Embed Size (px)
Citation preview

OSHPD Public OSHPD Public Reporting ProgramReporting Program
Zhongmin Li, Ph.D.Zhongmin Li, Ph.D.
UCD K-30 Methods in UCD K-30 Methods in Clinical ResearchClinical Research
July 26, 2006July 26, 2006

OverviewOverview
• What is OSHPD?What is OSHPD?
• What is CCORP?What is CCORP?
• How the CABG report cards were produced?How the CABG report cards were produced?

What is the Office of Statewide Health Planning What is the Office of Statewide Health Planning and Development (OSHPD)?and Development (OSHPD)?
• Facilities DevelopmentFacilities Development– Seismic safetySeismic safety
– Code complianceCode compliance
• Cal-Mortgage Cal-Mortgage – Facility financingFacility financing
• Workforce and Workforce and Community Community DevelopmentDevelopment
– Health professions Health professions trainingtraining
– Nursing initiativeNursing initiative
• Healthcare dataHealthcare data– PDD, utilization, financialPDD, utilization, financial– Inpatient, ED and ASCInpatient, ED and ASC
• Healthcare Quality Healthcare Quality and Analysis Division and Analysis Division
– Hospital outcome reports – Hospital outcome reports – (HOC)(HOC)
– Data dissemination - HIRCData dissemination - HIRC

Healthcare Outcomes Center (HOC)Healthcare Outcomes Center (HOC)
• 2 Programs within HOC: 2 Programs within HOC: – Clinical Data (Heart bypass surgery & ICU Clinical Data (Heart bypass surgery & ICU
outcomes)outcomes)
– Patient Discharge Data (heart attack, pneumonia)Patient Discharge Data (heart attack, pneumonia)
• 12 professional/administrative staff with 3 Senior 12 professional/administrative staff with 3 Senior Ph.D.-level research scientistsPh.D.-level research scientists
• Contracts with University of California researchersContracts with University of California researchers

OSHPD’s Outcome ProgramsOSHPD’s Outcome Programs
• Coronary Artery Bypass Coronary Artery Bypass Graft (CABG) Surgery Graft (CABG) Surgery (2006 – hospitals and (2006 – hospitals and surgeons)surgeons)
• Intensive Care Outcomes Intensive Care Outcomes (Final study and recc.-(Final study and recc.-2005)2005)
• Acute Myocardial Acute Myocardial Infarction (2002)Infarction (2002)
• Community-Acquired Community-Acquired Pneumonia (2004)Pneumonia (2004)
• Maternal Outcomes (2006)Maternal Outcomes (2006)
• Hip Fracture surgery Hip Fracture surgery (2006)(2006)
Studies Using Studies Using Clinical DataClinical Data
Studies Using Patient Studies Using Patient Discharge DataDischarge Data
Gold = Reports that have been or will shortly be releasedGold = Reports that have been or will shortly be released

OSHPD Reports and Report CardsOSHPD Reports and Report Cards

What is the California CABG Outcomes Reporting What is the California CABG Outcomes Reporting Program (CCORP)?Program (CCORP)?
• Started as voluntary program in 1995 by OSHPD & Started as voluntary program in 1995 by OSHPD & PBGHPBGH
• Mandatory data reporting for all Mandatory data reporting for all Coronary Artery Coronary Artery Bypass Graft Bypass Graft ((CABGCABG) surgery) surgery
• Risk-adjusted operative mortality reported Risk-adjusted operative mortality reported publicly reported for:publicly reported for:
– Hospitals (annually starting 2003 data)Hospitals (annually starting 2003 data)– Surgeons (bi-annually starting 2003-04 data) Surgeons (bi-annually starting 2003-04 data)
• A Clinical Advisory Panel of heart surgeons, A Clinical Advisory Panel of heart surgeons, consumers, cardiologists, and university consumers, cardiologists, and university researchersresearchers

