Embed Size (px)
Citation preview
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Guide to Musculoskeletal
Injections With Ultrasound

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
New York
Guide to Musculoskeletal
Injections With Ultrasound
Editors Mohammad Agha, MD, RMSK
Assistant Professor of Physical Medicine and Rehabilitation Assistant Professor of Clinical Orthopaedic Surgery
Department of Physical Medicine and Rehabilitation Department of Orthopaedic Surgery
University of Missouri–ColumbiaColumbia, Missouri
Douglas Murphy, MD, RMSKAssociate Professor of Physical Medicine and Rehabilitation
Department of Physical Medicine and RehabilitationVirginia Commonwealth University School of Medicine
Richmond, Virginia

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Visit our website at www.demosmedical.com
ISBN: 9781620700662e-book ISBN: 9781617052330
Acquisitions Editor: Beth BarryCompositor: diacriTech, Chennai
© 2016 Demos Medical Publishing, LLC. All rights reserved. This book is protected by copyright. No part of it may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the publisher.
Medicine is an ever-changing science. Research and clinical experience are continually expanding our knowledge, in particular our understanding of proper treatment and drug therapy. The authors, editors, and publisher have made every effort to ensure that all information in this book is in accordance with the state of knowledge at the time of production of the book. Nevertheless, the authors, editors, and publisher are not responsible for errors or omissions or for any consequences from application of the information in this book and make no warranty, expressed or implied, with respect to the contents of the publication. Every reader should examine carefully the package inserts accompanying each drug and should carefully check whether the dosage schedules mentioned therein or the contraindications stated by the manufacturer differ from the statements made in this book. Such examination is particularly important with drugs that are either rarely used or have been newly released on the market.
Library of Congress Cataloging-in-Publication DataGuide to musculoskeletal injections with ultrasound / editors, Mohammad Agha, Douglas Murphy. pages cm Includes bibliographical references and index. ISBN 978-1-62070-066-2—9781617052330 (e-book) 1. Musculoskeletal system—Ultrasonic imaging. 2. Injections, Intramuscular. I. Agha, Mohammad, editor. II. Murphy, Douglas (Douglas P.) editor. RC925.7.G84 2015 616.7’07548—dc23 2015015029
Special discounts on bulk quantities of Demos Medical Publishing books are available to corporations, professional associations, pharmaceutical companies, health care organizations, and other qualifying groups. For details, please contact:
Special Sales DepartmentDemos Medical Publishing, LLC11 West 42nd Street, 15th FloorNew York, NY 10036Phone: 800-532-8663 or 212-683-0072Fax: 212-941-7842E-mail: [email protected]
Printed in the United States of America by Courier.15 16 17 18 / 5 4 3 2 1

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
To my mother, Shamim Agha, who sets the example of the person I want to be—MTA
To Paul D. Murphy, MD and Andrea Murphy—DM

