Embed Size (px)
Citation preview
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 1/38
GUILLIAN BAARE
SYNDROME
Mr. JEO THOMAS
1ST M.sc NURSING
SCON

8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 2/38
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 3/38
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 4/38
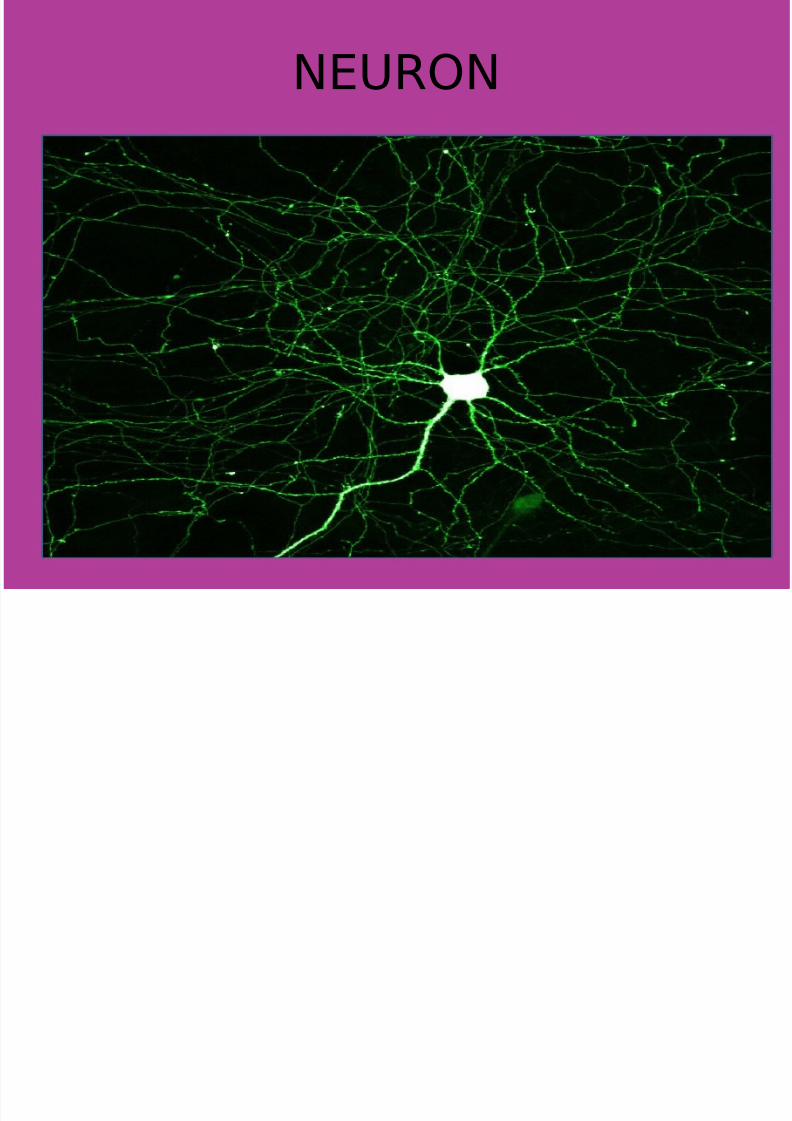
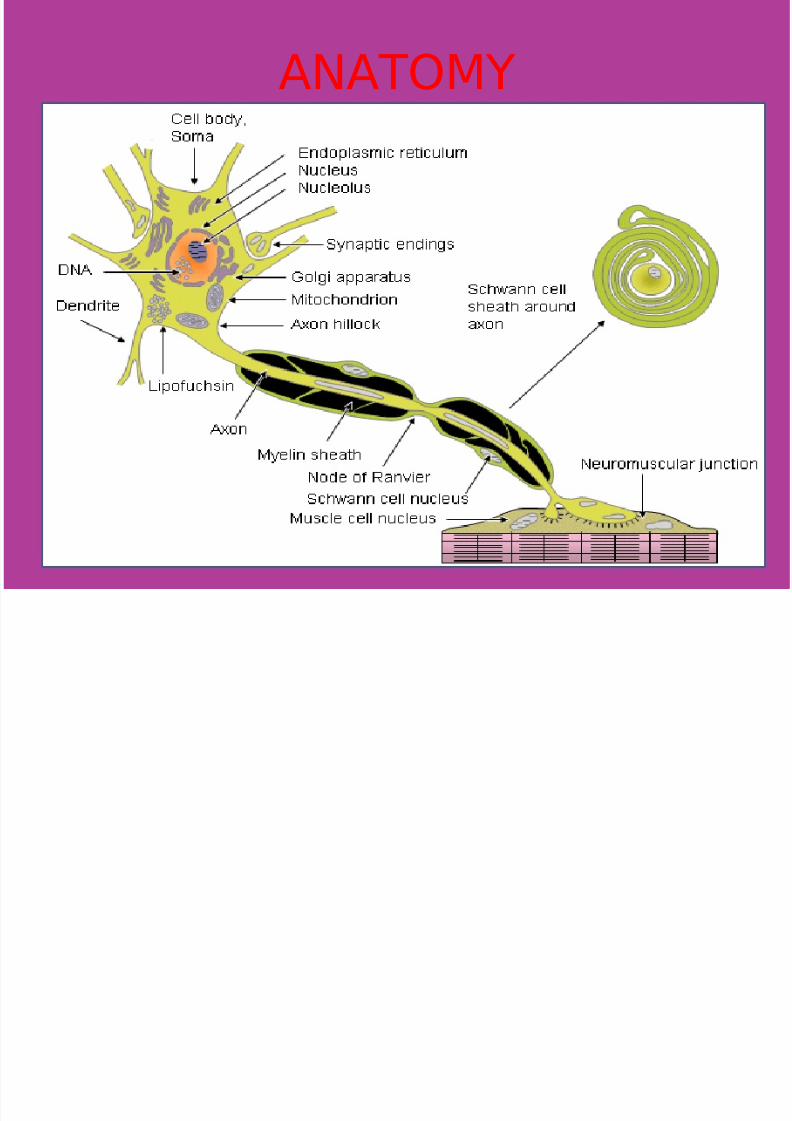
ANATOMY OF NEURON
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 5/38
ANATOMY
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 6/38
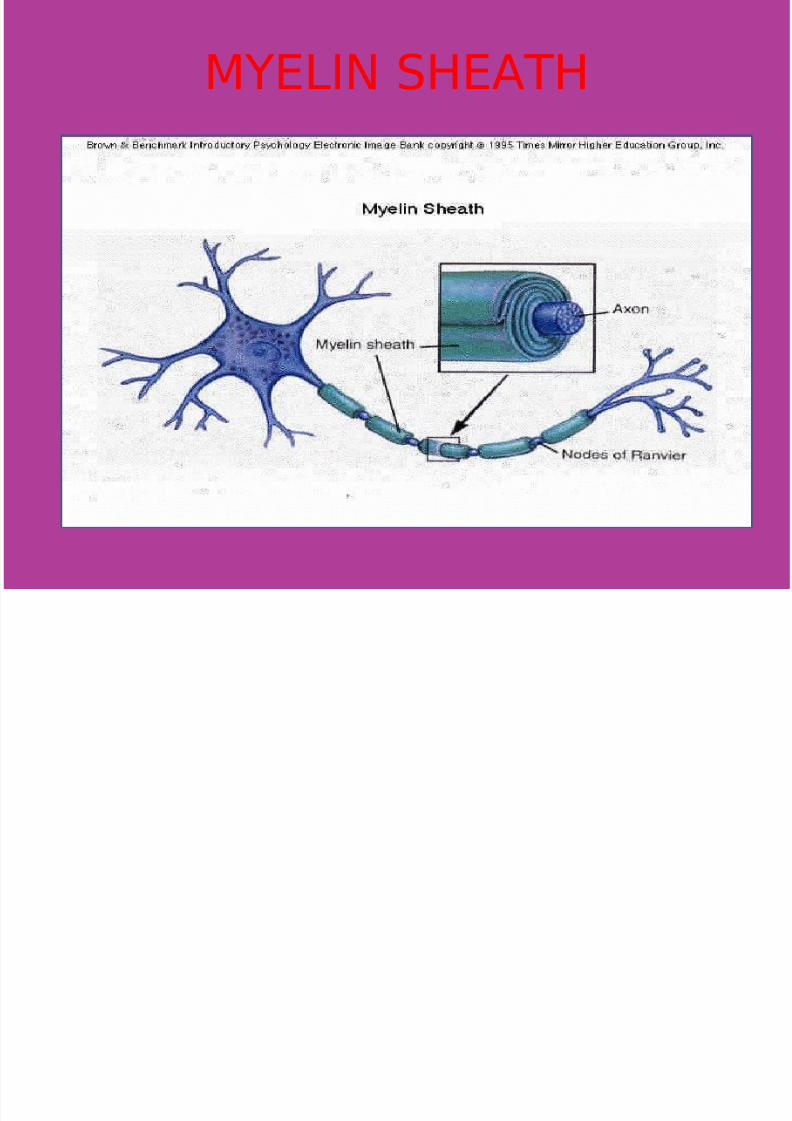
MYELIN SHEATH
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 7/38
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 8/38
DEFINITION
Guillain-Barre syndrome is a rareautoimmune disorder of theperipheral nervous system. GBS isa demyelinating disease, meaningthat segments of myelin arestripped from their insulatingposition around nerves, reducing
the propagation of electricalnerve impulses.This causes loss of reflexes, muscle weakness, andtemporary paralysis (loss of
muscle strength).
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 9/38
DEFINITION
Guillain-Barré syndrome is anautoimmune attack of theperipheral nerve myelin. Theresult is acute, rapid segmentaldemyelination of peripheralnerves and some cranial nerves,producing ascending weakness
