Embed Size (px)
Citation preview

Respiratory Medicine (2014) 108, 694e700
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier .com/locate /rmed
Guidance on handheld inhalers in asthmaand COPD guidelines
P.N. Richard Dekhuijzen a,*, Leif Bjermer b, Federico Lavorini c,Vincent Ninane d, Mathieu Molimard e, John Haughney f
a Department of Pulmonary Diseases (454), Radboud University Medical Centre, PO Box 9101,6500 HB Nijmegen, The Netherlandsb Department of Respiratory Medicine, Lund University Hospital, SE-22185 Lund, Swedenc Department of Experimental and Clinical Medicine, Careggi University Hospital, Largo Brambilla 3,50134 Florence, Italyd Service de Pneumologie, Saint-Pierre University Hospital Brussels, 322 rue Haute,B-1000 Brussels, Belgiume University of Bordeaux, INSERM U657, 33076 Bordeaux Cedex, Francef Centre of Academic Primary Care, University of Aberdeen, Foresterhill Health Centre, WestburnRoad, Aberdeen, AB25 2AY Scotland, UK
Received 18 November 2013; accepted 21 February 2014Available online 1 March 2014
KEYWORDSDry powder inhalers;Pressurised metered-dose inhalers;Asthma;Chronic obstructivepulmonary disease;Guidelines
* Corresponding author. Tel.: þ31 (0E-mail address: R.Dekhuijzen@LON
http://dx.doi.org/10.1016/j.rmed.200954-6111/ª 2014 Elsevier Ltd. All rig
Summary
Background: Inhaled therapy is the cornerstone of pharmacotherapy in patients with asthmaand chronic obstructive pulmonary disease (COPD). Appropriate inhalation device selectionis as important as drug choice but device-specific guidance appears to be lacking.Methods: To quantify the level of inhalation-device recommendations in clinical guidelines, areview was conducted by hand-searching national and international asthma and COPD guide-lines (Global Initiative for Asthma [GINA] and Global initiative for chronic Obstructive LungDisease [GOLD] guidelines) and an international guideline on device selection (the AmericanCollege of Chest Physicians/American College of Asthma, Allergy, and Immunology [ACCP/ACAAI]). For each guideline, the number of pages, tables/figures and references relating toinhalation devices was identified.Results: GINA and GOLD guidelines contain very little inhalation device-specific guidancebeyond recommendations for demonstrating and testing correct inhalation technique: <2%of pages or references and <3% of tables/figures are dedicated to devices. Device-related con-tent in the ACCP/ACAAI device selection guideline was considerably higher with 54% of pages,88% of tables/figures and 82% of references, respectively. Results in national guidelines reflectthose on international guidelines.Conclusions: These results indicate that there is a considerable lack of clear and specificguidance regarding inhalation devices in current asthma/COPD guidelines. More robust studies
) 243610325; fax: þ31 (0) 243610324.G.umcn.nl (P.N.R. Dekhuijzen).
14.02.013hts reserved.

Inhaler guidance in current guidelines 695
Fig
on the impact of inhalation devices are needed to increase the number of evidence statementsand recommendations regarding inhalation devices.ª 2014 Elsevier Ltd. All rights reserved.
Background
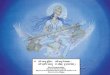
Healthcare professionals are faced with a range of chal-lenges when selecting the most appropriate inhalationtherapy for a patient with asthma or chronic obstructivepulmonary disease (COPD). A number of different factorscan adversely affect outcomes, including incorrect diag-nosis, poor compliance, and inadequate or inappropriatetherapy (Fig. 1) and the inhalation device to be used shouldalso be considered. Correct use of an appropriate inhala-tion device enables medication to be effectively delivereddirectly to the lungs, thus maximising clinical efficacy whileminimising potential systemic side effects [1]. Successfuldelivery to the lungs is influenced by factors includingparticle size, inhalation flow rate and inhaler resistance[2,3]. These and other factors differ between inhalationdevices and can affect inhaler technique, patient satis-faction and compliance with treatment.
