Embed Size (px)
Citation preview

9th Hand and Wrist Biomechanics International Symposium
Featuring
2nd International Thumb Osteoarthritis Workshop
June 15-17, 2015
In conjunction with
20th Congress of Federation of European Societies for Surgery of the Hand
June 17-20
Milano Congressi Milan, Italy

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Symposium Chairs
Marc Garcia-Elias, MD, Insitut Kaplan, SPAIN
Frederick W. Werner, MME, SUNY Upstate Medical University, USA
Local Organizing Committee Riccardo Luchetti, MD, Contract Professor, University of Milan, Milan, ITALY, Co-Chairman
Giorgio Pajardi, MD, Consultant Hand Surgeon, Milan, ITALY, Co-Chairman
International Program Committee Joseph J. Crisco, PhD, Brown University, USA
Kenneth Fischer, PhD, University of Kansas, USA
Zong-Ming Li, PhD, Cleveland Clinic, USA
David L. Nelson, MD, San Francisco Bay Area Hand Club, USA
Fong-Chin Su, PhD, National Cheng Kung University, TAIWAN
Frederick W. Werner, MME, SUNY Upstate Medical University, USA
International Advisory Committee Kai-Nan An, PhD, Mayo Clinic, USA
Moroe Beppu, MD, St. Marianna University, JAPAN
Zong-Ming Li, PhD, Cleveland Clinic, USA
David L. Nelson, MD, San Francisco Bay Area Hand Club, USA
Frederic Schuind, MD, PhD, Universite de Bruxelles, BELGIUM
William H. Seitz, Jr., MD, Cleveland Clinic, USA
Fong-Chin Su, PhD, National Cheng Kung University, TAIWAN
Scholarship Committee:
Kenneth J. Fischer, PhD, University of Kansas, USA
David L. Nelson, MD, San Francisco Bay Area Hand Club, USA
Frederick W. Werner, MME, SUNY Upstate Medical University, USA
Symposium Venue Milano Congressi (MICO), Milan, Italy
HWBI Program at a Glance Monday, June 15, 2015 Arrival, Group Tour & Reception
Tuesday, June 16, 2015 Morning/Afternoon Sessions, Evening Networking and Banquet
Wednesday, June 17, 2015 Morning Session followed by Afternoon FESSH Congress Events
Thursday, June 18, 2015 Morning Joint Session with FESSH

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
The Scholarship Committee for Hand and Wrist Biomechanics International (HWBI) 2015
Announces the Award Winners
Scholarship Award information and selection criteria: Four HWBI scholarship awards ($500 each) were available to students, residents and fellows. The scholarships are sponsored by the International Society of Biomechanics (ISB), by the Hand and Wrist Biomechanics International, and by the William H. Seitz, M.D. Research Fund. All trainees in one of the above categories who requested to be considered were evaluated for one of these scholarships. Awards were made based on the quality of the research, as judged by the abstracts. The ISB Award was given to the highest ranking abstract among ISB members under consideration.
Award Winners:
Joseph N. Gabra ISB-Sponsored Award Recipient Hand Research Laboratory, Departments of Biomedical Engineering, Cleveland Clinic, and Department of Chemical and Biomedical Engineering, Cleveland State University Cleveland, OH, U.S.A. Abstract: Three-dimensional stiffness of the wrist structure
Benjamin Goislard de Monsabert Aix-Marseille Université, Marseille, France Abstract: Estimation of subject-specific muscle capacities for musculoskeletal modeling of the hand and the wrist
Faes D. Kerkhof Department of Development and Regeneration @ Kulak, KU Leuven, Kortrijk, Belgium Abstract: In vivo analysis of joint function using dynamic CT
Giovanni F. Solitro Department of Orthopaedics, University of Illinois at Chicago, Chicago, Illinois, USA Abstract: Boutonniere Deformity Mechanics Captured and Defined Using Finite Element Methods
Special THANKS to our Award Sponsors!
Hand and Wrist Biomechanics
International
International Society of
Biomechanics
William H. Seitz, M.D.
Research Fund
Scholarship Committee: Kenneth J. Fischer, PhD, University of Kansas, USA (chair) David L. Nelson, MD, San Francisco Bay Area Hand Club, USA Frederick W. Werner, MME, SUNY Upstate Medical University, USA

HWBI and ITOW 2015
MONDAY, JUNE 15 Opening Reception
TUESDAY, JUNE 16
7:00 REGISTRATION
Opening Remarks 8:00 Frederick Werner, Zong-Ming Li & Joseph Crisco
Special Speaker 8:10 Kai-Nan An, PhD (Fred Werner, Moderator) History of Hand and Wrist Biomechanics at the Mayo Clinic
Wrist 8:40 Ken Fischer (Moderator) In Vivo Joint Contact Pressure Distributions in the Hand and Wrist
9:00 Frederick Werner Biomechanics of carpal instability
9:20 David Nelson Understanding the Wrist Radiograph
9:40Benjamin Goislard de Monsabert, Jérémy Rossi, Guillaume Rao, Eric
Berton, Laurent Vigouroux
Estimation of Subject-Specific Muscle Capacities for Musculoskeletal Modelling of
the Hand and the Wrist
9:50 Discussion
10:00 COFFEE BREAK
Arthroplasty 10:20 Peter Evans (Moderator) Ulnar head replacement
10:40 Arnold-Peter Weiss Limited and Total Wrist Fusions
11:00 Magnus K. Gislason, Euan Foster, David H. NashBiomechanical Comparison Between The Universal2 and Maestro Total Wrist
Implant: A Finite Element Study
11:10 Gaetano Maurizio Grippi Biarticular Concentric Carpal Mechanics and Coxa Manus Surgery
11:20 Discussion
Thumb I 11:30 Joseph Crisco (Moderator) CMC Joint Biomechanics
11:50Yusuke Kawano, Toshiyasu Nakamura, Mitsunori Tada, Yusaku
Kamata, Shinjiro Sueda, Dinesh Pai, Takeo Nagura, Kazuki Sato
Trapeziometacarpal Joint Fusion Reduced the Thumb-Tip Trajectory Area
Approximately 30% of the Original Trajectory Area: A Cadaveric Study
12:00Benjamin Dourthe, Priscilla d’Agostino, Filip Stockmans, Faes Kerkhof,
Evie Vereecke
Mathematical Modeling of the Trapeziometacarpal Joint For In Vivo Stress
Distribution Analysis
12:10 M. Conconi, E. Halilaj, V. Parenti Castelli, J. J. CriscoCT Scans Allows for Early Evaluation of Joint Space Narrowing Within the First
Carpo-Metacarpal Joint Osteoarthritis
12:20M.T.Y.Schneider, J. Crisco, A. C. Weiss, A. L. Ladd, P. Nielsen, T.
Besier, J. ZhangWomen have Similar Carpometacarpal Joint Morphology to Men
12:30 Discussion
12:40 LUNCH
Wrist II 14:00 Marc Garcia-Elias (Zong-Ming Li, Moderator)Dart-throwing motion in patients with scapholunate instability. A dynamic 4D
computed tomography study
14:20 Greg Couzens, Lance Wilson, Caroline Grant In Vitro Scapholunate Rotations with FDP Tendon Loading
Carpal Tunnel 14:30 Riccardo Luchetti (Moderator)Segmental Pressure along the Carpal Canal: A Study Performed with Changes in
Hand and Wrist Position in Patients with CTS and Controls
14:50 Zong-Ming Li Biomechanics of the Transverse Carpal Ligament
15:10 Y. Yoshii, T. Ishii, W.L. TungUltrasound Assessment for the Effectiveness of Carpal Tunnel Release on Median
Nerve Deformation
15:20 Ukadike C. Ugbolue, Quentin A. Fogg, Magnus K. Gislason Tensile Properties of the Transverse Carpal Ligament In-Situ
15:30 Joseph N. Gabra, Zong-Ming Li Three-Dimensional Stiffness of the Wrist Structure
15:40 William B. Ericson, JrSubclinical Nerve Compression: A Subtle Physical Finding with Extensive
Implications
15:50 Discussion
16:00 COFFEE BREAK
Distal Radius 16:20 David Nelson (Arnold-Peter Weiss, Moderator) Preventing complications with volar plating
16:40 Jorge Orbay The Biomechanics of Articular Fracture Fixation in Distal Radius Fractures
17:00Tracy Webber MD, Shaun Patel MD, Michael Pensak MD, Olukemi
Fajolu MD, Tamara Rozental MD, Jennifer Moriatis Wolf MDCorrelation Between Distal Radius Cortical Thickness and Bone Mineral Density
17:10 Greg Couzens, Graham Kerr, Derrick Maxwell Variation in Antagonist Activity in Isometric Forearm Muscle Contraction
17:20 Ronit WollsteinProprioception of the Wrist Following Distal Radius Fracture-a Protocol for
Evaluation and Treatment
17:30 Discussion
WEDNESDAY, JUNE 17
Manipulation and Motion 8:00 Veronique Feipel (Moderator) 3D Kinematics and Modeling of the Wrist and Fingers in vivo
8:20 Marco Santello Role of digit force-to-position modulation for dexterous manipulation
8:40Hsiu-Yun Hsu, Li-Chieh Kuo, Ta-Shen Kuan, Fong-Chin Su, Haw-Yen
ChiuPrecision Pinch Performance in the Hands of Patients following Nerve Repair
8:50 V. Gracia-Ibáñez, M. Vergara, J.L. Sancho-BruImportance of Grasp Types for Personal Autonomy During Activities of Daily Living
(ADL)
9:00 Hsiu-Ching Yang, Li-Chieh Kuo, Ta-Shen Kuan, Hsiu-Yun HsuReach-to-Grasp Movement under Different Sensory Conditions in Children with
Developmental Coordination Disorder: A Pilot Study
9:10Sebastian V. Gehrmann, Sabrina Pfau, Joachim Schaedle, Georg
Jansing, Joachim WindolfRange of motion of the wrist while driving a car
9:20 Discussion
9:30 COFFE BREAK
Fingers & Grasping 10:00 Fong-Chin Su (Moderator) Biomechanical Aspects of Trigger Finger
10:20Francisco J. Valero-Cuevas, Susan V. Duff, Dorit H. Aaron, Gloria R.
GogolaA Review of Innovative Evaluation of Dexterity
10:30Jérémy Rossi, Benjamin Goislard de Monsabert, Eric Berton, Laurent
Vigouroux
Is the Minimization of Secondary Moment During Finger Pressing Task Related to
Muscle Force Economy?
10:40 Giovanni F. Solitro, Farid Amirouche, Mark Gonzalez
Boutonniere Deformity Mechanics Captured and Defined Using Finite Element
Methods
10:50 Chien-An Shih, Fong-Chin Su, Po-Ting Wu, Chia-Lung Li, I-Ming Jou The Expressions of Estrogen Receptors in de Quervain’s Disease
11:00 Ronit Wollstein Evaluation of Forces During Two Different Pushup Styles
11:10 Discussion
Thumb II 11:20 Amy Ladd (Moderator) The Puzzle of the Thumb – Mobility, Stability, and Demands in Opposition
11:40Faes D. Kerkhof, Eddy Brugman, Filip Stockmans, Ilse Jonkers, Evie E.
VereeckeIn Vivo Analysis of Joint Function Using Dynamic CT
11:50Mireia Esplugas, Alex Lluch, Marc Garcia-Elias, Nathalie Mobargha,
Elisabeth Hagert Biomechanical Analysis of the Thumb Carpometacarpal Joint Ligaments
12:00Thomas J. McQuillan, Tarpit Patel, Deborah Kenney, Amy L. Ladd,
Arnold-Peter C. Weiss, Joseph J CriscoInterrater and Intrarater Reliability of the Radiographic Thumb Osteoarthritis Index
12:10 Jorge Orbay, Michael R. Mijares Power Grip and the Biomechanics of CMC Osteoarthritis
12:20Thomas J. McQuillan, Deborah Kenney, Joseph J. Crisco, Arnold-Peter
C. Weiss, Amy L. Ladd
Decreased Functional Pinch Strength is Associated with Early Thumb CMC
Osteoarthritis
12:30 Discussion
Closing Remarks 12:40 Kai-Nan An & Marc Garcia-Elias
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
HISTORY HAND AND WRIST BIOMECHANICS AT THE MAYO CLINIC
Kai-Nan An, PhD Mayo Clinic, Minnesota, USA
Building upon the well-established hand surgery practice at the Mayo Clinic, including pioneering contributions
from Dr. Ronald Linscheid and Dr. James Dobyns, hand and wrist biomechanics was developed in the early
1970s by Dr. Edmund Chao and Dr. William Cooney. Over the past four decades, numerous experimental and
analytical approaches have been established for biomechanical study. These include the electrogoniometer for
functional joint kinematics, biplanar stereoradiography, and dynamic CT for studying the functional anatomy of
carpal and metacarpal kinematics, tendon excursion for determining the mechanical efficiencies of tendon and
muscles, optimization methods for muscle force determination, rigid-body-spring model for joint stress analyses,
friction testing apparatus for assessing tendon gliding, and tissue engineering for soft tissue regeneration. All of
these laboratory bench studies were originally based on the bedside inquiry and clinically translated back, from
the bench to bedside to facilitate diagnosis and outcome evaluation, including joint replacement, ligament
reconstruction and tendon repair. The accomplishments are the results of dedicated efforts made by many post-
doctoral research fellows from around the world, as well as the contributions from younger generations of staff
surgeons at Mayo.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
IN VIVO JOINT CONTACT PRESSURE DISTRIBUTIONS IN THE HAND AND WRIST
Kenneth J. Fischer1, Qi Zheng1, Joshua E. Johnson1,2
1) University of Kansas, Lawrence, Kansas, USA 2) Worcester Polytechnic Institute, Worcester, Massachusetts, USA
INTRODUCTION. The hand and wrist are significantly and adversely impacted by osteoarthritis (OA), is the most
common degenerative joint disease. OA. In fact, prevalence of radiographic OA is highest for the hand. While age is
the primary risk factor for OA, post-traumatic OA costs 3 billion dollars annually, in the USA alone. Peak joint
contact pressures and abnormal pressure distributions are considered to be important mechanical factors. However,
assessing joint contact pressure in human subjects during functional activity is complex in large joints and even more
difficult in the small joints of the hand and wrist. This work demonstrates our efforts to evaluate in vivo joint
mechanics in normal, injured, and repaired radiocarpal carpal joints, as well as mechanics of the thumb
carpometacarpal (CMC) joint, during functional loading. Our goal is to assess risk of OA in joints of the hand and
wrist.
METHODS. All human subjects had unlilateral scapholunate dissociation and were recruited under an approved
research protocol. MRI images of the wrist and first carpometacarpal joint were acquired at high resolution
(0.2x0.2x0.5 mm) with the subject relaxed. The high resolution images were used to create contact models with high
geometric accuracy. While the subject performed active grasp with visual force feedback, lower resolution images
(0.3x0.3x1.0 mm) were acquired. These images were used to find the loaded positions and orientations of the bones.
Surface contact models and/or finite element analysis allowed were used to calculate the in vivo contact pressure
distributions. For each subject, we compared the normal, injured and surgically repaired/reconstructed radio carpal
mechanics. For the normal wrist, we also acquired and analyzed a feasibility data set for the contact mechanics of the
first CMC joint, and we compared males/females, and apparent changes with age.
RESULTS. For the radiocarpal, the contact mechanics of the injured wrists were significantly different from normal.
There was consistently clear lateral displacement of the scaphoid contact while the lunate had a relatively stable
contact location. The contact force and peak pressure were significantly higher in the radioscaphoid articulation. The
majority of subjects had direction ligament repair. After surgery, there was no statistical difference between normal
and repaired wrist, though qualitative differences persisted in some. Thumb CMC results showed interesting patterns
that appear to be different in men and women, but no statistical differences were found. More data are needed to verify
differences.
DISCUSSION. The findings confirm abnormal radiocarpal contact mechanics in the injured wrist. Change in contact
location and increased in peak contact pressure, as found in the radioscaphoid joint after scapholunate dissociation,
have previously been associated with increased risk of OA. Our study indicates that scapholunate repair/reconstruction
appears to be substantially effective in restoring near normal joint mechanics. Though the thumb CMC data is currently
limited and difficult to interpret, the in vivo imaging/modeling technique also shows promise for studying mechanics in
the thumb CMC joint.
Acknowledgements. Supported by NIBIB (National Institutes of Health) award R01EB008709.
COI. No conflicts of interest.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
BIOMECHANICS OF CARPAL INSTABILITY
Frederick W. Werner SUNY Upstate Medical University, Syracuse, NY, USA
Carpal instability can occur in the proximal carpal row as scapholunate or lunotriquetral instability or
distally as midcarpal instability, typically from a fall on an outstretched hand. Twenty to 30% of patients
following wrist trauma were found to have some form of carpal instability(1), 75% with complete ligamentous
disruptions. Instability results from ligamentous disruption but can be attenuated by variations in bony anatomy.
