Embed Size (px)
Citation preview

GONOCOCCAL VULVOVAGINITIS IN INFANTS ANDCHILDREN: A STUDY OF 240 CASES
BY
CHUNILAL MUKHERJEEFrom the Department of Obstetrics and Gynaecology, the Campbell Hospital Medical School,
Calcutta
(REaxva mR PuBUCATO Auour 25, 1949)
Gonorrhoea in women often produs miorsymptoms. This explains the comparative infre-quency of symptomatic gonorrhoea of the lowergenital tract in out-patient clinics. Gonococcalinfection of infants and children, on the other hand,at once attracts attention. Hence the reason whythe incdence of vulvovaginitis infantum appears tobe comparatively high. Nelson (1932) found theincidence of gonorrhoeal vulvovaginitis to be11-8% and Mukherjee (1940) 11%. In a sernes of2,464 cases in the female, diagnosed by bacterio-logical methods during 1933-46, we came across240 cases of gonorrhoeal vulvovagitis, a frequencyof 9-7%.Not all cases of vulvovaginitis are caused by
gonorrhoea. Foreign bodies, non-specific infectionscaused by unhygienic conditions, threadworms,exanthematous fevers, monilia, and diphtheriaaccount for a fair number. Fessler (1930) foundgonorrhoea in two out of 25 cases, and Clauberg(1930) failed to cultivate the gonococcus from 70children examined for the condition. Ruys (1935)found gonococci in 57 out of 292 children. Duringthe period under review the total number ofvulvovaginitis cases was 438, of which 240 (55%)were diagnosed as gonorrhoeal. This may appearto be high and is probably so, for most patients withsimple catarrhal vaginitis do not report to hospitalsfor invesfigation and treatment. It may be ofinterest to compare the relative frequency ofgonorrhoea with the other aetiological conditionscausing vulvovaginitis in children (Table 1).The incidence of gonococcal infection in any
study of vulvovaginitis is dependent on the meamemployed for the detection of gonococci. Theunreliability of smear examination alone has beenshown by several observers (Clauberg, 1930;Ruys, 1935). This is because of the presence ofGram-negative cocci, which are often arranged inpairs, in the norm valgina. Grenhill (1945)suggested that to identify gonococci one must
TABLE 1
COMPARISON oF AETmLoGIcAL CoNDnwrn CAUSINGVULVOVAGPNTM
Nature of Infection lNo. ofCases Perentage
Foreign bodies .. .. 26 5*9N a infti 1 '4;Ii .
discover more than ten typical organisms intra-cellularly in the same slide, and two or more withinthe same celL By a similar method it has beenpossible to elimnhate no fewer than 31 cases in thepresent series. Subsequently culture and theprogress of the patient demonstrated the usefulnessof this simple suggestion. There is another difficultyin chronic or inadequately treated cases. In thesethe vaginal exudate is scanty, and leucocytes arefewer and more disintegrated. In these cases, evenif Gram-negative diplococci are found in the smearthey are frequently exaellular. A negative reportin these cases does not completely rule out thepossibility of a true gonococcal infection.
Cultural results are more reliable, provided theexudate is fresh and inoculated imeatel.Clauberg (1930) was one of the earlier observers toemphasize the value of routine culture. Mascall(1933) also found a higher incidence of positive resultson cultural examination. Cohn, Steer, and Adler(1941) showed from the results of 1,070 examinationsthat cultures were positive in 98-9% of cases,whereas positive results on smear examination aloneobtained in 67 1%. These authors value culturalmethods not only in diagnosis but also in follow-up treatment. In our series culture was not possible
262
Protected by copyright.
on February 29, 2020 by guest.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.25.123.262 on 1 Septem
ber 1950. Dow
nloaded from
GONOCOCCAL VULVOVAGINITIS
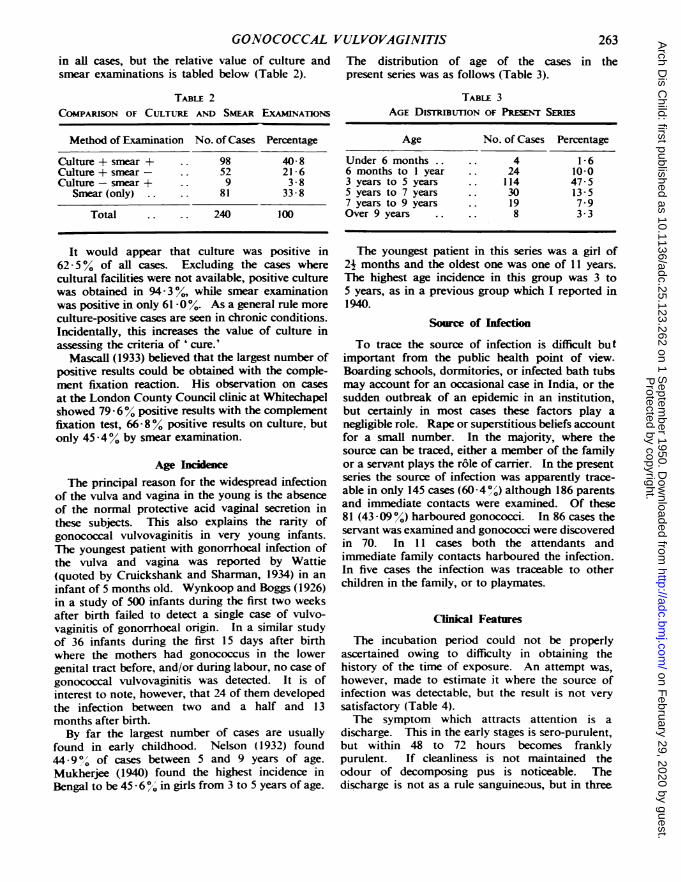
in all cases, but the relative value of culture and The distribution of age of the cases in thesmear examinations is tabled below (Table 2). present series was as follows (Table 3).