with dyskinesia (inability toexecute voluntary movements),hyporeflexia, and paresthesias
(numbness).
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 10/38
INCIDENCE
vThe annual incidence of Guillain-Barréis 0.4-4.0 cases perpopulation of 100,000
vEighty-five percent of patientsrecover with minimal residualsymptoms.
vDeath occurs in 3% to 8% of cases,
resulting from respiratory failure,autonomic dysfunction, sepsis, orpulmonary emboli.
vIt is slightly more common in menthan women, and can affect
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 11/38
ETIOLOGY
•
Guillain-Barre syndrome is anautoimmune disorder (the body'simmune system attacks itself).
• Exactly what triggers Guillain-
Barre syndrome is unknown.
• It often follows a minor infection,usually a lung infection or
gastrointestinal infection.Usually, signs of the originalinfection have disappearedbefore the symptoms of Guillain-
Barre begin
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 12/38
Common cause•
Campylobacter jejuni, abacterium that appears tocause the most commonly
reported infection precedingGBS, is widely prevalent inthe gastrointestinal tracts of many animals, notablycattle and poultry, swine,
sheep, and even in pets
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 13/38
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 14/38
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 15/38
CLASSIFICATIONvAcute inflammatory
demyelinatingpolyneuropathy (AIDP)
vAcute motor axonalneuropathy (AMAN)
vAcute motor sensory axonalneuropathy (AMSAN)
vMiller Fisher syndrome
(MFS)
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 16/38
Acute inflammatory demyelinatingpolyneuropathy (AIDP)
• It is the most common form of GBS,and the term is often usedsynonymously with GBS. It iscaused by an auto-immuneresponse directed againstSchwann cell membranes.
• Most common variant, 85% of cases
• Primarily Motor• Generally preceded by bacterail or
viral infection
• Symptoms generally resolve with
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 17/38
Acute Motor Axonal Neuropathy(AMAN)
• Motor only with early and severerespiratory involvement,primary axonal degeneration
• More prevalent amongst pediatricage groups
• Up to 75% positive for C. jejuni
serology• Characterized by a rapidly
progressive weakness, ensuing
respiratory failure, and good
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 18/38
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 19/38
Miller Fisher Variant
• Triad: opthalmoplegia, sensory ataxia,areflexia
• 5% of all cases
• Patients may also have mild limbweakness, ptosis, facial palsy, orbulbar palsy.
• The ataxia tends to be out of proportionto the degree of sensory loss.
