Embed Size (px)
Citation preview

879
Review
www.expert-reviews.com ISSN 1478-7210© 2010 Expert Reviews Ltd10.1586/ERI.10.76
Gram-negative organisms are a relatively in frequent but important cause of bacterial endocarditis and are associated with significant morbidity and mortality. Infective endocarditis due to Gram-negative organisms is traditionally classified into two main categories: HACEK (Haemophilus species, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens and Kingella species) bacteria and non-HACEK (mostly due to Pseudomonas species and members of the Enterobacteriaceae family) Gram-negative bacilli. While the incidence of HACEK endocarditis has remained relatively unchanged over time [1], recent data suggest a significant shift in epidemiology of non-HACEK Gram-negative endocarditis [2,3]. In this article, we review the changing epidemiology, risk fac-tors and contemporary management of HACEK and non-HACEK Gram-negative endocarditis.
EpidemiologyHACEKGram-positive bacteria remain the pre-dominant causative pathogens for bacte-rial endocar ditis, accounting for nearly 80% of cases. The reported incidence of Gram-negative endocarditis ranges from 1.3 to 10%, with HACEK organisms comprising the bulk of cases [1]. Within the HACEK group, Haemophilus species (Haemophilus parainfluenzae, Haemophilus aphro philus and Haemophilus
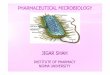
paraphrophilus) are responsible for the majority of endocarditis cases, with Eikenella corrodens being the least common pathogen. Figure 1 sum-marizes the relative distribution of endocarditis caused by various members of the HACEK group based on the review published by Das et al. [4].
Non-HACEKDue to its infrequent occurrence, estimates of non-HACEK Gram-negative endocarditis prevalence are variable and depend on the study period. Historical association of non-HACEK Gram-negative endocarditis with intravenous drug use has limited the scope of earlier studies to certain populations and geographical areas, thus introducing a reporting bias. For instance, the earliest systematic review of Gram-negative endocarditis, conducted from 1945 to 1977, con-centrated on intravenous drug users, reporting the prevalence of endocarditis in this population as 11–32%, with Gram-negative pathogens account-ing for 13% of cases [5]. Similarly, an investiga-tion by Cohen et al. reported 110 cases of Gram-negative endocarditis in intravenous drug users, with Pseudomonas and Serratia species accounting for nearly 80% of cases [5].
Such population selection bias also restricted earlier studies to large metropolitan cities, such as San Francisco (CA, USA), Cleveland (OH, USA), Detroit (MI, USA), Chicago (IL, USA) and New York (NY, USA). Interestingly, the
Sania S Raza1, Omer W Sultan1 and Muhammad R Sohail†1
1Mayo Clinic College of Medicine, Rochester, MN, USA †Author for correspondence:Division of Infectious Diseases, Department of Medicine, Mayo Clinic College of Medicine, Rochester, MN 55905, USA Tel.: +1 507 255 7938 Fax: +1 507 255 7767 [email protected]
Gram-negative endocarditis due to HACEK bacteria (Haemophilus species, Actinobacillus, Cardiobacterium, Eikenella and Kingella species) and non-HACEK organisms is an infrequent occurrence but is associated with significant morbidity and mortality. Traditionally, non-HACEK Gram-negative endocarditis has been associated with injection drug use. However, emerging data from more contemporary cohorts suggest changing epidemiology and risk factors for Gram-negative endocarditis, necessitating an updated review of this subject. Moreover, optimal management, including the need for surgical intervention, and strategies for the prevention of Gram-negative endocarditis need to be revisited.
Keywords: bacilli • endocarditis • Gram-negative • HACEK • management • recommendations
Gram-negative bacterial endocarditis in adults: state-of-the-heartExpert Rev. Anti Infect. Ther. 8(8), 879–885 (2010)
For reprint orders, please contact [email protected]
Exp
ert R
evie
w o
f A
nti-
infe
ctiv
e T
hera
py D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsid
ad d
e Se
villa
on
12/0
2/14
For
pers
onal
use
onl
y.

Expert Rev. Anti Infect. Ther. 8(8), (2010)880
Review
microbiology of endocarditis pathogens was associated with the profile of intravenous drugs used in different geographical loca-tions. Levine et al. reported a higher prevalence of pseudomonal endocarditis in Detroit among patients injecting pentazocine and tripelennamine, whereas Serratia species were responsible for two-thirds of cases of Gram-negative endocarditis in San Francisco [5,6].