TABLE 2COMPARISON OF CULTURE AND SMEAR EXAMINATiONS
Method of Examination No. of Cases Percentage
Culture + smear + .. 98 40- 8Culture + smear- .. 52 21-6Culture-smear + .. 9 3 8
Smear(only) .. .. 81 33- 8
Total .. 240 100
It would appear that culture was positive in62 5% of all cases. Excluding the cases wherecultural facilities were not available, positive culturewas obtained in 94- 3o/, while smear examinationwas positive in only 61-0%. As a general rule moreculture-positive cases are seen in chronic conditions.Incidentally, this increases the value of culture inassessing the criteria of 'cure.'
Mascall (1933) believed that the largest number ofpositive results could be obtained with the comple-ment fixation reaction. His observation on casesat the London County Council clinic at Whitechapelshowed 79 6% positive results with the complementfixation test, 66 8% positive results on culture. butonly 45-4% by smear examination.
Age IncdenceThe principal reason for the widespread infection
of the vulva and vagina in the young is the absenceof the normal protective acid vaginal secretion inthese subjects. This also explains the rarity ofgonococcal vulvovaginitis in very young infants.The youngest patient with gonorrhoeal infection ofthe vulva and vagina was reported by Wattie(quoted by Cruickshank and Sharman, 1934) in aninfant of 5 months old. Wynkoop and Boggs (1926)in a study of 500 infants during the first two weeksafter birth failed to detect a single case of vulvo-vaginitis of gonorrhoeal origin. In a similar studyof 36 infants during the first 15 days after birthwhere the mothers had gonococcus in the lowergenital tract before, and/or during labour, no case ofgonococcal vulvovaginitis was detected. It is ofinterest to note, however, that 24 of them developedthe infection between two and a half and 13months after birth.By far the largest number of cases are usually
found in early childhood. Nelson ( 1932) found44 -9o of cases between 5 and 9 years of age.Mukherjee (1940) found the highest incidence inBengal to be 45 - 6% in girls from 3 to 5 years of age.
TABLE 3AGE DISmIBUTION OF PREENT SERIES
Age No. of Cases Percentage
Under 6 months . . 4 i-66 months to I year 24 10-03 years to 5 years 114 47-55 years to 7 years .. 30 13-57 years to 9 years .. 19 7-9Over 9 years .. . 8 3-3
The youngest patient in this series was a girl of2j months and the oldest one was one of 11 years.The highest age incidence in this group was 3 to5 years, as in a previous group which I reported in1940.
Source of InfectioTo trace the source of infection is difficult but
important from the public health point of view.Boarding schools, dormitories, or infected bath tubsmay account for an occasional case in India, or thesudden outbreak of an epidemic in an institution,but certainly in most cases these factors play anegligible role. Rape or superstitious beliefs accountfor a small number. In the majority, where thesource can be traced, either a member of the familyor a servant plays the r6le of carrier. In the presentseries the source of infection was apparently trace-able in only 145 cases (60 -4 ,) although 186 parentsand immediate contacts were examined. Of these81 (43 -09%) harboured gonococci. In 86 cases theservant was examined and gonococci were discoveredin 70. In 11 cases both the attendants andimnediate family contacts harboured the infection.In five cases the infection was traceable to otherchildren in the family, or to playmates.
Clinical Features
The incubation period could not be properlyascertained owing to difficulty in obtaining thehistory of the time of exposure. An attempt was,however, made to estimate it where the source ofinfection was detectable, but the result is not verysatisfactory (Table 4).The symptom which attracts attention is a
discharge. This in the early stages is sero-purulent,but within 48 to 72 hours becomes franklypurulent. If cleanliness is not maintained theodour of decomposing pus is noticeable. Thedischarge is not as a rule sanguineous, but in three
263P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

ARCHIVES OF DISEASE IN CHILDHOODTABLE 4
ANALYSIS OF INCUBATION TiMES
Incubation Period No. of Cases Percentage
Less than 24 hours 10 12 825-48 hours .. .. 22 28 249-72 hours .. .. 28 35 973-96 hours .. .. 18 23-1
hyperacute cases a sanguineous discharge wasnoticed. Incidentally it may be mentioned that a sero-sanguineous or sanguino-purulent vaginal dischargein infants has been found in all cases of foreign bodyvaginitis. The discharge of vulvovaginitis is of aremarkably irritating nature and in a few days (lessthan four days in 86% cases) signs of irritation ofthe vulva, groin, perineum, and peri-anal regionsappear.
Dysuria was present in 194 cases (80- 80).Belladonna usually relieves this dysuria to a greatextent. A considerable part of the complaint isprobably due to urinary tract infection and spasm.The first symptom observed in the patient was:
(1) Discharge, 187 cases (77- 9%.); (2) vulvalirritation, 47 cases (19 6%); (3) dysuria, 6 cases(2 5 %).
Examination usually shows severe inflammationof the vulva. The labia are swollen, tender, andexcoriated. The vestibule is bathed in pus, and isangry and congested. The urethral orifice is swollenand pouting, but infection of Skene's glands wasnever noticed, nor was Bartholin's gland affected.In one case the infection was so severe, and lack ofcleanliness so pronounced, that noma of the vulvahad developed before relief was sought. The extentof ulceration of the vulva is usually proportional tothe infection. In such fulminating cases the natureof the basic infection is often missed, especially onculture, as secondary organisms grow exuberantly.This happened in no less than 23 (9- 60//) of ourcases. In such a predicament microscopicalexamination of a carefully prepared slide exposesthe possibility of the nature of the underlyinginfection. It must be said, however, that as thesecondary infection comes under control, culturinggonococcus from the vulvovaginal secretion becomesmore easy.
