Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ictx20
Download by: [University of Sydney Library] Date: 16 August 2017, At: 17:45
Clinical Toxicology
ISSN: 1556-3650 (Print) 1556-9519 (Online) Journal homepage: http://www.tandfonline.com/loi/ictx20
Evidence-based recommendations on the use ofintravenous lipid emulsion therapy in poisoning
Sophie Gosselin, Lotte C. G. Hoegberg, Robert. S. Hoffman, Andis Graudins,Christine M. Stork, Simon H. L. Thomas, Samuel J. Stellpflug, Bryan D. Hayes,Michael Levine, Martin Morris, Andrea Nesbitt-Miller, Alexis F. Turgeon,Benoit Bailey, Diane P. Calello, Ryan Chuang, Theodore C. Bania, BrunoMégarbane, Ashish Bhalla & Valéry Lavergne
To cite this article: Sophie Gosselin, Lotte C. G. Hoegberg, Robert. S. Hoffman, Andis Graudins,Christine M. Stork, Simon H. L. Thomas, Samuel J. Stellpflug, Bryan D. Hayes, Michael Levine,Martin Morris, Andrea Nesbitt-Miller, Alexis F. Turgeon, Benoit Bailey, Diane P. Calello, RyanChuang, Theodore C. Bania, Bruno Mégarbane, Ashish Bhalla & Valéry Lavergne (2016) Evidence-based recommendations on the use of intravenous lipid emulsion therapy in poisoning, ClinicalToxicology, 54:10, 899-923, DOI: 10.1080/15563650.2016.1214275
To link to this article: http://dx.doi.org/10.1080/15563650.2016.1214275
Published online: 08 Sep 2016. Submit your article to this journal
Article views: 3798 View related articles
View Crossmark data Citing articles: 11 View citing articles

REVIEW
Evidence-based recommendations on the use of intravenous lipid emulsiontherapy in poisoning�Sophie Gosselina,b,c , Lotte C. G. Hoegbergd, Robert. S. Hoffmane , Andis Graudinsf, Christine M. Storkg,h,Simon H. L. Thomasi, Samuel J. Stellpflugj, Bryan D. Hayesk,l, Michael Levinem, Martin Morrisn ,Andrea Nesbitt-Millern , Alexis F. Turgeono, Benoit Baileyp,q , Diane P. Calellor, Ryan Chuangs,Theodore C. Baniat, Bruno M�egarbaneu, Ashish Bhallav and Val�ery Lavergnew
aDepartment of Emergency Medicine, McGill University Health Centre, Montr�eal, Qu�ebec, Canada; bCentre Antipoison du Qu�ebec,Montr�eal, Qu�ebec, Canada; cProvince of Alberta Drug Information Services, Calgary, Alberta, Canada; dDanish Poisons Information Centre,Anaesthesiology, Copenhagen University Hospital Bispebjerg, Copenhagen, Denmark; eDivision of Medical Toxicology, Ronald O. PerelmanDepartment of Emergency Medicine, New York University School of Medicine, New York, NY, USA; fMonash Clinical Toxicology Service,Program of Emergency Medicine, Monash Health and School of Clinical Sciences at Monash Health, Faculty of Medicine, Nursing and HealthSciences, Monash University, Clayton, Victoria, Australia; gUpstate NY Poison Center, Syracuse, NY, USA; hDepartment of EmergencyMedicine, Upstate Medical University, Syracuse, New York, USA; iNational Poisons Information Service (Newcastle) and Medical ToxicologyCentre, Institute of Cellular Medicine, Newcastle University, Newcastle, UK; jDepartment of Emergency Medicine, Regions Hospital, SaintPaul, MN, USA; kDepartment of Pharmacy, University of Maryland Medical Center, Baltimore, MD, USA; lDepartment of Emergency Medicine,University of Maryland School of Medicine, Baltimore, MD, USA; mDepartment of Emergency Medicine, Section of Medical Toxicology,University of Southern California, Los Angeles, CA, USA; nSchulich Library of Science and Engineering, McGill University, Montr�eal, Qu�ebec,Canada; oDivision of Critical Care Medicine, Department of Anesthesiology and Critical Care Medicine, and CHU de Qu�ebec, Universit�e LavalResearch Center, Population Health and Optimal Health Practices Unit, Universit�e Laval, Qu�ebec City, Qu�ebec, Canada; pDivision ofEmergency Medicine, Department of Pediatrics, CHU Sainte-Justine, Montr�eal, Qu�ebec, Canada; qCentre Antipoison du Qu�ebec, Quebec,Canada; rMedical Toxicology, Department of Emergency Medicine, Morristown Medical Center, Emergency Medical Associates, Morristown,NJ, USA; sDepartment of Emergency Medicine, Division of Clinical Pharmacology and Toxicology, University of Calgary, Poison and DrugInformation Service, Calgary, Alberta, Canada; tSt Luke's Roosevelt Hospital, New York, NY, USA; uDepartment of Medical and ToxicologicalIntensive Care, Lariboisi�ere Hospital, Paris-Diderot University, INSERM UMRS1144, Paris, France; vDepartment of Internal Medicine, PostGraduate Institute of Medical Education and Research, Chandigarh, India; wDepartment of Medical Biology, Sacr�e-Coeur Hospital, Universityof Montr�eal, Montr�eal, Qu�ebec, Canada
ABSTRACTBackground: Although intravenous lipid emulsion (ILE) was first used to treat life-threatening local anesthetic(LA) toxicity, its use has expanded to include both non-local anesthetic (non-LA) poisoning and less severemanifestations of toxicity. A collaborative workgroup appraised the literature and provides evidence-basedrecommendations for the use of ILE in poisoning.Methods: Following a systematic review of the literature, data were summarized in four publications: LA andnon-LA poisoning efficacy, adverse effects, and analytical interferences. Twenty-two toxins or toxin categoriesand three clinical situations were selected for voting. Voting statements were proposed using a predeterminedformat. A two-round modified Delphi method was used to reach consensus on the voting statements.Disagreement was quantified using RAND/UCLA Appropriateness Method.Results: For the management of cardiac arrest, we recommend using ILE with bupivacaine toxicity, while ourrecommendations are neutral regarding its use for all other toxins. For the management of life-threateningtoxicity, (1) as first line therapy, we suggest not to use ILE with toxicity from amitriptyline, non-lipid solublebeta receptor antagonists, bupropion, calcium channel blockers, cocaine, diphenhydramine, lamotrigine,malathion but are neutral for other toxins, (2) as part of treatment modalities, we suggest using ILE in bupi-vacaine toxicity if other therapies fail, but are neutral for other toxins, (3) if other therapies fail, we recom-mend ILE for bupivacaine toxicity and we suggest using ILE for toxicity due to other LAs, amitriptyline, andbupropion, but our recommendations are neutral for all other toxins. In the treatment of non-life-threateningtoxicity, recommendations are variable according to the balance of expected risks and benefits for eachtoxin.For LA-toxicity we suggest the use of IntralipidVR 20% as it is the formulation the most often reported. Thereis no evidence to support a recommendation for the best formulation of ILE for non-LAs. The voting panel isneutral regarding ILE dosing and infusion duration due to insufficient data for non-LAs. All recommendationswere based on very low quality of evidence.Conclusion: Clinical recommendations regarding the use of ILE in poisoning were only possible in a smallnumber of scenarios and were based mainly on very low quality of evidence, balance of expected risks andbenefits, adverse effects, laboratory interferences as well as related costs and resources. The workgroupemphasizes that dose-finding and controlled studies reflecting human poisoning scenarios are required toadvance knowledge of limitations, indications, adverse effects, effectiveness, and best regimen for ILEtreatment.
ARTICLE HISTORYReceived 11 May 2016Revised 3 July 2016Accepted 13 July 2016Published online 8 Septem-ber 2016
KEYWORDSFat emulsion; lipidresuscitation; recommenda-tion; adverse effect; lipidinterference
CONTACT Dr. Sophie Gosselin [email protected] 1001 Boulevard D�ecarie, Room CS1-6014, Montr�eal, Qu�ebec, H4A 3J1 Canada�On behalf of the Lipid Emulsion Therapy workgroup. The Lipid Emulsion Therapy workgroup also includes Ami Grunbaum MD, Brian Gilfix MD, Carol Rollins,PharmD, Jos�e A. Morais MD, and Sheldon Magder, MD� 2016 Informa UK Limited, trading as Taylor & Francis Group
CLINICAL TOXICOLOGY, 2016VOL. 54, NO. 10, 899–923http://dx.doi.org/10.1080/15563650.2016.1214275
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

Introduction
The lipid emulsion workgroup was established as a collabora-tive effort among the American Academy of ClinicalToxicology, the European Association of Poison Centres andClinical Toxicologists, the American College of MedicalToxicology, the Asia Pacific Association of MedicalToxicology, the American Association of Poison ControlCenters, and the Canadian Association of Poison ControlCenters. This article presents the workgroup’s recommenda-tions regarding the use of intravenous lipid emulsion therapyin poisoning for a preselected set of toxins. These recom-mendations are based on the results of four systematicreviews,[1–4] derived from a comprehensive analysis of thepublished evidence and further followed by an expertconsensus.
Methods
The detailed methodology for the workgroup’s process waspreviously published.[5] Each association selected clinicalexperts to serve on this committee and additional selectionswere made for their specific expertise in related fields. Twomedical librarians assisted the workgroup in the design ofthe search strategies, article retrieval, and management ofcitations but did not vote on the recommendations. For thepublished systematic reviews, the following databases weresearched from inception to 15 December 2014: BIOSISPreviews (via Ovid), CINAHL (via EBSCO), the CochraneLibrary/DARE, Embase (via Ovid), Medline (Ovid), PubMed,Scopus, and Web of Science. The literature review wasupdated in December 2015 as described later. No languagerestrictions were applied. Articles in languages other thanEnglish were professionally translated. A methodologist withexpertise in systematic reviews and guideline developmentoversaw the process. The workgroup considered four system-atic reviews that summarized the evidence pertaining topotential benefits and harms of the use of lipid emulsion inpoisoning, which were published prior to finalizing the rec-ommendations, and an international survey evaluating ILEavailability and cost.[1–4,6]
The voting panel decided to evaluate only those toxins orcategories of toxins for which a minimum of three humancases were reported in the literature. The 22 toxins or cate-gories were selected as the following: amitriptyline, class 1antidysrhythmics, baclofen, bupivacaine, bupropion, lipid-soluble beta-receptor antagonists (defined as a positivelog D), non-lipid-soluble beta-receptor antagonists, cocaine,non-dihydropyridine calcium channel blockers (diltiazem andverapamil), dihydropyridine calcium channel blockers,diphenhydramine, ivermectin, lamotrigine, malathion, olanza-pine, selective serotonin receptor inhibitors, other cyclic anti-depressants, other antihistamines, other antipsychotics,other insecticides, other local anesthetics (LAs), and otherpesticides.
The workgroup determined clinical situations in whichlipid emulsion could be indicated. These were categorized as(1) cardiac arrest, (2) life-threatening toxicity, or (3) non-life-threatening toxicity (Table 1). Life-threatening toxicity was
defined as the presence of any of the following: dysrhyth-mias such as ventricular tachycardia with compromised organperfusion, ventricular fibrillation, status epilepticus, and/orhypotension with organ compromise. Shock or end-organcompromise was defined as the presence of cellular ischemiaas evidenced by increased lactate concentration, acute kid-ney injury as defined by the Kidney Disease ImprovingGlobal Outcomes (KDIGO) guideline,[7] increased troponin,altered mental status, or decreased capillary refill.Hypotension was defined as a low blood pressure as perage-related defined standards. Non-life-threatening toxicitywas defined as clinical situations without immediate threat tolife such as coma, altered mental status, simple seizure, hypo-tension without organ compromise, and dysrhythmias suchas sinus tachycardia or other stable dysrhythmias. Alteredmental status was defined as the impairment in one of thespheres of brain function: cognition, alertness or orientation,and coma a deep state of unconsciousness as per theAmerican Academy of Neurology.[8]
A generic format of voting statements was developed dur-ing several conference calls in order to refine the final word-ing and ensure generalizability to all toxins (Appendix 1).A two-round modified Delphi method was utilized to reach aconsensus on clinical recommendations. After consideringthe balance between desirable and undesirable outcomes,the quality of evidence for outcomes as well as costs andresource use, members of the voting panel cast their voteson a 9-point Likert scale for each proposed statement foreach toxin/category of toxins included. The RAND/UCLAAppropriateness Method was used to quantify disagreementbetween the votes cast by the panel. The median values, thelower/upper quartiles, and the disagreement indexes werecalculated for each of the two rounds of votes. Median val-ues ranging from 7 to 9 reflected that the workgroup was infavor of the proposed statement, 4 to 6 reflected a neutralposition, and 1 to 3 reflected that the workgroup was againstthe statement. The disagreement index describes the disper-sion of ratings and values less than or equal to 1 indicateagreement. A second round of voting determined the finalstrength of recommendations (Figure 1). A strong recommen-dation in favor (level 1) was defined as a median valuebetween 7 and 9 with a lower quartile between 7 and 9 anda disagreement index �1 (similarly, a strong recommenda-tion against was defined as a median value between 1 and 3with an upper quartile between 1 and 3 and a disagreementindex �1). A weak/conditional recommendation in favor(level 2) was defined as a median value between 7 and 9with a lower quartile between 4 and 6 and a disagreement
Table 1. Intravenous lipid emulsion (ILE) in poisoning: clinical situations.
Statements Clinical situations
ILE is indicated in cardiac arrest, after standard ACLS is started
ILE is indicated in life-threatening toxicity As first-line therapyAs part of treatment modalitiesIf other therapies fail (in last resort)
ILE is indicated in non-life-threateningtoxicity
As first-line therapyAs part of treatment modalitiesIf other therapies fail (in last resort)
900 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

index �1 (similarly, a weak/conditional recommendationagainst was defined as a median value between 1 and 3 withan upper quartile between 4 and 6 and a disagreementindex �1). A neutral position was resulted when the medianvalue was between 4 and 6 with a disagreement index �1.To better understand the reason for a neutral vote, memberscould specify if their position was neutral due to majoruncertainties in the evidence or to a balance between thedesirable and undesirable effects of adherence to the pro-posed statement. When the disagreement index exceeded 1,no recommendation resulted as this illustrated an inability ofthe voting panel to reach consensus. All recommendationsare followed by the strength of recommendations (1 or 2)and the grading of the level of evidence (A to D) (Table 2),in accordance with the GRADE methodology (Grading ofRecommendations Assessment, Development andEvaluation).[9]
A first vote occurred in October 2014 and results werediscussed in a face-to-face meeting in the same month.A second vote in September 2015 determined the final rec-ommendations. Results were discussed in a second face-to-face meeting in October 2015. An update of the literaturefor publications through 31 December 2015 was performedin January 2016 using the same search strategy previouslymentioned and is presented in Appendices 2–4. The litera-ture update was summarized and presented to the membersof the voting panel. Members were given an opportunity toupdate their votes in March of 2016.
Clinical recommendations
In the discussions that follow if there is no specific mentionof a scenario, it is implied that the voting was neutral.
The complete voting results for each statement for eachtoxin/category of toxins are presented in Appendix 5. Anexecutive summary of the recommendations for all toxins/categories of toxins is presented in Table 3.
Recommendations for local anesthetics
Indications:
� In cardiac arrest due to toxicity of bupivacaine, we recom-mend using ILE after standard ACLS is started (1D), whileour recommendation is neutral regarding its use in car-diac arrest due to other local anesthetics.
Rationale: The voting panel noted that bupivacaine is theLA for which the most data exist with results supportingthe efficacy of ILE. However, controlled data from animalexperiments suffer from several methodological shortcom-ings. These include: reporting a statistical difference forshort experimental time frames not directly relevant toclinical situations, the failure to perform autopsies to searchfor potential adverse effects, and the lack of reporting ofacidosis and hypoxia in study animals, both of which arecommon in human poisonings and can affect outcome.Human case reports are too heterogeneous and patientsreceived concurrent multiple other medications making itimpossible to definitively attribute any positive outcome toILE alone.
However, while the level of evidence is very low, the risk/benefit ratio in cardiac arrest favors the use of ILE with bupi-vacaine and the voting panel had strong agreement for thisindication. There are no data to allow an informed decisionon which resuscitative medication to use first among sodium
Figure 1. Voting process.
CLINICAL TOXICOLOGY 901
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