Recent data published by the International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS) sheds new light on the contemporary epidemiology of Gram-negative endo-carditis [3]. This cohort included cases from 61 centers in 28 coun-tries between 2000 and 2005, presenting a unique opportunity to review the changing epidemiology of Gram-negative endo-carditis. In their study, the reported incidence of non-HACEK Gram-negative endocarditis was near 2%, with the majority of cases caused by Escherichia coli (29%) and Pseudomonas (22%). Europe had the highest prevalence of non-HACEK Gram-negative endocarditis (53%, compared with 22% in North America). Other causative pathogens included Klebsiella (10%) and Serratia (8%) species. In another recent review, commonly reported pathogens for Gram-negative endocarditis also included Salmonella, Enterobacter, Proteus, Providencia and Citrobacter species [1].
Risk factors HACEKThe HACEK organisms are grouped together due to their oro-pharyngeal inhabitancy, fastidious nature of pathogenesis and special media requirement for isolation [7]. These pathogens also share common risk factors for endocarditis, particularly poor dental hygiene and recent dental procedures, thus gaining entry to the vascular compartment at the time of local trauma or infection [4]. Another well-recognized predisposing factor for HACEK endocarditis includes pre-existing valvulopathy that
facilitates bacterial adherence to the dam-aged endothelium. Owing to the nature of their pathogenesis, these risk factors for HACEK endocarditis have remained unchanged over several decades. Literature reviews from 1945 to 1977 illustrated similar risk factors including dental work, dental infection and upper respiratory tract infection as the predisposing event in the majority of HACEK endocarditis cases. Not surprisingly, the bulk of the patients also had degenerative heart disease [5]. Although the incidence of HACEK endo-carditis is quite low, it remains an important concern, especially with changing demo-graphic patterns. Increasing lifespan and a growing proportion of the elderly popula-tion is resulting in more degenerative valve diseases and placement of prosthetic heart valves, thus predisposing these patients to a higher likelihood of endocarditis [8].
Non-HACEKHistorically, endocarditis due to non-HACEK Gram-negative pathogens was regarded as a disease of intravenous drug users. Over the last decade, however, an increased incidence has been reported in prosthetic heart valve recipients and patients with cirrhosis [9]. A recent ana lysis by the ICE-PCS registry has shed more light on the changing profile of Gram-negative endocar-ditis, revealing that more than half of the patients with non-HACEK endocarditis (57%) had healthcare-associated infec-tions whereas injection drug use was rare (4%). Furthermore, the study confirmed previous reports of a rising incidence of non-HACEK Gram-negative endocarditis in patients with implanted endovascular devices, including prosthetic heart valves, perma-nent pacemakers and implantable cardioverter-defibrillators [3]. Given these findings, one should be cognisant of non-HACEK endocarditis in non-intravenous drug users and in patients with endovascular devices.
Recent data also suggest that diminished host immune status may serve as an additional risk factor for endocarditis with this group of pathogens [10,11]. Although non-HACEK organ-isms account for the majority of Gram-negative bacteremias, hemato genous seeding of the cardiac valves with resultant endo-carditis remains an infrequent event. This is probably due to their high sensitivity to serum bactericidal activity and low propensity to adhere to damaged endothelium. Exceptions to this general rule include Salmonella, possibly due to its abil-ity to bind, invade and proliferate in the normal endothelium and lymphoid tissue, and Pseudomonas, with its capability to produce and survive in a biofilm [10]. The importance of host immune status in preventing Gram-negative bacterial endo-carditis was highlighted in a study by Aubron et al. [10], who reported a higher incidence of Enterobacteriaceae endocarditis in immunocompromised patients (nearly 30% of all endocarditis
42%
20%
27%
4%7%
Haemophilus species
Actinobacillus actinomycetemcomitans
Cardiobacteriumhominis
Eikenella corrodens
Kingella kingae
Figure 1. Relative frequencies of infective endocarditis caused by HACEK microorganisms.
Raza, Sultan & Sohail
Exp
ert R
evie
w o
f A
nti-
infe
ctiv
e T
hera
py D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsid
ad d
e Se
villa
on
12/0
2/14
For
pers
onal
use
onl
y.

www.expert-reviews.com 881
Review
cases). Furthermore, HIV infection was noted as a predisposing factor for non-HACEK Gram-negative endocarditis, especially in cases due to Salmonella species.
Besides immunocompromised host status, other potential risk factors for non-HACEK Gram-negative endocarditis may include age and gender. Although the reported incidence of endocarditis is higher in males, a recent investigation by Dhawan demon-strated an increased rate of non-HACEK Gram-negative endo-carditis in elderly females, particularly with respect to E. coli, with the male:female ratio approaching 10:26 (72.2% females) [12]. Purported factors for predilection of Gram-negative endocar-ditis in this group of patients include altered vaginal mucosa and diabetes mellitus in this age group that further predispose them to urinary tract infections, which in turn may serve as a source of bacterial entry in the bloodstream and hematogenous seeding of the valves. This hypothesis was further supported by a study by Meyers et al., where they found that the urinary tract was the most common portal of entry for the majority (75%) of elderly patients (>70 years of age) with native valve bacterial endocarditis [13].
