Embed Size (px)
Citation preview

Suffolk County Medical Society
Suffolk Academy of Medicine
BULLETIN
VOLUME 89 No.1 www.scms-sam.org January 2012
HAPPY HOLIDAYS
The staff of the Suffolk County Medical Society & Suffolk Academy of Medicine would like to extend our best wishes for the upcoming New Year.
We thank you for your continued support and look forward to assist-ing you and your staff during 2012.
Stuart S. Friedman Barbara Baumgarten Donna DelVecchio
Linda LoPorto

2
Suffolk County Medical Society Officers July 1, 2011 - June 30, 2012
PRESIDENT Marc J. Yland, M.D.
PRESIDENT-ELECT Richard S. Zito, M.D.
VICE PRESIDENT George R. Ruggiero, D.O.
SECRETARY Maria A. Basile, M.D.
TREASURER William R. Spencer Jr., M.D.
EXECUTIVE DIRECTOR Stuart S. Friedman, MPS
OFFICE MANAGER/EDITOR Barbara Baumgarten
MEMBERSHIP Donna DelVecchio
EXECUTIVE SECRETARY/ Linda LoPorto
CME COORDINATOR
Suffolk Academy of Medicine Officers
July 1, 2011 - June 30, 2012
PRESIDENT Richard S. Zito, M.D.
VICE PRESIDENT George R. Ruggiero, D.O.
SECRETARY Maria A. Basile, M.D.
TREASURER William R. Spencer Jr., M.D.
January 11, 2012
March 21, 2012
May 23, 2012
Executive Committee Meetings Upcoming Meeting Times & Dates
All Meetings Begin at 6:00 PM at the SCMS Offices.
Board of Directors Meetings
These are open meetings to all members. Please contact the SCMS if you would like to attend a Board Meeting so appro-priate time can be provided on the agenda.
February 15, 2012
April 25, 2012
June 1, 2012 (Annual Meeting)
UPCOMING DATES TO REMEMBER IN 2012:
MSSNY State Legislative Day (Albany): Tuesday, March 20, 2012
Review of Resolutions: April 18, 2012
MSSNY House of Delegates (Saratoga): April 20-22, 2012
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
Happy Holidays And A Joyous
New Year

3
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
President Marc Yland, M.D.
Physicians have driven most advances in healthcare over the past 2 millennia. The practice of medicine is an art with scientific tools at its disposal. This remains true even today, despite many attempts by bureaucrats to legislate “evidence-based medicine.” There are few, if any examples
in which industry, or policy makers developed new successful treatments. Read the histories of vaccinations, organ transplantation, hemodialysis, vascular stenting, genome research, stem cell research, etc. Most of the time policy makers and industry were obstacles, until the cat was clearly out of the bag. Quality healthcare depends on having a strong physician community at the helm. The success of modern day medicine has turned healthcare into a windfall for many investors, and business leaders. The profitability of current treat-ments may well stand in the way of more effective future treatments. The cost of healthcare is preventing other industries from blossoming. Currently, we are in a situation in which physicians and patients are under siege by large business special interests. Please see the July and October Bulletins for references.
For a moment, let us compare healthcare with a car company. Consider physicians in the position of manage-ment, healthcare workers as personnel, and patients as the customers. In the healthcare business the bond-holders are the insurance companies, and bigpharma are the parts suppliers. The latter have taken charge of the company and forced physicians out of management. Now the parts suppliers have decided that we should all drive cars with 20 lights, even if we don’t need them. At the same time, the bond holders have eliminated all product warranties and ended new product development, leaving customers in the cold, while holding management responsible. Recently, a large franchise decided to hire physicians and nurses to staff walk-in clinics in their stores. The same franchise is a bulk wholesaler of pharmaceuticals and medical supplies. Does anyone really think that the treatments in these clinics are not going to be driven by what is already in store on the shelf, or whatever else the quarterly profit objective may be? We physicians need a seat at the table.
New York is about to embark on a bold new initiative allowing physicians to negotiate as a group with govern-ment and insurance companies. This bill has passed the senate with broad bipartisan support, and is going to the house next. We see this as a last resort effort to bring physicians back to the table and restore ownership. The insurance industry, the FTC, and others have objected and called this “unionizing.” They argue that union-izing would increase the already spiraling healthcare costs. Anybody who remotely knows physicians would understand this to be nonsense. For example, physicians are unlikely to ever strike. First of all, most of us couldn’t do this to our patients. Second, we are well educated hard working professionals that will move on to other endeavors when the obstacles to quality care for our patients become insurmountable. Most other countries have had negotiating bodies for physicians for decades. Indeed, the cost of healthcare is best con-tained in countries where physicians have a meaningful seat at the table. Most “socialized” countries have given up on traditional unions. In The Netherlands the age of retirement for all civil servants was recently in-creased to 67 from 65, and civil servant job protections were equalized with the private sector. The only ex-ception is military retirement at age 55. However, they don’t spend much on the military anyway. Even in Greece they never heard of the concept of “20 years of service” or “one election term” to satisfy a lifetime pension. In contrast, in Germany labor is working closely with management to propel productivity. Most un-ionized industries in this country are losing market share, and I am unaware of any new startups that are un-ionized. Generally speaking, in our country, unionization has become counterproductive for the industry and in the end for workers as well. A good example is our system of education. It is an axiom that our education system is the main reason for America’s lack of growth. We spend more money than anybody else on educa-tion, with far less to show for it. It takes us at least 2 years longer to educate a professional or a trade worker, then anywhere else. The depth and quality of training is not any better for it. Stress and unhappiness is high among teenagers that don’t have a sense of direction. I really don’t think we can continue to blame lack of re-sources, video games, parents, or government for this state of affairs. (Continued on pg. 4)