• Recovery generally occurs within 1-3
months
th h i l
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 20/38
pathophysiologyPrecipitating factors:c.jejuni,epsteinbarr
virus
Cellular and humoral immune
mechanisms activates.infectious agents are thought to induce
antibody production against specific
gangliosides and glycolipids, such asGM1 and GD1b, distributed throughoutthe myelin in the peripheral nervoussystem.
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 21/38
The virulence of organism is thought tobe based on the presence of specificantigens in its capsule that are
shared with nerves.
Immune responses directed against thecapsular components produceantibodies that cross-react withmyelin to cause demyelination.
Results in defects in the propagation of electrical nerve impulses, with eventualconduction block and flaccid paralysis. Insome patients with severe disease, asecondary consequence of the severe
inflammation is axonal disruption and loss.

8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 22/38
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 23/38
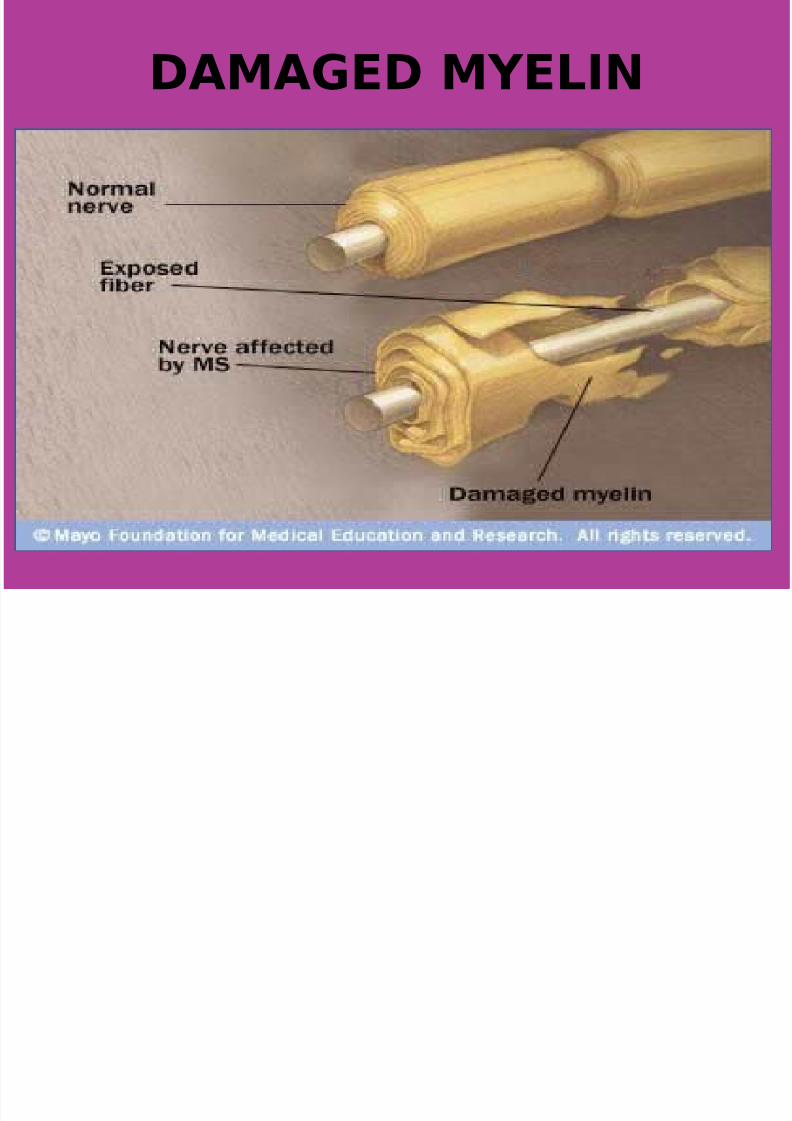
DAMAGED MYELIN
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 24/38
CLINICAL MANIFESTATIONAscending weakness usually
beginning in lower extremities andspreading rapidly to upperextremities and trunk and evenface.
Paresthesia: tingling sensation mayoccur at early stage of disease.
