Embed Size (px)
Citation preview

Promoting access to hepatitis C testing and treatment services
Philippa Easterbrook Global Hepatitis Programme
.

WHO global health sector strategy on viral hepatitis 2016–2021. Available at: http://www.who.int/hepatitis/strategy2016-2021/ghss-hep/en/ (accessed March 2018).
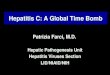
WHO Viral Hepatitis Elimination Targets: 2016
2
New
Infe
ctions a
nd D
eath
s (
Mill
ions)
2015 2020 2025 2030
10%
reduction
65%
reduction
0
0.5
1.0
1.5
2.0
2015 2020 2025 2030
30%
reduction90%
reduction
0
1.0
3.0
2.0
4.0
5.0
7.0
6.0
8.0
9.0
10.0
65% Reduction in Deaths from
Chronic HBV and HCV90% Reduction in New Cases of
Chronic HBV and HCV Infection
1.4 million deaths (in 2015) to
under 500,000 deaths (by 2030)6–10 million (in 2015) to 900,000 infections (by 2030)
95% decline in HBV infections
80% decline in HCV infections
DeathsNew infections
Roadmap to elimination of hepatitis as a public health threat

.
Impact targets consistent with scaling up six key intervention areas towards universal access
Global Health Sector Strategy for Viral Hepatitis, 2016

4
Cascade of care for HCV infection, WHO region 2016 Major testing and treatment gap
Majority of 71 m infected persons remain undiagnosed (80% testing gap)
1.76 million started HCV treatment in 2016 and 1.1 million in 2015 (75% treatment gap)
Source – WHO (Center for Disease Analysis )

.
Topic Recommendation
Who to test? Focused testing for most affected populations* , those with clinical suspicion of
chronic viral hepatitis, family members/children, healthcare workers.
General population testing: In settings with ≥2% or ≥5% (intermediate/high) HBsAg or HCV Ab prevalence.
Birth Cohort testing (HCV): where specific identified birth cohorts of older persons at higher risk of HCV infection
How to test? A single serological assay (EIA or RDT) that meets minimum performance standards with prompt viral load testing + linkage to care
Confirmation of HCV viraemia
Nucleic acid testing (NAT) (quantitative or qualitative RNA) or core HCV antigen assay, with comparable clinical sensitivity
Promoting uptake and linkage
Use of DBS specimens for virology ± serology On-site or immediate RDT testing with same day results Trained peer and lay health workers Clinician reminders to prompt provider initiated, facility-based testing Testing as part of integrated services at a single facility
WHO Hepatitis testing guideline recommendations 2017
* PWID, people in prisons, MSM, sex workers, HIV-infected, tattoos, transfusions, some migrant pops from endemic countries, children of HBV/HCV +ve mothers

Implement Good Practice Principles for Simplified Service Delivery
1. Guidelines for the Care and Treatment of Persons Diagnosed with Chronic Hepatitis, WHO 2018
1. Simple and standard algorithms across the continuum of care.
2. Strengthening the linkage from testing to care.
3. Integration of hepatitis testing, care and treatment with other
services.
4. Decentralized testing and treatment.
5. Task-shifting to support decentralized care.
6. Engagement with community.
7. Efficient procurement and supply management of quality
medicines and diagnostics.
8. Data systems to monitor the quality of care and coverage
Service delivery in specific populations
• Persons who inject drugs
• People in prisons and other closed settings
• MSM and sex workers
• Adolescents and Children
• Migrant/indigenous populations
• Pregnant women

Use of simplified and standardized algorithms

Simplifying Case-FindingWho to test and Where to test?

New WHO Evidence: Full decentralization of testing and treatment increased uptake of testing, linkage and treatment, and achieved comparable SVR12
Decentralised testing and treatment
140 studies; 33 countries. High Income countries- 120 (86%),
LMIC- 20 (14%)

And emerging evidence for…
Decentralised viraemia testing and treatment
Strengthening linkage from testing to treatment
WHO Recommended Strategies to Strengthen testing uptake and linkage to care 2
1. WHO Consolidated HIV Guidelines, 2016; 2. WHO Guidelines for the care and treatment of HCV, 2018; Shiha et al. 2018
1. Provision of hepatitis testing and treatment as part of integrated services e.g. harm reduction sites, ART clinics.
2. On-site rapid testing with same-day results.
3. Immediate or Reflex laboratory based nucleic acid testing
4. Clinician reminders to prompt provider initiated, facility testing.
5. Dried blood spots specimens for NAT ±serology
6. Trained peer or lay health worker support in community based settings.
7. Providing assistance with transportation±

03/07/2020 | Title of the presentation 11
Diagnostic Innovations and Opportunities
1. Role of point-of-care HCV viral load in improving linkage
2. Core Antigen RDT for confirmation of viraemic infection
3. Dried blood spots specimens for NAT ±serology (manafacturers protocols)
4. HCV self-testing to improve testing uptake
5. “Combo” RDT for HCV Ab, HBsAg, HIV and syphilis
6. Diagnostic integration
7. Use of integrated multi-disease platforms (HIV, HCV RNA and HBV DNA) (centralized/decentralised)
Finger-prick
Minivette capillary tube
Single-use test cartridge GeneXpert machine
Build on substantial existing lab and diagnostics capacity: Multiplatform testing (HIV/TB)

.
Different approaches to implement simplified service delivery models to achieve elimination
• Micro-elimination projects in specific populations (prisoners, PWID, HIV-infected)
• Rural setting/gen population: Comprehensive prevention, test-and- treat model for high prevalence rural setttings
• Hard to reach: Mobile/Same-Day HCV + HBV test and treat
• Model for cities/urban settings?
• Role of Self-testing

13
Example 1 - HCV Elimination models for rural populations
High coverage across HCV cascade
• Treatment coverage and cure of85% of estimated 17137 infectedvillagers aged 12-80 years across73 villages.
• 90% reduction in incidence and transmission
Shiha et al, J Hepatol 2019

Example 2- Model for hard-to-reach populationsPilot Study of Mobile Same-Day HCV/HBV Test and Treat in Egyptian Village

15
Acknowledgements
WHO HQ (Niklas Luhman, Fuqiang Cui, Yvan Hutin)
WHO Regional office (Antons Mozalevskis, LeandroSereno, Polin Chan, Fumni Lesi, Briget Mugisa, BB Rewari)
Other: Gamal Shiha, Rehham Soliman, Nabiel Mikahil(ELRIAH and Mansoura University)