Embed Size (px)
Citation preview

HEALTHCARE REFORM AND THE CASE MANAGER
Nancy Skinner, RN-BC, CCM

OBJECTIVES Detail financial and regulatory initiatives
that impact the current practice of case management.
Detail competencies for advancing collective accountability, personal responsibility and healthcare consumerism through each patient transition of care.
Identify current and proposed models of care coordination that enable appropriate patient “handovers” during each healthcare encounter.

THE AFFORDABLE CARE ACT (ACA)
Balancing access, quality, safety and cost!

“IT'S ABOUT BETTER CARE: CARE THAT IS SAFE, TIMELY, EFFECTIVE, EFFICIENT, EQUITABLE AND PATIENT-CENTERED.”
O’Reilly, K. Health Reform Law Will Boost Care Quality. Amednews.com.

SOME WORDS FROM THE SECRETARY
“Americans go the hospital to get well, but millions of patients are injured because of preventable complications and accidents. Working closely with hospitals, doctors, nurses, patients, families and employers, we will support efforts to help keep patients safe, improve care, and reduce costs. Working together, we can help eliminate preventable harm to patients.”
5
On March 22, 2011, the U.S. Department of Health and Human Services released its National Strategy for Quality Improvement in Health Care (National Quality Strategy). The Affordable Care Act required the Secretary of HHS to establish a national strategy to improve the delivery of health care services, patient health outcomes, and population health. This strategy is designed to guide federal, state, and local health initiatives. 6
Establishing the Goals

The National Quality Strategy establishes three broad aims: Better Care, Healthy People/Healthy Communities, and Affordable Care.
Six Strategies to Advance these AimsPrevention and Treatment of Leading Causes of
MortalitySupporting Better Health in CommunitiesMaking Care More Affordable Making care safer by reducing harm caused in
the delivery of careEnsuring that each person and family members
are engaged as partners in their carePromoting effective communication and
coordination of care

8
HALLMARKS OF ACA
Coordinated Team ApproachPatient and Family Centered CareTransitions of CareCare CoordinationDisease Management
Over half the funding of ACA, which will cost an estimated $938 billion over 10
years, comes from reductions in Medicare payments to hospitals and other
nonphysician providers.

9
FOCUS OF ACA
Improving Quality & Efficiency of Care
Reduction of Hospital Readmissions
Provisions for Medical Home
Provisions for Medication Therapy Management
Access to Care
Provisions for Care Coordination
Community-Based Care Transition programs
Chronic Care Disease Management
Transitional Care Provisions
Wellness Programs Shared Decision Making

IMPROVING THE QUALITY & EFFICIENCY OF CARE

11
Partnership for Patients: Better Care, Lower Costs is a program that "will help save 60,000 lives by stopping millions of preventable injuries and complications in patient care over the next three years” according to a Department of Health and Human Services statement.
Through the initiative, major hospitals, employers, healthcare providers, patient advocates, and government officials will work together toward two main goals: preventing harm in hospitalized patients and helping patients heal without complications.
Partnership for Patients will begin by focusing on nine kinds of medical errors and complications, including adverse drug reactions and pressure ulcers.
Partnership for Patients

PARTNERSHIP FOR PATIENTS TO IMPROVE CARE AND LOWER COSTS FOR AMERICANS
Keep hospital patients from getting injured or sicker. By the end of 2013, preventable hospital-acquired conditions would decrease by 40-percent compared to 2010. Achieving this goal would mean approximately 1.8 million fewer injuries to patients, with more than 60,000 lives saved over the next three years.
Help patients heal without complication. By the end of 2013, preventable complications during a transition from one care setting to another would be decreased so that all hospital readmissions would be reduced by 20-percent compared to 2010. Achieving this goal would mean more than 1.6 million patients will recover from illness without suffering a preventable complication requiring re-hospitalization within 30 days of discharge.
12

