium term
Complete regression of pain in the medium term up
57.1% of cases
Vertebroplasty Results
SHORT TERM MEDIUM TERM0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Partial improvement
Significant improvement
Complete regression

CASE N°2 48 year old woman treated by percutaneous
vertebroplasty in 2008 for aggressive vertebral hemangioma T12 with improvement of symptoms.

• Re-consulted in March 2011 for development of inflammatory back pain with sciatica andsphincter dysfunction.

a b c d e fMRI sequencesa: sagittale T2 weighted imageb,c : sagittale T1 weighted imagesd,e : sagittale T1 weighted images with contrast injectionf: axial T1 weighted image with contrast injection

What is the explanation of the recent symptoms?
A. Herniated disc
B. Spondylodiscitis
C. Vertebral metastasis
D. Reactivation of aggressive Angioma T12
E. Osteoporotic fracture

What is the explanation of the recent symptoms?
A. Herniated disc
B. Spondylodiscitis
C. Vertebral metastasis D. Reactivation of aggressive Angioma T12
E. Osteoporotic fracture

Which procedure could be proposed as a treatment?
A. SurgeryB. Arterial embolizationC. Surgery with preoperative embolizationD. VertebroplastyE. Sclerotherapy with Ethanol

Which procedure could be proposed as a treatment?
A. SurgeryB. Arterial embolization
C. Surgery with preoperative embolizationD. Vertebroplasty
E. Sclerotherapy with Ethanol

• The decision was to achieve sclerotherapy with
ethanol injection in the anterior epidural component

Sclerotherapy with ethanol injection

Sclerotherapy with ethanol injection

Sclerotherapy with ethanol injection

Sclerotherapy with ethanol injection

The outcome was favorable with disappearance of sphincter dysfunction and sciatica
and improvement of the low back pain

Control MRI in April 2012 (1 year after sclerotherapy)
April 2011 April 2012

Control MRI in April 2012 (1 year after sclerotherapy)
April 2011 April 2012

SCLEROTHERAPY WITH ETHANOL
•Direct percutaneous injection of Absolute alcohol
•Induces:
Thrombosis, edema and sclerosis of the Hemangioma Shrinkage of the lesion with radiculomedullary decompression

Intraosseous venography can be performed before alcohol injection
Provides information on the route of preferential venous drainage of the hemangioma
Chek for risk of paravertebral and intra ductal leakage
SCLEROTHERAPY WITH ETHANOL

•CT guidance
• Intravenous conscious sedation and analgesia
Technique

-Without significantly changing the absolute nature of the alcohol, we have made alcohol radioopaque by mixing it with contrast media
• Transpedicular approach Unipedicular Bipedicular
• Postero lateral apparoch
Technique

Potential risk of venous runoff
- Avoided by slow injection of Ethanol
Pleural complications and intercostal arteries injury
- Avoided by transpedicular approach
Incidents

Risk of collapse of the vertebral body
-Decreased by injecting a small volume of alcohol
Complications

•A number of methods have been used in the
treatment of symptomatic and aggressive
vertebral hemangioma, but none of them is
optimal.
•The therapeutic approach depends on the clinical
context, the topography and the involvement of
the lesion.
•The decision is multidisciplinary
CONCLUSION

•The interventional radiologist plays an important
role:
- Knowledge of the limitations and benefits
of each Interventional procedure
- Changes in products available
- perfect control of techniques
- Risk Measurement
CONCLUSION

MERCI Thank you