Embed Size (px)
Citation preview

Overview of biosimilar policies across 9 major markets in the battle to control healthcare sustainability
Global biosimilarpolicy comparison

Global biosimilar policy comparison
1
Table of contents I. Introduction .................................................................................................................... 3
1. Goal .......................................................................................................................... 3 2. Research team .......................................................................................................... 3 3. Data sources ............................................................................................................. 3 4. Background ............................................................................................................... 3
4.1. Biologic medicines .......................................................................................................... 3 4.2. Challenges for manufacturers .......................................................................................... 5 4.3. Challenges for policy makers ........................................................................................... 5
5. Summary of results ................................................................................................... 6 5.1. Current biosimilar penetration in each country .................................................................. 6 5.2. Major biosimilar products market-in ................................................................................. 7 5.3. Biosimilar pricing and reimbursement............................................................................... 7
6. Takeaways by country ............................................................................................... 8 6.1. EU ................................................................................................................................ 8 6.2. UK ................................................................................................................................ 8 6.3. Germany ....................................................................................................................... 8 6.4. France ........................................................................................................................... 8 6.5. Sweden ......................................................................................................................... 8 6.6. Norway ......................................................................................................................... 8 6.7. United States ................................................................................................................. 9 6.8. Canada ......................................................................................................................... 9 6.9. Australia ....................................................................................................................... 9 6.10. South Korea ................................................................................................................... 9
7. Acknowledgements ................................................................................................... 9
II. Research for major countries ......................................................................................... 10 1. UK .......................................................................................................................... 10
1.1. Current healthcare landscape ........................................................................................ 10 1.2. Market for pharmaceuticals ........................................................................................... 11 1.3. Market for biosimilars ................................................................................................... 14 1.4. Legal framework for biosimilars ..................................................................................... 15 1.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 17
2. Germany ................................................................................................................. 19 2.1. Current healthcare landscape ........................................................................................ 19 2.2. Market for pharmaceuticals ........................................................................................... 20 2.3. Market for biosimilars ................................................................................................... 22 2.4. Legal framework for biosimilars ..................................................................................... 24 2.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 26
3. France .................................................................................................................... 28 3.1. Current healthcare landscape ........................................................................................ 28 3.2. Market for pharmaceuticals ........................................................................................... 29 3.3. Market for biosimilars ................................................................................................... 32 3.4. Legal framework for biosimilars ..................................................................................... 34 3.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 35
4. Sweden ................................................................................................................... 36 4.1. Current healthcare landscape ........................................................................................ 36 4.2. Market for pharmaceuticals ........................................................................................... 37 4.3. Market for biosimilars ................................................................................................... 39 4.4. Legal framework for biosimilars ..................................................................................... 40 4.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 41
5. Norway ................................................................................................................... 43 5.1. Current healthcare landscape ........................................................................................ 43 5.2. Market for pharmaceuticals ........................................................................................... 44 5.3. Market for biosimilars ................................................................................................... 47 5.4. Legal Framework for biosimilars ..................................................................................... 48 5.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 49

Global biosimilar policy comparison
2
6. United States .......................................................................................................... 50 6.1. Current healthcare landscape ........................................................................................ 50 6.2. Market for pharmaceuticals ........................................................................................... 51 6.3. Market for biosimilars ................................................................................................... 53 6.4. Legal framework for biosimilars ..................................................................................... 54 6.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 57
7. Canada ................................................................................................................... 59 7.1. Current healthcare landscape ........................................................................................ 59 7.2. Market for pharmaceuticals ........................................................................................... 60 7.3. Market for biosimilars ................................................................................................... 61 7.4. Legal framework for biosimilars ..................................................................................... 63 7.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 64
8. Australia ................................................................................................................. 67 8.1. Current healthcare landscape ........................................................................................ 67 8.2. Market for pharmaceuticals ........................................................................................... 68 8.3. Market for biosimilars ................................................................................................... 70 8.4. Legal framework for biosimilars ..................................................................................... 70 8.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 73
9. South Korea ............................................................................................................ 76 9.1. Current healthcare landscape ........................................................................................ 76 9.2. Market for pharmaceuticals ........................................................................................... 77 9.3. Market for biosimilars ................................................................................................... 78 9.4. Legal framework for biosimilars ..................................................................................... 80 9.5. Additional factors and initiatives impacting the growth of biosimilars ................................ 81
III. Appendices .................................................................................................................... 83 1. Glossary ................................................................................................................. 83
IV. References .................................................................................................................... 86

Global biosimilar policy comparison
3
I. Introduction
1. Goal This study provides a strategic report on the market situation and healthcare policy of biosimilars in nine countries: the UK, France, Germany, Sweden, Norway, the United States, Canada, South Korea and Australia.
We give an overview of the healthcare system and pharmaceuticals market of each country, and then dive into specific issues of biologics, generics and biosimilars.
2. Research team EY Japan: Tetsuro Sano, Motohiro Aoki, Martin Killmann, Mitsuhiro Nagano
EY GDS (Global Delivery Service): Tanushree Jain, Stavita Bali, Abhimanyu Roy, Shraddha Arora; Namrita Negi
EY Country Expertise: Carlo Verri, Alexandra Baxter, Andrew Mina, Rikke Skyttersæter Iversen, Fanny Holgersson, Dhongjae Koo, Jean-Hugues Fournier, Gulraiz Khan
3. Data sources The search strategy used free search terms on the following websites and databases:
• The International Society for Pharmacoeconomics and Outcomes Research (ISPOR) (https://www.ispor.org/)
• Health Technology Assessment International (HTAi) websites for conference abstracts (https://www.htai.org/)
• BMI Research Report (https://www.bmiresearch.com/) • WHO, UN and OECD publications and statistical data • Government, healthcare administration and public healthcare system publications • Pharmaceutical industry organizations • MEDLINE (PubMed) (https://www.ncbi.nlm.nih.gov/pubmed) • Generics and Biosimilars initiative (GaBi) journal and website (http://www.gabionline.net/)
This review was completed through primary research and additional searches in National Health Authorities and Parliament websites, Google, and Google Scholar, as well as grey literature.
4. Background
4.1. Biologic medicines Unlike small molecule pharmaceuticals, which are created using chemical synthesis, biologics, or biopharmaceuticals, are manufactured using biological sources. Their components are isolated from living sources — human, animal, plant, fungal, or microbial. They include vaccines, blood, blood components, allergenics, somatic cells, gene therapies, tissues, and living cells used in cell therapy.
The focus of this report is a class of biologics called recombinant therapeutic proteins, which are produced using bacteria, yeasts or animal cell lines, which were modified through DNA recombination.
Major kinds of biopharmaceuticals include:
• Blood factors (Factor VIII and Factor IX) • Thrombolytic agents (tissue plasminogen activator) • Hormones (insulin, glucagon, growth hormone, gonadotropins) • Hematopoietic growth factors (Erythropoietin, colony stimulating factors) • Interferons (Interferons-α, -β, -γ) • Interleukin-based products (Interleukin-2) • Vaccines (Hepatitis B surface antigen) • Monoclonal antibodies (Various) • Additional products (tumor necrosis factor, therapeutic enzymes)
The first of these drugs entered the market in the 1980s. By 2016, they had reached 25% of global market share in terms of value. [1]
For biologics, the largest therapy areas by sales value are autoimmune diseases (20%), anti-diabetics (18%) and oncologics (15%), which together make up over half of the market compared to other fields (46%). [1]

Global biosimilar policy comparison
4
Differences between small-molecule pharmaceuticals and biologics
Category Small-molecule drug Biologic drug
Method of synthesis Chemical Living organism or cell
Structure Fully known Complex, frequently partially unknown
Susceptibility to contamination during manufacturing Low High
Sensitivity to physical factors (heat, light)
Low High
Manufacturing methods Simple, synthetic, continuous Complex, recombinant, in batches
Species for non-clinical studies Independent Specific
Immunogenicity Non-antigenic (generally) Antigenic (MW1 > 10k Da)
Absorption Rapid Slow (subcutaneous; intramuscular)
Distribution High Low
Metabolism Metabolized to active and non-active metabolites
Catabolism to amino acids similar to endogenous ones
Disposition Often target-mediated Rarely target-mediated
Pharmacokinetic profile Non-linear (often) Linear (frequently)
Half-life Short (variable) Long
Safety Toxicity (variable mechanisms) Exaggerated pharmacology
[2]
4.1.1. Biosimilars
The first patents on pioneering biologics started to expire in the 2000s, which opened the market to biosimilars, new drugs that mimic original biologic medicines. While the first expiring patents opened rather small markets, between 2015 and 2020, 7 major original medicines with over USD 5bn in sales will lose their patent protection. [3] This has created a rush in the development of biosimilars.
However, the larger size and biologic production methods of biosimilars pose a number of challenges compared to small molecule generics, making drug development longer and more costly. Finding a cell line that will reproduce an existing reference product is more time consuming developing a new product from scratch. [4]
The biological production process leads to differences in the final product, which poses a challenge in the approval process as the same clinical results are not guaranteed. The same challenges exist in ensuring consistent quality in the production process.
Over all, this creates higher entry barriers for biosimilars, compared to small molecule generics:
• Longer and costlier development process due to difficulty of creating an exact match • A challenging manufacturing process, especially in quality control • Established processes and market position of the originator medicine • A more complex regulatory approval process, with a partial need for clinical trials • No automatic substitution since different base materials and production processes lead to
differences in the overall composition of the product • Lower ability to compete on price due to higher costs compared to other generics • Intellectual property issues, such as additional patents on the manufacturing process
4.1.2. Biobetters
There is a second type of follow-on biologics, so-called biobetters where the manufacturer does not aim to create a product that is as similar as possible to the originator, but improves on the existing product in some way. These medicines need to undergo the full approval process of a new biologic, but they can also enjoy patent protection and non-patent exclusivity. One of the first such products was Amgen's Neulasta, an improved long-acting version of Amgen's Neupogen, approved in 2002. [5]
Biobetters can be seen as a defense strategy for the manufacturer of the originator drug, to take over the market with a more competitive product, even before the first biosimilars enter. [5]
1 Molecular weight (MW) in Dalton

