Embed Size (px)
Citation preview

Simpson-Golabi-BehmelSyndrome
H o s p i t a l U n i v e r s i t a r i o L a P a z M a d r i d
Rome, November 2009Pablo Lapunzina-INGEMM- Instituto de Genética Médica y Molecular
Instituto de Genética Médica y Molecular

Simpson Golabi Behmel- ClassificationHospital Universitario La Paz
Described independently by Simpson et al. (1975), Golabi & Rosen (1984) and Behmel et al. (1984)
Renamed in 1988 by G. Neri & co. as Simpson-Golabi-Behmel Syndrome
Simpson-Golabi-Behmel is an Overgrowth Syndrome
Neri et al., Am J Med Genet. 1988 May-Jun;30(1-2):287-99.

Overgrowth Syndromes. Classification5%
Hospital Universitario La Paz
• Hyperplasia• Hypertrophy• Increased interstitial fluid• Any combination of them

• A -TRUE:
• B –PARTIAL /LOCALIZED
• C - MISCELANEOUS:CHROMOSOMAL-ENDOCRINOLOGY-OTHERS
OGS Classification5%
Hospital Universitario La Paz
Bannayan-Riley-RuvalcabaBeckwith-WiedemannSotosWeaverMacrocephaly/capillary malformationSimpson-Golabi-BehmelPerlmanCostelloNon-syndromic OGS with or without MR
Hemihypertrophy/hemihiperplasiaKlippel TrenaunayProteusCLOVECLAPOChromosomal (Klinefelter; PallisterKillian; Trisomy 8 mosaic; Fragile X; Duplication 4p16.3; Deletion 22q13Endocrinologic (son of diabetic mother; hypophysis)Other (Marfan/ Homocystinuria)
Cohen, Neri and Weksberg. Overgrowth Syndromes.Oxford University Press

The OGS share some common characteristics:
Increased risk of mental retardation
Increased risk of tumours
Overgrowth Syndromes. Characteristics5%
Hospital Universitario La Paz

OGS. Mental retardation5%
Hospital Universitario La Paz
• In some disorders
Sotos syndrome ∼ 70 %Simpson Golabi Behmel syndrome ∼ 30-50 %Macrocephaly- Capillary Malf. ∼ 40 %Beckwith Wiedemann syndrome ∼ 2-3 %
OGS. Tumoral Risk5%
Hospital Universitario La Paz
Mild Tumor Risk
• Malignancies
Bannayan-Riley-RuvalcabaKlippel-TrenaunaySotos WeaverProteusMacrocephaly- Capillary Malformation
• Benign Tumors
HemihypertrophyBeckwith- Wiedemann
High Tumor Risk
• Malignancies
Perlman Simpson-Golabi-BehmelBeckwith-WiedemannHemihypertrophy
• Benign tumors
Proteus Bannayan-Riley-RuvalcabaKlippel-Trenaunay

SGBS- Common Clinical Findings5%
Hospital Universitario La Paz
SIMPSON-GOLABI BEHMEL SYNDROME
• Overgrowth (mainly in height and weight)• Coarse face• Dental crowding• Cleft palate- Cleft lip• Polydactyly• Lipomas and mesenchymatic tumors• Speech and language problems• Variable mental retardation• Increased tumor risk

SGBS-Data from the SOGSR5%
Hospital Universitario La Paz
Established in November 2003 at Hospital UniversitarioLa Paz (Madrid)About 1200 entries of at least 15 diff disordersNation-wide with participation of all regions
RESSC- Registro Español de Síndromes de SobrecrecimientoSOGSR- Spanish OvergrowthSyndrome Registry

Coarse faceHypertelorismLarge mouthMidline groove of tongue Cleft lip Cleft palateMalposition of teethCongenitally missing teethSupernumerary teeth Odontogenic keratocysts
SGBS- Clinical Findings - Face5%
Hospital Universitario La Paz
Krimmel M, Reinert S. Br J Oral Maxillofac Surg. 2000 Jun;38(3):221-3

SGBS- Facial features5%
Hospital Universitario La Paz

SGBS- Facial features5%
Hospital Universitario La Paz

SGBS- Clinical findings5%
Hospital Universitario La Paz

SGBS-Abdominal problems5%
Hospital Universitario La Paz
• Diaphragmatic herniae• Hepatomegaly• Splenomegaly (rare)• Extra nipples
Enns et al., Am J Med Genet. 1998 Sep 23;79(3):215-25
Slavotinek, Am J Med Genet C Semin Med Genet. 2007 May 15;145C(2):172-83