4
Tastefully Designed Office Features: 3 Examination Rooms, Physicians’ Consultation Room, Record Room
Separate Bathrooms for Staff and Patients, Private Kitchenette New Carpet, Newly Replaced Gas Heating and AC Units, Alarm Security System
Cable Ready, Wheel Chair Accessible, Ample Parking
For more information please call 631-831-7987
President Marc Yland, M.D. (Continued from pg. 3)
Instead of extending education we should be educating our youngsters faster than we used to. Clearly, our kids are growing into maturity faster than older generations did, both physically, and emotionally. Let us not stop them from growing intellectually. The new resources available in technology could facilitate this greatly. In short, physicians are well aware that innovation is the engine of progress, and are not interested in perpetuat-ing traditional unions.
In America, we have the human capital, the culture, and the entrepreneurial spirit to reaccelerate. However, innovation can only succeed in a somewhat level playing field. Today patients and physicians have the cards stacked against them. One day we all will be a patient to some degree, and when that time comes only a physi-cian, who can practice independently, will be able to provide quality, and compassionate care. Our specialty and professional societies are not allowed to negotiate with payers. Insurance companies and government are making decisions about patient care with full immunity, regardless of outcome. Premiums are escalating while benefits are reduced even though now we have a mandate for all of us to pay for insurance. Physicians need to be able to have their voices heard, and speak for our patients as equal healthcare team members. Contact your representative, support the Healthcare Consumer and Provider Protection Act (also known as the Physicians Collective Negotiations Bill (S3186A Hannon et al)/A2474A (Canestrari et al) please use the links on our web site or go to http://capwiz.com/mssny/state/main/?state=NY.
It is with Deep Regret We Announce the Passing of Dr. William E. Tesauro of Islip, L.I. Beloved hus-band of Patricia M. Tesauro, Loving father of Mimi (Charles) Tesauro, William E. (Kelly) Tesauro, Jr., Charles (Debra) Tesauro, Joan (C.J.) Tesauro, Christina Tesauro and Gabriella Tesauro. Grandfather of Ashley Rose, Quinn Morgan and Kelsea Joan. Brother of Gloria Bevilacque and the late Thomas H. Tesauro, Jr.
FURNISHED MEDICAL OFFICE AVAILABLE IMMEDIATELY FOR LEASE.
LOCATED IN A PRESTIGIOUS MEDICAL PROFESSIONAL PARK ON MAIN STREET IN SMITHTOWN
**COMING SOON NEW BENEFIT **
AVAILABLE ONLY TO SCMS MEMBERS
DOCBOOKMD DOCBOOKMD is a smartphone platform designed by physicians for physicians, DocBookMD provides doctors-on-the-go an exclusive HIPAA-compliant professional network to connect, communicate and collaborate. It is only available to SCMS mem-bers. More information to following in the next few weeks.
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org

5
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
Message From SCMS Councilor
Frank G. Dowling, M.D.
NEW YEAR BRINGS CHALLENGES AND OPPORTUNITIES
COLLECTIVE NEGOTIATIONS UPDATE—PASSAGE POSSIBLE IN 2012—IMPACT ALREADY SEEN Some may view 2011 with disappointment, while I would encourage physicians to view 2011 as a year when sig-
nificant steps were taken towards major achievements. Many of you may recall the sudden call to activism on liability reforms when the MRT (Medicaid Reform Team) recommended early in the year that liability reforms including a $250,000 cap on noneconomic damages would save N.Y. State $120 million or more per year. Additional savings for phy-sicians, hospitals and other facilities, likely would multiply savings that could then be used in giving care and would stop the medical “brain drain” that NY has faced the last several years with most residents and fellows leaving the state for better work opportunities than can be found in the current healthcare and liability climate in N.Y. State. In addition, the very difficult to measure but very real costs of defensive medicine would likely add further substantial savings of funds that can be used to give the high quality and efficient care that citizens of N.Y. deserve and the NY State physicians give to the best of their abilities. While the opportunity was lost when the cap was removed from the final budget that passed, liability reforms and a meaningful cap on noneconomic damages were actively discussed in N.Y. State as never before, finding some support in the Executive Branch, Senate and even some support in the Assembly. As the N.Y. State budget situation continues to be severe, and Albany leadership will again be forced to consider how to shave billions off the N.Y. State budget, it is inevitable that they will consider and debate meaningful liability reforms including the finan-cial benefits to N.Y. State and all citizens that can be achieved by a cap. While some legislative leadership remains strongly opposed, they do not wish to lose their seat or their sizable majority. They will respond to voter outcry on these issues. Physicians must be ready to call, email, and educate patients how this will decrease costs of care and greatly im-prove access to care.
The Healthcare Consumer and Provider Protection Act (also known as the Physicians Collective Negotiations Bill [(S3186A Hannon, et al)/A2474A (Canestrari, et al)] passed the Senate with bipartisan support by a wide 43-19 margin. When passed, this legislation will allow physicians to collectively negotiate contract terms/Utilization Review/policies and procedures, etc. with private insurance plans and to negotiate fees under certain conditions when a small number of plans dominate the market in an area of N.Y. State. MSSNY Division of Governmental Affairs staff and physician leader-ship have continued communications with the Executive Branch, Assembly and Senate leadership, and even the FTC to address reported concerns regarding potential to increase costs of insurance or care to N.Y. State or to citizens of N.Y. With half of the Assembly cosponsoring the legislation, as these concerns are addressed, we have realistic hopes that this bill can be brought to passage in 2012. Physician’s must be active on this issue and continue calls, letters, and emails to their legislators. In addition, physicians should be available to educate their patients as to how this legislation can im-prove their care by allowing docs to negotiate to improve contract terms that will allow better efficiencies, ability to seek insurance company approvals, and allow physicians practices to remain financially viable in N.Y. and to be more able to invest in technology and office improvements that will improve their care.
Thanks to the tremendous efforts of Charles Rothberg MD, other MSSNY physician leadership and DGA staff, an understanding was recently reached with United Healthcare to curtail the arbitrary use of “suspicion of fraud or abusive billing” to audit NY State physicians beyond the two years that N.Y. State law allows except in the case of fraud and abu-sive billing. As a result of this agreement, physicians will not be subject to audits beyond two years based on mere screening of billing data. Further looks back will occur only after direct patient chart audits uncover a serious problem that warrants further look back. See NONY (News of New York) December 2011 issue for further details. In my view, the fact that S3186A/A2474A passed the Senate and the bill has a realistic chance of passage in 2012, was a significant factor in the willingness of a large insurance carrier to work out an informal understanding on behalf of N.Y. State physicians. While those who oppose the bill might argue that the bill is unnecessary, we must remind Albany leadership that the opposite is true—the bill is absolutely necessary and is having a positive impact even before passage.
Stay tuned. Be ready to put your money where your mouth is. Contribute to MSSNYPAC so we can support the legislators who support patients and physicians. And of course be ready to make calls, send emails and letters, educate patients and meet with legislators regarding these vital issues. If each physician contributes just $100 per year to MSSNYPAC, N.Y. State physicians would have over $5,000,000 to advocate and support legislative allies. To learn more about MSSNYPAC, go to the following link: www.mssny.org/mssnyip.cfm?c=s&nm=MSSNYPAC.