Inspection of the vagina when the infection isacute is not only almost impossible but is alsodangerous, for an acute flaring up of the infectionis the usual consequence. Nevertheless, afterwashing the vulva under a gentle stream of normalsaline, the degree of severity of the infection can bejudged from the amount and nature of the vaginaldischarge. Gentle milking of the vagina with the
little finger introduced into the rectum is all that isnecessary. When the active infection is undercontrol the state of the vaginal mucous membranecan be inspected with a Kelly speculum or an electriccystoscope. A small dose of luminal about oneand a half hours before instrumentation helps toallay nervousness. The usual finding is a congestedswollen mucous membrane bathed in a purulentexudate. In 79 cases (32 9 o) superficial ulcerationswere noticed. Evidence of infection is as a rulemore marked in the lower half of the vagina thanin the upper and on the posterior wall than on theanterior. The cervix often shares the vaginalinfection (300').The spread of infection to the upper genital
passages is rare, owing to the protective barrier ofthe cervix. Nevertheless exploration of the pelvisduring rectal examination is sometimes rewarded.In our series only four children developed evidenceof peritoneal involvement (1 - 68o%). In a similarstudy by Schauffler (1940) of 266 infants andchildren with frank vaginal infections nine presentedsymptoms of pelvic involvement. Lees (1928) givesthe frequency as no less than 5 5 %.
In our series rectal symptoms were present in14 cases or 5- 80g. Rectal infection forms a hiddenfocus from which re-infection and relapse arefrequent. Fraser (1925), Williams (1933), andMartin (1935) were some of the earlier observers todirect attention to this possibility. Fraser foundrectal infection in 59 out of his 63 cases. Ruys(1935) observed it in all cases in his series. In anearlier report (1940) 1 found rectal infection in 82o/,.Material from the rectum was examined, by smearand culture, in 170 cases (70.8%) of this series.Culture was positive in 168 cases (98-8%); smearexamination was positive in 124 cases (72- 9I).
Collection of Material for DiagnosisIt is a mistake to collect the material from the
vulva because extraneous organisms are so abundantin this region. The following method has beenfound useful.
Method. The vulva is washed under a gentle streamof sterile warm normal saline. A narrow, but strong glasspipette is then introduced into the vagina and a drop ofexudate is collected from this region. Sometimes thepus is too thick for the calibre of the pipette. In thesecases about 4 to 1 ml. of sterile saline may be introducedbefore the material is collected. Inoculation in theculture medium on to hydrocele or ascitic fluid agar inpetri plates is made imnediately. After inoculationa smear preparation may be made with the remainderof the exudate and stained by Gram's method.
Examination of the rectal specimen formed a routine,except for the first 70 cases studied. The material was
264P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

GONOCOCCAL VULVOVAGINITIS
collected with a strong wire loop from half an inchinside the anus after holding the child in an exaggeratedlithotomy position and stretching the anal skin. Inocula-tion was done imdiately. For a rectal smear thedischarge collected on the loop may have to be mixedwith a drop of sterile saline on a slide.
CompricatioaComplications are uncommon in gonococcal
vulvovaginitis. Contrary to the usual expectationophthalmia develops only rarely. I have found(1940) the incidence to vary from I to 5%. In thepresent serie gonococcal ophthalmia developed in18 cases (7 5%). It is, however, interesting to notethat whereas in 14 cases the ocular infection followedthe vulvovaginal lesion, in two the infection of theeye was primary. In the rmaining two cases theparents declared the infection to be aboutsynchronous. It is also interesting to note that inall these instances the mother was a carrier ofinfection.
Arthritis was also found to be uncommon. Thejoint most commonly affected was the knee. Theonset is sudden and not infrequently it is confusedwith osteomyelitis of the lower end of the femur.The joint is swollen and a cutaneous flush may bepresent; pyrexia varies between 100-6 and 1030 F.The tenderness is, however, limited to the joint, thebone ends being free. The lesion is of the mono-articular type. Williams (1926) considers thiscomplication to be very frequent. In our series,however, it was encountered in only seven cases(2- 9%). The knee was the seat of lesion in all,though in two instances the ankle was subsequentlyaffected. Although the joint fluid was examined onnine occasions, gonococci were cultured only once.In no case did ankylosis or limitation of movementresult.
King, Mascall, and Price (1936) drew attentionto associated infection with trichomonas and statedthat it interfered with the demonstration ofgonococci. I can corroborate this statement. Inthe present series no less than 36 (15%) patientsharboured trichomonas, besides eight, in whichinfection was suspected but could not be confirmeduntil about three weeks after the first observation,a total incidence of 17 -5%. It has now been ourpractice to examine a hanging drop preparation ofthe vaginal discharge (diluted with saline) on threesuccessive days before associated trichomonasinfection is ruled out. In this connexion the casereported by Karnaky (1936) is interesting. Tricho-monas infection makes gonococcal infection moreresistant to treatment, besides causing the irritantvaginal discharge to persist even after the disappear-ance of gonococci. If the trichomonas infection is
missed initially it is usually detected later whenleucorrhoea becomes persistent, but early detectionshortens the course of treatment considerably. It hasnot been possible to detect the source ofthis obstinatesecondary invader. The vaginal mucous membraneof infants is very susceptible to trichomonas infection.The mutation of Trichomonas intestinalis intoT. vaginalis in vivo has been suspected but has notbeen actively proved. In 16 patients of the seriesintestinal trichomonas were detected in the faeces,but almost all these patients belonged to a class ofsociety where personal hygiene was minimal. Of86 'better class ' patients only one showed thissecondary infection.
Associated luetic infection cannot strictly beregarded as a complication, but it is imiportant.Out of 198 cases in this series where a routineWassermann test was done, 46 (23-2%) werepositive. This cannot be accepted as it standsbecause of the possibility of inherited syphilis. If37 cases, where the parents also had positive bloodtests, are excluded, the incidence of associatedsyphilitic infection appears to be only 4-5% (ninecases). It may be pointed out that in eight out ofthese nine cases a history of rape was either presentor suspected It appears that the presence of anassociated syphilitic infection, if inherited syphilisis excluded, indicates a criminal assault.