These examples highlight the importance of host immune defenses in protecting against Gram-negative endocarditis. With a changing demographic profile, notably a growing elderly population, and increasing rates of diabetes and other immuno-suppressive conditions (HIV, malignancies and autoimmune diseases), a higher incidence of non-HACEK endocarditis in immunocompromised patients is anticipated.
Clinical presentationHACEKDue to the fastidious nature of the organisms and nonspecific symp-toms, diagnosis of HACEK endocarditis may be delayed for several weeks. Symptoms may include fever, night sweats, anorexia, back pain and weight loss, with or without peripheral stigmata of infective endocarditis [1]. However, fever may be absent in elderly and immu-nocompromised patients [8]. The second major obstacle in mak-ing an early and accurate diagnosis of HACEK endocarditis is the requirement of special culture media and laboratory techniques for isolation. Historically, a longer incubation period was required for isolating HACEK organisms due to their slower growth. However, recent utilization of modern laboratory techniques has increased the yield of HACEK organisms with a standard 5–7 days of incuba-tion, thereby potentially diminishing the requirement for prolonged incubation [14]. A high index of suspicion and consultation with microbiology laboratory staff may increase the likelihood of isolat-ing HACEK organisms in suspected cases. Growth characteristics of HACEK organisms are summarized in Table 1.
Owing to frequent delay in diagnosis, HACEK organisms are also associated with a high rate of peripheral embolization, with reported rates ranging from 30 to 40% [4,7]. Of these, cer-ebral emboli and mycotic aneurysms are particularly concerning. Mycotic aneurysms may be clinically silent until they rupture. A CT or MRI scan of the head should be considered, especially if surgery is being planned. Cardiac surgery requires intra-operative heparinization and predisposes to risk of hemorrhagic transformation if clinically silent ischemic infarcts are present.
Among the HACEK organisms, Haemophilus and Actinobacillus species usually run a subacute course with a higher rate of periph-eral embolization (50%) and larger sized cardiac vegetation on echocardiography [7,15,16]. Infection with Cardiobacterium hominis is almost exclusively associated with endocarditis, especially in the setting of damaged cardiac valves. This organism is also notori-ous for an insidious course due to its markedly slower growth as compared with other HACEK pathogens. In fact, as part of the normal respiratory flora, it is usually overgrown by other organ-isms. The average duration of symptoms preceding diagnosis of C. hominis endocarditis is reported to be 138 days [1]. Kingella, responsible for 7% of HACEK endocarditis, is observed in all age groups, including children [7,17]. Unlike other HACEK pathogens, endocarditis caused by this organism can have a rapid progression. E. corrodens, best known for causing infections after human bites, is the least common cause of HACEK endocarditis. Interestingly, endocarditis caused by this pathogen has been associated with intra-venous drug users who lick needles thus allowing oropharyngeal contamination [1,18].
Non-HACEKFever remains the most common finding and first symptom in non-HACEK Gram-negative endocarditis. However, the duration of symptoms and severity of disease may vary depending on the particular pathogen and comorbid conditions of the patient [10]. ICE-PCS investigators reported time from onset of symptoms to clinical diagnosis as greater than 1 month in 90% of the cases of non-HACEK Gram-negative endocarditis [3].
Patients with E. coli endocarditis tend to be older with more debilitating illnesses. Understandably, mortality associated with non-HACEK Gram-negative endocarditis is also higher as con-firmed by several studies [3,13,19]. In the majority of these patients, presumed sources of acquisition include the genitourinary tract and non-oral gastrointestinal (GI) tract [3,19]. Consequently, persistent bacteremia in elderly patients with urinary tract and/or GI Gram-negative pathogens should raise the possibility of non-HACEK endocarditis.