6
Assistant Commissioner for MSSNY Governmental Affairs
Charles Rothberg, M.D.
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
BU I LD ING /MED ICAL OFF I CE FOR SALE 1850’s Federal Colonial Building on Main Street in Huntington.
Has been a physicians office for 60 years. Also has a rental apartment.
Prime Location 631-427-1690
Ezekiel Emanuel, in a recent New York
Times piece, is correct in his assertion
that cost savings (and outcome improvements) will be
realized if we focus on the sickest 10% of patients. But,
along with countless other policy “gurus” his solution
falls way short when he mischaracterizes payment
“bundling” as some sort of incentive toward these
goals.
Payment bundling, as described by Emanuel, is little
more than a cap on government payments, already no
incentive for innovation in healthcare. And, contrary to
Emanuel’s admonition, fee-for-service need not be the
enemy of innovation – while bad policy always is.
Proponents of bundling often cite those provider
groups that have had success with high touch or conci-
erge medicine. Sadly, these citations are made com-
pletely out of context. While some groups have indeed
achieved success, they did so by building upon the fee-
for-service experience, but not in its absence. Thus, it
is completely unreasonable to expect the success of
these groups to be replicated in a policy wonk’s
“bundled” world. Solely cutting provider resources
cannot drive innovation any better than asphyxia
would result in better oxygen metabolism.
A better strategy to drive both enhanced outcomes
and to achieve cost savings would be to enhance pay-
ments to providers. These payment enhancements
would be a catalyst that would first drive and then be
offset by the cost savings - savings realized through
better outcomes such as earlier interventions, im-
proved compliance and reduced hospital readmission
rates. That’s right - pay doctors to save money and im-
prove healthcare outcomes. Doctors already do pretty
much what they are paid to do, why not pay them to
innovate and to save money too?
It turns out that we have a long history of preventing
doctors from doing their own “bundling.” Policymak-
ers have long held the view that consumer interests
would be poorly served were doctors to collaborate on
an episode of care. But those same policymakers
would instead impose a third party (one motivated
solely by money) to do the “bundling” for us. It would
be more rational if physician engineered “bundles”
would see the same light of day as the ones envisioned
by Emanuel.
To achieve this, antiquated antitrust hurdles need to
be relaxed. This is necessary in order to permit the
necessary clinical integration, collaboration and robust
gain sharing strategies, where physicians share in the
cost savings they engineer, should be promoted rather
than be overly restricted.
But Emanuel’s most ill conceived notion is to task the
commercial payers to impose this payment methodol-
ogy upon physicians in lockstep with the government
payers – yet a further slap in the face to providers:
By shifting payer risk to providers he both fails to compensate physicians for that risk and fails to reward physicians for any savings that may result.
By coordinating payment “bundles” between Medicare and commercial insurers, Emanuel would impose all the tyranny of single payer yet introduce no offset of value for patients.
Policies, such as those promoted by Dr. Emanuel dem-onstrate two critical lapses:
The failure of policymakers to understand what motivates providers and physicians.
The failure to identify the existing barriers to integration faced by physicians.
This embrace of faulty and unproven notions leads to an unnecessary and counterproductive solution.

7
Institutional Membership Initiative – A Physician’s Perspective
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
For those of you who do not know me, my name is Maria Basile. I am a colon and rectal surgeon with a private practice in Port Jeffer-son, and have been a member of the medical
staff at John T. Mather Hospital since October of 2000. I am currently serving a year as Secretary of the Suffolk County Medical Society. I have been tasked by our leadership, Dr. Philip Schrank and Dr. Kara Kvilekval, to outline the benefits of our Medical Staff’s Institutional Membership with the Medical Society, to help you understand how our Institu-tional Membership has helped us – individually, as a medi-cal staff, and as a profession.
Individually, this membership has saved me, and at least 500 of you, my colleagues, more than $850 in individ-ual dues to SCMS and MSSNY.
Because of our institutional membership, 4 CME courses were brought to us and professionally taught on site on timely topics of our own choosing, such as:
Preparing Your Practice for an Audit
Accountable Care Organizations
Electronic Health Records/ Meaningful Use
Clinical Integration
Future offerings could include
ICD-10 Implementation
Employment Law
Captive PCs and IPAs
The MSSNY House of Delegates is my favorite opportu-nity to see firsthand how issues important to individual phy-sicians can shape and even become Medical Society Policy. At the Womens’ Caucus this spring I was exposed to the different ways that female physicians from all over New York State and at varying points in their career still navigate cloaked, hurtful, or thoughtless comments about women in our profession – how they balance home, family, and work-life demands, and explore new models of part time practice or manage reentry into full time practice after maternity, family health, or academic leave.
I witnessed how Dr. Schrank followed issues that spoke to his interest in Sports Concussion through the process of creating resolutions that protect and promote the issues important to doctors and watch them be considered, de-bated, voted upon, and adopted, or not adopted by the House.
I have sought individual legal support from the medical society for answers about ethical and legal matters, employ-ment contracts, and their ombudsman services against managed care companies’ administrative harassments.
This year our Medical Staff, its leadership and commit-tees, has also sought legal advice from MSSNY. Senior Counsel, Donald Moy, Esq. was able to attend a meeting of our medical leadership and ad-hoc committee on Captive PC’s to give an opinion on changes to our bylaws to accom-modate changing practice models and alignment strategies with our hospitals and what these changes mean in terms of
Medical Staff privileges. We should continue to seek MSSNY’s guidance as we revise our Medical Staff Bylaws to comply with MS 01.01.01 Joint Commission standards.
Because of our Medical Staff’s Institutional Member-ship, MSSNY Legislative Day was improved. Our Medical Staff at Mather and St. Charles Hospitals was chosen as one of 9 Remote “Satellite” nodes for live Internet streaming of the Physician Town Hall Meeting in Albany, an exciting new format designed to bring Physician Lobby Day to the com-munities where MSSNY members are practicing.
Because of our pioneering efforts as a Joint Medical Staff taking this leap to join MSSNY as an institution OTHER HOSPITAL STAFFS HAVE FOLLOWED suit. The entire Albany Medical College Faculty Practice, St. James Mercy Medical Center in Steuben County have joined as Institutional Mem-bers, and MSSNY is currently negotiating with 7 other insti-tutions using our model for Institutional Membership.
We ARE becoming the change we want to see in this world.
This year Medical Liability Reform has become part of budget discussion at the New York State level. At the na-tional level, our New York delegation was a vocal contin-gency to the AMA, pushing them to readopt a stance to have Med Mal Reform as part of the National conversation. “Med Mal Reform IS Health Care Reform,” was the mes-sage from NY to every other state delegation.
At a recent Legislative Breakfast at Suffolk County Medi-cal Society headquarters, I was so proud to watch our own Dr. Paul Lograno, speaking as president on behalf of his lo-cal specialty society, strategize and engage a room full of legislators emphasizing how critical Physician Collective Ne-gotiation would be to level the playing field between physi-cians and managed care.
These past few weeks thousands of people have been involved in the “Occupy Wall Street” protests in New York City and other cities around the world. Participants are be-ing roundly portrayed and criticized for being fractured, fringe actors, obstructionist, too individualized in motive, and lacking in a unified message.
OUR MEDICAL STAFF IS DIFFERENT in that we have found a way to use our numbers effectively to serve our priorities. We HAVE brought a unified voice to issues like Med Mal Reform and Physician Collective Negotiation to and through the NYS Legislature, the Governor’s office and into the National Conversation.
We HAVE found a way to harness all the trust, compas-sion, stability, and hope that we use each day with our pa-tients and each other to OCCUPY MEDICINE even as we con-tinue to practice medicine. This is how it has been with our institutional membership with the Suffolk County Medical Society and the Medical Society of the State of New York, and I want to thank each of you for what you have done to make this way a reality and as always for your kind atten-tion.