What is CCORP (Cont’d)?What is CCORP (Cont’d)?
• Clinical risk-adjustment to account for differences Clinical risk-adjustment to account for differences in patient severity of illness (case-mix)in patient severity of illness (case-mix)
• Yearly patient medical records audit to ensure Yearly patient medical records audit to ensure data integritydata integrity
• First data year: Jan-Dec 2003, received from First data year: Jan-Dec 2003, received from 121 121 hospitalshospitals
• Approximately Approximately 300 California surgeons300 California surgeons
• UCDMC has been participating since 1997UCDMC has been participating since 1997

Rationale for CCORPRationale for CCORP
• Senate Bill 680 (Figueroa, Statutes of 2001) Senate Bill 680 (Figueroa, Statutes of 2001)
• CABG is one of the most expensive hospital surgeries and CABG is one of the most expensive hospital surgeries and ranks among top 10 procedures for volume and mortality rateranks among top 10 procedures for volume and mortality rate
• Limitations of the voluntary OSHPD/PBGH programLimitations of the voluntary OSHPD/PBGH program• Comparative quality information informs:Comparative quality information informs:
– Consumer choiceConsumer choice– Healthcare purchasingHealthcare purchasing– Quality improvement by physicians and hospitalsQuality improvement by physicians and hospitals
• Salience of surgeon-level outcomes Salience of surgeon-level outcomes

CCORP Clinical Advisory Panel (CAP) MembersCCORP Clinical Advisory Panel (CAP) Members
• Robert Brook, M.D. (Chair) Robert Brook, M.D. (Chair) RAND and UCLARAND and UCLA
• Andrew Bindman, M.D. Andrew Bindman, M.D. UCSF and S.F. GeneralUCSF and S.F. General
• Ralph Brindis, M.D.Ralph Brindis, M.D.Kaiser Northern California Kaiser Northern California
• Cheryl Damberg, Ph.D. Cheryl Damberg, Ph.D. Pacific Business Group Pacific Business Group on Healthon Health
• Timothy Denton, M.D. Timothy Denton, M.D. Cedars SinaiCedars Sinai
• Coyness Ennix, M.D.Coyness Ennix, M.D.Alta Bates Medical CenterAlta Bates Medical Center
• Keith Flachsbart, M.D. Keith Flachsbart, M.D. Kaiser San FranciscoKaiser San Francisco
• Fred Grover, M.D.Fred Grover, M.D.University of Colorado, STSUniversity of Colorado, STS
• James MacMillan, M.D. James MacMillan, M.D. Valley Heart Surgeons, Valley Heart Surgeons, ModestoModesto

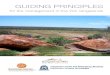
Unadjusted Isolated CABG Inpatient Mortality Unadjusted Isolated CABG Inpatient Mortality Rates for CA and Other States (1996-2004)Rates for CA and Other States (1996-2004)
NOTE: MA = 30-day mortalityNOTE: MA = 30-day mortality
3.09%
2.95% 2.93%2.86%
2.95%
2.71%
2.34%
2.63%
2.44%
2.22%2.15%
2.24%
2.32%
2.18%
2.27%
2.40%
2.00% 2.00%
3.37% 3.37%
2.60%
2.22%
2.01%
1.80%
2.19%
2.89%
1.50%
1.75%
2.00%
2.25%
2.50%
2.75%
3.00%
3.25%
3.50%
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Year
Ob
serv
ed
Mo
rtali
ty R
ate
California New YorkPennsylvaniaNew JerseyMassachusetts

Hospital Distribution of Unadjusted Hospital Distribution of Unadjusted In-Hospital Mortality Rate: Avg. = 2.4% (2003)In-Hospital Mortality Rate: Avg. = 2.4% (2003)
0
2
4
6
8
10
12
0.00 0.25 0.50 0.75 1.00 1.25 1.50 1.75 2.00 2.25 2.50 2.75 3.00 3.25 3.50 3.75 4.00 4.25 4.50 4.75 5.00 5.25 5.50 5.75 6.0+
Unadjusted Mortality % Midpoint
Nu
mb
er
of
Ho
sp
itals