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Contents
Contributors xiForeword David X. Cifu, MD xvPreface xviiAcknowledgments xix
Chapter 1. Essentials of Musculoskeletal Ultrasound 1Mohammad Agha
Chapter 2. Shoulder Injections 15Michael P. Schaefer and Victor Foorsov
Subacromial/Subdeltoid Bursa 16Biceps Tendon Sheath (Biceps—Long Head) 19Acromioclavicular Joint 23Glenohumeral Joint 26
Chapter 3. Elbow Injections 33Christopher Wolf, Brian Toedebusch, and Peter Dawson
Common Extensor Tendon 34Common Flexor Tendon 36Olecranon Bursa Injection 38Ulnar Nerve Injection (Below Cubital Tunnel) 40Pronator Teres Syndrome (Median Nerve) 42Intra-Articular Elbow Injection 44
Chapter 4. Wrist and Hand Injections 47P. Troy Henning
Carpal Tunnel Injection 48Cubital Tunnel Injection 51De Quervain’s Tenosynovitis 54Extensor Carpi Ulnaris Tenosynovitis 58Intersection Syndrome 62Carpometacarpal Joint Injection 65Trigger Finger/Thumb 69
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
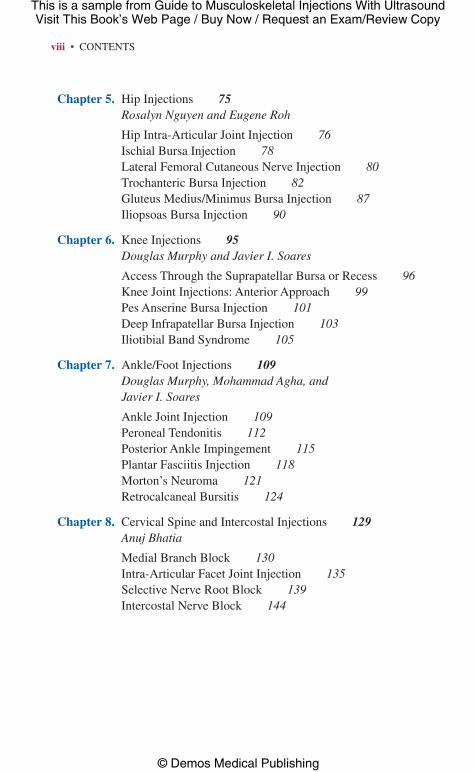
Chapter 5. Hip Injections 75Rosalyn Nguyen and Eugene Roh
Hip Intra-Articular Joint Injection 76Ischial Bursa Injection 78Lateral Femoral Cutaneous Nerve Injection 80Trochanteric Bursa Injection 82Gluteus Medius/Minimus Bursa Injection 87Iliopsoas Bursa Injection 90
Chapter 6. Knee Injections 95Douglas Murphy and Javier I. Soares
Access Through the Suprapatellar Bursa or Recess 96Knee Joint Injections: Anterior Approach 99Pes Anserine Bursa Injection 101Deep Infrapatellar Bursa Injection 103Iliotibial Band Syndrome 105
Chapter 7. Ankle/Foot Injections 109Douglas Murphy, Mohammad Agha, and Javier I. Soares
Ankle Joint Injection 109Peroneal Tendonitis 112Posterior Ankle Impingement 115Plantar Fasciitis Injection 118Morton’s Neuroma 121Retrocalcaneal Bursitis 124
Chapter 8. Cervical Spine and Intercostal Injections 129Anuj Bhatia
Medial Branch Block 130Intra-Articular Facet Joint Injection 135Selective Nerve Root Block 139Intercostal Nerve Block 144
viii • CONTENTS
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
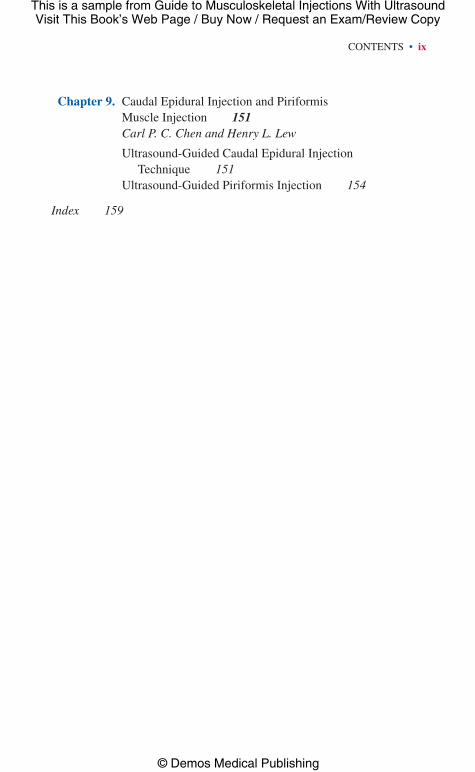
Chapter 9. Caudal Epidural Injection and Piriformis Muscle Injection 151Carl P. C. Chen and Henry L. Lew
Ultrasound-Guided Caudal Epidural Injection Technique 151
Ultrasound-Guided Piriformis Injection 154
Index 159
CONTENTS • ix

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Contributors
Mohammad Agha, MD, RMSKAssistant Professor of Physical Medicine and Rehabilitation Assistant Professor of Clinical Orthopaedic Surgery Department of Physical Medicine and Rehabilitation Department of Orthopaedic Surgery University of Missouri–ColumbiaColumbia, Missouri
Anuj Bhatia, MBBS, DNB, MD, FRCA, MNAMS, FFPMRCA, FIPP, FRCPC, EDRA, CIPSAssistant ProfessorDepartment of Anesthesia and Pain ManagementUniversity of Toronto;Department of Anesthesia and Pain ManagementToronto Western HospitalToronto, Ontario, Canada
Carl P. C. Chen, MD, PhDAssociate Professor/DirectorDepartment of Physical Medicine and RehabilitationChang Gung Memorial HospitalTaipei, Taiwan
Peter Dawson, MDResident PhysicianDepartment of Physical Medicine and RehabilitationUniversity of Missouri–ColumbiaColumbia, Missouri