Global biosimilar policy comparison
5
4.2. Challenges for manufacturers Complexities in development: Due to many variables influencing the manufacturing process, production results will vary between batches. Each manufacturer will have to solve these issues individually for each product. If changes occur in the molecule structure, the manufacturer has to prove that these changes are not clinically significant for each iteration. [1]
Development requirements and costs: Developing a biosimilar requires a similar skill set and manufacturing capabilities to developing a new biologic brand. In addition to development costs, they also require investment in promotional activities and patent litigation lawsuits. While there are successful smaller players, in general the field is more tempting for existing large biologics players who have the scale, market expertise and manufacturing capabilities. [1]
Uncertain market: Strong competition, slow uptake and pricing pressures have put a question mark over market opportunities for many players. [1]
Patent issues: Patent protection for biologics does not only cover the molecule, but also formulation, devices and manufacturing process. Changing the manufacturing process too far to avoid patent issues can cause the drug to be no longer truly biosimilar. [1]
Regulatory uncertainties: Biosimilar-related legislation is still an ongoing process in many countries, with different guidelines and processes in each market and only slow convergence. [1]
4.3. Challenges for policy makers Biologic medicines have seen strong demand from patients because many of them addressed previously unmet needs. However, per-patient costs are high, causing a heavy strain on the local healthcare system (or the patient’s personal finances).
One way to drive down costs is increased competition through market entry of biosimilars. However, legislators and policy makers have faced a number of challenges specific to biosimilars.
Market approval: Because biosimilars are not fully equivalent to the originator medicine, they cannot follow the established approval processes for generics. However, enforcing the same full approval process for a new biologic has proven to be a market deterrent. In this report, we look at what approval pathways the target countries have set in place specifically for biosimilars.
There have been a variety of approaches towards biosimilars, and the pathways are still evolving. The possible patterns for approval are:
• Market approval as a new biologic (despite similarities) • Market approval under the same rules as a generic (not used) • A tailored approval process for biosimilars, focusing on (1) structural similarity within natural
variability and (2) absence of meaningful clinical differences. This approach was pioneered by EMA in the EU in 2005
Pricing: When the patent for an originator runs out, and a biosimilar enters the market, prices are expected to fall. In this report, we look at what mechanisms legislators have put in place in each country to enforce price competition and price cuts. Often, these measures are in place for pharmaceutics in general, but some measures were enacted that target biosimilars specifically.
Reimbursement: High out-of-pocket costs can force a patient to abandon treatment. [6] For each of the target countries, we look at how far the insurance system covers the cost of expensive treatments such as therapies with biologics and biosimilars.
Switching and substitution: Because biosimilars are not identical to the originator, there has been resistance from physicians and patient organizations to switching existing patients to the biosimilar, or between biosimilars. However, after successful studies like NOR-SWITCH, regulators are becoming more open to the idea. [1]
A more contentious issue is substitution at the pharmacy level, which has been allowed in some areas with the requirement to inform the prescriber. Some countries, like Germany, allow the practice only between products that are produced by the same supplier (and are therefore identical).
Incentives and quotas: All policy makers have to balance the freedom of the physician to prescribe the drug that offers the best treatment option to the patient with constraints in the healthcare budget. Policy makers and payers thus adopt a number of strategies to increase biosimilar subscriptions by physicians, ranging from positive incentives like gain-share to negative incentives such as fines for not adhering to quotas.
Education towards physicians and patients: In the initial stages of biosimilar market entry, patients and physicians had strong reservations regarding the quality and interchangeability of the new market entrants. In each of the surveyed countries, legislators and industry organizations have undertaken studies and educational campaigns to address these concerns.

Global biosimilar policy comparison
6
Additional challenges for policy makers
The following issues also affect the market entry of biosimilars. However, they were not part of the scope of this report, and are therefore only touched on briefly.
IP, Patents, and Exclusivity: Biosimilar market entrants face a number of hurdles in the IP space, from initial patents on the molecule to manufacturing and delivery methods. In addition to IP rules, policy makers have to set rules on length of exclusivity for the originator, access to clinical data etc.
Labeling: Because of the inherent differences between a biosimilar and its reference biologic, there is an ongoing discussion on the details of labeling biosimilars, such as whether they should have the same INN or an INN with a suffix, whether the INN can or should be part of the brand name or not, and what information to include on the package insert. [7] [8]
Pharmacovigilance: Variance in production outcomes create a challenge for pharmacovigilance for biosimilars, and biologics in general. Different countries have enacted different rules towards batch labeling and reporting rules to support the collection of pharmacovigilance data after market entry of a new biosimilar.
Import / Export: A number of countries allow the import of brands that are approved for the domestic market to exert price pressure.
5. Summary of results
5.1. Current biosimilar penetration in each country
Country # of approved
biosimilars # of marketed
biosimilars
UK 31 [EMA] n/a2
Germany 31 [EMA] 18 [Pro Biosimilar]
France 31 [EMA] 19 [ANSM]
Sweden 31 [EMA] 13 [TLV]
Norway 31 [EMA] 12 [NoMA]
US 5 [FDA] 2 [FDA]
Canada 7 3 6
4
Australia 95 9
6
South Korea 8 [GaBI] 8 [GaBI]
(See brackets for source)
2 In the UK, medicines can be marketed directly after EMA approval.
3 Government of Canada Drug Product Database
4 Government of Canada Drug Product Database
5 Department of Health, Australia
6 Department of Health, Australia

Global biosimilar policy comparison
7
5.2. Major biosimilar products market-in
# Molecule DE FR NO SE UK US CA AU KR
1 insulin glargine ✓ ✓ ✓ ✓ ✓ Approved* ✓ ✓ ✓
2 epoetin alfa ✓ ✓ ✓ ✓ ✓ Patent expired,
but no biosimilars yet
Patent expired, but no
biosimilars yet ✓ N/A
3 follitropin alfa ✓ ✓ ✓ ✓ ✓ Patent expired,
but no biosimilars yet
Patent to expire in 2019 ✓ N/A
4 somatropin ✓ ✓ ✓ ✓ ✓ ✓** ✓ ✓** ✓
5 filgrastim ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ N/A
6 infliximab ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓
7 etanercept ✓ ✓ ✓ ✓ ✓ Approved ✓ ✓ ✓
* In the U.S., Basaglar (insulin glargine) and Omnitrope (somatropin) are not technically considered a biosimilar. ** In Australia, Omnitrope and Scitropin A (both somatropins) which are launched as biosimilar in several other
countries, were approved, but not as biosimilar because they had been authorized under prior regulatory pathway. Scitropin A is largely approved as a biosimilar in some of the Asian markets.
5.3. Biosimilar pricing and reimbursement Rules on price setting and reimbursement vary widely, and depend heavily on the national scheme for pharmaceutical pricing.
Country Biosimilar Pricing Cost to Patient Switching/Substitution
UK Set by manufacturer; Procured by NHS / CCGs PPRS rules apply
Free at point of care (except prescription charge in England) Paid by NHS / taxes
Switching Yes; Substitution No
Germany Free pricing in first year; Price group system; Rebate system to SHI
Co-payment limited to EUR 10 Surcharge if brand preferred
Substitution mandated if same manufacturing source; Regional prescription quotas
France
Originator price as limit; Mandatory price cuts; Hospital tenders; procurement at fixed price
Different co-payment levels based on needs / means
Switching allowed; Limited substitution; Excluded from mandatory INN prescriptions
Sweden Country-level tender (hospital use) In-patient cost covered by county councils
Preference for tender winner
Norway National tender for hospital use in 6 areas
Patient cost covered by Regional Health Authorities
Preference for tender winner
US Free pricing
Limited reimbursement by Medicaid / Medicare / VHA; Private health insurance required
Depends on state legislation; system still evolving
Canada Free pricing Different coverage depending on province
Switching Yes; Substitution No; Provincial level regulation
Australia
Similar to all reimbursed medicines, on patent expiry and second brand entry: a 16% price cut is enforced compared to originator on market entry. This will be increased to 25% as part of the Strategic Agreement.
Fixed co-payment; otherwise free if covered by PBS (Pharmaceutical Benefits Scheme)
Substitution for 3 biosimilars (via “a” flag) allowed on a case by case basis. 3 biosimilars are currently “a” flagged, through physician choice preserved
South Korea
Mandated price cut vs. originator (Initially 70% of originator)
Co-payment (in-hospital: 20%) Substitution prohibited

Global biosimilar policy comparison
8
6. Takeaways by country
6.1. EU The EU, and especially the European Medicines Agency (EMA) has been a major driver of biosimilar adoption by creating a single approval pathway for pharmaceuticals and adopting the first approval pathway for “similar biological medicinal products” in 2005. This pathway is valid in all EU and EEA member states, including the UK, Germany, France, Sweden and Norway, covered in this report. These rules also had a knock-on effect on other jurisdictions, with South Korea, Australia and Canada adopting similar legislation.
6.2. UK Biosimilar uptake in the UK is catching up with the high rates of generics uptake (84.3% in volume, 2014), with filgrastim (G-CSF) showing a high uptake (98%, 2015) compared to the reference product, and infliximab (80% of patients) and etanercept (58% of patients). [9]
As part of the EU (as of 2017), the marketing approval process for biosimilars through EMA is the same as in other EU countries. Biosimilars approved by EMA are available and reimbursed immediately (as long as they have the same label as the reimbursed originator)
The procurement process is carried out through regional tenders in England (4 regions), while Scotland, Wales and Northern Ireland have their own tenders. All biosimilar tenders are Framework Agreements. Decisions on which products to prescribe are made jointly by local commissioners and Hospital Trusts.
In England, the policy focus at the country level is on delivering efficiencies in medicines spend and reducing unwarranted variation between areas, as well as keeping drug prices stable via the PPRS agreement. Biosimilar uptake is driven by price competition between manufacturers, country level policies by NHS England as well as local policies set by CCGs.
6.3. Germany Like the UK, Germany has a high rate of generic uptake already (81% by volume). Adoption of biosimilars is mainly driven by the statutory health insurances within the framework of healthcare self-governance. SHIs have agreed on minimum prescription quotas for several biosimilars with the regional KV (physician associations).
This has led to high penetration for both EPO (81%, 2015) and G-CSF (78%, 2016).
Biosimilar manufacturers set their own pricing. Discounts on biosimilars give physicians an incentive to use their limited prescription budgets on biosimilars, and they gives health insurances an incentive to push adoption rates even higher. Germany also allows limited substitution of biosimilars at the pharmacy level, but only for substances provided by the same supplier.
From the industry side, Germany has a strong local presence of both innovators and generics makers, pushing both for better protection of originators and easier market access for biosimilars.
6.4. France While France has a low volume share of generics (25.9% in 2015), it has surpassed the UK in the uptake of biosimilars, with 19 approved and 14 marketed medicines, 86% (2016) uptake of G-CSF vs. originator and 45% (2015) uptake on EPO.
With a de-facto single-payer system, the French government is able to set national healthcare policy goals. To increase generics uptake, France has made INN prescriptions mandatory in 2015. However, for biologics, both INN and commercial name are required to prescribe. It allows substitution at the pharmacy level for treatment-naïve patients under conditions. Automatic substitution is not allowed.
For pricing, France has implemented mandatory price cuts for both the biosimilar and the originator at market entry of biosimilar, and a regular price re-evaluation every 1 or 2 years.
6.5. Sweden Sweden is one of the strongest adopters of biosimilars in Europe, with both EPO (94%, 2015) and G-CSF (94%, 2016) at very high adoption rates vs. their reference products.
All products that are used in hospitals are purchased through a regional tender and prescribed products are subjected to national negotiations with three parties (procurement authority, regions and manufacturers) for others, depending on the medicine/molecule.
6.6. Norway Similar to Sweden, Norway uses a tendering process to procure medicines. There are multiple tenders each year, covering the entire country.