SGBS- Abdominal findings5%
Hospital Universitario La Paz

SGBS- Clinical findings5%
Hospital Universitario La Paz

SGBS-Cardiovascular problems5%
Hospital Universitario La Paz
Cardiovascular problems in 26%
• Ischemic stroke (dissection of internal carotid )
• Hepatic vascular malformation• Tachyarrhythmias• Cardiomyopathy• Other electrocardiogram abnormalities
König et al., Am J Med Genet. 1991 Feb-Mar;38(2-3):244-7Lin et al., Am J Med Genet. 1999 Apr 23;83(5):378-81
Pénisson-Besnier et al., Am J Med Genet A. 2008 Feb 15;146A(4):464-7Cureton et al, 26: Am J Med Genet A. 2007 Jun 15;143A(12):1379-81

SGBS-Limbs anomalies5%
Hospital Universitario La Paz
Broad handsShort hands Hypoplastic finger nailsPostaxial hexadactylyDeep plantar creases

SGBS-Speech and language5%
Hospital Universitario La Paz
Speech characterized by a distorted articulationDistorted resonanceFluency failuresStereotype prosody
Van Borsel et al. Genet Couns. 2008;19(2):241-9.

SGBS- Other findings5%
Hospital Universitario La Paz
Anal atresiaHypospadiasPseudo hermaphroditismSevere mental retardationHydrocephalusEpilepsyObstructive sleep apnea
LYoung et al., Pediatr Neurol 2006;34:139-42; Paludetti et al., Int J Pediatr Otorhinolar 2003;67:1143-7
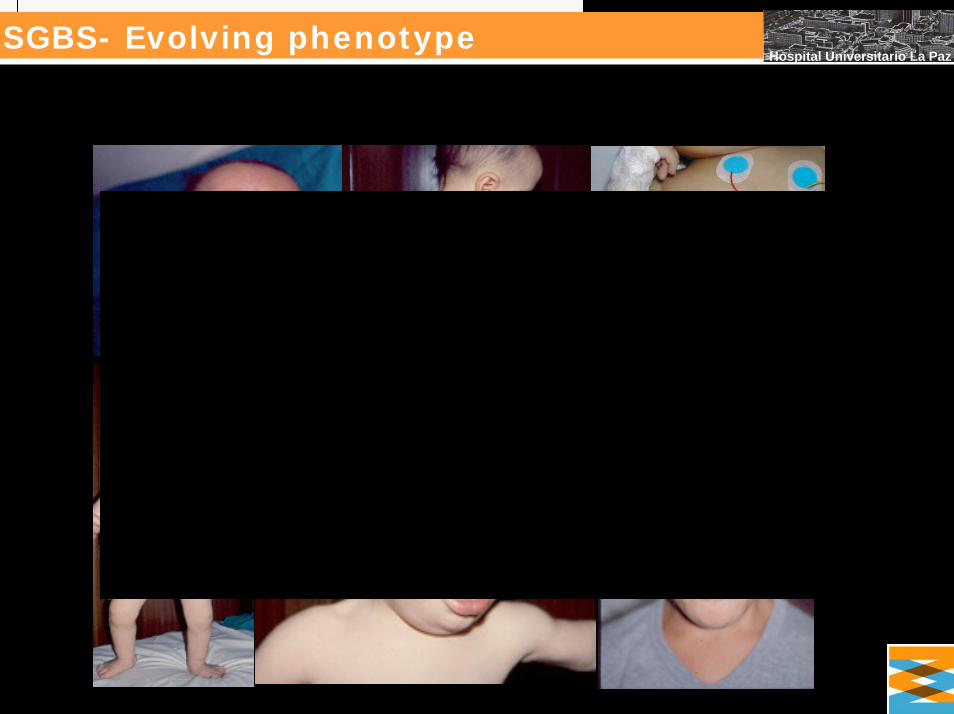
SGBS- Evolving phenotype5%
Hospital Universitario La Paz

SGBS- Etiology & Causes5%
Hospital Universitario La Paz
X-linked gene: glypican 3 (GPC3)
Maps Xq26
GPC3: more than 500 kb and 8 exons.
Protein: Glypican-3 has 580 amino acids.
Pillia et al., Nat Genet. 1996 Mar;12(3):241-7 Orth et al., Am J Med Genet. 1994 May 1;50(4):388-90Xuan et al., Hum Mol Genet. 1994 Jan;3(1):133-7

