Embed Size (px)
Citation preview

Drugs 36 (Suppl. I): 115-119 (1988) 0012-6667/88/0100-0115/$2.50/0 © ADIS Press Limited All rights reserved.
Haemodynamic Changes Associated with Long Term Antihypertensive Therapy with Ketanserin Hiroshi Noda, Masaaki Isaka, Yasushi Ito and Tashiro Fujita Department of Internal Medicine. Clinical Medicine. University of Tsukuba. Ibaraki, Japan
Ketanserin is a new serotonergic receptor-block-ing agent which has specific inhibitory action on the serotonin S2-receptors (Leysen et al. 1981) but is devoid of partial agonistic properties. Experi-mental and clinical studies ofketanserin have been conducted in patients with pathological conditions in which serotonin is considered to playa role, and the efficacy and safety of the drug have been re-ported (Janssen 1983). The antihypertensive effect of ketanserin has been clearly demonstrated in both animals and humans (Wenting et al. 1984). The mechanism of action ofketanserin as an antihyper-tensive agent is complex and remains to be fully clarified, but there is a possibility that ketanserin acts synergistically at S2-serotonergic and (XI-adren-ergic receptors to lower blood pressure. Another feature ofketanserin is that it does not have partial agonistic action on serotonin Sl-receptors or cause troublesome central nervous system side effects (Pettersson et al. 1985), which have been observed with conventional antiserotonin agents.
Since increases in peripheral vascular resistance are often seen in patients with essential hyperten-sion. the use of a drug with vasodilatory action is a desirable approach to correct some cardiodyn-amic abnormalities.
This study examined the haemodynamic and endocrinological effects of administration of ketan-serin for 12 weeks to ambulatory patients with es-sential hypertension.
1. Subjects and Methods
The subjects were IS outpatients (13 males and 2 females) with essential hypertension, ranging in age from 31 to 60 years (average age 49.8 ± 1.8 years). The severity of the hypertension was con-sidered to be mild if the total score (according to the classification system of the 3rd Department of Internal Medicine of Tokyo University) was 5 or less. In patients already taking antihypertensive medication, this was discontinued at least 2 weeks before the start of the study, and all of the patients were instructed to restrict their dietary salt intake to between 6 and 8g per day.
After it was confirmed that the systolic blood pressure was above 160mm Hg and/or the dia-stolic pressure was above 95mm Hg, cardiac haemodynamic measurements were recorded by M-mode and 2-dimensional echocardiography (Noda & Fujita 1987) when the patient was in the supine position. Two-dimensional views were used as a quality control check on the accuracy of the M-mode calculations. Blood was then collected after patients had rested for 30 minutes in the supine position. General haematological laboratory tests were performed, and plasma concentrations of sod-ium, potassium, chloride, creatinine, urea nitrogen, uric acid, total protein, cholesterol, alanine ami-notransferase (AL T), asparate aminotransferase (AST), alkaline phosphatase (ALP), lactate dehy-drogenase (LDH), gamma-guanosine triphosphate (-y-GTP), and creatine phosphokinase (CPK), as well as plasma renin activity (Fujita et al. 1982a) and plasma aldosterone concentration (Fujita et al. 1982b) were measured.
Ketanserin 40mg once daily was administered to all patients throughout the 12-week study. Blood pressure was checked every 2 weeks. Four weeks after the start of ketanserin administration, a di-uretic and/or ~-blocker was additionally given to

Haemodynamic Effects of Ketanserin
180
Ci 160
~~~~~~~~ u I 0: E 140 B E Ul _
.~ Q) 120 "0 ~ "0 iil c Ul 100 '" Q) .~ c. :§-g 80 * ~.Q 00.0 60
~ I I I I I I I I
-2 0 2 4 6 8 10 12
Time (weeks)
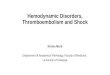
Fig. 1. Changes in systolic and diastolic blood pressures (mean ± SEM) during administration of ketanserin 40mg once daily for 12 weeks to 15 patients with mild to moderate hyper-tension; • = p < 0.001.
the patients whose systolic pressure had not fallen below 150mm Hg and/or whose diastolic pressure had not fallen to 90mm Hg or less, and to patients whose decrement of mean blood pressure was un-der 10%. Six patients were non-responders.