Selection of themost appropriate inhalation therapy in aneffective inhaler that the patient can easily use correctly isfurther complicated by the range of molecules available andthe fact that not all of themare available in all devices, alongwith the ever-increasing variety of inhaler designs andcharacteristics [4]. Incorrect inhaler technique can haveserious consequences for patients in terms of disease controland quality of life [5e8]. These preventable consequencesfurther increase the burden of asthma and COPD both on theindividual and on society [9]. It is, therefore, important that
ure 1 Reasons for poor asthm
clear and concise guidance is available to enable physiciansto select the most appropriate inhaler device to deliver themedication they decide an individual patient needs.
Unfortunately, the Global Initiative for Asthma (GINA)[10] and Global initiative for chronic Obstructive LungDisease (GOLD) [11] guidelines are both complex andlengthy documents to absorb and implement. In addition,they are pharmacologically oriented and provide limitedguidance regarding choice of devices. This study was con-ducted to quantitatively assess the proportion of guidelinecontent specifically dedicated to handheld inhalationdevices (pressurised metered-dose inhalers [pMDIs] with orwithout spacer devices and dry powder inhalers [DPIs]). Thelevel of guidance provided by evidence-based respiratoryguidelines on inhaler choice was also investigated andrecommendations on how this guidance could be improvedwere provided.
Methods
A review of inhalation-device recommendations in clinicalguidelines was performed by hand-searching major asthmaand COPD guidelines. These guidelines were identified bysearching the National Center for Biotechnology Informa-tion, U.S. National Library of Medicine (PubMed) databasefor publications with titles that contain the terms ‘COPD’ or‘asthma’ and ‘guideline’ or ‘guidelines’. Using these results
a control in clinical practice.

696 P.N.R. Dekhuijzen et al.
and the authors’ own knowledge of key international andlocal guidelines, reports from the following bodies/soci-eties were selected for review:
� British Thoracic Society/Scottish Intercollegiate Guide-line Network (BTS/SIGN) [12]
� Dutch Standard of COPD Care [13]� GINA [10]� GOLD [11]� Italian Guidelines for Asthma, COPD and Rhinitis (LIBRA)[14]
� International Primary Care Respiratory Group (IPCRG)[15,16]
� National Institute for Health and Clinical Excellence(NICE) [17]
� Haute Autorite de Sante (ANAES/HAS) [18]� Swedish Medical Products Agency (Lakemedelsverket)[19,20]
� The French-speaking Society of Pneumology (SPLF) [21]
In addition, the American College of Chest Physicians/AmericanCollegeofAsthma,Allergy, and Immunology (ACCP/ACAAI) guideline on device selection was reviewed [22].Although not disease specific, the ACCP/ACAAI guidelinesprovide evidence-based recommendations on inhalationdevices for respiratory disease and were considered to berelevant for inclusion. As this study is focused on evidence-based guidelines for the management of respiratory dis-ease, rather than guidance, the 2011 European RespiratorySociety/International Society for Aerosols in Medicine (ERS/ISAM) task force report on the delivery of pharmaceuticalaerosols [23] was not included in the review.
For each guideline, the number of pages, tables/figures,specific recommendations and references relating to inha-lation devices was identified.
Results
International guidelines
The proportion of device-related content in GINA and GOLDguidelines is very low, with <2% of pages or referencesdedicated to inhalation devices (Table 1), and 14 of 16 such
Table 1 The proportion of content specifically related toinhalation devices in current international treatmentguidelines for asthma and COPD.
Guideline Number (%)of pages
Number (%)of tables/figures
Number (%)of references
GINA [10] 1.8/110 (1.6%) 1/37 (2.7%) 17/902 (1.8%)GOLD [11] 0.66/78 (0.8%) 1/37 (2.7%) 5/488 (1.0%)ACCP/ACAAI
[22]20/37(54.0%)
21/24(87.5%)
116/142(81.7%)
ACCP/ACAAI, American College of Chest Physicians/AmericanCollege of Asthma, Allergy, and Immunology; COPD, chronicobstructive pulmonary disease; GINA, Global Initiative forAsthma; GOLD, Global initiative for chronic Obstructive LungDisease.
references for GINA and 4 of 5 references for GOLD werepublished more than 5 years prior to the guideline publi-cation. The level of device-specific content in tables andfigures is also low: GINA contains one table with a strategyfor choosing an inhalation device in children according toage range, while the GOLD guideline contains one tablethat outlines formulations and typical doses of COPDmedications including inhalers.
