Embed Size (px)
Citation preview
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 1
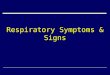
Danger Signs and Signs of Severe Illness
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Respiratory distress and Chest in-drawing
o Difficulty breathing
o Chest draws in on inspiration,
o Stridor
o Lung crepitations (crackles, rales) heard with a stethoscope
o Cyanosis
o Oxygen saturation <95%
Not able to drink, eat or breastfeed
Vomiting everything
Convulsions with present illness
Altered mental state, prostration or extreme weakness
o Unconscious, drowsiness or confusion
o Extreme lethargy, unable to sit or stand
o The child does not respond when you clap or stimulate the sternum
Severe Anemia
o Severe pallor--Palms are white
Severe Dehydration
o Skin pinch test of more than 2 seconds
o Rapid and deep breathing - faster than normal
o Child is drinking poorly
o Fast, weak pulse
o Lethargy or unconsciousness
o Cramping of the arms and legs
How long has the child had difficulty breathing?
Is the child able to drink or breastfeed?
Does the child does not drink when offered water or breast milk?
Is the child able to sit or stand without support?
Describe what happens when you offer your child something to drink.
Does the child vomit everything?
Has the child had convulsions with this current illness?
Does the child seem unusually sleepy or tired?
Pre-referral treatment for severe malaria:
Rectal artesunate shall be used as pre-referral treatment for severe malaria.
When rectal artesunate is not available or contraindicated, intramuscular quinine is the alternative pre-referral treatment.
Dosage of rectal artesunate in children under-5:
Weight (kg)
Age Artesunate dose (mg)
Suppository single dose
5-8.9 0-12 months 50 mg 1 supp (50 mg)
9-19 13-42 months 100 mg 2 supp (50 mg)
20-29 43-60 months 200 mg 1 supp (200 mg)
Pre-referral treatment for chest in-drawing and any general danger signs:
Give 1st dose antibiotic amoxicillin or IM chloramphenicol:
Weight (kg) Age Dose of amoxicillin
4-10 kg 2-12 months 125 mg
10-19 kg 12 months-5 years 250 mg
If unable to swallow Refer urgently
Pre-referral treatment for severe dehydration:
Refer urgently with mother giving frequent sips of ORS on the way.
Advise mother to continue breastfeeding.
If convulsing, give anticonvulsant:
Diazepam 200 micrograms (0.2mg)/ kg (max: 10mg) rectally or IV.

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 2
Meningitis
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Rapid onset of fever
Neck stiffness or neck pain—(Does the child bend his/her neck easily while looking around? Can the child look easily at his toes or umbilicus?)
Bulging fontanel in children under 18 month
Altered mental state, confusion, or coma
Convulsions
Meningococcal rash (petechial or purpuric)
Severe headache
Failure to feed
Photophobia (older children)
Signs of raised intracranial pressure:
o unequal pupils o rigid posture o focal paralysis in any of the limbs or
trunk o irregular breathing
When did the fever start?
Have you noticed any difficulty with your moving his/her neck?
Has the child had any convulsions? If yes, how often?
Does the child have a rash?
Have you noticed a change in the child’s behavior?
Has the child been eating?
Has the child complained of a headache?
Causative organisms not yet identified HC4:
Ceftriaxone 50-100 mg / kg daily IV or IM daily in 1-2 divided
doses for up to 14 days
Change to cheaper effective antibiotic if and when CNS results
become available.
If ceftriaxone not available, and at HC3 level:
Chloramphenicol 25 mg / kg IV every 6 hours for up to 14
days (use IM if IV not possible).
Once clinical improvement occurs, change to: 25 mg/kg per
dose orally every 6 hours to complete the course.