8
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
A Message From Your Executive Director Stuart S. Friedman, MPS
It seems like I just finished writing my 2010 year-end message and here we are at the beginning of another year. Your medical society has been extremely busy during 2011 under the expert guidance and leadership of SCMS President Marc J. Yland, MD.
A very successful legislative breakfast was held at the medical society offices and attended by almost all our Assembly and Senate representatives. Paul A. Hamlin, MD, MSSNY President and Robert A. Scher, MD, MSSNY Chair of The Board of Trustees were also in attendance and provided keen insight into many of the concerns of the physician community. The major topics of discussion centered around Albany’s deficit and its impact on healthcare in New York State, physician’s collective negotiations legislation and medical liability proposals. As with previous meetings of this type, the majority of legislators commented on the knowledge and expertise of our doctors and how much they enjoy and learn whenever they meet with us. While they may not always agree with everything we are looking to accomplish, they welcome the opportu-nity to enter into honest and open discussions.
Frank G. Dowling, MD, SCMS Councilor has been extremely active in helping to secure passage of Physician’s Collective
Negotiations legislation. As I am sure you are all aware, S3186/A2474 had passed the Senate by a 43-19 margin, with bi-
partisan support (with all four Suffolk Senators voting in support). Unfortunately, it has never come up for a vote in the
Assembly. (It is interesting to note also that almost all of our Assembly representatives had indicated that they would vote
for the bill if and when it is brought to the Assembly floor.) The bill will come up again when the legislature reconvenes in
2012.
With the Joint Select Committee on Deficit Reduction failing to reach any agreement on a deficit-reduction proposal, as of this writing, physicians still face a 27.4% cut in Medicare physician payments scheduled to take effect January 1, 2012. Congress has once again missed an opportunity to address the nation’s fiscal problems, stabilize the Medicare program and permanently repeal the flawed Sustainable Growth Rate (SGR) formula. We have heard that there is support in both chambers for legislation which would, among other things, include a two-year temporary fix to the Medicare physician payment crisis. While this obviously stops the 27.4% cut scheduled for January 1st, it will lead to a 37% cut on January 2014. We continue to urge members of Congress to once and for all, fix the problem and not create a larger fiscal debt for the Medicare program.
Extensive lobbying has also resulted in the elimination of a scheduled 3% tax withhold for Medicare payments. The stat-ute, originally passed in 2006, called for ALL federal, state and local government payments to individuals providing “goods and services,” to have 3% of the payment withheld until the following tax year.
I am also pleased to report that Senator Lee Zeldin has been instrumental in having the MTA payroll tax repealed. More than 700,000 employers, including physicians, currently paying this ridiculous tax, will see its complete elimination. Thanks Senator Zeldin for following through on your campaign commitment.
It is that time of the year again when I ask (implore) those physicians who have not yet paid their membership dues to give serious thought to what their future would be without organized medicine’s involvement on a county, state and national level. Do they honestly believe that they would be better off acting on their own without the influence, clout and over-sight which accompanies their membership? An unfortunate reality is that many physicians unwisely weigh their decisions to continue membership based solely upon the overall cost of dues. I would submit that in the long run, the cost of not belonging would be far greater. Medical societies, whether they are specialty, county, state or national, exist to protect and advocate for the interests of their members. While some of the decisions made by these organizations may, at times, be reviewed as “unpopular” or “incongruent with” a physician’s practice environment, political affiliation or philosophical outlook, it is important to remember that only organized bodies of medicine have the structure, manpower and expertise to be invited to provide opinion and commentary. Please understand that without your ongoing support, we become im-potent in our ability to continue to effectuate meaningful change and to provide input into those issues which affect both your professional and personal lives. While your dues dollars enable us to continue to represent you, your membership and participation will enable you to continue to have a voice in your future and in the future of your profession. With the many challenges now facing the medical profession, it is time for ALL physicians to come together and speak as one voice. If we are divided, we will not survive.
Please allow me to take this opportunity to wish everyone a joyous holiday season and a very happy and healthy new year.

9
PUBLIC HEALTH PAGE
From the Office of James L. Tomarken, MD, MPH, MBA, MSW, FACP, FRCPC
Commissioner of the Suffolk County Department of Health Services
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
SEASONAL INFLUENZA
Seasonal flu season 2011-2012 is here. Influenza is a contagious respiratory illness spread by coughing, talking, or sneez-ing droplets. It can also be spread by touching a surface that has the virus on it and then touching ones mouth, eyes or nose. The virus can be spread by people before they are symptomatic or while sick. The contagious period is from one day before symptoms to up to 5-7 days after developing symptoms. Children and those with impaired immune symp-toms may be able to spread the virus for longer periods.
The severity of flu illness varies depending on several factors — the particular virus, availability of vaccine, number of people vaccinated and the efficacy of the vaccine.
The usual symptoms include:
Fever or feeling of fever
Cough
Sore throat
Runny nose or congestion Myalgia
Headaches Fatigue
Children may have diarrhea and vomiting
Complications
Complications include bacterial pneumonia, infections of the ears and sinus, and dehydration. Chronic conditions such as asthma, diabetes and congestive heart failure may be worsened.
Prevention
The most effective method of prevention is the annual vaccination. The vaccination period begins in September of each year or as soon as the vaccine becomes available. The flu season runs from October through May of the following year with peaks generally in January or February or later.
Vaccination Candidates
All those 6 months and older are eligible for vaccination yearly. Those individuals susceptible at high risk of complica-tions or who care or live with people at high risk of complications should receive a flu vaccine. Those at risk of complica-tions are:
Children less than 5 years of age, especially younger than 2 years
Adults 65 years of age and older Pregnant women American Indians and Alaskan Natives
People with medical conditions including: Asthma-controlled or not Neurological and neurodevelopmental conditions Chronic lung disease (such as chronic obstructive pulmonary disease [COPD] and cystic fibrosis) Heart disease (such as congenital heart disease, congestive heart failure and coronary artery disease) Blood disorders (such as sickle cell disease) Endocrine disorders (such as diabetes mellitus) Kidney disorders Liver disorders Metabolic disorders (such as inherited metabolic disorders and mitochondrial disorders) Weakened immune system due to disease or medication (such as people with HIV or AIDS, or cancer, or those on chronic steroids) People younger than 19 years of age who are receiving long-term aspirin therapy People who are morbidly obese (Body Mass Index [BMI] of 40 or greater) (Continued on pg. 10)

