Embed Size (px)
Citation preview

Pediatric UrologyPediatric Urology
Horseshoe KidneyHorseshoe Kidney Duplication AnomaliesDuplication Anomalies Ambiguous genitaliaAmbiguous genitalia HydronephrosisHydronephrosis UPJ ObstructionUPJ Obstruction UTI’sUTI’s Tumors (Wilm’s)Tumors (Wilm’s) RefluxReflux
Bladder extrophyBladder extrophy HypospadiusHypospadius Patent UrachusPatent Urachus Painful ScrotumPainful Scrotum Nocturnal EnuresisNocturnal Enuresis CircumcisionCircumcision CryptorchidismCryptorchidism HydrocoelesHydrocoeles

GU AnomaliesGU Anomalies
Abnormal renal/ureteric developmentAbnormal renal/ureteric development Abnormal bladder/urethral developmentAbnormal bladder/urethral development Abnormal testicular developmentAbnormal testicular development

28 days28 days

Abnormalities of renal developmentAbnormalities of renal development
Anomalies of volume and structureAnomalies of volume and structure Anomalies of numberAnomalies of number Anomalies of form and fusionAnomalies of form and fusion Anomalies of ascentAnomalies of ascent Anomalies of rotationAnomalies of rotation

Renal agenesisRenal agenesis
BilateralBilateral
UnilateralUnilateral

Renal agenesisRenal agenesis
BilateralBilateral– Pulmonary hypoplasia-oligohydramniosPulmonary hypoplasia-oligohydramnios– Facial changes “Potter’s facies”Facial changes “Potter’s facies”– Limb anomaliesLimb anomalies
UnilateralUnilateral– 1 in 1100 births1 in 1100 births– Abnormality of ureteral bud rather than metanephrosAbnormality of ureteral bud rather than metanephros– Unilateral adrenal present, abnormality of other Unilateral adrenal present, abnormality of other
mesonephic duct structures (vas deferens)mesonephic duct structures (vas deferens)

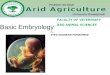
Anomalies of Form and FusionAnomalies of Form and Fusion
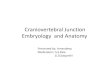
Horseshoe kidney is most common fusion Horseshoe kidney is most common fusion anomalyanomaly
4-64-6thth week gestation week gestation 1 in 4001 in 400 Ureter, kidney tend to be normalUreter, kidney tend to be normal

Horseshoe KidneyHorseshoe Kidney
Common to have other congenital Common to have other congenital anomaliesanomalies

Horseshoe KidneyHorseshoe Kidney
Common to have other congenital Common to have other congenital anomaliesanomalies– Skeletal, cardiovascular, neural tube defects, Skeletal, cardiovascular, neural tube defects,
anorectalanorectal– UPJ obstruction, stones, UTI, hypospadius, UPJ obstruction, stones, UTI, hypospadius,
cryptorchidismcryptorchidism– ? higher chance of renal cancer (Wilm’s)? higher chance of renal cancer (Wilm’s)

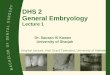
Multicystic Dysplastic KidneyMulticystic Dysplastic Kidney
Most common type of renal cystic diseaseMost common type of renal cystic disease Most common cause of abdominal mass in Most common cause of abdominal mass in
an infantan infant Bunch of grapesBunch of grapes No functioning renal tissueNo functioning renal tissue Atretic ureterAtretic ureter

Multicystic Dysplastic KidneyMulticystic Dysplastic Kidney
Tend to involute through childhoodTend to involute through childhood Higher rate of contralateral renal anomaliesHigher rate of contralateral renal anomalies
– UPJO, vesico-ureteric refluxUPJO, vesico-ureteric reflux Slight but definite risk of Wilm’s tumorSlight but definite risk of Wilm’s tumor

Antenatal HydronephrosisAntenatal Hydronephrosis
~ 0.5-1.0% of antenatal ultrasounds will ~ 0.5-1.0% of antenatal ultrasounds will detect a genitourinary anomalydetect a genitourinary anomaly

