Embed Size (px)
Citation preview

H3 HEAT Targetand
Max in the Middle
Dr Graham FosterConsultant in Public Health Medicine

Evidence Review• Primary and secondary approaches
• Individual needs and community development
• Not stigmatising
• Whole school approaches
• Change physical activity, diet and behaviour
• Long term view not one off projects or short term support

Examples of best practice
No single programme is model, but key elements can be identified

Multi-agency planning day

Existing Services and Programmes• Fit for Girls• Physical Activity Co-ordinators• Breakfast Clubs• Healthy Tuck shops• Leisure Centres and Sports Clubs• Hungry for Success

Existing Specialist Services
• Primary Care• Community Dieticians• Specialist Obesity Clinic• YUFF Programme

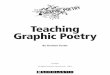
Primary 7 (aged 11-12)Source : Child Health Surveillance Programme - School
10%
15%
20%
25%
30%
35%
1999/00 2000/01 2001/02
Male -Overweight
Female -Overweight
Male -Obese
Female -Obese
Childhood Obesity in Scotland

And it just gets worse
• By age 40 almost 60% of females in Central Scotland are overweight or obese
• For males 50%

Conclusions
• Build on what we already have• Community / Family approach• Introduce a universal Level 1 -
Max• Join up the existing Level 2 • Expand the specialist Level 3 -
YUFF

Max in the Middle
• Why are we doing it?• What is it?

Max in the Middle
• School Based Programme• Whole class approach• Drama• Dance• Empowerment• Parental Involvement

What is - Max in the Middle• History –
– behavioural intervention whole class approach
– substance misuse– pilots on healthy behaviours
• An 18 hour, intensive school based, whole class intervention promoting healthy behaviours and engaging parents and families

Benefits - Max in the Middle• Universal–
– No Exclusions / withdrawals– Highly innovative– Exciting– Memorable– Not work– Links to Curriculum for excellence– Links to Community– Local Focus and relevance– Kids love it and want to participate– Families get enthused and engaged

Meeting Monday

Meeting Monday
• Meet the Team• Size up the class / school• Break the ice• Build confidence• Play games• Do some dance


Tasty Tuesday

Tasty Tuesday
• All about Food• Parental volunteers• Food is not dangerous• Handle food, taste food, enjoy
food• Memorable Messages• Healthy eating plate etc

Workout Wednesday

Workout Wednesday
• Elements of fitness• Physical Activity as ADL• Local Opportunities• Clubs and Groups• Walks, games, transport• More dancing

Thursday is Rehearsal Day

Friday - Performance

Friday - Performance
• Children do invites• All welcome• Big attendances even in most
deprived/least engaged schools• Opportunity to meet the parents• Interaction• NOT in front of school

Review of 2008/9• Max in 21 primary schools, 600 children
• 200 obese children completed a Max week
• Positive internal evaluation
• Only NHS Board to deliver agreed number of interventions

2009 to 2011• 42 schools per year, Approx 1200
children
• All introduced to level 2 (engagement)
• 40 referrals - YUFF/Specialist service
• NHS Health Scotland evaluation

2012 so far• 84 schools per year, Approx 2100 children
• 42 Full Max Experience (18 Hours) Primary 6• 42 Max Lite (1 in Service day of teacher training
and 6 1 hour school visits) Primary 5
• Heights and Weights on all children (our greatest challenge)
• Planning for Sustainability

Small changes count• 150 kcal xs per day = 7kg per year
• 150 kcal = 1 sandwichor
»1 can of cokeor
»1/2 Mars bar

• Thank you

Primary prevention – avoiding development of unhealthy weight
Secondary prevention – early detection of unhealthy weight to avoid development of health problems
Individual needs addressed within a community development approach
Evidence Base for Max Programme

• Ideally multi-level: individual, school & community
• Whole-school approaches should be used in schools, ideally
• Schools-based approaches need support from families & communities
•Multi-component with behaviour change strategies to: Increase physical activity Improve eating behaviour
Promote behaviour Change
•All components tailored to the setting

•Parental/carer obesity major risk factor for child obesity
• Parents should be actively involved
• Parents encouraged to have main responsibility for lifestyle changes
• Change can be hampered by complex living and working
• Participant engagement is fundamental to effectiveness
• Stakeholders (families, schools, others) need to be included
•Short term interventions and one-off events are insufficient

•Need to tailor advice and address potential barriers
• Consider groups such as ethnic minorities, low incomes etc
•Overweight and obese children with significant co-morbidities or complex needs should be referred to specialists