bicarbonate, epinephrine, or ILE. Some members pointed outthat if the total dose administered is within the known thera-peutic range and the route of exposure is clearly not intra-vascular, consideration of an allergic reaction to LA ratherthan LA systemic toxicity probably warrants the use of epi-nephrine first. Because of a lack of evidence for the use ofILE with other LAs, the voting panel was unable to provide afirm recommendation in the setting of cardiac arrest.However, several members noted that harm appears to below and there was a strong agreement for a neutral vote.Concerns about reports of an unclear interaction with con-current administration of epinephrine or other resuscitativemedications with ILE reported mainly in the local anestheticsliterature may explain the voting panel’s reticence to adviseon ILE administration during cardiac arrest associated withnon-bupivacaine LA toxicity.[10–13] Data were insufficient tomake an evidence-based recommendation for the use of ILEwith other LAs. In comparison with bupivacaine, both the lip-ophilicity and toxicity profiles of the other LAs vary consider-ably, thereby invalidating recommendations made byanalogy rather than data.
� In life-threatening toxicity due to bupivacaine, we suggestusing ILE as part of treatment modalities (2D) and we rec-ommend its use if other therapies fail/in last resort (1D).
Rationale: The voting panel had strong agreement in con-cluding that there are enough data to support the use of ILEas a part of treatment modalities for patients with life-threat-ening bupivacaine toxicity. Moreover, while the risk/benefitratio of this therapy is warranted if all other treatmentmodalities fail, the lack of data to guide the sequence ofadministration of resuscitative therapies made it impossibleto decide on whether ILE should be the first-line treatment.Some members of the voting panel were concerned thatwaiting for other therapies to fail may decrease the potentialefficacy of ILE and thus it should be given relatively early,
while there was consensus to use ILE if a patient was alreadyunresponsive to other treatments.
� In life-threatening toxicity due to other LAs, we suggestusing ILE if other therapies fail/in last resort (2D).
Rationale: There is a lack of convincing data for efficacy ofILE with other LAs. Despite this, there is a relatively favorablerisk/benefit ratio in cases of prolonged toxicity in patientswith a pulse but unresponsive to other treatments. As aresult, the voting panel agreed that ILE could be used ifother therapies fail or as a last resort. However, it was notedthat in only a minority of reported cases ILE was used as soletreatment.
� In non-life-threatening toxicity due to bupivacaine or otherLAs, our recommendation is neutral regarding the use of ILE.
Rationale: The voting panel agreed that, in this situation,there is equipoise between risk and benefits. There are notenough data reported to make an evidence-based decision.
Lipid regimen
1. ILE formulation:
� When ILE is indicated for bupivacaine and other LAstoxicity, we suggest using the brand IntralipidVR 20% (2D).
Rationale: Most of the data reported used this specific ILE for-mulation. The voting panel agreed that there were insuffi-cient data to discuss other formulations in human poisoningsuntil such time as comparative studies are reported.
2. ILE dosing:
� When ILE is indicated for bupivacaine and other LAs tox-icity, our recommendation is neutral regarding the choiceof ILE dosing.
Rationale: Although the voting panel agreement was for aneutral position, there was a slight preference for the mostcommonly reported dosing regimen: a bolus of 1.5mL/kgand an infusion of 0.25mL/kg/min of 20% ILE. Data are lack-ing with regards to ILE dose–response relationships for treat-ing any human toxicity. No studies evaluated the benefit ofan infusion after bolus vs. a bolus alone for toxins with arapid endogenous clearance compared with most other tox-ins. The literature reports a varied range of bolus doses, infu-sion rates, and durations that make analysis of the optimaldosing regimen impossible.
3. ILE cessation:
� When ILE is indicated for bupivacaine and other LAs tox-icity, our recommendation is neutral regarding which end-points to use to stop ILE administration (maximum doseor maximum duration).
Table 2. Strength of recommendation and level of evidence.
Strength of recommendation (consensus-based)Level 1: Strong recommendation (The course of action is considered appropri-
ate by the large majority of experts with no major dissension. The panel isconfident that the desirable effects of adherence to the recommendationoutweigh the undesirable effects.)
Level 2: Weak/conditional recommendation (The course of action is consideredappropriate by the majority of experts but some degree of dissension existsamong the panel. The desirable effects of adherence to the recommenda-tion probably outweigh the undesirable effects.)
Neutral position: The course of action is neither preferred nor rejected by themajority of experts; either due to a balance in the desirable and undesir-able effects of adherence to the recommendation or due to major uncer-tainties to its evaluation.
No recommendation: The group of experts reached no agreementLevel of evidence (GRADE system)Grade A: High level of evidence (The true effect lies close to our estimate of
the effect.)Grade B: Moderate level of evidence (The true effect is likely to be close to
our estimate of the effect, but there is a possibility that it is substantiallydifferent.)
Grade C: Low level of evidence (The true effect may be substantially differentfrom our estimate of the effect.)
Grade D: Very low level of evidence (Our estimate of the effect is just a guess,and it is very likely that the true effect is substantially different from ourestimate of the effect.)
902 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

Table 3. Executive summary of indications regarding the use of ILE in poisoning.
Toxins Clinical situations (strength of recommendation & level of evidence)a
Local anestheticsBupivacaine In cardiac arrest: we recommend using ILE (1D)
In life-threatening toxicity: we suggest using ILE as part of treatment modalities (2D) and werecommend using ILE if other therapies fail/in last resort (1D)
In non-life-threatening toxicity: neutral recommendationAll other local anesthetics In cardiac arrest: neutral recommendation
In life-threatening toxicity: we suggest using ILE if other therapies fail/in last resort (2D)In non-life-threatening: neutral recommendation
Non-local anestheticsAntidysrhythmics Class 1 In cardiac arrest: neutral recommendation
In life-threatening toxicity: neutral recommendationIn non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Amitriptyline In cardiac arrest: neutral recommendationIn life-threatening toxicity: we suggest using ILE if other therapies fail/in last resort (2D),
but we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we recommend not using ILE as first-line therapy (1D) and
we suggest not using ILE as part of treatment modalities (2D)Other tricyclic antidepressants In cardiac arrest: neutral recommendation
In life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE in any circumstances (2D)
Baclofen In cardiac arrest: neutral recommendationIn life-threatening toxicity: neutral recommendationIn non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Beta receptor antagonists (Lipid-soluble) In cardiac arrest: neutral recommendationIn life-threatening toxicity: neutral recommendationIn non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Beta receptor antagonists (Non lipid-soluble) In cardiac arrest: neutral recommendationIn life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D) nor as part
of treatment modalities (2D)Bupropion In cardiac arrest: neutral recommendation
In life-threatening toxicity: we suggest using ILE if other therapies fail/in last resort (2D),but we suggest not using ILE as first-line therapy (2D)
In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)Calcium channel blockers: Diltiazem and verapamil In cardiac arrest: neutral recommendation
In life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Calcium channel blockers: Dihydropyridines In cardiac arrest: neutral recommendationIn life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE in any circumstances (2D)
Cocaine In cardiac arrest: neutral recommendationIn life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D) nor as part
of treatment modalities (2D)Diphenhydramine In cardiac arrest: neutral recommendation
In life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we recommend not using ILE as first-line therapy (1D) and
we suggest not using ILE otherwise (2D)Other antihistamines Insufficient dataIvermectin In cardiac arrest: neutral recommendation
In life-threatening toxicity: neutral recommendationIn non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Other insecticides In cardiac arrest: neutral recommendationIn life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Lamotrigine In cardiac arrest: neutral recommendationIn life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D) nor as part
of treatment modalities (2D)Malathion In cardiac arrest: neutral recommendation
In life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Other pesticides In cardiac arrest: neutral recommendationIn life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Olanzapine In cardiac arrest: neutral recommendationIn life-threatening toxicity: neutral recommendationIn non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Other antipsychotics In cardiac arrest: neutral recommendationIn life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)In non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
Selective serotonin reuptake inhibitors In cardiac arrest: neutral recommendationIn life-threatening toxicity: neutral recommendationIn non-life-threatening toxicity: we suggest not using ILE as first-line therapy (2D)
aNeutral position if not otherwise specified.
CLINICAL TOXICOLOGY 903
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

Rationale: The voting panel attempted to define endpointsfor ILE treatment either with a maximum dose administered,a maximum duration of administration, or with resolution oftoxicity. Members expressed opinions that a maximum doseshould not be exceeded due to concerns about adverseeffects from lipid overload. There were no strong data toinform the threshold amount of ILE that results in lipid tox-icity. To avoid lipid overload, it was suggested from the vot-ing panel that ILE doses should be limited to a maximum of10% of total blood volume to limit possible complicationsarising from increased triglyceride concentrations in excess of15mmol/L (glycerol-blanked method) reported when ILE rep-resented more than 10% of test tube volumes.[14] This isalso to avoid fluid overload, which is an increasing concernin resuscitation as patients receiving ILE will likely havereceived other fluid solutions.[15] This is particularly of con-cern when administering ILE to obese patients, neonates, oryoung children. Assuming ILE remains mostly in the intravas-cular compartment, this rationale would indicate a total ILEdose of 560mL for a 70 kg adult patient with an estimatedblood volume of 5.6 L.
Also, given the pharmacokinetics of LAs and the lack ofhistorical data to indicate a recurrence of toxicity once clin-ical improvement occurs, resolution of toxicity may be con-sidered as an appropriate endpoint. The risk of prolonged ILEtherapy on immune function or other organ function is asyet undefined for infusions administered for less than 24 h.However, some members were of the opinion that waiting tosee a sustained improvement in the clinical status would beinadvisable, until such a time that studies report a benefit forcontinuation of therapy beyond the point of clinicalresolution.
There is no strong evidence guiding the maximum dur-ation of ILE therapy that could be safely administered if clin-ical improvement does not occur. However, the voting panelcommented that clinical protocols for the use of ILE shouldrecommend a specific duration and maximal volume of ther-apy to avoid administration of high doses of ILE over indefin-ite periods. This should take into consideration the adverseeffect profile and the maximum duration of ILE recom-mended during parenteral nutrition.[16] As most articlesreported use of ILE for 20–30min, it seems reasonable tolimit the duration of infusion to this time period until con-trolled experiments are published assessing specific treat-ment durations. Thus, the voting panel concluded that notenough evidence exists to inform on when to stop ILE.
Recommendations for non-local anesthetics
Amitriptyline and other tricyclic antidepressants
Indications:
� In cardiac arrest due to either amitriptyline or any othertricyclic antidepressants toxicity, our recommendation isneutral regarding the use of ILE.
� In life-threatening toxicity due to amitriptyline, we sug-gest using ILE if other therapies fail/in last resort (2D), butwe suggest not using ILE as first-line therapy (2D).
� In life-threatening toxicity due to other tricyclic antidepres-sants, we suggest not using ILE as first-line therapy (2D).
� In non-life-threatening toxicity due to amitriptyline, werecommend not using ILE as first-line therapy (1D) andfurthermore we suggest not using ILE as part of treatmentmodalities (2D).
� In non-life-threatening toxicity due to other tricyclic anti-depressants, we suggest not using ILE in any circumstan-ces (2D).
Rationale: One human RCT (published only in abstract andnot specifying which TCAs were involved) failed to show abenefit of ILE on the duration of cardiotoxicity when patientswere randomized to standard treatment with bicarbonate orILE.[17] This explains why ILE therapy is discouraged either asfirst-line therapy either in life-threatening toxicity or withnon-life-threatening toxicity. However, the situation ofwhether ILE might be beneficial in cases refractory to stand-ard therapy, including epinephrine and bicarbonate therapy,was not explored. Many human case reports exist with inher-ent publication bias. However, the voting panel noted thatsome animal experiments, including one with an orogastric-poisoning model most similar to the clinical poisoningreported no benefit and possibly even harm.[18] Decades ofpublished evidence for the efficacy of bicarbonate therapyexist. Thus, the panel voted for the use of ILE only in life-threatening toxicity from amitriptyline after failure of stand-ard therapies, with moderate agreement.
Beta-receptor antagonists
Indications:
� In cardiac arrest due to toxicity of both lipid soluble andnon-lipid soluble beta-receptor antagonists, our recom-mendation is neutral regarding the use of ILE.
� In life-threatening toxicity due to lipid soluble beta-receptor antagonists, our recommendation is neutralregarding the use of ILE.
� In life-threatening toxicity due to non-lipid soluble beta-receptor antagonists, we suggest not using ILE as first-linetherapy (2D).
� In non-life-threatening toxicity due to lipid soluble beta-receptor antagonists, we suggest not using ILE as first-linetherapy (2D).
� In non-life-threatening toxicity due to non-lipid solublebeta-receptor antagonists, we suggest not using ILE asfirst-line therapy nor as part of treatment modalities (2D).
Rationale: The voting panel had consistent agreement in theirvotes. Reasons cited for the results are the balance existingbetween risks and expected benefit of using ILE, the evi-dence for the safety and efficacy of high dose insulin eugly-cemia therapy and the possible use of extracorporeal assistdevices reporting problems with concurrent ILE use.Moreover, the distinction between lipid-soluble and non-lipidsoluble drugs, which were initially divided into two distinctcategories to account for differences in log D did not
904 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

influence the voting panel’s evaluation, except in cases oflife-threatening toxicity where benefits were not consideredto outweigh risk for non-lipid soluble beta receptor antagon-ist toxicity as a first-line therapy or in non-life-threateningtoxicity as part of treatment modalities.
Bupropion
Indications:
� In cardiac arrest due to bupropion toxicity, our recom-mendation is neutral regarding the use of ILE.
� In life-threatening toxicity due to bupropion, we suggestusing ILE if other therapies fail/in last resort (2D), but wesuggested not using ILE as first-line therapy (2D).
� In non-life-threatening toxicity due to bupropion, we sug-gest not using ILE as first-line therapy (2D).
Rationale: Few case reports exist with survival outcome and itis unclear if the patients would have survived without ILE.However, the voting panel mentioned the likelihood of publi-cation bias. Also, most cases of bupropion toxicity do wellwith non-specific therapies aimed at maintaining vital func-tions. Several case reports demonstrate improvement withbicarbonate therapy. It is unclear whether higher doses ofbicarbonate, a medication with an established safety profile,would yield similar outcomes to ILE. More controlled data areneeded to inform on whether or not ILE interferes with theefficacy of standard therapies such as benzodiazepines orbarbiturates for seizures. The concurrent use of ILE and othertherapies has not been studied in any detail. However, in thesituation of prolonged and refractory status epilepticus, a trialof ILE seems reasonable. Hence, a 2D recommendation wasmade for cases with life-threatening toxicity if other therapiesfail. However, in pulseless cardiac arrest, the voting panel feltILE was not indicated given the reported interference it hason the effect of epinephrine or extracorporeal treatments.Hence, there was not a favorable enough risk/benefit ratio.Once ROSC (return of spontaneous circulation) is achieved,then ILE is suggested if life-threatening toxicity persists.
Calcium channel blockers
Indications:
� In cardiac arrest due to toxicity from calcium channelblockers (including diltiazem, verapamil and dihydropyri-dines), our recommendation is neutral regarding the useof ILE.
� In life-threatening toxicity due to diltiazem, verapamil, ordihydropyridine calcium channel blockers, we suggest notusing ILE as first-line therapy (2D).
� In non-life-threatening toxicity due to diltiazem verapamil,or dihydropyridine calcium channel blockers, we suggestnot using ILE as first-line therapy (2D).
Rationale: Due to the inconsistent outcomes reported, rang-ing from sudden death to immediate response, in both
animal experiments and human case reports, no clear rec-ommendation can be made. Some members felt cardiacarrest presents a situation where little harm seems to existfor a “trial” of ILE. However, as noted above, other membersexpressed their concerns that ILE can enhance intestinalabsorption of toxins as is demonstrated in oral drug poison-ing models.[19] In addition, problems associated with theconcurrent use of ILE with extracorporeal assist devices andthe potential for interference with resuscitative medicationswith evidence of benefit, such as vasopressors and insulin–glucose, were also highlighted. A single study that mim-icked an oral overdose of verapamil demonstrated worseoutcomes when ILE was given. Animal studies showed noclinical benefit or benefit at dose requirements exceeding adose of 12mL/kg of 20% ILE.[19,20] No studies comparingthe current standard of care with vasopressors or insulin–glucose therapy are available in a model consistent withhuman clinical poisoning. Considering the lack of informa-tion on dose, potential adverse effects and especially inter-ference with extracorporeal assist devices or interferencewith medications known to be effective, the voting paneldetermined that the benefits were probably equal to therisks and thus, a neutral position resulted in the presenceof cardiac arrest.
Unless organ perfusion is compromised, the voting panelfelt that there was not enough information to make a deci-sion and at the very least a balance exists between risks andpotential benefits of ILE. Thus, there is a question as towhether ILE should be a part of the treatment modalities orused after standard therapy fails (last resort) in life-threaten-ing toxicity for all calcium channel blockers.
Furthermore, the reason for not suggesting lipid emulsionif other therapies fail, in cases of non-life-threatening toxicitydue to diltiazem and verapamil, and not suggesting ILE in allother circumstances of non-life-threatening toxicity due dihy-dropyridines, is based on a risk/benefit analysis. Certain signsand symptoms of CCB toxicity, such as ileus or bradycardiaand hypotension, may not respond or entirely correct withvarious therapies but only resolve with time and metabolismof the toxicant.
Cocaine
Indications:
� In cardiac arrest due to cocaine toxicity, our recommenda-tion is neutral regarding the use of ILE.
� In life-threatening toxicity due to cocaine, we suggest notusing ILE as first-line therapy (2D).
� In non-life-threatening toxicity due to cocaine, we suggestnot using ILE as first-line therapy (2D) or as part of treat-ment modalities (2D).
Rationale: Too few case reports exist, all with varied outco-mesto make a favorable recommendation. Several experi-mental studies with cocaine and ILE using pre-treatmentanimal models [21,22] were excluded a priori due to the lackof generalizability to the clinical setting of human cocainepoisoning. The voting panel was in agreement on a neutral
CLINICAL TOXICOLOGY 905
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