Most research on carpal instability has focused on the scapholunate joint, due in part to the high
occurrence of scapholunate injury and the complexity of the joint (2, 3, 4). At least 10 ligaments interact and
influence the scapholunate joint. The scapholunate interosseous ligament has been shown to be the primary
stabilizer with secondary roles from the radioscaphocapitate, scaphotrapezoid, long radial lunate, short radial
lunate, dorsal intercarpal and dorsal radiocarpal ligaments. Repetitive loading of the secondary structures,
following damage to the SLIL, may allow increasing scapholunate diastasis and angular changes to the scaphoid
and lunate. Since these can lead to pain and joint degeneration, researchers have quantified these changes as
predictors of clinical symptoms.
Scapholunate diastasis is a separation of the scaphoid and lunate with the capitate acting as a wedge
between them. During dynamic in vitro experiments disastasis can be readily measured, but in vivo it requires
high speed biplanar radiographic imaging. After SLIL sectioning, followed by repetitive loading and loss of
secondary stabilizers, the scaphoid will flex and ulnarly deviate while the lunate will extend and radially deviate.
These angular changes alter the pressure patterns on the radius by changing their location and magnitude.
Importantly, the presence of SLIL and associated ligaments tears may not always alter carpal kinematics
and loading. Bony geometry, such as the curvature of the scaphoid and radioscaphoid fossa can reduce
instability. This may explain why in Viegas's cadaver dissection (5) of 393 wrists, 28% had SLIL tears.
Complete tears of the SLIL may require reconstruction of the ligament with a graft or fusion of the carpal
bones. These surgical treatments frequently have limitations, such as failure to reduce pain, reduction of wrist
motion or development of bone degeneration. More research is needed to solve this clinical challenge.
References. 1. Stanley and Trail. Carpal instability. JBJS 1994. 2. Short et al. Biomechanical evaluation of
ligamentous stabilizers of the scaphoid and lunate. J Hand Surg(Am) 2002, 2005, 2007. 3. Viegas et al. Load
transfer characteristics of the wrist. J Hand Surg (Am)1987. 4. Rainbow et al. In vivo kinematics of the scaphoid,
lunate, capitate and third metacarpal in extreme wrist flexion and extension. J Hand Surg (Am) 2013. 5. Viegas
et al. Wrist Anatomy: Incidence, distribution, and correlation of anatomic variations, tears and arthrosis. J Hand
Surg (Am) 1993.
COI. I have no conflict of interests related to this presentation.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
UNDERSTANDING THE WRIST RADIOGRAPH David L. Nelson, M.D.
San Francisco, California, USA
The radiograph of the wrist is a challenge for anyone to read. A few tricks will help you to make sense of even
complex wrist problems.
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Estimation of subject-specific muscle capacities for musculoskeletal modelling of the hand and the wrist
Benjamin Goislard de Monsabert1, Jérémy Rossi2, Guillaume Rao1, Eric Berton1, Laurent Vigouroux1
1) Aix-Marseille Université, CNRS, ISM UMR 7287, 13288, Marseille, France 2) Laboratoire de Physiologie de l’Exercice (EA 4338), Université Savoie Mont Blanc, Le Bourget du Lac, France
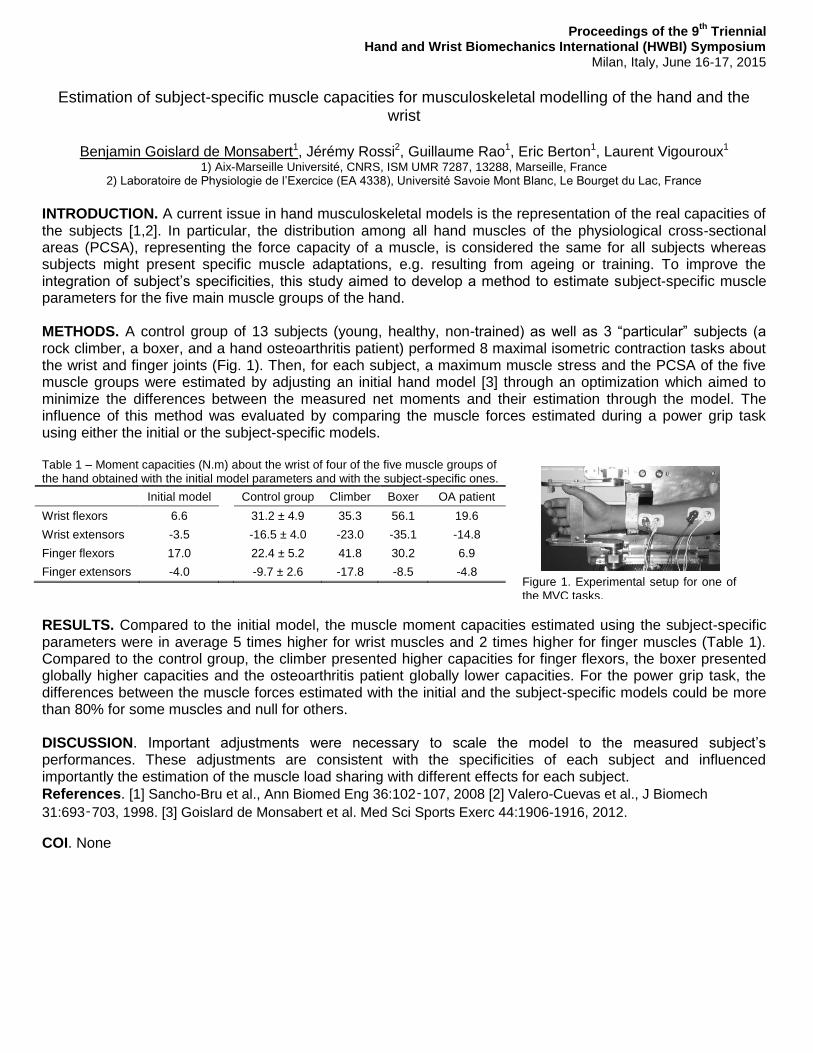
INTRODUCTION. A current issue in hand musculoskeletal models is the representation of the real capacities of the subjects [1,2]. In particular, the distribution among all hand muscles of the physiological cross-sectional areas (PCSA), representing the force capacity of a muscle, is considered the same for all subjects whereas subjects might present specific muscle adaptations, e.g. resulting from ageing or training. To improve the integration of subject’s specificities, this study aimed to develop a method to estimate subject-specific muscle parameters for the five main muscle groups of the hand. METHODS. A control group of 13 subjects (young, healthy, non-trained) as well as 3 “particular” subjects (a rock climber, a boxer, and a hand osteoarthritis patient) performed 8 maximal isometric contraction tasks about the wrist and finger joints (Fig. 1). Then, for each subject, a maximum muscle stress and the PCSA of the five muscle groups were estimated by adjusting an initial hand model [3] through an optimization which aimed to minimize the differences between the measured net moments and their estimation through the model. The influence of this method was evaluated by comparing the muscle forces estimated during a power grip task using either the initial or the subject-specific models. Table 1 – Moment capacities (N.m) about the wrist of four of the five muscle groups of the hand obtained with the initial model parameters and with the subject-specific ones.
Initial model Control group Climber Boxer OA patient
Wrist flexors 6.6 31.2 ± 4.9 35.3 56.1 19.6
Wrist extensors -3.5 -16.5 ± 4.0 -23.0 -35.1 -14.8
Finger flexors 17.0 22.4 ± 5.2 41.8 30.2 6.9
Finger extensors -4.0 -9.7 ± 2.6 -17.8 -8.5 -4.8
RESULTS. Compared to the initial model, the muscle moment capacities estimated using the subject-specific parameters were in average 5 times higher for wrist muscles and 2 times higher for finger muscles (Table 1). Compared to the control group, the climber presented higher capacities for finger flexors, the boxer presented globally higher capacities and the osteoarthritis patient globally lower capacities. For the power grip task, the differences between the muscle forces estimated with the initial and the subject-specific models could be more than 80% for some muscles and null for others. DISCUSSION. Important adjustments were necessary to scale the model to the measured subject’s performances. These adjustments are consistent with the specificities of each subject and influenced importantly the estimation of the muscle load sharing with different effects for each subject.
References. [1] Sancho-Bru et al., Ann Biomed Eng 36:102‑107, 2008 [2] Valero-Cuevas et al., J Biomech
31:693‑703, 1998. [3] Goislard de Monsabert et al. Med Sci Sports Exerc 44:1906-1916, 2012.
COI. None
Figure 1. Experimental setup for one of the MVC tasks.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Peter Evans Ulnar head replacement
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Limited & Total Wrist Fusions
Arnold-Peter C. Weiss, M.D.
Providence, RI USA
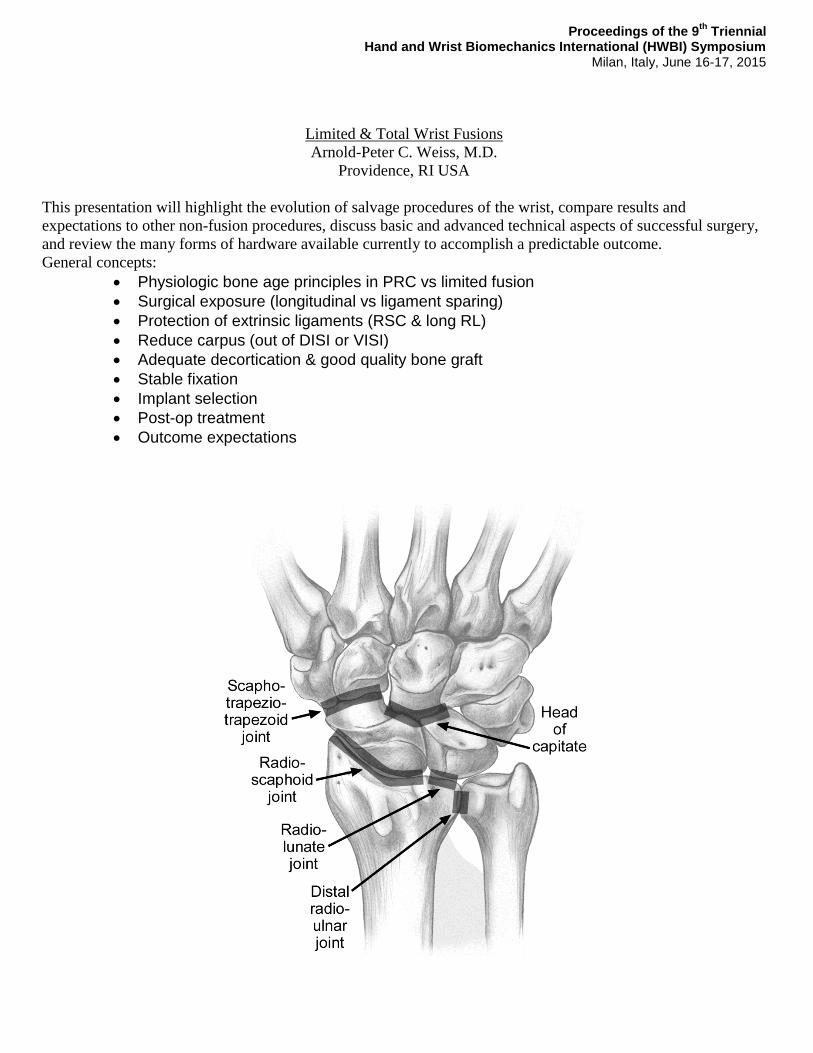
This presentation will highlight the evolution of salvage procedures of the wrist, compare results and
expectations to other non-fusion procedures, discuss basic and advanced technical aspects of successful surgery,
and review the many forms of hardware available currently to accomplish a predictable outcome.
General concepts:
Physiologic bone age principles in PRC vs limited fusion
Surgical exposure (longitudinal vs ligament sparing)
Protection of extrinsic ligaments (RSC & long RL)
Reduce carpus (out of DISI or VISI)
Adequate decortication & good quality bone graft
Stable fixation
Implant selection
Post-op treatment
Outcome expectations

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Biomechanical comparison between the Universal2 and Maestro total wrist implant: A finite
element study
Magnus K. Gislason1,2, Euan Foster3, David H. Nash3 1) Institute of Biomedical and Neural Engineering, Reykjavik University, Iceland
2) Department of Biomedical Engineering, University of Strathclyde, Glasgow, UK
INTRODUCTION. Total wrist implants have varied drastically in design from the introduction of the Swanson implant to the Meuli implant to the Volz and to the third generation of implants such as the Universal2, the Maestro and the ReMotion implants currently on the market [1]. Little research has been conducted into the mechanical response of the wrist implants under loading whereas much emphasize has been put on the hip and knee implants. The Universal2 implant and the Maestro implant are one of the most commonly used implants in the UK. The design features of the two implants vary significantly, in particular the carpal component, but additionally the polyethylene which is concave on the Maestro, but convex on the Universal2. The presented research studies the mechanical response of the two implants under a uniaxial compressive loading and investigates how the load is transmitted through the implant into the radius. METHODS. All components of the two implants were scanned using an industrial scanner and the components converted into STL formats. The model of the radius bone was created from images from a 7T MRI scan of a cadaveric specimen using the Mimics software (from Materialise). The implant objects were imported into Mimics, aligned and virtually inserted into the radius using Boolean operators. The objects were meshed and imported into Abaqus (from Simula) where the finite element model was created and solved. A 2000 N compressive load was applied to the model and the load distribution calculated. RESULTS. The results showed that the carpal component of the Maestro was subjected to higher stress values than the carpal component of the Universal 2. The load on the cancellous bone in the radius was greater for the Universal2 implant, suggesting improved long term stability.
Figure 1: Finite element models of
the implants
DISCUSSION. Both implant types demonstrated structural integrity under high degree of loading. The stress distribution of the Universal2 implant was more uniform than for the Maestro, resulting in higher stresses around the cancellous region of the radius, which would be beneficial for bone remodeling. Using the finite element method can give important information about the mechanical behavior of the wrist implants under loading and can lead to improved next generation implant designs. REFERENCES. [1] Adams BD, International Congress Series, 83-96, 2006. COI. The authors declare no conflict of interest.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Biarticular Concentric Carpal Mechanics and Coxa Manus Surgery
Gaetano Maurizio Grippi
Department of Hand Surgery in the UOA of Orthopaedic – S. Lazzaro Hospital - Alba (CN) - ASL CN2 of Piemont, Italy
INTRODUCTION. Concept and surgical applications of Biarticular Concentric Carpal Mechanics (BCCM) is discussed. This
assimilates the carpus to a bi-articular hip prosthesis that, in the small prosthetic head - reproduced from Capitate - has the center of
rotation (CR). Using this similitude, at the center of the carpus is identified the “ball and socket” joint of Coxa Manus (CM), the "true"
primitive carpal joint, where takes place the s.c. “dart-trowing motion” and whose disjointedness causes Carpal Instability, certified by
the static or dinamic dislocation of capitate’s head.
The Human bi-articular carpal joint comes from the Reptiles uni-carpal joint, with an onto-philogenetic development for which the
radio-carpal appears after the mid-carpal joint. So that, in wrist is possible to distinguish two parts: a distal, ancient: the Paleo-Carpus,
represented by couple capitate-hamate; the other proximal, recently: the Neo-Carpus, represented by the proximal carpal row .
METHODS. In generic radio-carpal injury of s.c. Adaptive Carpus (AC) is spontaneus decay of bi-articular towards uni-articular
function, basically centred on Coxa Manus and its “dart-trowing motion”. This patho-mechanics (resurrecting the ancestral Paleo-
Carpus leadership) is potential stereotype in any anatomical alteration (congenital or acquired) of Neo-Carpus: then, emerging in the
outcomes of distal radius fractures, in Madelung, in Kienböck, in SNAC-SLAC-SCAC wrist, etc.
In the same way – to recover problematic radio-carpal injures - valid surgical option is to concentrate all movement on capitate’
head. This concept is the s.c. "Grail of wrist surgery" and has produced the Coxa Manus Surgery methodology. Particularly useful and
versatile is the Reconstruction of Coxa Manus that consists in a volar radius-lunate-(hemi-scaphoid) arthrodesis (with scaphoid distal
resection). The intervention optimizes the physiological adaptation by bi-articular towards uni-articular function, implicit in Adaptive
Carpus. In this way, the capitate’s head is centred and provided with a new stable support.
Other surgical applications originate from the ascertainment that the resection of the first carpal row (RFCR) is an excellent
operation, because the bony demolition, so apparently serious, is a meniscectomy, after all. After this operation the axis of the hand and
the axis of the radio-ulnar carpal joint continue to converge in the head of the capitate where, under lee of the dimple of lunate, they
constitute a new carpal rotation centre. But, RFCR is contraindicate if the dimple of lunate or the head of the capitate have been
damaged. In this cases to overcome the obstacle can be carried out the Substitutive Center-carpic Resection consisting in the RFCR
associated with capitate prosthesis.