10
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
PUBLIC HEALTH PAGE (Continued from pg. 9)
People who live in nursing homes and other long-term care facilities
People who live with or care for those at high risk for complications from flu, including: Health care workers Household contacts of persons at high risk for complications from the flu Household contacts and caregivers of children younger than 5 years of age with particular emphasis on vacci-nating contacts of children younger than 6 months of age (children younger than 6 months are at highest risk of flu-related complications but are too young to get vaccinated)
Those who should not receive vaccination
People who have ever had a severe allergic reaction to eggs. People who have had a mild reaction to egg—that is, one which only involved hives—may receive Trivalent Inactivated Vaccine (TIV) with additional precautions. People should make their healthcare provider aware of any allergic reactions.
People who have ever had a severe allergic reaction to influenza vaccine.
People with a history of Guillain–Barré Syndrome (GBS) that occurred after receiving influenza vaccine and who are not at risk for severe illness from influenza should generally not receive vaccine.
People under 65 years of age should not receive the high-dose flu shot.
People who are under 18 years old or over 64 years old should not receive the intradermal flu shot.
If one is sick with a fever when one goes to get a flu shot, one should postpone receiving the vaccination. One can get a flu shot at the same time they have a respiratory illness without fever or with another mild illness.
Pregnancy
Pregnant women who get influenza vaccine pass their immunity to their babies in the form of flu antibodies. This protec-tion lasts for several months after birth. Influenza protection was seen in newborns up to four months old. Babies born to women who were not vaccinated during pregnancy showed no antibody protection.
Vaccines
The influenza (flu) viruses selected for the seasonal flu vaccines are updated each year based on information about which influenza viruses are being found, how they are spreading, and how well the previous season's vaccine viruses might protect against any that are being newly identified. Currently, 136 national influenza centers in 106 countries con-duct year-round surveillance for influenza viruses and disease activity. These laboratories then send influenza viruses for additional analyses to the five World Health Organization (WHO) Collaborating Centers for Reference and Research on Influenza, which are located in Atlanta, Melbourne, London, Tokyo, and Beijing.
The seasonal flu vaccine is a trivalent vaccine (a three-component vaccine) with each component selected to protect against one of the three main groups of influenza viruses circulating in humans. It is not 100% effective. It takes two weeks after the vaccination for a person’s body to build immunity for protection against influenza.
Three vaccine viruses are chosen to maximize the likelihood that the influenza vaccine will protect against the viruses most likely to spread and cause illness among people during the upcoming flu season. WHO recommends specific vac-cine viruses for influenza vaccine production, but then individual countries make their own decisions for their country. In the United States, the U.S. Food and Drug Administration determines what viruses will be used in U.S.-licensed vaccines.
Treatment
Antiviral treatment is recommended as early as possible (ideally within 48 hours of symptom onset) for any patient with confirmed or suspected influenza who
is hospitalized;
has severe, complicated, or progressive illness; or
is at higher risk for influenza complications.
Antiviral Medication
Influenza antiviral prescription drugs can be used to treat influenza or to prevent influenza.
Two FDA-approved influenza antiviral medications are recommended for use in the United States during the 2011-2012 influenza season: oseltamivir (Tamiflu®) and zanamivir (Relenza®).
Oseltamivir and zanamivir are chemically related antiviral medications known as neuraminidase inhibitors that have activity against both influenza A and B viruses.
Reference: CDC Seasonal Influenza (Flu) Accessed December 3, 2011.Retrieved from http://www.cdc.gov/flu/

11
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org

12
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
Legal Page: From the Office of Ruskin Mouscou Faltischek, PC Recommended New Year's Resolution:
Wage and Hour Compliance By: Jeffrey M. Schlossberg, Esq.
It is without question that government agencies and plaintiffs' attorneys are continuing their focus on employ-ers who are not complying with the minimum wage and overtime provisions of the Fair Labor Standards Act ("FLSA") and the New York State Labor Law. Two recent developments underscore an employer's need to focus its attention on wage and hour compliance. There is no time like the start of a new year to address this critical and potentially costly issue.
U.S. Department of Labor Recovers Over $2.3 million from Long Island Employers.
The U.S. Department of Labor recently announced that an ongoing enforcement initiative conducted by its Wage and Hour Division has found widespread noncompliance with the minimum wage, overtime and record-keeping provisions of the Fair Labor Standards Act among full-service restaurants on Long Island. As a result, the DOL completed 46 investigations and recovered $2,341,507 in back wages for 578 employees. In addition, the DOL has assessed $202,315 in civil money penalties against employers for willful and repeated FLSA viola-tions.
Secretary of Labor Hilda L. Solis said, "The Wage and Hour Division will continue to monitor full-service restau-rants and other industries in which unlawful pay practices are widespread."
When violations are found, the division is using all enforcement tools available - including litigation, adminis-trative subpoenas, civil money penalty assessments and liquidated damages – to ensure accountability and de-ter future violations.
Immigration Status Not Relevant to Wage and Hour Claim
Earlier this month, a federal judge in Manhattan ruled that an employee's immigration status and national ori-gin are irrelevant in determining whether the employee is entitled to minimum wage and overtime for time worked.
The Court distinguished the case from a 2002 United States Supreme Court decision that denied back pay to an undocumented immigrant who had fraudulently gained entry to the United States. In the Supreme Court case, the back pay was for a time period following an unlawful termination where the employee did not actually work.
In the recent case, the undocumented worker actually performed work but the employer did not adhere to the provisions of the FLSA. The federal judge stated that permitting "a claim for back pay on behalf of undocu-mented workers who earned, but were not paid, overtime wages vindicates not only the policy underlying the FLSA but also federal immigration policy." The court went on to note that the opposite result would permit an employer to be immunized from its duty to pay wages. Further, denying back pay would create a "backwards incentive" where an "unscrupulous employer seeking to minimize wages would have a strong temptation to hire illegal workers."
Please let us know if we can be of assistance in helping you address wage and hour issues. We can assist in
conducting an audit of your procedures as well as an analysis of the exempt vs. non-exempt classifications of
your employees.