Hospital Distribution of Risk Adjusted Hospital Distribution of Risk Adjusted Operative Mortality: Avg. = 2.9% (2003)Operative Mortality: Avg. = 2.9% (2003)
0
2
4
6
8
10
12
0.00
0.25
0.50
0.75
1.00
1.25
1.50
1.75
2.00
2.25
2.50
2.75
3.00
3.25
3.50
3.75
4.00
4.25
4.50
4.75
5.00
5.25
5.50
5.75
6.00
6.25
6.50
6.75
7.0+
Risk Adjusted Mortality % Midpoint
Nu
mb
er o
f H
osp
ital
s

CCORP 2003 Hospital Performance Ratings for CCORP 2003 Hospital Performance Ratings for Operative MortalityOperative Mortality
Total 121 100.0%Total 121 100.0%
Significantly Better 4 3.3%Significantly Better 4 3.3%
No Difference 113 93.4%No Difference 113 93.4%
Significantly Worse 4 3.3%Significantly Worse 4 3.3%
No. of Hospitals PercentNo. of Hospitals Percent
2003 CCORP public report was released in March 20062003 CCORP public report was released in March 2006
http://www.oshpd.state.ca.ushttp://www.oshpd.state.ca.us

How CABG Report Cards Were Produced? How CABG Report Cards Were Produced?
Data CollectionData Collection• SourceSource• Data elements (59; not exact same as STS) Data elements (59; not exact same as STS) • Hospital reporting toolsHospital reporting tools• Acceptance criteriaAcceptance criteria• Deadline and ExtensionDeadline and Extension• OSHPD staff supportOSHPD staff support
– Data abstraction manualData abstraction manual– Training of codersTraining of coders

How CABG Public Report Was Produced (Cont’d)?How CABG Public Report Was Produced (Cont’d)?
Data Cleaning and ValidationData Cleaning and Validation• Data quality report (DQR) Data quality report (DQR) • Data Linkage/discrepancy report (DDR)Data Linkage/discrepancy report (DDR)• On-site data auditOn-site data audit
– Audit strategyAudit strategy– Sample selectionSample selection
“ “As good as you can get”?As good as you can get”?

Risk AdjustmentRisk Adjustment
Central to the report cardsCentral to the report cards• Why Isolated CABGs onlyWhy Isolated CABGs only• Inpatient vs. operative mortalityInpatient vs. operative mortality• Risk modelRisk model
– DevelopmentDevelopment– ValidationValidation– Testing (c-statistics; calibration)Testing (c-statistics; calibration)– CAP approvalCAP approval
• Identification of quality outliers Identification of quality outliers – 95%CI95%CI– Exact Poisson ProbabilityExact Poisson Probability

Major Risk FactorsMajor Risk Factors
• Demographic (Age/Gender/Race/BMI)Demographic (Age/Gender/Race/BMI)• Operative statusOperative status• Pre-operative comobidities Pre-operative comobidities
(Creatinine/Dialysis/Diabetes/CVD/PVD/CLD/Hypertensio(Creatinine/Dialysis/Diabetes/CVD/PVD/CLD/Hypertension/Hepatic failure, etc.)n/Hepatic failure, etc.)
• Cardiac (Arrhythmia type/MI timing/CHF/Shock)Cardiac (Arrhythmia type/MI timing/CHF/Shock)• Previous intervention (Prior CABG/PCI)Previous intervention (Prior CABG/PCI)• Hemodynamic status (EF/Left main/# of diseased Hemodynamic status (EF/Left main/# of diseased
vessels/Mitral insufficiency)vessels/Mitral insufficiency)

