Embed Size (px)
Citation preview
Achieving Glucose Balance in
Type 2 Diabetes Mellitus:
Targeted Pharmacotherapy
Curtis Triplitt, PharmD, CDE
Texas Diabetes Institute
Assistant Professor, Medicine/Diabetes
University of Texas Health Science Center
at San Antonio
2
Faculty InformationPresenter
Curtis Triplitt, PharmD, CDE
Texas Diabetes Institute
Assistant Professor, Medicine/Diabetes
University of Texas Health Science Center at San Antonio
San Antonio, TX
Moderator
Elena Beyzarov, PharmD
Director, Scientific Affairs
Pharmacy Times Office of Continuing Professional Education
This activity is supported by an educational grant from
Bristol-Myers Squibb and AstraZeneca LP.
3
DisclosuresCurtis Triplitt, PharmD, CDE, has disclosed the following commercial financial relationships:
Consultant/Advisory Board: Roche, Takeda Pharmaceuticals
Speakers’ Bureau: Amylin, Eli Lilly, Pfizer
Pharmacy Times Office of Continuing Professional Education
Planning Staff—Judy V. Lum, MPA; Elena Beyzarov, PharmD; Jennifer Barrio; and Donna
W. Fausak— have no financial relationships with commercial interests to disclose related to
this activity.
The American Journal of Managed Care
Planning Staff—Jeff D. Prescott, PharmD, RPh; Kara Guarini, MS; Ida Delmendo; and
Christina Doong— have no financial relationships with commercial interests to disclose
related to this activity.
The contents of this webinar may include information regarding the use of products that may
be inconsistent with or outside the approved labeling for these products in the United States.
Pharmacists should note that the use of these products outside current approved labeling is
considered experimental and are advised to consult prescribing information for these
products.
4
Educational Objectives
After completion of this activity, participants should be
better able to:
•Describe the mechanisms of action of currently available
pharmacologic options for the management of type 2 diabetes
mellitus
•Address the pharmacologic target and outcome associated with
each medication
•Review emerging antidiabetic agents, their role in diabetes
management, and how they will address defects in glucose
regulation
5
Pharmacy Accreditation
Pharmacy Times Office of Continuing
Professional Education is accredited by the
Accreditation Council for Pharmacy Education
(ACPE) as a provider of continuing pharmacy
education. This activity is approved for 1 contact
hour (0.1 CEU) under the ACPE universal activity
number 0290-0000-11-061-H01-P. This activity is
available for CE credit through January 25, 2014.
Type of Activity: Knowledge
Achieving Glucose Balance in
Type 2 Diabetes Mellitus:
Targeted Pharmacotherapy
Curtis Triplitt, PharmD, CDE
Texas Diabetes Institute
Assistant Professor, Medicine/Diabetes
University of Texas Health Science Center
at San Antonio
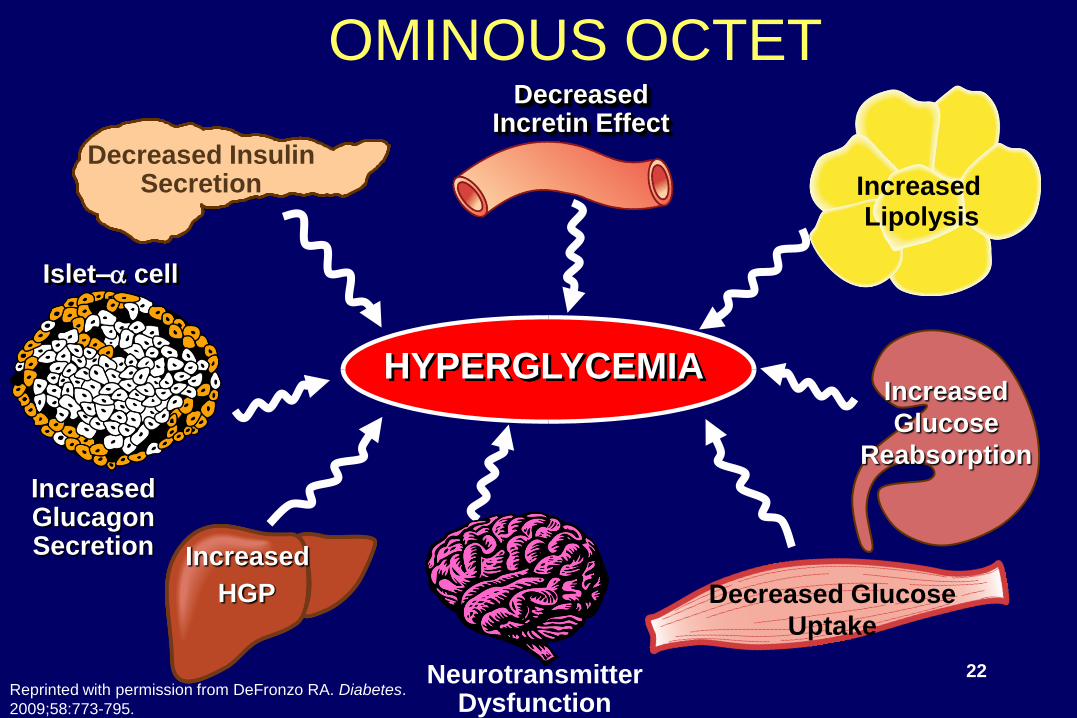
IncreasedHGP
Hyperglycemia
ETIOLOGY OF T2DM
DEFN75-3/99 Decreased GlucoseUptake
Impaired InsulinSecretion Increased Lipolysis
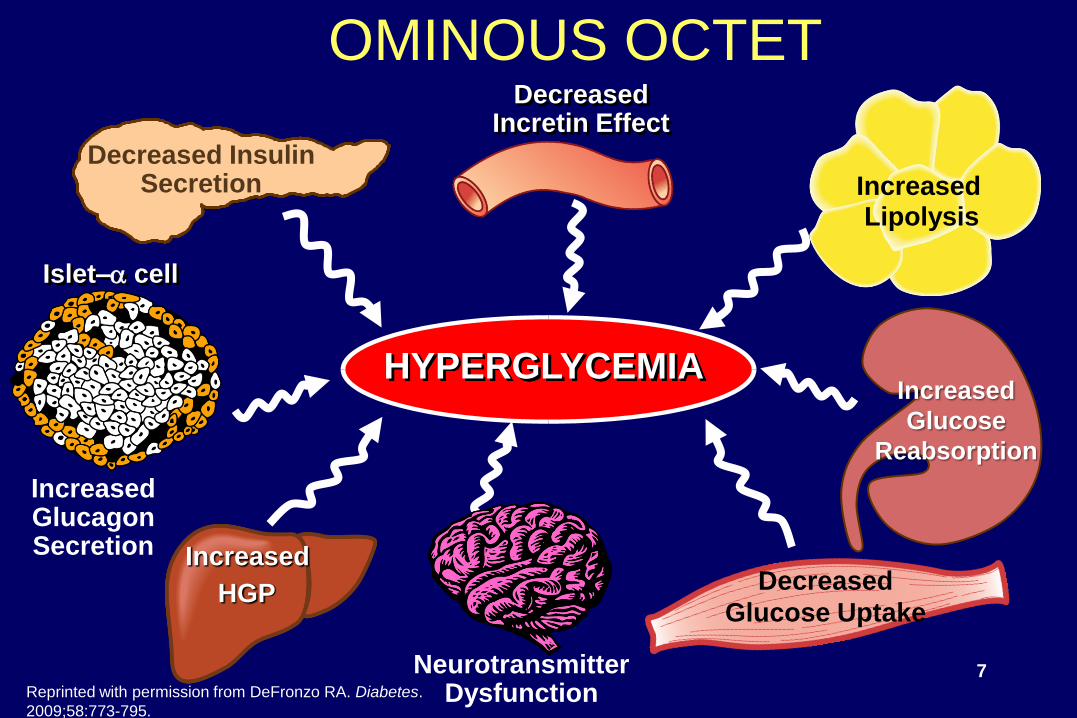
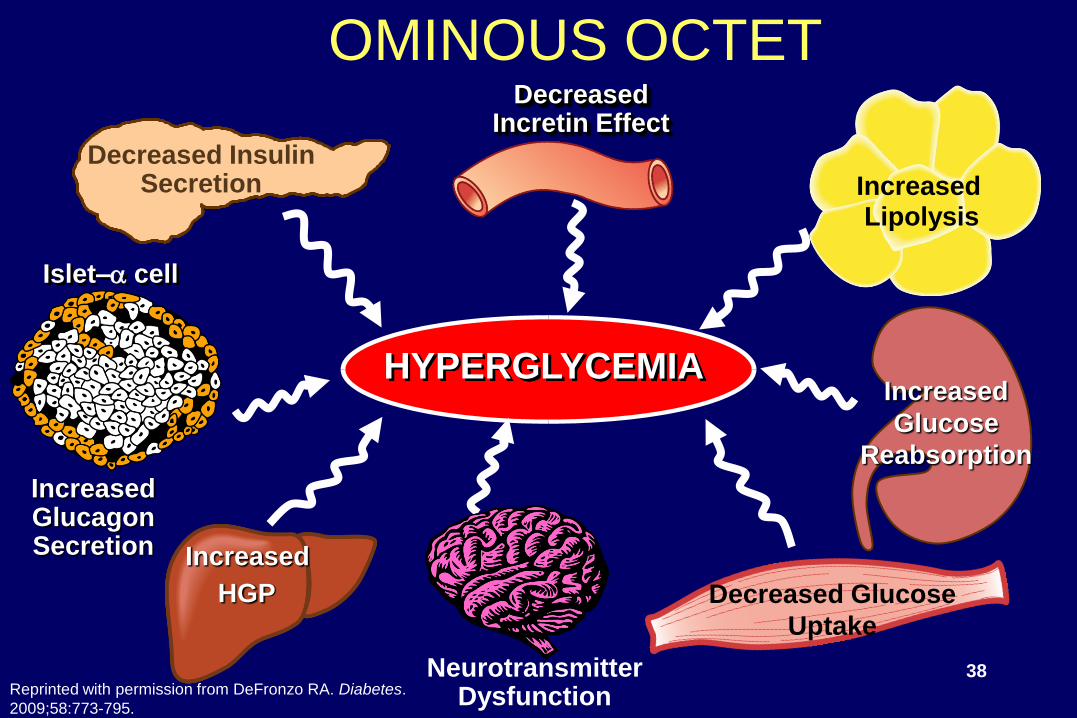
HYPERGLYCEMIA
DecreasedIncretin Effect
Decreased InsulinSecretion
Increased
HGP
Islet–a cell
IncreasedGlucagonSecretion
OMINOUS OCTET
IncreasedLipolysis
Increased
Glucose
Reabsorption
NeurotransmitterDysfunction
Decreased
Glucose Uptake
7Reprinted with permission from DeFronzo RA. Diabetes.
2009;58:773-795.