Global biosimilar policy comparison
9
Combined with strong regulator advocacy and highly publicized studies such as NOR-SWITCH, this has led to a high uptake of biosimilars, with EPO (87%, 2015), G-CSF (86%, 2016) and Anti-TNF (82%, 2016) biosimilars dominating compared to the originator. [10]
While the winner-takes-all nature of the national tender has led to large savings for the national healthcare system, it has also been criticized by analysts Simon Kucher & Partners as “prohibiting a sustainable business” as it “offers limited sales opportunities for the remaining manufacturers, hindering competition in the long run”. [11]
6.7. United States Compared to Europe, the United States has been a slow adopter of biosimilars legislation (2010) and it has taken even longer for the first market entrant under the new rules (2015). The situation is therefore still evolving. As the largest market for pharmaceuticals, the largest market for biologics, and the largest producer, future developments in the US will have a knock-on effect on other markets.
For now, the exact future development is hard to predict, but there is no doubt that this is the market with the highest future potential for growth.
6.8. Canada Biosimilars, like other biologic drugs, follow the New Drug Submission (NDS) drug approval pathway in Canada. However, the content of the NDS has been modified to allow inclusion of biosimilar specific information. With only 7 approved biosimilars, and a mere 3.5% market share for the strongest contender group (infliximab; Inflectra), the market is still in its infancy. With a market roughly half the size of an EU big 5 nation, further fragmented into individual provinces, there is no strong national policy to drive biosimilar adoption. The pan-Canadian Pharmaceutical Alliance (pCPA) conducts joint provincial/territorial negotiations for brand name drugs in Canada to achieve greater value for publicly funded drug programs and patients. Recently, the PCPA has started to address the reimbursement process for biosimilars, recognizing the different potential for this product category.
With pharmaceuticals prices cited as one of the current issues in the healthcare system, more efforts to bring down prices of biologics can be expected going forward.
6.9. Australia Australia has followed a similar model to Europe for market approval. The Australian government has decided to encourage further biosimilars market entrants by making biosimilars for both infliximab and etanercept substitutable at the pharmacy level which was done on a case by case basis (the physician is able to override the decision to prevent substitution [12]). The Australian government has also indicated it will introduce, on a case by case basis, further biosimilar uptake drivers, including naïve prescribing and differential prescribing authority.
Market data to show the results of that policy is currently not publicly available yet, but the Australian government is positive in its expectations that these measures will result in savings for the healthcare system.
6.10. South Korea South Korea is somewhat unique among the surveyed countries in that it has prioritized industry and manufacturing incentives for makers of biosimilars, based on its strengths in generics, before taking measures to foster a domestic market for biosimilars.
Currently, the market is still in its early stages, with an estimated biosimilars uptake of under 10%. This number is expected to grow as domestic players, or domestic partners of international players, establish a stronger portfolio and market position on their home market.
7. Acknowledgements This research were conducted by EY Advisory & Consulting Co., Ltd., and funded by Pfizer Inc. and Pfizer Japan Inc.

Global biosimilar policy comparison
10
II. Research for major countries
1. UK
1.1. Current healthcare landscape The United Kingdom has a universal healthcare system, which is split for each of the four countries that make up the UK. However, unlike in many other European countries, it is primarily financed through the general taxation system and overseen by the government, without a public health insurance company as intermediary. The National Health Service (NHS) is the collective name as well as the name used individually for each of the four public health services in the United Kingdom: the National Health Service in England, NHS Scotland, NHS Wales, and Health and Social Care in Northern Ireland.
Total healthcare expenditures as a share of GDP are slightly below other comparable European countries.
1.1.1. Country data
Indicator Value Year Source
Population (Mill) 65.4 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %) 0.65 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 11.85 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 18.12% 2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 42651 2016 OECD [14]
Doctors per 10,000 people 28.06 2015 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people
8.4 2015 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 26.1 2015 OECD [16]
Healthcare expenses (% of GDP) 9.7 2016 OECD [17]
Source: UN, Dept. of Economic and Social Affairs, WHO/Europe, HlthResDB, OECD
1.1.2. Healthcare system overview
In England, the Department of Health provides stewardship for the overall health system, but day-to-day responsibility for running the healthcare system rests with a separate public body, the National Health Service (NHS) England. There are 4 regions within the NHSE (North of England, Midlands and East of England, London and South of England). After a 2012 reform, commissioning of healthcare services by the NHS is handled by over 200 local Clinical Commissioning Groups (CCGs) within the regions. [18] The reforms also established the Any Qualified Provider (AQP) program, under which NHS patients can receive care at a private facility for a number of procedures.
In Scotland, Wales and Northern Ireland, healthcare legislation has been devolved to regional parliaments, oversight is transferred to the respective Departments of Health, and day-to-day operations to a separate NHS. There have been increasing differences between the individual systems, although the general priorities remain similar. [19]
The NHS in England is two-tiered, with General Practitioners (GPs) providing primary healthcare and making referrals to further services as necessary. Hospitals then provide more specialist services, including care for patients with psychiatric illnesses, as well as direct access to Accident and Emergency (A&E) departments. GPs are either self-employed, working under contract with the NHS, or they are employees of a private clinic, or they work for a local CCG.
The NHS owns and operates hospitals, and hospital staff are NHS employees.
Community pharmacies are privately owned but have contracts with the relevant health service to supply prescription drugs.
1.1.3. Health insurance system
Because of tax-funded universal coverage, there is less incentive in the UK to purchase private health insurance, but about 15% of healthcare spending is private, either through direct payment, or a private or employer-provided health insurance. This share is smaller than in comparable economies.
Healthcare is provided free at the point of contact to NHS patients.

Global biosimilar policy comparison
11
1.1.4. Current issues in the healthcare system
Efficiency demands: Faced with increasing demand from an ageing demographic, while healthcare budgets are reduced, forced each of the four systems to increase efficiency to keep up or improve service levels.
Increasing divergence between the four national systems: After control of the NHS in Scotland, Northern Ireland and Wales was divested to regional governments and parliaments in the 1990ies and 2000s, different policy approaches and spending priorities have led to different performance levels of the healthcare systems in each of the four countries. [20]
Brexit: The UK leaving the European Union has left a number of open questions for the healthcare system, such as whether physicians from EU countries will still be allowed to practice in the UK, and what the effect on approvals for new pharmaceuticals will be.
Waiting times: Waiting times for general practitioner appointments and specialist treatments are a recurring topic in discussions about the UK Healthcare system, and a number of reforms have targeted this specific KPI.
Quality issues: A string of recent safety scandals has put the spotlight on underperforming hospitals, and a number of measures have been undertaken to address the issue.
1.2. Market for pharmaceuticals
1.2.1. Market statistics
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 45.6 BMI
World market share % 4.10% BMI
Pharmaceutical sales / capita USD 700 BMI
Pharmaceutical sales / GDP % 1.74 BMI
Pharmaceutical sales / health expenditure % 20.9 BMI
Prescription drug sales USD bn 39.9 BMI
Patented drug sales USD bn 27.9 BMI
OTC medicine sales USD bn 5.7 BMI
Generic drug sales USD bn 12.0 BMI
Share of generics (value) % 34.90% OECD
Share of generics (volume) % 84.30% OECD
Source: BMI data tool, accessed on 25 July 2017; OECD 2014 [21]
1.2.2. Legal framework
Market authorization
As in all EU countries, pharmaceuticals can either be approved EU-wide by the EMA in the Centralized Procedure, or locally in the Decentralized Procedure, Mutual Recognition Procedure, or National Procedure. [22] The EMA approval pathway is likely to end with Brexit in 2019, but details have not been specified yet.
The responsible national body for market approval is the Medicines and Healthcare products Regulatory Agency (MHRA) under the Department of Health. Medicines are available on the market immediately after approval, but to gain market share, require a positive purchasing decision by the four UK health departments and later by CCGs in England only and for Scotland, Wales and Northern Ireland alternative structures.

Global biosimilar policy comparison
12
Pharmaceuticals pricing and reimbursement
Source: European Observatory on Health Systems and Policies [23] Note: The table above only details England and Scotland, but Wales and Northern Ireland have their own reimbursement bodies, and Wales has its own HTA body.
In England, the NHS acts as a wholesale buyer for pharmaceuticals. To be funded by NHS England, some originator pharmaceutical medicines must undergo assessment by NICE, the National Institute for Health and Care Excellence. NICE performs a value-based assessment based on clinical and economic evidence (health technology appraisal - HTA). For the cost efficiency calculation, NICE takes into account QALY, or Quality adjusted life years, i.e. how much the drug is able to extend the patient’s life and / or increase life quality. [24] For other originator pharmaceuticals that are not appraised by NICE, the medicines will be appraised by the four Regional Medicines Optimisation Committees
Manufacturers can set prices freely, and the UK Government and the Association of the British Pharmaceutical Industry (ABPI) have agreed on a scheme to keep prices stable. Under the Pharmaceutical Price Regulation Scheme (PPRS), the most recent introduced in 2014, manufacturers voluntarily enter a 5-year agreement with the UK government to keep the national medicines bill capped for two years, increasing by 1.8%, 1.8% and 1.9% in the final three years of the scheme. [25]
The industry agreed to refund any government spending above the agreed cap. In 2017, the repaid amount will be 4.75%. [26]
The scheme applies to licensed and branded medicines, including branded generics (biosimilars are branded). It does not include private prescriptions, unbranded generics and OTC products.
Companies who do not enter the PPRS scheme are forced to enter a statutory agreement that includes a 15% price cut. [26]
Non-branded generics are exempt from PPRS, which has led to price competition between generic medicines and falling prices for those medicines supplied by multiple companies. However, to qualify for reimbursement generic prices have to be either negotiated between the Department of Health (DoH) and the British Generic Manufacturers Association (BGMA) (for Category M and W) or to be calculated by the NHS Business Services Authority (for Category A – most common generics) [27]
In England, NHS procurement decisions for non-specialized medicines were devolved to local Clinical Commissioning Groups (CCGs) in 2012. This has further complicated matters, as now each CCG is developing their own formulary of available reimbursed drugs. Although legally required to make NICE-approved drugs available to patients where clinically appropriate, in practice CCGs do not always make such medicines available, according to a PharmaTimes interview. [28]. Some specialized biologics, notably in oncology, are commissioned nationally by NHS England via a centrally held specialized commissioning budget.
Additionally, NHS England has introduced Regional Medicines Optimization Committees (RMOCs) in order to evaluate new medicines, which are not subject to the NICE HTA evaluation, and subsequently to produce recommendations on whether the NHS should restrict or encourage the use of certain medicines. The plans are at an early stage but it is likely that there will be one RMOC fully dedicated to the evaluation of biosimilars; biosimilars are explicitly referred to in the proposal document. [29]
In Scotland, the main task of the Scottish Medicines Consortium (SMC) is to advice NHS Boards and their Area Drug and Therapeutics Committees (ADTCs) in Scotland about the clinical and cost-
Reimbursement UK / England UK / Scotland
Involved Institution for decision
NHS England (CCG at local level or CMU at national level)
NHS Scotland (Area Drugs and Therapeutic Committee formulary)
Involved Institution for evidence assessment, appraisal and recommendation
Appraisal Committee at NICE / external HTA institutes
Scottish Medicines Committee / New Drugs Committee
Interactions AC advises NHS NDC advises NHS
Pricing Free pricing, PPRS scheme Free pricing, PPRS
Type of reimbursement list National negative list + positive list per payer (“CCG formulary”)
National negative list + positive list per payer (“area drug list”)
Reimbursement restrictions Indication, patient group, prescriber group / context of prescription
Indication, patient group, prescriber group / context of prescription
Revision of decision Regular revision (1-3 years) Revision on initiative of NHSS / AD&TC due to change of evidence

Global biosimilar policy comparison
13
effectiveness of all newly licensed medicines including new formulations of existing medicines and new indications for established products (licensed from January 2002). [30]
Patient co-payment
While Scotland, Wales and Northern Ireland have abolished co-payments for prescriptions, NHS England requires a prescription charge of GPB 8.60 per item, outside the hospital setting. Patients have the option to prepay all prescription costs for a year for flat GPB 104.00. A substantial proportion of patients are exempt from prescription fees including children, retired people, people in receipt of state benefits, women who are pregnant or who have given birth in the last year, and people with certain long-term conditions. [31]
Co-payments also apply to dental care, eye care as well as wigs and fabric supports.
Generic substitution
A principal factor in stimulating generic medicines use has been the fact that medical students are taught to prescribe by international non-proprietary name (INN) in British medical schools. In 2008, 82% of all prescription items were prescribed by INN in England. [32]
Generic prescribing by GPs has been supported by computer programs such as PRODIGY (PRescribing ratiOnally with Decision support In General practice studY) which was introduced in 2000.
In line with MHRA guidelines, all biological medicines, including biosimilar medicines, must be prescribed by brand name. This ensures that automatic substitution of a biosimilar product does not occur when the medicine is dispensed by the pharmacist and supports ongoing pharmacovigilance of individual products. Therefore, generic substitution by pharmacists is not permitted if the Brand name is written on the prescription. Pharmacists earn a fixed fee per prescription item for a minority of medicines and the difference between NHS reimbursement and the purchase price. In the case of an INN prescription, the reimbursement level is listed in Part VIII of the Drug Tariff and depends on the category in which the medicine is placed. (Note that policy guidance does not consider biosimilars as generics). [33] [34]