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
xii • CONTRIBUTORS
Victor Foorsov, MDResidentDepartment of Physical Medicine and RehabilitationCase Western Reserve University/MetroHealth Medical CenterCleveland, Ohio
P. Troy Henning, DOAssistant ProfessorDepartment of Physical Medicine and RehabilitationUniversity of MichiganAnn Arbor, Michigan
Henry L. Lew, MD, PhDProfessorJohn A. Burns School of Medicine University of Hawaii at Ma-noa Honolulu, Hawaii;ProfessorDepartment of Physical Medicine and RehabilitationVirginia Commonwealth University School of MedicineRichmond, Virginia
Douglas Murphy, MD, RMSKAssociate Professor Department of Physical Medicine and RehabilitationVirginia Commonwealth University School of MedicineRichmond, Virginia
Rosalyn Nguyen, MDAssistant ProfessorSports Medicine, Physical Medicine and RehabilitationBaylor College of MedicineHouston, Texas

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
CONTRIBUTORS • xiii
Eugene Roh, MDClinical Assistant ProfessorPhysical Medicine and Rehabilitation Department of OrthopaedicsStanford UniversityRedwood City, California
Michael P. Schaefer, MD, RMSKDirector of Musculoskeletal Physical Medicine and RehabilitationDepartment of Physical Medicine and Rehabilitation and Orthopaedic and
Rheumatologic InstituteCleveland Clinic FoundationCleveland, Ohio
Javier I. Soares, MDPolytrauma and Amputee/MSK Rehab Fellow Physician Department of Physical Medicine and Rehabilitation Hunter Holmes McGuire VA Medical Center Richmond, Virginia
Brian Toedebusch, MDResident PhysicianDepartment of Physical Medicine and RehabilitationUniversity of Missouri–ColumbiaColumbia, Missouri
Christopher Wolf, DO, FAAPMRAssistant ProfessorDepartment of Physical Medicine and RehabilitationUniversity of Missouri–ColumbiaColumbia, Missouri

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Foreword
The Guide to Musculoskeletal Injections With Ultrasound is a must for clinicians. For too long and in too many studies, we have known that per-forming injections without guidance results in misplaced and poorly placed treatments and less than optimal results. Given the virtual explosion in the number and types of clinicians using therapeutic injections as an adjunct in the management of musculoskeletal medicine, this cutting-edge manual will quickly fill a vital niche in the clinic. While it can also serve as an excellent teaching tool for academics, it is first and foremost a hands-on tool for the practitioner. Finally, an easy-to-use, illustrated guide is here that allows clinicians to take advantage of ultrasound (US) technology to accurately and efficiently deliver injectate to where it can be most effec-tive. Drs. Agha and Murphy offer a practical approach to using diagnos-tic US to guide therapeutic injections. From the clear and succinct text to the illustrative photographs, this guide offers readers both a better under-standing of US technology and the functional anatomy it reveals. Years of experience and thousands of accurate injections went into the creation of this text, and readers will be able to quickly leverage all this expertise into their day-to-day practice. This guide will serve to accurately answer a key therapeutic question: Am I in the right spot? Given the challenges and complexities of musculoskeletal medicine, clarifying yet another element of the therapeutic approach is invaluable. I would advocate keeping a copy of Guide to Musculoskeletal Injections With Ultrasound in every clinic room in your offices.
David X. Cifu, MDChairman and Herman J. Flax, MD Professor
Department of Physical Medicine and RehabilitationFounding Director, Center for Rehabilitation Sciences and Engineering
Virginia Commonwealth University;National Director for Physical Medicine and Rehabilitation Services
Department of Veterans AffairsRichmond, Virginia