As expected, overone-half of thepagesof theACCP/ACAAIdevice-selection guideline contain device-specific contentand more than three-quarters of the tables/figures andreferences in this publication clearly relate to inhalationdevices (Table 1). Notably, one table describes the advan-tages and disadvantages of different types of aerosol-generating inhaler devices, including pMDIs and DPIs. How-ever, 100of the116device-related referenceswerepublishedmore than 5 years prior to the publication of this guideline.
The number of recommendations regarding inhalationdevices and specific recommendations according to patientsubgroup incurrent clinical guidelinesare reported inTable 2.Both GINA and GOLD guidelines advocate that factors such ascost, the ability and skill of the patient, preference and de-vice availability should be taken into account when selectingan inhalation device but provide little further guidance on thespecifics of these or other factors, such as patient age and thetypes of drugs being administered (Table 2).
Inhalation-device recommendations in the ACCP/ACAAIguideline are more all-encompassing and include both low-and high-quality evidence. These recommendations are notspecific to patient subgroups (e.g. paediatrics or the elderly)with the exception of a table on general age requirements forthe correct use of aerosol delivery device types based on theNational Asthma Education and Prevention program. How-ever, guidance on selecting an appropriate inhalation deviceand recommendations on appropriate devices for use invarious clinical settings is provided (Table 2).
Both GINA and GOLD guidelines recommend that a pa-tient’s inhalation technique is assessed at every visit totheir clinician. However, no guidance on correct inhalationtechnique is provided in the ACCP/ACAAI guideline andnone of the guidelines provide any specific information onhow clinicians should assess technique.
Generally, guidelines refer to pMDI or DPI universallyrather than to specific inhalation devices when makingrecommendations. The GINA guideline does not mention anybranded inhalation devices while the GOLD guideline men-tions the HandiHaler� and Respimat� devices in one para-graph. The ACCP/ACAAI guideline mentions Combivent�,Diskhaler�, Rotahaler�, Spinhaler�, Spiros�, Turbuhaler�
and Ventolin� inhalers in the context of describing clinicalstudies but does not provide any specific guidance.
Across all three guidelines, a notable proportion ofinhalation device-related content concerned the use ofspacer devices (Table 2).
National guidelines
The proportion of inhalation device-related content incurrent national treatment guidelines for asthma and COPDreflects that of the international guidelines (see Onlinesupplementary materials for further details).

Table 2 Guidance relating to inhalation devices in currentinternational treatment guidelines for asthma, COPD andpulmonary diseases.
Statement Guideline
GINA[10]
GOLD[11]
ACCP/ACAAIa
[22]
Considerations for appropriate inhalation device selection
Patient’s ability to usethe device correctly
U U U
Patient preference U U
Availability of the drug/device combination
U U
Compatibility betweenthe drug and deliverydevice
U
Time/skills to properlyinstruct the patient inthe use of the deviceor to monitorappropriate use
U
Cost of therapy U U
Potential forreimbursement
U
Both pMDIs and DPIs are
appropriate for the
delivery of SABA and ICS
U U
Preferred device in children
<4 years, pMDI inhalerplus dedicated spacerwith face mask
U n/a
4e6 years, pMDI inhalerplus dedicated spacerwith mouthpiece
U n/a
>6 years, DPI, or breath-actuated pMDI or pMDIwith spacer andmouthpiece
U n/a
pMDI should be used with a
spacer device
Ub U Uc
Training in inhaler technique
is important/essential
U U U
ACCP/ACAAI, American College of Chest Physicians/AmericanCollege of Asthma, Allergy, and Immunology; COPD, chronicobstructive pulmonary disease; DPI, dry powder inhaler; GINA,Global Initiative for Asthma; GOLD, Global initiative for chronicObstructive Lung Disease; ICS, inhaled corticosteroids; n/a, notapplicable; MDI, metered-dose inhaler; pMDI; pressurisedmetered-dose inhaler; SABA, short-acting b2-agonist.a Only recommendations provided for the outpatient setting
are included.b In children.c Except for the delivery of SABAs where a MDI may be
used � a spacer or holding chamber.
Inhaler guidance in current guidelines 697
Discussion
The results of this study indicate that current asthma andCOPD treatment guidelines lack clear and specific guidanceregarding inhalation devices. This is particularly notable in
the international GINA [10] and GOLD [15] guidelines, whichare used worldwide by respiratory clinicians and local so-cieties/governing bodies as the basis for their diagnosis andtreatment strategies. These guidelines, of course, onlyreflect published evidence and do not seek to offerguidance where published evidence of acceptable qualitydoes not exist [24].