recommendation concerning the use of ILE in cardiac arrestand commented there was a paucity of data on the efficacyof ILE to reverse signs and symptoms of cocaine toxicity. Thebody of evidence and published experience with other treat-ments such as sodium bicarbonate, and benzodiazepines ismuch greater than that for ILE therapy. More controlled dataare needed to assess whether or not ILE interferes with theefficacy of the standard therapies.
Diphenhydramine
Indications:
� In cardiac arrest due to diphenhydramine toxicity, our rec-ommendation is neutral regarding the use of ILE.
� In life-threatening toxicity due to diphenhydramine, wesuggest not using ILE as first-line therapy (2D).
� In non-life-threatening toxicity due to diphenhydramine,we recommend not using ILE as first-line therapy (1D) andwe suggest not using ILE otherwise (2D).
Rationale: Due to the efficacy of bicarbonate therapy and thelack of superiority of ILE over bicarbonate reported in one ani-mal experiment, the voting panel concluded there was noscenario where ILE would be clearly indicated at this time.There are no data to inform on the best timing of ILE adminis-tration. Diphenhydramine possesses sodium channel blockingproperties and a trial of ILE has clinical equipoise when con-sidering the possible risks of an acute administration of ILE incases otherwise unresponsive to repeated administration ofsodium bicarbonate (e.g. more than 200 mEq [23]). However,the role of ILE in non-life-threatening toxicity, such as anti-cholinergic delirium, was not reported in the literature at all.
A comment was made regarding the use of ILE with “otherantihistamines”. It was noted that if the lipid sink or conduittheories proves to be valid, there might be a theoretical bene-fit for ILE in severe toxicity from sedating antihistamines. Inparticular, those agents with a log D value of 2 or 3 whenother therapies have failed. However, more than 70% of thepanel voted that there were insufficient data to consider rec-ommendations in the category “other antihistamines”. Thismade it impossible to make a statement about any particularantihistamine, as described in the methodology.
Lamotrigine
Indications:
� In cardiac arrest due to lamotrigine toxicity, our recom-mendation is neutral regarding the use of ILE.
� In life-threatening toxicity due to lamotrigine, we suggestnot using ILE as first-line therapy (2D).
� In non-life-threatening toxicity due to lamotrigine, wesuggest not using ILE as first-line therapy (2D) nor as partof treatment modalities (2D).
Rationale: The voting panel determined that too few casereports exist with survival outcome reported. It is also unclear
if these patients would have survived without ILE.Additionally, the voting panel mentioned publication biasand the fact that most cases of lamotrigine toxicity do wellwith supportive care. More controlled data are needed toinform clinicians on whether or not ILE interferes with theefficacy of the standard therapies such as benzodiazepinesand sodium bicarbonate to reverse the proconvulsant andsodium channel blocking properties of lamotrigine. Severelamotrigine poisoning can also result in metabolic acidosisand acute kidney injury, which may require dialysis. The con-current use of ILE and other therapies has not been studiedin enough detail to provide comment. Of note, as describedin our adverse effect review article,[5] the use of ILE with anyextracorporeal circuit such as occlusion of the circulation.
Other toxins
This section includes the other toxins and categories oftoxins for which the voting results were similar. Therefore,rather than lengthy individual statements, the results are dis-cussed in aggregate. Once again the readers are referred tothe Appendices and tables for a complete record of thevoting.
� In cardiac arrest due to toxicity of Class 1Vaughan–Williams antidysrhythmics, baclofen, ivermectinand other insecticides, malathion and other pesticides,olanzapine and other antipsychotics, and selective sero-tonin reuptake inhibitors, our recommendation is neutralregarding the use of ILE.
� In life-threatening toxicity due to other insecticides, mala-thion and other pesticides, olanzapine, and other antipsy-chotics, we suggest not using ILE as first-line therapy (2D).
� In life-threatening toxicity due to Class 1Vaughan–Williams antidysrhythmics, baclofen, ivermectin,and selective serotonin reuptake inhibitors, our recom-mendation is neutral regarding the use of ILE.
� In non-life-threatening toxicity due to Class 1Vaughan–Williams antidysrhythmics, baclofen, ivermectin,and other insecticides, malathion and other pesticides,olanzapine and other antipsychotics, and selective sero-tonin reuptake inhibitors, we suggest not using ILE asfirst-line therapy (2D).
Rationale: Even though some of these toxins are lipid-soluble(defined by their log D) due to the paucity of data, the panelprimarily considered possible benefit, possible risks, and theavailability of other alternative treatments in their votes.
Animal data provide conflicting results for the pesticideand insecticide groups. Thus, adverse effects and potentialinterferences were a major consideration influencing the vot-ing. Moreover, these toxins represent a heterogeneous groupof chemicals that are not amenable to a common statementon treatment with ILE. Antipsychotics rarely cause significantcardiovascular mortality and status epilepticus is uncommon.Class 1 antidysrhythmics produce their toxic effect by block-ing sodium channels and no studies have compared bicar-bonate to ILE for these drugs. The controversy surrounding
906 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

efficacy, the adverse effect profile, and the potential interfer-ences with essential laboratory testing question the inclusionof ILE in the care of these poisonings. Clinically relevant stud-ies with clear meaningful endpoints and drug concentrationmeasurements to assess the toxic burden are required beforestronger recommendations can be made for these toxins.Thus, the panel vote resulted in a neutral recommendation,leaving the decision to the clinician to weigh the pros andcons of ILE in these situations.
Lipid regimen
The panel chose to vote on a preferred lipid regimen foreach category of toxins. However, the results were not sig-nificantly different from one toxin to another. In all cases, thevote was neutral with the median ranging from 4 to 6 andthe disagreement index always below 1, reflecting the con-sensus among panel members.
1. ILE formulation:
� When ILE is indicated in non-LAs toxicity, our recommen-dation is neutral regarding the formulation of ILE.
Rationale: Not enough data exist comparing various formula-tions of ILE. Most articles do not report the brand of ILE usedand simply list a concentration of 20%. There is no evidenceto support a recommendation for the best formulation of ILEfor non-LAs, even though the most common formulationused was IntralipidVR 20%. While there is experimental evi-dence suggesting that one lipid formulation might be prefer-able to another, it is unclear if the relationship is true for alltoxins or is applicable to human poisonings.[24]
2. ILE dosing:
� When ILE is indicated in non-LAs toxicity, our recommen-dation is neutral regarding the dosing of ILE.
Rationale: In the only ILE dose-finding study, the greatestbenefit to survival in a rodent model of IV verapamil toxicityoccurred with an ILE dose of 18.6mL/kg.[20] However, thegreatest benefit to HR, MAP occurred at 24.8mL/kg ILE. It isunknown how these doses would translate to human poison-ings. Additional concern was expressed over the IV model ofpoisoning and the risk for lipid-induced increase in gastro-intestinal absorption, as noted above. Nevertheless, the find-ing that increased survival occurred in the group treatedwith a lower dose of ILE suggests that a higher dose,although associated with greater hemodynamic improve-ment, may not be necessary in all cases.
Members expressed opinions that until the adverse effectprofile for acute ILE administration is properly defined, thelowest possible dose should be used. ILE dosing should beguided by clinically significant physiological endpoints, ratherthan arbitrary hemodynamic parameters. Importantly, analyt-ical interferences are likely to be shorter in duration or lesssignificant if a lower blood concentration of ILE is
achieved.[1] The maximum safe dose of ILE is unknown.Moreover, the reported ILE regimens may vary significantlyfrom the commonly recommended regimen of 1.5mL/kgbolus of ILE 20% followed by 0.25–0.5mL/kg/min.[25,26] Fora 70 kg person, this dose translates to more than 1 L of lipidemulsion in the first hour at the lowest rate and more than2 L if the highest infusion rate (0.5mL/kg/min) is adminis-tered. Parenteral nutrition guidelines limit the daily amountof ILE to between 500 and 1200mL per 24-h period or 10mLper kg of a 20% formulation.[27] Several reports cite a singlerodent study assessing the apparent safety and LD50 of ILE innine rats.[28] The LD50 is an imperfect measure of safety.Also, this study only included one ILE dose within the rangecurrently used in the clinical setting. No studies haveassessed varying doses and infusion rates or their combina-tions in humans.
The panel agreed that a maximum dose (per kg bodyweight) should be specified and the rate of infusion keptlow. Termination of the infusion should be considered whenthere is sustained clinical improvement or the maximumdose has been reached. This is speculative and dose-findingstudies are much needed. A recent publication called intoquestion cases where exceedingly large volumes of ILE wereused and created a pharmacokinetic–pharmacodynamicmodel to predict an infusion rate that would only produce“modestly lipemic plasma”. Although, based on their model,these authors recommend a regimen of 1.5mL/kg followedby 0.25mL/kg/min for 3min and then an infusion of0.025mL/kg/min for up 6.5 h,[29] this regimen should be vali-dated for safety and efficacy before it can be routinelyrecommended.
3. ILE cessation:
� When ILE is indicated in non-LAs toxicity, our recommen-dation is neutral regarding which endpoints to use tostop ILE administration (maximum dose or maximumduration).
Rationale: The group reached consensus that there is insuffi-cient information to determine when ILE should be stopped.The literature is heterogeneous in the endpoints to therapyfrom resolution of symptoms to an arbitrary decrease ofserum TCA concentration resulting in duration of therapy ofup to several days.[30] No clinical studies exploring differentendpoints to therapy have been published to date. The work-group suggests that clinical resolution is a desirable endpointif toxicity is unlikely to recur, but if this endpoint takes time,consideration should be made not to exceed the rate ofendogenous triglyceride metabolism as discussed above. Thegroup noted that in many of the reports ILE was startedalong with other therapies and continued for hours or dayseven though the effect of ILE was unclear. The workgroupcould not find evidence to suggest a specific endpoint.However, adverse effects seem to be associated with highervolume and faster infusion rates of ILE.[3] Analytical interfer-ences and inability to measure several biochemical parame-ters and the unknown effect of ILE on other medicationsmay justify lower doses and a shorter duration of infusion.[1]
CLINICAL TOXICOLOGY 907
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

Limitations
Despite the fact that our combined search strategies wereexhaustive and not limited by language, it is possible thatsome publications were missed; especially abstracts not yetpublished as full articles. The literature infrequently reportsthe concentration of the toxin, precise timing of interven-tions with regards to clinical improvement or importantinformation on the formulation, or total amount of ILEgiven. Also, in most case reports, multiple therapies wereadministered simultaneously, making the specific efficacy oflipid emulsion difficult to ascertain. Case reports are knownto be subject to publication bias. We also noticed themajority of publications failed to mention the presence orabsence of adverse effects and when events occurred therewas a tendency to attribute them to the toxin rather thanthe therapy. Our clinical appraisal for the non-LA toxins waslimited because most of the controlled studies occurred inanimals and the majority were not performed with modelsbearing any resemblance to clinical poisonings, which usu-ally involve ingestion of the toxin. The greatest limitation ofthese recommendations may be their reliance on publisheddata which is often of poor quality, may have significantpublication delay of up to several years, and cannot capturethe vast numbers of positive and negative outcomes of ILEthat remain unreported. Additionally, it should be notedthat the Delphi method is itself imperfect, with the greatestcriticism being its tendency to force “middle-of-the-road”consensus.[31] We feel we have addressed this concern inthree ways: limiting the number of rounds of voting to two,in order not to artificially force consensus by repeatedregression to the mean, using a disagreement index todemonstrate the true strength of the recommendations,and the inclusion of minority opinions in the commentsand rationale when they were provided by the workgroupmembers. Also, patients’ views and preferences were notdirectly sought in the development of the clinical recom-mendations due to the highly heterogeneous target popula-tion under study. Finally, as the study and clinical use ofILE continues to evolve, we recognize additional informationmay emerge to alter this analysis.
Discussion
Despite some early enthusiasm for the use of ILE in the treat-ment of acute poisoning, the voting panel found an absenceof evidence to recommend its use in most poisonings andclinical scenarios where its use is previously reported. Thusthe preponderance of neutral votes likely represents theworkgroups’ caution to make recommendations for oragainst a therapy where so little moderate- or high-qualityhuman data exist. Furthermore, it is worth reiterating thatthe neutral recommendations result from a balance betweenpro and con assessments (rather than a lack of data whichwould result in no recommendation at all) but rather; basedon disagreement index, represent a strong consensus aroundneutrality.
Moreover, many specific aspects of ILE therapy have notbeen validated in the clinical setting. These include the
optimal dose of ILE for clinical efficacy, the threshold dosefor adverse effects, and the minimum or maximum durationof therapy. It is acknowledged that clinicians may have per-sonal preferences for indication, dose, and duration of ILEtreatment. Given that there is a lack of evidence to supportany particular approach, the workgroup felt that it reason-able to comment that the most common formulationreported was IntralipidVR 20%, and that the most commonregimen was a bolus of 1.5mL/kg of ILE 20% followed byan infusion of 0.25mL/kg/min, in order to provide someguidance in situations were favorable recommendations orsuggestions were made. Additionally, the workgroup recog-nized the lack of data on which to guide the duration oftherapy, and, therefore, some members proposed a max-imum dose of 10% of blood volume based on safety con-cerns but this position was not officially voted upon. This issomewhat in keeping with parenteral nutrition recommen-dations to limit the maximum dosage of ILE between 10and 12.5mL/kg/d of 20% ILE [32] as well reported increasedtriglyceride concentrations in excess of 15mmol/L (glycerol-blanked method) when ILE represented more than 10% oftest tubes volumes,[14] which for a 70 kg individual with ablood volume of 80mL/kg would yield 8.0mL/kg.Indications in which it is easier to measure the risk andbenefit of ILE therapy, such as cardiac arrest or systemictoxicity with no other treatment alternatives, may warrant a“trial” of ILE therapy. Conversely, ILE should not be consid-ered in clinical scenarios where the risk of death or organdamage is small, or when there are other accepted treat-ments, which have not been used first. Concern wasexpressed as to the lack of data regarding the impact ofILE on the effectiveness of other resuscitative medicationsor antidotes, or the ability of ILE to interfere with the bio-chemical and drug assay testing. In addition, outcome datafrom animal models may not be directly translatable toclinical practice. Notably, the majority of animal studies ofILE efficacy administered toxins intravenously, whereas themajority of clinical poisonings (except for local anesthetics)are the result of oral exposure.
Future research questions
The voting panel is hopeful that randomized controlled tri-als will be undertaken to enable a more informed evalu-ation of the role of ILE in select poisonings. Efforts inanimals should be directed at designing controlled studiesevaluating the timing of administration, using orogastricadministration of the toxin. In particular, studyingthe dose–response relationship for the loading–dose andthe infusion is important, while clearly reporting on thepresence or absence of adverse effects. Ideally, these stud-ies would also focus on determining the optimal endpointfor ILE therapy. In vitro studies may be sufficient toevaluate the potential interferences of ILE on assays ofcommon co-ingestants or binding affinity with other medi-cations. Moreover, the efficacy of commercially availablelipid emulsions should be compared in order to determine
908 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