Management of Diabetes• Nonpharmacologic Therapy
• Pharmacologic Therapy– Sulfonylureas: many
– Biguanides: metformin
– Thiazolidinediones: pioglitazone, rosiglitazone
– Meglitinides (insulin secretagogues): repaglinide, nateglinide
– a-glucosidase inhibitors: acarbose, miglitol
– Insulins
– Incretin Therapy
• Mimetics (GLP-1 agonists): exenatide, liraglutide
• DPP-4 inhibitors: sitagliptin, saxagliptin, linagliptin
– Bile acid sequestrants: colesevelam
– Dopamine agonists: bromocriptine
– Amylinomimetics: pramlintide8
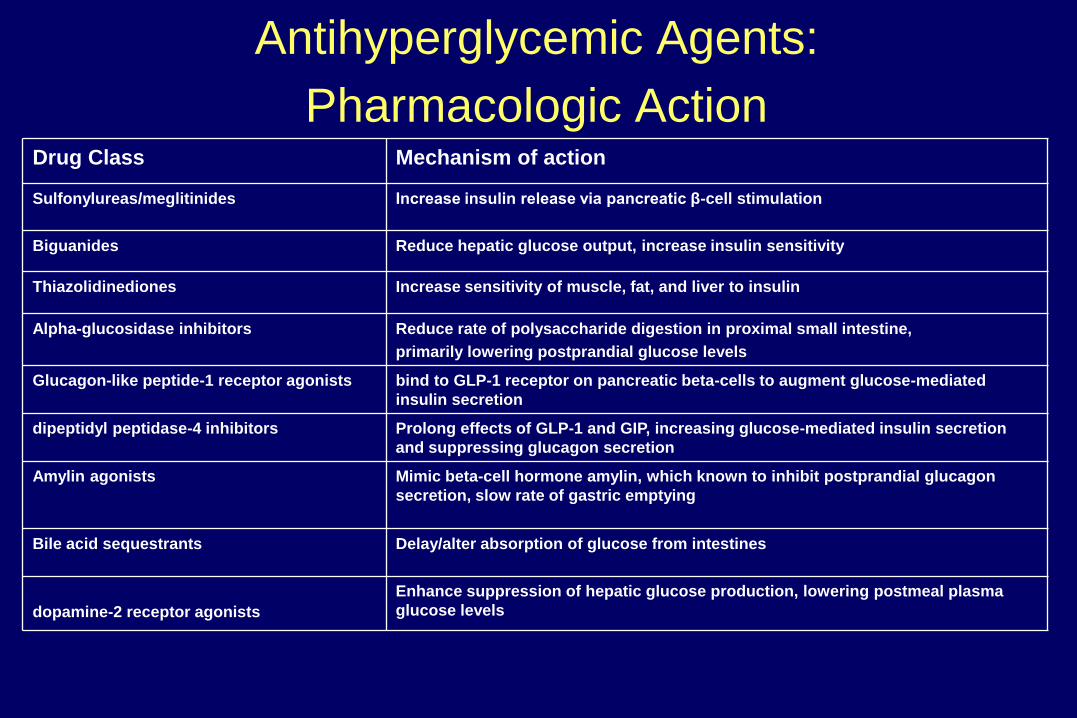
Antihyperglycemic Agents:
Pharmacologic ActionDrug Class Mechanism of action
Sulfonylureas/meglitinides Increase insulin release via pancreatic β-cell stimulation
Biguanides Reduce hepatic glucose output, increase insulin sensitivity
Thiazolidinediones Increase sensitivity of muscle, fat, and liver to insulin
Alpha-glucosidase inhibitors Reduce rate of polysaccharide digestion in proximal small intestine,
primarily lowering postprandial glucose levels
Glucagon-like peptide-1 receptor agonists bind to GLP-1 receptor on pancreatic beta-cells to augment glucose-mediated
insulin secretion
dipeptidyl peptidase-4 inhibitors Prolong effects of GLP-1 and GIP, increasing glucose-mediated insulin secretion
and suppressing glucagon secretion
Amylin agonists Mimic beta-cell hormone amylin, which known to inhibit postprandial glucagon
secretion, slow rate of gastric emptying
Bile acid sequestrants Delay/alter absorption of glucose from intestines
dopamine-2 receptor agonists
Enhance suppression of hepatic glucose production, lowering postmeal plasma
glucose levels
Sulfonylureas and Meglitinides
• Mechanism of Action
– Increase insulin release via pancreatic β-cell
stimulation
– Insulin helps to decrease hepatic glucose
production (decreases fasting blood glucose)
– May increase muscle glucose uptake slightly
through decrease in ―glucotoxicity‖
• Sulfonylureas
– Long half-life, long duration of action
• Meglitinides
– Short half-life, short duration of action 10
-50
0
50
100
150
200
250
300
Time (hours)
DF
rom
Ba
se
lin
e in
In
su
lin
AU
C0–
12
h(p
mo
l/L
)
10 1260 31 2 4 5 7 8 9 11
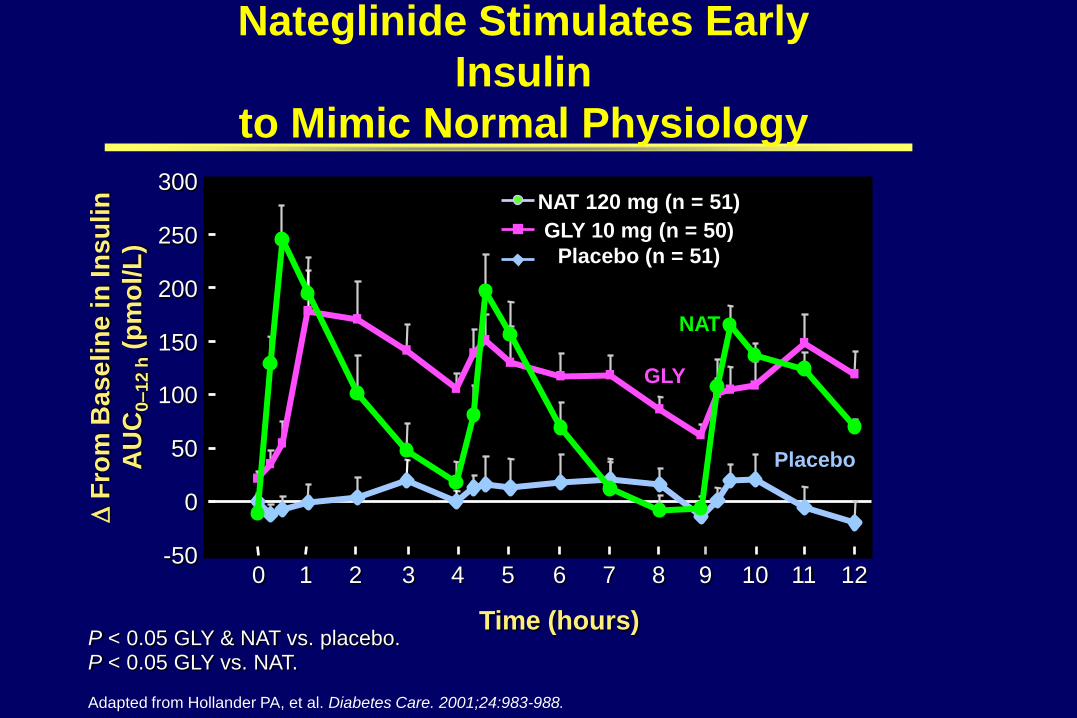
P < 0.05 GLY & NAT vs. placebo.P < 0.05 GLY vs. NAT.
Adapted from Hollander PA, et al. Diabetes Care. 2001;24:983-988.
Nateglinide Stimulates Early
Insulin
to Mimic Normal Physiology
NAT 120 mg (n = 51)
GLY 10 mg (n = 50)
Placebo (n = 51)
GLY
Placebo
NAT
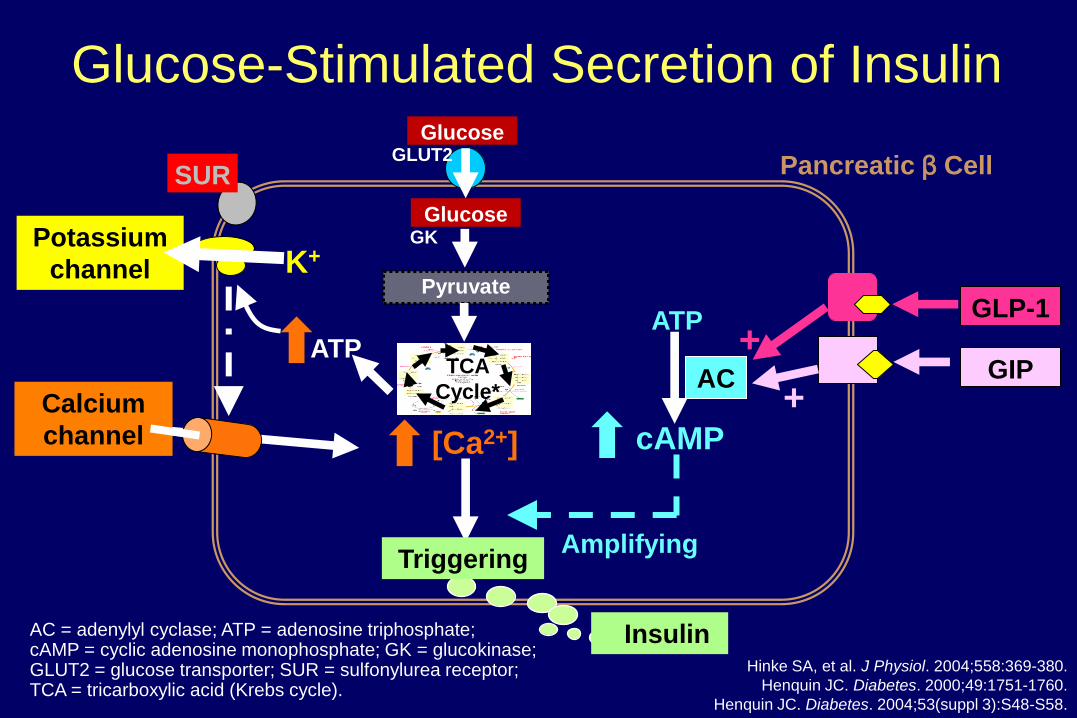
Pancreatic β Cell
Glucose-Stimulated Secretion of Insulin
AC
+GLP-1
GIP
+
AC = adenylyl cyclase; ATP = adenosine triphosphate; cAMP = cyclic adenosine monophosphate; GK = glucokinase; GLUT2 = glucose transporter; SUR = sulfonylurea receptor; TCA = tricarboxylic acid (Krebs cycle).
Hinke SA, et al. J Physiol. 2004;558:369-380.
Henquin JC. Diabetes. 2000;49:1751-1760.
Henquin JC. Diabetes. 2004;53(suppl 3):S48-S58.
K+Potassium
channel
SUR
cAMP
ATP
Amplifying
GLUT2Glucose
ATP
Pyruvate
GK
TCA
Cycle*
Glucose
Insulin
[Ca2+]
Triggering
Calcium
channel

Tan (n = 297)PERISCOPE (n = 181)
Hanefeld (n = 250)
Chicago (n = 230)UKPDS (n = 1573)
ADOPT (n = 1441)
Sulfonylureas
Change in A
IC (
%)
Glyburide
Glyburide
-2
-1
0
0 1 2 3 4 5 6 10
Glimepiride
Glyburide
Gliclazide
Glyburide
Thiazolidinediones
-2
-1
0
Change in A
IC (
%)
0 1 2 3 4 5 6
Durability of Glycemic Control:
Assessed by Serial A1C
PIO
Pioglitazone (PIO) Rosiglitazone
PIO
PIO
Adapted from DeFronzo RA. Diabetes. 2009;58:773-795.