Unlike GINA and GOLD, the ACCP/ACAAI guideline is notdisease specific and contains recommendations for deviceselection according to various settings (e.g. the emergencydepartment/hospital inpatient setting) rather than byparticular disease/patient groups [22]. These recommen-dations were made by the authors of a systematic reviewand meta-analysis that investigated whether device selec-tion has an effect on the efficacy and tolerability of inhaledcorticosteroids, b2-agonists and anticholinergics, andassessed the strength of recommendations on the basis ofthe quality of the evidence presented and net benefit tothe patient. The authors concluded that there were nodifferences between inhalation devices in terms of clinicalefficacy. However, this analysis only included randomisedcontrolled trials (RCTs), which frequently require goodinhaler technique as an inclusion criterion. Findings fromother studies that may have highlighted differencesbetween devices that impact on their effectiveness in thereal-world setting were excluded. Studies that wereincluded in the analysis were found to be heterogeneous interms of purpose, study design and patient selection. Fewstudies were designed to compare inhalation devices andinhalation technique was often not described. The dosesused in the bronchodilator studies that were included weregenerally at the top of the doseeresponse curve. Thesefactors may, at least in part, explain the finding of similarefficacy between different inhalers.
The 2011 ERS/ISAM task force report on the delivery ofpharmaceutical aerosols [23] recognises that patientsparticipating in RCTs receive more training in inhalationtechnique and counselling on the importance of adherencethan patients who are receiving routine clinical care. Thus,the recommendations provided in this report focused onthe patient-use aspect of inhalation devices with the aim ofeducating prescribers. Unfortunately, as this statement isnot an evidence-based guideline, it was not eligible forinclusion in this review.
Guidelines rely upon and reflect the quantity and qualityof published evidence currently available, so when there islittle high-quality evidence available, they are limited intheir ability to provide clear recommendations concerningthe importance of device choice in asthma and COPD.More studies are needed to enable clear, concise andspecific guidance in evidence statements and guidelinerecommendations. This ‘call to action’ [25] may finally bereceiving the attention it deserves with the January 2012update of the BTS/SIGN guidelines [12]. This containsrecommendations for research including three key ques-tions relating to inhalation devices: ‘What role does patientpreference play in deciding which inhaler to prescribe?Does this improve compliance? Does this improve effec-tiveness of treatment?’
Studies that randomise patients on the same therapy todifferent devices could provide answers as to which devicesare more effective and most suitable for particular

698 P.N.R. Dekhuijzen et al.
subgroups. Unfortunately, such studies are not necessarilyeasy to design and conduct. Clinical guidelines prefer tobase their recommendations on double-blind, double-dummy RCTs. Currently, published studies comparinginhalation devices are predominantly single-sponsoredasthma studies that only provide patient-reported out-comes data. The factors that may preclude classical evi-dence studies on devices include:
e The Hawthorne effect [26] (improved compliance andinhaler technique in RCTs may obscure real-worlddifferences between devices)
e Controlling bias in real-world studies (methodologicalissues make it difficult to ensure that observeddifferences in disease control are actually due to theinhalation device)
e Ethics of randomisation (it would be unethical to ran-domise patients to a device they are unable to use)
e Complexities of placebo-controlled and double-blind,double-dummy studies (patients may receive severaldifferent inhalers to maintain blinding to study treat-ments; hence the effect of one inhalation device cannotbe evaluated)
e Single-sponsor studies (these studies could be biasedtowards the product of the study sponsor).
Even if evidential studies could be conducted, they areunlikely to provide a true reflection of the considerationsthat need to be made when selecting an appropriateinhalation device for the individual patient, as this dependson a range of factors. These include objective factors, suchas the resistance and fine particle output characteristics ofthe device, and often its cost, along with more subjectiveelements, such as the patient’s dexterity, co-ordinationand inspiratory flow, previous experience with device,acceptability, convenience and visual preference [2,3]. Thekind of research required to identify which devices aremost suitable in the clinical setting does not fit easily withtraditional evidence grading systems. Asthma and COPD arecomplex chronic diseases and each patient has individualrequirements. Studies based on targeted, personalisedmedicine may be more appropriate than classical studiesthat generalise the population with grouped mean data.