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Preface
As an attending physician at an academic medical center, I frequently have residents and fellows rotating through my clinics to gain exposure to musculoskeletal ultrasound (US). Most of them want to learn how to do the “textbook” injections under US guidance. Specifically, they were looking for a book that could both help the beginner transition to an intermediate level and also provide the information in a digestible format they could readily use in clinic. With this book, bridging the experience gap is now much easier.
Thus, the goals of this handbook are simple: first, to help those who are new to the world of musculoskeletal US to safely and effectively learn common injections; second, to organize the information such that the reader can quickly access a small detail or read through the full range of specifics contained in an entire section. The content is focused on giving the beginner the knowledge and skills needed to know how to perform an injection in clinic. This handbook makes a process that requires a lot of practice easier, by building confidence, and launching clinicians on the road to proficiency.
This book is not meant to be the end-all of US books or the only tool needed in training; instead, view it as the bridge between your entry into the world of musculoskeletal US and the next level of proficiency. The final step to true expertise will then follow with repetition, practice, and mentorship. Most of the injections outlined in this handbook are com-monly performed in musculoskeletal and sports medicine clinics across the United States. The more specialized injections presented at the end of the book on cervical spine and pelvis injections highlight the exciting potential of more advanced interventional musculoskeletal US. All these techniques should be practiced and used with the appropriate level of supervision and mentorship, and I recommend that these more advanced skills be initially done in the setting of fellowship training to ensure that they are taught by experienced practitioners.

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
xviii • PREFACE
The authors and editors are enthusiastic about the use of this handbook to enhance the care of your patients. Dr. Murphy and I look forward to any questions and comments that you may have.
Mohammad Agha, MD, RMSK
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Acknowledgments
Anytime a group undertakes a large project such as this one, its success depends on the people involved. My thanks go out to the following peo-ple who helped make this book a reality: to my parents, Shamim and Dr. Sirajuddin Agha, who helped make me the person that I am today; to my uncles Dr. Amanullah Pathan and Dr. Karamullah Pathan, for being great role models; to my sisters Lubna, Rafiya, and Iram, and to my wife Aisha, for their support; and to the physicians who helped me get to where I am today: Dr. David Cifu, Dr. William McKinley, Dr. Doug Murphy, Dr. Abu Qutubuddin, and Dr. Robert Rinaldi. I also have to thank Dr. Greg Worsowicz and Dr. James Stannard for their decision to hire me onto the faculty at the University of Missouri. Thank you also to Dr. Ted Choma and Dr. Mark Drymalski for their mentorship. Thank you to Demos Medical Publishing and Beth Barry, who supported this project and helped get it off the ground. And finally, my thanks go out to the authors of each chapter, for helping to make this book a resource for ultrasound practitioners so they can practice medicine at a higher level.

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Guide to Musculoskeletal
Injections With Ultrasound

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
CHAPTER 1
Essentials of
Musculoskeletal Ultrasound
Mohammad Agha
CHARACTERISTICS OF ULTRASOUND
• Anultrasound(US)wave isgeneratedbyaUSmachine thatconvertselectricalenergytoasoundwaveatthetransducer/gelinterface(piezo-electriceffect).
• The wave is then propagated through tissue and returns back to thetransducer.
• Whenreturningtothetransducer,thewaveisconvertedbacktoelectri-calenergy,producingaUSimage(reversepiezoelectriceffect).
• MultipleoutcomesoccurwhenaUSwaveleavesthetransducer:
1. Refraction:wavedirectionchangesasitpassesthroughfluid.2. Reflection:wavehitsstructure,returningtotransducer.3. Scatter:Refraction+Reflectionawayfromtransducer(1,2).4. Artifacts(seethefollowing).
• Remember thatmostof theenergy from the transducer is lost asdis-sipatedheat.
US TRANSDUCERS
• Linear:goodforsuperficialstructures(Figure1.1).• Curvilinear:goodforcurved/deepstructures(Figure1.2).• Smallfootprint(“hockeystick”):goodforareasoflimitedcontact(wrist,
ankle)(Figure1.3).• Eachprobe’suseisdependentonthedepthofstructureofinterest.

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
2 • 1:ESSEnTiALSoFMUSCULoSkELETALULTRASoUnd
• Linearprobeshavehighfrequency(typically>10MHz),whichprovideshighresolution,butlowpenetration/depth(upto6cm).
• Curvilinear probes have lower frequencies, which provide lowerresolution, but increased penetration/depth (for structures such asthehip)(2).
Figure 1.1 Linear probe: L4-12t-RS LoGIQ e wide band linear array probe with 4.2–13 MHz frequency. Courtesy of GE.
Figure 1.2 Curvilinear probe: C1-5-RS LOGIQ e wide band convex array probe with 2–5 MHz frequency. Courtesy of GE.