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 3
Uncomplicated Malaria
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
No danger sign or sign of severe illness
History of fever
Raised body temperature (above 37.5 C as taken from the axilla)
Evidence of parasites in the blood – with a positive RDT (or blood smear), and:
Weakness
Lethargy
Nausea
Vomiting
Loss of appetite
Mild anemia (mild pallor of palms and mucous membranes); occurs commonly in children
Dehydration (dry mouth, coated tongue, and sunken eyes).
Enlarged spleen (in acute malaria it may be minimally enlarged, soft and mildly tender)
Does the fever come and go?
Has the child been unusually tired or weak?
Has the child vomited? How many times has he/she vomited since the vomiting began/
Has the child been eating?
Have you given the child any medicine?
Has the child had any convulsions?
Have the convulsions been with this illness?
Treatment of uncomplicated malaria:
The recommended first line medicine is artemether/lumefantrine.
The recommended first line alternative medicine is artesunate /
amodiaquine.
The recommended second line medicine is also an ACT,
dihydroartemisinin piperaquine (DHA-PPQ; 40 mg/320 mg).
The recommended second line alternative medicine is oral quinine
for all patients. WHO recommends that quinine be given with
tetracycline or doxycycline or clindamycin.
Dosage of artemether/lumefantrine 20/120 mg—Coartem tablets:
Weight (kg)
Age Day 1 Day 2 Day 3
5-14 4 months-
3 years
1 tab twice a day / 12
hourly
1 tab twice a day / 12
hourly
1 tab twice a day / 12
hourly
15-24 3-7 years 2 tab twice a day / 12
hourly
2 tab twice a day / 12
hourly
2 tab twice a day / 12
hourly
Dosage of artesunate (AS) tablets:
Age Day 1 Day 2 Day 3
5-11 months 15 mg
(= 1/2 tab)
15 mg
(= 1/2 tab)
15 mg
(= 1/2 tab)
1-6 years 50 mg 50 mg 50 mg
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 4
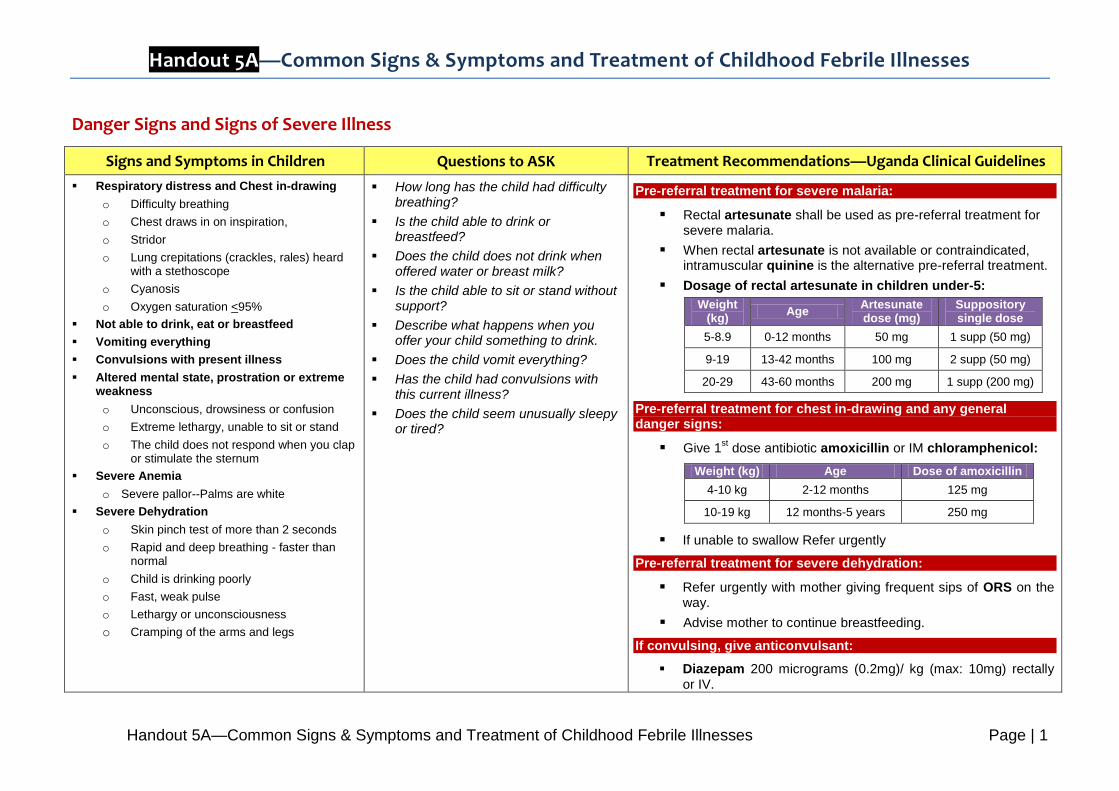
Dosage of amodiaquine (AQ) tablets:
Age Day 1 Day 2 Day 3
5-11 months 76 mg
(= 1/2 tab)
76 mg
(= 1/2 tab)
76 mg
(= 1/2 tab)
1-6 years 153 mg
(= 1 tab)
153 mg
(= 1 tab)
153 mg
(= 1 tab)
Dosage of dihydroartemisinin piperaquine (DHA-PPQ) 40 mg/320 mg:
Weight (kg)
Age Day 1 Day 2 Day 3
5.9.9 6 months-
1 year ½ tab ½ tab ½ tab
10-20 2-7 years 1 tab 1 tab 1 tab