TreatmentFor comparative study the results obtained in all
cases are presented in relation to the form oftreatment.Orhodox Local Treatment. The total number of
patients treated was 20. The treatment consisted ofhip bath, vaginal irrigation, and instillation of silvernitrate or mercurochrome solutions.
Straightforward uneventful recovery was anexception; relapses were frequent, the course oftherapy prolonged, and taxing to the patience ofthe parents and the medical attendant. The averageduration of treatment was 12 weeks, while theminimum was 10 weeks and the maximum 26. If itis considered that al patients with relapse cameback for treatment (an expectation which isextremely improbable) its incidence appears to be20-0% (four cases). It was also noted that therelapses were more refractory to local treatmentalone than the primary infection. The results oflocal therapy may. therefore, be consideredunsatisfactory.Sex Hormone Therapy. The total number of cases
treated with sex hormones was 102. In 70 of theseoestrogen therapy was combined with local anti-septic treatment. In the remaining 32 oestrogens
20
265P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

ARCHIVES OF DISEASE IN CHILDHOODalone were employed locally. Lewis (1933) observedthat female sex hormones in children producedproliferation of vaginal epithelium and the clearingup of the vaginal infection. But the effect ofoestrogens is not confined to the vagina. Wither-spoon (1935) suggested that prolonged use ofoestrogens might inhibit the pituitary and bringabout secondary atrophic changes in the ovaries.It has, however, not been conclusively shown thatsuch changes affect infants and children equally.Of the 102 patients of this series treated withoestrogens 31 have been followed up to the age ofpuberty and thereafter. The age of the menarchein this group may be tabulated here with advantage(Table 5).
TABLE 5
AGE OF MENARCHE OF CAsEs TREATS wrrH OEsTRocEm
AgeofMenarche No. of Cases Percentage Normal(years) Controls
11-12 8 25-9 3812-13 12 38-4 2913-14 8 25-9 2114-15 3 9.7 915-16 - - 3
Total 31 99 9 100
Table 5 shows that there is a tendency for a
delayed menarche in the group of children treatedwith oestrogenic hormones in infancy, but it mustbe admitted that the number of cases is so small thatthe difference may be more apparent than real.In any case the advantages of oestrogen therapy invulvovaginitis far outweigh the supposed fear ofpituitary inhibition and ovarian atrophy. Nodifference in results has been observed between oraland parenteral treatments if the dosage has beenadequate. Often both these means of administrationhave been combined.NATURAL OEsTRoGENs. The preparations
employed were 'progynon B oleosum," ' ovocyclinP,' and 'menformon.' The number of cases sotreated was 48 (64.4%, i.e. 20.0% of all cases).The dose employed was 1 mg. (10,000 I.U.). Exceptin the case of very small infants (up to 3 years) thiswas supplemented with a daily dose of 0-3 mg.
(3,000 I.U.) of oestrogen dragees orally in divideddoses. The course of treatment was checked byfrequent vaginal smear and culture and estimationof the vaginal acidity. Improvement was invariablyattended with a fall in the vaginal pH, often to theextent of 3 - 5 to 4. This substantiates the observa-tion made by Karnaky (1936) who recorded recovery
in every case in a series of 140 when the pH wasbrought down to 3 to 3-5. He used dextrose-acidtablets which were inserted into the vagina.Oestrogens produce a similar effect in an indirectmanner.SYNT1HIC OESrROGENS. The preparation used
was diethyl-stilboestrol. The number of casestreated in this group was 22 (35- 6%, i.e. 9 I0 ofall cases). All patients had oral medication in dosesof 1 mg. daily. Infants under 2 years of age weregiven 0- 5 mg. It may be mentioned here thatexcept in two cases no toxic symptoms were noted.These were manifested as vomiting and irritabilitywhich were relieved with small doses of calcium andsodium bicarbonate.
In both these groups the local treatment con-sisted of cleaning the vulva and vagina with 0 750Olactic acid and instillation of 200 mercurochrome inthe vagina.
It was observed that with oestrogens (bothsynthetic and natural) considerable improvementoccurred in about two and a half to three weeks,though for complete recovery the treatment had tobe continued forfive to six weeks, or longer. It mustbe mentioned, however, that examination forgonococci became negative on smear 10-14 daysearlier than on culture. If reliance is placed onsmear examination alone, the patient may stillremain a carrier and as such, a source of danger.Even after the vulva and vagina were free from
infection rectal infection persisted, and acted as afocus of reinfection for the vagina, with subsequentrelapse of the condition. In fact the incidence ofrelapses after oestrogen therapy was 15- 70 . Itwas, therefore, considered necessary to institutetreatment for the rectal condition while oestrogenswere being administered for the vulvovaginal lesion,for in the absence of rectal infection relapse ofvulvovaginitis never occurred after oestrogen treat-ment. The simplest remedy for the rectal infectionwas found to be 5% ' argyrol ' suppositories. Oneof these is inserted into the rectum at bedtime andretained.The change in vaginal acidity was noted as early
as eight days after the beginning of treatment.Irrespective of what the initial pH value was (thehighest recorded was 9 8), by this time a distinctthough slight acid reaction was noted. A steadyincrease in acidity continued until about the end ofthe third week when a pH of 4 5 to 4 8 was theusual finding. By about the beginning of the fifthweek the peak was reached and the level maintainedfor about a week after the treatment was over.The reaction returned near to neutrality by aboutthe seventeenth day after the suspension of treat-ment. The highest acidity which was obtained in
266P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

GONOCOCCAL VULVOVAGINITIS
the present series of cases was pH 3 -2. In spite offull courses of oestrogens the pH did not fall below5 -3 in four cases. In these patients residualinfection persisted in the vagina though the rectalinfection was under control with ' argyrolsuppositories. Lactic acid jelly (1 %) was instilledinto the vagina three times a day and completerecovery followed.
