Embed Size (px)
Citation preview

Student Presenters: Beth Rohling & Lusi MartinPublic Health Nutrition Students
University of Tennessee at Knoxville

Many forms of GSD type 1 (von Gierke’s disease) :
Type 1a through e
Major forms: Type 1a and 1b
Genetic metabolic disorder of the liver
Inability to breakdown glycogen to glucose
Glycogen is a storage form of glucose in the body
At risk for hypoglycemia

Definition
Type 1a
▪ Deficiency of (or defect in) glucose-6-phosphatase ▪ Normally found in liver, kidney, and intestine
Type 1b
▪ Defect in glucose-6-phosphate translocase▪ Affects transfer of glucose-6-phosphate into ER

Glycogen
Glucose-1-P
Glucose-6-P
Fructose-6-P
Fructose-1,6-P
PyruvateLactate Alanine
Acetyl-CoA
Fatty Acids
Triacylglycerols
Cholesterol
Glucose-6-phosphatase
Glucose
Adenine
Inosine
Uric Acid
ER
Hepatic Glycogen Metabolism in GSD 1

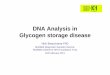
To identify deficiency of enzyme or microsomal translocase systems
Liver biopsy
DNA analysis
Note: CANNOT use cultured skin fibroblasts or blood for enzyme diagnosis because glucose- 6- phosphatase is not present in these cell types

Autosomal recessive disease A 25% chance that their child will develop the disorder
A 50% chance that their child will receive one defective gene from one of the parents, which means the child will not show symptoms of the disorder but is a "carrier"
A 25% chance their child will receive both normal genes, one from each parent, and will not have a GSD

Usually in the first year after birth
Hypoglycemia
Hepatomegaly
Growth retardation
Bleeding tendency
Severe neutropenia
Hyperlacticacidemia
Hyperuricemia
Hypertriacylglycerolemia
Hypercholesterolemia

Lack of newborn screening
GSD Type 1 is unlikely to occur more frequently than 1 case in 50,000 infants

In the past has been poor: Muscle wasting
Stunted growth
Death
With nutrition support: Proven beneficial
Well-controlled patients
Normal blood glucose concentration
Normal linear growth
Even with good metabolic control: Renal insufficiency
Hyperlipidemia

Diagnostic evaluation is most safely performed in a hospital, especially in infants, because of the potential for severe hypoglycemia
Many untreated children are admitted by a hematologist or gastroenterologist for the diagnosis of massive hepatomegaly
Young infants require continuous nasogastric tube feedings to sustain blood sugar levels
Older children can usually be switched to raw cornstarch feedings, which sustain blood glucose values for 4 – 6 hours
Large quantities for raw cornstarch may be necessary, because overall use of this material is impaired in patients compared with healthy control subjects

To correct primary imbalance in metabolic relationships
i. Maintain normal BG concentration by providing frequent complex dietary carbohydrate (CH2O)
ii. Maintain normal BG concentration throughout day and night to ameliorate secondary biochemical abnormalities
Note: Therapy is designed to provide just enough hepatic glucose for normal glycogenolysis and gluconeogenesis while keeping BG levels in an acceptable range.

To help maximize blood sugar and lactic acid control, nutrition and energy
Carbohydrate: - Complex vs. Simple Sugars- Combination of taking cornstarch and eating complex carbs with each meal is important to maintain appropriate blood sugar levels
Note: Complex Carbs should be avoided if they contain added sugar such as dried fruits and honey.
Complex Carbohydrate: breads, cereals, grains, rice, pasta, crackers, beans (garbanzo, pinto, kidney)
Simple sugars include: Glucose, Galactose (dairy, sugar), Lactose (galactose + glucose), Fructose (fruit sugar) and Sucrose (fructose + glucose)

SUGARS ALLOWED
Glucose Dextrose Maltose Maltodextrin Dextrin Pure Corn Syrup Corn Syrup Solids Karo dark corn syrup 98% glu Karo light syrup 97% glu Karo pancake syrup 94% gluc
SUGARS NOT ALLOWED
Fructose (natural sugar found in fruit) also a component of sucrose
Galactose (a component of lactose), Lactose (sugar found in milk)
Sucrose (common “table sugar”) Honey High Fructose Corn Syrup Corn Syrup (contains fructose) Brown Sugar Invert Sugar Powdered sugar, confectioners
sugar Maple Sugar Molasses Sorghum

Fruits contain fructose and should be avoided. If consumed, it should be in very small amounts and should not be consumed in a meal that includes foods that contain galactose
Vegetables are lower in sugar and low in calories and should be eaten. However it is necessary to avoid using more than 2 packets of ketchup at a time and limiting tomato/marinara sauces on foods to no more than ¼ cup per meal because of the fructose in the tomato
Milk/Dairy is usually limited to ½ serving (4 oz of milk or 1 oz of cheese) of a low fat dairy product per day. Use soymilk with caution due to added sugar.