Risk Adjustment ModelRisk Adjustment Model
• Expected rate = Intercept + X*B, whereExpected rate = Intercept + X*B, where– B-Coefficients estimated on CCORP data using logistic B-Coefficients estimated on CCORP data using logistic
regression (PROC LOGISTIC in SAS)regression (PROC LOGISTIC in SAS)– X includes age, gender and each of risk factorsX includes age, gender and each of risk factors
• Risk-adjusted rate=Risk-adjusted rate= Observed rate*Observed rate* (Population rate/Expected rate)(Population rate/Expected rate)
• Alternative formula:Alternative formula: Risk-adjusted rate=Risk-adjusted rate= Population rate*Population rate* (Observed rate/Expected rate)(Observed rate/Expected rate)

Risk Adjustment ExampleRisk Adjustment Example
• Risk adjustment “adjusts” the observed rate of Hospital Risk adjustment “adjusts” the observed rate of Hospital A to account for differences between the case-mix of A to account for differences between the case-mix of Hospital A and the reference populationHospital A and the reference population
• The larger the difference between the rate was The larger the difference between the rate was expected for Hospital A and the population rate, the expected for Hospital A and the population rate, the larger the adjustmentlarger the adjustment
• If a hospital has the same case-mix as the reference If a hospital has the same case-mix as the reference population, then no adjustment is madepopulation, then no adjustment is made

Risk Adjustment ExampleRisk Adjustment Example
• Population rate > Hospital A Expected ratePopulation rate > Hospital A Expected rate– Hospital A has a less severe case-mix than the populationHospital A has a less severe case-mix than the population– ““adjustment factor” is >1adjustment factor” is >1– Risk Adjusted rate is higher then observed rateRisk Adjusted rate is higher then observed rate– If hospital A had the same case-mix as the population, we If hospital A had the same case-mix as the population, we
would expect their observed rate to be higherwould expect their observed rate to be higher

Risk Adjustment ExampleRisk Adjustment Example
• Population rate < Hospital A Expected ratePopulation rate < Hospital A Expected rate– Hospital A has a more severe case-mix than the Hospital A has a more severe case-mix than the
populationpopulation– ““adjustment factor” is <1adjustment factor” is <1– Risk Adjusted rate is lower then observed rateRisk Adjusted rate is lower then observed rate– If hospital A had the same case-mix as the population, we If hospital A had the same case-mix as the population, we
would expect their observed rate to be lowerwould expect their observed rate to be lower

Report Review and Appeal ProcessReport Review and Appeal Process
Prior to public release:Prior to public release:
• Hospital review (60-day)Hospital review (60-day)• Surgeon review (30-day)Surgeon review (30-day)• Surgeon can appeal forSurgeon can appeal for
– Flawed dataFlawed data– Flawed risk adjustmentFlawed risk adjustment
• 11stst surgeon level report: Winter 2006 surgeon level report: Winter 2006

What’s Next for CCORP?: NQF National Voluntary What’s Next for CCORP?: NQF National Voluntary Cardiac Surgical MeasuresCardiac Surgical Measures
Gold = currently collected by CCORP or will be collected in 2006Gold = currently collected by CCORP or will be collected in 2006
1. Participation in a systematic database for cardiac surgery1. Participation in a systematic database for cardiac surgery2. Surgical volume for isolated CABG surgery, valve surgery, and 2. Surgical volume for isolated CABG surgery, valve surgery, and
CABG + valve surgeryCABG + valve surgery3. Timing of antibiotic administration for cardiac surgery patients3. Timing of antibiotic administration for cardiac surgery patients4. Selection of antibiotic administration for cardiac surgery patients4. Selection of antibiotic administration for cardiac surgery patients5. Pre-operative beta blockade5. Pre-operative beta blockade6. Use of internal mammary artery6. Use of internal mammary artery7. Duration of prophylaxis for cardiac surgery patients7. Duration of prophylaxis for cardiac surgery patients8. Prolonged intubation8. Prolonged intubation9. Deep sternal wound infection rate9. Deep sternal wound infection rate10. Stroke/cerebrovascular accident10. Stroke/cerebrovascular accident11. Post-operative renal insufficiency11. Post-operative renal insufficiency