Comparative refractoriness of the vaginal aciditywas noted in 17 patients in none of whom did thepHfall below 6-4 after three weeks' treatment. Heavyinfection with Trichomonas vaginalis was found in allof them. When this infection was controlled thenormal curve of the vaginal acidity was regained.The change in the vaginal smear was found to be
more gradual than that of the reaction. Polymor-phonuclear cells persisted until the disappearanceof the infection, although partially keratinizedepithelial cells appeared in the smear within twoweeks of the beginning of treatment. A real' oestrus smear ' was not obtained till the vaginawas free from infection.The average duration of treatment in this series
was 6-0 weeks (Table 6).
TABLE 6AVERAGE DURATION OF TREATMENT
No. of Weeks No. of Cases Percentage
4 17 24-35 18 25 -76 12 17-17 9 12-88 2 2-99 4 5-710 4 5- 7
11-12 4 5- 7
In eight (11 4o) cases of this series, althoughmarked relief of symptoms was obtained, the vaginalsecretion was not free from gonococci and the pHdid not fall below 6 -4. Cultures showed infectionwith staphylococci, which produce alkaline exudates.
These patients were subsequently treated withsulphonamides or/and penicillin and cured.
Tlhe criterion of cure was three consecutivenegative reports on culture and smear examination,the last one after a provocative painting of thevagina with 1% silver nitrate solution. In 13 cases
recurrence was noted within three to four weeks ofrecovery. The possibility of reinfection could bedefinitely eliminated in 11 patients. The incidenceof relapse in this series may therefore be takenas 15 7% and the corrected recovery rate as 72-9 %.An inquiry was made into the difference in results
obtained with natural and synthetic oestrogens(Table 7). It appeared that the synthetic productwas slightly superior to oestradiol derivatives in itseffects, besides being cheaper and more easilyadministered. Its toxic effects were not found tobe marked in infants, and when present they were
easily controlled.
Oestrogen Vaginal Suppositories. Thirty-twocases were treated with oestrogen vaginal supposi-tories. The preparations employed were ' kolpon'(organon) and stilboestrol jelly (10 mg. per g.tragacanth-glycerine jelly). Preliminary cleansingof the vulva and vagina with 0 750% lactic acidlotion was employed in all cases. No antisepticswere used, but the treatment of the rectal infectionwas not ormitted. Results were found to comparefavourably with oral and parenteral medication.The average course of treatment necessary was5 -0 we-ks (Table 8). More than half the totalnumber of cases needed only three to four weekstreatment for complete recovery. By the tenth dayconsiderable subjective improvement was oftennoted, while towards the beginning of the thirdweek the vaginal discharge was scanty and sero-
mucoid in nature in 29 cases (90.6%) of the series.A pH of 4-6 to 4-0 was usual about the middle ofthe third week. As with parenteral oestrogentherapy the initial change from alkaline to acidreaction took place in about eight to ten days, butonce the acidity was established the fall in pH was
TABLE 7
COMPARISON OF REsULTS OBTAINED FOR NATURAL AND SYmTHnC OESTROGENS
Course of TreatmentNo. ofCases Maximum Minimum Average Cure Relapse Failure
Natural oestrogens 48 12 5 -5 6-6 38 8 6(70 80o) (16 60o) (12'50o)
Synthetic oestrogens . 22 10-5 4-0 4- 7 17 3 2(77.3 0) (13 60o) (9.00o)
267P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

ARCHIVES OF DISEASE IN CHILDHOODTABLE 8
DURATION OF TREATmNTr wrrH OESTROGEN VAGiNALSuPPosITORIES
No. of Weeks No. of Cases Percentage
3 8 25 04 9 28-15 5 15 66 3 9-47 2 6-28 2 6-29 2 6-210 1 3-1
more or less steady and rapid. The rate of improve-ment was proportionate to the rate of attainment ofthis acid peak.The treatment was without effect in three cases
or 9*4',' The maximum vaginal acidity which wasobtained in these cases was pH 5 -2. Local treat-ment was continued for 12 weeks after whichparenteral natural oestrogen therapy was employedfor a further period of six weeks without anyimpression on the disease. Treatment withsulphonamides and penicillin subsequently curedthese patients.Permanent recovery was obtained in 26 cases or
81 i /o. This is undoubtedly much less than the980% cure reported by Te Linde (1938). Relapseoccurred in three cases or 9 4%. The intervalbetween apparent recovery and relapse was twoto three weeks, which is shorter than after generaloestrogen treatment. In these cases also thepersistence of rectal infection appeared to be thecause of recurrence of symptoms.UNToWARD SYMPTOMS OF OESrROGEN THERAPY.
Considering the dosage of oestrogens the incidenceof untoward symptoms was negligible. They werenot serious enough to call for withdrawal of thedrug. In our series of 102 cases treated withoestrogens enlargement of the breasts was notedin 11 (10 -8 %). Of these, in eight cases the mammarychanges were slight and just noticeable. In twocases where oestrogen injections were continued forover ten weeks the appearance of the mammaryglands simulated that which is normally noticeableat or about puberty. In one case there was secre-tion, and pigmentary change was marked, thoughthe hypertrophy was only moderate. Oestrogenicresponse of the breasts was more marked in thegroup treated with oral or parenteral oestrogens.Of the 72 cases subjected to general oestrogentherapy the breast changes were seen in nine or12-5%, whereas these changes were noticeable inonly two cases or 6.20% among the locally treatedgroup. It was also observed that mammary
hyperplasia was more likely to develop in thehigher age group children than in infants. Eightout of the 11 cases (72 -8 %/) with noticeable changesin the breast were above the age of 8 years, and twowere in the 6 to 7-years-old group. Only one casebelow the age of 3 years showed this change and itwas only slight. The two cases where the changewas marked were both over 9 years of age. In allcases, however, retrogressive changes set in withinten days of the cessation of the treatment except inthe two cases where the hypertrophy was excessive,and persisted to some extent until puberty. Rever-sion to normal occurred in less than four weeks.