INCENTIVE PAYMENTS TIED TO PATIENT SATISFACTION
Under the federal proposal for Hospital Inpatient Value-Based Purchasing incentive payments, patient experience scores will be used to determine 30% of reimbursement for discharges at more than 3,000 hospitals.
Beginning in 2012, every hospital will see a 1 percent reduction in the amount that Medicare reimburses for each service. Medicare will take that savings, which it estimates to be about $850 million in the first year, and redistribute it based on quality and patient satisfaction scores.
13
PATIENTS' PERCEPTION OF HOSPITAL CARE IN THE UNITED STATES
CAHPS data indicated the quality of clinical care and certain hospital characteristics, such as a higher ratio of nurses to patient-days, were associated with greater patient satisfaction.
Specific areas for improvement include nursing care, communication about medications, pain control, and provision of clear discharge instructions.
14

BUNDLED PAYMENTS FOR CARE IMPROVEMENT INITIATIVE (BUNDLED PAYMENTS INITIATIVE).Aligned payments for services delivered across an episode of care, such as heart
bypass or hip replacement, rather than paying for services separately. Bundled payments will give doctors and hospitals new incentives to coordinate care, improve the quality of care and save money for Medicare.
“Patients don’t get care from just one person – it takes a team, and this initiative will help ensure the team is working together,” said HHS Secretary Kathleen Sebelius. “The Bundled Payments initiative will encourage doctors, nurses and specialists to coordinate care. It is a key part of our efforts to give patients better health, better care, and lower costs.”
Funds a package of services patients receive to treat a specific medical condition during a single hospital stay and/or recovery from that stay – this is known as an episode of care. By bundling payment across providers for multiple services, providers will have a greater incentive to coordinate and ensure continuity of care across settings, resulting in better care for patients. Better coordinated care can reduce unnecessary duplication of services, reduce preventable medical errors, help patients heal without harm, and lower costs.
The Bundled Payments initiative is being launched by the new Center for Medicare and Medicaid Innovation (Innovation Center), which was created by the Affordable Care Act to carry out the critical task of finding new and better ways to provide and pay for health care to a growing population of Medicare and Medicaid beneficiaries.

BUNDLED PAYMENTS FOR CARE IMPROVEMENT INITIATIVE (BUNDLED PAYMENTS INITIATIVE).
“This Bundled Payment initiative responds to the overwhelming calls from the hospital and physician communities for a flexible approach to patient care improvement,” said CMS Administrator Donald Berwick, M.D. “All around the country, many of the leading health care institutions have already implemented these kinds of projects and seen positive results.”
This initiative is based on research and previous demonstration projects that suggest this approach has tremendous potential. For example, a Medicare heart bypass surgery bundled payment demonstration saved the program $42.3 million, or roughly 10 percent of expected costs, and saved patients $7.9 million in coinsurance while improving care and lowering hospital mortality.
“From a patient perspective, bundled payments make sense. You want your doctors to collaborate more closely with your physical therapist, your pharmacist and your family caregivers. But that sort of common sense practice is hard to achieve without a payment system that supports coordination over fragmentation and fosters the kinds of relationships we expect our health care providers to have,” said Dr. Berwick.
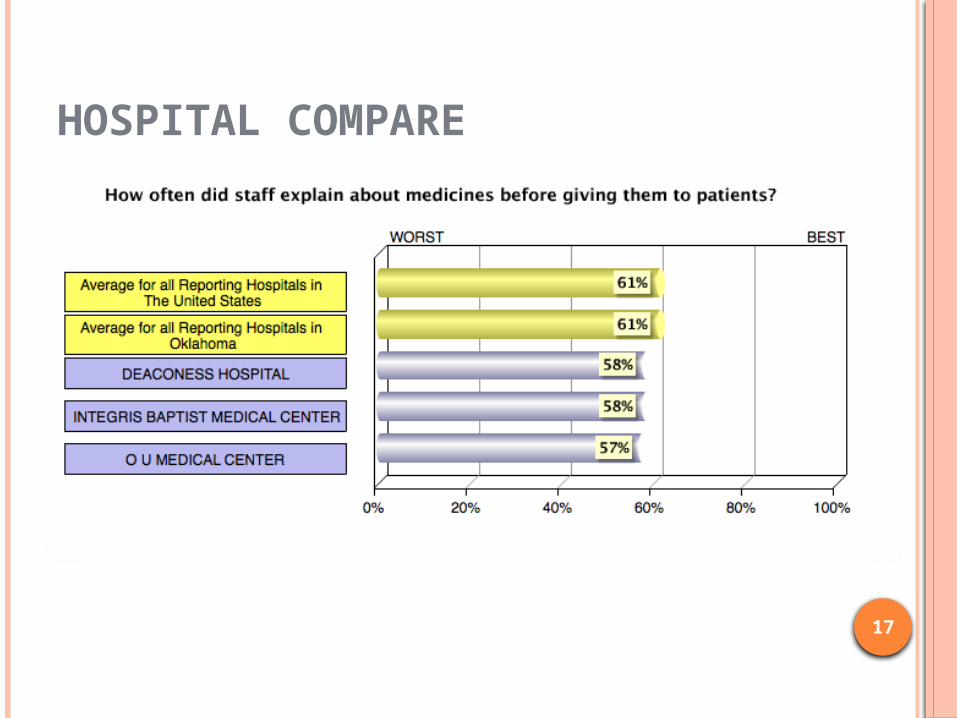
HOSPITAL COMPARE
17