Recommendations to address this issue
More (and better) evidenceClearly, more precise information about, and guidance on,the use of inhalation devices is warranted as device choicecan have a significant impact on inhaler technique andadherence to treatment [27], and more data are needed toenable treatment guidelines to provide recommendations.To this end, studies regarding the most appropriate devicesfor patient subgroups, such as those with low inspiratoryflow rates, paediatric and elderly populations, or patientswith cognitive, visual and hearing impairment that make itdifficult for them to synchronise inhalation with inhaleractivation, would be of particular importance. Moreover,these patient populations clearly indicate that an ‘ideal’inhaler device, suitable for all patients of all types, is notavailable at the present: in fact, some of these patients
may benefit more from the use of a nebuliser rather than ahandheld inhaler, despite the relative lack of portability.
Trials to address the gaps in evidence in comparisons ofdevices could use standard outcome measures (exacerba-tion rate, symptom control and healthcare utilisation) and,in addition, new specific endpoints such as ‘inability tomaintain correct use of a device’. This would involveregular objective assessments of each patient’s inhalertechnique, either at home by a visiting specialist nurse ortechnician, at additional study visits or by utilising tech-nologies such as video links, telemetry and other moni-toring techniques. Patient education on correct use of thedevice would be an important aspect of such an assessmentstudy. The main study would remain a robustly designedRCT, but if patients were unable to maintain correct use ofa device to which they were randomised, they would beclassed as a treatment failure and switched to an alterna-tive treatment arm using a different device. Tools to helpidentify suitable inhalers for individual patients should bedeveloped and validated. Cohort studies that utilise data-bases similar to the Clinical Practice Research Datalink [28]could also be viable. Step-by-step descriptions of how touse or teach the use of different types of inhaler correctlyare currently lacking in the GINA and GOLD guidelines. Suchinstructions are of vital importance if patients are tobenefit fully from an inhalation treatment and do, there-fore, need to be addressed by guidelines. In particular,differences between pMDIs and DPIs in preparation andactuation should be clearly described. The importance ofchecking and re-checking the patient’s inhaler use at eachvisit should also be more firmly stated. Finally, criteria tobe considered for choosing the most appropriate inhaler foran asthma or COPD patient, such as those recently pro-posed by Newman [29], should be reported and discussed inguidelines. The precision of dosing by the pulmonary routecan be improved by appropriate choice of inhaler deviceand by patient education.
Education of healthcare professionalsThe development and validation of appropriate educationaltools is necessary to assist clinicians and other healthcareprofessionals who are involved in selecting inhalation de-vices (i.e. ‘teach the teacher’) [30]. The ACCP/ACAAI meta-analysis [22] proposed some general principles for selectingand using inhalation devices while a small number of al-gorithms have been proposed in papers by the Aerosol DrugManagement Team (ADMIT) [31].
Patient educationIt is at least as important to educate patients, as they mayhave assumptions and expectations regarding their healthstatus, health provider, and the balance of benefits andside effects that influence their adherence to treatment[32]. Training is crucial for correct inhaler technique andthis is supported in all of the international guidelinesincluded in this study. Practical training tools are availableto help both the physician and the patient to understandhow to use an inhalation device properly. Some providereal-time feedback on use of the device while othersobjectively assess compliance with treatment [30]. Face-to-face training and follow-up (with the physician or witha trained nurse) is also necessary to ensure correct inhaler

Inhaler guidance in current guidelines 699
technique and treatment adherence but this could becombined with electronic follow-up (e.g. via the internet,smartphone applications and modern media), which alsohas the potential to collect real-life data regarding medi-cation use.
Conclusions
Clear and specific content on inhalation devices is scarce incurrent asthma and COPD guidelines. Treatment choiceshould strike a balance between appropriate medicationand inhalation device selection. More data are needed toenable guidelines to provide clear, current information toclinicians on how to appropriately assess patients andmatch them to a suitable device. Despite the difficulties inobtaining robust clinical data that can be translated intoguideline recommendations, there are potential solutionssuch as the inclusion of ‘inability to maintain correct use ofa device’ as a study endpoint. Additionally, the value ofboth healthcare professional and patient education shouldnot be overlooked.
Funding
Medical writing assistance for this manuscript was fundedby AstraZeneca.