13
Time (years)Time (years)
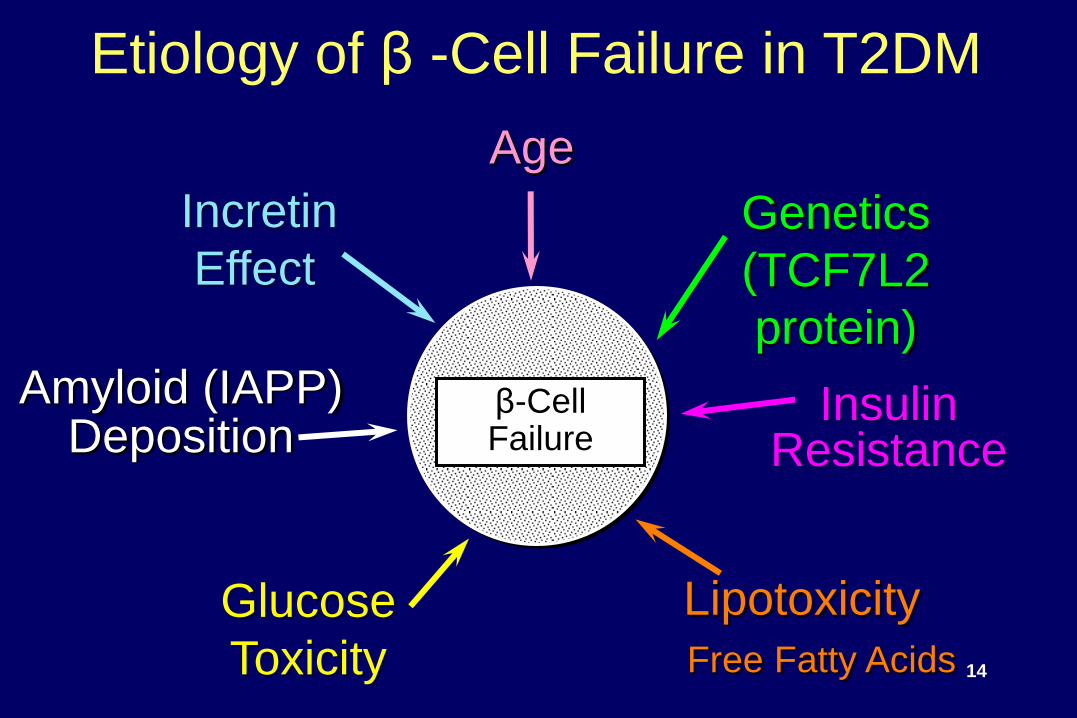
Insulin Resistance
Etiology of β -Cell Failure in T2DM
Genetics
(TCF7L2
protein)
Age
β-CellFailure
Lipotoxicity
Free Fatty Acids
Glucose
Toxicity
Amyloid (IAPP)Deposition
Incretin
Effect
14

Lipotoxicity
● Elevated plasma free fatty acids (FFAs)
● Increased tissue fat content
● Altered fat storage
● ―Sick‖ fat cell
15
Thiazolidinediones and Preservation
of β-Cell Function
● Direct effect on the β-cell (PPARg)
● Amelioration of insulin resistance
● Reduction in plasma FFAs (lipotoxicity)
● Mobilization of toxic lipid metabolites
(FACoA, DAG, ceramides) out of the β-cell
(lipotoxicity)
● Reversal of glucotoxicity
16
17
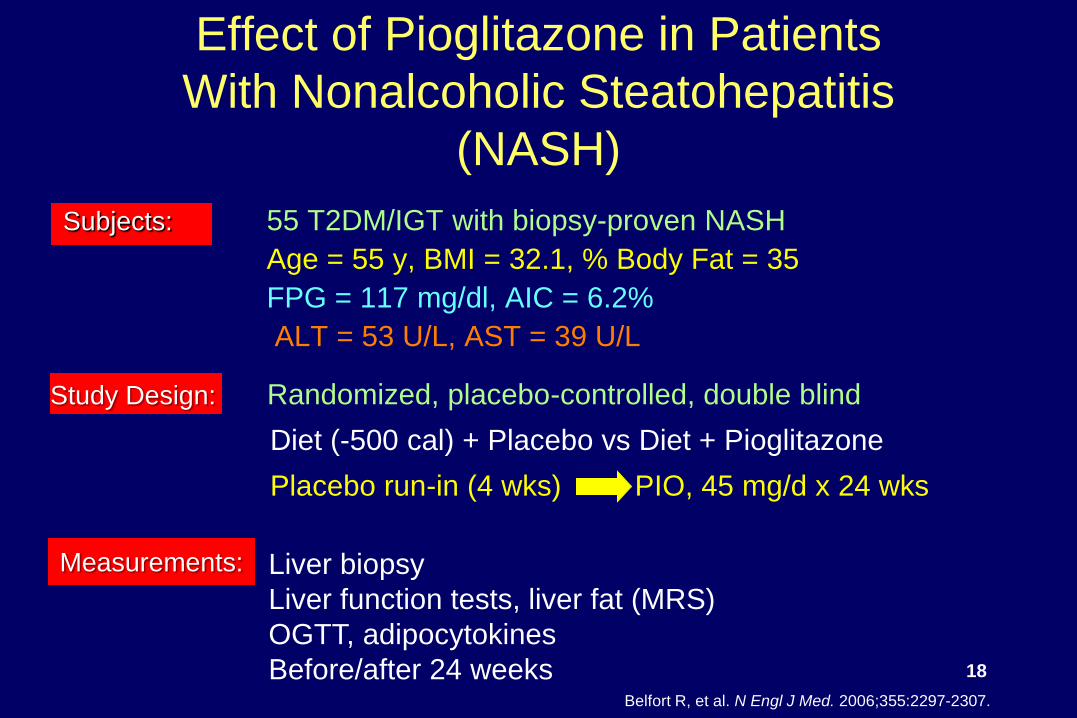
Effect of Pioglitazone in Patients
With Nonalcoholic Steatohepatitis
(NASH)
Subjects: 55 T2DM/IGT with biopsy-proven NASH
Age = 55 y, BMI = 32.1, % Body Fat = 35
FPG = 117 mg/dl, AIC = 6.2%
ALT = 53 U/L, AST = 39 U/L
Measurements:
Study Design: Randomized, placebo-controlled, double blind
Diet (-500 cal) + Placebo vs Diet + Pioglitazone
Placebo run-in (4 wks) PIO, 45 mg/d x 24 wks
Liver biopsy
Liver function tests, liver fat (MRS)
OGTT, adipocytokines
Before/after 24 weeksBelfort R, et al. N Engl J Med. 2006;355:2297-2307.
18
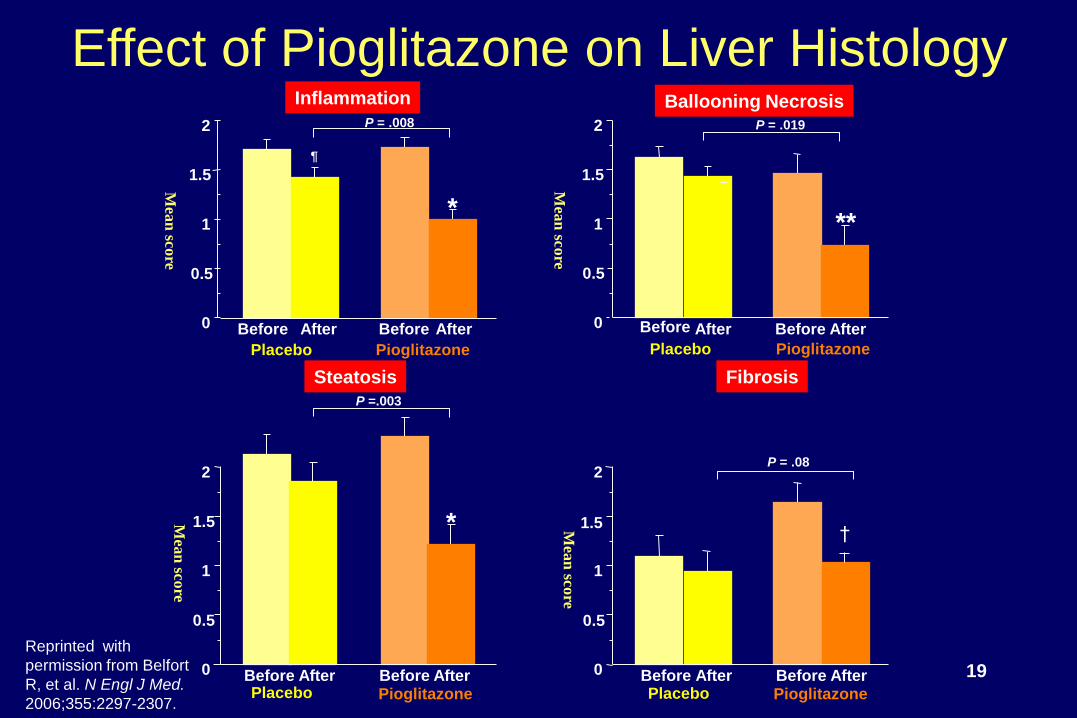
Steatosis
Inflammation
0
0.5
1
1.5
2
Before After
Pioglitazone
Before After
Placebo
*
¶
P = .008
Ballooning Necrosis
0
0.5
1
1.5
2
Before After
Pioglitazone
Before After
Placebo
**
P = .019
Fibrosis
P =.003
0
0.5
1
1.5
2
*
Before AfterPioglitazone
Before AfterPlacebo
0
0.5
1
1.5
2
Before AfterPioglitazone
Before AfterPlacebo
†
P = .08
Effect of Pioglitazone on Liver Histology
19
Reprinted with
permission from Belfort
R, et al. N Engl J Med.
2006;355:2297-2307.
Mea
n sco
re
Mea
n sco
re
Mea
n sco
re
Mea
n sco
re
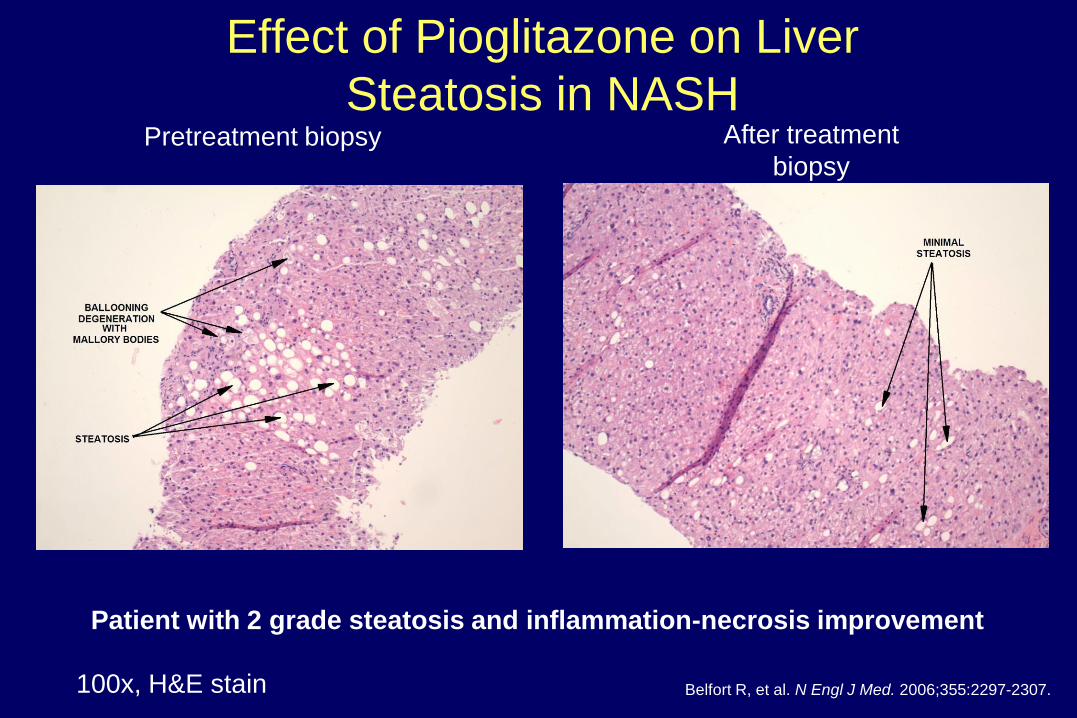
Patient with 2 grade steatosis and inflammation-necrosis improvement
Effect of Pioglitazone on Liver
Steatosis in NASHPretreatment biopsy After treatment
biopsy
100x, H&E stain Belfort R, et al. N Engl J Med. 2006;355:2297-2307.

Glitazones: Documented Issues
• Fluid retention
– Edema, congestive heart failure (CHF) risk
• CHF
– Black box warning for use in NYHA class III and IV
• Signs and symptoms: short of breath, dyspnea on exertion,
peripheral edema, sleeping on more pillows than normal
• Fracture risk: osteocyte, osteoclast, osteoblast effect
– Do not use in documented osteoporosis, consider risk/benefit in post-
menopausal women
Rosiglitazone: ischemic events, restricted use
Pioglitazone: bladder carcinoma, 3 extra cases in 10,000 patient/year
exposure
Actos [package insert]. East Hanover, NJ: Takeda Pharmaceuticals America, Inc; 2011.
Avandia [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2011.
IncreasedHGP
Hyperglycemia
ETIOLOGY OF T2DM
DEFN75-3/99 Decreased GlucoseUptake
Impaired InsulinSecretion Increased Lipolysis
HYPERGLYCEMIA
DecreasedIncretin Effect
Decreased InsulinSecretion
Increased
HGP
Islet–a cell
IncreasedGlucagonSecretion
OMINOUS OCTET
IncreasedLipolysis
Increased
Glucose
Reabsorption
NeurotransmitterDysfunction
Decreased Glucose
Uptake
22Reprinted with permission from DeFronzo RA. Diabetes.
2009;58:773-795.