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
ARTiFACTS • 3
SCANNING TECHNIQUE
• PositiontheUSmachinenearpatientformaximalviewingarea.• Holdtheprobebetweenyourthumbandfingerofyourdominanthand.• Besuretowrapyourentirehandaroundtheprobe,withtheendofthe
probenearthefifthdigit.• Maintainscanninghandcontactwithpatientatalltimeswhilescanning—
itincreasesstabilitywhenscanningandinjectingapatient.• keepyourscanninghandlowerthanyourshoulder.• keepyourelbowclosetoyourbody.• Canperformtwotechniqueswithprobetoimproveimageresolution.
• Heel-toe:movingtheprobelong-axis.• Toggling:movingprobeshort-axis(2).
ARTIFACTS
• Anisotropy: when the sound wave is not perpendicular to object ofinterest,theimagingtraitofthetissue(whenoffaslittleas5°)islost.Thistypicallyresultsindarkeningoftissue,mimickingpathology.
Figure 1.3 Hockey stick probe: L8-18i-RS LOGIQ e wide band high-frequency linear array probe with 6.7–18 MHz frequency. Courtesy of GE.

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
4 • 1:ESSEnTiALSoFMUSCULoSkELETALULTRASoUnd
• Shadowing: US beam is refracted, reflected, or absorbed, causing ananechoic(black)imagedeeptotheobject(typicallybeneathbone,withgas,ordeeptoacalcification).
• Posterior acoustic shadowing: soft tissuedeep to anobject is hypere-choic(brighter)comparedtoadjacentsofttissue.Typicallyoccurswithpresenceoffluidorsolidsofttissuetumor.
• Posterior reverberation: a smooth/flat object reflects the sound beambackandforthbetweenitselfandthetransducer,causinglinearechoesdeep to the structure. if it continuesdeeper, called ring-down artifact(associatedwithmetal).
• Comettail:deephyperechoicechoesduetosofttissuegas.• Beamwidthartifact:beamtoowiderelativetoimagedobject.Corrected
byaddingfocalzone(seethefollowing)tolevelofobject(1).
DOPPLER
• dopplereffect:colorflowchangesasobjectmovestowardorawayfromanobject.
• Colorflow:coloredbloodflowindicatingdirectionofbloodflow(red:towardtransducer;blue:away).
• duplexdoppler:US+waveformrecorded.• Powerdoppler:sensitive tobloodflowandtransducermovement,but
doesnotprovidedirectionalinformation.• increasedflowonpowerdopplercanindicateinflammation,increased
perfusion,orneovascularization.• Powerdopplercanalsohelpwithidentifyingotherstructures.• Masswithflowgenerallyindicatesmalignancy,comparedtomasswithout
flow,whichgenerallyindicatesbenign;mass(alwaysbiopsytobesure).• Lymphnode:noflow/hilarflow:generallybenign; spotted/peripheral/
mixedflow:generallymalignant(again,biopsytobesure).• Complexfluidversussynovitis.• Complexfluid:nointernalflowonpowerdoppler.• Synovitis:increasedflow(1).
US PROBE CHARACTERISTICS
Linear: high frequency (>10 MHz), better resolution, less depth(Table1.1).
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
iMAGEoPTiMiZATion • 5
Curvilinear:lowerfrequency(2–5MHz),decreasedresolution,increaseddepth(Table1.2).Hockey stick: high frequency (>10 MHz), increased resolution, lessdepth,bestforsmallerstructures.
IMAGE OPTIMIZATION
1. Selecttheproper transducer.2. Adjustfocal zonestoimprovebrightnessattheleveloftheobjectofinterest
(onlyaddminimumnumberneeded;otherwiseitreducesframerate).3. Adjustgainforappropriateoverallbrightnessonscreentoidentifylocal
structures.4. Adjustdepth gain/time gain compensationtoaddbrightnessatspecific
areaofscreen(3).
Theimageproducedhasobjectswithdifferenceintensities:• Hyperechoic: object brighter than surrounding objects (ligament, ten-
don,bone,calcification).• Hypoechoic:objectdarkerthansurroundingstructures(fluid,tendinosis,
tear).• isoechoic: object has equal brightness in relation to surrounding
structures.• Anechoic:object/areadark(black)(2)(bloodvessel,fluid,cartilage).
Table 1.1 Advantages of Ultrasound
High-resolution images
Real-time imaging
Dynamic examination
Procedure guidance
Can compare contralaterally
No radiation
Portable
No known contraindications
Relatively inexpensive
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
6 • 1:ESSEnTiALSoFMUSCULoSkELETALULTRASoUnd
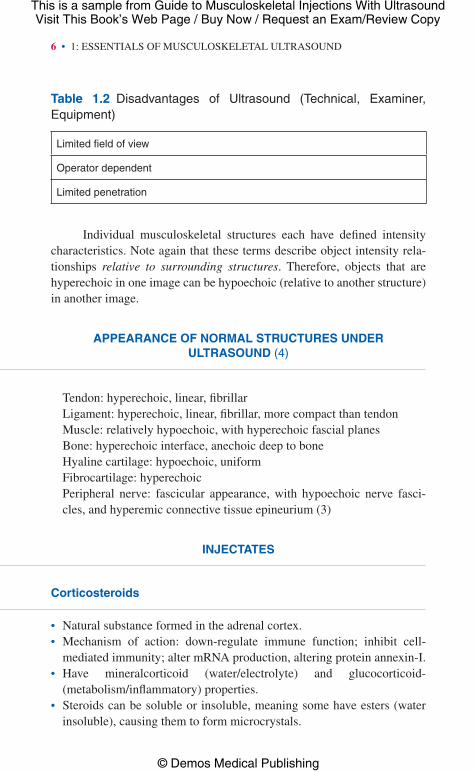
individual musculoskeletal structures each have defined intensitycharacteristics.noteagainthatthesetermsdescribeobjectintensityrela-tionships relative to surrounding structures. Therefore, objects that arehyperechoicinoneimagecanbehypoechoic(relativetoanotherstructure)inanotherimage.
APPEARANCE OF NORMAL STRUCTURES UNDER ULTRASOUND (4)
Tendon:hyperechoic,linear,fibrillarLigament:hyperechoic,linear,fibrillar,morecompactthantendonMuscle:relativelyhypoechoic,withhyperechoicfascialplanesBone:hyperechoicinterface,anechoicdeeptoboneHyalinecartilage:hypoechoic,uniformFibrocartilage:hyperechoicPeripheral nerve: fascicular appearance, with hypoechoic nerve fasci-cles,andhyperemicconnectivetissueepineurium(3)
INJECTATES
Corticosteroids
• naturalsubstanceformedintheadrenalcortex.• Mechanism of action: down-regulate immune function; inhibit cell-
mediatedimmunity;altermRnAproduction,alteringproteinannexin-i.• Have mineralcorticoid (water/electrolyte) and glucocorticoid-
(metabolism/inflammatory)properties.• Steroidscanbesolubleorinsoluble,meaningsomehaveesters(water
insoluble),causingthemtoformmicrocrystals.
Table 1.2 Disadvantages of Ultrasound (Technical, Examiner, Equipment)
Limited field of view
Operator dependent
Limited penetration