13 Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
Top EHR Implementation Tips From The AMA:
Many practices rush into implementing electronic health record (EHR) systems and other forms of health information technology (IT). With federal incentives now in place, it is especially important for practices to slow down, plan and be strategic about their decisions. Prolonged productivity loss or abandoning a system is the last thing any practice can afford. You and your practice can avoid popular missteps by following a few fundamental rules of thumb.
1. Plan. Planning is key. Implementing an EHR is large under-taking for any practice, and your success depends upon how diligently you plan. Begin by appointing a project champion, or maybe two—one physician and one administrator—followed by a project team. The team should represent leaders who will manage and have ownership of the project. The team should meet regularly and outline each stage of the preparation, selection, implementation, deployment and optimization of the EHR.
2. Focus on people and change management. Getting the whole practice on board is key to your success. IT-related projects, no matter the industry, have a high failure rate1 that is largely due to poor change management. Remember, an EHR system will likely change the roles and duties for every staff person, which, in turn, can lead to fear and anxi-ety. Change of this magnitude changes the culture of the practice. So it’s important for the project champion(s) and project team to address staff concerns openly. All staff must feel his or her feedback is important and that the change is in the best interest of the practice and its patients.
3. Communicate. Communicating the business case for change will help the staff see the reasons for the change. It’s best to have a written vision statement. You must prove to the staff that the HER system represents an improvement over your current paper process. Keep constant communica-tion with staff throughout the project. Continue to identify the perceptions and sources of resistance. Spend more time working with staff members who are less comfortable with technology. They might just end up being superusers!
4. Select the right system. Many EHR options exist today. Some systems are more robust, others offer more limited functionality. Keep in mind that to be eligible for the current federal incentives for EHR you must use “Certified EHR tech-nology” as defined by the Department of Health and Human Services. Certified EHR technology may come in the form of a “complete EHR” or a combination of “EHR modules.” Find certified EHR technology here. EHR systems can also be ac-cessed differently. Some systems are installed on a server in your practice; other systems are hosted by application ser-vice providers and accessed via the Internet. The key is to
identify which system best fits your needs. You may only need basic functionality; anything else may be distracting or go unused. You may also opt to have someone else maintain and upgrade the EHR. This can save you a large upfront in-vestment, and you won’t need IT resources to maintain the system.
5. Visit practices. If at all possible, visit a practice that uses the EHR system you are considering. This will give you a far better idea how the system will work in a real practice than a vendor’s demonstration.
6. Document workflows/processes. Before you can imple-ment an EHR system, you must understand how your entire practice operates. Consider such things as patient flows for different types of visits, point-of-care documentation, in-office communication and document management (e.g., dealing with paper information you receive from other sources). After documenting these processes, you can begin to plan for new processes with the EHR. Once the system is in place, you can modify and finalize your processes.
7. Determine data conversion method. Moving data from the paper chart into the EHR is major concern for many practices. Determine a process to get information from pa-per charts pre-loaded into the EHR. Remember, before you go live, you will need to load demographic data for all pa-tients from your practice management system (or billing service). Most practices will also enter certain basic data into the EHR for about 20 percent of patients—most typi-cally those with chronic illnesses, those with an upcoming visit, and those with a history of several visits in the past year. Preload these patients’ active problem and medication lists and their allergies. Some practices also add data from the most recent diagnostic studies (e.g., ECGs, mammo-grams, colonoscopies). Create a checklist of each item to ensure that all items have been collected and entered into the EHR.
8. Train and re-train. One-day training will not yield the type of system use you need. Staff will need training before “go live” and after. Taking on smaller pieces of technology may help make your staff’s transition easier. There is nothing wrong with training staff to use the computer, then the practice management system, electronic prescribing and other small applications, and finally the EHR.
9. Avoid too much customization. A thorough system selec-tion process should get you close to choosing a system you can use without modification. While it’s tempting to think you need customization, it will invariably cost you time and money. Instead, focus more on learning the system as it is designed and on selecting from the options provided.

14
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org

15
ALAN D. KAHN, CPA, MBA, CLU, ChFC THE AJK FINANCIAL GROUP
33 Queens Street, Suite 102, Syosset, NY 11791 Tel. (516) 677-0270 l Fax (516) 677-0273
www.ajkfinancialgroup.com
Endorsed Estate & Retirement Planners For the Suffolk County Medical Society
RETIREMENT PLANNING FOR 2011 & 2012!!!
UPDATING YOUR ANNUAL QUALIFIED RETIREMENT BENEFIT LIMITS
The Internal Revenue Service recently announced the 2012 inflation-adjusted Pension Plan Limi-tations, which are detailed below. In summary, there were some changes to contribution limits because the increase in the cost of living index met statutory thresholds that triggered their ad-justment.
Remember, the key advantage to qualified retirement plans is that your contributions are tax de-ductible and grow tax-deferred. This will result in more dollars for your retirement years. In ad-dition, for most readers who are self-employed, there is tremendous flexibility in selecting the appropriate plan to maximize your contributions.
QUALIFIED PLANS - MAXIMUM ANNUAL CONTRIBUTION
Don't forget the "catch-up provisions" for those individuals who are age 50 or older!! These additional amounts will not only save on your taxes, but also will help cushion your retirement nest egg!!!
Determining Your Best Retirement Program!!!
The key to maximizing your retirement contributions and minimizing your taxes today is to select a re-tirement program that works best for your professional practice.
AND REMEMBER, PEOPLE DON'T PLAN TO FAIL, THEY JUST FAIL TO PLAN
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
Type of Plan 2011 2012
Defined-contribution plans/SEP Plans $49,000 $50,000
Defined-benefit plans $195,000 $200,000
401(k), 403(b) and 457 plans
50 + Catch-up
Total for 401(k), 403(b), and 457 plans
$16,500
$5,500
$22,000
$17,000
$5,500
$22,500
Savings incentive match plans for employees (SIMPLEs)
50 + Catch-up
Total for SIMPLEs
$11,500
$2,500
$14,000
$11,500
$2,500
$14,000
Traditional and Roth IRAs
50 + Catch-up
Total for Traditional and Roth IRAs
$5,000
$1,000
$6,000
$5,000
$1,000
$6,000

16
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
Electronic Medical Records and Electronic Health Records What's the difference between EMR and EHR?
The terms Electronic Medical Record (EMR) and Electronic Health Record (EHR) are often used interchangeably. Technically, there is a distinction, but it's one that's been blurred by common usage. At a minimum, EMR systems replicate all aspects of your paper charting. They are designed to facilitate all the documentation you do in your office already—lab results, visit notes, diagnostic test results, insurance information, demographics, health histo-ries, medication information, and more.
EHRs, on the other hand, are essentially EMRs with the capacity for greater electronic exchange; that is, they may be able to follow patients from practice to practice and allow for things like data exchange and messaging between physicians.
What they do?
EHR systems can help physicians and office staff better navigate patient information before, during and after an office visit. Here are just a few of the multiple things that an EHR system may capture during a typical clinical visit.
Before a patient even steps into your office - manage scheduling, patient registration and insurance status, health history, medication lists; electronically preview a patient's medical history.
During a patient's clinical visit - type in your clinical documentation, electronically prescribe medication, order tests and labs.
After the patient leaves - manage billing, claims submittal and coding. Electronically communicate with their con-sulting providers, payers, labs and pharmacies. In some cases, allow patients to view their results through a patient portal.
Who is using them?
EHRs are quickly becoming the norm in many physician practices. As more practices adopt EHRs, the more effective they become as the circle of physicians who are able to "speak" to each other widens.
What they require?
While some EHR systems are more robust than others, the functionality of an EHR system can be defined within the context of patient care: pre-visit functionality, visit functionality and post-visit functionality. Evaluate which functions are important to you and your practice before you begin talking to vendors.
Things to consider
If you have an existing practice management system (PMS), talk to your vendor to make sure that any proposed EHR will "talk to" the PMS you're currently using. These systems need to connect to ensure the patient's insurance, demographics, coding and billing information are exchanged between the two applications. In some cases it is more cost effective to choose an integrated PMS/EHR, which means replacing your PMS instead of paying to inte-grate your current system and the EHR.
Certified EHR technology
The Centers for Medicare & Medicaid Services states that Certified EHR Technology is either a:
Complete EHR that meets the requirements included in the definition of a Qualified EHR and has been tested and certified, or a
Combination of EHR Modules in which each constituent EHR Module has been tested and certified and the re-sultant combination also meets the requirements included in the definition of a Qualified EHR. Link:
http://www.ama-assn.org/ama/pub/physician-resources/health-information-technology/health-it-basics/emrs-ehrs.page#