Global biosimilar policy comparison
14
1.3. Market for biosimilars
1.3.1. Available biosimilars
Biosimilars can be marketed freely, immediately after EMA approval, if the originator was assessed positively by NICE.
The list below includes the 10 biosimilars which are included in the British National Formulary of NHS England, however, all 31 biosimilars approved by EMA can be marketed and commissioned on the regional or local level.
Biosimilar brand name
Active substance
Company EMA authorization
date Net price7
Benepali [35] etanercept Biogen 14/01/2016 1-mL prefilled pen =GBP164
Abasaglar (prev. Abasria) [36]
insulin glargine Eli Lilly / Boehringer Ingelheim
09/09/2014 -
Bemfola [37] follitropin alfa Finox Biotech AG 27/03/2014 0.125 mL (75 units) = GBP23.50
Inflectra [38] infliximab Hospira 10/09/2013 100-mg vial = GBP377.66
Remsima [39] infliximab Napp 10/09/2013 100–mg vial = GBP377.66
Nivestim [40] filgrastim Hospira
08/06/2010 12 million-units (120 micrograms)/0.2 mL = GBP36.00
Zarzio [41] filgrastim Sandoz 06/02/2009 30 million-units (300 micrograms)/0.5 mL = GBP50.15
Ratiograstim [42] filgrastim Ratiopharm 15/09/2008 30 million-units (300 micrograms)/0.5 mL = GBP62.25
Retacrit [43] epoetin zeta Hospira 18/12/2007 1000 units = GBP5.66
Binocrit [44] epoetin alfa Sandoz 28/08/2007 1000 units = GBP4.33
Omnitrope [45] somatropin Sandoz 12/04/2006 1.5 mL (5-mg, 15-unit) cartridge = GBP73.75
Source: National Institute for Health and Care Excellence (NICE), accessed on 4 August 2017
7 Basic NHS net prices are given in the BNF to provide an indication of relative cost. Where there is a choice of suitable preparations for a particular disease or condition
the relative cost may be used in making a selection. Cost-effective prescribing must, however, take into account other factors (such as dose frequency and duration of treatment) that affect the total cost. [351]

Global biosimilar policy comparison
15
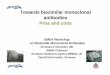
1.3.2. Biosimilars market share
Captured below is the 2016 market share of biosimilars (in comparison with the reference product, accessible market and the total market) in the product classes of EPO, G-CSF, HGH, Anti-TNF and follitropin alpha. [10]
Source: The Impact of Biosimilar Competition in Europe, IMS (sourced from a publicly available report) [10]
8
1.3.3. Market outlook
The biosimilars market in the UK is expected to exhibit high growth. Cost pressures and well-developed generics market are likely to drive the adoption of biosimilars. NICE generally recommends the lowest cost biologic to be used.
The market size (US$ million) of biosimilars in the UK is as follows:
Source: Global biosimilars market (2016-2020), Technavio [46]
1.4. Legal framework for biosimilars
1.4.1. Market approval
The UK follows a centralized regulatory pathway established by the European Medicines Agency (EMA) in 2006 (for details refer to the section on EMA’s regulatory framework on biosimilars). After EMA’s approval, the Medicines and Healthcare Products Regulatory Agency (MHRA) is responsible for the registration of the drug in the UK/ England.
The UK is currently scheduled to leave the EU in 2019. Regulations and responsibilities for the post-Brexit period have not been determined yet.
In addition to EMA’s guidance of pharmacovigilance, the MHRA has issued a drug safety update requesting that brand name and batch number should be provided when reporting a suspected adverse drug reactions to a biologic. [47]
8 EPO: epoetin; G-CSF: Granulocyte-colony stimulating factor; HGH: Human Growth Hormone; TNF: Tumor Necrosis Factor; Biosimilar vs. reference product - TD
biosimilars as % of TD reference products; Biosimilar vs. accessible market - TD biosimilars as % of TD accessible market; Biosimilar vs total market - TD biosimilars as % of TD total market
6% 3% 1%
98%86%
58%
22%11% 11%
33% 33%16%18% 17%
6%1% 1% 0%
Biosimilar vs. referenceproduct
Biosimilar vs. accessiblemarket
Biosimilar vs. total market
Biosimilar market share (% of treatment days)
EPO (2015) G-CSF (2016) HGH (2016)
Anti-TNF (2016) Follitropin alfa (2016) Insulin glargine (2016)
60.5
491.9
2015 2020E
US$ millions
CAGR: 52.1%

Global biosimilar policy comparison
16
1.4.2. Biosimilar pricing and reimbursement
England
NICE does not routinely review biosimilars. NICE can apply the guidance for the originator to the biosimilar, unless it decides that an evidence summary for a new medicine is required. Benefits and risks are inferred by the similarity to the reference medicine in terms of quality, efficacy and safety. [48] [49] [11]
The initial price of the biosimilar is set by the manufacturer. There are no defined pricing rules for originator drugs after the launch of biosimilar medicines. [27] [11] There are no specified price discount for biosimilars in the UK/ England. [49]
As per paragraph 3.19.8 of the 2014 Pharmaceutical Price Regulation Scheme (PPRS), biosimilars are subject to the PPRS rules. [50]
Scotland
Scottish Medicines Consortium (SMC) does not routinely assess biosimilars on the basis of a full submission. Biosimilars are considered ‘out of remit’ when the reference biologic has been accepted by SMC for the same indication(s) and in the same population. Full submissions for the biosimilars is required for indication(s)/populations where the reference biologic is not recommended by SMC. [51]
The table below depicts that Inflectra is recommended in more indications as compared to its reference biologic Remicade:
Approved indications Inflectra [52] Remicade [53] [54] [55] [56] [57] [58]
Rheumatoid arthritis ✓ NA
Psoriasis ✓ ✓
Psoriatic arthritis ✓ NA
Adult ankylosing spondylitis ✓ ×
Adult ulcerative colitis ✓ ×
Pediatric ulcerative colitis ✓ ✓
Adult Crohn’s disease ✓ ×
Pediatric Crohn’s disease ✓ ✓ Source: Scottish Medicines Consortium, accessed on 4 August 2017
Wales
The All Wales Medicines Strategy Group (AWMSG) does not conduct an appraisal of a biosimilar if the following conditions have been satisfied: [59]
• The reference product has been accepted by either the AWMSG or NICE for the same set of indications and population OR The reference drug was available or licensed before 1 October 2002
• The biosimilar is not priced more than the reference drug
1.4.3. Switching and substitution
Switching in all 4 countries of the UK: Physicians are allowed to switch patient’s medicines on case to case basis [60] [33]
Substitution in all 4 countries of the UK: NHS guidelines do not allow automatic substitution of biosimilars at the pharmacist level [61] [33]
1.4.4. INN prescribing
MHRA recommends that biologics, including biosimilars, should be prescribed by their brand name in the UK. [62] This is done to ensure that these products are not automatically substituted at pharmacy level, as biosimilar and reference biologic have the same international non-proprietary name (INN), but cannot be presumed to be identical in the same way as small molecule medicines. [48]

Global biosimilar policy comparison
17
1.5. Additional factors and initiatives impacting the growth of biosimilars
1.5.1. Marketing or education initiatives regarding biosimilars
The following are the initiatives taken in the UK / England to increase the awareness and education of biosimilars:
• NHS has started a program to increase confidence of clinicians and understanding of decision makers (commissioners, clinicians, pharmacists and patients) in their consideration for the appropriate use of biosimilars. This contains publication of information on biosimilars and a work program to improve education and understanding of biosimilars.
• NHS shares the experiences (real-life examples) of using biosimilars through a series presentations regarding current practice.
• MHRA, NHS England, NICE, the Royal Pharmaceutical Society and industry associations have collaborated and published a report on biosimilar medicines, entitled “What is a biosimilar medicine?” [33] The objective of this report is to provide stakeholders with the information on the appropriate use of all biological medicines, including biosimilars. [63]
• NICE has published articles such as “introducing biosimilar versions of infliximab: Inflectra and Remsima” with an objective of introducing biosimilars into care pathways safely and effectively. [48]
• The British Biosimilars Association (BBA), part of the British Generic Manufacturers Association, was set up in April 2016 to improve access to biosimilars by focusing of increasing the understanding and use of biosimilar medicines in the UK. [64]
• In 2017, Regional Medicines Optimization Committees (RMOCs) were set up, with one of the tasks being to promote the uptake of biosimilar medicines [65]
• NHS England has published a commissioning framework for biosimilars. [9]
1.5.2. Government incentives to increase biosimilar prescriptions
Incentives to doctors / hospitals / pharmacies
NHS England adopted Commissioning for Quality and Innovation (CQUIN) scheme GE3 to incentivize biosimilar uptake. Healthcare providers who achieve a set target of adopting 90% best value generic / biologic products in new patients and 80% in existing patients receive an incentive of 1% of contract value for tariff-excluded high cost drugs. [66] [67]
Local CCGs have entered gain share agreements with providers, allowing them to keep a percentage of the cost savings achieved by prescribing lower-cost medicines.
In addition, there are guidelines for prescribing biologics. For e.g., the British Society of Gastroenterology has published guidelines on the use of infliximab biosimilars for the treatment of inflammatory bowel disease. [48]
Prescription quotas
There are currently no biosimilar prescription quotas for the physicians. However, they have a budget limit for pharmaceuticals, which may encourage them to prescribe the cheapest option. [11]
1.5.3. Procurement policy
NHS procurement decisions are made via tender. In England, tenders are held at regional level and lead to framework agreements in the four NHS regions, which then inform local prescribing decisions. All biological medicines are contracted regionally by the Commercial Medicines Unit (CMU) on behalf of NHS England, under the branded clinical category tranche tendering process. [9] Local contracting processes must also take account of the unique considerations related to the use of biological medicines, including biosimilar medicines.
Scotland, Wales and Northern Ireland have separate, country-level tender mechanisms for biologics.
1.5.4. Other country-specific issues that influence the introduction and adoption of biosimilars
• Payers, i.e. the NHS bodies and CCGs, are focused on reducing the total treatment cost in the UK. Therefore, they favor the use of biosimilars. For example, the use of infliximab biosimilars is recommended for 90% of naïve patients, whereas switching existing patients from an originator to biosimilars is expected for 80% of patients under the GE3 program. [66] [68] [11]
• NICE recommends that starting of the treatment should be done with the most cost-effective option [11]

Global biosimilar policy comparison
18
1.5.5. Industry position on biosimilars
Association of the British Pharmaceutical Industry (ABPI) — the following are the recommendations made by the body on biosimilars in May 2015:
• Biosimilars should be prescribed by their brand names and not by INN • Automatic substitution is not suitable for biologics, including biosimilars. A biologic or a biosimilar,
must only be substituted under the supervision and with the consent of the physician • Patients should be completely informed about the medication given to them and should be
consulted if any medication is changed • Biosimilars should undergo appropriate health technology assessment processes • Tenders and framework contracts for biologics should not have a single product source as
precaution needs to be taken when a biologic medication of the patient is switched • Indication extrapolation for biosimilars should be evaluated by regulators on a case by case basis • A biosimilar’s summary of medicinal product characteristics (SmPC) should clearly indicate the
source of information contained within it. For e.g., relevant clinical trial data from both biosimilar and the reference biologic [69]