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
AdVERSEEFFECTS • 7
• BetamethasoneanddexamethasonedonoThaveesters, thustheyarebrokendownviahydrolysisbythebody’scellesterases.
• Thisleadstolongereffectinjoint.• Estershavequickeronset,butdecreasedduration(Table1.3,Table1.4).
ADVERSE EFFECTS
• Septicarthritis• Postinjection flare (most common adverse effect, develops in a few
hours,lasts2–3days)
Table 1.3 Commonly Injected Corticosteroids
Steroid Equivalent Potency % Particles >10 µm
Methylprednisolone acetate 4 45
Triamcinolone acetonide 4 45
Betamethasone acetate/sodium phosphate
0.75 35
Dexamethasone sodium phosphate
0.75 0
Table 1.4 Different Steroid Doses for Variably Sized Joints (5)
Joint Size
Methylprednisolone Acetate (mg)
Triamcinolone Acetate (mg)
Betamethasones (mg)
Dexamethasone Sodium Phosphate (mg)
Large 20–80 10–15 1–2 2–4
Medium 10–40 5–10 0.5–1.0 2–3
Small 4–10 2.5–5 0.25–0.5 0.8–1
Large: shoulder, hip, knee, ankle. Medium: elbow, wrist. Small: MCP, AC joint.
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
8 • 1:ESSEnTiALSoFMUSCULoSkELETALULTRASoUnd
• Localtissueatrophy• Tendonrupture• Cartilagedamage• Facialflushing• Chills/shakes/headache(histaminereleasefromsteroid)• increasedbloodglucoselevels• Localtissuenecrosis• Calcification• Skinatrophy/depigmentation
ADVERSE CENTRAL NERVOUS SYSTEM EFFECTS
• Tetraplegia/paraplegia• Can be due to brain/spinal cord infarction, vascular injury, embolism
from steroid particulate (most likely), neurotoxicity from preservative(benzylalcohol),ordrugvehicle(polyethyleneglycol)
CONTRAINDICATIONS FOR CORTICOSTEROID INJECTIONS
• Absolute:Sepsis (systemic/intra-articular), intra-articular fracture, andjointinstability.
• Relative: Juxta-articular osteoporosis, coagulopathy, joint injectionmorethanthreetimesperyear,oroneinjectioninthelast6weeks.
LOCAL ANESTHETICS (TABLE 1.5)
• inhibitnerveexcitationthroughsodiumchannelblockadeatcellmem-brane(inhibitsactionpotential).
• Effective analgesic due to blocking smaller diameter nerves (ie, painfibers).
• Twocategories:amides(lidocaine)andesters.• Canbeadministeredwithvasoconstrictortodecreasevascularabsorp-
tion,increasingduration.• Anesthetic characteristics determined by acid dissociation pK
a, lipid
solubility,proteinbinding.

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
LoCALAnESTHETiCS • 9
• pKa:onsetofaction.
• Lipidsolubility:nervemembranepenetration(highersolubility:higherpenetration).
• Proteinbinding:durationofaction.
Contraindications
• Sensitivitytoamideanesthetic• Localinfection• Coagulopathy• Epinephrine use if patient uses monoamine oxidase (MAo) inhibitor/
tricyclicantidepressants(TCA)(prolongedhypertension).
Adverse Side Effects
• Centralnervoussystem:shivering,muscletwitches,tremor,hypoventi-lation,andconvulsions.
• Cardiac:arrhythmias,cardiovascular(CV)depression/collapse.• Anaphylaxis:lossofconsciousness,convulsions,andCVeffects.• Skeletalmuscletoxicity:necrosis,cellapoptosisduetopermanentintra-
cellularcalcium,muscleweakness,andchondrocytetoxicity.