Liver and Kidney
• Liver: Major source of net endogenous glucose
production
– Kidney: potentially responsible for 10% to 15% of fasting
glucose production
• Accomplished by gluconeogenesis and
glycogenolysis when glucose levels are low
• Glycogen synthesis when glucose levels are high
• Can oxidize glucose for energy and convert to fat;
may be incorporated into VLDL for transport. 23
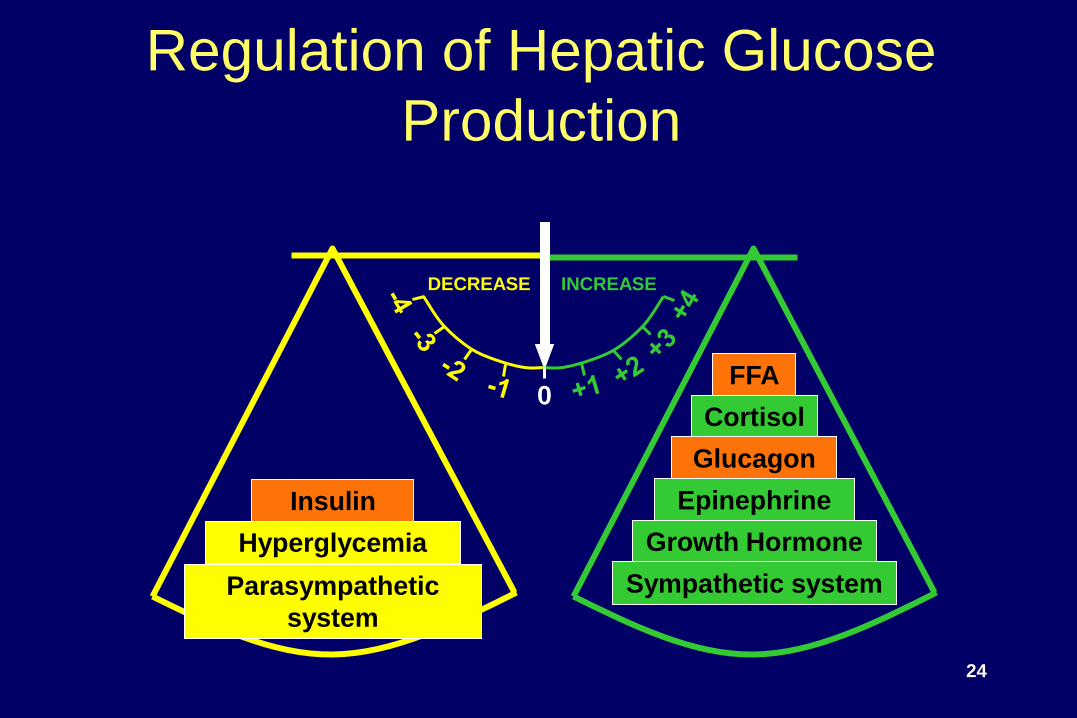
Regulation of Hepatic Glucose
Production
DECREASE INCREASE
0
Parasympathetic
system
Hyperglycemia
Insulin
FFA
Cortisol
Glucagon
Epinephrine
Growth Hormone
Sympathetic system
24
In general, monotherapy, most
commonly involving metformin or
sulfonylureas, may not have durable
effects in advancing hyperglycemia
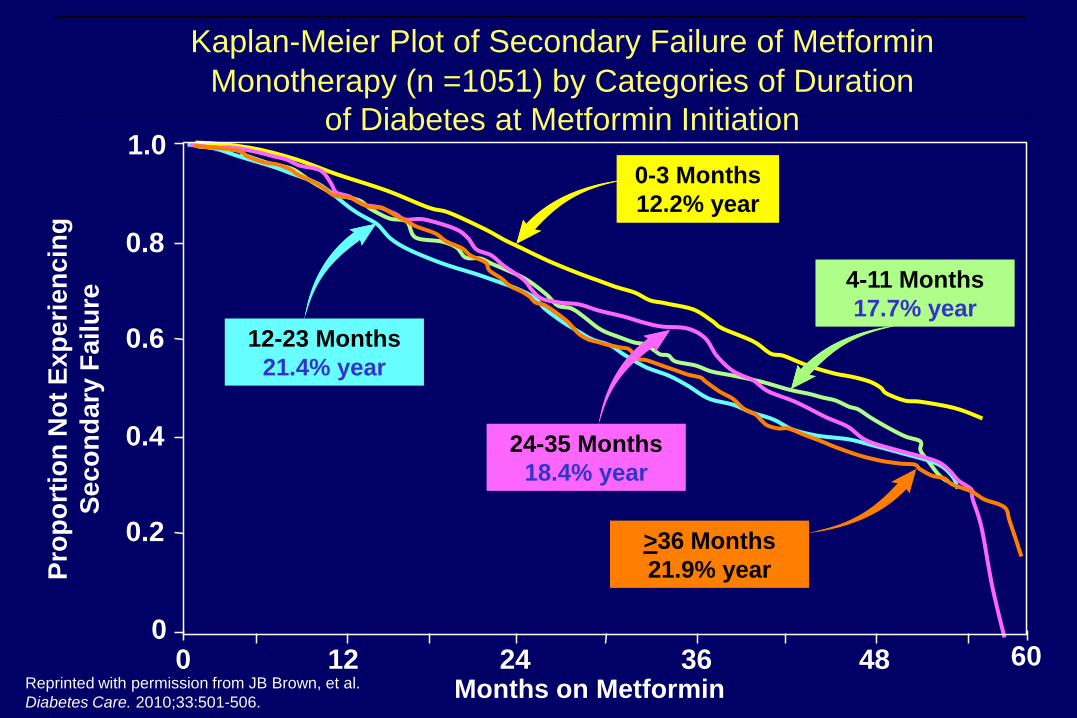
Kaplan-Meier Plot of Secondary Failure of Metformin
Monotherapy (n =1051) by Categories of Duration
of Diabetes at Metformin Initiation
0
0.2
0.4
0.6
0.8
1.0
0 12 24 36 48 60
0-3 Months
12.2% year
24-35 Months
18.4% year
>36 Months
21.9% year
12-23 Months
21.4% year
4-11 Months
17.7% year
Months on Metformin
Pro
po
rtio
n N
ot
Ex
pe
rie
nc
ing
Se
co
nd
ary
Fa
ilu
re
Reprinted with permission from JB Brown, et al.
Diabetes Care. 2010;33:501-506.
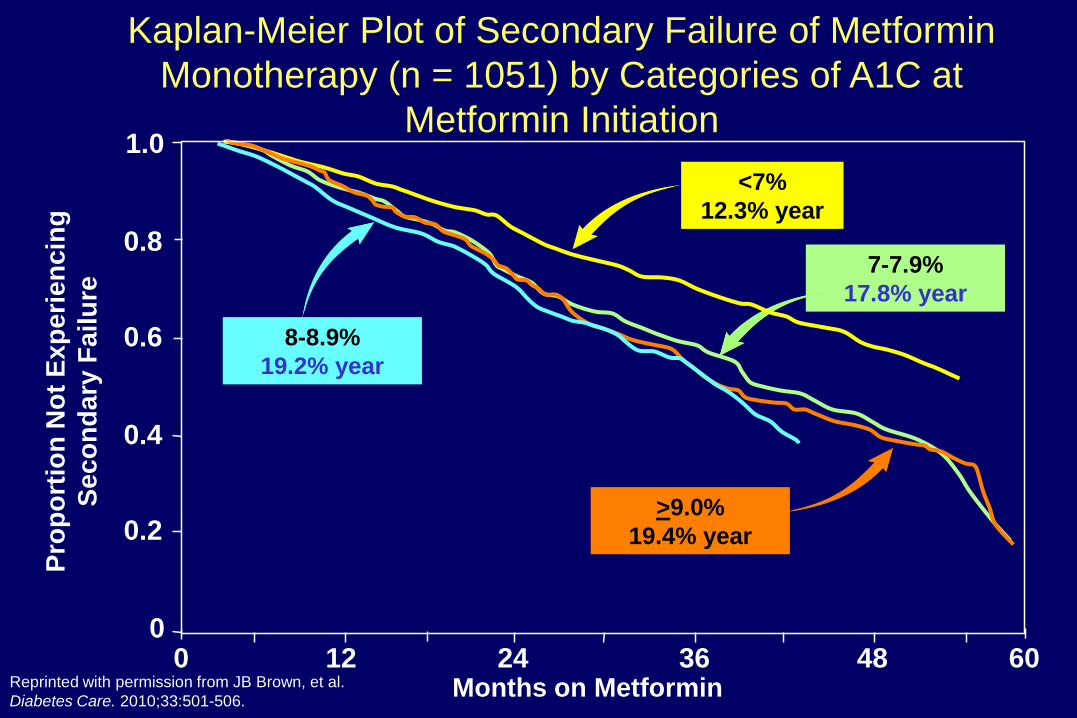
0
0.2
0.4
0.6
0.8
1.0
0 12 24 36 48 60
<7%
12.3% year
>9.0%
19.4% year
8-8.9%
19.2% year
7-7.9%
17.8% year
Months on Metformin
Pro
po
rtio
n N
ot
Ex
pe
rie
nc
ing
Se
co
nd
ary
Fa
ilu
re
Kaplan-Meier Plot of Secondary Failure of Metformin
Monotherapy (n = 1051) by Categories of A1C at
Metformin Initiation
Reprinted with permission from JB Brown, et al.
Diabetes Care. 2010;33:501-506.

0
4
8
12
25-44 (n=1000) 45-59 (n=1586) > 60 (n=648)
Lifestyle Metformin Placebo
Diabetes Incidence Rates by Age
Age (years)Knowler WC, et al; for the Diabetes Prevention Program Research Group. N Engl J Med. 2002;346:393-403.
Cases/1
00 p
ers
on
-yr
28
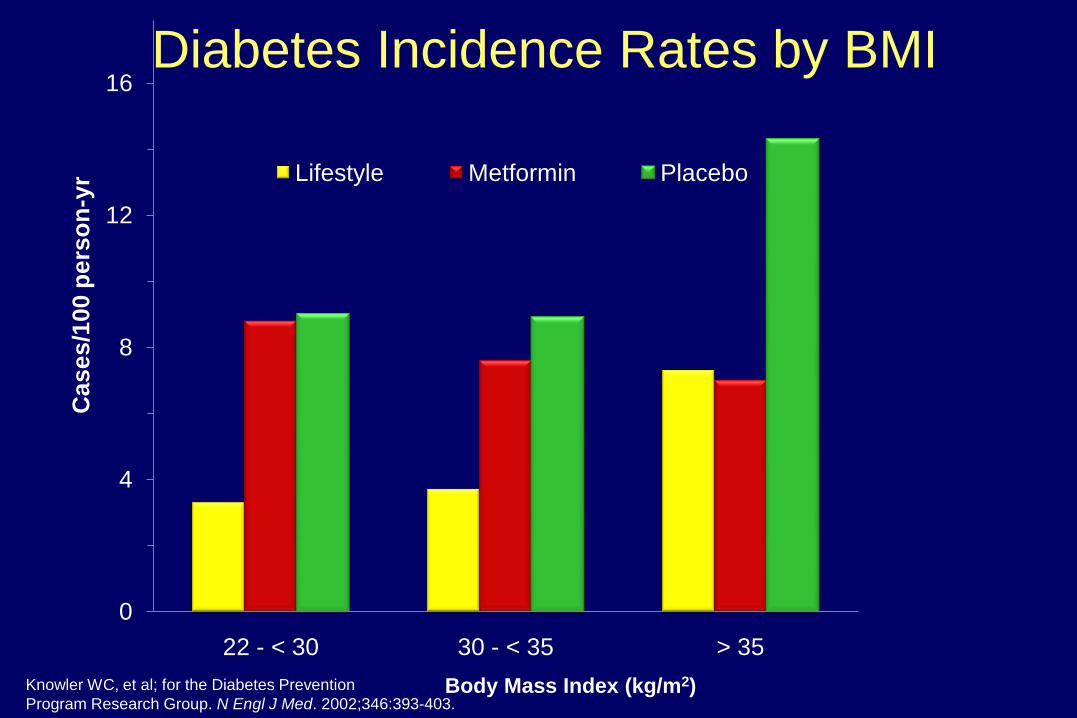
0
4
8
12
16
22 - < 30 30 - < 35 > 35
Ca
se
s/1
00
pe
rso
n-y
r Lifestyle Metformin Placebo
Diabetes Incidence Rates by BMI
Body Mass Index (kg/m2)Knowler WC, et al; for the Diabetes Prevention
Program Research Group. N Engl J Med. 2002;346:393-403.
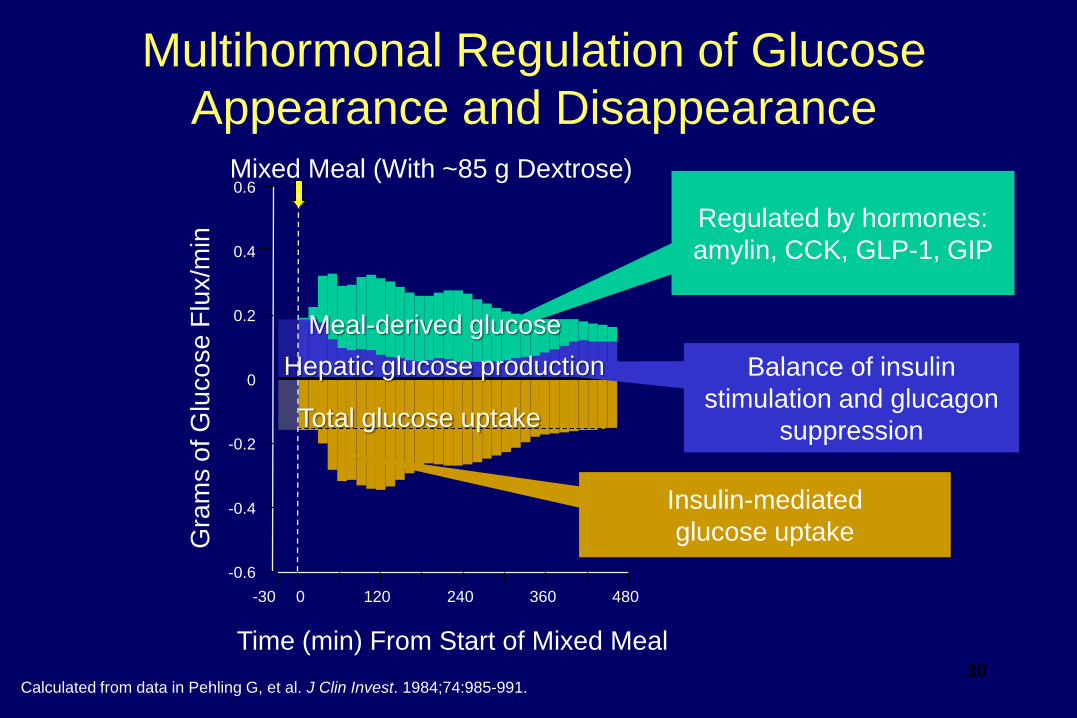
Time (min) From Start of Mixed Meal
Mixed Meal (With ~85 g Dextrose)
0 120 240 360 480
-0.6
-0.4
-0.2
0
0.2
0.4
0.6G
ram
s o
f G
luco
se
Flu
x/m
in
-30
Calculated from data in Pehling G, et al. J Clin Invest. 1984;74:985-991.
