Embed Size (px)
Citation preview

Graft vs Host Disease
• Remains the major cause of treatment related morbidity and mortality in allogeneic HCT.
• Caused by donor derived alloreactive T cells.• B cells may also play a critical role in GVHD
pathophysiology.• Chronic GVHD linked most closely with the
beneficial GVT response.

Approaches to the Prevention of GVHD
• Pharmacologic– CNI/MTX– CNI/MTX vs Rapa/CNI – RAPA/MMF– Post transplant cyclophosphamide
• Graft source– BM, PBPC, UCB
• T Cell depletion– CD34 Selection– ATG, Campath
• Immune regulatory mechanisms– Treg – NK-T – MSCs

BMT CTN 0402:Phase 3 Randomized Multicenter Trial comparing Sirolimus/tacrolimus vs
Tacrolimus/MTX for Acute GVHD Prophylaxis
• Primary Objective• Compare rates of acute grade 2-4 GVHD survival after HLA-
matched sibling allogneic HCT
• Secondary Objectives• 1 year relapse-free and overall survival• Incidence of grade 3-4 acute GVHD• Incidence of chronic GVHD• Neutrophil and platelet engraftment• Infection incidence• VOD incidence

BMT CTN 0402:Tac/Sir vs Tac/MTX for aGVHD Prophylaxis
Accrual completed Oct, 2011
• Age 2 – 60 yo• Diagnoses:
• Low risk: AML,ALL CML, MDS• HLA matched sibling
RANDOMIZE
Tacrolimus/Sirolimus
n= 156
Tacrolimus/ MTX
n= 156
Prep regimens allowed:- TBI/VP16 or TBI/Cy
HCT

Acute GVHD
Chronic GVHD
Randomized Trial Incorporating F-ATG in URD Allogeneic Transplants
Finke et al. Lancet Oncology 10:855, 2009

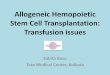
Cumulative incidence of extensive chronic GVHD by treatment groups overall and by prognostic subgroups.
Socié G et al. Blood 2011;117:6375-6382
©2011 by American Society of Hematology

TLI/ATG Reduced Intensity Conditioning
• Animal studies have demonstrated that novel conditioning with TLI/ATS results in protection from GVHD
• Pillai et al. J Immunol 178:6241, 2007 • Pillai et al. Blood 113:4458, 2009
• Translation to the clinic demonstrating low acute GVHD incidence and severity and low TRM
• Lowsky et al. N. Engl. J Med 353:1321, 2005• Kohrt et al. Blood 114:1099, 2009

Host NK T cells
Host T cell
TLI +
ATG
CD1d
InvariantTCR
APC
IL-4
Naïve donor CD4 and CD8 T cells
CD4+CD25+ donor Treg
Polarized donor Th2 cell
IL-4
GVHD
Donor HSC
HOST CELLS DONOR GRAFT
+
+

TLI and ATG Conditioning
ATG 1.5 mg/kg/day
Day 0
Day 180
Days -11 to -7
CSA
MMF
TLI 800 cGy over 10 fractionsDays -4 to -1Days -11 to -7
Infection ProphylaxisHSV: if +ve acyclovir 400 mg BIDCMV: blood PCR weeklyEBV: blood PCR every 2 weeksPCP: Septra DS BID weekends D+42Fungus: if prior infection or URD

Related Donors Unrelated Donors
1.5%
11%
Kohrt et al. Blood 2009
Incidence of Acute GVHD (II-IV)

CD4+CD25+ Regulatory T Cells• Major population of cells which regulate immune
reactions
• Express transcription factor FoxP3
• Deficiency or mutation of FoxP3 has autoimmune consequences in animal models and humans
• Cell contact-dependent suppression of alloreactive responses in mixed lymphocyte reactions (MLR)
• Prevent organ specific autoimmune diseases in animal models (e.g. IBD, diabetes)