Global biosimilar policy comparison
19
2. Germany
2.1. Current healthcare landscape The German healthcare system gives stakeholder organizations, especially for health insurances (payers), physicians and pharmacists, strong influence and the ability to set their own policies.
As the country with the highest population, the largest market for pharmaceuticals and the biggest pharmaceutical producer in the EU, healthcare policy decisions in Germany also affect its neighboring countries.
2.1.1. Country data
Indicator Value Year Source
Population (Mill) 81.71 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %)
0.2 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 17.26 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 21.12% 2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 48,839 2016 OECD [14]
Doctors per 10,000 people 41.25 2014 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people
6.45 2014 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 81.3 2015 OECD [16]
Healthcare expenses (% of GDP) 11.3 2016 OECD [17]
Source: UN Dept. of Economic and Social Affairs, WHO and OECD
2.1.2. Healthcare system
The German healthcare system is largely governed by independent public and private entities, which are governed by a system of self-regulation that is based on direct negotiation between players such as hospitals, professional associations of doctors and nurses, pharmacists, and health insurances. Together, they are represented in the most important body, the Federal Joint Committee.
The federal government acts as a legislator, but only has a minor role as a payer. The main source of funds in the system are health insurance premiums paid by employers and insured.
Healthcare delivery is split between physicians in private, ambulatory care clinics and hospitals, with differences in how the two sectors are evaluated and paid. [70]
Primary care is provided by general practitioners (GP) in private, for-profit clinics. Patients have free choice of provider, but the statutory health insurance (SHI) only reimburses specialist visits after referral, making GPs de-facto gatekeepers.
Hospitals traditionally focus strictly on in-patient care, but roles have shifted recently towards more ambulatory care. They are usually run by the local municipality (about half of all hospital beds), universities under state ownership, religious organizations or private companies. [70]
2.1.3. Health Insurance system
Health insurance is compulsory in Germany. Most citizens are enrolled in a Statutory Health Insurance (SHI), also called a “sickness fund”, one of over 100 non-profit health insurance funds. These funds used to focus on specific professions, but funds are now open to anyone after reforms. Insurance premiums are fixed, based on income, and split between the insured and the employer. Health insurance for recipients of social insurance is co-paid by the local municipality.
Around 11% of the population have opted out of the SHI system and are enrolled in private insurance, which is open to citizens with high income (above ca. EUR 57,000 per year), civil servants and students. Premiums are based on risk instead of salary, and private insurance provides additional benefits at lower premiums compared to SHI rates for the same income group.
Of a total of EUR 185bn spent by statutory health insurance, 61bn is spend on hospital treatment, 34bn for treatment by physicians, 31bn on pharmaceuticals and 9.4bn on administrative costs. [70]

Global biosimilar policy comparison
20
2.1.4. Current issues in the healthcare system
Demographic change: Increased life expectancy and low birth rate will cause a decline in the overall population in Germany over the next decades, while the percentage of elderly will continue to increase. The decline has been temporarily halted due to increased migration in 2016, but the overall trend continues. The main challenge will be to manage healthcare costs while faced with a shrinking payer base. [71]
Increasing competition between health insurance providers: The statutory health insurance system left little room for competition between insurances, as premiums are tied to a fixed percentage of income and service levels are mostly standardized. In 2015, a system of optional additional premiums was introduced. This allows insurance providers to charge an additional fee of a few percent of income in exchange for additional services. However, customers have the right to switch to a different insurance when these bonus premiums are raised. [72]
2.2. Market for pharmaceuticals
2.2.1. Market statistics
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 60.8 BMI
World market share % 5.47 BMI
Pharmaceutical sales / capita USD 754 BMI
Pharmaceutical sales / GDP % 1.75 BMI
Pharmaceutical sales / health expenditure % 15.7 BMI
Prescription drug sales USD bn 53.4 BMI
Patented drug sales USD bn 41.8 BMI
OTC medicine sales USD bn 7.4 BMI
Generic drug sales USD bn 11.5 BMI
Share of generics (value) % 36% OECD
Share of generics (volume) % 81% OECD
Source: BMI data tool, accessed on 25 July 2017; OECD 2014 [21]
The sales channel for pharmaceuticals in Germany is dominated by brick-and-mortar pharmacies, which cover 84% of sales (hospitals: 8%, other: 8%). Pharmacies are privately owned, and the owner must be a pharmacist. Most pharmacies are single-store operations. Branches are allowed, but they are a minority.
72% of pharmaceutical costs are carried by statutory health insurance, 7% by private health insurance, 16% by private households and organizations, and 5% by others. [73]
2.2.2. Legal framework
Market authorization
As in all EU countries, pharmaceuticals can either be approved EU-wide by the EMA in the Centralized Procedure, or locally in the Decentralized Procedure or Mutual Recognition Procedure.
The Federal Institute for Drugs and Medical Devices (Bundesinstitut für Arzneimittel und Medizinprodukte, BfArM) is responsible for the approval, i.e. marketing authorization, of medicinal products, including biosimilars, in Germany.
The BfArM authorizes finished medicinal products on the basis of the German Medicines Act (Arzneimittelgesetz, AMG). In the course of these licensing procedures it reviews the proof of efficacy, safety, and adequate pharmaceutical quality of the finished medicinal products.
Licenses are limited to five years. Renewals are granted upon application and after new evaluation. BfArM must be notified of variations to already licensed medicinal products. Major variations can only be implemented after authorization by BfArM. [70]

Global biosimilar policy comparison
21
Pricing
Until 2011, pharmaceutical firms were free to set their own wholesale prices for prescription medicines. As part of a package of health care reforms intended to deal with an €11 billion budget deficit, a 2011 law, AMNOG, was enacted and mandated clinical benefit assessments of new drugs vs. existing drugs. The Institute for Quality and Economical Use of Resources in Healthcare (IQWiG) conducts these assessments and serves as a scientific advisor to the G-BA. Launch prices for medicines may be freely set by manufacturers and this price point is maintained for up to 12 months while the G-BA assessment and price negotiations with the SHI Head Association take place. After six months G-BA’s conclusions are then used as a basis to negotiate reimbursement prices with the industry. The product is only granted a higher price if an additional benefit over existing products or treatments can be proven. The price is a top-level cap, and pharmaceutical companies are free to set lower prices.
The 2006 Arzneimittelversorgungs-Wirtschaftlichkeitsgesetz (AVWG) allowed pharmaceutical companies to negotiate price discounts for specific medicines with health insurances or hospitals.
Reimbursement
Involved Institution for decision, appraisal and recommendation
Federal Joint Committee (G-BA)
Involved Institution for evidence assessment
Institute for Quality and Efficiency in Healthcare (IQWiG)
Interactions G-BA commissions IQWiG or a third party
Pricing • Free Pricing for first year after market entry (originators) • Internal reference pricing “Festbeträge“ • Value-based pricing (AMNOG process) • External reference pricing for outpatient medicines as secondary
criterion, references 15 EU countries, weighted based on market size and PPP
Type of reimbursement list De-facto negative list
Reimbursement restrictions Restriction of prescription due to inappropriateness / inefficiency
Revision of decision Benefit assessment on application by manufacturer or investigation by G-BA due to new evidence
Source: European Observatory on Health Systems and Policies [74]
On top of the fixed manufacturer price, wholesalers are allowed by law to charge a fixed fee of EUR 0.70 plus a variable fee of 3.15%, capped at EUR 37.80. Retail pharmacies charge a fixed fee of EUR 8.35, a variable handling fee of 3%, and 19% VAT. [75]
On average, the list price of a prescription pharmaceutical is comprised of 50.3% manufacturer revenues, 3.5% wholesale revenues, 14.1% pharmacy revenues, and 16% taxes. In retail, that list price is, on average, reduced by a mandatory rebate from pharmaceutical companies to SHIs of 13.3% of the list price. The remainder is given to the consumer as discounts by pharmacies (14.1%). [73]
Generics and INN prescriptions
INN prescriptions are not mandatory, but substitution rules introduced with the AVWG require Pharmacists to substitute prescribed products for a cheaper product, unless the physician has specified a brand name and ruled out substitution. Physicians must explain a medical reason for their decision to block substitution. This effectively creates a situation where there is no difference between a brand name and an INN prescription unless the prescriber has ruled out substitution. This system has led to a volume market share of over 80% for generics, one of the highest worldwide. [75]
Co-payment
Statutory health insurances reimburse prescription drug’s retail price to the consumer, subject to a 10% co-payment that is limited to a minimum of EUR 5 and a maximum of EUR 10. A number of generics are exempt from co-payment as a sales incentive.
Co-payments are limited to a maximum of 2% of gross income per year. If a patient chooses a brand that is more expensive than the reference price, the difference is charged to the patient. [70] [76]

Global biosimilar policy comparison
22
2.3. Market for biosimilars
2.3.1. Available biosimilars
Biologic drugs are a huge cost factor in the budget of Statutory Health Insurance (SHI). Biosimilars in particular represented a share of EUR 1bn in the first half of 2016. [77]
See the appendix for a list of biosimilars approved for marketing in the EU by EMA. In Germany, pharmaceutical products can be sold immediately after EMA approval.
The table below lists biosimilars that are actively marketed by their manufacturer in Germany. They represent around 60% of the biosimilars approved by EMA.
Biosimilar brand name Active substance Company BfArM
authorization date
Truxima rituximab Celltrion Healthcare Hungary Kft. 22/02/2017
Flixabi infliximab Samsung Bioepis UK Limited (SBUK) 30/05/2016
Benepali etanercept Samsung Bioepis UK Limited (SBUK) 14/01/2016
Accofil filgrastim Accord Healthcare Ltd 18/09/2014
Abasaglar (previously Abasria)
insulin glargine Eli Lilly Regional Operations GmbH 09/09/2014
Bemfola follitropin alfa Gedeon Richter Plc. 27/03/2014
Grastofil filgrastim Apotex Europe BV 18/10/2013
Ovaleap follitropin alfa Teva Pharma B.V. 27/09/2013
Inflectra infliximab Hospira UK Limited 10/09/2013
Remsima infliximab Celltrion Healthcare Hungary Kft. 10/09/2013
Nivestim filgrastim Hospira UK Ltd
08/06/2010
Filgrastim Hexal filgrastim Hexal AG 06/02/2009
Retacrit epoetin zeta Hospira UK Limited 18/12/2007
Silapo epoetin zeta Stada Arzneimittel AG 18/12/2007
Abseamed epoetin alfa Medice Arzneimittel Pütter GmbH & Co. KG 28/08/2007
Binocrit epoetin alfa Sandoz GmbH 28/08/2007
Epoetin Alfa Hexal epoetin alfa Hexal AG 28/08/2007
Omnitrope somatropin Sandoz GmbH 12/04/2006 Source: Pro Biosimilar market data, accessed on 8 August 2017 [78]