Insulin-mediated
glucose uptake
Balance of insulin
stimulation and glucagon
suppression
Regulated by hormones:
amylin, CCK, GLP-1, GIP
Meal-derived glucose
Hepatic glucose production
Total glucose uptake
Multihormonal Regulation of Glucose
Appearance and Disappearance
30
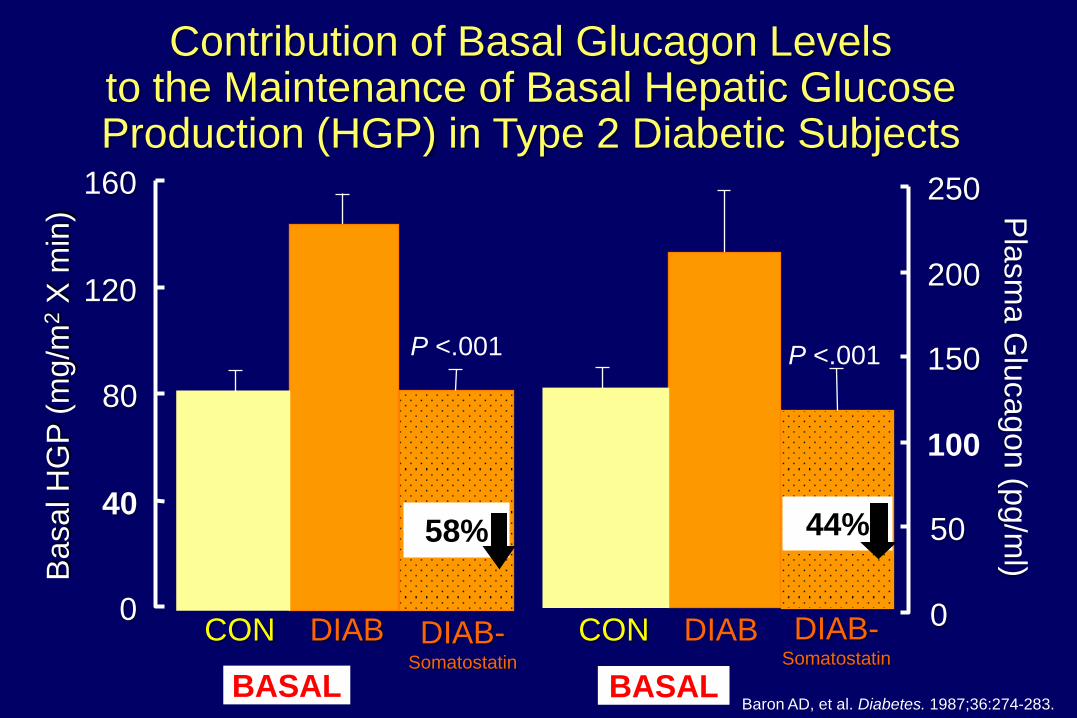
Contribution of Basal Glucagon Levels to the Maintenance of Basal Hepatic Glucose Production (HGP) in Type 2 Diabetic Subjects
Baron AD, et al. Diabetes. 1987;36:274-283.
0
50
100
150
200
250
Pla
sm
a G
luca
go
n (p
g/m
l)Basal H
GP
(m
g/m
2X
min
)
0
40
80
120
160
BASAL BASAL
CON DIAB DIAB-Somatostatin
P <.001
58%
CON DIAB DIAB-Somatostatin
P <.001
44%

Time After Sustacal Meal, min
0
5
10
15
20
-30 0 30 60 90 120 150 180
Pla
sm
a A
mylin
, p
mo
l/L
Meal
T1DM (n = 190)
Insulin-using T2DM (n = 27)
Without diabetes (n = 27)
Amylin Is Cosecreted With Insulin
and Deficient in Diabetes
Pla
sm
a In
su
lin,
pm
ol/L
30
25
20
15
10
5
Time, 24 h
600
400
200
0
Meal Meal Meal
Amylin
Insulin
Pla
sm
a A
mylin
, pm
ol/L
Healthy male adults (n = 6)
7 AM Midnight5 PM12 Noon
Central satiety, decreases glucagon, slows gastric emptying
Reprinted with permission from Kruger DF, et al. Diabetes Educ. 1999;25:389-397.
32
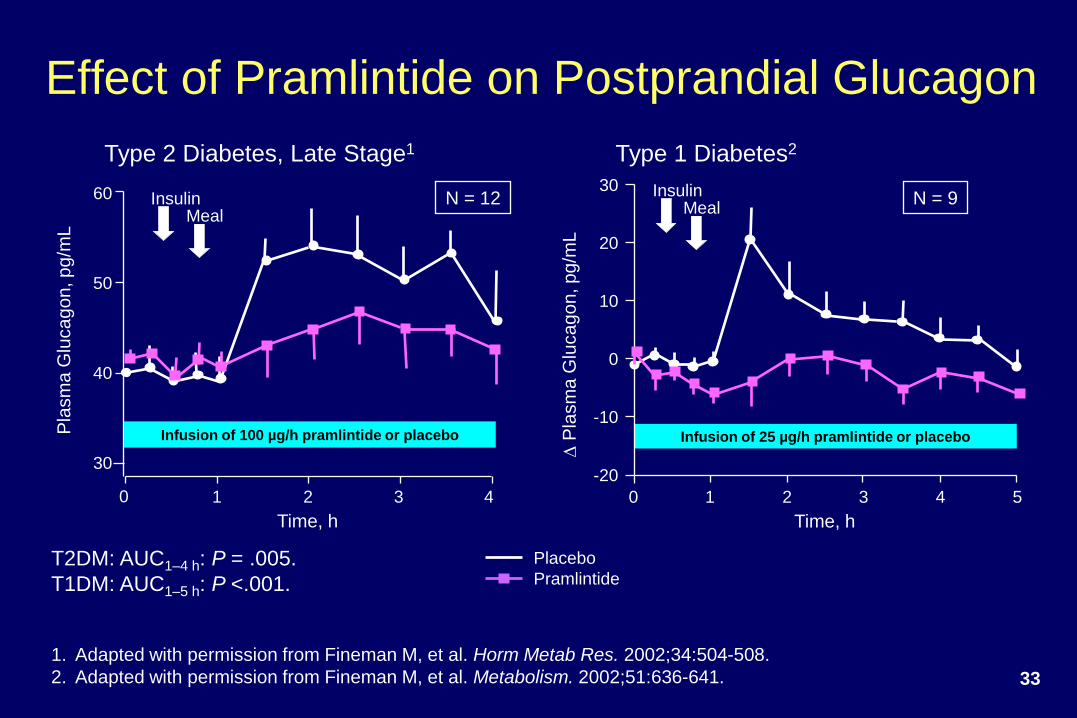
33
Effect of Pramlintide on Postprandial Glucagon
Type 1 Diabetes2
Time, h
Placebo
Pramlintide
Infusion of 25 µg/h pramlintide or placebo
-20
0
10
20
30
-10
InsulinMeal
0 2 3 4 51
Type 2 Diabetes, Late Stage1
Time, h
Pla
sm
a G
luca
go
n, p
g/m
L
InsulinMeal
60
40
30
50
Infusion of 100 µg/h pramlintide or placebo
0 1 2 3 4
DP
lasm
a G
luca
go
n, p
g/m
LT2DM: AUC1–4 h: P = .005.
T1DM: AUC1–5 h: P <.001.
1. Adapted with permission from Fineman M, et al. Horm Metab Res. 2002;34:504-508.
2. Adapted with permission from Fineman M, et al. Metabolism. 2002;51:636-641.
N = 12 N = 9
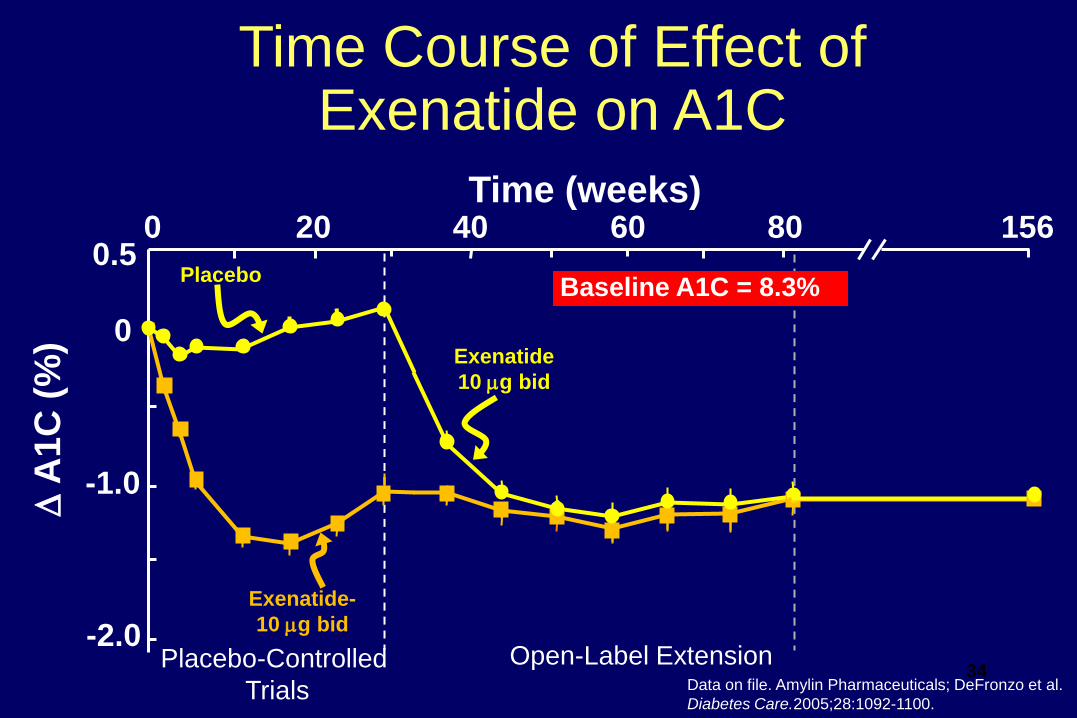
Open-Label Extension
Baseline A1C = 8.3%
Time Course of Effect of Exenatide on A1C
Time (weeks)
D A
1C
(%
)
0 20 40 60 80 156
-2.0
-1.0
0
0.5
Placebo-Controlled
Trials
Exenatide-
10 g bid
Placebo
Exenatide
10 g bid
Data on file. Amylin Pharmaceuticals; DeFronzo et al.
Diabetes Care.2005;28:1092-1100.
34

Thyroid: No Signal With Liraglutide
Out to 104 Weeks
Center for Drug Evaluation and Research. Application Number: 22-341. NDA for Victoza (Liraglutide [rDNA]) Injection. Novo Nordisk, Inc.
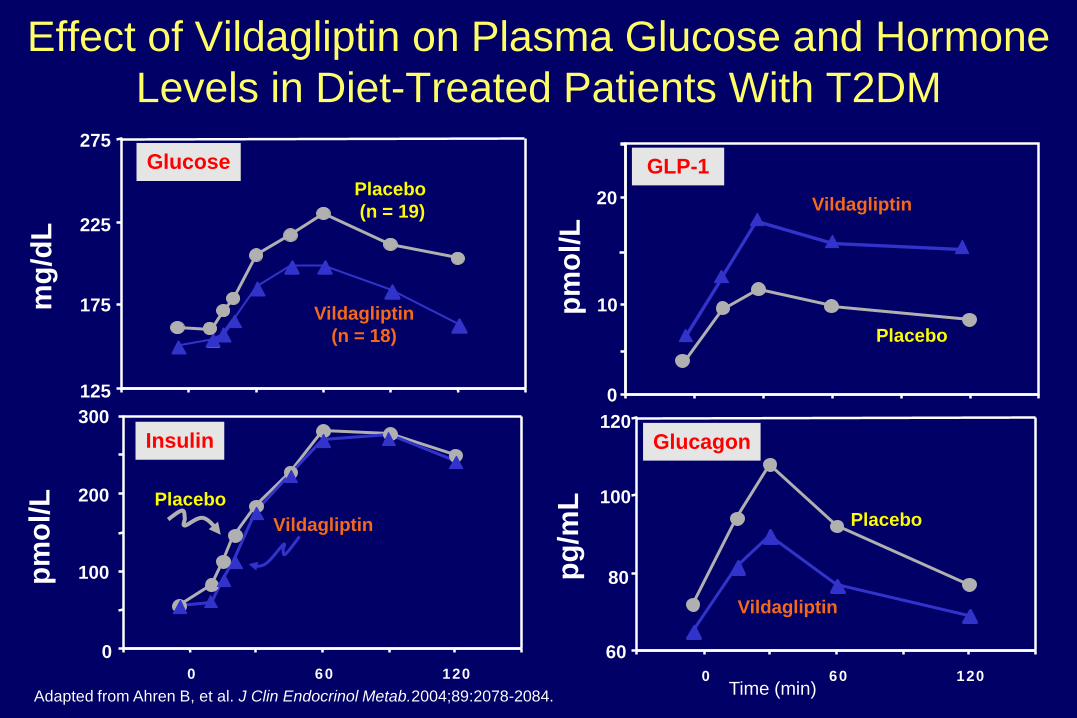
Adapted from Ahren B, et al. J Clin Endocrinol Metab.2004;89:2078-2084.