Subsequent laboratory and haemodynamic studies were performed only on the 9 patients classified as responders according to the above def-inition after administration of ketanserin for 2 to 4 weeks.
The SPSS (Statistical Package for Social Sci-ence) of the Scientific Processing Center of Tsu-kuba University was used for statistical analysis, and the results were expressed as mean ± SE.
2. Results 2.1 Blood Pressure Changes
The changes in sitting systolic and diastolic blood pressure are shown in figure 1. After 2 weeks of ketanserin administration, both the systolic and diastolic blood pressures were reduced signifi-cantly, and there was a gradual further decrease in blood pressure up to 12 weeks. Mean blood pres-sure decreased significantly by 15.5 ± 1.3%, from 119.3 ± 1.0mm Hg before ketanserin administra-tion to 100.8 ± 1.6mm Hg 12 weeks later.
116
2.2 Haemodynamic Changes
Heart rate, cardiac index and total peripheral resistance index measurements before and after ke-tanserin treatment are shown in table I. The changes in heart rate and cardiac index were not significant, although the decrease in total peripheral resistance index was.
As shown in figure 2, there was a significant, positive correlation between the magnitude of de-crease in mean blood pressure and the decrease in total peripheral resistance index.
2.3 Hormonal Dynamics
Plasma renin activity and plasma aldosterone concentration increased slightly after ketanserin administration, but these changes were not signifi-cant (table II).
2.4 Laboratory Test Results
Ketanserin administration was not associated with any significant changes in any of the routine laboratory test values listed in section 1; however, the uric concentration increased slightly in 2 patients (5.5 to 8.0 mgfdl; 6.7 to 7.3 mg/dl). Fast-ing blood glucose and bodyweight were also un-changed.
2.5 Side Effects
Although some side effects were reported, in no patient was an adverse event considered to be caused by the administration of ketanserin.
3. Discussion
The mechanisms responsible for increased blood pressure and, by extension, the mode of action of compounds which control essential hypertension are still unclear, but one pathological element may be an increase in peripheral vascular resistance. Therefore, drugs which have vasodilatory action are thought to be particularly suitable for the treat-ment of hypertension.

Haemodynamic Effects of Ketanserin 117
Table I. Haemodynamic changes in patients with mild to moderate essential hypertension after 12 weeks' treatment with ketanserin 40mg daily
Patient no. Heart rate (beats/min) Cardiac index (L/min/m2) Total peripheral resistance index (dyne' sec· cm-5 • m2)
before after "loll before after %Il before after %Il
1 72.3 74.2 2.6 3.29 3.34 1.52 2773 2434 -12.2 2 70.6 71.6 1.4 3.31 3.18 -3.93 2852 2632 -7.7 3 68.7 73.2 6.6 3.21 2.93 -8.72 2903 2518 -13.3 4 70.8 72.3 2.1 3.31 3.26 -1.51 2876 2470 -14.1 5 82.6 84.2 1.9 3.38 3.30 -2.37 2933 2452 -11.4 6 65.3 68.2 4.4 3.40 3.27 -3.82 2730 2256 -17.4 7 72.5 73.3 1.1 3.30 3.33 0.91 2836 2453 -13.5 8 74.2 75.8 2.1 3.28 3.35 2.13 2926 2522 -13.8 9 72.4 73.9 2.1 3.12 3.12 0.0 3089 2542 -17.7 Mean ± SE 72.2 ± 1.6 74.1 ± 0.9 2.7 ± 1.6 3.29 ± 0.03 3.23 ± 0.04 -1.B ± 1.1 2880 ± 33 2475 ± 33 -14.0 ± 1.0 Significance NS NS
-20
l ~ ::> '" '" ~ a. -10 "0 0 0 :0 c: '" Q)
~ <I
0 -10 -20
.l Total peripheral resistance (%)
Fig. 2. Relationship between the magnitude of the decrease in total peripheral resistance and that in mean blood pressure in 9 patients with mild to moderate hypertension who responded to treatment with ketanserin; r = 0.664. n = 9, P < 0.05.