RESULTS In support are presented 102 operated cases from 1997 to 2014. The results, (assessed according to the parameters of the
Mayo Wrist Score Chart, with 6,5 years average follow-up) have been satisfactory in over 80 percent of patients.
DISCUSSION. We believe that BCCM has re-built the knowledge of wrist physiology with a new and simple biomechanical concept.
Beginning in 1997 from these concepts we have projected and carried out the Coxa Manus Surgery that has given and proved good
results. This, certainly could be an interesting and fecund future field of wrist surgery.
References. 1)- Grippi GM: Cinematica del condilo carpale con introduzione al Modello Carpale Biarticolare Concentrico (MBC) e sua applicazione al problema dell’instabilità carpale. Riv. Chir. Riab.Mano Arto Sup., 34 (3), 389-401, 1997.
2 )- Grippi GM: Patomeccanica “regressiva” delle fratture articolari del radio distale e salvataggio con l’intervento di Ricostruzione della Coxa Manus. Min. Ort. Traum.
Vol. 59, n° 5, ottobre 2008. 3)- Grippi GM, Cugola L.: Carpo adattativo e trattamento con la chirurgia della Coxa Manus. Riv. Chr. Mano – Vol. 48 (2) 2011.
4)- Grippi GM: La ricostruzione della “Coxa Manus” Indicazioni e tecnica chirurgica. Riv. Chir. Mano – Vol. 40 (3) 2003.
5)- Grippi GM: La protesizzazione del capitato – indicazioni e tecnica chirurgica. Riv Chir Mano – Vol. 43(1) 2006 6)- Grippi GM: La Chirurgia della Coxa Manus: Riv. Chir. Mano – Vol. 45 (2) settembre 2008.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
CMC Joint Biomechanics
Joseph J. Crisco, Ph.D.
Brown University, Providence, Rhode Island, USA Much of the hand’s functional capacity is due to the versatility of the motions at the first
carpometacarpal (CMC) joint of the thumb. Utilizing our established methodology to accurately track in vivo
skeletal kinematics, we have been able to gain new insight into the complete envelope of motion at CMC joint
during the performance of functional tasks. These new insights, along with those changes that occur with early
stage osteoarthritis at CMC joint, will be presented.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Trapeziometacarpal joint fusion reduced the thumb-tip trajectory area approximately 30 % of the original trajectory area: a cadaveric study
Yusuke Kawano1, Toshiyasu Nakamura2, Mitsunori Tada3, Yusaku Kamata1, Shinjiro Sueda4,
Dinesh Pai5, Takeo Nagura6, Kazuki Sato1 1) Department of Orthopaedic Surgery, School of Medicine, Keio University, Tokyo, Japan
2) Clinical Research Center, International University of Health and Welfare, Tokyo, Japan
3) Digital Human Research Center, National Institute of Advanced Industrial Science and Technology, Tokyo, Japan
4) MIT Computer Graphics Group, Computer Science & Artificial Intelligence Laboratory, Massachusetts Institute of Technology, Cambridge, MA, U.S.A
5) Department of Computer Science, University of British Columbia, Vancouver, Canada
6) Department of Clinical Biomechanics, School of Medicine, Keio University, Tokyo, Japan
INTRODUCTION: Although a number of articles discussed the clinical outcomes of arthrodesis of the thumb trapeziometacarpal (TMC) joint, to the best our
knowledge, there is no biomechanical cadaveric study examining reduced area of the thumb-tip trajectory after the TMC joint fusion. The objective of our study was to
investigate how large area of the thumb-tip trajectory was reduced due to the TMC joint fusion.
METHODS: 6 fresh-frozen cadavers were used in this study. Three optical markers were fixed directly to the bones by stainless steel wires drilled into the scaphoid,
trapezium, metacarpal, proximal phalanx, and distal phalanx of the thumb and 6 optical markers were fixed to the base of the custom-built experimental apparatus.
The external fixation pins were screwed to the third metacarpal and radius to fix the specimen to the apparatus. Four extrinsic tendons (FPL, EPL, EPB, APB) were
pulled independently by computer-controlled serve motors. Tension by the servo motors was applied to the distal tendons of 4 extrinsic thumb muscles, while tension
by static weight was applied to 4 intrinsic muscles (APB, FPB, AdD, OP) through Nylon cords representing the direction of each muscle [1]. Finger motion was measured
under six different intrinsic muscle tensions, 0.00N, 0.98N, 1.96N, 2.94N, 3.92N, and 4.90N, before and after the TMC fixation with pins. The motions of these markers
were recorded by a motion capture system (OptiTrack Flex 13; Natural Point, Inc.) (Fig. 1). Surface geometries of the markers and bones created from the CT images
were fit into the marker trajectories from the motion capture system to reconstruct the 3-dimensional bone motion.
RESULTS: Fig. 2 shows the area of the thumb-tip trajectories for six different tensions of the APB, when the FPL was pulled in one specimen, before (Fig. 2A) and
after (Fig. 2B) the TMC joint fixation. Fig. 3 demonstrates the superimposed trajectories. This figure clearly indicates that the fingertip trajectory area was extremely
smaller when the TMC joint was fixed. Trajectory area was limited to approximately 30% of the original area after the TMC joint was fixed.
Figure 1
Figure 2A
Figure 2B
Figure 3
DISCUSSION: Arthrodesis of the TMC joint provides stability of the thumb, while resulting in decrease of the range of motion of the thumb. Despite the marked
decrease in motion, subjective functional complaints may be minimal [2]. In this study, we revealed how the area of thumb-tip trajectory was decreased after the TMC
joint fixation compared with no fixation. The trajectory area decreased to approximately 30% of original area after the TMC joint fusion. We consider that this
technique and result of this study will be useful for understanding thumb motion after the TMC arthrodesis.
SIGNIFICANCE. This study revealed the reduction of the thumb-tip trajectory area by the TMC joint fixation compared with no TMC arthrodesis. The trajectory area
was reduced to approximately 30% of the original trajectory area after the TMC joint fixation.
Acknowledgements. The authors would like to sincerely thank the Clinical Anatomy Laboratory, Department of Anatomy, School of Medicine, Keio
University, Japan, for allowing access to the fresh cadaver upper extremity specimens. The authors also wish to express their profound appreciation to
Prof. Jinzaki and Prof. Kuribayashi, Department of Diagnostic Radiology, School of Medicine, Keio University for CT analysis.
References. [1] Pearlman JL et al, J Orthop Res, 306-12, 2004 [2] Bamberger HB et al, J Hand Surg Am, 605-11, 1992
COI. None declared.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
MATHEMATICAL MODELING OF THE TRAPEZIOMETACARPAL JOINT FOR IN VIVO STRESS
DISTRIBUTION ANALYSIS
Benjamin Dourthe1, Priscilla d’Agostino1, Filip Stockmans1, 2, Faes Kerkhof1, Evie Vereecke1 1) Development and Regeneration, KU Leuven, Kortrijk, Belgium
2) AZ Groeninge, Kortrijk, Belgium
INTRODUCTION. Evaluating the stress distribution within the trapeziometacarpal (TMC) joint during daily activities is a clinically
relevant way to investigate the biomechanical behavior of this complex joint. Such insights are essential to achieve a better
understanding of joint functioning and are particularly important in establishing new prevention approaches for osteoarthritis (OA).
METHODS. Static CT scans of the hand region of 20 female volunteers (mean age: 60.8 years) were taken in three different
configurations: relaxed neutral, lateral pinch and power grasp, using a radiolucent jig with embedded load cell (Brown University,
USA). Four subjects showing signs of OA were excluded from the study. Scans were segmented using Mimics (Materialise,
Belgium) and 3D models of the first metacarpal (MC1) and the trapezium were created. The articular area of each bone was
quantified based on manual measurements performed on the 3D bone models. A custom-written Matlab code - based on the
finite deformation biphasic theory1 and cartilage deformation properties
1, 2 - was used to evaluate the contact area and stress
distribution of each bone. A quadrant division method3 was used to identify articular sub-regions subjected to the highest stress.
RESULTS. No significant difference was observed between the total articular area of the MC1 and trapezium. The contact area
of the trapezium was slightly smaller compared to MC1, but this was only statistically significant in the lateral pinch position (p <
0.05). Contact stress calculation revealed a similar amount of stress between neutral and lateral pinch. More stress was reported
during power grasp. Very consistent results for high stress location on the volar/ulnar articular sub-region were found in the
neutral and power grasp configuration. More variation was reported during lateral pinch.
DISCUSSION. The findings suggest that a power grasp task elicit higher contact stresses and might therefore represent a more
critical configuration for clinical evaluation of the TMC joint. Lateral key pinch, on the other hand, is less reproducible and might
create a higher joint instability. The mathematical model presented in this paper offers the possibility to predict contact stress and
stress distribution based on in vivo CT scans, which is relevant for the investigation of the onset of OA and might contribute
towards better prevention and treatment strategies.
Acknowledgements. The author wishes to thank Dr. Eddy Brugman and the technical staff of the radiology department at the
AZ Groeninge (Kortrijk, Belgium) for their contribution to this study.
References. [1] Kwan et al., J. Biomech, 23: 145-155, 1990; [2] Koff et al., J Hand Surg, 28A: 597-604, 2003; [3] Momose et al.,
J. Hand Surg, 24A: 491-495, 1999
COI. The author reports no potential conflict of interests.
FIGURE: Stress distribution pattern of one subject during power grasp: a) MC1; b) Trapezium (right hand)
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
CT scans allows for early evaluation of joint space narrowing within the first carpo-metacarpal
joint osteoarthritis.
M. Conconi1, E. Halilaj2, V. Parenti Castelli1, J. J. Crisco2
1) Health Science and Technology Center (HST-CIRI), University of Bologna, Italy 2) Center for Biomedical Engineering, Brown University, Providence, RI, USA
INTRODUCTION. The International Society of Osteoarthritis Research (OARSI) recognizes as the current gold
standard for assessing joint damage in osteoarthritis (OA) the plane radiography. The most reliable method of
staging for the first carpo-metacarpal (CMC) joint is the Eaton and Littler classification. Radiological staging
systems show suboptimal interobserver agreement [1] and they lack of the quantitative characterization of the
disease required for a longitudinal study [2]. In line with the OARSI recommendations, this work aims at
identifying geometrical quantities whose numerical evaluation allows for the characterization of OA onset and
progression. In particular we want to investigate if joint space narrowing (JSN), normally associated with later
stage of OA (Eaton Stage III and IV), may be a meaningful quantitative marker for detecting OA onset via CT
scan.
METHODS. After receiving IRB approval and informed consents, 59 asymptomatic subjects (34 women, age
42.3 ± 16.4; 25 men, age 36.8 ± 13.6) and 39 patients with early OA (Eaton Stage I; 31 women, age 53.9 ± 6.8;
7 men, age 56.3 ± 6) were recruited and examined by a board-certified orthopedic surgeon. The CMC joints in
the dominant or OA affected hands were CT-scanned in neutral position (General Electric, Milwaukee, WI;
80kVp and 40mA; slice thickness 0.625mm; in-plane resolution 0.4mm x 0.4mm). 3-D polygonal meshes of the
trapezium and the first metacarpal bone were segmented (Mimics®, Materialise, Leuven, Belgium). The relative
bone to bone distance was evaluated through distance maps [3]. Joint space (JS) was computed as the fifth
percentile of the distances distribution of the trapezium respect to the first metacarpus. Four-way ANOVA was
used to determine the effects of sex, age, pathology and bone size on the JS. Statistical significance was set at
p<0.05.
RESULTS. The JS is independent on the gender (p=0.70), age (p=0.33) or bone size (p=0.17) but does vary
with the pathology onset (p<0.0001). In the healthy population the JS is 0.99 (±0.18) mm, while in arthritic
population at Eaton Stage I is 0.65 (±0.26) mm.
DISCUSSION. Despite JSN for the CMC joint is radiographically associated only with the late progression of
OA (Eaton Stage III and IV), Ct scan allows for its early evaluation (Eaton Stage I) in the CMC joint. The
numerical evaluation of JSN here proposed may possibly be used in diagnosis and longitudinal evaluation of
the OA progression.
Acknowledgements. This work was supported by NIH AR059185.
References. [1] Spaans (et al.), J Hand Surg Am. 36, 1467–1470, 2011. [2] Sonne-Holm (et al.), Osteoarthr.
Cartil.. 14, 496–500, 2006. [3] Tersi (et al.), EURASIP Journal on Advances in Signal Processing, pages 1–10,
2010.
COI. No actual or potential conflict of interest in relation to this article.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
WOMEN HAVE SIMILAR CARPOMETACARPAL JOINT MORPHOLOGY TO MEN
M.T.Y.Schneider1, J.J. Crisco2, A.C. Weiss2, A.L. Ladd3, P. Nielsen1,4, T. Besier1,4, J. Zhang1
1) Auckland Bioengineering Institute, The University of Auckland, Auckland, New Zealand
2) Department of Orthopaedics, Brown University, RI, USA
3) Department of Orthopaedic Surgery, Stanford, Stanford University, CA, USA
4) Department of Engineering Science, The University of Auckland, Auckland, New Zealand INTRODUCTION. It is believed that the morphology of the CMC joint may play a role in the mechanical onset of CMC OA (Ateshian et
al., 1992), providing an explanation for the discrepancy in the prevalence of disease between men and women (North and Rutledge, 1983; Felson et al., 2000). However, previous studies have reported inconsistent articular shape differences (North and Rutledge, 1983; Ateshian et al., 1992). Recent evidence suggests that the morphology of the CMC joint does not differ between men and women (Halilaj et al. 2014). Statistical shape models have the potential to realistically describe anatomy and its variation in a population by decomposing shapes into a set of mathematical descriptors (Cootes et al., 1992). Here we present a statistical shape model of the articular surfaces of the first metacarpal and trapezium bones to characterize the size and shape of the CMC joint and investigate any differences in morphology with respect to sex and age. METHODS. A training set of 50 healthy CMC joints were manually segmented from CT images of the hand with a resolution of
0.4x0.4x0.625mm (age range: 18 yrs to 67 yrs; 24 females and 26 males). A custom piecewise parametric template mesh was created
for the articulating surface, and fitted to manual segmentations of the articulating surface to create a set of correspondent meshes of the
CMC joint surface. Principal component analysis was performed on this training set resulting in a SSM of the articular surface. We then
performed linear regression and one-way ANOVA on the mode scores against age and sex.
RESULTS. As expected, the first mode (size) of the articular surface correlated with sex (p< 0.001) (Figure 1). None of the other modes
(of morphological variation) were correlated to sex. After size-normalization, none of the modes were correlated with sex. Furthermore,
none of the modes showed significant correlation with age.
Figure 1 – Statistical shape model of CMC joint showing variation along the first principal component (size) from 2 std (men), to 0 std, to
+2 std (women).
DISCUSSION. The purpose of this research was to characterize the size and shape of the articular surfaces of the trapezium and first
metacarpal bones with the novel use of a statistical shape model. Contrary to our expectations, we discovered that the only difference in
the morphology between men and women was size. In terms of CMC OA, these data in conjunction with previous data from our study on
entire CMC joint morphology suggest that size, not shape, may be the main morphological contributor towards increased prevalence of
OA in women. Size is important when considering activities of daily living that involve the wrist and hand, and a smaller trapezia and
metacarpal will affect the mechanics and function of the CMC joint. For example, if we consider that the moment arms of muscles
crossing the joint would scale with bone size, the forces required to generate the same torques for a given task would be higher. If we
consider this together with the smaller articular surfaces, this points towards potentially higher stresses in a smaller hand.
Acknowledgements. We would like to thank the Auckland Bioengineering Institute, Stanford Orthopaedics, and the NIH for funding.
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
“Dart-throwing motion in patients with scapholunate instability.
A dynamic 4D computed tomography study”
Authors: M. GARCIA-ELIAS, MD PhD (*), X. ALOMAR SERRALLACH, MD (**), J. MONILL SERRA, MD (**)
(*) From the Institut Kaplan. Hand and Upper Extremity Surgery. Barcelona (Spain)
(**) From the Clínica Creu Blanca. Department of Radiology. Barcelona (Spain)
Correspondence: Dr. Marc Garcia-Elias. Institut Kaplan. Passeig de la Bonanova, 9, 2on 2ª. 08022 Barcelona (Spain). Phone number: (+34) 934 178 484.E-mail address: [email protected]
Abstract
The purpose of this study was to assess differences in carpal bone motion between normal individuals and patients with scapholunate interosseous ligament (SLIL) disruptions using four-dimensional computed tomography (4D-CT) scans
4D-CT scans of the wrist of 6 normal volunteers and 6 patients with SLIL injury (3 partial, 3 complete) were obtained while moving the wrist along the dart throwing (DT) plane. Once processed, movies were assessed by 3 independent investigators who identified and scored differences in carpal bone motion between the three wrist conditions.