Selection of CD4+CD25+ Regulatory T Cells (U. Perugia)
Cells (x109) 1060 (540-1370) 280 (202- 390)
%CD4CD25 3.0 (1.5-7.45) 92.4 (90-97.1)N° cells (x 106) 330 (221-1020) 256 (185.6-365.4)
%CD4CD25high 0.3 (0.12- 0.89) 33.6 (14.4-39.6)N° cells (x 106) 36.12 (19.98 - 84) 68.6 (20.9-143)
Starting fraction Final fraction
CD
25
CD127
CD4
FoxP3
Gate on CD4CD25+high
Gate on CD4CD25+
Fox P3+ cells 71.9 ± 15 %
ImmunomagneticSelection of
CD4+CD25+Cells
1st step:Depletion of CD8+/CD19+cells
2ndstep:Enrichment of CD25+ cells

TBI CD34+
Fludarabine
T regs
Tcons
days
Treg Haploidentical Protocol – Unversity of Perugia
CytoxanTT
8 Gy TBI in a single fraction at 16 cGy/m Thiotepa 4 mg/kg/dayCytoxan 35 mg/kg/dayFludarabine 40 mg/sqm/day
D’Ianni et al. Blood 2011

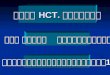
Evaluable Patients
Patients with CMV reactivation
0-30 31-60 61-90 91-120 121-150 151-180 181-365 >3650
10
20
30
40
50
60
70
80
90
100100
96
8275
67
5648
2928
50
34
22
9 91 1
0-30 31-60 61-90 91-120 121-150 151-180 181-365 >3650
5
10
15
20
25
30 27
21
16
109
5
212
5
1 0 0 0 0 0
Days after transplant
Days after transplant
CMV reactivation episodes
Tregs Group
Control Group
p<0.05

Outcomes – U. of Perugia
Event-Free Survival 12/26 (46%)
• Regimen Related Toxicities:– Veno-occlusive disease (3)– Multi-organ failure (1)
• Acute GVHD grade III-IV (2)• Serious infections (7)
• Relapse (AML 1)
Median follow-up 18.5 months (range 16.1-27.6)
D’Ianni et al. Blood 2011

Ex Vivo Expanded UCB Treg
Brunstein C G et al. Blood 2011;117:1061-1070

Treatment plans
Brunstein C G et al. Blood 2011;118:282-288

Risk of GVHD following Double UCB and Haploidentical BMT with post-transplant Cy
Brunstein C G et al. Blood 2011;118:282-288

Treatment for Acute GVHD
• Corticosteroids the mainstay of therapy• Many phase II studies showing a variety of
agents may have biological impact• Day 28 response most predictive of long term
outcome

Etanercept (N=46)
MMF (N=45)
Denil(N=47)
Pentostatin (N=42)
Complete Response
44% 73% 55% 62%
Complete Response(Excl. prior MMF)
53% 73% 61% 64%
Treatment Failure *
24% 9% 26% 29%
BMT CTN Phase II Pick the Winner Strategy
* Treatment Failure = no response, progression, or addition of another immunosuppressive agents by day 56.
Alousi et al, Blood, 2009

Where now for treatment of Acute GVHD?
• Phase III MMF vs Placebo CTN study halted for futility
• New phase II trial with other agents?– ATG, Campath– ECP– MSCs– Rapamycin– Cytokines

Chronic GVHD
• Major source of morbidity and some mortality • Immunosuppression with PSA and CNI remains the
mainstay of treatment• Alternative approaches
– Rapamycin– ECP– Rituximab– TKIs– MSCs– Cytokines

Ratio of Treg:Tcon post IL-2
Koreth et al. NEJM, 2011

Long term administration of IL-2 for cGVHD
Koreth et al. NEJM 2011

Future Risk Adapted Strategies
• Genetics of donor – recipient pairs• Treatment of the donor
– Statins• Earlier detection
– Biomarkers– Imaging