the relative effectiveness of the commercially availableproducts.
Conclusion
ILE is a recent therapy for which there is an incompleteunderstanding of its efficacy, mechanisms of action, safety,and associated analytical interferences. Clinical recommenda-tions regarding the use of ILE in poisoning were only pos-sible in a small number of scenarios based on a very lowquality of evidence, balance of risks and benefits, andresource use. The workgroup emphasizes that human dose-finding and randomized controlled studies are required toadvance knowledge of limitations, indications, adverseeffects, effectiveness, and best regimen for ILE treatment.
External review
The American Academy of Clinical Toxicology, the AmericanCollege of Medical Toxicology, the American Association ofPoison Control Centers, the Asia Pacific Association ofMedical Toxicology, the European Association of PoisonCentres and Clinical Toxicologists, and the CanadianAssociation of Poison Control Centers endorsed these recom-mendations prior to publication.
Applicability
The recommendations will be circulated to the membershipof each association, published in a participating association’ssponsored-journal and presented at internationalconferences.
Planned update
These recommendations are to be updated in 5 years unlessnew data warrants an earlier review.
Acknowledgements
The workgroup gratefully acknowledge the work of the AACT staff forthe arrangement of meetings and conference calls and MarielleCarpenter for copy editing.
Disclosure statement
All members completed a conflict of interest form for the AACT andreceived no honoraria. Webcast conference and rooms for meeting wereprovided by the AACT. No member with a financial or academic conflictof interest preventing an objective assessment of the literature partici-pated in the reviews or the elaboration of the recommendations (i.e. nocommittee member’s livelihood or academic career is depending on agrant studying lipid emulsion in poisoning).
Funding
Dr. Turgeon is a recipient of a New Investigator Award from theCanadian Institutes of Health Research (CIHR). Dr. Lavergne is a recipientof a salary support award from the Fonds de la Recherche du Qu�ebec –Sant�e (FRQS).
ORCiD
Sophie Gosselin http://orcid.org/0000-0002-0694-5588Robert. S. Hoffman http://orcid.org/0000-0002-0091-9573Martin Morris http://orcid.org/0000-0002-5659-2995Andrea Nesbitt-Miller http://orcid.org/0000-0002-0054-7132Benoit Bailey http://orcid.org/0000-0003-2520-1258
References
[1] Grunbaum AM, Gilfix BM, Hoffman RS, et al. Review of the effectof intravenous lipid emulsion on laboratory analyses. Clin Toxicol.2016;54:92–102.
[2] Hoegberg LC, Bania TC, Lavergne V, et al. Systematic review ofthe effect of intravenous lipid emulsion therapy for local anes-thetic toxicity. Clin Toxicol. 2016;54:167–193.
[3] Hayes BD, Gosselin S, Calello DP, et al. Systematic review of clin-ical adverse events reported after acute intravenous lipid emul-sion administration. Clin Toxicol. 2016;54:365–404.
[4] Levine M, Hoffman RS, Lavergne V, et al. Systematic review of theeffect of intravenous lipid emulsion therapy for non-local anes-thetics toxicity. Clin Toxicol. 2016;54:194–221.
[5] Gosselin S, Morris M, Miller-Nesbitt A, et al. Methodology for AACTevidence-based recommendations on the use of intravenous lipidemulsion therapy in poisoning. Clin Toxicol. 2015;53:557–564.
[6] Cormier M, Gosselin S. Cost and availability of intravenous lipidemulsion therapy: a worldwide survey. [Abstract] 36th InternationalCongress of the European Association of Poisons Centres andClinical Toxicologists (EAPCCT) 24–27 May, 2016, Madrid, Spain.Clin Toxicol (Formerly J Toxicol: Clin Toxicol). 2016;54:495–496.
[7] Andrassy KM. Comments on ‘KDIGO 2012 clinical practice guide-line for the evaluation and management of chronic kidney dis-ease’. Kidney Int. 2013;84:622–623.
[8] American Academy of Neurology. Coma [Internet] [cited 2016 Jun15]. [Available from: https://patients.aan.com/disorders/index.cfm?event¼view&disorder_id¼893.
[9] Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging con-sensus on rating quality of evidence and strength of recommen-dations. Br Med J. 2008;336:924–926.
[10] Hiller DB, Gregorio GD, Ripper R, et al. Epinephrine impairs lipidresuscitation from bupivacaine overdose: a threshold effect.Anesthesiology. 2009;111:498–505.
[11] Carreiro S, Blum J, Jay G, et al. Intravenous lipid emulsion altersthe hemodynamic response to epinephrine in a rat model. J MedToxicol: Off J Am Coll Med Toxicol. 2013;9:220–225.
[12] Hicks SD, Salcido DD, Logue ES, et al. Lipid emulsion combinedwith epinephrine and vasopressin does not improve survivalin a swine model of bupivacaine-induced cardiac arrest.Anesthesiology. 2009;111:138–146.
[13] Mayr VD, Mitterschiffthaler L, Neurauter A, et al. A comparison ofthe combination of epinephrine and vasopressin with lipid emul-sion in a porcine model of asphyxial cardiac arrest after intraven-ous injection of bupivacaine. Anesth Analg. 2008;106:1566–1571.
[14] Grunbaum AM, Gilfix BM, Gosselin S, et al. Analytical interferencesresulting from intravenous lipid emulsion. Clin Toxicol (Formerly JToxicol: Clin Toxicol). 2012;50:812–817.
[15] Aditianingsih D, George YW. Guiding principles of fluid and vol-ume therapy. Best Pract Res Clin Anaesthesiol. 2014;28:249–260.
[16] Intralipid [package insert]. Missisauga (ON): Fresenius Kabi; 2013.[17] Kasnavieh SMH. Intravenous lipid emulsion for the treatment of
tricyclic antidepressant toxicity a randomized controlled trial. VIIthMediterranean Emergency Medicine Congress; 2013 September8–11; Marseille, France.
[18] Perichon D, Turfus S, Gerostamoulos D, et al. An assessment ofthe in vivo effects of intravenous lipid emulsion on blood drugconcentration and haemodynamics following oro-gastric amitrip-tyline overdose. Clin Toxicol. 2013;51:208–215.
CLINICAL TOXICOLOGY 909
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

[19] Perichon D, Turfus S, Graudins A. Intravenous lipid emulsion doesnot improve hemodynamics or survival in a rodent model of oralverapamil poisoning. Clin Toxicol. 2013;51:277.
[20] Perez E, Bania TC, Medlej K, et al. Determining the optimal doseof intravenous fat emulsion for the treatment of severe verapamiltoxicity in a rodent model. Acad Emerg Med. 2008;15:1284–1289.
[21] Carreiro S, Blum J, Hack JB. Pretreatment with intravenous lipidemulsion reduces mortality from cocaine toxicity in a rat model.Ann Emerg Med. 2014;64:32–37.
[22] Heinonen JA, Litonius E, Backman JT, et al. Intravenous lipidemulsion entraps amitriptyline into plasma and can lower itsbrain concentration – an experimental intoxication study in pigs.Basic Clin Pharmacol Toxicol. 2013;113:193–200.
[23] Jang DH, Manini AF, Trueger NS, et al. Status epilepticus andwide-complex tachycardia secondary to diphenhydramine over-dose. Clin Toxicol. 2010;48:945–948.
[24] Li Z, Xia Y, Dong X, et al. Lipid resuscitation of bupivacaine tox-icity: long-chain triglyceride emulsion provides benefits overlong- and medium-chain triglyceride emulsion. Anesthesiology.2011;115:1219–1228.
[25] American College of Medical Toxicology Position Statement:interim guidance for the use of lipid resuscitation therapy. J MedToxicol: Off J Am Coll Med Toxicol. 2011;7:81–82.
[26] American College of Medical Toxicology Position Statement:Guidance for the Use of Intravenous Lipid Emulsion. J MedToxicol: Off J Am Coll Med Toxicol. 2016 [cited 2016 Apr 27].
[27] Mirtallo J, Canada T, Johnson D, et al. Safe practices for parenteralnutrition. JPEN J Parenter Enteral Nutr. 2004;28:S39–S70.
[28] Hiller DB, Di Gregorio G, Kelly K, et al. Safety of high volume lipidemulsion infusion: a first approximation of LD50 in rats. RegAnesth Pain Med. 2010;35:140–144.
[29] Fettiplace MR, Akpa BS, Rubinstein I, et al. Confusion about infusion:rational volume limits for intravenous lipid emulsion during treat-ment of oral overdoses. Ann Emerg Med. 2015;66:185–188.
[30] Agarwala R, Ahmed SZ, Wiegand TJ. Prolonged use of intravenouslipid emulsion in a severe tricyclic antidepressant overdose.J Med Toxicol: Off J Am Coll Med Toxicol. 2014;10:210–214.
[31] Yousuf MI. Using experts’ opinions through Delphi technique.Pract Assess Res Eval. 2007;12:1–8.
[32] Mirtallo JM, Dasta JF, Kleinschmidt KC, et al. State of the art review:intravenous fat emulsions: current applications, safety profile, andclinical implications. Ann Pharmacother. 2010;44:688–700.
[33] Udelsmann A, Melo S. Hemodynamic changes with two lipidemulsions for treatment of bupivacaine toxicity in swines. ActaCirurgica Brasileira/Sociedade Brasileira Para DesenvolvimentoPesquisa Em Cirurgia. 2015;30:87–93.
[34] Zaballos M, Sevilla R, Gonzalez J, et al. Analysis of the temporalregression of the QRS widening induced by bupivacaine afterIntralipid administration. Study in an experimental porcine model.Revista Espanola Anestesiol Y Reanimacion. 2016;63:13–21.
[35] Bourque S, Panahi S, Mittal R, et al. Intralipid reverses propofolmediated hypotension in rats. FASEB J Conference: Exp Biol.2015;29. 1 (Meeting Abstracts).
[36] Ceccherini G, Perondi F, Lippi I, et al. Intravenous lipid emulsionand dexmedetomidine for treatment of feline permethrin intoxi-cation: a report from 4 cases. Open Vet J. 2015;5:113–121.
[37] Herring JM, McMichael MA, Corsi R, et al. Intravenous lipid emul-sion therapy in three cases of canine naproxen overdose. J VetEmerg Crit Care (San Antonio). 2015;25:672–678.
[38] Jourdan G, Boyer G, Raymond-Letron I, et al. Intravenous lipidemulsion therapy in 20 cats accidentally overdosed with ivermec-tin. J Vet Emerg Crit Care (San Antonio). 2015;25:667–671.
[39] Peacock RE, Hosgood G, Swindells KL, et al. A randomized, con-trolled clinical trial of intravenous lipid emulsion as an adjunctivetreatment for permethrin toxicosis in cats. J Vet Emerg Crit Care(San Antonio). 2015;25:597–605.
[40] Saqib M, Abbas G, Mughal MN. Successful management of iver-mectin-induced blindness in an African lion (Panthera leo) byintravenous administration of a lipid emulsion. BMC Vet Res.2015;11:287.
[41] Seitz MA, Burkitt-Creedon JM. Persistent gross lipemia and sus-pected corneal lipidosis following intravenous lipid therapy in acat with permethrin toxicosis. J Vet Emerg Crit Care (SanAntonio). 2016.
[42] Varney SM, Bebarta VS, Boudreau SM, et al. Intravenous lipidemulsion therapy for severe diphenhydramine toxicity: a random-ized, controlled pilot study in a swine model. Ann Emerg Med.2016;67:196–205 e3.
[43] Williams K, Wells RJ, McLean MK. Suspected synthetic cannabin-oid toxicosis in a dog. J Vet Emerg Crit Care (San Antonio).2015;25:739–744.
[44] Glavas J, Flam D, Istvanic T, et al. Abstracts and Highlight Papersof the 34th Annual European Society of Regional Anaesthesia &Pain Therapy (ESRA) Congress 2015. Reg Anesth Pain Med.2015;40:e1–e72. [WorldCat]
[45] Goucher HC, Asher Y. The best-laid plans: a case report of an epi-dural anesthetic gone awry in a medically challenging patient.Anesth Analg. 2015;1:S471.
[46] Kamel I, Trehan G, Barnette R. Intralipid therapy for inadvertentperipheral nervous system blockade resulting from local anes-thetic overdose. Case Rep Anesthesiol. 2015;2015:486543.
[47] Musielak M, McCall J. Lipid rescue in a pediatric burn patient.J Burn Care Res: Off Publ Am Burn Assoc. 2015.
[48] Procopio G, Gupta A, Hernandez M, et al. Lipid emulsion for inad-vertent intrathecal administration of local anesthetics in the ED.Crit Care Med. 2015;1:309.
[49] Riff C, Guilhaumou R, Dupouey J, et al. Amino-amides anestheticssystemic toxicity: about nine cases. Fundam Clin Pharmacol.2015;29:48.
[50] Shih RD, Calello D. Complete spinal paralysis following a brachialplexus block treated with lipid infusion. Clin Toxicol.2015;53:310–311.
[51] Stella FA, Panzavolta FG, Sesana F, et al. Intravenous lipid emul-sion for treatment of local anesthetic systemic toxicity. ClinToxicol. 2015;53:313.
[52] Agulnik A, Kelly D, Bruccoleri R, et al. Severe carbamazepine over-dose treated with lipid emulsion therapy, hemodialysis, andplasmapheresis. Crit Care Med. 2015;43:154.
[53] Aksel G, Guneysel O, Tasyurek T, et al. Intravenous lipid emulsiontherapy for acute synthetic cannabinoid intoxication: clinicalexperience in four cases. Case Rep Emerg Med. 2015;2015:180921.
[54] Barton CA, Johnson NB, Mah ND, et al. Successful treatment of amassive metoprolol overdose using intravenous lipid emulsionand hyperinsulinemia/euglycemia therapy. Pharmacotherapy.2015;35:e56–e60.
[55] Baruah U, Sahni A, Sachdeva HC. Successful management of alu-minium phosphide poisoning using intravenous lipid emulsion:report of two cases. Indian J. 2015;19:735–738.
[56] Bayram B, Kose I, Avci S, et al. Successful treatment of propafe-none intoxication with intravenous lipid emulsion.Pharmacotherapy. 2015;35:e149–e152.
[57] Besserer F, Chuang R, Mink M, et al. Tilmicosin toxicity success-fully treated with calcium, insulin, and lipid emulsion. ClinToxicol. 2015;53:711–712.
[58] Brumfield E, Bernard KR, Kabrhel C. Life-threatening flecainideoverdose treated with intralipid and extracorporeal membraneoxygenation. Am J Emerg Med. 2015;33:1840 e3–5.
[59] Christianson D, Vazquez-Grande G, Strumpher J, et al. Veno-arter-ial extracorporeal membrane oxygenation to treat cardiovascularcollapse following a massive diltiazem overdose. AmericanJournal of Respiratory and Critical Care Medicine Conference:American Thoracic Society International Conference, ATS; 2015.P. 191 (no pagination).
[60] Czerwonka E, Heim M. Lipid rescue therapy and hyperinsuline-mia/euglycemia for atenolol and zolpidem overdose. Crit CareMed. 2015;43:316.
[61] Doepker B, Healy W, Cortez E, et al. High-dose insulin and intra-venous lipid emulsion therapy for cardiogenic shock induced byintentional calcium-channel blocker and Beta-blocker overdose:a case series. J Emerg Med. 2014;46:486–490.
910 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