Owing to its pathogenesis and virulence factors, pseudomonal endocarditis affects native as well as prosthetic valves. Although pre-vious studies reported a predominance of right heart involvement, a higher incidence of left-sided endocarditis was noted at the begin-ning of 1980, perhaps pointing to evolution of demographic charac-teristics and risk factors associated with pseudomonal endocarditis [20]. When affecting the left side, the disease has an acute course with a mean duration of illness from onset to diagnosis reported as 15 days, and a significantly higher rate of complications including peripheral embolization (40%), congestive heart failure, valve-ring abscesses, splenic abscesses and neurological sequelae (53% in older studies) [20]. As expected, mortality is high, ranging from 69% in earlier published series to 10% in more contemporary cohorts with improved medical and surgical therapies [20–22]. Although earlier studies had noted a mortality benefit with surgical intervention, Reyes et al. reported no significant difference in outcome between medical treatment alone versus combined medicosurgical interven-tion between the 1969–1975 and 2006–2008 time periods [21]. This
Gram-negative endocarditis
Exp
ert R
evie
w o
f A
nti-
infe
ctiv
e T
hera
py D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsid
ad d
e Se
villa
on
12/0
2/14
For
pers
onal
use
onl
y.

Expert Rev. Anti Infect. Ther. 8(8), (2010)882
Review
could perhaps be explained by introduction of fourth-generation cephalosporins, such as cefepime, with enhanced potency and higher affinity against Gram-negative pathogens [21].
Salmonella species remain a rare cause of non-HACEK endocar-ditis (0.2–0.4%). However, when present, they are very destructive, with an increasing rate of valve-ring abscess, valve perforations, cusp rupture and peripheral embolization. Mortality associated with Salmonella aortitis and endocarditis remains high (40–45%), especially in infants, adults older than 50 years and patients with comorbid condition [11]. Because infection caused by Salmonella can take different forms (ranging from febrile illness and gastro-enteritis to bacteremia and endovascular infections), diagnosis of Salmonella endocarditis remains hindered, requiring a high level of suspicion. Another factor is the relative inadequacy of transthoracic echocardio graphy for diagnosing bacterial endocarditis [11]. Due to the aggressive nature of this disease, patients suspected of Salmonella bacteremia should undergo further investigation to delineate under-lying endovascular infection in the appropriate clinical setting, especially known cardiac valvulopathy and vascular aneurysms.
In summary, endocarditis with non-HACEK Gram-negative bacilli should be a consideration in patients with history of injec-tion drug use or bacteremia in the setting of pre-existing valvulo-pathy, cardiovascular implantable electronic devices (pacemakers and defibrillators) and prosthetic heart valves or vascular grafts. Furthermore, elderly patients with several comorbid conditions, immunocompromised status, and recent GI and/or genitourinary infection with persistent bacteremia also merit further investigation for non-HACEK endocarditis. Peripheral vascular or immunologic phenomena are present in only a third of the cases. Consequently, a lack of peripheral manifestations should not dissuade clinicians from consideration of bacterial endocarditis in the above scenario.
Role of echocardiographyTransthoracic echocardiogram has a low sensitivity for detection of smaller vegetations, perivalvular extension of endocarditis and myocardial abscesses, especially in patients who are obese, have chronic obstructive pulmonary disease or chest wall deformi-ties, and those with prosthetic heart valves [8]. Consequently,
Table 1. Characteristic features of infective endocarditis due to HACEK microorganisms.
Organism Growth characteristics
Epidemiology Valvular involvement Comments
Haemophilus species • Pleomorphic Gram-negative coccobacilli
• Require X (hemin) and/or V (nicotinamide adenine dinucleotide) factors for growth
• Responsible for 0.5–1% of all cases of IE
• Haemophilus aphrophilus is the most common species responsible for IE cases. The majority of IE cases are presumably secondary to dental pathology, followed by otitis media or sinusitis
• Mitral and aortic valves are most commonly involved
• Majority of patients (50–80%) have underlying valvular disease
• Peripheral embolization reported in 30–50% of cases. IE cases due to Haemohphilus parainfluenzae may have an acute presentation
Actinobacillus actinomycetemcomitans
• Grow in trypticase soy broth
• Periodontal disease is the most frequently cited risk factor
• Aortic valve involved in 60% of cases, followed by mitral valve (30%)
• Prosthetic valve IE reported in 25% of cases
• Peripheral embolization reported in 40% of cases
Cardiobacterium hominis
• Gram-negative or Gram-variable pleomorphic rods
• Bulbous swelling of both ends is a characteristic feature
• Only isolated in IE cases • Mitral valve involved in 45% of IE cases followed by aortic valve (35%)
• Majority (75%) of the patients have underlying valvular disease
• Arterial embolization reported in 40% of cases
Eikenella corrodens • Gram-negative pleomorphic rods
• Corrodes (or pit) the agar during growth
• Colonies produce chlorine bleach odor
• Associated with IE in injection drug users (especially those who lick the needles before injecting drugs or ‘clean’ the venipuncture site with saliva)
• Mostly in patients with pre-existing valvular disease
• May be associated with septic pulmonary emboli
Kingella species • Small Gram-negative coccobacilli
• May cause pitting of the agar during growth
• Kingella kingae is the most common species isolated in IE cases
• Extremely rare
• Aortic and mitral valve are mostly involved
• Unlike other HACEK microorganisms, IE due to Kingella species can have rapid progression
HACEK microorganisms: Haemophilus species, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens and Kingella species.IE: Infective endocarditis.