17
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
Electronic Prescribing Systems
What they do?
Electronic prescribing (ePrescribing or eRx) transmits prescription or prescription-related information between a prescriber, dispenser, pharmacy benefit manager or health plan. ePrescribing includes, but is not limited to, two-way transmissions between the physician practice and the phar-macy that can allow you to:
Manage all your patients’ prescriptions from your computer, including receiving electronic notification when you need to authorize refills
View potential drug interactions, side effects and potential allergic reactions—as an added benefit, decision support is often integrated into these systems
View prescription drug coverage and insurance information
Who is using ePrescribing?
For many physicians, ePrescribing is an attractive and intuitive first step into health IT. Physicians can choose to implement an ePrescribing system without implementing other health IT applications.
What it requires?
There is a wide range of e-Prescribing systems and functionality. To help you navigate your options and choose a system that meets your practice’s needs, you may want to visit Zero-InRx™, the AMA’s ePrescribing Learning Center.
“Electronic systems can check each prescription as it is written, either for internal inconsistencies such as excessive dos-age or for conflicts with the patient’s known allergies, interactions with other active medications, duplicate therapy and many other conditions.”— eHealth Initiative. Electronic Prescribing: Toward Maximum Value and Rapid Adoption, 2004
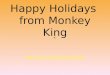
(Left to Right): Moe Auster (MSSNY DGA), Paul Hamlin, MD (MSSNY President), Sam Unterricht, MD (MSSNY Vice Presi-dent), Senator Charles Schumer, Joseph Sellers, MD (MSSNYPAC Chair), Andy Kleinman, MD (MSSNY Treasurer), Charles Rothberg, MD (MSSNY Assistant Treasurer), Rick Abrams (MSSNY EVP)
MSSNY Meeting With Senator Charles Schumer

18
LPIX AND NYCLIX HAVE JOINED TO BE HEALTHIX, Inc. ™ By Jason S. Thaw — Outreach Manager for LIPIX
RHIO Merger Overview Two of New York State’s largest Regional Health Information Organizations, or RHIOs, are merging to form the largest ac-tive RHIO in the country. The New York Clinical Information Exchange (NYCLIX), and the Long Island Patient Information exchange (LIPIX), are combining their technologies, operations and governance. The merged entity will be called Healthix Inc. ™ and will be headquartered in Manhattan.
Healthix's membership includes over 100 healthcare organizations including hospitals, long-term care and rehabilitation centers, homecare agencies and large ambulatory practices throughout downstate New York. In a joint statement, Dr. Benjamin Stein, Chief Executive Officer of LIPIX and the new CEO of Healthix, and Dr. Gil Kuperman, Executive Director of NYCLIX, said they were “proud that our two organizations could overcome competitive concerns and come together in a spirit of collaboration that should change the landscape of health information technology throughout the region and the country.”
Healthix™ Service Offerings
Clinical Viewer
This service enables clinicians to securely, easily, and comprehensively view relevant clinical information, such as lab val-ues, radiology reports, discharge summaries and other documentation on their patients when the clinician needs it most. The Clinical Viewer not only allows clinicians access to information from their own organization, but also enables clinicians, with their patients’ permission, access to clinical information from the entire Healthix™ network of care provid-ing organizations:
Lab Test Results
Radiology Reports
Discharge Summaries and Other Clinical Documentation
Procedure Information
Allergy Information
And Much More…
Clinical Event Notification
This service enables Healthix participants to subscribe to and receive notifications of specific events that occur during the course of their patients’ care, such as the registration of a patient into an Emergency Department or admission of a pa-tient to a hospital. Messages can be received via secure fax, secure email, or direct delivery into a provider’s EHR through standard HL7 or CCD messaging.
Clinical Information Distribution This service enables Healthix participants to subscribe to and receive clinical result information on their patients, such as a lab results, radiology reports or discharge summaries from any Healthix participating facility. Messages can be received via secure fax, secure email, or direct delivery into a provider’s EHR through standard HL7 or CCD messaging.
HealthBook™ This product offers a suite of services that facilitate effective and secure clinician to clinician communications and clini-cian to patient communication.
Appointment Scheduling:
Allows patients to find, schedule and manage appointments with clinicians through an easy to use web interface.
Clinician to Clinician Secure Messaging:
Through basic free-form text or templates customized for your needs
Clinician to Patient/Proxy Secure Messaging:
Through basic free-form text or templates customized for your needs
ePrescribing This service enables Healthix participants to check patient insurance eligibility and formulary for brand medications, and send their prescriptions electronically to either retail or mail order pharmacies.
Medication Reconciliation This service enables Healthix participants to easily perform well informed and complete medication reconciliations for their patients during transitions of care or other points in patient care.
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org

19
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
EMERITUS COMMITTEE DOINGS Sheldon Feinberg, MD, Chair
Stephen Green, MD, Co-Chair
Yale Solomon, MD, Co-Chair
Heretofore, our Committee has pursued ideas, with members working as a group. But now, each member is engaged in pursuing his or her own area of individual interest. That’s a new and exciting way to conduct the business of our committee.
For example, Doctor Al Stahman has decided to improve our Emeritus Committee’s SCMS Personal Repre-sentative Form, and Doctor Yale Solomon has suggested that we dress up a future Emeritus meeting with a bit of learning and conviviality. Yale will arrange for one of the Stony Brook physicians to lecture on a topic of interest, and Stuart Friedman MPS, our Executive Director, will encourage conviviality with hero sand-wiches.
We add with pride that Doctor Ed Norris is already pursuing his special interest, by helping some two hun-dred and fifty occupants of the Jefferson’s Ferry Independent and Assisted Living Facility.
Doctor Nate Newman will be looking into ways that we can offer pro bono medical care for patients, and Doctor Tevia Lipitz, a retired pediatrician, will be setting up lecture and discussion meetings for parents.
At the next meeting, we will be embarking on a very important endeavor, and a description of that will be shared with Society members in the next issue of the SCMS Bulletin.
If you are retired or working part-time and would like to join our group, please give us a call and drop in to our next meeting (date to be announced) 631-851-1400.