SGBS Mutations and Deletions5%
Hospital Universitario La Paz
Li et al., Am J Med Genet. 2001 Aug 1;102(2):161-8Rodríguez-Criado et al. Am J Med Genet A. 2005 Oct 15;138A(3):272-7
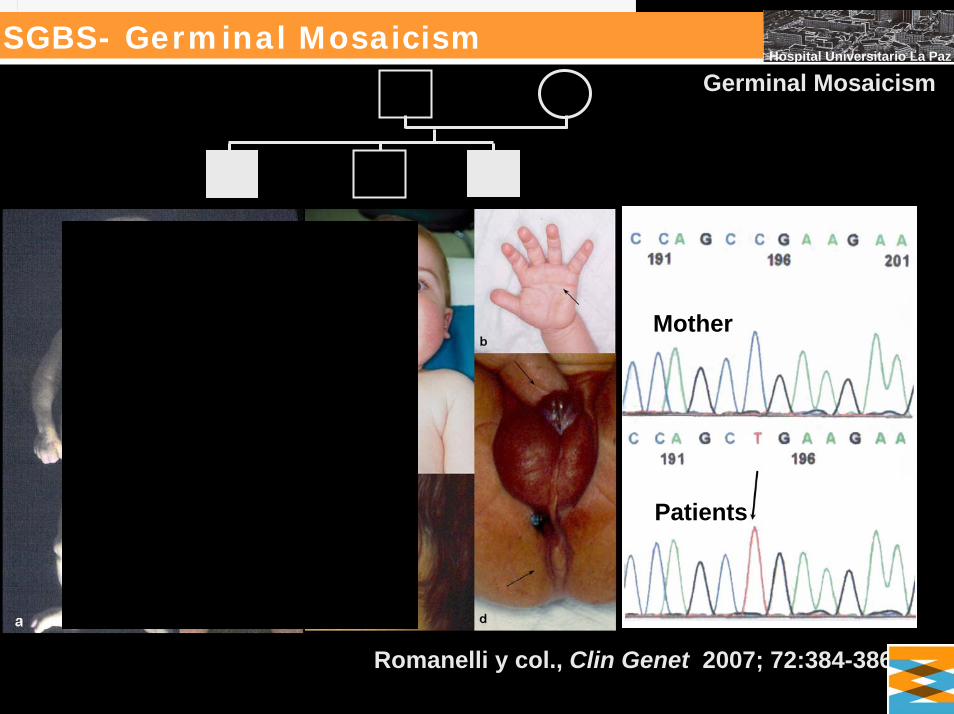
SGBS- Germinal Mosaicism5%
Hospital Universitario La Paz
Germinal Mosaicism
Romanelli y col., Clin Genet 2007; 72:384-386.
Mother
Patients

SGBS. Genotype Phenotype correlation5%
Hospital Universitario La Paz
No specific genotype-phenotype correlation
No major differences between patients with deletions and point mutations
Mariani et al., J Pediatr Endocrinol Metab. 2003 Feb;16(2):225-32Hughes-Benzie et al., 6: Am J Med Genet. 1996 Dec 11;66(2):227-34

SGBS. Differential Diagnosis5%
Hospital Universitario La Paz
Beckwith Wiedemann syndrome
Macrocephaly-capillary malformation
Sotos syndrome
Non-syndromal OG with or without mental retardation

SGBS. Differential Diagnosis5%
Hospital Universitario La Paz
(Macrocephaly-Capillary Malforamtion)
• Overgrowth• Capillary malformation• Nevus flammeus• Capillary malformation in the upper lip/philtrum• Asimmetry/Hemihypertrophy• Hemimegalencephaly• Macrocephaly• Polydactyly• Mental retardation 50%

Differential Diagnosis- M-CM5%
Hospital Universitario La Paz
75%

Differ. Diagnosis- Beckwith Wiedemann5%
Hospital Universitario La Paz

Differential Diagnosis-Sotos syndrome5%
Hospital Universitario La Paz

SGBS-Transgenic mice5%
Hospital Universitario La Paz
Gpc3-deficient mice display a high incidence of :
Ventricular septal defects, common atrioventricular canal and double outlet right ventricle.Delay in endochondral ossificationSomatic overgrowth, renal dysplasia, accessory spleens, polydactyly, and placentomegalyPerinatal death, cystic and dyplastic kidneys, and abnormal lung development. Mandibular hypoplasiaImperforate vagina.
Viviano et al., Dev Biol. 2005 Jun 1;282(1):152-62Cano-Gauci et al., J Cell Biol 199;146:1; 255-264Chiao et al., 58: Dev Biol. 2002 Mar 1;243(1):185-206

SGBS-Transgenic mice5%
Hospital Universitario La Paz
WT
Tg
Mandibular hypoplasiaComplete lack of mandiblein the mutant embryo.
Cano-Gauci et al., J Cell Biol 199;146:1; 255-264