Global biosimilar policy comparison
23
2.3.2. Biosimilars market share
Uptake of biosimilars in Germany by volume is one of the highest among EU5, Captured below is the market share of biosimilars (in comparison with the reference product, accessible market and the total market) in the product classes of EPO, G-CSF, HGH, Anti-TNF and follitropin alpha. [10]
Source: The Impact of Biosimilar Competition in Europe, IMS (sourced from a publicly available report) [10]9
2.3.3. Market outlook
The biosimilars market in Germany is expected to exhibit high near-term growth primarily driven by Germany’s significant investment in physician education and mandatory prescription quotas. The biosimilars market in Germany is expected to grow at a CAGR of 31% in the period 2014-2025, according to a study by Visiongain. [79]
The market outlook of biosimilars in Germany is as follows [79]:
Source: Visiongain [79]
9 EPO: epoetin; G-CSF: Granulocyte-colony stimulating factor; HGH: Human Growth Hormone; TNF: Tumor Necrosis Factor; Biosimilar vs. reference product - TD
biosimilars as % of TD reference products; Biosimilar vs. accessible market - TD biosimilars as % of TD accessible market; Biosimilar vs total market - TD biosimilars as % of TD total market
0.14 0.21 0.330.50
0.76
1.08
1.451.70
1.962.20
2.452.70
2014 2015E 2016E 2017E 2018E 2019E 2020E 2021E 2022E 2023E 2024E 2025E
Biosimilar revenue forecast 2014-2019 (US$ billions)
81%
67%
37%
78%
65%
12%
32%
15% 15%17% 17%9%
19%11%
6%4% 3% 1%
Biosimilar vs. referenceproduct
Biosimilar vs. accessiblemarket
Biosimilar vs. total market
Biosimilar market share (% of treatment days)
EPO (2015) G-CSF (2016) HGH (2016)
Anti-TNF (2016) Follitropin alfa (2016) Insulin glargine

Global biosimilar policy comparison
24
2.4. Legal framework for biosimilars
2.4.1. Market approval
Approval pathway: The country follows a centralized regulatory pathway established by the European Medicines Agency (EMA) in 2006 (for details refer to the section on EMA’s regulatory framework on biosimilars). Some low-molecular weight heparins derived from porcine intestinal mucosa may be approved at the national level by the national competent authorities which in case of Germany is the Federal Institute for Drugs and Medical Devices (BfARM).
In addition to the European approval pathway, Germany has also opened domestic approval process for biosimilars. The process is based on the approval process for generics, however, according to paragraph 24b part 5 of the pharmaceuticals law (AMG, Arzneimittelgesetz), additional documentation of pre-clinical and clinical studies can be required if base material and production process of the biosimilar differ from the reference product. [80] [81] [82]
2.4.2. Pricing and reimbursement
The AMNOG process does not apply to biosimilars. Biosimilars do not have to undergo the additional benefit assessment similar to newly authorized pharmaceuticals as defined in the Act on the Reform of the Market for Medicinal Products (AMNOG) on 11 November 2010. [11]
Biosimilars are included in reference pricing system alongside their originator drug. A biosimilar’s price is set by the manufacturer but cannot be higher than that of the branded drug. These reference price groups are used as a cost containment tool. [80] [11] [83]
Biosimilars generally attract major discounts vs. originator medicines. For example, the price discount on infliximab biosimilars is around 40%.
Rebates and tendering form part of the procurement system in Germany and high number of SHIs have created an opportunity for market access via tendering and contracts.
• Rebates: Rebates have been introduced to reduce the net price to SHIs particularly for infliximab and partially for epoetins, filgrastims and somatropins
• Tendering/ Open house contracts: SHIs have started open house contracts, allowing manufacturers (of both biosimilars and original biologics) to be part of contracts that offer a rebate on reduce selling price.
In December 2016, the healthcare oversight body, G-BA in Germany, launched a consultation that would investigate the inclusion of infliximab in a fixed price group. [84]

Global biosimilar policy comparison
25
2.4.3. Switching and substitution
When giving a prescription, physicians are expected to inform the patients on co-payment options as they choose between a biosimilar and its reference product. [82]
Interchangeability: Interchangeability of prescription drugs is stipulated in a framework agreement (Rahmenvertrag) between the top-level organization of the statutory health insurances (GKV) and the pharmacists association (Deutscher Apothekerverband). This agreement is based on paragraph 129 of the Social Code V (Sozialgesetzbuch, SGB).
Substitution: A list of biosimilars was included in the list of interchangeable medicines for the first time in 2011, then updated in 2015. Only products that are considered “bio-identical” are added to the list. Products that are manufactured by the same supplier, on the same production line, but sold under different brand names are considered bio-identical. Therefore, even within the same active ingredient group, some originators and biosimilars are considered interchangeable, while others are not. [85]
These bio-identical biosimilars are interchangeable at the pharmacy level.
Biosimilars that can be automatically substituted at the pharmacy level as per the framework agreement
Active substance Biosimilar brand name Company Automatic
substitution start date
epoetin alfa
Abseamed Medice Arzneimittel Pütter GmbH & Co. KG
01/10/2011 Binocrit Sandoz GmbH
Epoetin alfa Hexal Hexal AG
epoetin zeta Retacrit Hospira UK Limited
01/10/2011 Silapo Stada Arzneimittel AG
epoetin theta Biopoin Teva GmbH
01/06/2015 Eporatio ratiopharm GmbH
filgrastim (1)
Biograstim AbZ-Pharma GmbH
01/06/2015 Ratiograstim Ratiopharm GmbH
Tevagrastim Teva GmbH
filgrastim (2) Filgrastim Hexal Hexal AG
01/06/2015 Zarzio Sandoz GmbH
filgrastim (3) Accofil Accord Healthcare Ltd
01/06/2015 Grastofil Apotex Europe BV
infliximab Inflectra Hospira UK Limited
01/06/2015 Remsima Celltrion Healthcare Hungary Kft.
Interferon beta-1b
Betaferon Bayer Pharma AG 01/10/2011
Extavia Novartis Source: GKV-Spitzenverband [85]
2.4.4. INN prescribing
In general, biosimilars are exempt from INN prescription. If a biosimilar is prescribed by INN, pharmacists need to consult the prescribing physician before dispensing the drug. [11]

Global biosimilar policy comparison
26
2.5. Additional factors and initiatives impacting the growth of biosimilars
2.5.1. Marketing or education initiatives regarding biosimilars
In Germany, the statutory health insurers and physician associations have been proactive in reaching out to physicians to encourage them to prescribe biosimilars. Physicians were approached by their Kassenärztliche Vereinigung (KV, regional physicians’ association) early on, using open communication channels and discussion forums to build trust in the biosimilar concept. In addition, prescribing quotas were put in place immediately which were explained to doctors using doctors’ letters (Ärztebriefe). KV enforcement and education campaigns highlighting the savings potential of biosimilar medicines have proven to be valid tools to foster competition and increase uptake in the country. [11]
In addition to payers, physician associations have taken the following initiatives to encourage biosimilar prescription:
• The “biolike” initiative — Initiative brought forward by the physician association KV Westfalen-Lippe and the statutory health insurance Barmer GEK
• Besides foreseeing the provision of detailed information on biosimilars, the agreement between KV Westfalen-Lippe and Barmer GEK focuses on getting physicians to help boost biosimilar uptake [11]
2.5.2. Government incentives to increase biosimilar prescriptions
The German government has been supportive of biosimilars in the country through the creation of an incentive system that consists of reference pricing system, regional SHI and physician quotas and a rebate system. [86]
Incentives to doctors / hospitals / pharmacies
Gain sharing at the physician level via the following initiatives has supported biosimilar uptake in the country:
• Contract on inflammatory bowel disease (IBD) — The physician association KV Westfalen-Lippe and the statutory health insurance Barmer GEK closed a contract geared toward improving care of IBD patients • The agreement indicates that patients with ulcerative colitis or Crohn's disease are to be treated
with a drug-based therapy of primarily infliximab biosimilars • Absolute savings generated from prescribing infliximab biosimilar will be equally split between
the treating physician and the Barmer GEK [11]
• As part of the “biolike” initiative, physicians who achieve set biosimilar quotas are allowed to bill additional services to their patients. Under this agreement, absolute savings from prescribing the biosimilar infliximab will be split between the treating physician and health insurance. [11]
The incentive system towards manufacturers is based on voluntary price concessions and rewards low priced offers with volume and potential uptake. [11]
Germany also instated a system of clinic-level overall pharmaceutical budgets. In the case that physicians exceed the budget by 125%, they need to pay any amount which is over 115%. [86]
Prescription quotas
Since 1998, Germany has a system of prescription quotas, which are agreed on a yearly basis between regional physician associations (KVs) and SHIs in a pharmaceuticals agreement (Arzneimittelvereinbarung) based on paragraph 84 part 1 Social Code (SGB) V. Quotas define prescribing targets for frequently prescribed drug classes. They are set as a % of total Defined Daily Dose (DDD), either as a maximum for an originator or a minimum for the generic / biosimilar.
While these targets are defined in a national level for each KV region (roughly equivalent to the states), local administrations are allowed to diverge from them and set additional targets for other medicines.
In 2017, biologics with a country-wide biosimilar prescription quota were erythropoietin (Baden-Württemberg 21.2% - Bremen 68.2%; since 2010), infliximab (Hamburg 11.5% - Westfalen-Lippe 44.8%; since 2015) and etanercept (Sachsen 0.5% - Westfalen-Lippe 11.9%; since 2016). [87]

Global biosimilar policy comparison
27
2.5.3. Procurement policy
Government policies to support manufacturing and supply of biosimilars
Historically, the German government has assisted the pharmaceutical industry through supportive programs and funding opportunities, making it the third largest industry in the country. [88]
Pharma-dialogs (agreement between industry and payers/ policy makers) in the current procurement process for biosimilar and generic medicines have put the system at an increased risk of supply guarantee. Consequently, the policy makers have agreed to support parallel supply from multiple manufacturers of generic and biosimilar medicines in future measures. [11]
Import regulations
Germany like other EU countries, follows EMA regulations on biosimilar imports. As per EMA regulations, manufacturers and importers of biosimilar medicines are legally obliged to hold a valid Manufacturer’s and Importer’s Authorization (MIA)/ GMP certificate issued by an EU national competent authority. [89]
Other Country-specific Issues that Influence the Introduction and Adoption of Biosimilars
Significant efforts in introducing prescribing quotas and physician education have resulted in the positive stake-holder perception that has been driving biosimilar uptake in Germany.
• Their acceptance is growing, as physicians are usually fearful of financial penalties if prescription targets are exceeded [90]
• Payers prefer to use biosimilars to reduce their costs [90]
2.5.4. Industry position on biosimilars
Association of Research-based Pharmaceutical Companies (VfA) The body published a position paper with the following requests: [91]
• Pharmacovigilance studies are required before and after market entry of a biosimilar • No INN prescribing, and tracking of batches in case of side effects • No pharmacy-level substitution • Freedom to prescribe for the physician
Pro Generika The association of generics manufacturers, said in a paper submitted to the German Ministry of Economics and Technology in 2013, that the presence of tenders is unsuitable as they may act as a market barrier by creating price pressures on the manufacturer which may lead to drug shortage. [92]
Pro Biosimilars The German biosimilars lobby called fixed price groups for biosimilars “problematic” in press articles. [93]

Global biosimilar policy comparison
28
3. France
3.1. Current healthcare landscape The World Health Report 2000 ranked France as the best performing healthcare system in the world. While it did not rank best in any of the subcategories, the overall balance of good ratings between population health status, public insurance coverage, cost, equity and responsiveness put it at the top. [94]
3.1.1. Country data
Indicator Value Year Source
Population (Mill) 64.46 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %)
0.45 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 12.21 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 18.94% 2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 41,490 2016 OECD [14]
Doctors per 10,000 people 32.27 2015 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people
10.91 2015 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 61.3 2015 OECD [16]
Healthcare expenses (% of GDP) 11 2016 OECD [17]
Source: UN Dept. of Economic and Social Affairs, WHO and OECD
3.1.2. Healthcare system
According to “Médecine Libérale” principles, patients are free to choose the doctors they want; doctors are free to prescribe whatever they want; doctors are paid directly by the patients who are subsequently reimbursed by health funds; doctors are free to settle wherever they want. There is no gate-keeping, and patients can directly access any specialist in an ambulatory setting.
All prices are regulated; doctors are directly paid by funds; the list of drugs that are restricted to hospital or to specialist use keeps expanding; there is a growing tendency to issue quality control procedures and clinical guidelines which limit doctors’ freedom and autonomy.
Some doctors – called “sector 2” doctors – were allowed in the 1980s, to price their services above the regulated fees; patients being still reimbursed on the basis of the regulated fee. The extra fee has kept rising in recent years, passing from 10-15% at the origin to 50% and more at present. In some medical professions – especially surgery and obstetrics – and in some regions – especially large cities– it becomes difficult to find a doctor who does not charge these extra fees. As public insurance does not reimburse these fees and private insurance is more and more reluctant to pay the bill, this situation is creating a real access problem.
3.1.3. Health insurance system
The French population is 100% covered by a group of mandatory public health insurances. Funds are independent of the state, financed by payroll taxes (60%) and, since 1990, by a proportional income tax (40%), called the CSG (“Contribution sociale généralisée”). Affiliation to a fund is split by profession (worker, farmer etc.). As premiums and benefit packages are identical across funds, France has a de facto single payer system.
After treatment, patients have to co-pay a share of the financial burden. About 9 million people with a severe medical condition are exempted from co-payment, about 15% of the population responsible for about 60% of health care expenditures.
92% of the population hold a complementary private or employer-based health insurance contract on top of the base public insurance coverage. Premiums for these contracts are generally based on income rather than on risk. This creates a unique two-tier health insurance system. Remaining out-of-pocket payments after both tiers do not exceed 9% of total health expenditures.
Since 1999, 4 to 5 million people (out of 60 million), who cannot afford a private contract, may receive a free affiliation to a public complementary health insurance system.