20
Your Patients Receive Your Services While We Collect Your Past Due Receivables
We are in business over 20 years on Long Island
Medical collection experience
Handle delinquent accounts in a professional and timely manner
Improve receivables while maintaining the good will of patients
Team concept ensures a staff knowledgeable in medical terminology
Reduced contingency fee for Members of the SCMS
Let CTech’s professional, courteous and experienced staff work for you!
CTech Collections, Inc. 5505 Nesconset Highway Suite 200
Mt. Sinai, New York 11766
Phone: 631-828-3150 Fax: 631-331-9566
www.ctech-collects.com
Call for a
No Obligation
Appointment
LEARN THE REAL ISSUES OF ESTATE ANALYSIS & RETIREMENT PLANNING
Coordinating Retirement & Estate Analysis Disability Income Insurance
Preserving Your Pension/ IRA / Keogh Assets Business Agreement Funding
Using Trusts in Estate Analysis Group Health Insurance
Creative Uses of Life Insurance Evaluation of Long Term Care Insurance Policies
Planning for Families with Disabled Children Investments*
THE AJK FINANCIAL GROUP
Specializing in Assisting Professional Medical Practices
Endorsed by the Suffolk County Medical Society
Alan D. Kahn, CPA, MBA, CLU, ChFC 33 Queens Street, Suite 102
Syosset, NY 11791
Tel: (516) 677-0270 / Fax: (516) 677-0273
Website: www.ajkfinancialgroup.com *Alan D. Kahn is a Registered Representative of and offers securities products, investment advisory and financial planning services through MML Inves-tors Services, Inc., Member SIPC, 6800 Jericho Turnpike, Suite 202W, Syosset, NY 11791, (516) 364-9797. The AJK Financial Group is not a subsidiary or affiliate of MML Investors Services, Inc., and is not engaged in rendering legal or tax advice. Insurance offered through Massachusetts Mutual Life Insurance Company and other fine companies. CRN 201108-124490
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org

21
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
MLMIC RESIDENTS
Alexa S. Calero, M.D.
SUNY @ Stony Brook; Neonatal-Perinatal
David O. Malaka, M.D.
No. Shore/LIJ Southside Hospital; Family Medicine
TRANSFERRED IN Audrey L. Eisenstadt, M.D.
Dix Hills; Diagnostic Radiology
RE-ELECTIONS Mel B. Kaplan, M.D.
Southold; Internal Medicine
Paul C. Moulinie, M.D.
Huntington; Cardiovascular Diseases
Phyllis J. Smith, M.D.
Huntington; Dermatology
Joseph M. Caputo
Neva A. Castro
James J. Connolly
Robert Diep
Danielle Duhame
Geri L. Galotti
Bradley Kay
Abdul Kouanda
Wilmina N. Landford
Pavel Mazirka
Saira Mehmood
Samantha J. Palmaccio
Ruksana Rangwala
Alexandra Rodman
Brianne Sullivan
Varun R. Ralanki
Richard Zheny
ACTIVE MEMBERS
Steven B. Schwartz, DDS, MD
Pt. Jefferson Station; Maxillofacial Surgery
Dana R. Cohen, M.D.
Northport; Psychiatry
Recruited by Robert A. Scher, M.D.
Amy E. Hearne, M.D.
Northport; OB/GYN
Recruited by Lawrence A. Horn, M.D.
Sarala K. Reddy, M.D.
Huntington; Psychiatry
Daniel M. Van Arsdale, D.O.
Westhampton Beach; Family Medicine
STUDENTS – SUNY @ Stony Brook
CONGRATULATIONS William Spencer Jr, MD, the SCMS Treasurer has recently been elected as a County Leg-islator for the 18th district of Suffolk County. He is the first physician to ever hold a position as a County Legislator in Suffolk. In all likelihood, Dr. Spencer will be asked to Chair the health section within the Department of Health and Human Services, where he will have the ability to draft and introduce legislation that will impact public health and safety-additionally, anything that may restrict unfair business practices in the County would come under his perview.
Dr. Spencer is board certified in Otolaryngology, a Diplomate of the American Board of Otolaryngology, and the National Board of Medical Examiners, and is a Fellow of the American Academy of Pediatrics.
WELCOME TO OUR NEW APPLICANTS

22
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org

23
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
PHYSICAL & OCCUPATIONAL THERAPY
Sheldon G. Lieberman, P.T. Director
Joshua M. Lieberman, O.T.R/L
Daily, Evening & Weekend Appointments Home Care Available
Sports injuries l Pre & Post Surgical Rehab l TMJ l Message Therapy l Spinal Trauma l Carpal Tunnel Pain Management
Neck & Back Pain l Fall Prevention l Sports Rehab l Auto Accidents l Work Place Injuries l Headaches l Painful Joints School Based OT Evaluation & Treatment
We Accept No Fault, Workman’s Compensation & Medicare, Most Other Insurances Accepted
Se Habla Espanol
WE NOW HAVE THE NEW BIODEX COMPUTERIZED BALANCE SYSTEM
HAUPPAUGE COMMACK SAYVILLE
631-265-3910 631-499-8376 631-563-8487
501 Route 111 160 Commack Rd. 299 Raft Ave.
HUNTINGTON - WEST HILLS 850 SF of office with the option of an additional 1500 SF.
Free-standing modern building on the Nassau/Suffolk border.
Office is centrally located on Jericho Turnpike, and has ample parking.
Will build to suit.
Call 631-423-1008.

24
Happy Holidays from Spa Belle Meade
The Medical Spa Where Health Meets Beauty
S u f f o l k C o u n t y M e d i c a l S o c i e t y
S u f f o l k A c a d e m y o f M e d i c i n e
1 7 6 7 V E T E R A N S M E M O R I A L H I G H W A Y S U I T E 1 4 I S L A N D I A , N E W Y O R K 1 1 7 4 9
Reward yourself with a visit to Spa Belle Meade: The Medical Spa, where highly trained profes-sionals practice the latest anti-aging techniques and offer expert advise to keep you looking your best. As a medical spa, Spa Belle Meade integrates the ambience, cosmetic services and benefits of day spas, with sophisticated and therapeutic care. Our exquisite, state of the art facility features a staff of plastic surgeons, nurses, medical esthetics and licensed massage therapists. All treatments are performed by the board certified physicians at Suffolk Plastic Surgeons, P.C.
Dr’s. Hilton C. Adler , Stephen F. Coccaro and Kenneth C. Kneessy of Suffolk Plastic Surgeons, P.C. are proud members of the Suffolk County Medical Society. We are conveniently located in East Setauket. Cal us today re-garding how you or your patients could possibly benefit from medical spa treatments (631)751-2693. or visit us at www.spabellemeade.com
Suffolk County Medical Society Bulletin January 2012 www.scms-sam.org
Offering Facials, Body Wraps,
& Massages
Advanced techniques in facial rejuvenation including: Botox, CosmoPlast, Collagen,
Permanent Make-up, Peels, Microdermabrasion, Fotofacials, Professional Skin Care.