[62] Gerard L, Galloy AC, Capron A, et al. Mixed amlodipine/valsartanoverdose treated by the molecular adsorbent recirculating system(MARS). Clin Toxicol. 2015;53:573–577.
[63] Hatten BW. QRS widening associated with quetiapine toxicity.Clin Toxicol. 2015;53:698–699.
[64] Johnson-Arbor K, Salinger L, Luczycki S. Prolonged laboratoryinterference after administration of intravenous lipid emulsiontherapy. J Med Toxicol: Off J Am Coll Med Toxicol. 2015;11:223–226.
[65] Jovic-Stosic J, Putic V, Zivanovic D, et al. Failure of intravenouslipid emulsion in treatment of cardiotoxicity caused by mixedoverdose including dihydropyridine calcium channel blockers.Vojnosanit Pregl. 2016;73:88–91.
[66] Khan A, Raman J, Lateef O. ECMO for shock due to drug over-dose: timely transfer to ECMO capable center can save lives.Chest. 2015;148:197A.
[67] Laes JR, Williams DM, Cole JB. Improvement in hemodynamicsafter methylene blue administration in drug-induced vasodilatoryshock: a case report. J Med Toxicol: Off J Am Coll Med Toxicol.2015;11:460–463.
[68] Li K, Gugelmann H, Tabas JA. Young woman with seizures. AnnEmerg Med. 2015;66:363–367.
[69] Lookabill SK, Carpenter C, Ford MD. Accidental pediatric flecainideoverdose treated with intravenous lipid emulsion and sodiumbicarbonate. Clin Toxicol. 2015;53:701–702.
[70] Markota A, Hajdinjak E, Rupnik B, et al. Treatment of near-fatalbeta blocker and calcium channel blocker intoxication withhyperinsulinemic euglycemia, intravenous lipid emulsions andhigh doses of norepinephrine. Signa Vitae. 2015;10:144–150.
[71] Matsumoto H, Ohnishi M, Takegawa R, et al. Effect of lipid emul-sion during resuscitation of a patient with cardiac arrest afteroverdose of chlorpromazine and mirtazapine. Am J Emerg Med.2015;33:1541 e1–2.
[72] McBeth PB, Missirlis PI, Brar H, et al. Novel therapies for myocar-dial irritability following extreme hydroxychloroquine toxicity.Case Rep Emerg Med. 2015;2015:692948.
[73] Montague AJ, Topeff JM, Katzung KG, et al. High dose insulin totreat propranolol toxicity in a 7-month-old infant. Clin Toxicol.2015;53:740.
[74] Mukhtar O, Archer JR, Dargan PI, et al. Lesson of the month 1:acute flecainide overdose and the potential utility of lipidemulsion therapy. Clin Med (London, England). 2015;15:301–303.
[75] Ovakim DH, Gill GK, Kaila KS, et al. Near cardiovascular collapsefollowing intentional European Yew (Taxus baccata) ingestion.Clin Toxicol. 2015;53:747–748.
[76] Ozcete E, Uz I, Kiyan S. Cardiac arrest due to a lethal dose ofpropafenone and first case to survive following treatment withintravenous fat emulsion. Nobel Med. 2015;11:89–92.
[77] Radley D, Droog S, Barragry J, et al. Survival following massiveamitriptyline overdose: the use of intravenous lipid emulsion ther-apy and the occurrence of acute respiratory distress. J IntensiveCare Soc. 2015;16:181–182.
[78] Reynolds JC, Judge BS. Successful treatment of flecainide-inducedcardiac arrest with extracorporeal membrane oxygenation in theED. Am J Emerg Med. 2015;33:1542 e1–1542.
[79] Sampson CS, Bedy SM. Lipid emulsion therapy given intraos-seously in massive verapamil overdose. Am J Emerg Med.2015;33:1844 e1.
[80] Schult R, Gorodetsky RM, Wiegand TJ. Intravenous lipid emulsionfor amlodipine/benazepril toxicity: a case report. Clin Toxicol.2015;53:251–252.
[81] Sebe A, Disel NR, Acikalin Akpinar A, et al. Role of intravenouslipid emulsions in the management of calcium channel blockerand beta-blocker overdose: 3 years experience of a universityhospital. Postgrad Med. 2015;127:119–124.
[82] Su J. Early venoarterial extracorporeal membrane oxygenation forrefractory shock secondary to amlodipine overdose. J Am CollCardiol. 2015;65:A627.
[83] Szadkowski M, Caravati EM, Gamboa D, et al. Treatment of flecai-nide toxicity in a 12-monthold child using intravenous lipid emul-sion. Clin Toxicol. 2015;53:724.
[84] Tse CW, Chan YC, Lau FL. Intravenous lipid emulsion as antidote:experience in Hong Kong. Hong Kong J Emerg Med. 2015;22:100–107.
[85] Tse J, Ferguson K, Whitlow KS, et al. The use of intravenous lipidemulsion therapy in acute methamphetamine toxicity. Am JEmerg Med. 2016;34:1732.e3–4.
[86] Vodnala D, Rosman H, Shakir A. A wide complex rhythm, does ittell the whole story? J Am Coll Cardiol. 2015;65:A750.
[87] Watt P, Malik D, Dyson L. Gift of the glob – is it foolproof?Anaesthesia. 2009;64:1031–1033.
[88] Yesilbas O, Kihtir HS, Altiti M, et al. Acute severe organophos-phate poisoning in a child who was successfully treated withtherapeutic plasma exchange, high-volume hemodiafiltration, andlipid infusion. J Clin Apher. 2015. Epub 2015 Aug 14.
Appendix 1: Voting statements
General statement
Lipid emulsion is indicated in the treatment of XYZ toxicity.
Specific indications
Lipid emulsion is indicated in the treatment of XYZ toxicity:
a. In the presence of cardiac arrest, after Standard ACLS (CPR, airways)has been started
b. In the presence of LIFE-THREATENING toxicity� Lipid emulsion should be administered as first line therapy� Lipid emulsion be administered as part of treatment modalities� Lipid emulsion should be administered if other therapies fail
(last resort)c. In the presence of NON LIFE-THREATENING toxicity
� Lipid emulsion should be administered as first line therapy� Lipid emulsion be administered as part of treatment modalities� Lipid emulsion should be administered if other therapies fail
(last resort)
Types of ILE
The type of ILE to be used is…
� IntralipidVR 10%� IntralipidVR 20%� IntralipidVR 30%� ClinOleicVR 20%� LipofundinVR 20%� Other
If using a bolus of ILE the dose of the bolus indicated is…
� 0.25mL/kg� 0.50mL/kg� 0.75mL/kg� 1.0mL/kg� 1.25mL/kg� 1.5mL/kg� 1.75mL/kg� 2.0mL/kg� Other
CLINICAL TOXICOLOGY 911
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

If using an infusion of ILE the dose of the infusion indicated is…
� 0.25mL/kg/min� 0.5mL/kg/min� 0.75mL/kg/min� 1.0mL/kg/min� Other
Cessation of ILE
The decision to terminate the ILE treatment is indicated based on:
� Total (maximum) duration of the infusion regardless of dose or clin-ical improvement status
� Total (maximum) dose administered regardless of duration of infusionor clinical improvement status
� Clinical improvement regardless of dose or duration administered� Other
In considering the total duration of the infusion as a criterion, lipid emul-sion cessation is indicated, regardless of other factors such as clinicalimprovement or dose after…
� 10–20min� 21–30min� 31–40min� 41–50min� 51–60min� Other
In considering the maximum dose of lipid emulsion administered as acriterion, lipid emulsion cessation is indicated, regardless of clinicalimprovement or duration after…
� 8mL/kg or less� 8.1–10.0mL/kg� 10.1–12.0mL/kg� 12.1–14.0mL/kg� 14.1–16.0mL/kg� 16.1–18.0mL/kg� 18.1–20.0mL/kg� Other
In considering the clinical improvement as a criterion, lipid emulsion ces-sation is indicated, regardless of dose or duration after…
� As soon as symptoms resolution occurred� After resolution of symptoms for 15–30min� After resolution of symptoms for 31–45min� After resolution of symptoms for 46–60min� Other
Appendix 2
Literature update
Search results for the year 2015 update: 1026 citations were reviewed toidentify studies reporting the use of ILE in poisoning (Figure 2). Of those,942 were excluded after reviewing abstracts since the ILE administrationwas not related to poisoning. Of the 84 remaining articles, 28 were fur-ther excluded after reviewing complete manuscripts: one was excludedbecause ILE was not used for the treatment of poisoning, two were pre-treatment studies, one was an animal experiment that was not generaliz-able to humans, 18 were review articles without original data, two onlyreported survey information, and four did not present sufficient data forevaluation. A total of 56 studies were included in the update, from
which eleven were animal reports, two regarding LA and nine non-LApoisonings.[33–43]. Forty-five human reports, eight regarding LA and 37non-LA were included.[44–88] A summary of the new included articles ispresented in Appendices 3 and 4.
Local anaesthetics
No new clinical trials were found in humans. Seven case reports and onecase series reported a total of twelve cases.[44–51] The LAs reportedwere lidocaine (n¼ 2), levobupivacaine (n¼ 1), bupivacaine (n¼ 3), ropi-vacaine (n¼ 3), combination of bupivacaine and ropivacaine (n¼ 1), andropivacaine and lidocaine (n¼ 2). Patients experienced LA toxicity fromdifferent routes of exposure: nerve block (n¼ 7), intravenous (n¼ 4), epi-dural (n¼ 1), subcutaneous (n¼ 1), and intrathecal (n¼ 1) use. Tworeports included two routes of LA exposure, intravenous plus epiduraland intravenous plus subcutaneous. The toxic effects from LAs includeda variety of cardiovascular and central nervous system symptoms includ-ing hypotension, cardiac arrest, agitation and coma. The concentrationof ILE used was reported as 20% (n¼ 5) or not reported (n¼ 7). Dosingregimens and other treatments received were often not reported. Ineight cases, authors noted that the symptoms resolved following ILEdosing. Details are provided in Appendix 3.
Two controlled animal experiments in swine assessed the response ofbupivacaine toxicity to ILE. In one trial, 12 swine were administered4–6mg/kg of bupivacaine until the QRS complex duration was 150% ofbaseline value. Six swine were then given ILE 1.5mL/kg followed by0.25mL/kg/min and six were given the same volume of 0.9% saline ascontrols. All animals survived. QRS duration decreased from 184± 62%ms to 132± 65% ms in the ILE-treated group, while there was no changein QRS duration (230± 56% ms) in the control animals (p¼ 0.03).[34] Theother trial included 30 swine, 10 serving as control, 10 receiving ILE aslong-chain triglycerides (LCT) and 10 receiving ILE as 50% LCT and 50%medium-chain triglycerides (MCT). All animals were administered 5mg/kg of bupivacaine followed by the study drug while monitoring hemo-dynamic parameters. A dose of 4mL/kg of either ILE preparation orsaline was administered to each group one minute after bupivacainedosing. Both ILE groups had a similar improvement in the majority ofthe hemodynamic parameters compared to control.[33] Details arereported in Appendix 4.
There were no new LA case reports described in animals.
Non-local anesthetics
No new clinical trials in humans were identified. Thirty-seven casereports or case series with miscellaneous toxins were found.[52–88] Thesummary of human case reports is presented in Appendix 3.
Three animal experiments studied ILE for non-LA toxicity.[35,39,42] Inone trial, 20 cats with 14 additional controls were exposed dermally topermethrin. ILE was administered to the treatment group at 15mL/kg asa continuous intravenous infusion over 60minutes. A grading system forneurologic effects detected a decrease in the duration and severity ofpoisoning in the treatment group reported as a decrease in the durationand severity of poisoning in the treatment group.[39] Another random-ized experiment in swine sought to determine a difference in meanarterial blood pressure (MAP), QRS duration and survival after diphen-hydramine poisoning. Twenty-four animals were equally divided into twogroups. One group received ILE (7mL/kg) and the other sodium bicar-bonate. Diphenhydramine was administered intravenously until MAP fellby 50%. No differences were found between groups in the measuredparameters.[42] In the third study, rats received intravenous propofol10mg/kg to achieve a 55%±2% drop in MAP. The rats were not rando-mised but the study included a control group receiving saline. Theauthors reported that propofol-mediated hypotension was completelyreversed by ILE, and the effects on the anaesthetic potency of the drugwere minimal.[35] Of note, propofol was not chosen as a toxin to beevaluated for clinical recommendations by the workgroup because ofthe lack of human data. A summary of the animal case reports is avail-able in Appendix 4.
912 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

Search dates: December 16, 2014-December 30, 2015
Records iden�fied through database searching
(n = 3205)
Addi�onal records iden�fied through other sources
(n = 10)
Records a�er duplicates removed (n = 1026)
Ar�cles excluded (n = 28) REASONS ILE not used in poisoning (n = 1) Pre-treatment models (n = 2) Review/opinion ar�cle (no new data) (n = 18) Animal trials could not be extrapolated to humans (n = 1) Survey only (n = 2) Not enough data (n = 4)
Ar�cles included in qualita�ve synthesis for local and non-local anesthe�cs
(n = 56)
11 animal studies 45 human studies
5 RCSs
Full text assessed for eligibility (n = 84)
0 RCTs
6 case reports or case series
45 case reports or series
Records screened (n = 1026)
Records excluded (n = 942)
Figure 2. Selection of articles flow diagram for 2015 update. RCS: randomized controlled studies; RCT: randomized controlled trials; ILE: intravenous lipid emulsion.
CLINICAL TOXICOLOGY 913
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