Vaginal bleeding is another untoward sequel.Though it is of no grave consequence it often causesanxiety. Schauffier (1947) noticed it in only twocases in his series. In our series of 102 cases vaginalbleeding occurred in only seven (6-9%). With theexception of one, where the bleeding appearedduring the course of treatment, in all the haemor-rhage was of the nature of oestrogen withdrawalbleeding and started six to eight days after thecompletion of treatment. In none was thehaemorrhage excessive and it stopped spontaneouslyin four to seven days' time. - In one case (aged9 years 7 months) the bleeding was accompaniedby cramp-like pain in the lower abdomen. Allcases of vaginal bleeding belonged to the group ofcases treated with parenteral and oral oestrogens.Here also, as in the preceding instance, susceptibilityto vaginal bleeding appeared to increase withincrease in age. Only one out of the seven caseswas below the age of 7 years, four cases were over9 years of age, and two between 8 and 9 years.There appeared to be some relation between vaginalbleeding and mammary congestion and hypertrophy,for all the seven cases in which vaginal bleedingoccurred showed breast changes.A sparse growth of fine pubic and axillary hair
was noticed in four cases (3 9 oo), in all of which thetreatment was continued for ten weeks or more.Two of these patients were over 9 years old, onejust over 7, and another just under 5 years of age.In all cases spontaneous retrogression occurred inless than six weeks.
Suomamide TherapyThe advent of sulphonamides induced high hopes
of success in the treatment of vulvovaginitis. Thisoptimism has not been wholly rewarded. Hoffman,Schneider, Blatt, and Herrold (1938) reported curein 75% of cases after one of two courses ofsulphanilamide. Brown (1939) obtained a similarrecovery rate, although she succeeded in curing81-4% with a four-day course of sulphapyridine.
268P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

GONOCOCCAL VULVOVAGINITISLewis (1940) obtained a 900% recovery rate with thisdrug. Cohn, Steer, and Adler (1941) succeeded inobtaining negative cultures in all cases with sulpha-pyridine. Adair and Hac (1942) made a compara-tive study of the value of the different sulphonamideproducts and found that the rate of cure withsulphanilamide was 76%~with sulphapyridine 86%,with sulphathiazole 93%0, and with sulphadiazine96 %/.
In our series of 240 cases sulphonamides wereadministered to 83 patients. Sulphanilamide andsulphapyridine were used in only 10 and 13 casesrespectively. Toxic symptoms appeared frequentlywhen these drugs were used. These 23 cases havenot been included in the series under review. Ofthe 83 patients considered here, 46 were treated withsulphathiazole and 37 with sulphadiazine. Nospecial local treatment was given except cleansingand hip bath.The dosage employed was 32 mg. per lb. body
weight. With sulphadiazine in the case of feeblechildren a slightly smaller dose (24 mg. per lb. bodyweight) was employed. The initial dose was doublethe calculated dose. The maintenance dose wasrepeated every four hours. In the case of childrenweighing more than 15 to 16 lb. the dosage was soregulated that the total intake did not exceed 2 g.a day, and 16 g. during the whole course. Thiswas found to be the maximum safe limit.
Within 48 hours of the administration of sulpha-thiazole or sulphadiazine subjective improvementwas noted. The majority of cases showed a negativesmear and culture in less than 96 hours, but it wasfound unwise to withhold the drug at the firstnegative reading, for in a number of such casesrecurrence occurred. The minimum course oftreatment compatible with recovery was found tobe one of four days, and the maximum eight days,while the average duration of treatment was 5 9days. The distribution was as follows:
4 days ..
5 days ..
6 days ..
7 days ..
8 days ..
11 cases (13-2%)29 cases (34 9%)32 cases (38%)7 cases (8 4%)4 cases (4-8%)
Lewis (1940) believed that if the patient didnot improve after five days' treatment with sulpha-thiazole, sulphadiazine should be substituted afteran interval of two to three weeks. In our experience,however, this observation was not substantiated,as the subsequent analysis of the results will show.Sulphathiazole-resistant cases also appeared to beresistant to sulphadiazine, but penicillin providedthe remedy on these occasions. A change fromsulphonamides even to oestrogens was found more
satisfactory than merely changing the type ofsulphonamide.Of the 83 cases presented in this series permanent
recovery was obtained in 76 cases (915%). Pro-gressive diminution of the coccal flora of the vaginaand disappearance of the polymorphonuclear cellsand macrophages were the characteristic features.Diphtheroids and certain strains of E. coli,however, persisted or appeared simultaneously withthe disappearance of the pathogenic cocci. Thechange was observed on the second day in 69 outof 76 cases cured. In the relaining seven casesthis change was noticeable between the third andfourth days. Once this change appeared theprogress was steady and rapid. With completerecovery the vaginal secretion was found to consistof a few polymorphs and lymphocytes, immaturevaginal epithelial cells, diphtheroids, E. coli, andoccasionally enterococci and faecal streptococci.The reaction of the vaginal secretion was also
tested, but the only change which was noted was adiminution in the degree of alkalinity. The lowestpH recorded during sulphonamide treatment was6 8. All the cured cases settled down to a pH of7-2 to 7-5.
Failures were much less common than afteroestrogen treatment, and the failure rate was 2 5 %.In these two cases the symptoms were markedlyameliorated, and the vaginal discharge becamescanty and white. Culture was positive in both.Obviously, an outcome like this is more dangerousthan a frank failure, for the symptomatic relief maybe mistaken for a cure while the child still remainsa carrier and a source of potential danger.