Antenatal HydronephrosisAntenatal Hydronephrosis
Differential diagnosisDifferential diagnosis– UPJ obstructionUPJ obstruction– Vesico-ureteric refluxVesico-ureteric reflux– MCDKMCDK– Posterior urethral valvesPosterior urethral valves– UVJ obstructionUVJ obstruction– Primary megaureterPrimary megaureter– Ectopic ureterEctopic ureter– Transient hydronephrosis Transient hydronephrosis

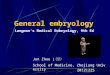
Antenatal Hydronephrosis:Antenatal Hydronephrosis:UPJ ObstructionUPJ Obstruction
UPJO represents a relative narrowing of the UPJO represents a relative narrowing of the proximal ureter impeding drainageproximal ureter impeding drainage
Pain, hematuria, UTI or a flank mass in a Pain, hematuria, UTI or a flank mass in a child or young adultchild or young adult
~ 1/3 kidneys deteriorate and/or develop ~ 1/3 kidneys deteriorate and/or develop complications which require surgerycomplications which require surgery


UPJO TreatmentUPJO Treatment
Surgery if pain, infection or affecting Surgery if pain, infection or affecting function of the kidneyfunction of the kidney– Open, laparoscopic, percutaneousOpen, laparoscopic, percutaneous

Primary Vesicoureteric Reflux Primary Vesicoureteric Reflux
A congenital, abnormal retrograde flow of A congenital, abnormal retrograde flow of urine from bladder to ureter +/‑ kidneyurine from bladder to ureter +/‑ kidney
Results from inadequate length of Results from inadequate length of submucosal ureteric tunnelsubmucosal ureteric tunnel


Pediatric Urinary Tract InfectionsPediatric Urinary Tract Infections
3% girls, 1% boys UTI3% girls, 1% boys UTI 30-40% of children with UTI's have vesicoureteric 30-40% of children with UTI's have vesicoureteric
reflux (VUR)reflux (VUR) ~17% infection-related renal scarring~17% infection-related renal scarring 10-20% with scarring will become hypertensive10-20% with scarring will become hypertensive

Duplication/Ectopic AnomaliesDuplication/Ectopic Anomalies


Ectopic ureterEctopic ureter
Can empty anywhere into Wolfian Can empty anywhere into Wolfian (mesonephric) duct(mesonephric) duct– Prostate, seminal vesical, posterior urethraProstate, seminal vesical, posterior urethra– Epoophoron, Gartner’s duct, vagina, cervixEpoophoron, Gartner’s duct, vagina, cervix
Can cause obstruction of kidney, UTICan cause obstruction of kidney, UTI Incontinence in girlsIncontinence in girls

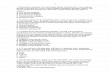
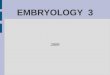
UreterocoeleUreterocoele
Cystic dilation of the terminal ureterCystic dilation of the terminal ureter ? Persistence of Chwalle’s membrane (37 ? Persistence of Chwalle’s membrane (37
days gestation) between ureteric bud and days gestation) between ureteric bud and urogenital sinusurogenital sinus
Often associated with a duplicated Often associated with a duplicated collecting systemcollecting system

DuplicationDuplication
1 in 1251 in 125 Bifid pelvis to complete duplicationBifid pelvis to complete duplication

DuplicationDuplication
Weigert Meyer lawWeigert Meyer law

Anomalies of the bladder and urethraAnomalies of the bladder and urethra

Posterior urethral valvesPosterior urethral valves

Posterior urethral valvesPosterior urethral valves
Variable presentationVariable presentation Renal failure, reflux, bladder dysfunction, Renal failure, reflux, bladder dysfunction,
UTIUTI TreatmentTreatment
– Incision of valvesIncision of valves– Manage secondary problemsManage secondary problems

CryptorchidismCryptorchidism
3.5% of full-term boys3.5% of full-term boys 0.7% of one year olds0.7% of one year olds 0.7% of adults0.7% of adults More common in pre-term babiesMore common in pre-term babies


Why Fix It? Why Fix It?
Histologic changes present by 1 year old Histologic changes present by 1 year old Allows surveillance for malignancyAllows surveillance for malignancy Less prone to trauma Less prone to trauma May enhance fertility potential May enhance fertility potential Fix associated hernia Fix associated hernia CosmesisCosmesis