Three phases : Initial phase
Plateau phase
Recovery phase
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 25/38
Weakness
– The classic clinical picture of weakness
is ascending and symmetrical innature. The lower limbs are usuallyinvolved before the upper limbs.Proximal muscles may be involvedearlier than the more distal ones.
Trunk, bulbar, and respiratory musclescan be affected as well.
– Weakness develops acutely andprogresses over days to weeks.
Severity may range from mildweakness to complete tetraplegia withventilatory failure. Peak deficits arereached by 4 weeks after the initialdevelopment of symptoms.The
progression of symptoms beyond that
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 26/38
Sensory changes
–Most patients complain of paresthesias, numbness, orsimilar sensory changes.Sensory symptoms oftenprecede the weakness. Theyare frequently ascending innature and are morepronounced in a distaldistribution.
–
Sensory symptoms are usually
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 27/38
Cranial nerve involvement
– Cranial nerve involvement isobserved in 45-75% of patientswith GBS. Common complaintsmay include the following:
• Facial droop
• Diplopias
• Dysarthria
• Dysphagia
– Facial and oropharyngeal weaknessusually appears after the trunk and limbs are affected.
PAIN
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 28/38
PAIN – Most patients complain of back and leg
pain, often described as aching or
throbbing in nature. The mechanismof pain is thought to be inflamednerve roots. Dysesthesias frequentlyare described as burning, tingling, orshock like sensations and are often
more prevalent in the lowerextremities than in the upperextremities. Other pain syndromes inGBS include the following:
• Myalgic complaints, with cramping andlocal muscle tenderness
• Visceral pain• Pain associated with conditions of
immobility (eg, pressure nerve palsies,decubitus ulcers)
– The intensity of pain on admission
correlates poorly with neurologic
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 29/38
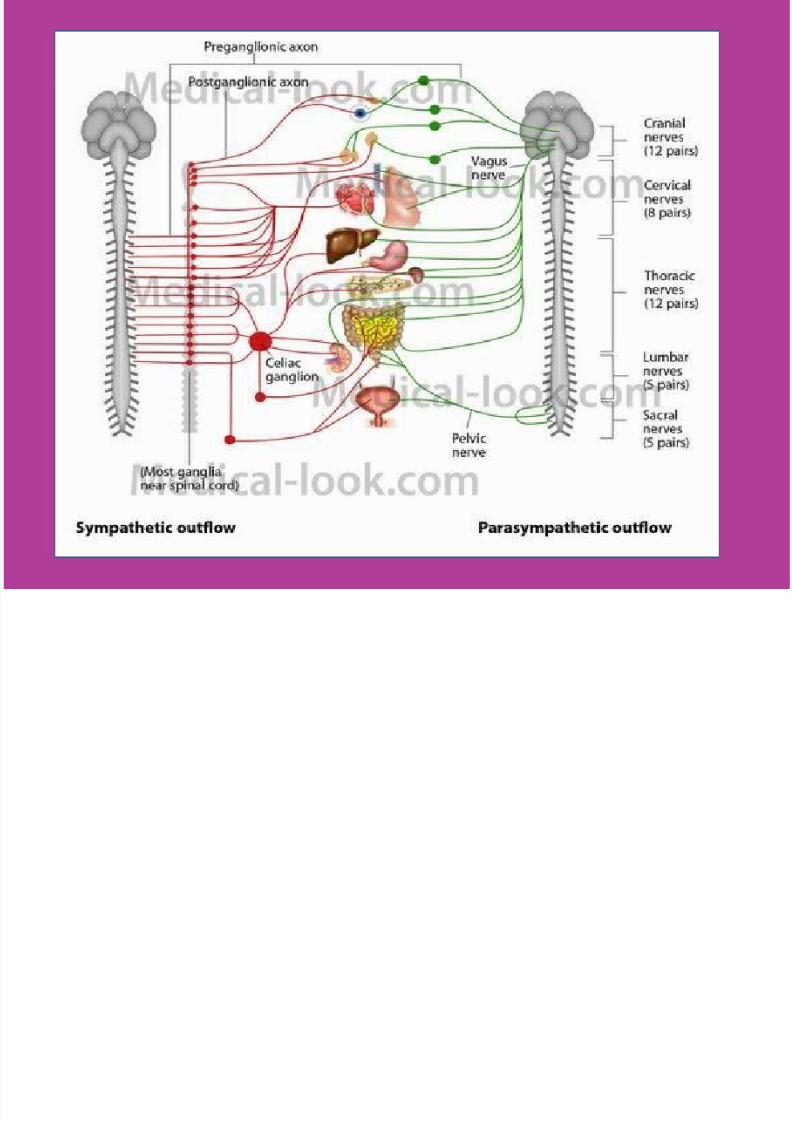
Autonomic changes
– Autonomic nervous systeminvolvement with dysfunction in thesympathetic and parasympatheticsystems can be observed in patientswith GBS.