App
endix3.
Summaryof
the72
patientsinclud
edin
the2015
update
ontheefficacyof
ILEin
poison
ing.
Article
Stud
ytype
Age/sex
Drug,
dose
androute
[Quantitativedrug
con-
centratio
n](coing
estant)
LogDc
Symptom
sILEused
ILEbo
lusdo
sea
ILEinfusion
dose
(total
dose)a
Other
treatm
ents
received
ILEeffect
Outcome
Locala
nesthetics
Glavaset
al.[44]
Case
repo
rt64
y/F
Levobu
pivacaine10
mg
Epidural/In
travenou
s(amoxicillin)
2.68
Hypotension
Coma
20%
200mL
NR
(total:2
00mL)
IVfluids,
Pressors,
Anesthetics,
Atropine
Yes
Survival
Gou
cher
&Asherb
[45]
Case
repo
rt60
y/F
Lido
caine18
mL2%
Intravenou
s1.26
PVC
Coma
NR
150mL
NR
(total:1
50mL)
Epinephrine
Yes;
Nohemod
ynam
iccom-
prom
isethroug
hout
Survival
Kamel
etal.[46]
Case
repo
rt51
y/F
Bupivacaine80
mL5%
Nerve
block
2.68
Dizziness
Agitatio
nPosturing
Loss
ofleftlower
extrem
-ity
sensation
20%
100mL
400mLin
20min
(total:5
00mL)
Epinephrine,
Anesthetics
Unclear
ifdrug
effect
hadjust
wornoff;
Neurologicsymptom
simproved
after
administration
Survival
Musielak&McCall[47]
Case
repo
rt6y/M
Bupivacaine3mg/kg
Subcutaneous/
Intravenou
s
2.68
Hypotension
Bradycardia,asystole
Cardiacarrest
Apnea
Coma
NR
1.5mg/kg
f0.25
mg/kg/m
inforf6h
(total:9
1.5mg/kg)f
Epinephrine,
Pressors,(no
repineph
-rin
e,epinephrine,vaso-
pressin,
phenylephrine)
Unclear
Survival
Procop
ioet
al.[48]
Case
repo
rt43
y/M
Bupivacaine10
mL
Ropivacaine30
mL
Intrathecal
2.68
4.21
Hypotension
Bradycardia
Apnea
Coma
20%
1.5mL/kg
125mLin
2h
(total:N
R)Pressors
Improved
30min
after
ILE
Survival
Riffet
al.d[49]
Case
series,No1
AgeNR/sexNR
Ropivacaine220mg
Nerve
block
[4.20mcg/m
L]
4.21
Seizures
Coma
NR
NR
NR
NR
Authorsstate“quick
symptom
sresolving”
NR
Case
series,No3
AgeNR/F,pregnant
Ropivacaine150mg
Nerve
block
[4.80mcg/m
L]
4.21
Obtun
datio
nNR
NR
NR
NR
Authorsstate“quick
symptom
sresolving”
NR
Case
series,No4
AgeNR/F,pregnant
Ropivacaine100mg
Nerve
block
[0.66mcg/m
L]
4.21
Obtun
datio
nNR
NR
NR
NR
Authorsstate“quick
symptom
sresolving”
NR
Case
series,No7
AgeNR/F,pregnant
Ropivacaine40
mg
[0.51mcg/m
L]Lido
caine200mg
[1.01mcg/m
L]Nerve
block
4.21
1.26
Seizure
Mydriasis
NR
NR
NR
NR
Authorsstate“quick
symptom
sresolving”
NR
Case
series,No8
AgeNR/sexNR
Ropivacaine40
mg
[0.29mcg/m
L]Lido
caine200mg
[0.58mcg/m
L]Nerve
block
4.21
1.26
Hypotension
Bradycardia
Metallic
taste
NR
NR
NR
NR
Authorsstate“quick
symptom
sresolving”
NR
Shih
&Calello
b[50]
Case
repo
rt56
y/F,
weigh
tNR
Bupivacaine30
mL
0.25%
Nerve
block
2.68
Hypotension
Apnea
Coma
Lactate4mmol/L
20%
85mL
NR
(total:8
5mL)
IVfluids,
Pressors,
Anesthetics
Motor
andsensoryfunc-
tionimproved
over
4h
Survival
Stella
etal.b[51]
Case
repo
rt<1week/NR
Lido
caine6mg/kg,then
6mg/kg/h
for18
h,then
4mg/kg/h
for12
hIntravenou
s
1.26
Bradycardia,wideQRS
20%
2mL/kg
NR
NR
WideQRS
andbradycar-
diaresolved
Survival
Non-locala
naesthetics
Agulnik[52]
Case
repo
rt15
y/F
Carbam
azepine56
gOraling
estio
n[138
mcg/m
L]
2.67
Status
epilepticus
Coma(in
ducedwith
barbitu
rates,technically
notfrom
ingestion)
Lactaterepo
rted
ashigh
NR
NR
NR
Plasmapheresis,HDI,
CVVH
DUnclear
Survival
(continued)
914 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7
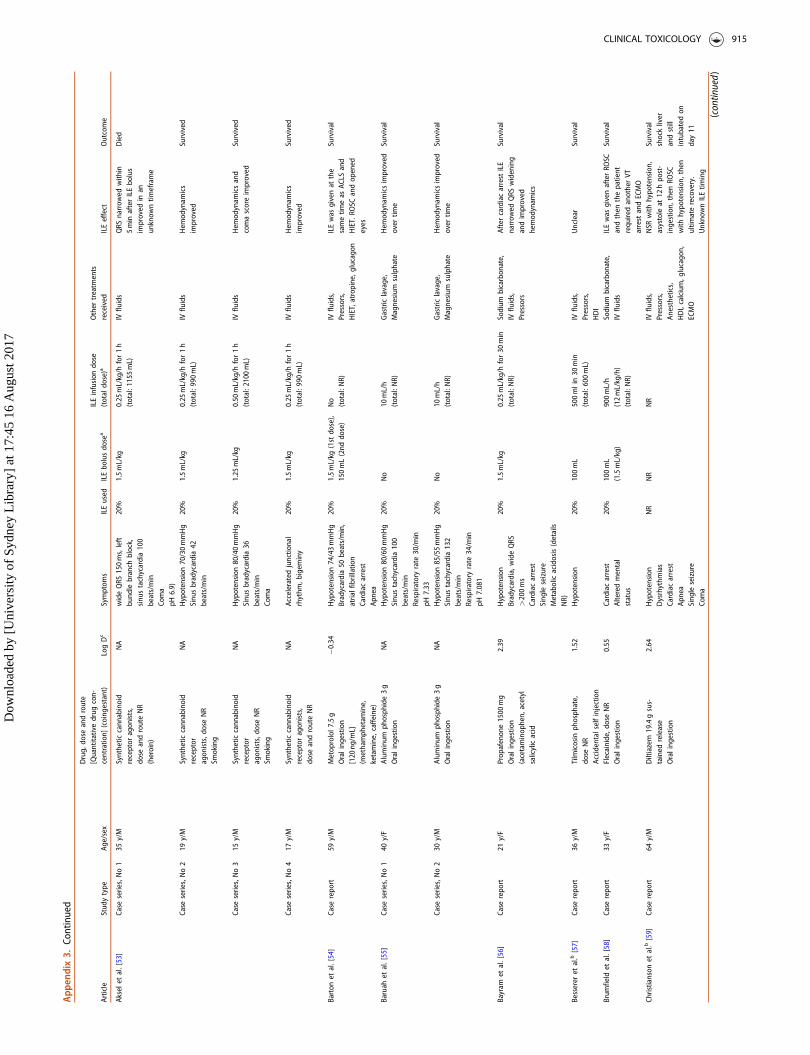
App
endix3.
Continued
Article
Stud
ytype
Age/sex
Drug,
dose
androute
[Quantitativedrug
con-
centratio
n](coing
estant)
LogDc
Symptom
sILEused
ILEbo
lusdo
sea
ILEinfusion
dose
(totaldo
se)a
Other
treatm
ents
received
ILEeffect
Outcome
Aksele
tal.[53]
Case
series,No1
35y/M
Synthetic
cann
abinoid
receptor
agon
ists,
dose
androuteNR
(heroin)
NA
wideQRS
150ms,left
bund
lebranch
block,
sinu
stachycardia100
beats/min
Coma
pH6.9)
20%
1.5mL/kg
0.25
mL/kg/h
for1h
(total:1
155mL)
IVfluids
QRS
narrow
edwith
in5min
afterILEbo
lus
improved
inan
unknow
ntim
eframe
Died
Case
series,No2
19y/M
Synthetic
cann
abinoid
receptor
agon
ists,d
oseNR
Smoking
NA
Hypotension
70/30mmHg
Sinu
sbradycardia42
beats/min
20%
1.5mL/kg
0.25
mL/kg/h
for1h
(total:9
90mL)
IVfluids
Hem
odynam
ics
improved
Survived
Case
series,No3
15y/M
Synthetic
cann
abinoid
receptor
agon
ists,d
oseNR
Smoking
NA
Hypotension
80/40mmHg
Sinu
sbradycardia36
beats/min
Coma
20%
1.25
mL/kg
0.50
mL/kg/h
for1h
(total:2
100mL)
IVfluids
Hem
odynam
icsand
comascoreimproved
Survived
Case
series,No4
17y/M
Synthetic
cann
abinoid
receptor
agon
ists,
dose
androuteNR
NA
Acceleratedjunctio
nal
rhythm
,bigem
iny
20%
1.5mL/kg
0.25
mL/kg/h
for1h
(total:9
90mL)
IVfluids
Hem
odynam
ics
improved
Survived
Barton
etal.[54]
Case
repo
rt59
y/M
Metop
rolol7
.5g
Oraling
estio
n[120
ng/m
L](m
ethamph
etam
ine,
ketamine,caffe
ine)
�0.34
Hypotension
74/43mmHg
Bradycardia50
beats/min,
atrialfibrillatio
nCardiacarrest
Apnea
20%
1.5mL/kg
(1st
dose),
150mL(2nd
dose)
No
(total:N
R)IV
fluids,
Pressors,
HIET,atropine,g
lucago
n
ILEwas
givenat
the
sametim
eas
ACLS
and
HIET.RO
SCandop
ened
eyes
Survival
Baruah
etal.[55]
Case
series,No1
40y/F
Alum
inum
phosph
ide3g
Oraling
estio
nNA
Hypotension
80/60mmHg
Sinu
stachycardia100
beats/min
Respiratory
rate
30/m
inpH
7.33
20%
No
10mL/h
(total:N
R)Gastriclavage,
Magnesium
sulphate
Hem
odynam
icsimproved
over
time
Survival
Case
series,No2
30y/M
Alum
inum
phosph
ide3g
Oraling
estio
nNA
Hypotension
85/55mmHg
Sinu
stachycardia132
beats/min
Respiratory
rate
34/m
inpH
7.081
20%
No
10mL/h
(total:N
R)Gastriclavage,
Magnesium
sulphate
Hem
odynam
icsimproved
over
time
Survival
Bayram
etal.[56]
Case
repo
rt21
y/F
Prop
afenon
e1500
mg
Oraling
estio
n(acetaminop
hen,
acetyl
salicylicacid
2.39
Hypotension
Bradycardia,wideQRS
>200ms
Cardiacarrest
Sing
leseizure
Metabolicacidosis(details
NR)
20%
1.5mL/kg
0.25
mL/kg/h
for30
min
(total:N
R)Sodium
bicarbon
ate,
IVfluids,
Pressors
Aftercardiacarrest
ILE
narrow
edQRS
widening
andimproved
hemod
ynam
ics
Survival
Besserer
etal.b[57]
Case
repo
rt36
y/M
Tilmicosin
phosph
ate,
dose
NR
Accidental
selfinjection
1.52
Hypotension
20%
100mL
500mlin30
min
(total:6
00mL)
IVfluids,
Pressors,
HDI
Unclear
Survival
Brum
field
etal.[58]
Case
repo
rt33
y/F
Flecainide,d
oseNR
Oraling
estio
n0.55
Cardiacarrest
Alteredmental
status
20%
100mL
(1.5mL/kg)
900mL/h
(12mL/kg/h)
(total:N
R)
Sodium
bicarbon
ate,
IVfluids
ILEwas
givenafterRO
SCandthen
thepatient
requ
iredanotherVT
arrest
andECMO
Survival
Christianson
etal.b[59]
Case
repo
rt64
y/M
Diltiazem
19.4gsus-
tained
release
Oraling
estio
n
2.64
Hypotension
Dysrhythm
ias
Cardiacarrest
Apnea
Sing
leseizure
Coma
NR
NR
NR
IVfluids,
Pressors,
Anesthetics,
HDI,calcium,g
lucago
n,ECMO
NSR
with
hypo
tension,
asystole
at12
hpo
st-
ingestion,
then
ROSC
with
hypo
tension,
then
ultim
aterecovery.
Unkno
wnILEtim
ing
Survival
shockliver
andstill
intubatedon
day11
(continued)
CLINICAL TOXICOLOGY 915
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

App
endix3.
Continued
Article
Stud
ytype
Age/sex
Drug,
dose
androute
[Quantitativedrug
con-
centratio
n](coing
estant)
LogDc
Symptom
sILEused
ILEbo
lusdo
sea
ILEinfusion
dose
(total
dose)a
Other
treatm
ents
received
ILEeffect
Outcome
Czerwon
ka&Heim
b[60]
Case
repo
rt33
y/F
Atenolol,d
oseNR
Oraling
estio
n(zolpidem,acetamino-
phen,ethanol)
�2.03
Hypotension
Coma
NR
NR
NR
IVfluids,
Pressors,
Anesthetics
HDI,bloodprod
ucts,
activated
charcoal,ace-
tylcysteine,calcium
Unclear
Survival
Doepker
etal.e[61]
Case
series,No1
35y/M
Metop
rolol1
180mg
Amlodipine
150mg
Verapamil10.26gER
Oraling
estio
n(in
sulin)
�0.34
2.00
2.91
Non
-measurableblood
pressure
Bradycardicarrest
<20
beats/min
Coma
20%
1.5ml/kg
(130
mL)
0.25
mL/kg/m
infor1h
(total:N
R)IV
fluids,
Pressors,
HDI,atropine,calcium
,glucagon
Authorsno
teabenefit
ofILEtherapyforthe
amlodipine
overdo
se
Survival
Case
series,No2
59y/M
Metform
in30
gAm
lodipine
300mg
Lisino
pril300mg
Simvastatin,d
oseNR
Oraling
estio
n
�5.44
2.00
�1.80
4.60
Hypotension
78/36mmHg
Bradycardia54
beats/min
Lactate6.6mmol/L,
aniongap17
20%
1.5mL/kg
(105
mL)
0.25
mL/kg/m
infor1h
(total:N
R)IV
fluids,
Activated
charcoal,d
ex-
trose,calcium,g
lucago
n,HDI
Authorsno
teabenefit
ofILEtherapyforthe
amlodipine
overdo
se
Survival
Gerardet
al.[62]
Case
repo
rt58
y/F
Amlodipine
480mg
Valsartan3680
mg
Oraling
estio
n
2.00
�0.34
Hypotension
78/57mmHg
Tachycardia103beats/min,
QT555ms
Lactate18
mmol/L
pH7.23
20%
No
8mL/kg
for10
min
(total:8
0mL/kg)
IVfluids,
Pressors,
Calcium,H
IET,methylene
blue,M
ARS
Improvem
entwas
not
seen
with
ILE,respon
ded
totheuseof
MAR
S
Survival
Hatten[63]
Case
repo
rt32
y/F
Quetiapine,d
oseNR
Oraling
estio
n[5929ng
/mL]
(heroin;
positive,
unknow
nmatricxfor
morph
ine,oxycod
one)
1.82
Hypotension
Tachycardia,wideQRS
>160ms(previou
s92
ms)
Cardiacarrest
Apnea
Coma
Lactate25
mmol/L
pH7.27
NR
NR
NR
Sodium
bicarbon
ate,
IVfluids,
Pressors,
Anesthetics,
Naloxon
e
Hem
odynam
icsdidno
tchange
inrelatio
nto
ILE,
QRS
narrow
edwith
bicarbon
ate
Died;
Nocomplications
repo
rted
toILE
John
son-Arbo
ret
al.e
[64]
Case
repo
rt43
y/F
Prop
rano
lol1
2g
[3.5mg/Lafter23
h]Tram
adol
1.5g
Zolpidem
200mg
Alprazolam
15mg
Acetam
inop
hen,
dose
NR
Oraling
estio
ns
0.99
0.40
2.35
2.50
0.40
Hypotension
64/47mmHg
Cardiogenic
shock,ejectio
nfractio
n20%
Apnea
Coma
20%
1.5mL/kg
x30.25
mL/kg/m
in(total:N
R)IV
fluids,
Pressors,
Anesthetics,
Insulin,G
lucago
n
No
Died,
Labo
ratory
evalu-
ationimpo
ssible
dueto
lipem
ia
Jovic-Stosicet
al.[65]
Case
series,No1
24y/F
Amlodipine
150mg
[0.05mg/L]
Metform
in10
g[6.32mg/L]
Gliclizide2.4g
[3.95mg/L]
Oraling
estio
n
2.00
�5.44
0.16
Hypotension
Dysrhythm
ias
Cardiacarrest
Lactate
4.9mmol/L,p
H7.27
20%
100mL
900mL
(total:1
000mL)
IVfluids,
Pressors,
Anesthetics,Glucago
n
Transientbloodpressure
improvem
entthen
none
further
Died
Case
series,No2
41y/M
Nifedipine,d
oseNR
[0.62mg/L]
Metop
rolol,do
seNR
[0.57mg/L]
Diazepam,d
oseNR
[1.04mg/L]
Oraling
estio
n
3.45
�0.34
3.86
Hypotension
Dysrhythm
ias,type
2,then
type
3AV
block
Cardiacarrest
Apnea
Coma
20%
500mL
NR
(total:5
00mL)
IVfluids,
Pressors,
Calcium,G
lucago
n
Noimprovem
entin
hemod
ynam
ics
Died
(continued)
916 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