Cryptorchidism & Malignancy Cryptorchidism & Malignancy
10x more frequent than in normal testes 10x more frequent than in normal testes Approximately 1% life time risk Approximately 1% life time risk The higher the testicle, the greater the risk The higher the testicle, the greater the risk Seminoma most common tumor Seminoma most common tumor Orchidopexy probably doesn't reduce risk Orchidopexy probably doesn't reduce risk
but allows surveillancebut allows surveillance

Hypospadius and EpispadiusHypospadius and Epispadius
HypospadiusHypospadius– 1:300 boys 1:300 boys – Abnormally proximal ventral urethral meatus Abnormally proximal ventral urethral meatus – Deficient foreskin ventrallyDeficient foreskin ventrally– Ventral bend to penis (chordee) Ventral bend to penis (chordee) – Otherwise normally virilized male babiesOtherwise normally virilized male babies– Vast majority not associated with some other Vast majority not associated with some other
endocrinopathy or GU anomalyendocrinopathy or GU anomaly


Hypospadius RepairHypospadius Repair
Usually at 1 year of age + Usually at 1 year of age + Many techniques Many techniques Flaps…tubularized foreskin flaps, local skin Flaps…tubularized foreskin flaps, local skin Grafts…bladder mucosal, buccal mucosal, Grafts…bladder mucosal, buccal mucosal,
skin graftsskin grafts

Abnormalities of sexual Abnormalities of sexual differentiationdifferentiation
Establishment of chromosomal sex at Establishment of chromosomal sex at fertilizationfertilization
Development of gonads into testes or ovaryDevelopment of gonads into testes or ovary Differentiation of internal ducts/external Differentiation of internal ducts/external
genitaliagenitalia– ~ 6 weeks bi-potential of gonadal ridge, ~ 6 weeks bi-potential of gonadal ridge,
gonads, internal ducts and external genitaliagonads, internal ducts and external genitalia


Ambiguous GenitaliaAmbiguous Genitalia
Male pseudohermaphroditismMale pseudohermaphroditism Female pseudohermaphroditismFemale pseudohermaphroditism True hermaphroditismTrue hermaphroditism Mixed gonadal dysgenesisMixed gonadal dysgenesis


True hermaphroditismTrue hermaphroditism
Have both testicular tissue with Have both testicular tissue with seminiferous tubules and ovarian tissue seminiferous tubules and ovarian tissue with follicleswith follicles
Often 2 ovotestesOften 2 ovotestes Variable internal ducts and external Variable internal ducts and external
genitaliagenitalia

Wilms' TumourWilms' Tumour
A malignant childhood renal tumor arising A malignant childhood renal tumor arising from renal blastema containing various from renal blastema containing various stages of normal renal development stages of normal renal development histologically.histologically.
Most common solid abdominal tumor of Most common solid abdominal tumor of childhood.childhood.

Wilms' Tumour Wilms' Tumour
Peak incidence between 2-5 years of agePeak incidence between 2-5 years of age Incidence 8/million Incidence 8/million
– ~ 40 cases per year in Canada~ 40 cases per year in Canada


Wilms' Tumour Wilms' Tumour
Heritable (15‑20%) and non-heritable formsHeritable (15‑20%) and non-heritable forms Unique association with other anomalies:Unique association with other anomalies:
– Cryptorchidism 30/1000Cryptorchidism 30/1000– Renal anomalies 26/1000Renal anomalies 26/1000– Hemi‑hypertrophy 25/1000Hemi‑hypertrophy 25/1000– Aniridia 8/1000Aniridia 8/1000– Hypospadias, 18/1000 Hypospadias, 18/1000

TreatmentTreatment
General approach is surgical excision General approach is surgical excision (nephrectomy) followed by multi-agent (nephrectomy) followed by multi-agent chemotherapy +/- radiotherapychemotherapy +/- radiotherapy
Prognosis based on stage and pathological Prognosis based on stage and pathological subtypesubtype
More than 85% cure rate with current multi-More than 85% cure rate with current multi-modal therapymodal therapy