Author contributions
All authors participated fully at every stage in the devel-opment of this review.
Conflicts of interest
Richard Dekhuijzen has received reimbursements forattending symposia, fees for speaking, organising educa-tional events, funds for research or fees for consulting fromAstraZeneca, Boehringer Ingelheim, Chiesi, Merck Sharp &Dohme, Mundipharma, Novartis, Takeda, Almirall and Teva.
Leif Bjermer has during the last 3 years receivedhonorariafor attending advisory board meetings or giving lectures forthe following companies: Almirall, AstraZeneca, Airsonette,Andre Pharma-Chiesi, Boehringer Ingelheim, GlaxoSmithK-line, Meda, Merck, Mundipharma, Nigaard Pharma, Novartis,Pfizer, Takeda/Nycomed and Teva.
Federico Lavorini has received reimbursements forattending meetings and fees for speaking from Meda Pharma,Teva,Mundipharma,Chiesi,Menarini IndustrieFarmaceuticheand AstraZeneca.
Vincent Ninane has received reimbursements for attendingsymposia, fees for speaking or fees from consulting fromAstraZeneca, GlaxoSmithKline, Novartis, BoehringerIngelheim, Roche, Lilly and Olympus.
Mathieu Molimard is a consultant for or has participatedin advisory board meetings for AstraZeneca, Bristol-MyersSquibb, GlaxoSmithKline, Novartis, Pfizer and Stallergen.
John Haughney has received reimbursements forattending symposia, fees for speaking, organising educa-tional events, funds for research or fees for consulting from
Almirall, AstraZeneca, GlaxoSmithKline, Merck Sharp &Dohme, Mundipharma, Novartis, Nycomed and Teva.
Acknowledgements
Medical writing assistance was provided by RachelHattersley-Dykes and David Candlish of inScience Commu-nications, Springer Healthcare.
Appendix A. Supplementary data
Supplementary data related to this article can be found athttp://dx.doi.org/10.1016/j.rmed.2014.02.013.
References
[1] Rau JL. The inhalation of drugs: advantages and problems.Respir Care 2005;50:367e82.
[2] Capstick TG, Clifton IJ. Inhaler technique and training inpeople with chronic obstructive pulmonary disease andasthma. Expert Rev Respir Med 2012;6:91e101. quiz 2e3.
[3] Usmani OS, Biddiscombe MF, Barnes PJ. Regional lung depo-sition and bronchodilator response as a function of beta2-agonist particle size. Am J Respir Crit Care Med 2005;172:1497e504.
[4] Crompton GK, Barnes PJ, Broeders M, Corrigan C, Corbetta L,Dekhuijzen R, et al. The need to improve inhalation techniquein Europe: a report from the Aerosol Drug ManagementImprovement Team. Respir Med 2006;100:1479e94.
[5] Cochrane MG, Bala MV, Downs KE, Mauskopf J, Ben-Joseph RH.Inhaled corticosteroids for asthma therapy: patient compli-ance, devices, and inhalation technique. Chest 2000;117:542e50.
[6] Giraud V, Roche N. Misuse of corticosteroid metered-doseinhaler is associated with decreased asthma stability. EurRespir J 2002;19:246e51.
[7] Horn CR, Clark TJ, Cochrane GM. Compliance with inhaledtherapy and morbidity from asthma. Respir Med 1990;84:67e70.
[8] Lindgren S, Bake B, Larsson S. Clinical consequences of inad-equate inhalation technique in asthma therapy. Eur J RespirDis 1987;70:93e8.
[9] Fink JB, Rubin BK. Problems with inhaler use: a call forimproved clinician and patient education. Respir Care 2005;50:1360e74 [discussion 74e5].
[10] Global Initiative for Asthma (GINA). The global initiative forasthma. GINA report, global strategy for asthma managementand prevention [cited 2013 January 24th]. Available from:www.ginasthma.org; 2012.
[11] Global Initiative for Chronic Obstructive Lung Disease. Globalstrategy for diagnosis, management, and prevention of COPD(2011 update) [cited 2012 February 9th]. Available from:http://www.goldcopd.org/uploads/users/files/GOLD_Report_2011_Jan21.pdf; 2011.
[12] British guideline on the management of asthma. Thorax 2003;58(Suppl. 1):i1e94.