App
endix3.
Continued
Article
Stud
ytype
Age/sex
Drug,
dose
androute
[Quantitativedrug
con-
centratio
n](coing
estant)
LogDc
Symptom
sILEused
ILEbo
lusdo
sea
ILEinfusion
dose
(total
dose)a
Other
treatm
ents
received
ILEeffect
Outcome
Khan
etal.[66]
Case
repo
rt31
y/F
Amlodipine,d
oseNR
Losartan,d
oseNR
Oraling
estio
n
2.00
1.61
Hypotension
Apnea
Coma
NR
NR
NR
IVfluids,
Pressors,
ECMO
Noimprovem
entwith
pharmacolog
ictherapy
Survival
Laes
etal.e[67]
Case
repo
rt61
y/M
Atenolol
500mg
Amlodipine
200mg
Losartan
375mg
Oraling
estio
n
�2.03
2.00
1.61
Hypotension
,MAP
55mmHg,
ejectio
nfrac-
tion60-65%
Lactate4.5mmol/L
20%
1.5mL/kg
NR
IVfluids,
Pressors,
HIET/CV
VHD,m
ethylene
blue
2mL/kg
in30
min
Minimal
change
inblood
pressure
orheartrate
Survival
Liet
al.[68]
Case
repo
rt25
y/F
Diphenh
ydramineoral
mixture,d
oseNR
Oraling
estio
n
1.92
Hypotension
WideQRS
120ms
Status
epilepticus
20%
Yes,do
seNR
NR
Sodium
bicarbon
ate,
IVfluids,
Pressors
ILEgivenafterother
treatm
ents
failedand
better
<1hwith
improved
hemod
ynam
ics
andnarrow
edQRS
Survival
Lookabill
etal.b[69]
Case
repo
rt17
mth/F
Flecainide
100mg
RouteNR
0.55
Hypotension
64/41mmHg
WideQRS
162ms
Coma
20%
11mL
(1mL/kg)
165mL/h
0.25
mL/kg/m
in(total:
NR)
Sodium
bicarbon
ate
Unclear;Sym
ptom
simproved
afterconcur-
rent
bolusof
bicarbon
ate
Survival
Markota
etal.[70]
Case
repo
rt66
y/M
Bisoprolol
450mg
Amlodipine
300mg
Doxazosin
200mg
Nifedipine
600mg
Torsem
ide150mg
Acetylsalicylicacid
4000
mg
Ibup
rofen5000
mg
Oraling
estio
n
0.11
2.00
0.54
3.45
1.44
�1.69
0.45
Hypotension
Coma
Lactate8.5mmol/L
pH7.12
20%
100mL
150mLin
60min
(total:2
50mL)
IVfluids,
Pressors,
Calcium,G
lucago
n,HDI
Unclear
Possible
improvem
entcoinciding
with
ILE
Survival
Matsumotoet
al.[71]
Case
repo
rt24
y/F
Chlorpromazine3g
Mirtazapine990mg
Oraling
estio
n
3.42
2.40
Hypotension
80/50mmHg
Asystole
Cardiacarrest
Apnea
Coma
Lactate138mg/dL
pH7.13
20%
100mLx2
No
(total:2
00mL)
Pressors,
ECMO
Norespon
seto
1stdo
se.
ECMOinitiated
after
ROSC
2min
after2nd
dose
ILE
Survival
McBethet
al.[72]
Case
repo
rt23
y/F
Hydroxychloroqu
ine40
gOraling
estio
n[6425mmol/L
at12
h]
1.96
Hypotension
92/60mmHg
anddeclining
Ventricular
fibrillatio
n,PM
VT,Q
RS140ms,QT
576ms
Apnea
Coma
pH7.33
20%
1.5mL/kg
DoseNR,
duratio
n30
min
(total:5
00mL)
Sodium
bicarbon
ate,
IVfluids,
Pressors,
HD,calcium
channel
blocker
Authorsrepo
rt“im
provem
entafterILE
andHD”
Survival
Mon
tagu
e[73]
Case
repo
rt7mth/F
Prop
rano
lol1
08mg
Oraling
estio
n0.99
Hypotension
Bradycardia
Coma
20%
No
1.5mL/kg
in2h
(total:1
.5mL/kg)
IVfluids,
HIET
Hem
odynam
icsdidno
timprovewith
ILE
Survival
Muktar[74]
Case
repo
rt13
y/F
Flecainide
900mg
Oraling
estio
n(bisop
rolol,acetylsali-
cylic
acid)
0.55
Hypotension
70/39mmHg
VT,ventricular
fibrillatio
n,TdP,
Brug
adapattern
Cardiacarrest
Veno
uspH
7.55
20%
70mL
225mLin
20min
(total:2
95mL)
Sodium
bicarbon
ate,
IVfluids,
Pressors,
Glucago
n
ILEgivenafterRO
SCfor
cardiacarrest
notbefore
Survival
Ovakim
etal.b[75]
Case
repo
rt21
y/F
Yew
250mLcutleaves
Oraling
estio
nNA
Hypotension
WideQRS,irregular
heart
rhythm
Coma
NR
NR
NR
Sodium
bicarbon
ate,
IVfluids
Nodescrip
tionof
any
changesafterILE
Survival
(continued)
CLINICAL TOXICOLOGY 917
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

App
endix3.
Continued
Article
Stud
ytype
Age/sex
Drug,
dose
androute
[Quantitativedrug
con-
centratio
n](coing
estant)
LogDc
Symptom
sILEused
ILEbo
lusdo
sea
ILEinfusion
dose
(totaldo
se)a
Other
treatm
ents
received
ILEeffect
Outcome
Ozceteet
al.[76]
Case
repo
rt35
y/F
Prop
afenon
e150mg
Oraling
estio
n2.39
Hypotension
Dysrhythm
ias,QRS
160ms
Cardiacarrest
Sing
leseizure
Status
epilepticus
Coma
NR
100mL
0.25
mL/kg/h
for1h
(total:N
R)Sodium
bicarbon
ate,
IVfluids,
Pressors,
Atropine
Unclear
Survival
Radley
[77]
Case
repo
rtNR/NR
Amitriptyline4.8g
Oraling
estio
n(ethanol,venlafaxine,
zopiclon
e)
3.96
Hypotension
QTc
prolon
gatio
n3isolated
seizures
x3pH
7.45-7.6
NR
NR
NR
(total:5
00mL)
Sodium
bicarbon
ate,
IVfluids,
Pressors,
Midazolam
Improvem
entin
MAP
anddecreaseduseof
Pressorsrequ
iredlate,
butno
toxin
confirm
ation
Survival;
ARDSon
day3
Reynolds
&Judg
e[78]
Case
repo
rt24
y/F
Flecainide,d
oseNR
Oraling
estio
n[11,085ng
/mLat
4h]
0.55
Hypotension
Bradycardia,wideQRS
Cardiacarrest
(PEA
)Ap
nea
Sing
leseizure
Status
epilepticus
Coma
Lactate4mmol/L
Arterialp
H7.08
20%
200mL
No
(total:2
00mL)
Sodium
bicarbon
ate,
IVfluids,
Pressors
Noeffect
ofILE
Survival
Sampson
e[79]
Case
repo
rt24
y/F
Verapamil7.2gER
and
80mgimmediate-release
Oraling
estio
n
2.91
Hypotension
65/30mmHg
Tachycardia80
beats/min
20%
60mLIO
andthen
60mLIV
No
(total:1
20mL)
IVfluids,
Pressors,
Glucago
n,HIET
Noeffect
ofILE
Died
(The
patient
repo
rted
pain
dur-
ingIO
bolus
infusion
)Schu
ltet
al.[80]
Case
repo
rt12
y/F
Amlodipine
240mg
[87ng
/mL]
Benazepril480mg
Oraling
estio
n
2.00
�0.71
Hypotension
Coma
20%
100mL
NR
NR
NR
NR
Sebe
etal.[81]
Case
series,No1
27y/F
Diltiazem
2400
mg
(40mg/kg)
Oraling
estio
n
2.64
Hypotension
2nddegree
heartblock
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids,
Calcium,H
IET,
Tempo
rary
pacemaker
Normotensive
afterILE
Survived
Case
series,No2
21y/F
Amlodipine
140mg
(1.86mg/kg)
Oraling
estio
n
2.00
Hypotension
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids,
Calcium,H
IET
Normotensive
afterILE
Survived
Case
series,No3
51y/M
Metop
rolol1
800mg
(30mg/kg)
Oraling
estio
n
�0.34
Cardiacarrest
20%
1.5mL/kg
x3No
(total:4
.5mL/kg)
IVfluids,
Glucago
n,Mechanicalventilation
Noimprovem
entin
hemod
ynam
ics
Died
(ARD
S)
Case
series,No4
44y/F
Valsartan1600
mg
(17.7mg/kg)
Amlodipine
100mg
(1.11mg/kg)
Oraling
estio
n
�0.34
2.00
Hypotension
20%
1.5mL/kg
x3No
(total:4
.5mL/kg)
IVfluids,
Calcium,H
IET
Noimprovem
entin
hemod
ynam
ics
Survived
Case
series,No5
22y/F
Amlodipine
90mg
(1.63mg/kg)
Oraling
estio
n
2.00
Hypotension
20%
1.5mL/kg
x3No
(total:4
.5mL/kg)
IVfluids,
Calcium,H
IET
Noimprovem
entin
hemod
ynam
ics
Survived
Case
series,No6
32y/F
Amlodipine
150mg
(1.76mg/kg)
Oraling
estio
nAcetam
inop
hen
(paracetam
ol)
2.00
3rddegree
heartblock
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids,
Calcium,A
cetylcysteine,
Tempo
rary
pacemaker
Normotensive
afterILE
Survived
Case
series,No7
31y/F
Amlodipine
110mg
(1.46mg/kg)
Oraling
estio
n
2.00
Hypotension
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids
Calcium,H
IET
Normotensive
afterILE
Survived
Case
series,No8
23y/F
Carvedilol7
50mg
(12.5mg/kg)
Oraling
estio
n
3.16
Hypotension
Bradycardia
20%
1.5mL/kg
x2No
(total:3
.0mL/kg)
IVfluids,
Glucago
nTempo
rary
pacemaker
Normotensive
afterILE
Survived
(continued)
918 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

App
endix3.
Continued
Article
Stud
ytype
Age/sex
Drug,
dose
androute
[Quantitativedrug
con-
centratio
n](coing
estant)
LogDc
Symptom
sILEused
ILEbo
lusdo
sea
ILEinfusion
dose
(totaldo
se)a
Other
treatm
ents
received
ILEeffect
Outcome
Case
series,No9
18y/F
Verapamil2880
mg
(41.1mg/kg)
Oraling
estio
n
2.91
Cardiacarrest
20%
1.5mL/kg
x2No
(total:3
.0mL/kg)
IVfluids,
Calcium,H
IET
Mechanicalventilation
Normotensive
afterILE
Hypoxic,ischemic
enceph
alop
athy
Case
series,No10
21y/F
Prop
rano
lol9
60mg
(11.3mg/kg)
Oraling
estio
n
0.99
Hypotension
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids,
Glucago
nNormotensive
afterILE
Survived
Case
series,No11
31y/M
Amlodipine
210mg
(2.33mg/kg)
Oraling
estio
n
2.00
Hypotension
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids,
Calcium,H
IET
Normotensive
afterILE
Hypoxicischem
icenceph
alop
athy
Case
series,No12
26y/F
Carvedilol6
25mg
(9.6mg/kg)
Oraling
estio
n
3.16
Hypotension
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids,
Glucago
nNormotensive
afterILE
Survived
Case
series,No13
44y/F
Verapamil1320
mg
(16.5mg/kg)
Oraling
estio
n
2.91
Hypotension
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids,
Calcium,H
IET
Normotensive
afterILE
Survived
Case
series,No14
24y/M
Prop
rano
lol,do
seNR
Oraling
estio
n0.99
Hypotension
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids,
Glucago
nNormotensive
afterILE
Survived
Case
series,No15
33y/M
Prop
rano
lol8
00mg
(0.94mg/kg)
Oraling
estio
n
0.99
Hypotension
20%
1.5mL/kg
No
(total:1
.5mL/kg)
IVfluids
Glucago
nNormotensive
afterILE
Survived
Sub[82]
Case
repo
rt17
y/M
Amlodipine
1.25
gOraling
estio
n(m
anycoingestants
(unspecified))
2.00
Hypotension
50/30mmHg
Bradycardia40
beats/min,
3rddegree
block
NR
NR
NR
IVfluids,
Pressors,
Calcium,Insulin,
Glucago
n,ECMO
Improvem
entwas
not
seen
with
ILE,patient
improved
with
ECMO
Survival
Szadkowskie
tal.[83]
Case
repo
rt12
mth/M
Flecainide,d
oseNR
RouteNR
[2.57mcg/m
L]
0.55
Hypotension
Dysrhythm
ias
Apnea
Coma
20%
1.5mL/kg
0.25
mL/kg/h
for2h.
Then
stop
pedfor30
min
andthen
restarted
Sodium
bicarbon
ate,
IVfluids,
Pressors
VTrecurred
30min
after
1stinfusion
ended,
resolved
afterrestartin
gILEinfusion
andsodium
bicarbon
ate.
Survival
Tseet
al.[84]
Note:Poison
center
stud
yof
avariety
oftox-
ins,2ndhand
inform
ation
Case
series,No1
45y/M
Prop
rano
lol,do
seNR
Dothiepin,d
oseNR
Oraling
estio
n
0.99
2.92
Cardiacarrest
20%
100mL
NR
Sodium
bicarbon
ate
Positiveeffect
ofILEon
ROSC
Survival
Case
series,No2
46y/F
Amitriptyline,do
seNR
Oraling
estio
n3.96
QRS
changes(detailsNR)
Cardiacarrest
20%
100mL
0.25
mL/kg/m
infor30
min
(total:N
R)
Sodium
bicarbon
ate,
Pressors
Authorsrepo
rt“Effe
cton
hemod
ynam
ics”
Survival
Case
series,No3
45y/F
Amitriptyline,do
seNR
Oraling
estio
n3.96
WideQRS
NR
No
0.25
mL/kg/m
infor2h
Sodium
bicarbon
ate
NR
Survival
Tseet
al.[85]
Case
repo
rt55
y/M
Methamph
etam
ine“egg
size”do
seOraling
estio
n
�0.57
Tachycardia
Adrenergicsymptom
s20%
1.5mL/kg
NR
(total:1
.5mL/kg)
NR
Resolutio
nof
hyperadre-
nergicexcess
in20
min
Survival
Vodn
ala[86]
Case
repo
rt50
y/M
Flecainide,d
oseNR
Oraling
estio
n[5.89mcg/m
L](cardizem,arip
iprazole)
0.55
Hypotension
WideQRS,Q
T700ms
Cardiacarrest
Sing
leseizure
Coma
NR
NR
NR
Sodium
bicarbon
ate,
IVfluids
ILEdidno
tappear
toaffect
theou
tcom
eDied
Wattet
al.[87]
Case
Series,No1
Youn
g/F
Quetiapine
4.3g
Oraling
estio
n(diazepam
300mg,
acet-
aminop
hen(paraceta-
mol)/dihydrocod
eine,fer-
rous
fumarate)
1.82
Coma
20%
NR
NR
(reports‘Stand
ardlipid
rescue
protocol’)
NR
No
Survival
Case
series,No2
Middle-aged/F
Quetiapine
4.6g
Oraling
estio
nAcetam
inop
hen
(paracetam
ol)
1.82
Hypotension
Sinu
stachycardia120
beats/min,Q
Tc550ms
Coma
20%
NR
NR
(reports‘Stand
ardlipid
rescue
protocol’)
IVfluids,
Acetylcysteine
No
Survival
(continued)
CLINICAL TOXICOLOGY 919
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

