Embed Size (px)
Citation preview

Group 2
CLASS II MALOCCLUSION

Outline•Definition•Types•Diagnosis•Epidemiology•Treatment•Cases•Future

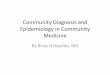
Definition • Class II (or distocclusion) – In this classification, the maxillary first molar is even with, or anterior to, the mandibular first molar; the buccal groove of the mandibular first molar is distal to the mesiobuccal cusp of the maxillary first molar. The distal surface of the mandibular canine is distal to the mesial surface of the maxillary canine by at least the width of a premolar. The facial profile of both divisions is termed retrognathic.

Which one is class II?

Class II Division 1•Class II, Division 1 occurs when the permanent maxillary central incisors are either normal or slightly protruded out toward the lips.

Class II Division 2•Class II, Division 2 occurs when permanent maxillary central incisors are retruded and tilting inwards towards the tongue.

Cephalometric apperance

Diagnosis

Causes•Whatrole does genetics play in the etiology of Class II malocclusions? According to the study by Lundstrom • (1984), investigations published prior to that article have suggested that about 40%of commonanomalies in tooth position and in the relationship between maxil- lary and mandibular dental arches are due to genetic differences between individuals. Corruccini and Potter (1980), in studies of different dental and occlusal vari- ables, found the heritability of dental overjet wasre- duced to zero. Several syndromes have Class II maloc- clusions as a major finding. Of these syndromes, Treacher Collins, hemifacial microsomia, achondropla- • sia, and mobius syndromeare a few of the more widely known. • Inter-arch problems such as Class II and Class III malocclusions are genetic in nature,

Causes• How do habits relate to Class II malocclusions? As •Was previously stated, the light continuous forces are muchmore detrimental to the oral complex than are heavy intermittent forces. Habits such as thumb suck- ing, when performed for fewer than 6 hr per day, have not been shownto be responsible for anterior open bites or Class II malocclusions. Forward positioning of the tongue (seen during swallowing in patients with ante- rior openbite) is morelikely to be an effect than a cause.
• Timothy Shaughnessy, DDS, MS, Workshop Leader Lawrence H. Shire, DDS, Workshop Recorder

Diagnosis and Records• History• Clinical examination• Radiographs• Mounted casts• Photographs

Epidemiology• study were to determine caries prevalence, oral hygiene and orthodontic status of Bedouin children in a desert around Al-Qasseem Region of Saudi Arabia. One hundred and fifty three children were examined for caries, oral hygiene and orthodontic status with mirror and explorer utilizing natural light. • One hundred and fifty one (98.6%) children had class I molar relation and 2 (1.4%) children had class II molar relation. Anterior open bite, anterior crossbite and posterior crossbite were found in one case (0.7%) each.
• Caries prevalence, oral hygiene and orthodontic status of Saudi Bedouin children.•Wyne A1, al-Dlaigan Y, Khan N.

Treatment
Treatment approaches
Preadolescents
Intra oral devices
Extra oral devices
Adult
surgical camouflage

Preadolescence

Preadolecense*Functional appliance
Stimulates and enhances mandibular growth
Ex: activator, bionator, frankel, twin block

Preadolecense*Extra oral force (headgear) :
Retards the maxillary growth

Adults*orthognathic surgeries

Adults*Class II elastics:
Camouflage

Case 1*21-year-old Saudi male was referred to the orthodontic clinic
*“Bothering anterior teeth.”

Treatment
• Pre surgical orthodontic treatment:• Upper and lower first premolars
were extracted to get space for retracting the lower incisors, alleviation of lower arch crowding, uprighting the upper incisors, and severing dental class II relation.
• Surgery:• Le Fort I osteotomy• bilateral sagittal split osteotomy

Post surgical

Post surgical orthodontic treatmentclose minor spaces
final occlusal settling.
8 months

Results

• Case Report
• Surgical Orthodontic Treatment of Severe Skeletal Class II
• Fahad F. Alsulaimani,1 Maisa O. Al-Sebaei,2 and Ahmed R. Afify1
• 1Orthodontic Division, Department of Preventive Dental Sciences, Faculty of Dentistry, King Abdul-Aziz University, Jeddah, Saudi Arabia2Oral and Maxillofacial Surgery Department, Faculty of Dentistry, King Abdul-Aziz University, Jeddah, Saudi Arabia

Class II treatment by cervical headgear

Drag picture to placeholder or click icon to add

Thank you