Raza, Sultan & Sohail
Exp
ert R
evie
w o
f A
nti-
infe
ctiv
e T
hera
py D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsid
ad d
e Se
villa
on
12/0
2/14
For
pers
onal
use
onl
y.

www.expert-reviews.com 883
Review
transesophageal echocardiography (TEE) should be performed in all cases of suspected Gram-negative bacterial endocarditis and resultant complications. Intracardiac abscesses were reported in 25% of the patients with non-HACEK Gram-negative endocar-ditis in the ICE-PCS registry, while paravalvular complications were noted in 31% of cases [3]. TEE also provides better visualiza-tion of vegetations attached to pacemaker or defibrillator leads in cases of device-related Gram-negative endocarditis [23].
ManagementHACEKHistorically, b-lactam antibiotics such as penicillin or ampicillin, with or without the addition of aminoglycoside, were considered the drugs of choice for HACEK endocarditis. However, more recent data suggest an increasing frequency of b-lactamase-producing pathogens in the HACEK group [9,24]. Current practice guidelines from the American Heart Association (AHA) recommend empiric treatment with a third-generation cephalosporin (e.g., ceftriaxone 2 g intraveously or intramuscularly every 24 h) or ampicillin–sulbactam (12 g every 24 h in four equally divided doses) as the first line of therapy for HACEK endocarditis [9]. The recommended duration of therapy is 4 weeks. Alternative treatment options include the use of fluoroquinolones (e.g., ciprofloxacin 500 mg orally every 12 h or 400 mg intravenously every 12 h) in patients who are allergic to or unable to tolerate cephalosporins and ampicillin. However, AHA guidelines caution that use of fluoroquinolones should be avoided in patients younger than 18 years of age.
Non-HACEKCardiac surgery has traditionally been recommended as a corner-stone of therapy for non-HACEK, especially Pseudomonas, endo-carditis because of the high mortality associated with conservative medical management. However, in a more contemporary cohort of non-HACEK endocarditis reported by ICE-PCS investigators [3], the mortality rate did not statistically differ between patients who received medical therapy alone compared with those receiving com-bined medical and surgical intervention. In their study, in-hospital mortality rate remained high (24%) despite higher rates of cardiac surgery (51%). Most patients (63%) received combined antibi-otic therapy with a b-lactam plus aminoglycoside and/or fluoro-quinolone, while 38% received monomicrobial treatment. Once again, there was no difference in outcome among patients receiving single as opposed to combination antibiotic therapy with amino-glycosides [3]. However, one major limitation of this investigation was the lack of follow-up and outcome data after hospital discharge.
We recommend a thorough evaluation of patients with non-HACEK Gram-negative endocarditis to assess the necessity of surgical intervention. Decision to treat medically versus combined medical and surgical treatment should be individualized and made on a case-by-case basis. Patients with TEE evidence of valve perfora-tion, chordae tendineae rupture, intra-cardiac abscesses or paraval-vular extension of infection should be promptly referred for surgical evaluation. In addition, traditionally described indications for valve surgery such as worsening heart failure, persistently positive blood cultures and isolation of multidrug-resistant Gram-negative bacteria
may be additional considerations for cardiac surgery. Whether the large size of the vegetation (>1 cm) or location (anterior mitral leaflet) alone are indications for valve replacement surgery in bacterial endocarditis remains a subject of debate. Recurrent embolization during appropriate antimicrobial therapy also warrants surgical consultation.
PreventionFor the last few decades, antimicrobial prophylaxis before invasive dental procedures was considered a crux of preventing bacterial endocarditis from oropharyngeal organisms, in particular the viridian group streptococci and HACEK organisms, in a variety of cardiac valvulopathies. However, these recommendations were based on small, uncontrolled studies and personal anecdotes. With more contemporary and better designed population-based studies, the routine use of antibiotic prophylaxis before dental procedures has come under question. A recent study by Lockhart et al. dem-onstrated a higher incidence of bacteremia from daily tooth brush-ing than after ‘periodic’ dental procedures [25]. Others have also demonstrated frequent bacteremias from activities of daily life such as chewing food, urinating, defecating and tooth brushing. Based on these data, the AHA revised their guidelines for endocarditis prophylaxis in a statement published in 2008 [26]. Revised practice guidelines place greater emphasis on optimal oral hygiene over prophylactic antibiotics for dental procedure. Use of antimicrobial prophylaxis is now reserved for certain high-risk situations that include presence of prosthetic heart valves, previous history of infective endocarditis, uncorrected or recently corrected congeni-tal cardiac defects and development of cardiac valvulopathy after cardiac transplantation. However, no clinical data or guidelines are available for prevention of non-HACEK Gram-negative bacilli endocarditis during GI or genitourinary procedures.