However, studies in experimental models and clinical trials of serotonergic-receptor antagonists in essential hypertension suggest that central sero-tonergic neurons have a role in the development and maintenance of an increased vascular resist-ance in essential hypertension. For example, it has been observed that in spontaneously hypertensive rats, hypertension can be suppressed when the
P < 0.001
serotonin neurons in the central nervous system are destroyed by the administration of 5,6-dihy-droxytryptamine (Buckingham et al. 1976), and that hypotensive effects are achieved in spontaneously hypertensive dogs (De Clerck et al. 1982) and rats (Jarrott et al. 1975) by the administration of the tryptophan hydroxylase inhibitor parachlorophen-ylalanine and ketanserin.
An antiserotonin agent, ketanserin, has recently been introduced in humans; consequently the re-lationship between the serotonergic nervous sys-tem and essential hypertension has been attracting considerable attention. The antihypertensive ef-fects of ketanserin, when administered orally or intravenously to patients with essential hyperten-sion, have been reported by several authors (Hed-ner et al. 1985; Wenting et al. 1984), and clinical studies of ketanserin as an antihypertensive agent are now underway in Japan. This drug is fre-quently described as a serotonin S2-receptor ant-agonist that has some al-adrenoceptor antagonist activity, although it has been reported that the al-blocking action does not contribute to the anti-hypertensive mechanism when ketanserin is given in standard doses (Schalekamp 1985). There is some suggestion that the vasodilatory and antihyperten-sive actions of this drug may be caused by a syn-

Haemodynamic Effects of Ketanserin 118
Table II. Effect of 12 weeks' treatment with ketanserin on plasma renin activity and plasma aldosterone concentration in 9 patients with mild to moderate essential hypertension
Patient no. Plasma renin activity (ng/ml/h)
before after LI.
1 0.4 0.2 -0.2 2 0.4 0.9 0.5 3 0.1 0.8 0.7 4 0.4 1.0 0.6 5 1.7 1.8 0.1 6 0.7 0.9 0.2 7 0.4 1.4 1.0 8 1.4 0.4 -1.0 9 0.3 0.1 -0.2 Mean ± SE 0.64 ± 0.17 0.83 ± 0.17 0.19 ± 0.19 Significance NS
ergistic effect at S2-serotonergic and ai-adrenergic receptors.
Since almost no ketanserin penetrates the blood-brain barrier, it appears that the antihypertensive effects are caused by a lowering of resistance and dilatation of peripheral vascular vessels. Serotonin-induced platelet aggregation is mediated via the serotonin Sz-receptor. The inhibition of platelet ag-gregation by ketanserin indicates the involvement ofSz-serotonergic receptors in the antihypertensive action of ketanserin.
In the present study, haemodynamic and other tests were performed only in the 9 patients whose blood pressure was reduced to target values during treatment with ketanserin alone. Mean blood pres-sure decreased by 15.5 ± 1.3% after 12 weeks of ketanserin administration. There was no change in heart rate (1.7 ± 1.1 %), but total peripheral vas-cular resistance decreased significantly (14.0 ± 1.0%). In addition, there was a statistically signifi-cant, positive correlation between the decrement in mean blood pressure and that in total peripheral resistance. These results appear to reconfirm ear-lier reports and suggest that a direct vasodilatory action contributes to the antihypertensive action of ketanserin.
The absence of change in heart rate indicated that ketanserin caused little reflex sympathetic
Plasma aldosterone concentration (ng/mll
before after LI.
6.7 4.7 -2.0 6.1 7.4 1.3 3.4 5.8 2.4 3.6 6.4 2.8 6.0 4.2 -1.8 5.8 4.7 -1.1 4.3 7.2 2.9 6.5 8.9 2.4 4.3 5.2 0.9 5.19 ± 0.40 6.06 ± 0.49 0.82 ± 0.65 NS
nerve stimulation, such as is seen with conven-tional vasodilators.