Global biosimilar policy comparison
29
Health funds try to channel patients by imposing a “family doctor” (“médecin traitant”) which is not mandatory but allows patients to be better reimbursed; recently, a pay-for-performance system was introduced, allowing doctors to win financial bonuses if they reached some defined and quantified individual objectives. [94]
3.1.4. Current issues in the healthcare system
Cost control measures: The large health funds ran into deficits in the early 2000s, causing the government to shift the burden towards complimentary insurance and co-payments. [94] A study by the now dissolved Collectif interassociatif sur la Santé (CISS) claims that this has led to a rise in hidden costs that are directly charged to patients rather than covered by the insurance system or direct government payments. [95] According to a 2015 WHO report, voluntary health insurance now covers 13.8% of all health expenditure, while out-of-pocket payments comprise 7.5%. [96]
Solidarity: The French system is built on the principle that the more you need treatment, the less you pay. This carries potential for conflict when expensive treatments like biologics are burdened on the general public. [94]
Government control vs. liberal medicine: Over the post-war period, the French state has exerted more and more control over the healthcare system, to the point where it can be considered a fully state-controlled system. [94]
3.2. Market for pharmaceuticals
3.2.1. Market statistics
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 36.9 BMI
World market share % 3.32 BMI
Pharmaceutical sales / capita USD 570 BMI
Pharmaceutical sales / GDP % 1.50 BMI
Pharmaceutical sales / health expenditure
% 12.9 BMI
Prescription drug sales USD bn 30.1 BMI
Patented drug sales USD bn 23.1 BMI
OTC medicine sales USD bn 6.8 BMI
Generic drug sales USD bn 6.9 BMI
Share of generics (value) % 15.50% OECD
Share of generics (volume) % 25.90% OECD
Source: BMI data tool, accessed on 25 July 2017; OECD 2014 [21]

Global biosimilar policy comparison
30
3.2.2. Market authorization and pricing
Market authorization
As in all EU countries, pharmaceuticals can either be approved EU-wide by the EMA in the Centralized Procedure, or locally in the Decentralized Procedure, Mutual Recognition Procedure, or National Procedure. [22]
The French Health Agency (Agence nationale de sécurité du médicament et des produits de santé – ANSM) is responsible for market approval.
Pricing and reimbursement
Before a new prescription drug is available to patients, it must undergo a price setting process.
Source: European Observatory on Health Systems and Policies [25]
The first stage of the price-setting process is an evaluation of the Clinical Benefit (SMR) and Improvement in Clinical Benefit (ASMR) over existing products, conducted by the Transparency commission of the French National Authority for Health (HAS). The agency assigns one of five benefit levels to the product, between ASMR V (no improvement) and ASMR I (significant improvement).
Manufacturing company
Dossier submitted following marketing authorization by the ANSM
Haute Autorité de Santé (HAS) – It gives recommendations for medical product usage Economic committee for healthcare products (CEESP) Responsible for medico-economic assessment for innovative drugs that have an ASMR rating of I, II, or III and with expected annual revenues in excess of 20 million Euros
Transparency Committee (TC) Assesses clinical benefits of drugs as compared to existing ones; also responsible for setting reimbursement rates
Comité Economique des Produits de Santé (CEPS) Responsible for setting the prices of reimbursable products, reference price list for generics and the hospital price list outside the fee-for-service scheme Gives advice to MoH (Ministry of social affairs and health), which determines if the new drug will be added to the reimbursement list
[97]
Reimbursement
Involved Institution for decision Ministry of Social Affairs and Health
Involved Institution for evidence assessment, appraisal and recommendation
French National Authority for Health (HAS)
Interactions Committee at HAS performs assessment and advises the minister; for highly innovative and expensive medicines, the Economic and Public Health committee (CEESP) performs an economic assessment
Pricing • External reference pricing for ASMR I, II, or III (Outpatient medicines and some inpatient medicines (not financed through DRG system)); References DE, ES, IT, UK; No specified calculation method
• Internal reference pricing • Value-based pricing • Negotiation
Type of reimbursement list Positive list
Reimbursement restrictions Therapeutic benefit, patient group
Revision of decision Every 5 years or ad-hoc due to new evidence, change of indication, or ministerial request

Global biosimilar policy comparison
31
The price setting is then conducted in two separate processes, for in-patient and out-patient.
For outpatient use, if the product receives a favorable opinion, it is categorized as a reimbursable drug and subject to price negotiation. Price setting is then conducted between the manufacturer and the Comité Economique des Produits de Santé (CEPS), based on the ASMR. In case of a low ASMR (V), the price is set below competitor products. In case of minor ASMR (IV), pricing depends on the target population. In case of a high ASMR (I – III), the price is set by comparing to price levels in neighboring European countries.
In case of an unfavorable opinion, it enters the market as a non-reimbursable drug under free pricing.
For hospital use, outpatient drugs have the same pricing as for outpatient use, set by CEPS if reimbursable or unregulated if not.
There are two additional categories for hospital use. Innovative drugs can have a registered maximum price, set by the manufacturer, which is used as a basis for reimbursement.
For hospital drugs included in activity-based costing, there exists a hospital-based tender process.
Co-payments
Co-payment levels for patients are set by the French Health Insurance Fund (UNCAM) based on therapeutic benefit (SMR). There are four reimbursement levels: none, low (15%), medium (30%) and high (65%).
INN prescriptions and generic substitution
Starting from 2015, INN prescriptions are mandatory in France, and generic substitution by pharmacists is incentivized, but so far the policy has only led to a volume market share for generics of over 25%.
But if the prescriber considers that an incomprehension risk exists for the patient, or if it is necessary to keep the same specialty in the treatment, the doctor can provide the name of the brand in addition to the INN. HAS developed an official list of the different situations where INN prescription is not desirable. [98] [74]

Global biosimilar policy comparison
32
3.3. Market for biosimilars
3.3.1. Available biosimilars
As of August 2017, 19 biosimilars have been approved by the Agence nationale de sécurité du médicament et des produits de santé (ANSM) in France and of these, 15 are being marketed:
Biosimilar brand name
Active substance
Company EMA
authorization date
ANSM authorization
date
Commercialization status
Truxima rituximab Celltrion Healthcare Hungary Kft.
17/02/2017 17/02/2017 Marketed
Lusduna insulin glargine
Merck Sharp & Dohme Limited
04/01/2017 04/01/2017 Not marketed
Flixabi infliximab Samsung Bioepis UK Limited (SBUK)
26/05/2016 26/05/2016 Marketed
Benepali etanercept Samsung Bioepis UK Limited (SBUK)
14/01/2016 14/01/2016 Marketed
Accofil filgrastim Accord Healthcare Ltd 18/09/2014 18/09/2014 Marketed
Abasaglar insulin glargine
Eli Lilly Regional Operations GmbH
09/09/2014 09/09/2014 Marketed
Bemfola follitropin alfa
Gedeon Richter Plc. 27/03/2014 27/03/2014 Marketed
Grastofil filgrastim Apotex Europe BV 18/10/2013 18/10/2013 Not marketed
Ovaleap follitropin alfa
Teva Pharma B.V. 27/09/2013 16/09/2014 Marketed
Inflectra infliximab Hospira UK Limited 10/09/2013 10/09/2013 Marketed
Remsima infliximab Celltrion Healthcare Hungary Kft.
10/09/2013 10/09/2013 Marketed
Nivestim filgrastim Hospira UK Ltd 08/06/2010 08/06/2010 Marketed
Zarzio filgrastim Sandoz GmbH 06/02/2009 06/02/2009 Marketed
Ratiograstim
filgrastim Ratiopharm GmbH 15/09/2008 15/09/2008 Not marketed
Tevagrastim filgrastim Teva GmbH 15/09/2008 06/02/2012 Marketed
Retacrit epoetin zeta Hospira UK Limited 18/12/2007 11/10/2010 Marketed
Abseamed epoetin alfa Medice Arzneimittel Pütter GmbH & Co. KG
28/08/2007 28/08/2007 Not marketed
Binocrit epoetin alfa Sandoz GmbH 28/08/2007 28/08/2007 Marketed
Omnitrope somatropin Sandoz GmbH 12/04/2006 12/04/2006 Marketed Source: ANSM directory, accessed on 8 August 2017 [99]

Global biosimilar policy comparison
33
3.3.2. Biosimilars market share
Biosimilars of epoetin, G-CSF and HGH have been able to capture a larger share as compared to anti-TNF and follitropin alpha.
Captured below is the market share of biosimilars (in comparison with the reference product, accessible market and the total market) in the product classes of EPO, G-CSF, HGH, Anti-TNF and follitropin alpha. [10]
Source: The Impact of Biosimilar Competition in Europe, IMS (sourced from a publicly available report) [10]10
3.3.3. Market outlook
The biosimilars market in France is expected to exhibit high growth, primarily driven by government policies to reduce the healthcare budget. [97]
The market size (EUR million) of biosimilars in France is as follows:
Source: Les Echos Etudes – GERS data [100]
10
EPO: epoetin; G-CSF: Granulocyte-colony stimulating factor; HGH: Human Growth Hormone; TNF: Tumor Necrosis Factor; Note: Biosimilar vs. reference product - TD biosimilars as % of TD reference products; Biosimilar vs. accessible market - TD biosimilars as % of TD accessible market; Biosimilar vs total market - TD biosimilars as % of TD total market
45%
26%
10%
86%
52%
15%
34%
16% 16%14% 14%8%
13% 9% 5%
Biosimilar vs. referenceproduct
Biosimilar vs. accessiblemarket
Biosimilar vs. total market
Biosimilar market share (% of treatment days)
EPO (2015) G-CSF (2016) HGH (2016) Anti-TNF (2016) Follitropin alfa (2016)
125
625
2015 2020E
EUR millions
CAGR: 37.9%