18
A SNAPSHOT OF QUALITYA Gauge for the Future

19
www.leapfroggroup.org
Transparency

AND EVEN MORE TRANSPARENCY!
20

PROVISIONS FOR MEDICATION THERAPY MANAGEMENT
Requirements for Medication Therapy Management Programs (MTMP): Under 423.153(d), a Part D sponsor must have established a MTM program that:
Ensures optimum therapeutic outcomes for targeted beneficiaries through improved medication use
Reduces the risk of adverse events Is developed in cooperation with licensed and practicing pharmacists and
physicians Describes the resources and time required to implement the program if
using outside personnel and establishes the fees for pharmacists or others May be furnished by pharmacists or other qualified providers May distinguish between services in ambulatory and institutional settings Is coordinated with any care management plan established for a targeted
individual under a chronic care improvement program (CCIP) Each Part D Sponsor is required to incorporate a Medication Therapy
Management Program (MTMP) into their plans' benefit structure. Annually, Sponsors must submit a MTMP description to CMS for review and approval. A CMS-approved MTMP is one of several required elements in the development of Sponsor' bids for the upcoming contract year.

COMMUNICATION
Doctors and patients alike say that when they communicate well, healing goes better, and it can even make the difference between life and death. But a national survey of doctors and hospitalized patients fiound that, in reality, effective communication often is sorely lacking.
Only 48% of patients said they were always involved in decisions about their treatment, and 29% of patients didn't know who was in charge of their case while they were in the hospital.
www.usatoday.com/yourlife/health/healthcare/studies/2010-12-06-1Adoctalks06_ST_N.htm

COMMUNICATION
When physicians have more personalized discussions with their patients and encourage them to take a more active role in their health, both doctor and patient have more confidence that they reached a correct diagnosis and a good strategy to improve the patient's health. That approach can help eliminate or reduce unnecessary and costly testing and referrals to specialists
Journal of the American Board of Family Medicine (www.ncbi.nlm.nih.gov/pubmed/21551394).

HEALTHCARE CONSUMERS Reform legislation is attempting to control unruly
medical costs by making it easier for patients with limited health literacy skills to understand results from health screenings and tests for cancer, how to take prescription drugs and make follow-up appointments.
What's more, the Joint Commission started requiring earlier this year that hospitals use plain-language materials and include graphics. They also must "communicate in a manner that meets the patient's oral and written communication needs".
Industry experts and government officials hope that, in addition to reducing readmission rates costs, simple and clear communication will ease the flood of 32 million currently uninsured Americans who will get coverage in 2014 under the reform.
24

ACCESS TO CARE BENEFITS Starting in 2014, most U.S. citizens and legal residents will be
required to obtain health coverage, or pay a penalty. Some exemptions will be granted, for example, for those with religious objections or where insurance would cost more than 8% of their income.
Medicaid will be expanded to cover nearly all individuals under age 65 with incomes up to 133% of the federal poverty level ($14,400 for an individual or $29,300 for a family of four in 2010).
Individuals without access to affordable coverage who purchase coverage through the new insurance Exchanges and have incomes up to 400% of the federal poverty level will be eligible for premium tax credits based on their income.
The law does not require employers to provide health benefits. However, it does impose penalties, in some cases, on larger employers (those with 50 or more workers) that do not provide insurance to their workers or that provide coverage that is unaffordable.
Undocumented immigrants are not eligible to receive financial help from the government to buy health insurance, nor are they eligible for Medicaid or to purchase insurance with their own money in the new Exchanges.