Table 1.5 Commonly Used Local Anesthetics
Generic Name (min)
Relative Potency
Onset Duration of Action (min)
Procaine hydrochloride
1 Moderate 30–60
Lidocaine hydrochloride
2 Rapid 80–120
Ropivacaine hydrochloride
6 Moderate 140–200
Bupivacaine hydrochloride
8 Long (2–10 min) 180–360
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
10 • 1:ESSEnTiALSoFMUSCULoSkELETALULTRASoUnd
PLATELETRICH PLASMA (6)
• Plateletshavealphagranulesthatreleasegrowthfactors.• Thesegrowthfactorsaresmallpeptidesthatbindmembranereceptors
andpromotedownstreampathways.• Also mediate chemotaxis and cell migration through “chemical
mediators.”• Canalsoaffectmitosis,angiogenesis,andcelldifferentiation.• Platelet-richplasma(PRP)preppedfromautologouswholeblood.• Spundownbycentrifugetoproducethreelayers:
1. plasmalayer(top)2. plateletsandwhitebloodcells(WBC)3. redbloodcells
• Middlelayer(PRP)suctionedout;canaddcalciumchlorideorthrombintoactivateplatelets.
• Thisreleases70%growthfactorsin10minutes.• it’sbelievedthatneedlingthestructureofinterestcausesfocalbleeding
andacuteinflammatoryresponse,aidingcellrecruitmentandrepair.
VARIOUS BLOOD PRODUCTS
• Autologousconditionedserum:wholeblooddrawnintoglassbeadstostartmonocyteactivation.
• Autologousplasma rich ingrowth factors (PRGF):venousbloodcol-lectedin5mLtubeswith3.8%trisodiumcitrate,centrifugedat1,800rpmfor8minutes.0.25to1mLfractiontransferredtosteriletubes.Calciumadded,formingfibrinmatrixwithplatelets.
• Autologousconditionedplasma:wholebloodcentrifugedtoformPRP,thenplaced intobottlewithcalciumchloride incentrifuge toproduceplateletfibrinmatrix.
• Plateletleukocyte-richgel:centrifugewholebloodtoproducePRPandleukocyte-richplasma(toplayer),whicharemixedtogetherwiththrom-binorcalciumchloridetoformagel.it is thoughtthataddingWBCsconfersantibacterialproperties.
• Autologousbloodinjections:wholevenousbloodmixedwithlidocaineorbupivacaineforinjection.
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
STEMCELLS • 11
STEM CELLS (7)
• Threebasiccategories:embryonic,adult (mesenchymal), and inducedpluripotent.
• Moststudied:mesenchymalstemcells.• isolatedfrommanytissues(bonemarrow,muscleadipose).• Thecloseratissueistocelllineofdesiredtissue,themoreeffectiveat
differentiatingintodesiredcellline.• Cellscanbeusedfromculturedlinesorsame-daysample.
To Culture Stem Cells
• Seedcellsontomonolayerflask• Attachtosurface• Adherentcellsgetculturemediumtogrow• Growthcontinuesuntilcellstoucheachother• oncetheytouchtheystopgrowing(confluence)• Cellsarethenplacedintoanotherflaskandmedium(passage)
SameDay Use
• Harvesttissuefromadipose• Releasecellsorgetfractionbybreakingdowncollagenmatrixtocentri-
fugecells
Mechanisms of Action
• Celldifferentiation• Paracrine effects (chemokine secretion, suppressed dendritic cells,
reducedeffectorTcells/nkcells/MHCClassiicells)• Macrophagedeactivation(preventsfurthermetabolism)
Autologous vs. Allogeneic Cell Lines
• Autologous: carry more genetic variants; decreased differentiation ifolderpatients.
• Allogeneic:massproductionpossible;canactivatehostimmunesystem(iL-6deregulation).

Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
12 • 1:ESSEnTiALSoFMUSCULoSkELETALULTRASoUnd
• AdministrationofstemcellsregulatedbyFoodanddrugAdministration(FdA)(FdATissueRegulation,21CFRPart1271)(8).
• FdAdoesnotallowextendedexvivoculturingofgrowthfactors,andonlyallows“minimallymanipulatedtissue”(8).
Visit This Book’s Web Page / Buy Now / Request an Exam/Review CopyThis is a sample from Guide to Musculoskeletal Injections With Ultrasound
© Demos Medical Publishing
REFEREnCES • 13
REFERENCES
1. Jacobson JA. introduction. Fundamentals of Musculoskeletal Ultrasound.Philadelphia,PA:ElsevierSaunders;2007:1–14.
2. kirschnerJS.introduction.in:SpinnerdA,kirchsnerJS,HerreraJE.Atlas of Ultrasound Guided Musculoskeletal Injections. new York,nY:Springer;2014:1–4.
3. Smith J, Finnoff JT. diagnostic and interventional musculoskeletalultrasound.Part1:fundamentals.PM&R.2009;1(1):64–75.
4. Smith J, Finnoff JT. diagnostic and interventional musculoskeletalultrasound.Part2:clinicalapplications.PM&R.2009;1(2):162–177.
5. MacMahon PJ, Eustace SJ, kavanagh EC. injectable steroids andlocal anesthetic preparations: a review for radiologists. Radiology.2009;252(3):647–661.
6. nguyen RT, Borg-Stein J, Mcinnis k. Applications of platelet-richplasma in musculoskeletal and sports medicine: an evidence-basedapproach.PM&R.2011;3:226–250.
7. Centeno CJ. Clinical challenges and opportunities of mesenchymalstemcellsinmusculoskeletalmedicine.PM&R.2014;6:70–77.
8. BashirJ,ShermanA,LeeH,etal.Mesenchymalstemcelltherapiesinthetreatmentofmusculoskeletaldiseases.PM&R.2014;6:61–69.





