With respect to the effects on the renin-angio-tensin system, PRA was 0.64 ± 0.17 ng/ml/h and 0.83 ± 0.17 ng/ml/h before and after administra-tion, respectively, and PAC was 5.2 ± 0.4 ng/ml before and 6.1 ± 0.5 ng/ml after administration. The lack of effect of ketanserin on plasma renin activity and plasma aldosterone concentration after 12 weeks of administration indicated that the drug had little effect on the renin-angiotensin system. In addition, since the bodyweight of patients did not change significantly throughout the study, there did not seem to be any sodium retention.
A slight increase in plasma uric acid concentra-tions occurred in 2 patients after administration of ketanserin. Neither these nor any of the other mi-nor changes in laboratory test values were signifi-cant.
Adverse effects reported sporadically with the use of conventional vasodilators - dizziness, stag-gering, giddiness on standing and palpitations -were not observed in any patients.
It can be concluded from the above results that, when administered to patients with mild to mod-erate essential hypertension, ketanserin is well tol-erated and produces an antihypertensive effect which is associated with a significant decrease in total peripheral resistance.

Haemodynamic Effects of Ketanserin
References
Buckingham RE, Hamilton TC, Robson D. Effect of intracere-broventricular 5,6-dihydroxytryptamine on blood pressure of spontaneously hypertensive rats. European Journal of Pharma-cology 36: 431-437, 1976
De Clerck F, Jageneau A, Dom J. Haemorheological effects of ketanserin, a selective 5-HT 2 receptor antagonist, in aged, spontaneously hypertensive dogs. Archives Internationales de Pharmacodynamie et de Therapie 258: 100-115, 1982
Fujita T, Sato y, Ando K, Noda H, Ueno N, et al. Dynamic responses of active and inactive renin and plasma norepi-nephrine during exercise in normal man. Japanese Heart Jour-nal 23: 545-551, 1982a
Fujita T, Ando K, Noda H, Sato Y, Yamashita N, et al. Hemo-dynamic and endocrine changes associated with captopril in diuretic-resistant hypertensive patients. American Journal of Medicine 73: 341-347, 1982b
Hedner T, Pettersson A, Persson B. Blood pressure reduction and pharmacokinetics of ketanserin in patients with essential hypertension. Satellite symposium to the 2nd European Meet-ing on Hypertension, Milan, June 9,1985, Abstract, p. 35,1985
Janssen PAJ. 5-HT 2 receptor blockade to study serotonin-induced pathology. Trends in Pharmacological Sciences 4: 198-206, 1983
Jarrott B, McQueen A, Graf L, Louis WJ. Serotonin levels in vascular tissue and the effects of a serotonin synthesis inhibitor
119
on blood pressure in hypertensive rats. Clinical and Experi-mental Pharmacology and Physiology (Suppl. 2): 201-205, 1975
Leysen JE, Awouters F, Kennis L, Laduron PM, Vandenberk J, et al. Receptor binding profile of R 41 468, a novel antagonist at 5-HT2 receptors. Life Sciences 28: 10 15-1 022, 1981
Noda H, Fujita T. Left ventricular hypertrophy in young patients with borderline hypertension. Nippon Naika Gakkai Zasshi (Journal of the Japanese Society of Internal Medicine)76: 1211-1217,1987
Pettersson A, Gradin K, Hedner T, Persson B. Antihypertensive mechanism of action of ketanserin and some ketanserin dia-logues in the spontaneously hypertensive rat. Naunyn-Schmie-deberg's Archives of Pharmacology 329: 394-397, 1985
Schalekamp MADH. Haemodynamic effects of ketanserin: mech-anism of the antihypertensive action. Satellite symposium to the 2nd European Meeting on Hypertension, Milan, June 9, 1985, Abstract, p. 9, 1985
Wenting GJ, Woittiez AJJ, Man in't Veld AJ, Schalekamp MADH. 5-HT, alpha-adrenoceptors, and blood pressure. Effects of ke-tanserin in essential hypertension and autonomic insuffi-ciency. Hypertension 6: 100-109, 1984
Author'S address: Dr Hiroshi Noda, Fourth Department of Internal Medicine, University of Tokyo School of Medicine, 3-28-6 Mejirodai, Bunkyo-ku, Tokyo 112 (Japan).