NQF National Voluntary Cardiac Surgical Measures NQF National Voluntary Cardiac Surgical Measures (Cont’d)(Cont’d)
12. Surgical re-exploration12. Surgical re-exploration
13. Anti-platelet medications at discharge13. Anti-platelet medications at discharge
14. Beta blockade at discharge14. Beta blockade at discharge
15. Anti-lipid treatment at discharge15. Anti-lipid treatment at discharge
16. Risk-adjusted inpatient operative mortality for CABG16. Risk-adjusted inpatient operative mortality for CABG
17. Risk-adjusted operative mortality for CABG17. Risk-adjusted operative mortality for CABG18. Risk-adjusted operative mortality for AVR18. Risk-adjusted operative mortality for AVR19. Risk-adjusted operative mortality for MVR19. Risk-adjusted operative mortality for MVR20. Risk-adjusted operative mortality for MVR+CABG20. Risk-adjusted operative mortality for MVR+CABG21. Risk-adjusted operative mortality for AVR+CABG21. Risk-adjusted operative mortality for AVR+CABG

IMA Usage Rates as a Reportable Process Measure of IMA Usage Rates as a Reportable Process Measure of QualityQuality
Internal Mammary Artery GraftInternal Mammary Artery Graft• ““Standard” conduit for CABGsStandard” conduit for CABGs• Supported by extensive clinical trials and researchSupported by extensive clinical trials and research• Priority research area of performance - NQFPriority research area of performance - NQF• Process of Care element - STSProcess of Care element - STS• Reported by “Leap Frog” GroupReported by “Leap Frog” Group• IMA data and clinical info. available - CCORP IMA data and clinical info. available - CCORP

Hospital Variation in Left Internal Mammary Artery Hospital Variation in Left Internal Mammary Artery (LIMA) Use: CCORP 2003(LIMA) Use: CCORP 2003
Percent LIMA Use*Percent LIMA Use*
<60<60 --
60-7460-74 --
75-8475-84 --
85-9485-94 --
9595 --
Avg. LIMA Use: 89.1% Avg. LIMA Use: 89.1% --
* Rates are after exclusions for * Rates are after exclusions for certain patient subgroupscertain patient subgroups
Number of Hospitals (%)Number of Hospitals (%)
1 (1%)1 (1%)
11 (9%)11 (9%)
17 (14%)17 (14%)
48 (40%)48 (40%)
44 (36%)44 (36%)
121 total hospitals121 total hospitals
*UCDMC - 92.5%*UCDMC - 92.5%

CPB Used vs. OPCABGCPB Used vs. OPCABG
Operative MortalityOperative Mortality
Off Pump CABGsOff Pump CABGs
9,025 (22.3%)9,025 (22.3%) 2.17% 2.17%
On Pump CABGsOn Pump CABGs
31,380 (77.7%)31,380 (77.7%) 3.36%3.36%
• UCDMC - < 2%UCDMC - < 2%

How Are Hospital CABG Report Results Used?How Are Hospital CABG Report Results Used?
• Hospital tiered networks: Hospital tiered networks: Blue Cross Cardiac Blue Cross Cardiac “Centers of Expertise” and Blue Shield “Cardiac “Centers of Expertise” and Blue Shield “Cardiac Quality Initiative” Quality Initiative”
• Private Healthcare data providers such as SubimoPrivate Healthcare data providers such as Subimo• Purchaser coalitions such as Leapfrog, PBGH Purchaser coalitions such as Leapfrog, PBGH
(Healthscope consumer website)(Healthscope consumer website)• Public Access through OSHPD website:Public Access through OSHPD website:http://www.oshpd.state.ca.us/HQAD/Outcomes/index.htmhttp://www.oshpd.state.ca.us/HQAD/Outcomes/index.htm
• CHARTCHART• Hospital PromotionHospital Promotion

QuestionsQuestions
• OSHPD web site (OSHPD web site (www.oshpd.ca.gov))• Contact HIRC at (916) 322-2814 to obtain copy Contact HIRC at (916) 322-2814 to obtain copy
of the reportof the report