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 5
Severe Malaria
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Presence of parasitaemia confirmed by positive malaria test and the presence of one or more of the following clinical features:
Impaired consciousness including unrousable coma (danger sign)
Prostration, generalized weakness so that the child unable to sit, stand or walk without assistance (danger sign)
Multiple convulsions: more than two episodes within 24 hours (danger sign)
Deep breathing and respiratory distress, acidotic breathing (danger sign)
Failure to feed (danger sign)
Acute pulmonary oedema and acute respiratory distress syndrome
Circulatory collapse or shock, systolic blood pressure < 50mm Hg in children;
Acute kidney injury
Clinical jaundice plus evidence of other vital organ dysfunction
Abnormal bleeding
Does the fever come and go?
Has the child been unusually tired or weak?
Has the child vomited?
Has the child been eating?
Have you given the child any medicine?
Has the child had any convulsions?
Have the convulsions been with this illness?
Have you noticed any yellow in the eyes?
Treatment of severe and complicated malaria:
Intravenous artesunate is the recommended first line
medicine for severe malaria.
Intravenous quinine or intramuscular artemether is the
alternative to be used when artesunate is not available.
Once the patient is able to take orally after at least 24 hours
of parenteral treatment, treatment should be completed with a
treatment, treatment should be completed with a full course of
oral first line ACT.
Dosage of intravenous artesunate for severe malaria: 2.4 mg/kg:
Dose Time of administration
First dose on admission At 0 hours
Second dose At 12 hours
Third dose At 24 hours
Then once a day until patient is able to tolerate oral medication
If convulsing, give anticonvulsant:
Diazepam 200 micrograms (0.2mg)/ kg (max: 10mg) rectally or IV

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 6
Pneumonia (non-severe)
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
No danger sign or sign of severe illness
Tachypnoea (rapid breathing):
o 0-2 months >60 /min
o 2-12 months >50 /min
o 12-60 months >40 /min
Nasal flaring
Stridor (high pitched wheezing sound when the child breathes)
Cough
Lethargy
High pulse rate
Is the child having difficulty breathing?
Does the child have a cough? If yes, how long has the child had a cough?
What is the quality of the cough? Dry? Productive?
When did you first notice the child breathing fast?
Has the child been tired or weak?
Have you noticed any harsh noises when the child breathes in?
Treat with antibiotics:
Amoxicillin every 8 hours for 5 days
Age Weight (kg) Dose
2-12 months 4-10 125 mg
12 months-5 years 10-19 250 mg
If amoxicillin is not available, give Cotrimoxazole 24 mg/kg every 12 hours for 5 days or PPF 50,000 IU/kg IM daily for at least 3 days
Give vitamin A to all children with pneumonia:
6-11 months: 100,000 IU single dose
1-6 years: 200,000 IU single dose
Manage fever:
Paracetamol 10 mg/kg every 8 hours for 3 days.
If wheezing is present:
Salbutamol 100 micrograms (0.1 mg)/kg every 8 hours until wheezing stops HC3
Reassess child for progress; if no improvement in 2 days or condition deteriorates:
Switch to chloramphenicol 25 mg/kg IV every 6 hours until the child improves then continue with oral chloramphenicol for a total of 10 days HC4.