Expert commentary & five-year viewThis article illustrates that, although epidemiology and man-agement of HACEK group endocarditis has remained relatively unchanged over time, fundamental changes are needed in our understanding of non-HACEK Gram-negative endocarditis. First, healthcare contact now represents a primary risk factor for acquisition of Gram-negative endocarditis due to these organ-isms. Historically, non-HACEK Gram-negative endocarditis has remained an infrequent diagnosis and one postulate for this relative rarity is extreme serum sensitivity of Gram-negative pathogens to complement-mediated bactericidal activity which, in turn, reduces the possibility of bacteremia from distant sources to persist long enough to colonize the endocardium. However, with the growing size of the elderly population with degenerative valve diseases, an increased rate of immuno suppression and a rising incidence of pros-thetic valve implantations, we anticipate an increase in incidence of non-HACEK Gram-negative bacterial endocarditis in the future.
Second, while surgery was considered the cornerstone of therapy for non-HACEK Gram-negative endocarditis in earlier reported series, recent data from the ICE-PCS study challenge the conventional practice of routinely referring these patients for surgical intervention [3]. It is quite possible that a subset of patients who do not have cardiac complications on TEE (such as valve
Gram-negative endocarditis
Exp
ert R
evie
w o
f A
nti-
infe
ctiv
e T
hera
py D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsid
ad d
e Se
villa
on
12/0
2/14
For
pers
onal
use
onl
y.

Expert Rev. Anti Infect. Ther. 8(8), (2010)884
Review
perforation, dehiscence, severe regurgitation, intracardiac abscess or para valvular extension of infection) may be managed conserva-tively with antimicrobial therapy alone. These patients should be monitored carefully as surgery may be needed if bacteremia does not clear or if they develop symptomatic heart failure that would require surgical intervention. Unfortunately, the ICE-PCS study did not provide long-term follow-up after discharge from hospital. Therefore, it is conceivable that some of these patients may develop valvular dysfunction or symptomatic heart failure as a late complication and require surgical intervention.
Third, the benefit of dual antibacterial therapy for non-HACEK Gram-negative endocarditis must be re-examined. Combination antibiotic therapy for severe Gram-negative infections, especially Pseudomonas bacteremia and endocarditis, has been a long standing paradigm in infectious diseases for several reasons: to have syner-gistic action based on each agent’s distinct mechanism of action; to amplify the extent and rapidity of killing; and to prevent emer-gence of resistance to one of the agents used in combination. A combination of cell-wall active agents (such as b-lactams) and low-dose aminoglycosides has been historically used to achieve rapid killing of Gram-negative bacteria, especially Pseudomonas bloodstream infection. Once again, data from the ICE-PCS study did not demonstrate an advantage of combination antibacterial therapy for non-HACEK Gram-negative endocar ditis over treat-ment with a single effective agent. However, caution must be exer-cised to avoid overinterpretation of their data. The ICE-PCS study
was a prospective observational study and was not designed or powered to show a superiority of combination antibiotic therapy over monotherapy. Moreover, several other factors such as presence or absence of cardiac and metastatic complications, surgical versus conservative medical therapy, antimicrobial susceptibility profile of the causative Gram-negative pathogen and comorbid conditions of the host, influence the outcome of endocarditis in these cases. We believe that combination anti microbial therapy should be used in the earlier phase of treatment while awaiting antimicrobial sus-ceptibility testing of the causative pathogens. However, once the bloodstream clears the pathogen and drug susceptibility data are available, completing the treatment course with a single drug may be adequate. Ideally, these management issues should be exam-ined in large, well-controlled and randomized prospective clinical trials. However, considering the rarity of non-HACEK Gram-negative endocarditis, such trials are unlikely to be performed in the near future and therapy must be guided by expert opinion and consultation with infectious diseases specialists for individual cases.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Key issues
• Healthcare contact is an emerging risk factor for non-HACEK Gram-negative endocarditis. Injection drug use is a relatively infrequent cause of endocarditis in this group of patients in more contemporary cohorts.
• All patients with suspected Gram-negative endocarditis should undergo transesophageal echocardiography (TEE) to confirm the diagnosis and assess for cardiac complications such as intracardiac abscesses and paravalvular extension of infection.