PROVISIONS FOR CARE COORDINATION Crossing the continuum of care

27
Care Coordination
Definition:
Care coordination is a function that helps ensure that the patient’s needs and preferences for health services and information sharing across people, functions, and sites are met over time.
Coordination maximizes the value of services delivered to patients by facilitating beneficial, efficient, safe, and high-quality patient experiences and improved healthcare outcomes.National Quality Forum (NQF) - ENDORSED DEFINITION AND FRAMEWORK FOR MEASURING CARE COORDINATION

NQF CARE COORDINATION STANDARDS
www.qualityforum.org/projects/care_coordination.aspx

SHARED DECISION MAKING
Shared decision-making is a model of patient-centered care that enables and encourages people to play a role in the management of their own health. It operates under the premise that, armed with good information, consumers can and will participate in the medical decision-making process by asking informed questions and expressing personal values and opinions about their conditions and treatment options. This intervention can be implemented by medical groups, but it is typically put in place and financed by health plans.
Shared decision-making is an opportunity for patients and providers to engage in open communication, which allows patients to choose care options that are based on the best available evidence and optimally suit their needs and preferences.

BALANCING COSTS WITH QUALITY!
The White House made clear in a fact sheet on the debt deal, “Any cuts to Medicare would be capped and limited to the provider side.”
The entire U.S. health care system is caught between a budgetary rock and an obligatory hard place. On the demand side, American people are living longer and sicker – judging by the increasing percentage of people who are obese and suffering from chronic diseases. And, in 2014, 15% of the population who are currently uninsured will be added into the health care system. On the budget side, our nation is quickly running out of money to pay health care providers.


No Margin = No Mission.
32

IN A POST-ACA WORLD, THE HEALTHCARE CASE MANAGER IS A CORNERSTONE OF CARE DELIVERY.
How will we accomplish?

CASE MANAGER WILL BE THE "LINCHPIN" OF ACCOUNTABLE CARE SUCCESS
Many "naive policymakers, out-of-touch regulators, inflexible legal experts and physician-leader apparatchiks" contend primary care physicians can manage all the elements of an ACO. Jaan Sidorov, MD, publisher of ACO Watch and The Disease Management Care Blog, disagrees. "Docs don't mind being ultimately responsible, but they have little interest in reviewing, recruiting or educating lists of patients. They are happy to delegate such tasks to case managers. In other words, the case managers will be the linchpin to ACO success." (ACO Watch)

www.cmsa.org/SOP
THE CONTINUUM OF HEALTH CARE
DEFINITION OF A TEAM
On a recent flight, I heard
“Welcome aboard Flight 5322 to Atlanta. To operate your seat belt,
insert the metal tab into the buckle, and pull it tight. It works just like every other seat belt; and, if you don't know
how to operate one, you probably shouldn't be out in public
unsupervised.”

MEMBERS OF THE TEAM
Patient/family/caregiver Physician Health care supportive team Payer Community And…………

38
THE INTEGRATED TEAM Physicians Wellness or Health
Coaches Lab and Radiology
Professionals Rehab Skilled Case
Managers Patient
Pharmacists Specialists Hospitalists Nurses Therapists Behavioral Health Family Caregivers

PATIENT FAMILY CAREGIVERThe most important team members

PHYSICIANS THROUGH EACH TRANSITION OF CAREWorking in Partnership with the Patient in Directing the Team!

ONE FAMILY’S COMMENTS
Specifically we liked the doctor’s attentiveness, curiosity, flexibility, and presence – all qualities of mindfulness.
Can we say that all team members develop and maintain this quality?

PCMH AND ACO’SSome of the Alphabet Soup of ACA
43
NEXT STEPSThe Future as I See It!