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 7
Gastroenteritis / Dysentery
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
4 to 10 loose stools a day
Blood or mucus in the stool
Abdominal pain
Nausea and vomiting
Loss of appetite
Signs of dehydration:
Dryness of the mouth and tongue
Child is thirsty and drinks eagerly or not able to drink or drinking poorly.
Sunken eyes
Irritability, restlessness, weakness, and dizziness
Skin pinch test of 1 second
Crying with few or no tears
Passing very little urine which is often dark
Headache
Has the child had any watery stools?
How many lose stools does the child have in one day?
How many days has the child had diarrhea?
Is there blood in the stool?
Has the child been vomiting?
Has the child been very thirsty?
When was the last time the child urinated?
Is the child eating?
Has the child complained of abdominal pain?
Treatment for diarrhoea and dehydration:
Oral rehydration salts (ORS) for 3 days. Give small but frequent sips.
Age (Months) Weight (kg) ORS (mL)
<4 <6 200-400
4-12 6-9.9 400-700
13-24 10-11.9 700-900
25-60 12-19 900-1400
Zinc (10-20 mg) daily for 10 days:
Age Dose
<6 months 10 mg daily x 10 days
>6 months 20 mg daily x 10 days
Vitamin A
o 6-11 months: 100,000 IU
o 1-6 years: 200,000 IU
Continue breastfeeding, giving fluids and feeding
Follow up in 5 days
Treatment of dysentery (shigellosis—bloody diarrhoea) child >3 month:
Cotrimoxazole 24 mg/kg every 12 hours for 5 days
or
ciprofloxacin 30 mg/kg twice daily for 3 days
or
nalidixic acid 15 mg/kg per dose
Follow up in 3 days

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 8
Measles
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Generalized rash without pustules or vesicles (which began behind the ears and on the neck) and one of these:
o Cough
o Runny nose
o Conjunctivitis (red eyes)
Barking cough
Recent exposure to a measles case
Koplik’s spots (grey white spots inside the mouth)
No documented measles immunization
Anorexia and vomiting
Mouth ulcers (severe measles)
Pus draining from eye (severe measles)
Clouding of the cornea (severe measles)
If the child has had fever for more than 7 days, has the fever been present every day?
Has the child had measles within the last 3 months?
Has the child been vaccinated for measles?
Does the child have a rash?
When did you first notice the rash?
Where did you first notice the rash?
Does the rash itch?
Does the child have a cough?
How long has the child had a runny nose?
Have you noticed any drainage from the eyes?
Have you noticed any sores in the child’s mouth?
How long has the child had clouding in the eyes?
Management (symptomatic) HC2:
Apply tetracycline eye ointment 1% every 12 hours for 5 days
Increase fluid intake
Give vitamin A 200,000 IU
o 1st dose: At diagnosis
o 2nd dose: The next day
o 3rd dose: 2-4 weeks later
Management of mouth ulcers:
Paint the mouth with gentian violet aqueous paint 0.5%
twice daily
Management of eye infection:
Clean both eyes 3 times daily:
o Wash hands
o Ask child to close eyes
o Use clean cloth with clean water to gently remove pus
o Use a different part of the cloth for each eye
o Clean each eye from nose-side to ear-side to avoid passing the infection from one eye to the other
Apply tetracycline eye ointment 1% to each eye
o Ask the child to look up
o Squirt a small amount (5 mm length) on the inside of the lower eyelid
o Wash hands again
Continue application until the redness has gone
Do not put anything else into the eye

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 9
Acute Otitis Media (Ear Infection)
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Pus drainage from ear
Ear pain
Child repeatedly tugging or touching the infected ear
Tenderness or swelling behind the ear
Swollen lymph nodes in anterior neck
Red tympanic membrane on otoscopy
Have you noticed any drainage from the child’s ears?
What colour is the drainage?
When did you first notice the ear drainage?
Has the child been pulling at one ear?
Has the child had an ear infection before?
Treat with antibiotics::
Amoxicillin every 8 hours for 5 days
Age Weight (kg) Dose
2-12 months 4-10 125 mg
12 months-5 years 10-19 250 mg
Dry the ear at least 3 times daily:
Dry ear by wicking Roll clean absorbent cloth or soft gauze into a wick
Place this in the ear and remove when wet
Replace wick with a clean one
Repeat this process until the ear is dry
Manage pain:
Paracetamol 10 mg/kg every 8 hours for 3 days