• Transthoracic echocardiogram has low sensitivity and, if negative, should be followed by TEE to exclude endocarditis.
• Not all cases of non-HACEK Gram-negative bacterial endocarditis necessarily require surgical intervention. Indications for surgical intervention in patients with Gram-negative endocarditis are similar to those with endocarditis due to Staphylococcus aureus.
• Combination antibacterial therapy does not necessarily result in better outcomes in patients with non-HACEK, especially Pseudomonas, endocarditis.
• Patients with native or prosthetic valve HACEK endocarditis can be managed with a single agent administered intravenously for 4 weeks.
• Good oral hygiene is considered the mainstay of preventing HACEK endocarditis from a dental source and routine use of antimicrobial prophylaxis is not recommended.
• Antimicrobial prophylaxis for prevention of HACEK bacterial endocarditis before invasive dental procedures should be reserved for selected high-risk patients with prosthetic heart valves, previous history of endocarditis, uncorrected congenital heart defects and those who develop valvulopathy after cardiac transplant.
• All patients with Gram-negative bacterial endocarditis should be managed in consultation with an infectious diseases specialist.
ReferencesPapers of special note have been highlighted as:• of interest
1 Reyes MP, Reyes KC. Gram-negative endocarditis. Curr. Infect. Dis. Rep. 10(4), 267–274 (2008).
• AuthorsreviewthepublishedliteratureregardingGram-negativeendocarditisandreporttheirinstitutionalexperiencefrom2005to2007.
2 Lampe AS, Schroijen MA, Smith SJ. Endocarditis due to Aggregatibacter (formerly: Actinobacillus) actinomycetemcomitans, a bacterium that grows in characteristic star-shaped colonies. Nederlands Tjdschrift Vor Gneeskunde 52(14), 827–830 (2008).
3 Morpeth S, Murdoch D, Cabell CH et al. Non-HACEK Gram-negative bacillus endocarditis. Ann. Int. Med. 147(12), 829–835 (2007).
• DatafromanInternationalCollaborationonInfectiveEndocarditisProspectiveCohortStudy(ICE-PCS).Authorsreportthatnon-HACEK Gram-negativeendocarditisisnolongeradiseaseofinjectiondrugusersandthatmostcasesincontemporarypracticeareassociatedwithhealthcarecontact.Asignificantproportionofthesepatientshadimplantedendovasculardevices.Mortalityremainedhigh,despiteahighrateofsurgicalintervention.
Raza, Sultan & Sohail
Exp
ert R
evie
w o
f A
nti-
infe
ctiv
e T
hera
py D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsid
ad d
e Se
villa
on
12/0
2/14
For
pers
onal
use
onl
y.

www.expert-reviews.com 885
Review
4 Das M, Badley AD, Cockerill FR, Steckelberg JM, Wilson WR. Infective endocarditis caused by HACEK microorganisms. Ann. Rev. Med. 48, 25–33 (1997).
• AuthorsreportMayoClinicexperiencerelatedtoHACEK endocarditis.ResultssupporttheproposedpathogenesisofHACEKendocarditisandtheoropharyngealoriginofbacteremiainthemajorityofcases.Survivalremainedhighdespitealongdelay(severalweeks)betweensymptomonsetanddiagnosisofendocarditisinasignificantproportionofcases.
5 Cohen PS, Maguire JH, Weinstein L. Infective endocarditis caused by Gram-negative bacteria: a review of the literature, 1945–1977. Prog. Cardiovasc. Dis. 22(4), 205–242 (1980).
6 Levine DP, Crane LR, Zervos MJ. Bacteremia in narcotic addicts at the Detroit Medical Center. II. Infectious endocarditis: a prospective comparative study. Rev. Infect. Dis. 8(3), 374–396 (1986).
• MultiplevalveinvolvementwasmostcommoninpatientswithPseudomonas endocarditis.
7 Feder HM Jr, Roberts JC, Salazar JC, Leopold HB, Toro-Salazar O. HACEK endocarditis in infants and children: two cases and a literature review. Pediatr. Infect. Dis. J. 22(6), 557–562 (2003).
8 Mylonakis E, Calderwood SB. Infective endocarditis in adults. N. Engl. J. Med. 345(18), 1318–1330 (2001).
9 Baddour LM, Wilson WR, Bayer AS et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation 111(23), e394–e434 (2005).
10 Aubron C, Charpentier J, Trouillet JL et al. Native-valve infective endocarditis caused by Enterobacteriaceae: report on 9 cases and literature review. Scand. J. Infect. Dis. 38(10), 873–881 (2006).