App
endix3.
Continued
Article
Stud
ytype
Age/sex
Drug,
dose
androute
[Quantitativedrug
con-
centratio
n](coing
estant)
LogDc
Symptom
sILEused
ILEbo
lusdo
sea
ILEinfusion
dose
(totaldo
se)a
Other
treatm
ents
received
ILEeffect
Outcome
Yesilbas
etal.[88]
Case
repo
rt8y/M
Organop
hosphate
(from
eatin
gleeks)
Oraling
estio
n
NA
Bradycardia
Coma
20%
NR
8g/kg/day
for2days
(total:1
6g/kg)
Atropine,P
ralidoxime,
CVVH
DNoimmediate
improve-
mentandothertreat-
ments
given.
Improved
over
4days
Survival
ACLS:Ad
vanced
cardiaclifesupp
ort;AR
DS:
Acuterespiratory
distress
synd
rome;
BP:BLoodPressure;CV
VHD:Co
ntinuo
usVeno
veno
usHem
odialysis;
ECMO:Extracorpo
real
mem
braneoxygenation;
ER:Extend
edrelease;
HDI:Highdo
seinsulin;HD:
Hem
odialysis;HIET:
High-do
seinsulin
euglycem
iatherapy;
ILE:
Intravenou
slipid
emulsion
;MAR
S:Molecular
AdsorbentRecirculationSystem
;MAP
:Meanarterialpressure;NA:
notapplicable;NR:
Not
repo
rted;NSR:Normal
sinu
srhythm
;PEA:
Pulseless
electrical
activity;P
MVT:P
olym
orph
icventricular
tachycardia;PV
C:Prem
atureventricular
contractions;R
OSC:R
eturnof
spon
taneou
scirculation;
RSI:Rapidsequ
ence
indu
ction;
TdP:
Torsadede
pointes;VA
:Veno-arterial;VES:
Ventricular
extrasystoles;VT:
Ventricular
tachycardia.
a The
totald
osein
g/kg
was
infrequentlyavailable,andcouldon
lybe
calculated
ifbo
dyweigh
twas
repo
rted.
bAvailableas
abstract
onlyat
thetim
eof
writing.
c Adapted
from
www.chemspider.com
.The
logDrefersto
thelogarithm
ofoctano
l/water
partition
coefficient.
dIndividu
alpatient
details
areno
trepo
rted
forthecase
series.
e Fulltextarticle
includ
edas
itisavailableat
thetim
eof
writing,
andinclud
esmoreinform
ationcomparedto
abstract
referenceinclud
edin
thesystem
aticreview
(5).
f These
dosesarelikelyin
mL/kg
butaretranscrib
edas
repo
rted
intheoriginalarticle.
920 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

App
endix4.
Summaryof
the11
animalstud
iesinclud
edin
the2015
update.
Article
(Species)
Mod
elPoison
,doseand
route
LogD
Symptom
sILEused
ILEbo
lusa
ILE
infusion
Stud
yarms
Timingof
rescue,
timefrom
LAterm
ination
Other
treatm
ents
received
bParameter
measured
Outcome
Supp
orteffect
ofILE
Locala
nesthetics
RCS
Udelsman
[33]
(Pigs)
Rand
omized
trial
Bupivacaine
5mg/kg
Intravenou
s
2.68
Fallin
arterialB
P,andventricular
sys-
tolic
workindex
NR
4mL/kg
No
LCT
vs LCT/MCT
vs Saline
Stud
ytreatm
ents
1min
afterLA
NR
ArterialB
P,CI
and
ventricular
systolic
workindex
Survival
NR
Yes;Bo
thlipid
emulsion
swereeffi-
cientandsimilar
optio
nsto
reverse
hypo
tension
Zaballos[34]
(Pigs)
Rand
omized
trial
Bupivacaine
4–6mg/kg
Intravenou
s
2.68
150%
increase
inQRS
20%
1.5mL/kg
0.25
mL/kg/m
inTimeNR
ILE
vs Saline(detailsNR)
NR
NR
QRS
Survival:
ILE6/6
Saline6/6
Yes;Bu
tcontrol
grou
pQRS
was
wider
Non-locala
nesthetics
RCS
Bourqu
e[35]
(Rats)
Controlledtrial
Prop
ofol
10mg/kg
Intravenou
s3.88
Hypotension
NR
4mL/kg
No
ILE
vs Saline
NR
NR
MAP
,cortical
activ-
ityassessmentsby
EEG
Survival
rate
NR
ILEsuperio
rto
salinein
therever-
salo
fdecreased
MAP
with
minimal
effect
ontheanes-
theticprofile
ofprop
ofol
Yes
Peacock[39]
(Cats)
Rand
omized
trial
Perm
ethrin,d
ose
NR
Topical
6.47
Somehadsing
leseizures
20%
No
15mL/kg
in60
min
ILE
vs Saline
Variable
Supp
ortive,details
NR
Metho
carbam
olfor
seizure-likeactivity,
diazepam
Authorsgraded
the
cats’n
eurologicsta-
tusesandfoun
da
decrease
inthe
timeandseverityof
poison
ingin
the
treatm
entgrou
p
Survival:
ILENR/20
SalineNR/14
Yes;ILE-treatedcats
improved
earlier
comparedto
con-
trol
cats
Varney
[42]
(Pigs)
Rand
omized
trial
Diphenh
ydramine
1mg/kg/m
inIntravenou
s
1.92
Diphenh
ydramine
dosing
continued
until
MAP
was
60%
ofbaseline
20%
7mL/kg
0.25
mL/kg/m
inILE
vs Bicarbon
ate
Other
treatm
entand
stud
ytreatm
ent
immediatelyafter
diph
enhydram
ine
Bicarbon
ate:2
mEq/kgplus
anequalvolum
eof
norm
alsalinesolu-
tion
systolicBP,M
AP,
cardiacou
tput,Q
RSandtim
eto
death
Survival:
ILE1/12
Bicarbon
ate2/12
No;
nodiffe
rencein
outcom
emeasures
betweengrou
ps
Case
Repo
rts/
Series
Ceccherin
i[36]
(Cats)
Case
series
(N¼4)
Perm
ethrin,d
ose
androuteNR
6.47
Musclefascicula-
tions
andseizures
NR
Variabledo
ses
Variabledo
ses
NA
NR
Dexmedetom
idine,
dose
NR
NR
Survival:
4/4
Yes;seizure-like
activity
respon
ded
Herrin
g[37]
(Dog
s)Case
series
(N¼3)
Naproxen2.2–2.5g
Oraling
estio
n0.45
NR
20%
2mL/kg
0.25
mL/kg/m
infor
30min
NA
NR
NR
NR
Survival:
3/3
Theanimalswere
empiricallytreated
dueto
thehigh
dose
anditis
impo
ssible
toinfer
anyclinical
benefit
over
supp
ortive
care
alon
eJourdan[38]
(Cats)
Case
series
(N¼20)
Ivermectin
4mg/kg
Subcutaneous
5.76–6.21
NR
20%
1.5mL/kg
(N¼16)
andotherILE
bolusesgivenun
tilclinical
resolutio
ncom-plete
0.25
mL/kg/m
infor
30min
(following
thebo
lusin
N¼4
animals)
NA
Early
initiation
NR
NR
Survival:
20/20
Theanimalswere
empiricallytreated
dueto
thehigh
dose
anditis
impo
ssible
toinfer
anyclinical
benefit
over
supp
ortive
care
alon
e (continued)
CLINICAL TOXICOLOGY 921
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

App
endix4.
Continued
Article
(Species)
Mod
elPoison
,doseand
route
LogD
Symptom
sILEused
ILEbo
lusa
ILE
infusion
Stud
yarms
Timingof
rescue,
timefrom
LAterm
ination
Other
treatm
ents
received
bParameter
measured
Outcome
Supp
orteffect
ofILE
Saqib[40]
(Lion)
Case
repo
rtIvermectin
3mg/kg
Oraling
estio
n5.76–6.21
Hypotension
Bradycardia50-60
beats/min
Ataxia,app
arent
hallucinatio
ns,sin-
gleseizure
Coma
Blindn
ess
Bradypnea10–15
breath/m
inDecreasingbo
dytemperature
20%
1stdo
se:1
.5mL/kh
1stdo
se:0
.25mL/
kg/m
infor30
min
2nddo
se:0
.5mL/
kg/m
infor30
min
NA
1stILEdo
seafter
app.
72h
2ndILEdo
seafter
92h
IVfluids
Activated
charcoal
andlatergastric
lavage
Glucose,d
iazepam,
atropine,n
eostig-
mine,ceftriaxone
Mechanical
ventilatio
n
NR
Survival
Yes
Seitz
[41]
(Cat)
Case
repo
rtPerm
ethrin,d
ose
NR
Topical
6.47
Sing
leseizure
20%
1.5mL/kh
0.25
mL/kg/m
infor2h
(total:3
1.5mL/kg)
NA
NR
IVfluids
Metho
carbam
ol,
diazepam
NR
Survival;seizure
ter-
minationpriorto
ILE
persistent
grosslip-
emiaandsuspected
corneallipidosis
Yes
Williams[43]
(Dog
)Case
repo
rtSynthetic
cann
abin-
oidreceptor
agon
ist
NR
Bradycardia60
beats/min
Coma
Perio
dicapnea
Hypotherm
ia32.5
� C
20%
1.5mL/kh
0.5mL/kg/h
for6h
(total:2
mL/kg)
NA
NR
IVfluids
Supp
ortivecare
Mechanical
ventilatio
n
Vitalp
aram
eters
Drugs
measured:
9-TH
C,AM
-2201,
JWH-122
Survival;m
entalsta-
tusimproved
fol-
lowingILE
Unclear
a The
bolusdo
sein
g/kg
andinfusion
dose
ing/kg/h
couldon
lybe
calculated
iflipid
concentrationwas
repo
rted.
bDrugs
used
forgeneralanesthesiaor
euthanasia
areno
tinclud
ed.
BP:B
lood
pressure;C
I:Cardiacindex;EEG:electroenceph
alog
raph
y;ILE:Intravenou
slipid
emulsion
;IV:
Intravenou
s;LA:Localanesthetic;LCT:Lon
gchaintriglycerid
e;MAP
:Meanarterialp
ressure;MCT:M
edium
chaintriglycerid
e;NA:
Not
applicable;N
R:Not
repo
rted;R
CS:R
ando
mized
controlled
stud
ies.
922 S. GOSSELIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7

Appendix 5. Vote results
Life-threatening toxicity Non-life-threatening toxicity
Toxins Cardiac arrestAs first linetherapy
As part of treatmentmodalities
If other therapies fail (inlast resort)
As first linetherapy
As part of treatmentmodalities
If other therapies fail (inlast resort)
Local anestheticsBupivacaine Recommended
(M:7, LQ:7, DI:0.2)Neutral(M:6, DI:0.5)
Suggested(M:7, LQ:6, DI:0.2)
Recommended(M:8, LQ:7, DI:0.2)
Neutral(M:5, DI:0.5)
Neutral(M:5, DI:0.5)
Neutral(M:6, DI:0.5)
All other local anesthetics Neutral(M:6, DI:0.3)
Neutral(M:5, DI:0.4)
Neutral(M:6, DI:0.5)
Suggested(M:7, LQ:6, DI:0.4)
Neutral(M:5, DI:0.7)
Neutral(M:5, DI:1.0)
Neutral(M:6, DI:0.3)
Non-local anaestheticsAntidysrhythmics Class 1 Neutral
(M:5, DI:0.3)Neutral(M:4, DI:0.7)
Neutral(M:5, DI:0)
Neutral(M:6.5, DI:0.5)
Not suggested(M:3, UQ:5, DI:0.7)
Neutral(M:5, DI:0.6)
Neutral(M:5, DI:0.4)
Amitriptyline Neutral(M:6, DI:0.5)
Not suggested(M:2.5, UQ:4.5, DI:0.3)
Neutral(M:5, DI:0.5)
Suggested(M:7, UQ;5, DI:0.4)
Not recommended(M:1, UQ:2, DI:0.1)
Not suggested(M:3, UQ:4, DI:0.5)
Neutral(M:5, DI:0.8)
Other tricyclicantidepressants
Neutral(M:5.5, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:5, DI:0.9)
Neutral(M:6, DI:0.6)
Not suggested(M:1, UQ:4, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.8)
Not suggested(M:3, UQ:5, DI:0.8)
Baclofen Neutral(M:5, DI:0.1)
Neutral(M:5, DI:0.7)
Neutral(M:5, DI:0)
Neutral(M:5, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.7)
Neutral(M:4, DI:0.7)
Neutral(M:5, DI:0.7)
Beta receptor antagonists(lipid-soluble)
Neutral(M:6, DI:0.3)
Neutral(M:4, DI:0.4)
Neutral(M:5, DI:0.3)
Neutral(M:6, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:4, DI:0.7)
Neutral(M:5, DI:0.6)
Beta receptor antagonists(Non lipid-soluble)
Neutral(M:5, DI:0.5)
Not suggested(M:2, UQ:4, DI:0.5)
Neutral(M:4, DI:0.7)
Neutral(M:5, DI:0.3)
Not suggested(M:1, UQ:3.5, DI:0.2)
Not suggested(M:1, UQ:5, DI:0.8)
Neutral(M:5, DI:0.8)
Bupropion Neutral(M:6, DI:0.5)
Not suggested(M:2, UQ:5, DI:0.4)
Neutral(M:5, DI:0.4)
Suggested(M:7, LQ:5, DI:0.7)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:4, DI:0.8)
Neutral(M:5, DI:0.8)
Calcium channel blockersDiltiazem and verapamil
Neutral(M:6, DI:0.5)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:5, DI:0.1)
Neutral(M:6, DI:0.1)
Not suggested(M:1, UQ:4, DI:0.5)
Neutral(M:4, DI:0.7)
Neutral(M:5, DI:0.7)
Calcium channel blockersDihydropyridines
Neutral(M:5, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.5)
Neutral(M:5, DI:0.2)
Neutral(M:6, DI:0.5)
Not suggested(M:1, UQ:4.5, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.8)
Not suggested(M:2, UQ:5, DI:0.8)
Cocaine Neutral(M:5, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.5)
Neutral(M:5, DI:0.7)
Neutral(M:6, DI:0.4)
Not suggested(M:1, UQ: 3.75, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:5, DI:0.8)
Diphenhydramine Neutral(M:5, DI:0.3)
Not suggested(M:1, UQ:4, DI:0.2)
Neutral(M:5, DI:0.4)
Neutral(M:6, DI:0.6)
Not recommended(M:1, UQ:2, DI:0.1)
Not suggested(M:1, UQ:4, DI:0.2)
Not suggested(M:2, UQ:5, DI:0.8)
Other antihistamines N/A N/A N/A N/A N/A N/A N/AIvermectin Neutral
(M:5, DI:0)Neutral(M:4.5, DI:0.7)
Neutral(M:5, DI:0)
Neutral(M:5, DI:0.4)
Not suggested(M:2, UQ;5, DI:0.8)
Neutral(M:5, DI:0.8)
Neutral(M:5, DI:0.7)
Other insecticides Neutral(M:5, DI:0)
Not suggested(M:3, UQ:5, DI:0.8)
Neutral(M:5, DI:0.3)
Neutral(M:5, DI:0.4)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:4, DI:0.7)
Neutral(M:5, DI:0.4)
Lamotrigine Neutral(M:6, DI:0.4)
Not suggested(M:3, UQ: 5, DI:0.8)
Neutral(M:5, DI:0.4)
Neutral(M:6.5, DI:0.4)
Not suggested(M:1.5, UQ: 5, DI:0.5)
Not suggested(M:3, UQ:5, DI:0.8)
Neutral(M:5, DI:0.8)
Malathion Neutral(M:5, DI:0)
Not suggested(M:3, UQ:5, DI:0.7)
Neutral(M:5, DI:0.1)
Neutral(M:5, DI:0.2)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:4, DI:0.6)
Neutral(M:5, DI:0.3)
Other pesticides Neutral(M:5 DI:0.1)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:5, DI:0)
Neutral(M:5, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.5)
Neutral(M:5, DI:0.8)
Neutral(M:5, DI:0.5)
Olanzapine Neutral(M:5, DI:0.3)
Neutral(M:5, DI:0.7)
Neutral(M:5, DI:0.1)
Neutral(M:5, DI:0.4)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:5, DI:0.7)
Neutral(M:5, DI:0.7)
Other antipsychotics Neutral(M:5, DI:0.3)
Not suggested(M:3, UQ:5, DI:0.7)
Neutral(M:5, DI:0)
Neutral(M:5, DI:0.4)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:5, DI:0.7)
Neutral(M:5, DI:0.6)
Selective SerotoninReuptake Inhibitors
Neutral(M:5, DI:0.1)
Neutral(M:4, DI:0.8)
Neutral(M:5, DI:0.1)
Neutral(M:5, DI:0.3)
Not suggested(M:2, UQ:5, DI:0.8)
Neutral(M:5, DI:0.7)
Neutral(M:5, DI:0.6)
M: Median; LQ: Lower quartile; UQ: Upper quartile; DI: Disagreement index; N/A: not applicable.
CLINICAL TOXICOLOGY 923
Dow
nloa
ded
by [
Uni
vers
ity o
f Sy
dney
Lib
rary
] at
17:
45 1
6 A
ugus
t 201
7