Effect of Vildagliptin on Plasma Glucose and Hormone
Levels in Diet-Treated Patients With T2DM
Time (min)
00 60 120
125
275
Glucose
Insulin
Vildagliptin
(n = 18)
Placebo
(n = 19)
Vildagliptin
Placebo
pm
ol/L
mg
/dL
60
80
100
120
0 60 120
GLP-1
Glucagon
0
10
20
Placebo
pm
ol/L
pg
/mL
Vildagliptin
Placebo
Vildagliptin
175
225
100
200
300
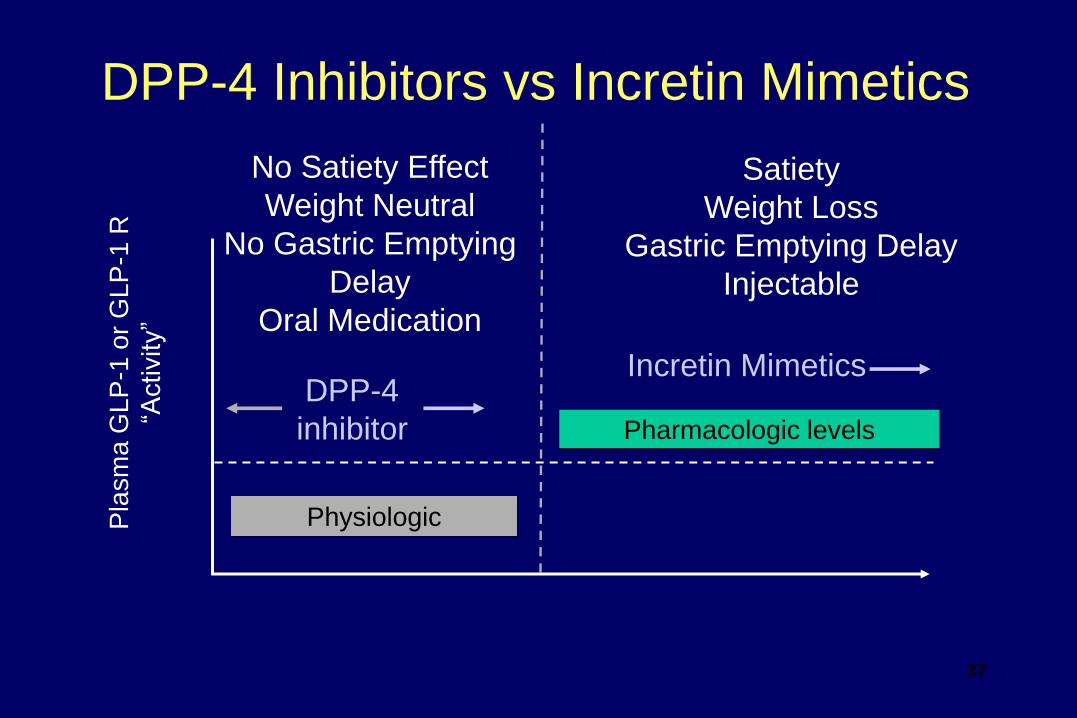
Physiologic
Pharmacologic levels
DPP-4
inhibitor
Incretin Mimetics
Pla
sm
a G
LP
-1 o
r G
LP
-1 R
“Activity”
Satiety
Weight Loss
Gastric Emptying Delay
Injectable
No Satiety Effect
Weight Neutral
No Gastric Emptying
Delay
Oral Medication
DPP-4 Inhibitors vs Incretin Mimetics
37
IncreasedHGP
Hyperglycemia
ETIOLOGY OF T2DM
DEFN75-3/99 Decreased GlucoseUptake
Impaired InsulinSecretion Increased Lipolysis
HYPERGLYCEMIA
DecreasedIncretin Effect
Decreased InsulinSecretion
Increased
HGP
Islet–a cell
IncreasedGlucagonSecretion
OMINOUS OCTET
IncreasedLipolysis
Increased
Glucose
Reabsorption
NeurotransmitterDysfunction
Decreased Glucose
Uptake
38Reprinted with permission from DeFronzo RA. Diabetes.
2009;58:773-795.
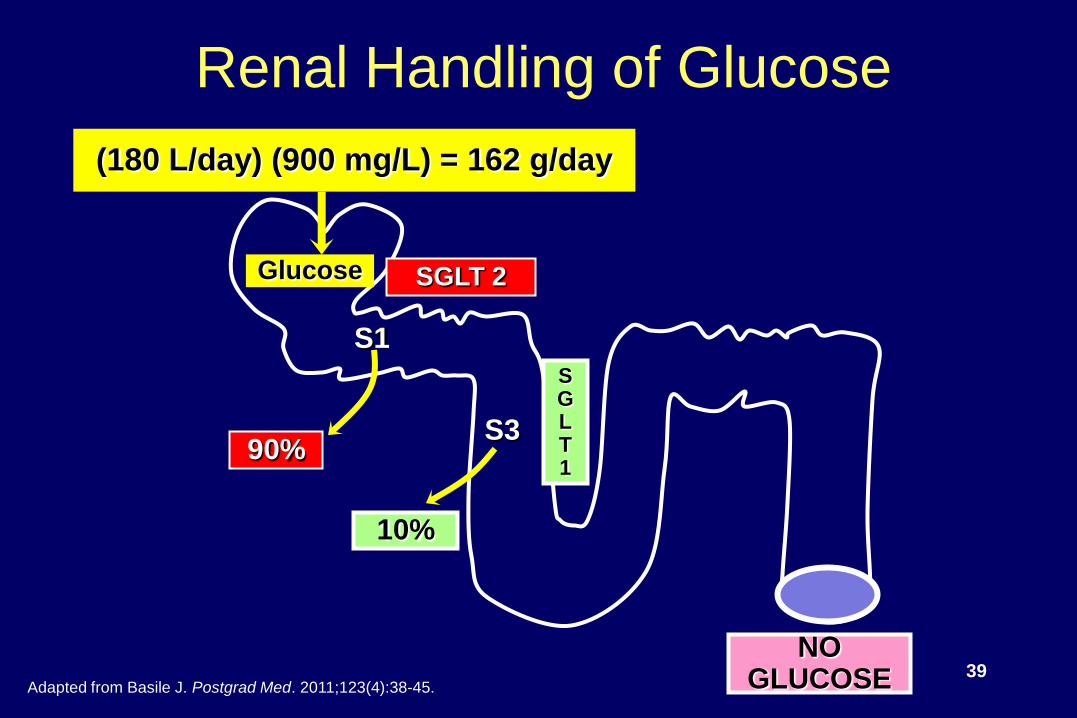
SGLT1
SGLT 2
Renal Handling of Glucose
(180 L/day) (900 mg/L) = 162 g/day
10%
90%
Glucose
NOGLUCOSE
S1
S3
39Adapted from Basile J. Postgrad Med. 2011;123(4):38-45.
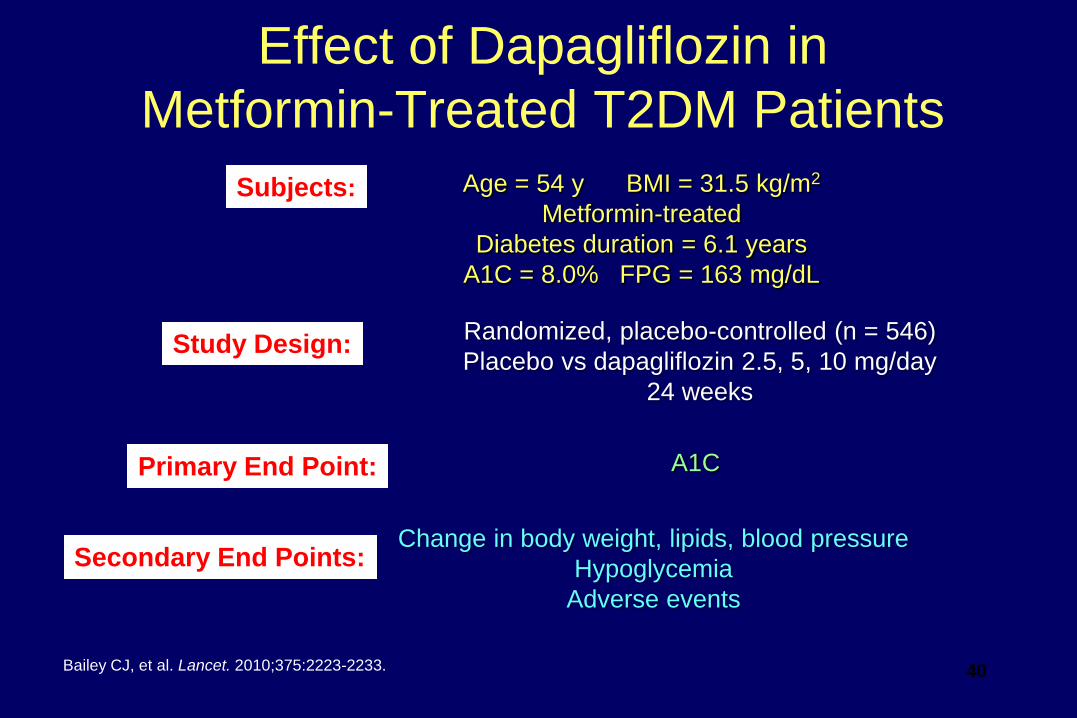
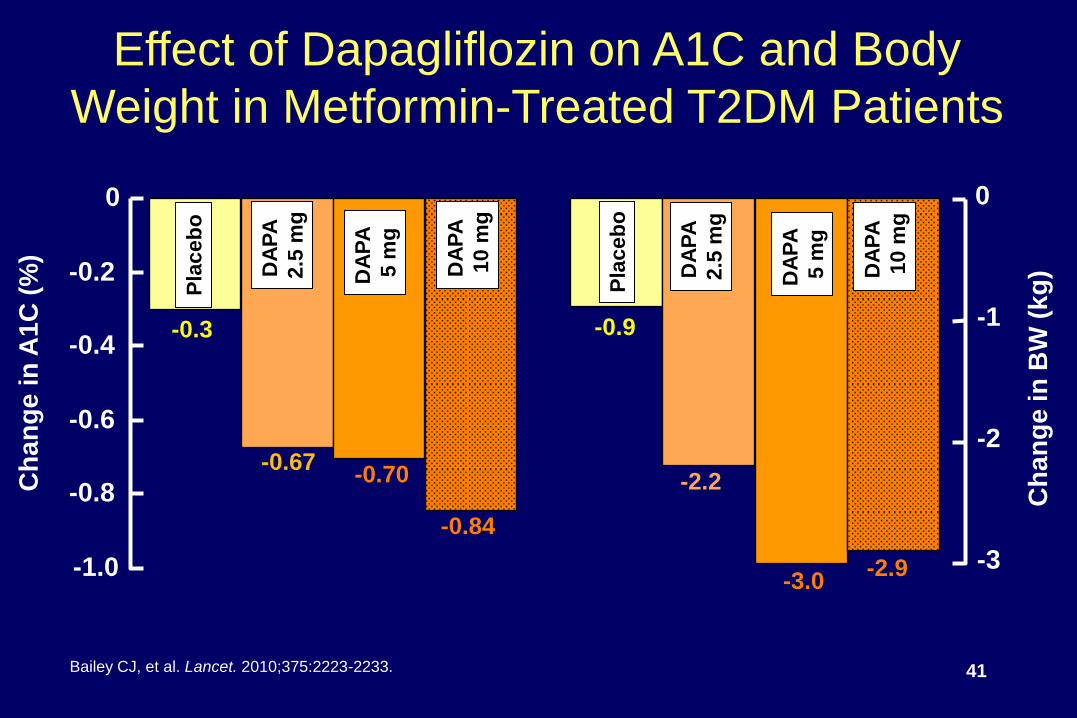
Effect of Dapagliflozin in
Metformin-Treated T2DM Patients
Bailey CJ, et al. Lancet. 2010;375:2223-2233.