Most meat dishes are low in sugar. Avoid meats cooked in sweet sauces
Dietary fat limited to 20% of total daily calories with equal distribution between monoun, polyun, and saturated fats. Cholesterol should be limited to <200mg/dL
Avoid beverages that contain fructose, lactose or extra calories should be avoided

• Restrictions require supplementation
- Multi-vitamin (avoid taking together with iron & multivitamin)
- Calcium
Note: Calcium is better absorbed with food
Calcium Supplement and Multivitamin Suggestion in Type 1 GSD
Calcium supplement suggestions • UpCal D (powder) - Global Health Products• Cal-Quick (liquid) –Twin Lab• Calci-Mix (powdered capsule) – Watson Pharmaceuticals• CitraCal (tablet) or any type of calcium citrate•Tums (tablet) - available in sugar free• Calcium Carbonate
Multivitamin suggestion • One-A-Day (sugar-free, children’s and adult varieties available) or generic equivalent• Flinstone’s complete (sugar-free available)• Centrum or generic equivalent.

Most significant problem is metabolic acidosis precipitated by minor illnesses
If vomiting illness persists child should be seen and assessed for dehydration, acidosis, and hypoglycemia

Gender: Female- Full term: 7 lbs 6oz
Age: 11 yrs 1 month
Height: 126.9 cm (50in)
Weight: 31.3 kg (68.9lbs)

10-25th %ile wt for age
<3rd %ile ht for age
Height age: 7 yrs 10 mths
Exp wt for ht: 25.5kg (56.1lbs)
%ile BMI for age: 50 – 75th %ile
Evaluation:Short stature, above exp wt for ht, resulting in higher BMI

Emily Marsh

Mother, Father, & Two Full Siblings living in the home
No family history of GSD
Insurance through Aetna

Diagnosed with GSD type 1a 3 months of age
Generally healthy & no dental problems
No known allergies
Medication: Zantac 75mg

Lab Test Lab Value Normal Range
Glc 88 65 - 100
Uric acid 7.8mg/dL 3 – 8.7 mg/dL
Lactic acid 2.6mg/dL H 0.4 – 2.0mg/dL
Cholesterol 302mg/dL H < 200mg/dL
Gamma GT 39U/L 8 – 78 U/L
TG 913 mg/dL H < 150 mg/dL
Prealbumin 30.6 mg/dL 17 – 34 mg/dL
Evaluation:
1. Elevated TG level: Common to GSD1
2. Elevated Cholesterol: Common to GSD1
3. Elevated Lactic acid: Common to GSD1

Vitamin/Mineral supplement (2 tablets/daily)
Formula:
60g Elecare
2.5 Tbsp Soy Protein Isolate
8 Tbsp Cornstarch
1tsp CalQuick
All mixed w/ water to a total volume of 16 fl oz

Chooses foods off of school menu
Mother concern for high CHO & limited vegetable choices
Mother is concern for low BG in the mornings and lunch hours
Good appetite

3 Day Food Record provided
Intake (3 day avg) Prescribed
Calories (kcals) 1720 1627
Protein (g) 43.0 (9%) 52 (13%)
Fat (g) 54 (28%) 41 (23%)
Carbohydrate (g) 260 (60%) 258 (64%)
Calcium (mg) 510** 1300
** Calculated without CalQuick. Approximately 885mg when calculated
with ¾ tsp Calquick.

Impaired nutrient utilization (P) related to diagnosis of GSD type 1A (E) as evidenced by altered lab value (S)

Hypoglycemia
Hepatomegaly
Short stature
Lactic acidemia
Hypertrigylceridemia
ICD- 9 Code: 271.0

Increase protein intake to meet prescribed diet to prevent muscle wasting & promote growth
Limit dietary intake to prescribed levels to improve plasma TG & cholesterol values
Take calcium supplements regularly as prescribed to promote bone health and growth

Assessing food intake
Diet Prescription
Nutrition Education
Support
Monitoring & Evaluating Progress

Questions???