In five cases (6%° the recovery was only apparent,for the condition relapsed. The interval betweenthe apparent recovery and recurrence was eight daysin one case, 12 to 13 days in three cases, and 17 daysin the remaining one. In three out of these fivecases the material collected from the rectum wasnegative for gonococcus on culture at the time ofrelapse.
All these seven cases where sulphonamides failedto establish a cure were put on a second course ofthe drug after an interval of three weeks (Table 9).With a second course of treatment in the failure
or relapse cases only one out of seven was cured.The other six were subsequently treated withoestrogens and penicillin with recovery in all cases.
Penicilin TherapyPenicillin has been given ample trial in the
treatment of gonorrhoea and found uniformlysatisfactory. For this reason it was employed inthe treatment of 35 cases of vulvovaginitis.
269P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

ARCHIVES OF DISEASE IN CHILDHOODTABLE 9
ANALYS OF FAED SULPHONAMDE CAsES
First Course Second Course Resultof No. of of
Sulphonamide Cases Sulphonamide Recovery Failure
Suiphathiazole 2 Sulphadiazine 2Sulphathiazole 2 Sulphapyridine 1 1Sulphadiazine I Sulphathiazole 1Sulphadiazine 2 Sulphapyridi - 2
In the earlier part- of the investigation the drugwas given by three-hourly intramuscular injectionsbut the treatment was found to be painful. In thelast 20 cases penicillin was administered locally inthe form of a jelly, the drug being introduced intothe upper part of the vagina every three hours bymeans of an applicator of the type supplied withcontraceptive jellies.The dosage employed was the same for both
intramuscular and local treatment, 10,000 Oxfordunits being given every three hours, one nocturnaldose being omitted. The vaginal jeliy was made byadding mucilag of tragacanth and glycerine toconcentrated penicillin solution in the proportionof 4:1 in order to make a concentration of 10,000units per ml. The solution was loaded in a syringeand kept in a refrigerator. The applicator wassterilized each time after use and kept separately.With sensible and educated parents the instillationof this penicillin jelly into the vagina every threehours has never caused any difficulty.
In general, the results obtained were verygratifying. The course of treatment necessary wasshort, the average being 4-1 days. In two casespositive culture persisted in spite of eight days'continuous treatment and a total dosage of over560,000 units. These have been regarded asfailures.The course taken by the disease treated with
penicillin follows closely that under sulphonamiletreatment. Enterococci and anaerobic steptococcipersisted in all cases even after complete disappear-ance of gonococci. In all instances of recovery,the pH of the vagina settled down to 7 2 ± 0 2.Rectal infection appeared to be slightly morepersistent than that in the vagina, as in none of thecases studied did the rectum become negative onculture at the same time as the vaginal culture, andrequired 24 to 36 hours' further treatment. Thisapplied equally to local and parenteral penicillin. Inlocal penicillin therapy the rectum was also treated inthe same manner as the vagina, i.e. by insillation ofpenicilln jelly with a separate applicator iside therectum, about i to 1 inch above the anal margin.
The immediate recovery rate was 94 3%,O i.e. 33out of 35 cases. This, however, did not representthe permanent recovery rate, for in two cases mildrelapse was noticed. Reappearance of symptomsoccurred in both cases within two weeks of thesuspension of treatment. The clinical manifesta-tions ofrelapse in both ofthem were of a mild nature.These patients were put on further courses ofpenicillin, but even with three full courses recoverydid not occur. Each repeated course of penicillinbrought about a temporary relief of symptoms, butneither smear nor culture was negative. Thesewere probably examples of penicillin-resistantgonorrhoea. Taking into account these cases thecorrected recovery rate was 88 -6 %.
Treatment of Relpe and Faihle Cases
In our series of 240 cases, 42 (17 -5° fell intothis unfortunate category. It will appear that theincidence of such cases was low in the penicillinand sulphonamide treated groups, whereas theorthodox and oestrogen treatment showed higherfigures. It was found that repetition of the sameline of treatment did not produce satisfactoryresults. The general principles which were followedare: (1) Oestrogen-resistant cases were put on acourse of sulphonamides after a period of rest fortwo weeks, during which period nothing more thangeneral cleansing was done. (2) Sulphonamide-resistant cases were put on penicillin and vice versaafter a similar period of rest for two weeks. (3) Assoon as the infection appeared to be coming undercontrol in either group of cases, oestrogens wereadministered with a view to increasing the acidityand the local resistance of the vagina. This lastmeasure was found to be immensely helpful as theresults will show.
It will appear that by combined treatment inwhich oestrogens played a not negligible role, atotal salvage of 41 out of 42 cases was obtained anda recovery rate of 98 6%. It will also appear thatwithout combined oestrogen treatment there wasgenerally a greater tendency to relapse.
270P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

GONOCOCCAL VULVOVAGINITISTABLE 10
ANALYSIS OF DRUG RESISTANT CASES
Nature of Drug No. ofResistance No. of Cases*, Nature of Drug Employed Cases Cure Relapse Failure
Oestrogen 31 (30 40o) Sulphonamide 11 5 4 2Sulphonamide and oestrogen 20 19 - I
Sulphonamide 14 (15 S°o) Penicillin and oestrogen 5 3 1 1
Penicillin 6 (14 60o) Sulphonamide and oestrogen 6 5 1 -
* This number totals more than 42, as failures in one group are included in the next.
Sueent Fate of Chidren with VulvovaginitisOestrogens, penicillin, or sulphonamides fre-
quently cure the vulvovaginal infection, but thequestion is: ' Will there be any relapse or recurrence
after puberty, and will the disease in any wayinterfere with the future process of conception ? '
This is an important sociological problem, so asmany cases as possible were followed up throughpuberty and early married life.