Age = 54 y BMI = 31.5 kg/m2
Metformin-treated
Diabetes duration = 6.1 years
A1C = 8.0% FPG = 163 mg/dL
Subjects:
Randomized, placebo-controlled (n = 546)
Placebo vs dapagliflozin 2.5, 5, 10 mg/day
24 weeks
Study Design:
A1CPrimary End Point:
Change in body weight, lipids, blood pressure
Hypoglycemia
Adverse events
Secondary End Points:
40
C
ha
ng
e in
A1
C (
%)
Pla
ceb
o
-0.3
DA
PA
2.5
mg
-0.67-0.70
-0.84
DA
PA
5 m
g
DA
PA
10 m
g
-1.0
-0.8
-0.6
-0.4
-0.2
0
Effect of Dapagliflozin on A1C and Body
Weight in Metformin-Treated T2DM Patients
Ch
an
ge
in
BW
(k
g)
Pla
ceb
o
-0.9
DA
PA
2.5
mg
DA
PA
5 m
g
DA
PA
10 m
g
-3
-2
-1
0
-2.2
-3.0-2.9
Bailey CJ, et al. Lancet. 2010;375:2223-2233. 41
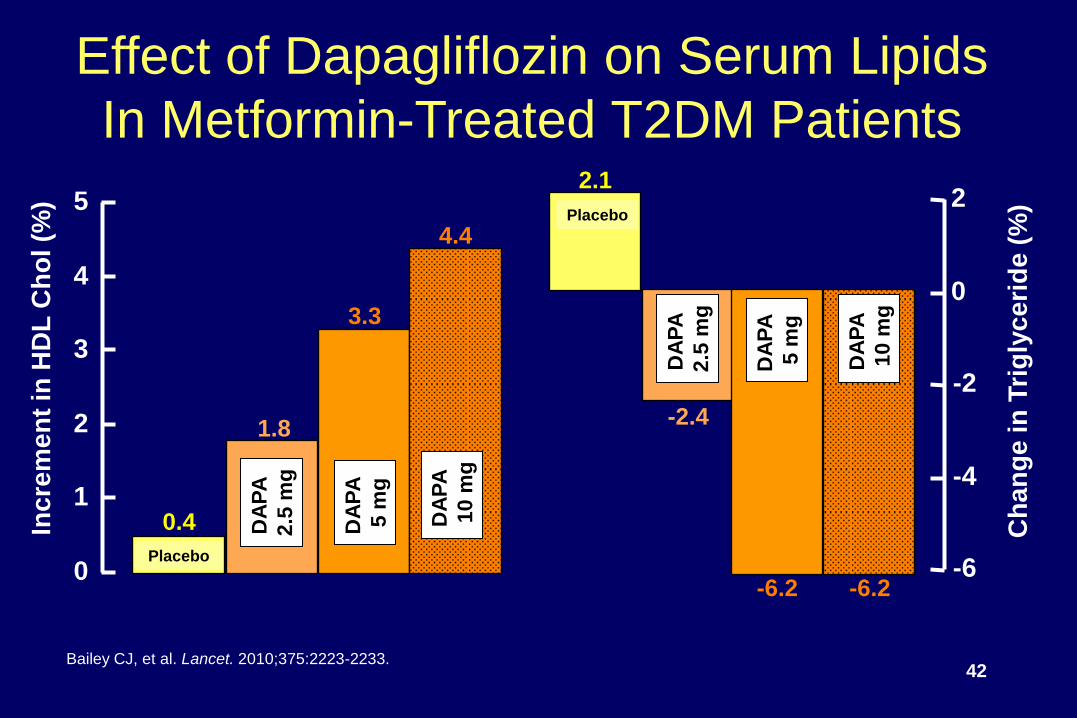
Effect of Dapagliflozin on Serum Lipids
In Metformin-Treated T2DM Patients
0
1
2
3
4
5
Inc
rem
en
t in
HD
L C
ho
l (%
)
0.4 DA
PA
2.5
mg
1.8
3.3
4.4
DA
PA
5 m
g
DA
PA
10 m
g
Placebo-6
-4
-2
0
22.1
DA
PA
2.5
mg
DA
PA
5 m
g
DA
PA
10 m
g
-2.4
-6.2 -6.2
Placebo
Ch
an
ge
in
Tri
gly
ce
rid
e (
%)
Bailey CJ, et al. Lancet. 2010;375:2223-2233.42
-5
-4
-3
-2
-1
0
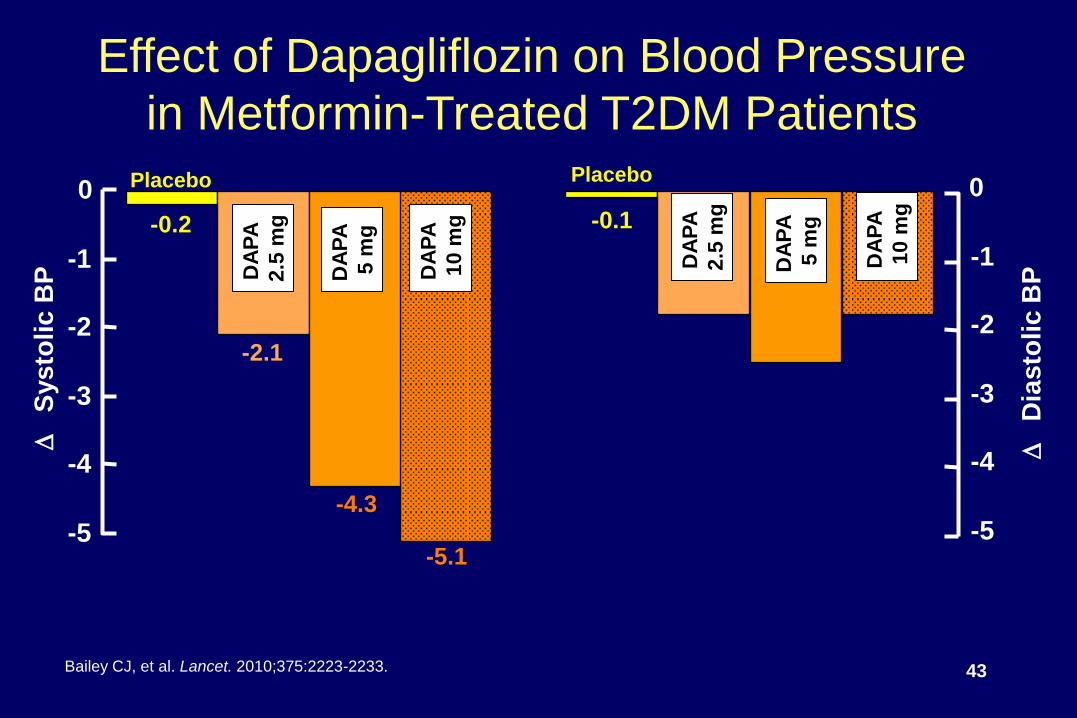
Effect of Dapagliflozin on Blood Pressure
in Metformin-Treated T2DM Patients
Bailey CJ, et al. Lancet. 2010;375:2223-2233.
D
Sys
tolic
BP
D
Dia
sto
lic
BP
-5
-4
-3
-2
-1
0Placebo
-0.2
Placebo
-0.1
DA
PA
2.5
mg
-2.1
-4.3
-5.1
DA
PA
5 m
g
DA
PA
10 m
g
DA
PA
2.5
mg
DA
PA
5 m
g
DA
PA
10 m
g
43
Safety Considerations
● Urinary tract infection
● Intravascular volume depletion (osmotic diuresis)
● Electrolyte imbalance (Na+, K+, Ca++, PO43-)
● Nephrotoxicity (AGEs)
● Nocturia
● Drug-drug interactions
44
Unanswered Questions
About SGLT2 Inhibition
Weight May wane over time loss
Safety and The long-term safety of this class
tolerability remains to be proven
Risk of genitourinary infections may limit
use in some patients
Cancer risk must be negative
Renal Efficacy wanes as eGFR declines
impairment
45
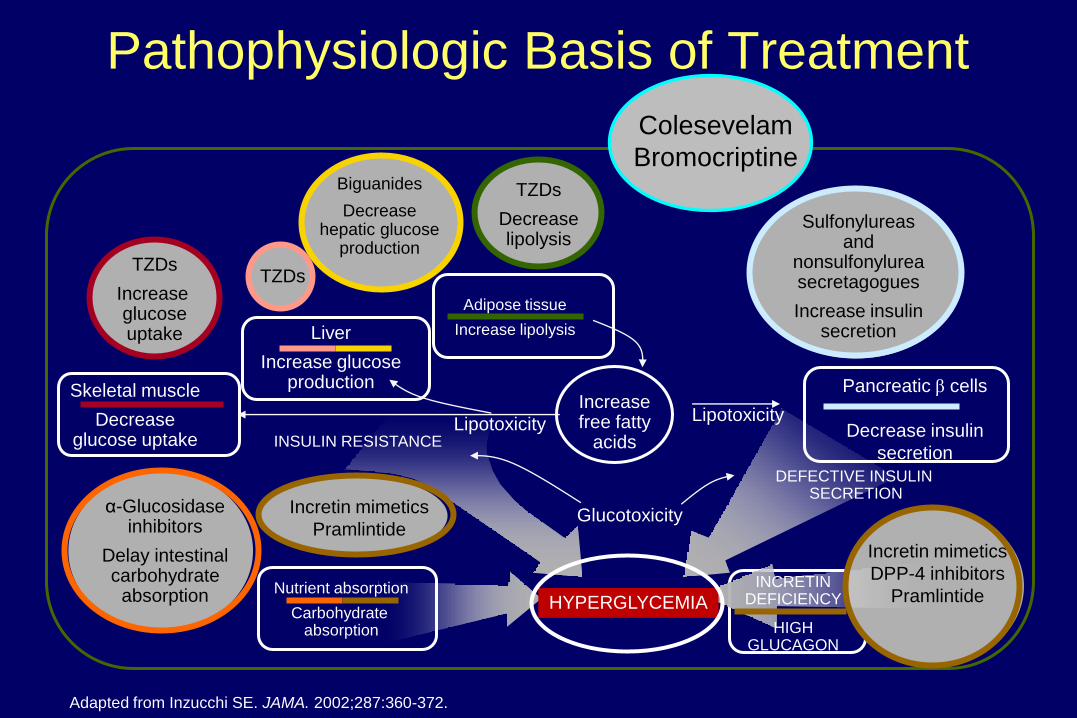
Pathophysiologic Basis of Treatment
Adapted from Inzucchi SE. JAMA. 2002;287:360-372.
Incretin mimetics
Pramlintide
Nutrient absorption
Carbohydrate absorption
INCRETIN DEFICIENCY
HIGH GLUCAGON
Incretin mimetics
DPP-4 inhibitors
Pramlintide
TZDs
Increase glucoseuptake
TZDs
Decreaselipolysis
Adipose tissue
Increase lipolysis
TZDs
Increasefree fatty
acids
Pancreatic β cells
Decrease insulin
secretion
Sulfonylureasand
nonsulfonylureasecretagogues
Increase insulinsecretion
HYPERGLYCEMIA
α-Glucosidaseinhibitors
Delay intestinalcarbohydrate
absorption
Liver
Increase glucoseproductionSkeletal muscle
Decreaseglucose uptake INSULIN RESISTANCE
Glucotoxicity
LipotoxicityLipotoxicity
DEFECTIVE INSULIN SECRETION
Biguanides
Decreasehepatic glucose
production
Colesevelam
Bromocriptine
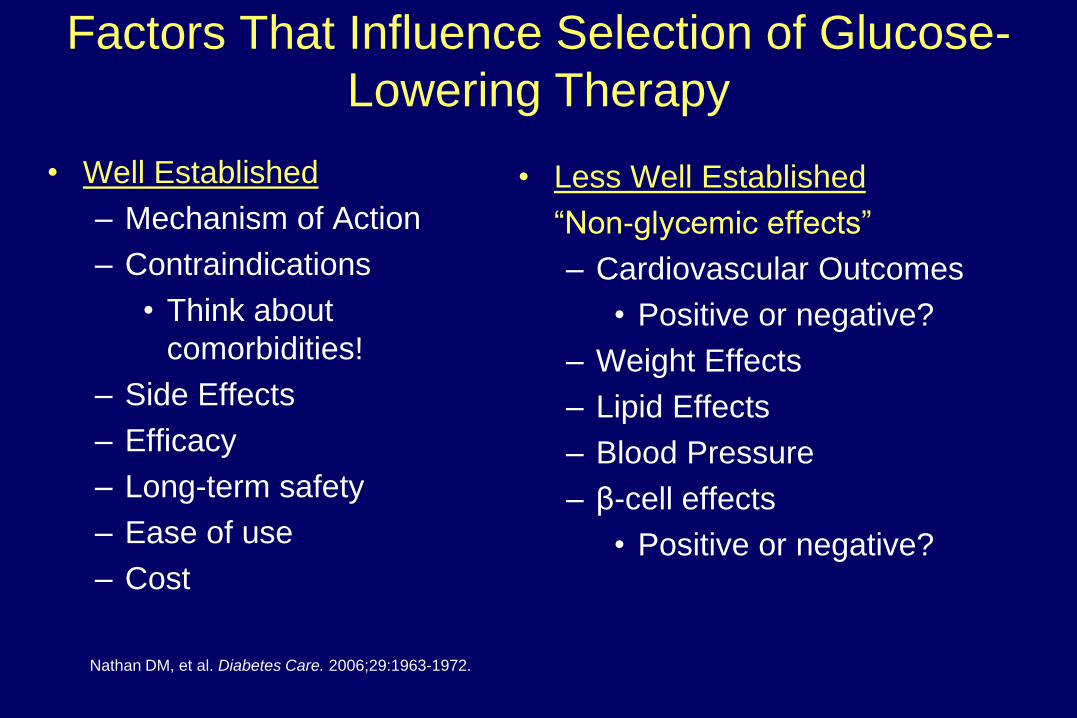
Factors That Influence Selection of Glucose-
Lowering Therapy
• Well Established
– Mechanism of Action
– Contraindications
• Think about
comorbidities!