During DT rotation, most motion occurs at the midcarpal joint, the scaphoid and lunate remaining still. When the SLIL is completely ruptured, by contrast, the scaphoid moves together with the capitate, as if it was a distal row bone. Up to some extend the lunate follows the scaphoid only when the SLIL is partially torn.
This preliminary study suggests: 1) that the degree of SLIL rupture may be deducted by observing intracarpal motion along the DT plane. 4D-CT scans have shown to facilitate this assessment; and 2) If the SLIL is completely ruptured, "dart.throwing" exercises may have a negative impact in the healing potential of the disrupted ligaments.
In this presentation the feasibility of these type of studies, taking into consideration the amount of radiation involved in such scanning, will be discussed

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
IN VITRO SCAPHOLUNATE ROTATIONS WITH FDP TENDON LOADING
Greg Couzens1,2, Lance Wilson2, Caroline Grant2
1Brisbane Hand & Upper Limb Clinic, Brisbane, Queensland, Australia
2Institute of Health & Biomedical Innovation, Queensland University of Technology, Brisbane, Queensland, Australia
INTRODUCTION. The effect of grip on the scapho-lunate interval is recognised in the clench fist XR. Grip
strengthening is often introduced early in post-surgical or injury rehabilitation despite little being known on the
effects on carpal bone rotations. We loaded FDP tendons in cadaver wrists to determine the effect of load and
wrist angle on SL rotations.
METHODS. Three cadaver wrists had the carpus exposed preserving the capsular ligaments. Optotrac (NDI,
Ontario, Canada) markers were placed in the bones of interest and the forearm mounted in a custom jig that
allowed loading of the tendons. The positions of the carpal bone markers were recorded with the wrist in 30
degrees of flexion, neutral and 30 degrees of extension with the FDP tendons loaded from 0 to 50 Newtons.
The 3D motion was calculated using custom software written in Matlab (Mathworks, Matick, Ma) and the relative
motion of the bones determined. The cadaver forearms were CT scanned pre and post testing and solid models
of the carpal bones created (Amira, FEI, Oregon & Solidworks, Waltham, Ma).
RESULTS This is a small series and only limited conclusions can be made. The rotations induced ni the carpal
bones are small. The rotations increase with load. The lunate moves further in same direction with increasing
load. Although absolute carpal bone rotations increase with load the relative motion may decrease with load.
The least absolute and relative rotations occurred with loading in neutral wrist position. Relative carpal bone
rotations occurred maximally in supination then extension then ulnar deviation.
DISCUSSION. Relative lunate supination and radial deviation load the dorsal Scapholunate ligament. Approximately 20kg of load (which may represent as little as 2-3 kg of load at the finger tip) is predicted to produces 5 degrees of supination of the lunate.
0
2
4
6
0 10 20
Lunate supination wrt Scaphoid in 30 degrees extension
Series1
Linear (Series1) 0.00
2.00
4.00
6.00
0 5 10
Lunate ulnar deviation wrt Scaphoid 30 degrees flexion
Series1
Linear (Series1)

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
SEGMENTAL PRESSURE ALONG THE CARPAL CANAL: A STUDY PERFORMED WITH CHANGES IN HAND AND WRIST POSITION IN PATIENTS WITH CTS AND CONTROLS
Riccardo Luchetti (*), Rudolf Schoenhuber (**), Peter Nathan (***)
(*)Contract Professor, University of Milan, Milan, Italy, (**) General Hospital, Bolzano (Italy), (***) Portland Hand Surgery and Rehabilitation Center, Portland (USA)
We investigated pressure at 1 cm interval along the carpal tunnel in 39 patients with carpal tunnel syndrome
(CTS) and 12 controls. Pressure were measured for relaxed and gripping hand positions in combination with
neutral, extended and flexed wrist position. Patient pressure exceeded control pressure, were below the
previously reported 30 mmHg threshold for four of five locations in the relaxed neutral position and were
typically greater in extension (fig 1) than in flexion (fig 2). In the neutral position, both patients and control
pressures were slightly above threshold levels just distal to the tunnel. Maximum intratunnel pressure were
generally found in the central part of the tunnel and minimum pressures in the distal tunnel. Gripping hand
pressures in the tunnel were lowest with the wrist flexed. In both controls and CTS patients, only in the neutral
wrist and relaxed hand positions were pressures highest at the point where nerve conduction studies have
indicated the nerve is most likely to be compromised.
Fig 1
Fig 2

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
BIOMECHANICS OF THE TRANSVERSE CARPAL LIGAMENT
Zong-Ming Li Hand Research Laboratory
Departments of Biomedical Engineering, Orthopaedic Surgery, and Physical Medicine & Rehabilitation Cleveland Clinic, Cleveland, Ohio
The transverse carpal ligament (TCL) is a significant constituent of the wrist and forms the volar boundary of the
carpal tunnel. It has biomechanical and physiological functions that include serving as a pulley for the flexor tendons,
anchoring the thenar and hypothenar muscles for hand strength, stabilizing the bony structure, and providing wrist
proprioception. The TCL has attracted extensive research attention during the past two decades, and considerable
knowledge has been gained from basic science research and its clinical implications in hand surgery. The science of
this ligament has progressively evolved with regard to its cellular mechanisms, histological composition, fiber
architecture, neural anatomy, morphological characteristics, material properties, and structural mechanics.
This presentation will review our recent studies regarding the biomechanical role of the TCL in the compliant
characteristics of the carpal tunnel. First, force applied to the TCL from within the carpal tunnel increased the arch
height and area due to arch width narrowing from the migration of the bony insertion sites of the TCL. These
experimental findings were further elucidated through geometric modeling which revealed the relationships among
arch width, height, and area. Second, carpal arch deformation showed that the carpal tunnel was more flexible at the
proximal level than at the distal level, and was more compliant in the inward direction than in the outward direction.
The hamate-capitate joint had larger angular rotations than the capitate-trapezoid and trapezoid-trapezium joints for
their contributions to changes of the carpal arch width. Third, pressure application inside the intact and released carpal
tunnels led to increased carpal tunnel cross-sectional areas, which were mainly attributable to the expansion of the
carpal arch formed by the TCL. Transection of the TCL led to an increase of carpal arch compliance that was nine
times greater than that of the intact carpal tunnel. The carpal tunnel, while regarded as a stabile structure,
demonstrates compliant properties that help to accommodate biomechanical and physiological variants such as
changes in carpal tunnel pressure.
Additional discussions will include the areas of future studies and their clinical translation. Transecting the TCL
has been shown to benefit patients by relieving symptoms of carpal tunnel syndrome. However, disrupting the tunnel
structure may compromise other aspects of hand function; these implications remain to be further clarified.
Alternative surgical techniques and non-surgical strategies related to the TCL continue to be explored, each
warranting rigorous scientific investigation to establish evidence-based interventions. Regarding the many etiological
factors of carpal tunnel syndrome, thickening and stiffening of the TCL are suggested as possible mechanisms of
median nerve compression and carpal tunnel syndrome. Future studies are needed to elucidate the potential
mechanobiological effects on the TCL resulting from repetitive hand use that involves biomechanical interactions
among tissues. For carpal tunnel biomechanics and its relationship to the TCL, a validated computational model of
the wrist with high fidelity constitutive components is valuable to assist our understanding of pathomechanisms and
to provide patient-specific simulation and intervention. More effort is needed to investigate TCL and wrist function in
the in vivo, physiological environment with the aid of dynamic imaging modalities, such as ultrasound, fluoroscopy,
computed tomography, and magnetic resonance imaging. Such advancement of knowledge in the TCL and its integral
structure will further improve clinical management of hand and wrist conditions.
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
ULTRASOUND ASSESSMENT FOR THE EFFECTIVENESS OF CARPAL TUNNEL RELEASE ON
MEDIANERVE DEFORMATION
Y. Yoshii1, T. Ishii1, W.L. Tung2 1) Department of Orthopaedic Surgery, Tokyo Medical University Ibaraki Medical Center, Ami, Ibaraki, Japan
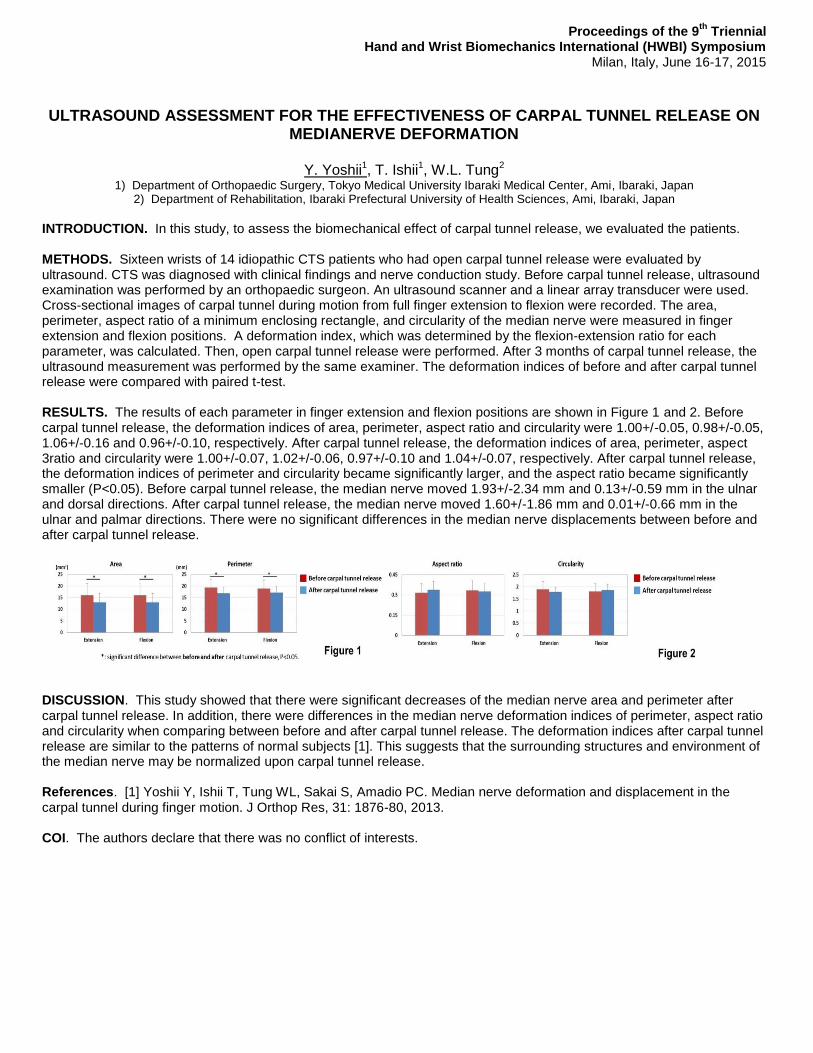
2) Department of Rehabilitation, Ibaraki Prefectural University of Health Sciences, Ami, Ibaraki, Japan INTRODUCTION. In this study, to assess the biomechanical effect of carpal tunnel release, we evaluated the patients. METHODS. Sixteen wrists of 14 idiopathic CTS patients who had open carpal tunnel release were evaluated by ultrasound. CTS was diagnosed with clinical findings and nerve conduction study. Before carpal tunnel release, ultrasound examination was performed by an orthopaedic surgeon. An ultrasound scanner and a linear array transducer were used. Cross-sectional images of carpal tunnel during motion from full finger extension to flexion were recorded. The area, perimeter, aspect ratio of a minimum enclosing rectangle, and circularity of the median nerve were measured in finger extension and flexion positions. A deformation index, which was determined by the flexion-extension ratio for each parameter, was calculated. Then, open carpal tunnel release were performed. After 3 months of carpal tunnel release, the ultrasound measurement was performed by the same examiner. The deformation indices of before and after carpal tunnel release were compared with paired t-test. RESULTS. The results of each parameter in finger extension and flexion positions are shown in Figure 1 and 2. Before carpal tunnel release, the deformation indices of area, perimeter, aspect ratio and circularity were 1.00+/-0.05, 0.98+/-0.05, 1.06+/-0.16 and 0.96+/-0.10, respectively. After carpal tunnel release, the deformation indices of area, perimeter, aspect 3ratio and circularity were 1.00+/-0.07, 1.02+/-0.06, 0.97+/-0.10 and 1.04+/-0.07, respectively. After carpal tunnel release, the deformation indices of perimeter and circularity became significantly larger, and the aspect ratio became significantly smaller (P<0.05). Before carpal tunnel release, the median nerve moved 1.93+/-2.34 mm and 0.13+/-0.59 mm in the ulnar and dorsal directions. After carpal tunnel release, the median nerve moved 1.60+/-1.86 mm and 0.01+/-0.66 mm in the ulnar and palmar directions. There were no significant differences in the median nerve displacements between before and after carpal tunnel release.
DISCUSSION. This study showed that there were significant decreases of the median nerve area and perimeter after carpal tunnel release. In addition, there were differences in the median nerve deformation indices of perimeter, aspect ratio and circularity when comparing between before and after carpal tunnel release. The deformation indices after carpal tunnel release are similar to the patterns of normal subjects [1]. This suggests that the surrounding structures and environment of the median nerve may be normalized upon carpal tunnel release. References. [1] Yoshii Y, Ishii T, Tung WL, Sakai S, Amadio PC. Median nerve deformation and displacement in the carpal tunnel during finger motion. J Orthop Res, 31: 1876-80, 2013. COI. The authors declare that there was no conflict of interests.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
TENSILE PROPERTIES OF THE TRANSVERSE CARPAL LIGAMENT IN-SITU
Ukadike C. Ugbolue1, Quentin A. Fogg2, Magnus K. Gislason3
1) School of Science and Sport, Institute for Clinical Exercise & Health Science, University of the West of Scotland, UK 2) School of Life Sciences, College of Medical, Veterinary and Life Sciences, University of Glasgow, UK
3) Biomedical Engineering Department, School of Science and Engineering, Reykjavik University, Iceland
INTRODUCTION. The clinical motivation for this study is Carpal Tunnel Syndrome (CTS) which is regarded as
the most common peripheral neuropathy affecting the hand. In the years gone by, hand research studies have
grown and continue to gain popularity. These developments have been channeled towards biomechanical
related research studies designed to elucidate some of the underlying mechanisms and biomedical aspects
associated with the carpal tunnel complex. Recently, a novel method has been developed to determine the
tensile properties of the Transverse Carpal Ligament (TCL) in-situ [1]. This study aims to describe the
biomedical aspects of the novel TCL tensile testing procedure.
METHODS. Biomechanically, the TCL has been studied to determine its compressive [2] and tensile [3, 4]
properties. Although, these methods have involved either excising the TCL or determining the biomechanical
properties of the TCL intact / transected, experimentally there is still no widely accepted method designed to
specifically evaluate the tensile properties of the TCL and Carpal Tunnel Complex (CTC). Hence, to date, there
are no known methods to test the TCL to failure in-situ. The proposed method uses video analysis techniques
together with a Maillon Rapide Delta (similar to a Carabiner) to determine the tensile properties of the TCL–
CTC. Six embalmed cadaveric specimens amputated at the mid-forearm and aged (Mean (SD)): 82 (6.29)
years were tested. Using trigonometry and geometry the elongation and strain of the TCL and carpal arch were
calculated. Tensile properties of the TCL–CTC and Load–Displacement data were also obtained. Descriptive
statistics, one-way ANOVA together with a Post-hoc analysis (Tukey) and t-tests were incorporated.
RESULTS. The TCL failed either at the mid-substance or at their bony attachments. There were no significant
differences between the original TCL width and TCL at peak elongation (p = 0.108). There were significant
differences between the original Carpal Arch (CA) width and CA width at peak elongation (p = 0.002). At
maximum deformation the peak load and maximum TCL displacements ranged from 285.74N to 1,369.66N and
7.09mm to 18.55mm respectively. The load at tensile strength ranged from 272.09N to 1293.36N and the
ultimate tensile strength mean (SD) was 23.99 (10.68) Nmm-2.
DISCUSSION. A novel method to determine the tensile properties of the TCL–CTC has been developed. The
methodology has been validated and is capable of generating highly repeatable data.
References. [1] Ugbolue et al, Br J Sports Med, 48: A69-A70, 2014; [2] Holmes et al J Orthop Res, Nov; 29(11):
1682-7, 2011; [3] Li et al, J Biomech Eng, 131(8): 081011 (6 page) (Abstract), 2009.