IMPORTANT MESSAGE AND VITAL STEP IN ADVANING ALL QUALITY INTIATIVES
View Transitions of
Care As a Process Not An
Event 44

CARE COORDINATION
The Essential Components of Care Coordination include:
Patient engagement
Patient education
Patient empowerment
45

PATIENT ENGAGEMENT
A means for persons to make thoughtful choices on treatments and behaviors associated with getting the most from their own efforts and the healthcare system along with doing their part to ensure affordability if they are to continue to have healthcare at all.
"Actions individuals must take to obtain the greatest benefit from the health care services available to them”
Signifies that a person is involved in a process through which he harmonizes robust information and professional advice with his own needs, preferences and abilities in order to prevent, manage and cure disease.
46

PATIENT EMPOWERMENT
Health care needs to be more inclusive, integrated and collaborative. Specialists working together with primary care physicians to
prescribe the best medical treatment for patients Physicians teaching their patients about new medical
procedures and techniques relevant to their disease state diabetic patients networking over Facebook to learn how they
can better manage their current condition and overall health and wellness.
Collaboration or “team care,” appears to be the direction the medical profession will need to head to address some of the growing complexities of today’s health care system.
Health care knowledge is global but health care delivery is local.
PATIENT EMPOWERMENT
An individual being an active member of his/her disease management or treatment team.
The patient empowerment concept asserts that to be truly healthy, people must bring about changes in their social situations and in the environment that influences their lives, not only in their personal behavior.
The providing of information regarding therapeutic options so that a patient can actively participate in the decision on whether to undergo a diagnostic or therapeutic procedure, or pursue alternatives.
48

PATIENT/FAMILY/CAREGIVER EDUCATION
Does the patient know What’s wrong? What they need to do? Why is it important?
IF not What’s your plan for
Patient/caregiver education Identifying and removing barriers to adherence
Who implements the plan? Who gathers information and outcome information

PATIENT EDUCATION
The process of providing information to a patient on his or her medical condition, treatment regimen, or processes in which he or she becomes involved with healthcare staff (e.g., contact investigation). Information is based on patient’s level of understanding, existing knowledge, and feedback (e.g., body language or questions) he or she provides. (www.cdc.gov)
The process by which health professionals and others impart information to patients that will alter their health behaviors or improve their health status.
The process of informing a patient about a health matter to secure informed consent, patient cooperation, and a high level of patient adherence and persistency.
50

PATIENT EMPOWERMENT AND ENGAGEMENT
Informed decision making
Active participant in treatment decisions and care
Understand how to access care
Knows payment process for receiving care
Maintains a medication list
An opportunity to control their own destiny
Includes targeted education on self-management/monitoring
Appropriate support/caregivers included
Can state all diagnoses, treatment plan and the benefits of
adherence and persistency
Advances patient accountability and responsible
51

ACTIVE PATIENT & FAMILY ENGAGEMENT
Patient’s and family caregivers need resources they can use and understand
Health coaching supports patients and their family caregivers in addressing interaction with the providers and team collaboration
Written directions without any support or coaching are often loss, forgot or not understood
The patient is the expert in his or her own life Understanding the patient’s perspective and
motivation is key to bi-directional communication

53
CHALLENGESThat Impact Effective Transitions of Care
COMPONENTS ESSENTIAL TO EVERY INITIATIVE
“Transitions Of Care According to Nancy”
54

COMMUNICATING MORE EFFECTIVELY TO PREVENT UNSAFE DISCHARGES
Six Steps for oral communication: Slow down and sit down Plain language Pictures Limited information Repeat Teach-back Shame free environment
Provide oral and written information
55

ELEMENTS OF BEST PRACTICE
Medication List/Reconciliation/Adherence Transition Summary at Transition Follow-up Visit – PCP/Specialist Care Plan Coaching with Patient and Family Caregivers Post Transition Call and/or Visit – Determined
by Population Accountability for Sending & Receiving
Communication56

Improving Communication
National Transitions of Care Coalition (NTOCC) Measures Workgroup. Transitions of care measures. 2008.
57
FACILITATING A SAFE TRANSITION
Medication reconciliation at discharge
Comprehensive discharge planning
Post-discharge support (e.g. Pharmacist call, home care.) in specific conditions is essential!
58
Transitional planning

FACILITATING A SAFE TRANSITION
Recognize high-risk nature of discharge process
It is a Team Effort! And, each member of the team is
personally accountability for their individual role in the transition of care process
Actively involve patients early in the discharge process
59
Care Coordination Begins at or before Admission