– Side Effects
– Efficacy
– Long-term safety
– Ease of use
– Cost
• Less Well Established
―Non-glycemic effects‖
– Cardiovascular Outcomes
• Positive or negative?
– Weight Effects
– Lipid Effects
– Blood Pressure
– β-cell effects
• Positive or negative?
Nathan DM, et al. Diabetes Care. 2006;29:1963-1972.
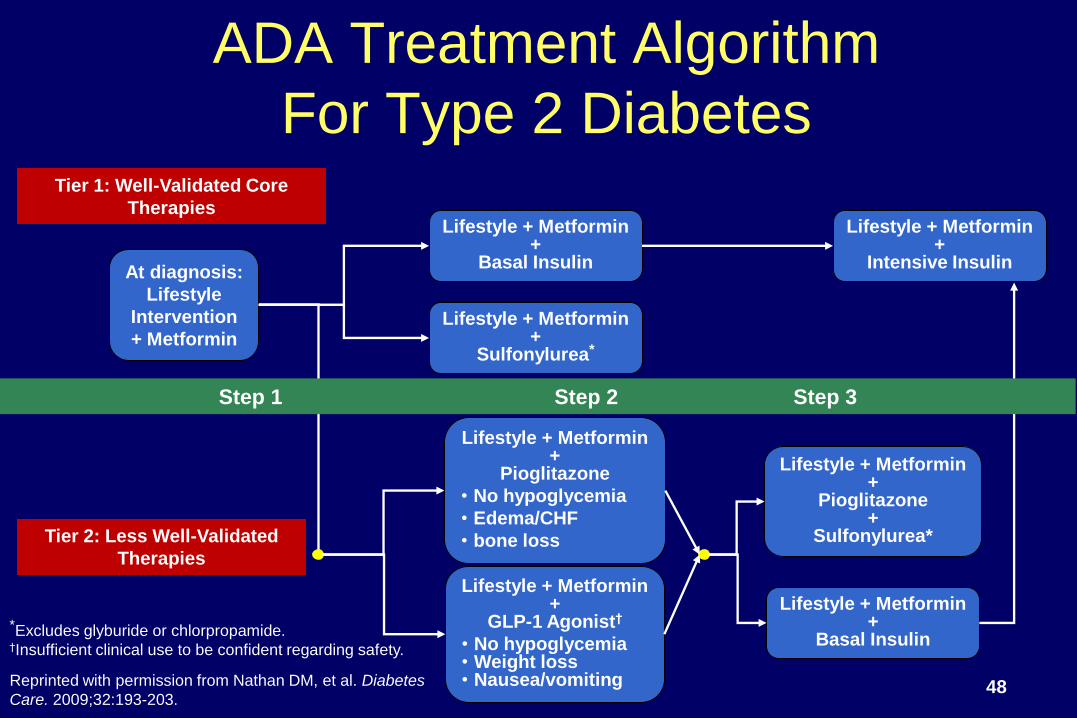
ADA Treatment Algorithm
For Type 2 Diabetes
Reprinted with permission from Nathan DM, et al. Diabetes
Care. 2009;32:193-203.
Tier 1: Well-Validated Core
Therapies
Tier 2: Less Well-Validated
Therapies
At diagnosis:
Lifestyle
Intervention
+ Metformin
Lifestyle + Metformin+
Basal Insulin
Lifestyle + Metformin+
Sulfonylurea*
Lifestyle + Metformin+
Intensive Insulin
Lifestyle + Metformin+
Pioglitazone
• No hypoglycemia
• Edema/CHF
• bone loss
Lifestyle + Metformin+
GLP-1 Agonist†
• No hypoglycemia• Weight loss• Nausea/vomiting
Lifestyle + Metformin+
Pioglitazone+
Sulfonylurea*
Lifestyle + Metformin+
Basal Insulin*Excludes glyburide or chlorpropamide.†Insufficient clinical use to be confident regarding safety.
Step 1 Step 2 Step 3
48
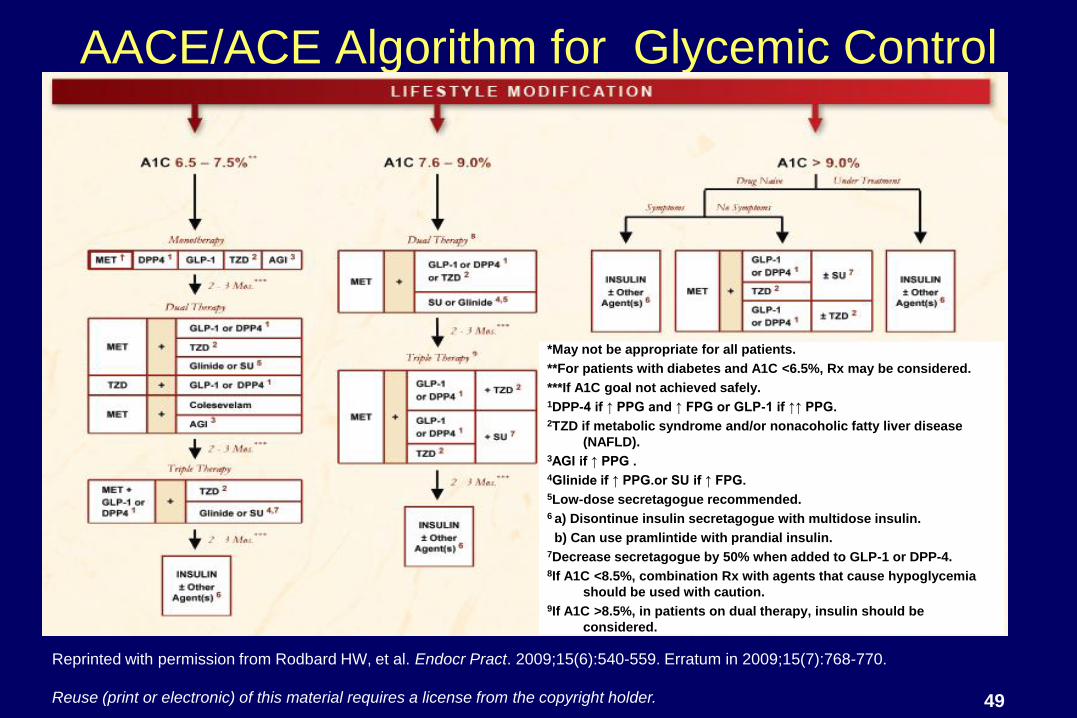
AACE/ACE Algorithm for Glycemic Control
Reprinted with permission from Rodbard HW, et al. Endocr Pract. 2009;15(6):540-559. Erratum in 2009;15(7):768-770.
Reuse (print or electronic) of this material requires a license from the copyright holder.
*May not be appropriate for all patients.
**For patients with diabetes and A1C <6.5%, Rx may be considered.
***If A1C goal not achieved safely.1DPP-4 if ↑ PPG and ↑ FPG or GLP-1 if ↑↑ PPG.2TZD if metabolic syndrome and/or nonacoholic fatty liver disease
(NAFLD).3AGI if ↑ PPG .4Glinide if ↑ PPG.or SU if ↑ FPG. 5Low-dose secretagogue recommended.6 a) Disontinue insulin secretagogue with multidose insulin.
b) Can use pramlintide with prandial insulin.7Decrease secretagogue by 50% when added to GLP-1 or DPP-4.8If A1C <8.5%, combination Rx with agents that cause hypoglycemia
should be used with caution.9If A1C >8.5%, in patients on dual therapy, insulin should be
considered.
49
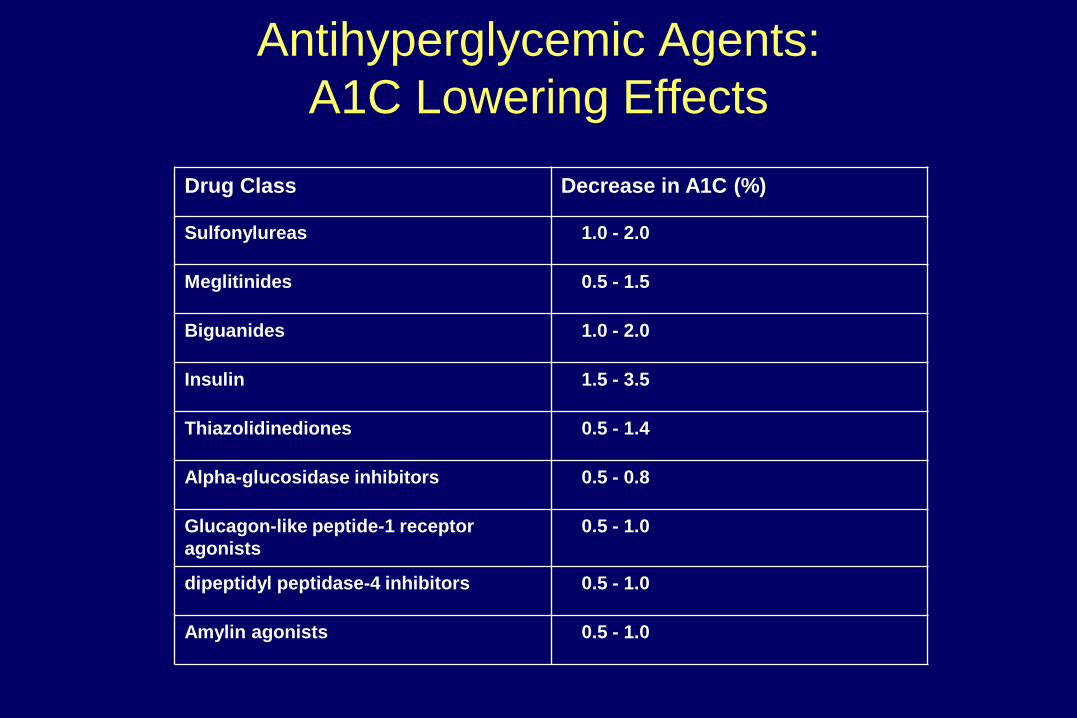
Antihyperglycemic Agents:
A1C Lowering Effects
Drug Class Decrease in A1C (%)
Sulfonylureas 1.0 - 2.0
Meglitinides 0.5 - 1.5
Biguanides 1.0 - 2.0
Insulin 1.5 - 3.5
Thiazolidinediones 0.5 - 1.4
Alpha-glucosidase inhibitors 0.5 - 0.8
Glucagon-like peptide-1 receptor
agonists
0.5 - 1.0
dipeptidyl peptidase-4 inhibitors 0.5 - 1.0
Amylin agonists 0.5 - 1.0

Summary• Multiple drugs are likely necessary to address the underlying
abnormalities
– Brain: amylinomimetics, GLP-1 agonist, dopamine agonist
– Fat: thiazolidinediones (TZDs)
– Liver and muscle: Metformin and TZDs but HGP can be reduced
by ―mass action‖ through increased insulin
– Glucagon: GLP-1 agonist, DPP-4 inhibitors, amylinomimetics
– Insulin: Insulin, sulfonylureas, meglitinides, DPP-4 inhibitors, and
GLP-1 agonists
– Incretins: GLP-1 agonists and DPP-4 inhibitors,
alpha glucosidase inhibitors?, bile acid sequestrants?
– Renal glucose absorption: SGLT2 inhibitors (several being
developed)51
Targeted Pharmacotherapy
Summary
(1) Will require multiple drugs in combination to
correct multiple pathophysiologic defects
(2) Should be based upon known pathogenic
abnormalities, and NOT simply on the reduction in
A1C
(3) Must be started early in the natural history of
T2DM, if progressive β-cell failure is to be
prevented
52
53
Thank You!





