COI. There are no conflicts of Interest associated with this study. Acknowledgements. None

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Three-Dimensional Stiffness of the Wrist Structure
Joseph N. Gabra1,2
, Zong-Ming Li1,2
1) Hand Research Laboratory, Departments of Biomedical Engineering, Orthopaedic Surgery, and Physical Medicine and Rehabilitation,
Cleveland Clinic, Cleveland, OH, U.S.A.
2) Department of Chemical and Biomedical Engineering, Cleveland State University, Cleveland, OH, U.S.A INTRODUCTION. The wrist structure is composed of irregularly shaped carpal bones interconnected by
numerous ligaments, resulting in complex structural mechanics. Previous studies of wrist structural
biomechanics were mainly limited to uniaxial and planar experimentation and computation, but the mechanical
properties in 3D is not well understood. The purpose of this study was to examine the 3D stiffness
characteristics of the wrist with displacement perturbations applied to the carpal arch.
METHODS. A custom apparatus held a cadaveric hand in a vertical position. The hamate was fixed to the
stationary apparatus and the trapezium was free to be displaced in 3D. An instrumented 6 DOF robot arm
displaced the ridge of the trapezium and measured 3D reaction forces. The displacement perturbations were
implemented with various magnitudes (0.5, 1.0, 1.5, and 2.0 mm) from its initial position towards 14 directions
that were equally spaced in 3D with an anatomically defined coordinate system (X, Y, Z axes corresponding to
the lateral(+), distal(+),and volar(+) directions, respectively) . Preconditioning was performed prior to
experimentation by displacing the trapezium 2 mm in each direction ten times. The force-displacement data
were used to determine a symmetric stiffness matrix [K] according to {f} = [K]{d}, where {f} and {d} are force and
displacement vectors, respectively. The matrix was determined by fitting the force-displacement data with least-
squares optimization procedures. Matrix eigendecomposition was used to determine the magnitudes and
directions of principal stiffness components.
RESULTS. The 3D stiffness matrix was determined (right, R2 =
0.8960). Eigendecomposition of the stiffness matrix resulted in
the three principal components as 20.80, 3.55, 3.04 N/mm
with corresponding principal directions as (0.84, -0.06, 0.55), (-0.46, 0.45, .76), and (0.29, 0.89, -0.35). The magnitudes and directions of the principal stiffnesses are shown in Figure 1. The determinate of the matrix was 224.36 N3/mm3. DISCUSSION. The wrist structure demonstrated an anisotropic behavior as indicated by the different magnitude
of principal components. The maximum principal stiffness component was 6.8 times greater than the minimum
principal component. The maximum principal stiffness occurred in a direction that is close to be in the
transverse plane; this may be due to ligament alignment, typically in the transverse direction, and the tightly
bound distal carpal row. The wrist structure had a minimum principal stiffness that was generally in the
longitudinal direction and it may be attributed to the less constraining articulations of the midcarpal joints. This
study provides advanced characterization of the wrist’s 3D structural stiffness for an improved insight of wrist
biomechanics, stability, and function.
Acknowledgements. NIH/NIAMS R21AR062753 and the CSU Dissertation Research Award
COI. There are no conflicts of interest to report.
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Subclinical Nerve Compression: A Subtle Physical Finding with Extensive Implications
William B. Ericson, Jr., MD, FACS Ericson Hand Center, Seattle, Washington, USA
INTRODUCTION. Symptomatic peripheral nerve compression is thought to affect a small percentage of the
general population. It is this author’s opinion that subclinical nerve compression (no symptoms but abnormal
physical exam findings) is actually ubiquitous. This observation has profound implications in the etiology of a
large number of clinical conditions of the hand and arm.
METHODS. The strength of the flexor digitorum profundus of the index finger (FDP IF) and flexor pollicis
longus (FPL) are noted by the author to dependent on wrist position, whereas the strength of the long, ring and
small finger flexors (FDP LF, FDP RF, FDP SF) are not. Specifically, with the wrist flexed, the FPL and FDP IF
are weak, but FDP LF, FDP RF, and FDP SF are strong. This weakness is localized to the anterior
interosseous nerve (AIN), yet EMG and NCV testing have a false negative rate of about 97% when evaluating
this weakness. The Blix curve [1] [2] is applied to the flexors and accordingly 45 degrees of wrist extension
increases the length of the flexor muscle-tendon units by approximately 3cm. This increase in length results in
sufficient tension from stretch (rather than contraction) to compensate for the weakness of the FPL and FDP IF.
RESULTS. The weakness of the FPL and FDP IF is immediately and consistently reversed by surgical
decompression of the anterior interosseous nerve at the elbow. Operative experience at this time is quite large.
DISCUSSION. The concept of subclinical nerve compression and its significance has not been described
previously. An individual’s adaptation to painless weakness of the FPL and FDP IF occurs spontaneously and
without conscious effort or even awareness, but can be implicated in painful conditions involving the thumb,
index finger, and forearm that are otherwise lacking a unifying explanation.
Acknowledgements. This work is the original work of the author
References. [1] Blix, Magnus. Skandinavisches Archiv für Physiologie, p399-409, 1893 [2] Blix, Magnus. Skandinavisches Archiv für Physiologie, p240-251, 1896
COI. None.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
David Nelson Preventing complications with volar plating

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
THE BIOMECHANICS OF ARTICULAR FRACTURE FIXATION IN DISTAL RADIUS FRACTURES
Jorge Orbay MD Miami Hand Institute, Miami, Florida
The distal radius fracture is the most common fracture of the human skeleton. A fall on the outstretched hand is
the most common injury mechanism producing high impact loads. These forces interact with local bone and soft
tissue anatomy to produce characteristic fracture patterns. The basis of operative treatment is reduction of
deformity, stabilization of fracture fragments and early rehabilitation. Fixation implant design and technique of
application greatly influence the ability to maintain reduction. Physiologic forces during rehabilitation may
adversely affect results by causing fragment redisplacement.
This presentation examines the forces that cause the distal radius fracture and analyzes the biomechanical aspects
of fracture fixation in order to facilitate decision making during surgical treatment and provide insight to
improving implant design.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Correlation Between Distal Radius Cortical Thickness and Bone Mineral Density
Tracy Webber MD1, Shaun Patel MD2, Michael Pensak MD1, Olukemi Fajolu MD2, Tamara
Rozental MD2, Jennifer Moriatis Wolf MD1
1) Department of Orthopaedic Surgery, University of Connecticut Health Center, Farmington, Connecticut, USA 2) Department of Orthopaedic Surgery, Beth Israel Deaconess Medical Center, Boston, Massachusetts, USA
INTRODUCTION. Distal radius fractures occur commonly in elderly women, often in the setting of underlying osteopenia
or osteoporosis.1 A relationship between proximal humeral cortical width and bone density was noted previously.
2 We
hypothesized that there would be a similar relationship at the wrist. Our goal in this study was to determine the
interobserver reliability in measuring the cortical thickness3 of distal radii on posteroanterior radiographs obtained at the
time of injury, and to determine if there was a correlation between distal radius cortical thickness and hip and lumbar spine
scores on dual energy x-ray absorptiometry (DXA).
METHODS: Four blinded orthopaedic surgeons at two academic institutions reviewed standard posteroanterior wrist
radiographs of 80 women over the age of 50 years with distal radius fractures with DXA data obtained within the last two
years. Radial bicortical widths were measured at 50 mm and 70 mm proximal to the distal ulnar articular surface, and mean
bicortical thickness was calculated from radiographs of the injured wrist. The average bicortical width was compared to
each patient’s femoral and lumbar spine bone density measures. Data were analyzed using Pearson correlation
coefficients and simple linear regression. Inter-rater reliability was evaluated using intra-class correlation coefficients (ICC).
RESULTS: The inter-rater reliability for the average bicortical thickness had a high ICC value of .91. Average bicortical
thickness showed a statistically significant positive relationship with femoral bone density. Average bicortical thickness was
statistically correlated with femoral bone density values, with a one-mm increase in average bicortical thickness associated
with a 0.05 increase in femoral density (g/cm2). Average bicortical thickness was not associated with lumbar bone density.
DISCUSSION: Bicortical thickness of the distal radius was positively correlated with femoral bone density, although not
with lumbar spine density. This may reflect similarity in quality and loading properties of the femur and radius as
appendicular bones, compared to the axial spine. Identification of thinned distal radial cortices in association with distal
radius fracture is a simple qualitative observation that should prompt further evaluation with DXA and medical management
of bone insufficiency.
Acknowledgements: This work was funded from grants by the Orthopaedic Research and Education Foundation and the American
Foundation for Surgery of the Hand.
References. 1. Lauritzen JB et al. Osteoporos Int. 1993;3(3):133-7.
2. Mather J et al, J Shoulder Elbow Surg. 2013;22(6):732-8.
3. Schuind FA et al. J Bone Joint Surg Am. 1992;74(9):1418-29.
COI. Wolf - Salary, J Hand Surgery and Elsevier, Inc – editorial work. No other conflicts noted.
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
VARIATION IN ANTAGONIST ACTIVITY IN ISOMETRIC FOREARM MUSCLE CONTRACTION
Greg COUZENS1,2, Graham Kerr2, Derrick Maxwell2
1Brisbane Hand & Upper Limb Clinic, Brisbane, Queensland, Australia
2Institute of Health & Biomedical Innovation, Queensland University of Technology, Brisbane, Queensland, Australia
INTRODUCTION. Processed Surface EMG signal can be correlated to force output under certain
circumstances. Brand considered that the absolute force generated by muscle is not as important as the relative
balance of forces acting across a joint. Quantifying the forces generated in the antagonist muscles woud be
useful for in-vitro loading studies and in prescribing isometric strengthening in rehabilitation.
METHODS. A custom made jig with a forearm brace and a pulley wheel connected to cables with a strain
gauge attached was used to record load. Surface EMG was recorded over six forearm muscles
(ECRL,ECRB,ECU,APL,FCR,FCU) in16 volunteers (8M/8F) during isometric contraction at wrist angles of -40
to +40 degrees. Recordings were made at 0%,10%,25%,50%,75% and 100% of maximal effort. Data were
processed with custom software written in Labview and plotted in MS Excel.RESULTS. Describe your findings.
Figures/Tables are welcome to fit in a single page. Limit image size so the file is under 5MB.
DISCUSSION. There was a trend for increasing maximum extension force from extension to flexion. In
isometric flexion and extension processed sEMG signal correlated with percentage of maximum effort. APL was
equally active in flexion and extension. The proportional activity of the antagonists does not vary much with
percentage of effort. In maximum isometric flexion and extension the resultant vector of moment arm and
physiologic cross sectional area is in ulnar flexion and radial extension respectively. This places it in the DTM
axis which is the most stable. The minimal variation in the proportion of antagonist activity suggests that
variation in contribution of the antagonist muscles is not a mechanism for stabilizing the wrist under physiologic
loads in isometric loading.
Acknowledgements. Nil
COI. No conflict of interest

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Proprioception of the Wrist Following Distal Radius Fracture-a Protocol for Evaluation and Treatment
Ronit Wollstein MD1,2
, Dafna Michael CHT3, Hani Harel CHT
3
1. University of Pittsburgh Medical School, Pittsburgh, PA
2. Technion University School of Medicine, Haifa, Israel
Introduction:
Proprioception has been used in rehabilitation; most commonly to treat neurological and joint injuries. Our clinical
impression is that in distal radius fracture (DRF) there is a temporary loss of proprioception that should be addressed
following surgical treatment.
We describe a protocol for evaluation of proprioception and a treatment protocol following surgery for DRF. A series of
10 patients undergoing surgery for a comminuted intraarticular fracture of the distal radius was evaluated and treated
using our protocol.
Methods:
Since sensorimotor response loops are complex and it is difficult to isolate the effect of the different types of input, both
the evaluation and the treatment protocols include a comprehensive technique.
The evaluation protocol is performed blinded and includes Semmes- Weinstein evaluation, static and moving 2-point
discrimination, vibration, temperature testing, Moberg pick-up test, as well as specific testing for stereognosis and
proprioception. The treatment protocol incorporates general postoperative treatment modalities for the improvement of
range-of –movement, strength and function as well as specific sensorimotor and proprioceptive treatments.
Results:
The patients demonstrated significant sensorimotor deficits following surgery for DRF. There was documented
improvement with the treatment protocol.
Discussion:
Patients after DRF demonstrate significant sensorimotor deficits, which seem to improve utilizing a comprehensive
sensorimotor treatment protocol. Further study is necessary to provide sensorimotor therapeutic guidelines following
surgery for DRF.
The authors have no conflicts to disclose.
1. Schiftan GS, Ross LA, Hahne AJ. The effectiveness of proprioceptive training in preventing ankle sprains in sporting populations: A systematic
review and meta-analysis. Journal of science and medicine in sport / Sports Medicine Australia 2014. 2. Smith TO, King JJ, Hing CB. The effectiveness
of proprioceptive-based exercise for osteoarthritis of the knee: a systematic review and meta-analysis. Rheumatology international
2012;32(11):3339-51. 3. da Silva KN, Teixeira LE, Imoto AM, et al. Effectiveness of sensorimotor training in patients with rheumatoid arthritis: a
randomized controlled trial. Rheumatology international 2013;33(9):2269-75. 4.Hagert E. Proprioception of the wrist joint: a review of current
concepts and possible implications on the rehabilitation of the wrist. Journal of hand therapy : official journal of the American Society of Hand
Therapists 2010;23(1):2-16; quiz 7. 5. Aimonetti JM, Morin D, Schmied A, et al. Proprioceptive control of wrist extensor motor units in humans:
dependence on handedness. Somatosensory & motor research 1999;16(1):11-29.
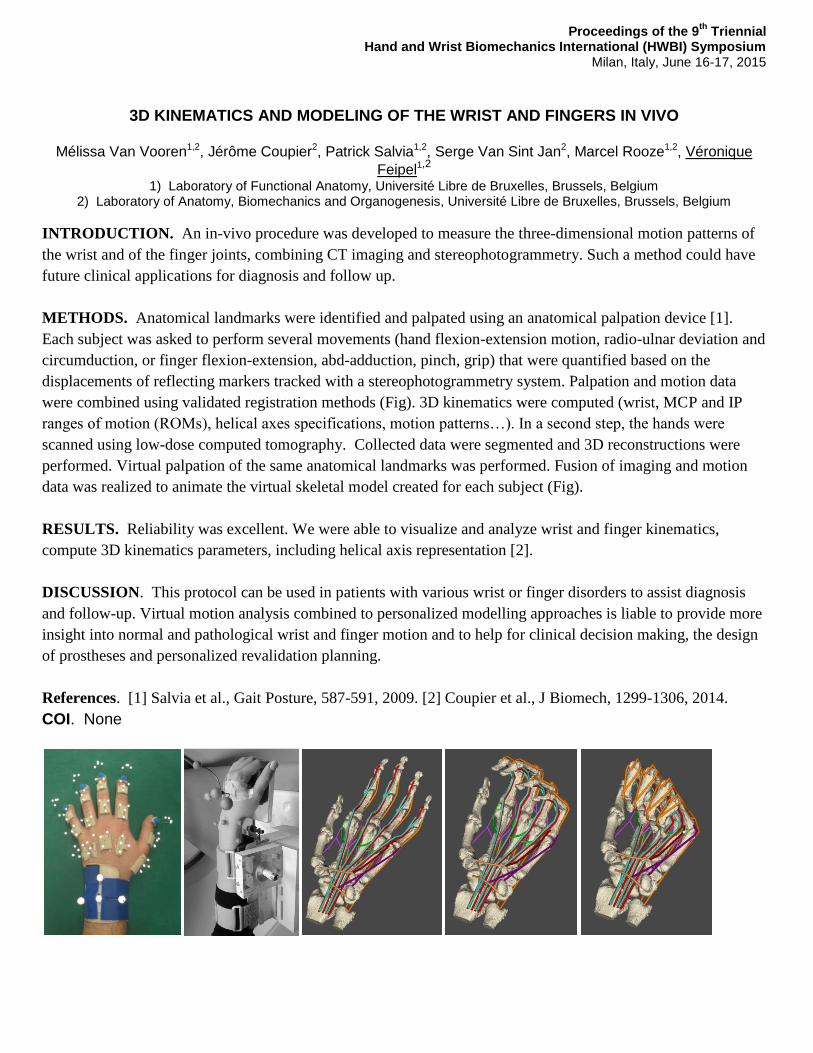
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
3D KINEMATICS AND MODELING OF THE WRIST AND FINGERS IN VIVO
Mélissa Van Vooren1,2, Jérôme Coupier2, Patrick Salvia1,2, Serge Van Sint Jan2, Marcel Rooze1,2, Véronique
Feipel1,2
1) Laboratory of Functional Anatomy, Université Libre de Bruxelles, Brussels, Belgium
2) Laboratory of Anatomy, Biomechanics and Organogenesis, Université Libre de Bruxelles, Brussels, Belgium
INTRODUCTION. An in-vivo procedure was developed to measure the three-dimensional motion patterns of
the wrist and of the finger joints, combining CT imaging and stereophotogrammetry. Such a method could have
future clinical applications for diagnosis and follow up.