COORDINATION OF CARE COMPETENCIES
Patient Care Medical Knowledge Professionalism Interpersonal and Communication
skills Practice-based learning and
improvement Systems-based practice
60

COORDINATION OF CARE
The responsibility of EVERY member of the multidisciplinary treatment team.
Patients should be able to answer:• What’s wrong with me?
• What do I need to do about it?
• When do I need to do it?
• How long do I need to do it?
• Why is it important?
• Who will direct my care?61
NTOCC. www.ntocc.org

62
SUCCESS OF THE MULTI-DISCIPLINARY TEAMS
Will depend upon:Nursing, Case Management, Physician and other
Professional disciplines coming together on Collaborative Efforts
Support of PI Teams focus and resource toolsOpen lines of CommunicationActive ListeningConstant striving for improvement and educationActive Participation in other Process Improvement
TeamsSharing knowledge of the Evidence Based
ProtocolsDevelopment and implementation of Shared Tools

63

ENGAGEMENT & MOTIVATIONAL INTERVIEWING: R-U-L-E
R – Resist the temptation to “fix” the patient problem
U – Uncover and understand the patient’s motivation for engaging, working and changing behavior
L – Listen carefully to the patient and try to understand their perspective that may be different than yours
E – Encourage the patient in their ability to self manage adherence to the care plan and change
Four Basic Principals of Motivational Interviewing: R-U-L-E, Glovsky, E., MI Institute, Jan 2011

ELEMENTS OF BEST PRACTICE
Medication List/Reconciliation/Adherence Transition Summary at Transition Follow-up Visit – PCP/Specialist Care Plan Coaching with Patient and Family
Caregivers Post Transition Call and/or Visit –
Determined by Population Accountability for Sending & Receiving
Communication 65

Transitioning The Continuum of Care with Bi-Directional Communication
Pharmacy Employer
PCP/Medical Home
Specialist
PatientTOC CM
Hospital
Community HealthCenter
Health Plan
AdherenceAssessment & Support
Health Promotion
Motivational Advocacy
Prescr
iption
Assessm
ent &
Care
Plan
Motivational InterventionsAdvocate
Assessment
Medication Reconciliation
Care Plan
AdherenceAssessment & SupportCoordination & Care Plan
Non-Adherence
Behavior Health Change
Facilitation
Increase Productivity
LTC
Home Care
Hospice

PATIENT/CLIENT EDUCATION WITHIN THE CARE COORDINATION PLAN
Communication is the Key!
67

THE COMMUNICATION EXCHANGE
What is the easiest way for you to
learn?
Consider health literacy
Explain things clearly in plain language
Focus on key messages and repeat
68

IDENTIFY THE PROBLEM
What is your biggest concern? Can you tell me what was hard for you? Can you tell me what you might change this
time? How do you know you are doing well? Not
doing so well? What “tools or medical supplies” do you use
to help you know how you are doing? What do you do then? What is a typical day in your life?
69

DEVELOPING A COLLABORATIVE PLANAND ESTABLISHING A GOAL
Not this – “It will be okay!” Not this – “What do you need?” Would you consider having a nurse come to
your home to work with you to help you ….. Was there anything that has hard for you to
do or get when you left the hospital before? What is important to you when you go home?
70

AND, MY GOAL FOR BETTER HEALTH IS…
Weight does not increase for 2 weeks I will review my medication list every
morning and evening and take my medications as listed. If I am not able to take them I will call my doctor. The doctor’s name is
I will check my blood sugar two times every day.
I will bring a copy of my discharge information to my doctor visit
71

MODELS

TOC MODELS Care Transitions Intervention - Dr. Eric Coleman
- Transition Coaching -http://www.caretransitions.org
Transitional Care Model - Dr. Mary Naylor - Advanced Nurse Practitioners-http://www.nursing.upenn.edu/media/transitionalcare/Pages/default.aspx
Guided Care - Dr. Chad Boult - Guided Care Nurse -http://www.guidedcare.org
Project RED - Dr. Brian Jack - Boston University Medical Center - Re-engineering Discharges – http://www.bu.edu/fammed/projectred/
Project BOOST - Society of Hospital Medicine –http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/CT_Home.cfm

TOOLS






