SGBS-Transgenic mice5%
Hospital Universitario La Paz
Gpc3/DeltaH19 double mutants (bialellicexpression of Igf2 gene by imprint relaxation),
Omphalocele and skeletal defects.
Compatible with a model positing that there is downstream convergence of the independent signalling pathways in which either IGFs or GPC3 participate
Chiao et al., 58: Dev Biol. 2002 Mar 1;243(1):185-206

SGBS-Transgenic mice5%
Hospital Universitario La Paz
Glypican-3 inhibits Hedgehog signalling during development by competing with patched for Hedgehog binding.
GPC3 null embryos display increased Hedgehog signalling GPC3 inhibits Hedgehog activity GPC3 interacts with Hedgehog but not with its receptor, Patched GPC3 competes with Patched for Hedgehog binding.GPC3 induces Hedgehog endocytosis and degradation. The heparan sulfate chains of GPC3 are not required for its interaction with Hedgehog. GPC3 acts as a negative regulator of Hedgehog signalingduring mammalian development and that the overgrowth observed in SGBS patients is, at least in part, the consequence of hyperactivation of the Hedgehog signalingpathway.
Capurro et al., Dev Cell. 2008;14:700-11

SGBS-Biology5%
Hospital Universitario La Paz
Direct interaction of GPC3 with CD26
GPC3 without the GPI anchor is capable of inducing apoptosis indicating that neither the GPI anchor nor the membrane attachment is required for apoptosis induction.
Davoodi J et al., Proteomics 2007;7:2300-10

SGBS-Biology5%
Hospital Universitario La Paz
Loss of glypican-3 induces alterations in Wnt signaling.
Matting of GPC3 knockout mice with insulin receptor substrate-1 (IRS-1) nullizygous mice.
GPC3 regulates somatic growth independent of IRS-1, GPC3 does not modulate IGF signaling. GPC3 knockout mice exhibit alterations in the Wnt signaling pathway, GPC3 led to the inhibition of the non-canonical Wnt/JNK signalingpathway and activation of canonical Wnt/beta-catenin signaling. At least in some cell types GPC3 serves as a selective regulator of Wnt signaling, by potentiating non-canonical Wnt signaling, while inhibiting the canonical Wnt signaling pathway.SGBS may in part result from a loss of GPC3 controls on Wntsignaling and requires the cooperation of both the protein and the heparan sulfate moieties of the proteoglycan.
Song et al. J Biol Chem. 2005;280:2116-25.; De Cat et l., J Cell Biol. 2003;163:625-35

SGBS-Oncogenicity5%
Hospital Universitario La Paz
GPC3 bound specifically through its N-terminal proline-rich region to both Insulin-like growth factor (IGF)-II and IGF-1R. GPC3 stimulated the phosphorylation of IGF-1R and the downstream signaling molecule extracellular signal-regulated kinase (ERK) in an IGF-II-dependent way. GPC3 knockdown in HCC cells decreased the phosphorylation of both IGF-1R and ERK. GPC3 confers oncogenecity through the interaction between IGF-II and its receptor, and the subsequent activation of the IGF-signaling pathway.
Cheng et al. Carcinogenesis 2008;29:1319-26.

SGBS-BiologyHospital Universitario La Paz
GPC3IGF2
IGF1R
ERK
P
P
IGFpathway
(+)(-)
(-)
Patched comp

SGBS-Oncogenicity5%
Hospital Universitario La Paz
Wilms tumourHepatoblastoma.HepatocarcinomaAdrenal tumour
Buonuomo et al., Pediatr Hematol Oncol 2005;22:623-8Lapunzina et al., J Med Genet 1998;35:153-6Zynger et al., Am J Surg Pathol 2006;30:1570-5

SGBS-Surveillance for WT5%
Hospital Universitario La Paz
Surveillance for Wilms tumour
Should be offered to children at >5% risk of Wilmstumour. Should only be offered after review by a clinical geneticist. Should be carried out by renal ultrasonography every 3-4 months. Should continue until 7 years. Can be undertaken at a local centre, but should be carried out by someone with experience in paediatric ultrasonography. Screen-detected lesions should be managed at a specialist centre.
Scott et al, Arch Dis Child. 2006;91:995-9.

Overgrowth Syndromes- Risk of Tumours5%
Hospital Universitario La Paz
Lapunzina, Am J Med Genet C Semin Med Genet. 2005;137:53-71; Gracia and Lapunzina, J Pediatr Endocrinol Metab. 2005 Dec;18 Suppl 1:1227-35

SGBS-SummaryHospital Universitario La Paz
Simpson-Golabi-Behmel syndrome
Rare, X-linked overgrowth syndromeTypical craniofacial featuresGPC3 Mild to moderate mental retardationTumour riskSurveillance for embryonal tumours





