– Autonomic changes can include thefollowing:
• Tachycardia
• Bradycardia
• Facial flushing
• Paroxysmal hypertension
• Orthostatic hypotension
• Anhidrosis and/or diaphoresis
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 30/38
• Urinary retention and paralytic ileusalso can be observed.
• Dysautonomia is more frequent in
patients with severe weakness andrespiratory failure.
• Autonomic changes rarely persist in
a patient with GBS
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 31/38
Respiratory involvement
40% of patients have respiratory or
oropharyngeal weakness. Typical complaints include the
following:• Dyspnea on exertion
• Shortness of breath
• Difficulty swallowing
• Slurred speech
• Ventilatory failure with requiredrespiratory support is observed inup to one third of patients at some
time during the course of their
v Typical symptoms include:
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 32/38
Typical symptoms include:v Loss of reflexes in the arms and legs
v Muscle weakness or loss of muscle function (paralysis)v In mild cases, there may be no weakness or paralysis
v May begin in the arms and legs at the same time
v May get worse over 24 to 72 hours
v May occur in the nerves of the head only
v May start in the arms and move downward
v May start in the feet and legs and move up to the arms and head
v Numbness,decreased sensation
v Sensation changes
v
Tenderness or muscle pain (may be a cramp-like pain)v Uncoordinated movement
v Additional symptoms may include:
v Blurred vision
v Clumsiness and falling
v Difficulty moving face muscles
v Muscle contractionsv Palpitations (sensation of feeling heartbeat)
v Emergency symptoms (seek immediate medical help):
v Breathing temporarily stops
v Can't take a deep breath
v Difficulty breathing v Difficulty swallowing
COMPLICATION
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 33/38
COMPLICATIONvRespiratory weakness/failure (20-30%
will need intubation at some point
during admission)vAutonomic dysfunction in up to 65%
including: arrythmias, hypotension orhypertension, fluctuating BP, , urinary
retention.vPain in up to 85%: typically back
pain,and musculoskeletal, the straightleg raise test will be positive
vPapilledema (secondary to high CSFprotein)
vDVT
vSIADH (26%)
vAcute Renal Injury (secondary to IVIG TX)
DIAGNOSTIC MANAGEMENT
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 34/38
DIAGNOSTIC MANAGEMENT• HISTORY COLLECTION
• PHYSICAL EXAMINATION• Serum lab tests
• Lumbar Puncture
• Electromyogram (EMG orElectromyography)
• Nerve Conduction Study
(Electroneurograph)• Echocardiogram (ECHO) or
Electrocardiogram (ECG)
•
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 35/38
Medical management
•
Plasmapheresis (PlasmaExchange)
• Intravenous Immunoglobulin(IVIg)
• Medications:Muscle and joint pain can betreated with over-the-counter
analgesics such as aspirin. If necessary, stronger painmedication (e.g., acetaminophenwith hydrocodone) may be
prescribed. Muscle spasms can be
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 36/38
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 37/38
NURSING DIAGNOSES
• Ineffective breathing pattern and
impaired gas exchange related• to rapidly progressive weakness and
impending respiratory• failure•
• Impaired physical mobility related toparalysis• • Imbalanced nutrition, less than body
requirements, related• to inability to swallow• • Impaired verbal communication
related to cranial nerve• dysfunction• • Fear and anxiety related to loss of
control and paralysis
8/14/2019 Guillian Baare Syndrome
http://slidepdf.com/reader/full/guillian-baare-syndrome 38/38
THANK YOU