[13] Gommer AM. (RIVM) PMR. Exploration national vision ofhealthcare e prevalence, incidence, and mortality in COPD.Bilthoven: RIVM; 2010 24 June.
[14] Il Progetto Libra. Italian guidelines for asthma, COPD andrhinitis; 2002.
[15] Bellamy D, Bouchard J, Henrichsen S, Johansson G,Langhammer A, Reid J, et al. International Primary Care

700 P.N.R. Dekhuijzen et al.
Respiratory Group (IPCRG) guidelines: management of chronicobstructive pulmonary disease (COPD). Prim Care Respir J2006;15:48e57.
[16] van der Molen T, Ostrem A, Stallberg B, Ostergaard MS,Singh RB. International primary care respiratory group (IPCRG)guidelines: management of asthma. Prim Care Respir J 2006;15:35e47.
[17] National Institute for Health and Clinical Excellence (NICE).Chronic obstructive pulmonary disease: management ofchronic obstructive pulmonary disease in adults in primaryand secondary care [cited 2012 February 9th]. Available from:http://guidance.nice.org.uk/CG101; 2010.
[18] French National Agency for Accreditation and Evaluation inHealthcare (ANAES). Medical follow-up of patients withasthma e adults and adolescents. Available from: http://www.has-sante.fr/portail/upload/docs/application/pdf/asthma_follow-up_guidelines.pdf; 2004.
[19] Swedish Medical Products Agency. Farmakologisk behandlingvid astma e Behandlingsrekommendation; 2007.
[20] Lundback B. Farmakologisk behandling vid astma e Bak-grundsdokumentation. Available from: http://www.lakemedelsverket.se/upload/halso-och-sjukvard/behandlingsrekommendationer/bakg_dok/astma_bakgrund2007.pdf;2007.
[21] The French-speaking Society of Pneumology recommendationson the management of COPD. Rev Mal Respir 2010;27(Suppl.1):S1e76 [I-XXXI].
[22] Dolovich MB, Ahrens RC, Hess DR, Anderson P, Dhand R,Rau JL, et al. Device selection and outcomes of aerosoltherapy: evidence-based guidelines: American College ofChest Physicians/American College of Asthma, Allergy, andImmunology. Chest 2005;127:335e71.
[23] Laube BL, Janssens HM, de Jongh FH, Devadason SG, Dhand R,Diot P, et al. What the pulmonary specialist should know
about the new inhalation therapies. Eur Respir J 2011;37:1308e31.
[24] Fabbri LM, Boschetto P, Mapp CE. Global Initiative for ChronicObstructive Lung D, Global Initiative for Asthma M, Preven-tion. COPD guidelines: the important thing is not to stopquestioning. Am J Respir Crit Care Med 2007;176:527e8.
[25] Papi A, Haughney J, Virchow JC, Roche N, Palkonen S, Price D.Inhaler devices for asthma: a call for action in a neglectedfield. Eur Respir J 2011;37:982e5.
[26] Braunholtz DA, Edwards SJ, Lilford RJ. Are randomized clinicaltrials good for us (in the short term)? Evidence for a trial ef-fect. J Clin Epidemiol 2001;54:217e24.
[27] Vincken W, Dekhuijzen PR, Barnes P, Group A. The ADMITseries e issues in inhalation therapy. 4) How to choose inhalerdevices for the treatment of COPD. Prim Care Respir J 2010;19:10e20.
[28] Clinical practice reseach datalink [database on the Internet,cited 22nd January 2013] Available from: http://www.cprd.com/intro.asp; 2013.
[29] Newman S. Improving inhaler technique, adherence to ther-apy and the precision of dosing: major challenges for pulmo-nary drug delivery. Expert Opin Drug Deliv; 2014 [Epub aheadof print].
[30] Lavorini F, Levy ML, Corrigan C, Crompton G, Group AW.The ADMIT series e issues in inhalation therapy. 6) Trainingtools for inhalation devices. Prim Care Respir J 2010;19:335e41.
[31] Dekhuijzen PN, Magnan A, Kneussl M. The ADMIT series e
issues in inhalation therapy. 1) The goals of asthma treat-ment: can they be achieved? Prim Care Respir J 2007;16:341e8.
[32] Horne R. Compliance, adherence, and concordance: implica-tions for asthma treatment. Chest 2006;130:65Se72S.