11 Mutlu H, Babar J, Maggiore PR. Extensive Salmonella enteritidis endocarditis involving mitral, tricuspid valves, aortic root and right ventricular wall. J. Am. Soc. Echocardiogr. 22(2), 210.e1–210.e3 (2009).
12 Dhawan VK. Infective endocarditis in elderly patients. Clin. Infect. Dis. 34(6), 806–812 (2002).
• Elderlypatientsfrequentlypresentwithatypicalfindingsandahighindexofsuspicionisnecessarytomakeanaccuratediagnosisofendocarditisinthispatientpopulation.
13 Meyers BR, Sherman E, Mendelson MH et al. Bloodstream infections in the elderly. Am. J. Med. 86(4), 379–384 (1989).
14 Baron EJ, Scott JD, Tompkins LS. Prolonged incubation and extensive subculturing do not increase recovery of clinically significant microorganisms from standard automated blood cultures. Clin. Infect. Dis. 41(11), 1677–1680 (2005).
• Contrarytocommonlyheldbelief,mostHACEKorganismscanberecoveredfrombloodculturesafterastandard5-dayincubationperiod.Specializedmethodsaremoreimportantthanextendedincubationforrecoveryofthesefastidiouspathogens.
15 Berbari EF, Cockerill FR 3rd, Steckelberg JM. Infective endocarditis due to unusual or fastidious microorganisms. Mayo Clin. Proc. 72(6), 532–542 (1997).
16 Nwaohiri N, Urban C, Gluck J, Ahluwalia M, Wehbeh W. Tricuspid valve endocarditis caused by Haemophilus parainfluenzae: a case report and review of the literature. Diagn. Microbiol. Infect. Dis. 64(2), 216–219 (2009).
17 Dubnov-Raz G, Scheuerman O, Chodick G, Finkelstein Y, Samra Z, Garty BZ. Invasive Kingella kingae infections in children: clinical and laboratory characteristics. Pediatrics 122(6), 1305–1309 (2008).
18 Krcmery V, Demitrovicova A, Hricak V, Kisac P. Endocarditis due to Gram-negative bacteria. Int. J. Infect. Dis. DOI: 10.1016/j.ijid.2009.08.022 (2010) (Epub ahead of print).
• Authorsreport42casesofGram-negativeendocarditisfromSlovakia.MortalityinthisgroupofpatientswascomparabletoendocarditiscausedbyGram-positiveorganisms.
19 Micol R, Lortholary O, Jaureguy F et al. Escherichia coli native valve endocarditis. Clin. Microbiol. Infect. 12(5), 401–403 (2006).
20 Komshian SV, Tablan OC, Palutke W, Reyes MP. Characteristics of left-sided endocarditis due to Pseudomonas aeruginosa in the Detroit Medical Center. Rev. Infect. Dis. 12(4), 693–702 (1990).
21 Reyes MP, Ali A, Mendes RE, Biedenbach DJ. Resurgence of Pseudomonas endocarditis in Detroit, 2006–2008. Medicine 88(5), 294–301 (2009).
22 Mocchegiani R, Nataloni M. Complications of infective endocarditis. Cardiovasc. Hematol. Disord. Drug Targets 9(4), 240–248 (2009).
23 Sohail MR, Uslan DZ, Khan AH et al. Infective endocarditis complicating permanent pacemaker and implantable cardioverter-defibrillator infection. Mayo Clin. Proc. 83(1), 46–53 (2008).
24 Dall L, Barnes WG, Gibbs HR, Nohinek B, Zee-Cheng CS. Endocarditis caused by b-lactamase-producing Haemophilus influenzae. South. Med. J. 80(3), 405–406 (1987).
25 Lockhart PB, Brennan MT, Sasser HC, Fox PC, Paster BJ, Bahrani-Mougeot FK. Bacteremia associated with toothbrushing and dental extraction. Circulation 117(24), 3118–3125 (2008).
• Randomized,doubleblind,placebo-controlledstudyof290subjects.Authorsconcludethatdailytoothbrushingmaybeagreaterriskfactorforbacteremiaandendocarditisinpatientswithpre-existingvalvulopathycomparedwithoccasionaldentalextraction.
26 Nishimura RA, Carabello BA, Faxon DP et al. ACC/AHA 2008 guideline update on valvular heart disease: focused update on infective endocarditis: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Catheter Cardiovasc. Interv. 72(3), E1–E12 (2008).
Gram-negative endocarditis
Exp
ert R
evie
w o
f A
nti-
infe
ctiv
e T
hera
py D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsid
ad d
e Se
villa
on
12/0
2/14
For
pers
onal
use
onl
y.