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 10
Pharyngitis / Tonsillitis (Sore Throat)
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Pain and difficulty in swallowing
Drooling of saliva
Mild cough
Swollen lymph nodes in the anterior neck
Red and inflamed tonsils
White coating over the throat or tonsils
Has the child complained of a sore throat?
Has the child had pain or difficulty swallowing?
Have you notice any swelling or tenderness of the neck?
Does the child have a cough?
If streptococcal pharyngitis suspected:
Benzathine penicillin 1.2 MU IM single dose
o Child: <30 kg: 30,000 IU/kg
or
PPF 20,000 IU/kg IM daily for 10 days
or
Phenoxymethyl penicillin 12.5 mg/kg every 6 hours for 10 days
If allergic to penicillin:
Erythromycin 12.5 mg/kg per dose every 6 hours for 10 days
Note:
If not properly treated, streptococcal pharyngitis may lead to
acute rheumatic fever and retropharyngeal or peritonsillar
abscess. Therefore. ensure that the full 10-day courses of
antibiotics are completed where applicable
Cotrimoxazole is not effective for the treatment of
streptococcal pharyngitis, and it should not be used.

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 11
Typhoid
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Fever rises in steps
Gradual onset of chills and weakness
Headache
Anorexia (failure to feed)
Epistaxis (nose bleed)
Backache and constipation
Abdominal pain and tenderness
Bradycardia (very slow heart rate)
Confusion, delirium and stupor
Tender splenomegaly
Seriously and obviously ill with no apparent cause
Is the child eating?
Has the child complained of a headache?
Has the child complained of abdominal pain?
Has the child had a nose bleed?
Has the child been confused?
Does the child been very tired?
Treat with antibiotics:
Chloramphenicol 25 mg/kg IV or oral every 6 hours for 10-14 days
or
Ciprofloxacin 10-15 mg/kg every 12 hours for 5-14 days
or
Cotrimoxazole 24 mg/kg every 12 hours for 3 days dose
or
Amoxicillin 25 mg/kg every 8 hours
Cystitis (Urinary Tract Infection)
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Crying when passing urine
Urinary frequency or dysuria
Urgency which manifests as incontinence in previously continent child
Dark or foul smelling urine
Blood in the urine
Vomiting
Poor feeding
Lethargy and/or irritability
Lower abdominal tenderness
Costo-vertebral angle or suprapubic tenderness
Does the child cry when passing urine?
Have you noticed the child urinating more than usual?
Have you noticed any blood in the urine?
Does the urine smell unusually bad?
Has the child been eating?
Have you noticed the child has had accidents urinating?
Has the child been very tired?
Treat with antibiotics:
Cotrimoxazole 48 mg/kg single dose
or
Ciprofloxacin 10-15 mg/kg single dose
Ensure high fluid intake

Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses
Handout 5A—Common Signs & Symptoms and Treatment of Childhood Febrile Illnesses Page | 12
Chicken Pox (varicella zoster)
Signs and Symptoms in Children Questions to ASK Treatment Recommendations—Uganda Clinical Guidelines
Low grade temperature
Sore throat
Itchy rash on the head and torso
Vesicular rash with superficial blister in centre which erupts and forms a crust.
Papules may ooze clear fluid or be dry
Rash with pus like discharge is a sign of sepsis
Complications may include septicaemia, pneumonia, fulminating haemorrhagic varicella, and meningoencephalitis
When did the rash begin?
Are there other children in the community with similar rash?
What have you given the child to stop the itching?
When did the rash begin to dry up?
Relieve pain and itching from rash:
Apply Calamine lotion every 12 hours plus chlorphenamine 4 mg every 12 hours for 3 days
Paracetamol 1 mg every 12 hours for 3 days
Prevent spread of infection:
Advise to avoid contact between infected persons and immunosuppressed persons.