METHODS. Anatomical landmarks were identified and palpated using an anatomical palpation device [1].
Each subject was asked to perform several movements (hand flexion-extension motion, radio-ulnar deviation and
circumduction, or finger flexion-extension, abd-adduction, pinch, grip) that were quantified based on the
displacements of reflecting markers tracked with a stereophotogrammetry system. Palpation and motion data
were combined using validated registration methods (Fig). 3D kinematics were computed (wrist, MCP and IP
ranges of motion (ROMs), helical axes specifications, motion patterns…). In a second step, the hands were
scanned using low-dose computed tomography. Collected data were segmented and 3D reconstructions were
performed. Virtual palpation of the same anatomical landmarks was performed. Fusion of imaging and motion
data was realized to animate the virtual skeletal model created for each subject (Fig).
RESULTS. Reliability was excellent. We were able to visualize and analyze wrist and finger kinematics,
compute 3D kinematics parameters, including helical axis representation [2].
DISCUSSION. This protocol can be used in patients with various wrist or finger disorders to assist diagnosis
and follow-up. Virtual motion analysis combined to personalized modelling approaches is liable to provide more
insight into normal and pathological wrist and finger motion and to help for clinical decision making, the design
of prostheses and personalized revalidation planning.
References. [1] Salvia et al., Gait Posture, 587-591, 2009. [2] Coupier et al., J Biomech, 1299-1306, 2014.
COI. None

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
ROLE OF DIGIT FORCE-TO-POSITION MODULATION FOR DEXTEROUS MANIPULATION
Marco Santello
School of Biological and Health Systems Engineering Arizona State University, Tempe, Arizona, U.S.A.
Anticipatory control of movement has been characterized in motor tasks as a way through which the central
nervous system can bypass delays associated with reflex-based control. We have been studying how humans
learn anticipatory control of manipulation tasks to characterize the mechanisms underlying the transformation
from multiple sources of sensory feedback to the coordination of multiple degrees of freedom of the hand. In our
approach, we have removed constraints on digit placement to study how subjects explore and choose relations
between digit forces and positions. The main difference between grasp control at constrained vs. unconstrained
object locations is that anticipatory control of grasping in the former scenario can rely on sensorimotor memories
built through previous manipulations. In contrast, trial-to-trial variability of digit placement associated with
unconstrained grasping limits the extent to which force planning can rely on sensorimotor memories of digit
forces. Consequently, successful execution of manipulation of object grasped at self-chosen contacts likely
requires sensing of digit placement for modulating digit force distribution. I will review our recent work on grasp
planning and execution and underlying neural mechanisms inferred through transcranial magnetic stimulation.
We found that cortical excitability at contact is significantly different when grasping an object at self-chosen vs.
constrained locations. Furthermore, digit force development during unconstrained grasping is characterized by
significantly more feedback-driven corrections than constrained grasping. These results are consistent with the
proposition that grasping at constrained vs. unconstrained object locations is mediated by different sensorimotor
processes.
Acknowledgements. This research was partially supported by a Collaborative Research Grant BCS-
1153034.
COI. None

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Precision Pinch Performance in the Hands of Patients following Nerve Repair
Hsiu-Yun Hsu1, Li-Chieh Kuo2, Ta-Shen Kuan1, Fong-Chin Su3, Haw-Yen Chiu4
1) Department of Physical Medicine and Rehabilitation, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, TAIWAN
2) Department of Occupational Therapy, National Cheng Kung University, Tainan, TAIWAN 3) Department of Biomedical Engineering, National Cheng Kung University, Tainan, TAIWAN
4) Section of Plastic Surgery, Department of Surgery, Chi-Mei Medical Center, Tainan, TAIWAN
INTRODUCTION. An injury to a nerve can result in the problems of muscle and sensory function. However,
the impact of nerve injury on precision pinch performance in the hands has seldom been discussed. The objective
of this cohort study was to explore the impact of nerve injury and regeneration on the precision pinch
performance of the hand.
METHODS. The PHUA [1], moving and static two-point discrimination (M2PD and S2PD), Semmes-
Weinstein monofilament (SWM) tests and maximum pinch strength were conducted at monthly intervals
following nerve repair for eighteen patients (9 males and 9 females with the mean age of 33.0±12.0 years old)
with digital or median nerve repairs. In addition, eighteen age- and gender-matched healthy subjects were
recruited as controls. Peak force ratio (FRPeak, the maximum pinch force during the lifting
performance/maximum load force at the onset of maximum upward acceleration) for the PHUA test were used to
determine the improvements in precision pinch performance with time following nerve regeneration. The Mann–
Whitney U test was used to examine the difference in the measuring outcomes between the nerve injury patients
and healthy control; The Wilcoxon signed-rank test examined the difference of the results between two different
assessing time-points for the patients.
RESULTS. The patients with nerve injuries showed deteriorations in pinch strength, sensibility and precision
pinch performance (force adjustment) in the PHUA test (p<0.001) in comparison with the healthy controls.
Following the nerve regeneration, there were significant changes in hand sensibility and precision pinch
performance (Table 1).
Table 1: Sensibility, strength and sensorimotor control at varying times during nerve regeneration (n 18)
SWM Mean (SD)
M2PD Mean (SD)
S2PD Mean (SD)
Pinch strength (N) Mean (SD)
FRPeak
Mean (SD)
Percentage of maximal pinch strength (%) Mean (SD)
1st
Evaluation 4.25
(.48)
16.1
(8.6)
17.5
(8.2)
33.99 (17.35) 3.07 (.38) 49.36 (20.32)
2nd
Evaluation 3.89
(.40)
13.8
(7.7)
15.3
(8.1)
34.96 (13.46) 2.75 (.22) 39.75 (13.90)
p-value .001* .036* .040* .586 .002* .010*
DISCUSSION. This study found that nerve injury can result in precision pinch performance deficits. In
addition, following nerve regeneration, improved sensory functioning can help restore precision pinch
performance. Therefore, the parameters detected form the PHUA test can assist clinicians in their assessment of
nerve injury and determining the specific functional deficits of the hand.
References. [1] Chiu, H. Y.(et al.), J Orthop Res,1116-1121,2009.
COI. No relevant potential conflict of interests.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Importance of grasp types for personal autonomy during activities of daily living (ADL)
V. Gracia-Ibáñez, M. Vergara, J.L. Sancho-Bru Dpto. de Ingeniería Mecánica y Construcción. Universitat Jaume I, Castellón, ESPAÑA
INTRODUCTION. The World Health Organization established the International Classification of Functioning, Disability and Health
(ICF) as a framework for measuring health and disability, which classifies the ADL in 9 chapters, subdivided into groups of activities.
The function of the hand has been profusely studied in biomechanics, hand surgery or rehabilitation; however, the importance of each
type of grasp for personal autonomy when performing ADL has not been assessed yet.
METHODS. A field study of grasps used in ADL was conducted, based on the observation of videos of real tasks. The study was
focused on three ICF chapters (4 to 6), as more than 80% of their ADL involve the hand directly. Sixty-four videos, representative of
these ADL, were registered. The time using different grasp types was recorded, and a 9-type grasp taxonomy [1] was considered (Fig.
1): Cylindrical (Cyl), Oblique palmar (Obl), Hook (Hook), Lumbrical (Lum), Intermediate power-precision (IntPP), Pinch (Pinch),
Lateral Pinch (LatP), Special pinch (SpP) and Non-prehensile grasp (NonP). In order to calculate the importance of the grasp types for
personal autonomy during ADL, two weightings of the time recorded were performed. One weighting equaled the total time recorded
of each ICF group of activities, and another one accounted for the relative importance of each activity in personal autonomy by using
two scales [2]: 'Scale 1' comes from common assessment scales of disability, and 'Scale 2' from sociological surveys about dependence.
RESULTS. Table 1 shows the importance of each grasp for the chapters 4 to 6 of the ICF.
Table 1. Importance of grasps for personal autonomy, measured with both scales.
Chapter Cyl
(%)
SpP
(%)
Hook
(%)
intPP
(%)
LatP
(%)
Lum
(%)
nonP
(%)
Obl
(%)
Pinch
(%)
4. Mobility Scale 1 14.6 0.9 11.4 0.04 8.6 12.8 23.3 4.8 23.6
Scale 2 9.2 0.5 6.7 0.05 5.2 7.5 50.0 6.9 13.9
5. Self care Scale 1 9.3 4.1 4.3 5.5 10.7 2.8 17.1 9.9 36.2
Scale 2 8.9 4.0 5.7 4.7 12.5 2.7 19.4 10.6 31.7
6. Domestic life Scale 1 15.0 0.5 3.1 3.0 8.8 16.3 8.3 9.3 35.6
Scale 2 14.8 0.6 2.8 3.1 8.8 15.9 8.3 9.5 36.3
DISCUSSION. Knowledge of the importance of each grasp type for the autonomy in ADL is critical for the fields of
rehabilitation or hand prosthesis design. Results show that Pinch is the most important grasp for autonomy within the ICF
chapters studied, followed by NonP and Cyl, so that rehabilitation processes or hand prosthesis design should be based on
them. Furthermore, these results should be addressed also to achieve a more fairly method to assess disability. Although
the same activities have been analyzed, the two weighted scales provide different results, especially in Chapter 4
(Mobility). This highlights the need of improving the scales for rating the activities, in order to get more consistent
assessments of disability.
Acknowledgements. We are grateful to the Universitat Jaume I for funding through the project P1- 1B2014-10.
References. [1] Vergara M. (et al.), Journal of Hand Therapy 27 (2014) 225-234
[2] Querejeta-González M., IMSERSO, 2004, http://www.index-f.com/lascasas/documentos/lc0181.pdf
COI. Authors declare that there are no conflict of interests.
Figure 1. Types of grasps
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Reach-to-Grasp Movement under Different Sensory Conditions in Children with Developmental
Coordination Disorder: A Pilot Study
Hsiu-Ching Yang1, Li-Chieh Kuo 2, Ta-Shen Kuan 1, Hsiu-Yun Hsu 1 1) Department of Physical Medicine and Rehabilitation, National Cheng Kung University Hospital, Tainan, Taiwan
2) Department of Occupational Therapy, National Cheng Kung University, Tainan, Taiwan
INTRODUCTION. Motor coordination impairment is a main characteristic of developmental coordination
disorder (DCD). But many studies suggested that children with DCD seem to have sensory processing problems,
especially recent researchers indicate the postural control was affected by visual, somatosensory, or both more in
children with DCD than normal controls. Furthermore, the hand skills associate with our daily life, the reach-to-
grasp movement is a foundation of various hand skills. However, few studies have investigated how sensory
contributed to reach-to-grasp movement in children with DCD. Therefore, the purpose in this pilot study was to
examine the reach-to-grasp movement under altered sensory conditions of children with DCD.
METHODS. Five children with DCD (3 males, 2 females, mean age = 7.07 years) and 5 children with typical
development (TD; 3 males, 2 females, mean age = 7.13 years) enrolled in the present study. MiniBird system
(Ascension Technology Corporation, Burlington, VT, USA) was used to record the kinematic data of the reach-
to-grasp trials in two size targets (large, L / small, S), under different visual (normal visual, V / non-visual, N)
and tactile (normal tactile, T / modified tactile, M) conditions.
RESULTS. DCD group didn’t show different from TD group in age, arm length, finger spam, sensitivity of
touch in thumb and index finger tips. For kinematic variables of reach-to-grasp movement, DCD group appeared
significantly longer MT (movement time) in TVL and TNL conditions; larger NJS (normalized jerk score) in
TVL, TVS, MVL, MVS, and MNL conditions; more MU (movement unit) in TVL, TVS, and TNS conditions;
and smaller NMGA (normalized maximal grip aperture) in MNL and MNS conditions than TD group.
DISCUSSION. In present study, DCD group seemed longer MT than TD group, the result was similar to Zoia et
al. (2005), but it seemed to be more significant in non-visual conditions. For NJS, which derived from the three
order differentiation of position to represents the smoothness of movement trajectory, DCD group seemed larger
than TD group, and more significant in MNL condition. For MU, larger MU means the larger number of
correctional times and poorer motor coordination, and more significant in TNS and MNL conditions. However,
DCD showed smaller NMGA than TD in MNL and MNS conditions. In summary, DCD group have a trend of
longer executive time, poor motor smoothness in normal tactile and normal visual conditions, but while sensory
inputs (tactile and vision) was insufficient, it appeared that more threatened to their motor smoothness, and they
seemed to not use the strategy of larger grip aperture as TD group. However, we still needed larger sample size
to support such significant findings.
COI. No relevant potential conflict of interests.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Range of motion of the wrist while driving a car
Sebastian V. Gehrmann1, Sabrina Pfau1, Joachim Schaedle2, Georg Jansing2, Joachim Windolf1
1) Department of Trauma and Hand Surgery, University Clinic Duesseldorf, Germany 2) Department of Applied Mathematics, University of Duesseldorf, Germany
INTRODUCTION. "Doctor, when can I drive?". Activities of daily living often require a wide range of motion at
the wrist, especially when driving a car. Motion impairment in wrist disorders often lead to uncertainty in
patients. So far, little is known about the needed amount of motion of the wrist when driving a car. The aim of
the study was to investigate the range of motion of the wrist in healthy volunteers when driving. The hypothesis
was, that the maximal range of motion capacity of the wrist is not fully exploited during a test drive.
METHODS. Nineteen healthy male right-handed subjects performed a test drive. Patients were seated in a
medium-sized vehicle with manual gear change and were asked to drive a predetermined serpentine track.
Motion of the right wrist was continuously captured by an elecrogoniometric motion analysis system
(Biometrics). To determine maximum motion boundaries of the wrist, subjects were asked to perform maximal
circumduction of the wrist. Further analyses were conducted with a custom-made MATLAB program.
Flexion/Extension and Radial-/Ulnarabduction were recorded. Motion areas were calculated as well as a heat
map to demonstrate the spatial distribution.
RESULTS. The graphical analysis of the heat maps revealed zones of high activity, where the wrists were
found to be placed more often. Three main motion directions were identified with a steady semicircular motion
for steering and two periodical evasive movements. The envelope area covered by the wrist during the test
drive (8835 ± 2086 Grad²) was smaller than the area for maximum motion capacity (12869 ± 3368 degree², p <
0,01). The maximal Extension was 59 ± 44°, Flexion bei 48 ± 17°, Radial Abduktion 18 ± 15° and Ulnar
Abduktion bei 46 ± 11°.
DISCUSSION. The study is a first attempt to quantify wrist motion during driving a car. Although the area
covered by the envelope is significantly smaller during the test drive than the circumduction, maximum wrist
motion is still high. Evaluation of wrist motion is important prior to driving a car.
Acknowledgements. Funds received by Arthrose e.V.
COI. There is no relevant potential conflict of interests to declare.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
BIOMECHANICAL ASPECTS OF TRIGGER FINGER
Fong-Chin Su Department of Biomedical Engineering, National Cheng Kung University, Tainan, Taiwan
Although trigger finger is relatively common hand disorder, its etiology is not ruled out. We investigated
the biomechanical changes after different extent of pulley release in human fingers. Kinematic and kinetic
performance of trigger fingers has been evaluated in vivo. The extensor tendon force is needed to overcome the
catching flexors in trigger fingers. In order to quantify catch-and-release, a biomechanical model was developed
to quantitatively estimate the flexor/extensor tendon force at triggering in trigger fingers. It can used for
quantitative classification of trigger digits in clinical examination. Also, subjective and objective hand function
evaluations were performed before and after surgery. The effect of different extent of pulley release on the
function of trigger digit was investigated. No significant difference was found between A1 and Half A2. The
pulley release for trigger finger treatment may extend to the half proximal A2 pulley. In addition, postoperative
rehabilitation protocol for trigger finger is another issue. A proposed sequential movements from straight finger,
intrinsic plus, straight fist, fist, hook, and then back to original straight finger were used for rehabilitation in
patients. Results demonstrated that the rehabilitation group had better recovery than the controls. Finally, to
understand the limited hand functions, the force coordination applied by individual fingers during the functional
precision grasping between patients with trigger digits was also examined. Biomechanical investigations of
trigger finger improve the understanding of trigger finger, provide suggestions for clinical practice, and develop
better assessment and treatment programs.
Acknowledgements. Supported by National Health Research Institutes grant NHRI-EX102-10040EI and
Ministry of Science and Technology grant 100-2627-B-006-008, Taiwan.