It was found that 54 out of 78 traceable patientshad attained puberty and menarche. Of these,23 were married for a period of one to five years.Eighteen among the married group conceived withintwo to three years of marriage. Of the remainingfive who did not conceive, four were married for
less than two years and one was seeking treatmentin a sterility clinic. It may be of int-rest to pointout that one of those who conceived normally haddeveloped signs of upper genital tract infectionduring the attack of vulvovaginitis. Though nopositive conclusion can be arrived at, one maypresume that the effects of vulvovaginitis onsubsequent reproductive functions are not ofconsiderable importance. Enquiry was made alsoabout the menstrual history, but nothing outstandingwas discovered, which could be due to the infectionin childhood. Investigation, however, revealed that71 among 78 cases traced showed considerable sex
consciousness dating from soon after the disease.Records showed that 60 out of these 71 cases had
undergone energetic local treatment. This is a mildwarning against the indiscriminate use of intensivelocal treatment in vulvovaginitis of young children.
SummaryGonorrhoea accounts for probably not more
than half the cases of vulvovaginitis in infants andchildren. Neither oestrogens nor penicillin norsulphonamides offer an absolute therapeutic remedy.No matter what treatment is employed a certainnumber of cases appear to be resistant. Withoestrogens a 72 to 750% cure is about the averagewhich can be expected. With penicillin andsulphonamides a 900% recovery rate is a modestexpectation. A comparative study of the resultsobtained with these three therapeutic measures istabulated (Table 11).The difference between results obtained with
sulphonamides and penicillin is not striking.Sulphonamides, however, possess some toxicity andas such sulphonamide treated cases require to bewatched carefully. The duration of treatment isabout the same in both cases. Penicillin is atpresent expensive and the frequent medicationnecessarily is a drawback. The results of localpenicillin treatment have been very encouraging andcan be depended upon if the parents can cooperate.
Oestrogens also possess a distinct place in thetreatment of vulvovaginitis. With the use ofsynthetic drugs expense is not a serious problem,
TABLE 11COMPARATIVE STUDY OF RESULTS wrrH OEsTRoGENs, SlLPHONAMIDES, AND PENicILLIN
Nature of Percentage of Average Duration Cure Relapse FailureTherapy Cases* of Treatment (0o) (00) (00)
Oestrogens .. 42-5 5-6 weeks 75 -5 13-7 10-8Sulphonamides 34-6 5-9 days 91-5 6-0 2-5Penicillin 14-6 4-1 days 88-3 5 7 5 7
* Twenty cases treated with local antiseptics only are not includxed
271P
rotected by copyright. on F
ebruary 29, 2020 by guest.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.25.123.262 on 1 S
eptember 1950. D
ownloaded from

272 ARCHIVES OF DISEASE IN CHILDHOOD
but the course of treatment is prolonged and therecovery rate lower than with either sulphonamidesor penicillin. The value of oestrogen therapy is,however, considerably increased in the treatment ofrelapsed or refractory cases. It is in these that thecombination of oestrogens with either sulphonamideor penicillin is almost always rewarded with success.
REFERENcESAdair, F. L., and Hac, L. R. (1942). New Eng. J. Med.,
227, 465.Brown, D. K. (1939). Brit. ned. J., 1, 320.Clauberg, K. W. (1930). Dtsch. med. Wschr., 56, 524.Cohn, A., Steer, A., and Adler, E. L. (1941). Amer. J.
Syph., 25, 329.Fessler, A. (1930). Urol. cutan. Rev., 34, 444.Fraser,A.R.(1925). Med.J.S.Afr.,21,31; 73.Greenhill, J. P. (1945). 'Office Gynecology,' p. 66.
Chicago.Hoffman, S. J., Schneider, M., Blatt, M. L., and Herrold,
R. D. (1945). J. Amer. med. Ass., 26, 105.Kamaky, K. J. (1936). Sth. med. J., Nashville, 29, 939.
Quoted by Greenhill, J. P. (1936). 'Year Bookof Obstetrics and Gynaecology,' p. 438. Chicago.
King, A. J., Mascall, W. N., and Price, I. N. 0. (1936).Lancet, 2, 18.
Lees, D. (1928). Edinb. med. J., 35, Trans. Obstet. Soc.,61.
Lewis, R. M. (1933). Amer. J. Obstet. Gynec., 26, 593.(1940). Trans. Amer. Neisserian med. Soc., (June10-11). P. 34.
Martin, C. L. (1935). J. Amer. med. Ass., 104, 192.Mascall, W. N. (1933). Lancet, 2, 233.Mukherjee, C. L. (1940). J. Obstet. GYnaec. Brit. Enp.,
47. 275.Nelson, N. A. (1932). New Engl. J. Med., 207, 135.Ruys, A. C. (1935). J. Amer. med. Ass., 105, 862.Sako, W., Tilbury, R., and Colley, J. (1945). Ibid.,
128, 508.Schauffler, G. C. (1940). Surg. Gynec. Obstet., 71, 286.
(1947). 'Pediatric Gynecology,' p. 148. Chicago.Te Linde, R. W. (1938). J. Amer. med. Ass., 110, 1633.Wattie, N. Quoted by Cruickshank, R., and Sharman,
A. (1934). J. Obstet. Gynaec. Brit. Emp., 41, 217.Williams, P. F. (1926). Amer. J. Obstet. Gynec., 11, 487.
(1933). In Curtis' 'Obstetrics and Gynecology,'Vol. 11., p. 535. Philadelphia.
Witberspoon, J. T. (1935). Amer. J. Obstet. Gynec.,29, 906.
Wynkoop, E. J., and Boggs, E. 0. (1926). N.Y. St. J.Med., 26, 894.
Protected by copyright.
on February 29, 2020 by guest.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.25.123.262 on 1 Septem
ber 1950. Dow
nloaded from





