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
A Review of Innovative Evaluation of Dexterity
Francisco J. Valero-Cuevas 1, Susan V. Duff 2, Dorit H. Aaron3, Gloria R. Gogola 4
1) Biomedical Engineering, and Biokinesiology & Physical Therapy, University of Southern California, Los Angeles, CA, USA 2) Physical Therapy, Thomas Jefferson University, Philadelphia, PA, USA
3) Aaron & Winthrop Hand Therapy Services, Inc, Houston, TX, USA 4) Shriners Hospitals for Children, Houston, TX, USA
INTRODUCTION. Hand dexterity is multifaceted and essential to the performance of daily tasks. Timed
performance and precision demands are the most common features of quantitative dexterity testing.
Measurement concepts such as rate of completion, in-hand manipulation and dynamic force control of
instabilities are being integrated into assessment tools for the pediatric population.
METHODS. To present the fundamental concepts behind the Strength-Dexterity Test, and provide an overview
of the clinical results to date. In particular, we review measurement concepts inherent in pediatric dexterity
testing and introduce concepts that are infrequently measured, or novel, as exemplified with two assessment
tools [1].
RESULTS. The Functional Dexterity Test (FDT) and the Strength-Dexterity (SD) Test show promise as means
to quantify important features of in-hand manipulation. In-hand manipulation depends critically on the ability to
dynamically regulate and orchestrate fingertip forces and finger motions. Whole-arm tasks, or purely sensory or
strength measurements, do not capture these complex sensorimotor interactions.
DISCUSSION. When placed in context of prior work on fMRI and physiological recordings in various
populations, these metrics open new dimensions of quantifiable function in the clinic [2-4]. They also challenge
the cortico-centric view of neuromuscular control of the hand for dexterous manipulation [3].
Acknowledgements. NIH Award Numbers AR050520 and AR052345 to FVC. SVD was supported by NICHD
T32 award HD064578.
References. [1] Duff (et al.), Innovative evaluation of dexterity in pediatrics, Invited Review, Journal of Hand
Therapy, Accepted, 2015. [2] Lightdale-Miric (et al.) Quantitative Assessment of Dynamic Control of Fingertip
Forces After Pollicization, Best Paper Award – GCMAS, Gait & Posture, 41:1, p. 1-6, 2014. [3] Lawrence (et al.)
Quantification of dexterity as the dynamical regulation of instabilities: comparisons across gender, age, and
disease. Invited Paper. Frontiers in Neurology - Movement Disorders, 5:53, 2014. [4] Dayanidhi (et al.)
Decrease in muscle contraction time complements neural maturation in the development of dynamic
manipulation. Journal of Neuroscience, 33(38): p. 15050-55, 2013.
COI. FVC holds US Patent No. 6,537,075 on some of the technology used, but has no active or pending
licensing agreements with any commercial entity.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Is the minimization of secondary moment during finger pressing task related to muscle force
economy?
Jérémy Rossi1, Benjamin Goislard de Monsabert2, Eric Berton2, Laurent Vigouroux2 1) Laboratoire de Physiologie de l’Exercice (EA 4338), Université Savoie Mont Blanc, Le Bourget du Lac, France
2) Aix-Marseille Université, CNRS, ISM UMR 7287, 13288, Marseille, France
INTRODUCTION. When applying a force with the index, middle, ring and little fingers simultaneously, the
central nervous system (CNS) has to deal with a redundancy problem since, for a given resultant force level, the
number of possible force sharing between fingers is infinite [1]. Surprisingly, numerous studies observed that
this finger force sharing seems relatively stable across subjects [2,3]. Li et al. [2] suggested that the adopted
sharing might aim to minimize secondary moments along the pronation/supination wrist axis. Such behavior
would in fact allow the CNS to minimize the muscular effort required for the task [4]. Although this principle of
secondary moment minimization has been extensively studied and demonstrated [5], no study has yet proved the
relationship between this motor control behavior and the effective minimization of muscle forces. The aim of the
present study was to test this hypothesis in a simulation context by using a hand biomechanical model.
METHODS. A hand biomechanical model consisting of 23 degrees of freedom mobilized by 42 muscles was
used to estimate the resultant four-finger force and the finger force sharing. Kinematic data were taken from
Vigouroux et al. [3]. Several multi-objective optimization processes were used to determine the forces exerted by
each finger during a maximal finger pressing task and corresponded to different combinations of the following
criterions: maximization of the resultant four-finger force (a), minimization of muscle stresses (b) and
minimization of the secondary moment (b). The weights associated to the criterions were determined through a
Monte Carlo method and were chosen to reduce the differences between experimental data [3] and simulated
finger forces. The obtained results and the residuals were compared between the different optimization functions.
RESULTS and DISCUSSION. The table below present the typical results obtained with a multi-objective
function which only combines the a and b criterions and show that the hand biomechanical model can estimate a
resultant force and a finger force sharing that are very similar to the experimental measurements. Our
preliminary results show that using a criterion, which includes the muscle stress minimization, may be
worthwhile only if they distinguish the functions of the muscles around the joints involved in the secondary
moments.
Resultant
four-finger force (N)
Finger force (%)
Index Middle Ring Little
Simulation 65.7 37.9 33.1 20.0 9.0
Experiment [3] 65 ± 15 32.8 ± 4.7 32.2 ± 3.3 21.6 ± 2.8 13.4 ± 4.1
REFERENCES. [1] Bernstein, Archive Biology Sciences, 1-35, 1935. [2] Li et al., Exp Brain Res, 276-286,
1998. [3] Vigouroux et al. Hum Moc Sci, 396-407, 2008. [4] Prilutsky et al. Exerc Sport Sci Rev, 32-38, 2002. [5]
Zatsiorsky et al. Biol Cybern, 40-49, 2002.
COI. There is no current or potential conflict of interest concerning this study.
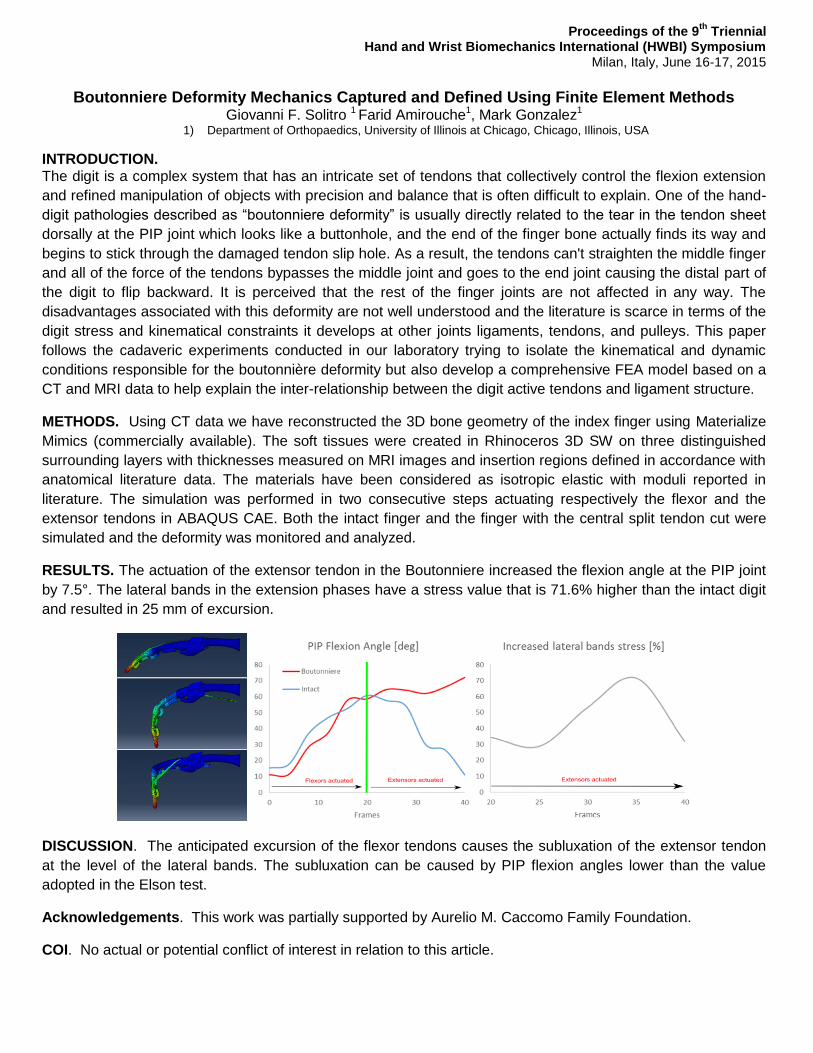
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Boutonniere Deformity Mechanics Captured and Defined Using Finite Element Methods
Giovanni F. Solitro 1 Farid Amirouche1, Mark Gonzalez1 1) Department of Orthopaedics, University of Illinois at Chicago, Chicago, Illinois, USA
INTRODUCTION. The digit is a complex system that has an intricate set of tendons that collectively control the flexion extension
and refined manipulation of objects with precision and balance that is often difficult to explain. One of the hand-
digit pathologies described as “boutonniere deformity” is usually directly related to the tear in the tendon sheet
dorsally at the PIP joint which looks like a buttonhole, and the end of the finger bone actually finds its way and
begins to stick through the damaged tendon slip hole. As a result, the tendons can't straighten the middle finger
and all of the force of the tendons bypasses the middle joint and goes to the end joint causing the distal part of
the digit to flip backward. It is perceived that the rest of the finger joints are not affected in any way. The
disadvantages associated with this deformity are not well understood and the literature is scarce in terms of the
digit stress and kinematical constraints it develops at other joints ligaments, tendons, and pulleys. This paper
follows the cadaveric experiments conducted in our laboratory trying to isolate the kinematical and dynamic
conditions responsible for the boutonnière deformity but also develop a comprehensive FEA model based on a
CT and MRI data to help explain the inter-relationship between the digit active tendons and ligament structure.
METHODS. Using CT data we have reconstructed the 3D bone geometry of the index finger using Materialize
Mimics (commercially available). The soft tissues were created in Rhinoceros 3D SW on three distinguished
surrounding layers with thicknesses measured on MRI images and insertion regions defined in accordance with
anatomical literature data. The materials have been considered as isotropic elastic with moduli reported in
literature. The simulation was performed in two consecutive steps actuating respectively the flexor and the
extensor tendons in ABAQUS CAE. Both the intact finger and the finger with the central split tendon cut were
simulated and the deformity was monitored and analyzed.
RESULTS. The actuation of the extensor tendon in the Boutonniere increased the flexion angle at the PIP joint
by 7.5°. The lateral bands in the extension phases have a stress value that is 71.6% higher than the intact digit
and resulted in 25 mm of excursion.
DISCUSSION. The anticipated excursion of the flexor tendons causes the subluxation of the extensor tendon
at the level of the lateral bands. The subluxation can be caused by PIP flexion angles lower than the value
adopted in the Elson test.
Acknowledgements. This work was partially supported by Aurelio M. Caccomo Family Foundation.
COI. No actual or potential conflict of interest in relation to this article.
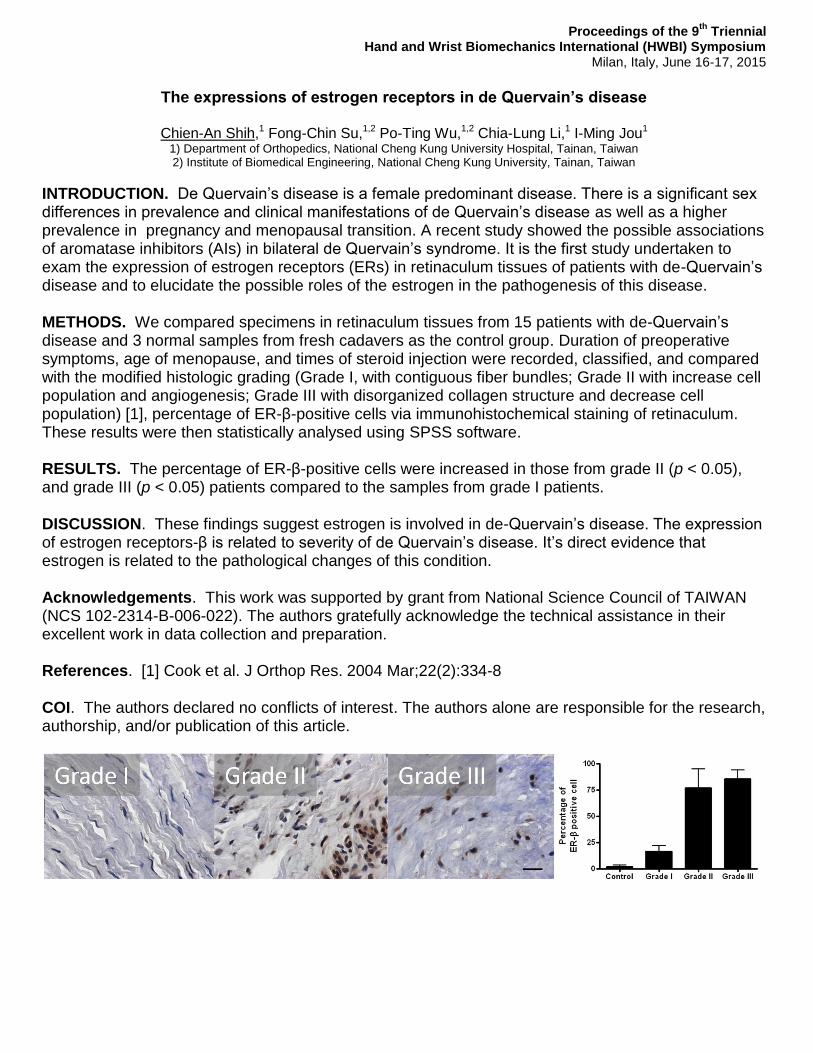
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
The expressions of estrogen receptors in de Quervain’s disease
Chien-An Shih,1 Fong-Chin Su,1,2 Po-Ting Wu,1,2 Chia-Lung Li,1 I-Ming Jou1
1) Department of Orthopedics, National Cheng Kung University Hospital, Tainan, Taiwan 2) Institute of Biomedical Engineering, National Cheng Kung University, Tainan, Taiwan
INTRODUCTION. De Quervain’s disease is a female predominant disease. There is a significant sex differences in prevalence and clinical manifestations of de Quervain’s disease as well as a higher prevalence in pregnancy and menopausal transition. A recent study showed the possible associations of aromatase inhibitors (AIs) in bilateral de Quervain’s syndrome. It is the first study undertaken to exam the expression of estrogen receptors (ERs) in retinaculum tissues of patients with de-Quervain’s disease and to elucidate the possible roles of the estrogen in the pathogenesis of this disease. METHODS. We compared specimens in retinaculum tissues from 15 patients with de-Quervain’s disease and 3 normal samples from fresh cadavers as the control group. Duration of preoperative symptoms, age of menopause, and times of steroid injection were recorded, classified, and compared with the modified histologic grading (Grade I, with contiguous fiber bundles; Grade II with increase cell population and angiogenesis; Grade III with disorganized collagen structure and decrease cell population) [1], percentage of ER-β-positive cells via immunohistochemical staining of retinaculum. These results were then statistically analysed using SPSS software. RESULTS. The percentage of ER-β-positive cells were increased in those from grade II (p < 0.05), and grade III (p < 0.05) patients compared to the samples from grade I patients. DISCUSSION. These findings suggest estrogen is involved in de-Quervain’s disease. The expression of estrogen receptors-β is related to severity of de Quervain’s disease. It’s direct evidence that estrogen is related to the pathological changes of this condition. Acknowledgements. This work was supported by grant from National Science Council of TAIWAN (NCS 102-2314-B-006-022). The authors gratefully acknowledge the technical assistance in their excellent work in data collection and preparation. References. [1] Cook et al. J Orthop Res. 2004 Mar;22(2):334-8 COI. The authors declared no conflicts of interest. The authors alone are responsible for the research, authorship, and/or publication of this article.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Evaluation of Forces During Two Different Pushup Styles,
Olga Polovinets BSc1, Alon Wolf PhD
1, Ronit Wollstein MD
2,3
1. Department of Mechanical Engineering, Technion Institute, Haifa, Israel
2. Technion University Medical School, Haifa, Israel
Introduction:
Pushups performed on a hyperextended wrist are ubiquitously used in sports, fitness and the military. Our impression is
that pushups on a hyperextended wrist are harder to perform when there is any type of injury to the wrist. The purpose
of this study was to compare the forces in the wrist during pushups on a hyperextended wrist (military style pushups) and
during pushups performed on a straight wrist (knuckle pushups).
We hypothesize that knuckle pushups differ from pushups on a hyperextended wrist in force distribution.
Methods:
Fourteen healthy right-handed male volunteers with strict physical parameters were recruited to perform pushups in 2
different patterns: on a straight wrist (knuckle pushups) and on a hyperextended wrist (military style pushups). For each
pattern the subjects performed two sets of 10 pushups in random order. The pushups were performed in a gait analysis
lab using 13 sensors for each upper extremity. We used the Vicon motion capture system to follow the kinematics and
two AMTI force plates. The subjects had 2 seconds to do down and 2 seconds to go up in each pushup. The force vectors
were computed using Matlab software. We evaluated the uniformity of the forces passing through the capitate, the
horizontal distance between the capitate and point of applied force, and the total angle distribution for the force vector.
The position of the capitate was determined by ultrasound and one of the sensors was applied to the skin over the point
in the middle of the capitate. The components of the vectors were compared using Norm 2 (showing normalized vector
components).
Results:
In both methods, the force was not uniform throughout the pushup experience. In knuckle pushups, the force vector was significantly more uniform throughout the pushup in the vertical direction when compared to the military style pushups (in both hands). The horizontal distance between the capitate bone location and force origin was smaller in the hyperextended wrist position. Discussion:
The forces through the wrist are distributed differently during the different types of pushup. Further study is necessary to delineate the differences between both types of pushups especially in regards to the anatomical location of force transmission and the amount of load being transmitted.
The authors have no conflicts to disclose
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
The Puzzle of the Thumb - Mobility, Stability, and Demands in Opposition
Amy L. Ladd MD
Background
The paradoxical demands of stability and mobility reflect the purpose and function of the human thumb.
Absence, injury, and degeneration underscore its functional importance. Prevailing literature and teaching
implicate the thumb carpometacarpal’s unique shape, as well as its ligament support, applied forces, and
repetitive motion, as culprits causing common osteoarthritis (OA). Sex, ethnicity, and occupation may influence
its presence.
Questions/purposes
What is the current, measurable evidence linking ligament structure, forces, and motion to progressive
carpometacarpal (CMC) disease? Specifically: 1) Do unique attributes of the bony and ligamentous anatomy
contribute to OA? 2) Can discrete joint load patterns be established that contribute to OA? And, finally, 3) Can
thumb motion at the fine and gross level be measured that characterizes OA?
Methods
This manuscript addresses the morphology, load, and movement of the human thumb emphasizing the CMC
joint in normal and arthritic states. We present comparative anatomy, gross dissections, microscopic analysis,
multimodal imaging, and live subject kinematic studies to support or challenge the current understanding of the
thumb CMC joint and its predisposition to disease.
Results
The current evidence suggests structural differences and loading characteristics predispose the thumb CMC to
joint degeneration, especially related to volar or central wear. The patterns of degeneration, however, are not
consistently identified, suggesting influences beyond inherent anatomy, repetitive load, and abnormal motion.
Conclusions
Additional studies to define patterns of normal use and wear will provide data to better characterize CMC OA,
and opportunities for tailored treatment: including prevention, delay of progression, and joint replacement.
Key words: Thumb carpometacarpal, osteoarthritis, morphology, loading, kinematics
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
in vivo analysis of joint function using dynamic CT
Faes D. Kerkhof1, Eddy Brugman2, Filip Stockmans1, 2, Ilse Jonkers3, Evie E. Vereecke1
1) Department of Development and Regeneration @ Kulak, KU Leuven, Kortrijk, Belgium 2) AZ Groeninge, Kortrijk, Belgium 3) Department of Kinesiology, KU Leuven, Leuven, Belgium
INTRODUCTION. Previous research has shown that dynamic CT can be used to directly quantify movements
of individual (meta)carpal bones. This technique enables accurate investigation of 3D kinematics in functional
tasks, making it a promising method to explore joint (dys)function. The aim of this study is to further validate the
use of dynamic CT for the quantification of bone kinematics and to demonstrate the potential of dynamic CT in
the investigation of pathological joint functioning.
METHODS Six cadaveric human forearms were placed in a motion simulator controlling thumb opposition. A
dynamic CT scan was acquired during full thumb opposition using a 64 slice CT scanner. For validation
purposes, a calibration cube with eight silicon-nitride beads was placed on the lateral side of the first metacarpal
(MC1) during each acquisition. In one specimen, silicon-nitride beads were inserted inside the MC1 base to test
the use of rigid body dynamics to calculate arthrokinematics. Distances between pairs of beads were compared
between frames, as well as to the known machined distances. Image segmentation was semi-automated using
an algorithm developed by Materialise®. Bone motion was quantified using helical axes and their inclination
angles with an anatomically defined plane using Matlab.
In a case study of pathological joint function, dynamic CT scans of a 41-year-old male with pain at the basal
thumb joint were made during active abduction-adduction, flexion-extension and opposition-reposition of the
thumb. Image acquisition, segmentation and kinematic analysis were done using the same protocol as in the
cadaveric study. In addition, changes in contact patterns between the articular facets during the motion cycle
were mapped.
RESULTS. Inter-centroid distances of the calibration beads deviated on average 0.23 mm (+/- 0.02 mm) from
the known machined distances. Differences between frames were <0.2 mm. During passive thumb opposition,
there is motion at both the trapeziometacarpal and trapezioscaphoid joints. However, joint motion patterns,
defined as changes in inclination angles during opposition, differ between specimens. In the clinical case, dorsal
luxation of MC1 could be clearly seen and quantified during the full range of motion. Furthermore, we were able
to quantify the change in articular contact area over time for each active motion.
DISCUSSION. Dynamic CT allows to quantify thumb arthrokinematics with submillimeter accuracy making it a
valuable tool for in vivo analysis and quantification of native and pathological joint function. Using a larger
sample size, including both healthy volunteers and symptomatic patients, will improve our understanding of joint
(dys)functioning and eventually lead to better prevention and treatment strategies for osteoarthritis of the thumb.
Acknowledgements. Funding for this study was obtained from the Materialise-Kulak Chair for Hand Surgery.
COI. None.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
BIOMECHANICAL ANALYSIS OF THE THUMB CARPOMETACARPAL JOINT LIGAMENTS
Mireia Esplugas (1), Alex Lluch (2), Marc Garcia-Elias (2), Nathalie Mobargha (3), Elisabeth Hagert (3).
1) Activamutua , Tarragona, Spain.
2) Institut Kaplan, Barcelona, Spain.
3) Karolinska Institutet, Stockholm, Sweden.
INTRODUCTION. The thumb carpometacarpal joint (CMC1joint) has seven major ligaments: three dorsal, two volar and two ulnar. It has been
shown that there are considerable anatomical, histological, histomorphometric and sensory differences between them. These observations have
lead to support the theory that dorsal ligaments are the primary CMC1 stabilizers. Nevertheless, this has not been fully proven. To further
define their stabilizing role, we serially sectioned the three groups of ligaments in eleven fresh human cadaver specimens, and assessed the effects
of each individual sectioning in the spatial position of the base of the first metacarpal bone (baseMTC1).
METHODS. Eleven fresh frozen human cadaver specimens, without signs of CMC1joint osteoarthritis, were dissected. The 4 extrinsic and 5
intrinsic muscles acting on the CMC1joint (abductor pollicis brevis, flexor pollicis brevis, opponens pollicis, flexor pollicis longus, adductor pollicis,
abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus and first dorsal interosseous muscles) were identified and their distal
tendon isolated. The 3 groups of CMC1joint ligaments were dissected. The DORSAL group included the dorsal radial, the dorsal central, and the
posterior oblique ligaments. The VOLAR group included the anterior oblique and ulnar collateral ligaments; and the ULNAR group included the dorsal
and the intermetacarpal ligaments. The specimens were attached to a specially designed testing jig with the CMC1joint in neutral
abduction/flexion/opposition position. Strings were attached to the proximal ends of the tendons and weights proportional to each muscle
physiologic cross-sectional area were used to load the joint. A Fastrak® motion tracking device was used to study the effects of randomly
sectioning each ligament group in the spatial position of one sensor inserted into the baseMTC1. Statistical analyses of the translation in
millimeters was performed using One-way ANOVA and a paired t-Test.The results were considered statistically significant at p<0,05.
RESULTS After VOLAR ligaments section, the baseMTC1 moved dorsally in all cases (0,150mm; SD: 0,072; range: 0,050-0,220). After
ULNAR ligaments transaction, the baseMTC1 moved dorsally in 3 cases (0,064; SD: 0,301). After DORSAL ligaments cutting, the baseMTC1
moved dorsally (0,523mm; SD: 0,0512). A trend towards statistical significance (p=0,095) was found when comparing the translation along
the X axis, (dorsopalmar translation) after ligament sectioning, but not along the Y,Z axis.
DISCUSSION. When all muscles are loaded, and the thumb (without CMC1 osteoarthritis) is in neutral position, the baseMTC1 moves always
dorsally regardless what ligament has been cut. The dorsal group, however, is the one that induces the most important translation. Based on
these findings, we suggest that: (1) the so-called dorsal deltoid ligament (dorsal group) is the most important CMC1joint stabilizer, as it has also
been suggested by other investigators; (2) the dorsal deltoid ligament is the primary restraint to CMC1joint dorsoradial subluxation; and (3)
CMC1joint stability is provided by the additive and synergistic effects of the different groups of ligaments analyzed in the present study. This
study could have 2 clinical applications: 1) CMC1 joint stabilizing procedures should specifically reconstruct the dorsal deltoid ligaments. (2)
arthroscopical capsular shrinkage should be performed through a volar portal.
ACKNOWLEDGEMENTS: The experiments have been performed at the Biomechanical Laboratory of the Anatomy Department at the Barcelona University. We thank Dr Manel
Llusà for his help. The statistics analysis has been conducted by Dr. Angel Vila Corcoles. We thank him for his help.
COI: No potential conflict of interests.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Interrater and Intrarater Reliability of the Radiographic Thumb Osteoarthritis Index
Thomas J. McQuillan1, Tarpit Patel2, Deborah Kenney1, Amy L. Ladd1, Arnold-Peter C. Weiss2
Joseph J. Crisco2
1) Robert A. Chase Hand and Upper Limb Center, Department of Orthopedics, Stanford University Medical Center, Stanford, CA, USA 2) Department of Orthopedics, Warren Alpert Medical School, Brown University, Providence, RI, USA
INTRODUCTION. The thumb osteoarthritis (ThOA) index provides a clinically relevant measurement for
quantifying the severity of thumb carpometacarpal (CMC) osteoarthritis (OA) [1]. Using a single Robert’s view of
the wrist, the ThOA is calculated by measuring the trapezial height-to-width ratio. This provides a measurable,
quantifiable alternative to Eaton staging [2], and is associated with articular wear in surgically excised
trapeziums. The purpose of this study was to evaluate the interrater and intrarater reliability of the ThOA index
in early OA patients.
METHODS. Ten Robert’s view radiographs of the CMC joint were selected from a pool of subjects with
symptomatic early OA [3]. Measurements of the width and height of the trapezium were calculated using the
open-source software ImageJ (NIH, http://rsb.info.nih.gov/ij), and the height-to-width calculation was stored
using a macro that we developed for the program. Three users analyzed the ten x-rays on seven different
occasions over a two-week period, with a minimum of 24 hours between re-analyzing the series of x-rays.
Intrarater reliability was calculated for each user over the period, and interrater reliability was assessed by
comparing the initial ThOA measurements for each user. Data were analyzed in StataMP 13.1 (College Station,
Texas, USA) and reliability for each user was assessed using the intraclass correlation coefficient (ICC).
RESULTS. Intrarater reliability was very high. User #3 had the highest ICC of 0.97 (95% CI 0.93-0.99), while
User #1 had the lowest with 0.94 (95% CI 0.88-0.98). Interrater reliability was also high, with an ICC of 0.84
(95% CI 0.55-0.96).
DISCUSSION. The ThOA index demonstrates high intrarater and interrater reliability for users, suggesting that
it is a reproducible instrument for evaluating thumb CMC OA. Quantifiable measurements may serve to
supplement Eaton staging in assessing the severity of CMC disease, but more research needs to be done to
correlate the ThOA index to specific CMC pathology.
Acknowledgements. This study was supported by NIH/NIAMS R01AR059185 and the Stanford University
MedScholars Program.
References. [1] Ladd, AL et al., Journal of Hand Surgery (in press), 2014.
[2] Eaton, RG et al., Hand Clinics, 455-471, 1987.
[3] Halilaj, E et al., Clinical Orthopaedics and Related Research, 1114-1122, 2014.
COI. The authors report no conflicts of interest.
Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Power Grip and the Biomechanics of CMC Osteoarthritis
Jorge L. Orbay1, Michael R. Mijares2
1) Department of Orthopaedics, The Miami Hand Institute, Miami, FL, USA
2) Department of Orthopaedics, The Miami Hand Institute, Miami, FL, USA
Introduction
Thumb carpometacarpal arthritis is a common yet controversial problem. Despite avid discussion, there remains a lack of
understanding; the pathophysiology of CMC disease is largely unexplained. Dorsal subluxation is universal among
arthritic CMC joints. Free body analysis of the thumb during pinch and power grip show a dorsally directed force only
present during power grip. We hypothesized CMC osteoarthritis is the result of forces generated during this action.
Materials and Methods
A mid humerus fresh-frozen cadaver specimen was mounted on a wooden frame using Steinman pins. The wrist
was stabilized in neutral with Kirschner wires and the last 4 MCP joints in flexion. The thumb carpometacarpal joint was
dissected and exposed, initially preserving the native ligaments. The APB, FPL, FDP-Index, and FDP-III, IV, and V were
dissected and each tendon was prepared for weight suspension. These tendons were loaded with lead weights until a
stable configuration was obtained for key pinch and power grip. The dorsal ligaments were resected and its effects on
thumb stability observed for both key pinch and power grip positions.
Results
With the hand positioned in key pinch and the dorsal ligaments excised, the thumb CMC joint was stable with static and
dynamic testing. However, when placed in power grip, the thumb became grossly unstable.
Discussion
Our study demonstrates that the loaded thumb CMC joint is intrinsically stable in key pinch and unstable in power grip.
COI.
Author JLO, Skeletal Dynamics, LLC. Author MRM, None.

Proceedings of the 9th
Triennial Hand and Wrist Biomechanics International (HWBI) Symposium
Milan, Italy, June 16-17, 2015
Decreased Functional Pinch Strength is Associated with Early Thumb CMC Osteoarthritis
Thomas J. McQuillan1, Deborah Kenney1, Joseph J. Crisco2, Arnold-Peter C. Weiss2, Amy L. Ladd1
1) Robert A. Chase Hand and Upper Limb Center, Department of Orthopedics, Stanford University Medical Center, Stanford, CA, USA 2) Department of Orthopedics, Warren Alpert Medical School, Brown University, Providence, RI, USA
INTRODUCTION. Thumb carpometacarpal (CMC) osteoarthritis (OA) is an important contributor to orthopaedic
morbidity worldwide. Self-reported pain, weakness, and physical exam may supplement radiographic findings in
the diagnosis of early thumb CMC OA. Our goal was to examine the association between declining pinch
strength and early OA diagnosis for three different types of pinching.
METHODS. This case-control study recruited 23 normal and 91 symptomatic early OA patients (Eaton stage 0
or I) for a comprehensive history, physical exam, strength measurements and radiographic evaluation. Strength
was assessed using three different pinch modalities: key pinch, tripod pinch, and tip pinch. Multivariate logistic
regression was used to estimate the predictive value of key pinch, tripod pinch and tip pinch strength on the
likelihood of early OA diagnosis. We controlled for age, sex, and BMI, which are known risk factors for OA, in
order isolate the effect of declining pinch strength on the likelihood of early OA. Data were analyzed using Stata
(College Station, Texas, USA).
RESULTS. Decreased key pinch strength was the strongest predictor of early OA diagnosis in both our crude
and adjusted model. We estimated that a 20% decrease in key pinch strength from the control baseline was
associated with a 9.73% increase in the likelihood of early OA diagnosis (p<.01) after controlling for age, sex,
and BMI. A decline in 20% of tripod pinch was associated with a 4.89% (p<.05) increase in the likelihood of
early OA, and tip pinch was associated with a 5.95% p<.05 increase in likelihood of early OA.
DISCUSSION. This study suggests that declining pinch strength is an early indicator of the degenerative
process of OA. Declining key pinch strength is the most sensitive of the three pinch modalities that we
examined in our study, possibly due to the increased load in the volar direction on the CMC joint in this position
[1, 2]. More research is needed to describe the pathogenesis of weakness in early CMC disease.
Acknowledgements. This study was supported by NIH/NIAMS R01AR059185 and the Stanford University
MedScholars Program.
References. [1] Villafañe, JH et al, Journal of Physical Therapy Science, 993-995, 2014.
[2] Halilaj, E et al, Clinical Orthopaedics and Related Research, 1114-1122, 2014.
COI. The authors report no conflicts of interest.
Hand and Wrist Biomechanics International
H W B I affiliated with
International Society of Biomechanics (ISB) International Federation of Societies for Surgery of the Hand (IFSSH)
Visit us at
http://www.hwbi.org





