Global biosimilar policy comparison
34
3.4. Legal framework for biosimilars
3.4.1. Market approval
Approval pathway: The country follows a centralized regulatory pathway established by the European Medicines Agency (EMA) in 2006 (for details refer to the section on EMA’s regulatory framework on biosimilars)
For the national pathway, approval is given by the national regulatory body, National Agency of Medicine Security and Healthcare Products (ANSM). This body is also responsible for traceability and appropriate patient monitoring for biosimilars.
3.4.2. Pricing and reimbursement
The process for pricing biosimilars is same as that for innovative medicines. However, there are chances of a shortened Transparency Committee (TC) review. This committee is a part of Haute Autorité de Santé (HAS) and is responsible for evaluating new drugs. The biosimilar price negotiation doctrine is currently under discussion between the trade association LEEM and the CEPS; the end of negotiations is expected before the end of 2017.
Innovative medicines are given an Amélioration du Service Médical Rendu (ASMR) rating of V (no clinical improvement) to I (major improvement), which forms the basis of price negotiations with The Comité Economique des Produits de Santé (CEPS). Biosimilars receive a systematic rating of V. [101] An official evaluation of treatment and cost benefits is conducted on a case by case basis to demonstrate their benefits on treatment costs.
Both originator and typically one biosimilar are on the same formulary. Price of the product is the main driver for procurement and reimbursement. [97]
Below are the guidelines for different distribution channels: [11]
In the hospital setting:
• The price of the biosimilar must be equal to or lower than originator price • Mandatory price cut of at least 10% for originator medicine subsequent to the launch of biosimilars • Price revision for both products (reference biologics & biosimilars) every 18-24 months based on
the average value of hospital tenders In the retail setting:
• Biosimilars are expected to be priced ~25-35% below the originator’s initial price, • Originator’s price subsequently undergo mandatory price cut of ~15-20% • Price revision for both products (reference biologics & biosimilars) every 2 years
3.4.3. Switching and substitution
Switching: ANSM initially recommended against the switching of patients already treated with a biologic, to limit the immunogenicity risk and ensure traceability for pharmacovigilance monitoring. However, ANSM changed its position in May 2016, because of the positive real-world evidence available for biosimilars. It stated that switching can be considered during treatment if the patient is informed about the potential switch, his or her consent is obtained, and treatment is closely monitored. [59]
A new ministerial instruction (issued on October 12th 2017) specifies that the switch can be made at any time of the treatment, and that it does not require additional obligations, other than those of any biological medication in terms of patient information and traceability of the prescription.
Substitution: In December 2013, the French Parliament passed a law “2014 Social Security Financing Law (LFSS)”. This regulation permitted a new form of pharmacy-level “substitution” in cases where biosimilars meet the following conditions:
• Should be of the similar biologic group as that of prescribed biologic • The patient is molecule naïve (undergoing treatment with the molecule for the first time) • The physician should not have prohibited substitution with a mention “Non substitutable” • The prescriber must be informed about the substitution (i.e. automatic substitution is not allowed) • Once a substitution to a biosimilar has been carried out, a further substitution to a different
biosimilar cannot take place. The same biosimilar that was previously delivered must continue to be delivered, in order to ensure continuity in the treatment.
• Substitution cannot generate an additional cost to the Public HealthCare System. [102]
Despite the 2014 LFSS and the 2017 LFSS regulation, the legal decree that would permit substitution has not been published yet, so while substitution is possible in theory, it is still not allowed in practice. [103]

Global biosimilar policy comparison
35
3.4.4. INN prescribing
Even though INN prescriptions are mandatory, the law of 26 January 2016 (art. 149) makes the prescription both in INN & in commercial name mandatory for all biological drugs, including biosimilars. In case of INN prescribing, there does not exist any information on comparability between these biosimilars and the traceability of the prescription would not be ensured. [104]
3.5. Additional factors and initiatives impacting the growth of biosimilars
3.5.1. Marketing or education initiatives regarding biosimilars
France Foundation (consisting of medical education professionals) [105] [106] — since 2014, the Foundation has served as a biosimilars educational resource for nearly 14,500 clinicians through the delivery of numerous educational initiatives targeting various clinical disciplines. Some of the recent initiatives in this direction include the following:
• It has recently launched an on-demand initiative that will identify the needs of learners and will direct individuals towards the appropriate education that addresses them
• In 2016, the body collaborated with The Calibre Institute for Quality Medical Education to increase clinician awareness, knowledge, and confidence regarding the role of biosimilars in clinical care
ANSM — the body has created a reference list of similar biologic groups to increase physicians’ awareness of the existence of biosimilar versions of biologics.
3.5.2. Government incentives to increase biosimilar prescriptions
Incentives to doctors / hospitals / pharmacies
With the exception for a compensation on public health goals (ROSP) for insulin glargine biosimilars for outpatients, there are no incentives and obligations for the physicians to prescribe biosimilars, however, the physician’s decision is based on the products that are available in the hospital formulary. [11]
However, hospitals are incentivized via gain sharing as the difference between reimbursement tariff and the actual paid price is divided between hospitals and social security. Hospitals can avail these benefits only if they purchase products listed in the Tarification à l’activité (T2A) or retrocession list (drugs that are part of this list are not included in global Diagnosis Related Group costs11). [11]
As hospital budgets are limited in the case of non-T2A drugs, the use of gainsharing has encouraged the uptake of biosimilars in the country. [11]
Prescription quotas
There are no prescribing quotas for physicians. [11] However, a new 2018-2020 National Biosimilar Support Plan announced by the Ministry of Health in October 2017 will require that 70% of relevant prescriptions for out-patients should be for biosimilars – this will be set up in new contracts with hospitals from 2018 onwards. [107]
3.5.3. Other country specific issues that influence the introduction and adoption of biosimilars
• Patients’ and physicians’ willingness is largely based on robust clinical study data demonstrating comparability, safety and efficacy
• Physicians are favorable towards the adoption of biosimilars, but have a negative opinion towards pharmacy-level substitution
• Payers prefer to use biosimilars in order to reduce costs • Fixing the tariff at parity for the biosimilar and its originator is intended to trigger competition,
since hospitals can keep part of any discounts negotiated below the list price
3.5.4. Industry position on biosimilars
The Strategic Council for Healthcare Industries (CSIS) and Sectoral Strategic Committee (CSF) had suggested in 2013 to form a working group for developing a legal framework for manufacturing, economic and public health challenges relating to biosimilars. Les entreprises du médicament (LEEM), the French pharmaceutical industry association, criticized that the 2014 social security finance bill (Loi de financement de la sécurité sociale (LFSS)) contradicted this measure. Therefore, the working group continues to work to establish a sustainable and balanced biosimilar model. [108]
11
Diagnosis Related Groups (DRG) is a mode of payment linking funding in hospitals to optimal utilization of resources. The system, Tarification à l’activité (T2A), was introduced in France in 2004/2005. Drugs which are listed in Hors T2A are excluded from the global DRG cost and are 100% reimbursed

Global biosimilar policy comparison
36
4. Sweden
4.1. Current healthcare landscape The Swedish health care system is mainly government-funded and decentralized, although private health care also exists. The health care system in Sweden is financed primarily through taxes levied by county councils and municipalities.
4.1.1. Country data
Indicator Value Year Source
Population (Mill) 9.76 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %) 0.78 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 1.91 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 19.57% 2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 49076 2016 OECD [14]
Doctors per 10,000 people 41.07 2013 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people 7.55 2013 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 24.4 2015 OECD [16]
Healthcare expenses (% of GDP) 11 2016 OECD [17]
Source: UN Dept. of Economic and Social Affairs, WHO and OECD
4.1.2. Healthcare system overview
Sweden's health care system is organized and managed on three levels: national, regional and local. At the national level, the Ministry of Health and Social Affairs sets the political agenda for health and medical care and establishes principles and standards for care. The ministry along with other government bodies supervises activities at the lower levels, allocates grants and periodically evaluates services to ensure correspondence to national goals. It also handles negotiation with large providers, including pharmaceutical firms, approval of drugs, and levels of patient contributions.
The pharmaceutical and other cost budget is split within the hospitals down to the clinic level. This means that each Head of clinic is a budget holder, i.e. every clinic head at the hospitals are responsible for the cost control and staying with in the cost budget.
Primary care is chiefly provided by publicly owned primary care centers that employ up to four GPs as well as nurses, physiotherapists, social workers and other healthcare specialists. GPs do not act as gatekeepers to secondary care. [109]
County councils own and operate most hospitals. However, since the 1990s there has been a push for more flexibility in the system, with more private providers and choice of provider for patients. Private providers are required to enter into a contract with the county councils, which regulate prices and level of service offered. Patients are not reimbursed for services from private providers who do not have such an agreement. Different governments have pushed and halted the privatization of healthcare, depending on their political alignment. [109]
Pharmacies were taken over by a state monopoly in the 1970s, but this decision has been reversed and the sector was liberalized in 2008. Most pharmacies are now owned by one of four dominant chains, in addition to the state-owned corporation. [109]
4.1.3. Health insurance system
Sweden operates under a public single-payer insurance system with universal coverage.
The system covers public health and preventive services, inpatient and outpatient hospital care, primary health care, prescription drugs, mental healthcare, dental care, rehabilitation, disability support, home care and nursing home care.
Financing is provided from proportional income taxes levied by county councils and municipalities.
County councils finance primary and hospital care, while municipalities cover nursing and home care. The central government provides subsidies for prescription drugs. The central government also provides financial support to local governments to alleviate geographical inequalities.

Global biosimilar policy comparison
37
Primary care visits involve out-of-pocket charges of SEK 100 to 320. There are exemptions for those with low means and total annual payments are capped at around SEK 4400 for all services other than dental. [110]
An increasing percentage of the population, up to 10%, is now covered by supplemental private health insurance, often provided by employers. The public health system has had issues with long waiting times to access specialist treatment, which can be cut short by taking on private insurance.
4.1.4. Current issues in the healthcare system
Long wait times: According to an international comparison in the Euro Health Consumer Index, Sweden has traditionally scored high on the quality and egalitarian access to healthcare, but it is mired in problems with long waiting times, particularly for specialist treatment such as cancer. Recently, the Swedish government has attempted to solve the problem by pumping more money into the system, without success. The waiting time problems are systemic, and increase overall health care costs through the inefficiencies they cause. [111]
Increase in supplementary private health insurance: Long wait times and inconsistent quality have led to a rising trend of private supplemental insurance, often financed by employers. Private insurance allows patients to skip waiting queues for specialists and gain access to more expensive treatment options. The public debate in Swedish newspapers centers on the question whether this trend is beneficial to the public health care system by alleviating stress from it, or detrimental as it the idea of a two-track healthcare system clashes with the idea of egalitarianism. [112] [113]
4.2. Market for pharmaceuticals
4.2.1. Market statistics
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 4.6 BMI
World market share % 0.42 BMI
Pharmaceutical sales / capita USD 471 BMI
Pharmaceutical sales / GDP % 0.94 BMI
Pharmaceutical sales / health expenditure
% 10.3 BMI
Prescription drug sales USD bn 4.2 BMI
Patented drug sales USD bn 3.5 BMI
OTC medicine sales USD bn 0.4 BMI
Generic drug sales USD bn 0.7 BMI
Share of generics (value)12
% 16.9% BMI
Share of generics (volume) % N/A -
Source: BMI data tool, accessed on 25 July 2017
4.2.2. Market authorization and pricing
Market authorization
As in all EU countries, pharmaceuticals can either be approved EU-wide by the EMA in the Centralized Procedure, or locally in the Decentralized Procedure, Mutual Recognition Procedure, or National Procedure. [22]
The authority responsible for marketing authorization is the Medical Products Agency (Läkemedelsverket, LV).
12
Share of generics (% of Value) = (Generic drug sales in USD bn*100)/ Prescription drug sales in USD bn

Global biosimilar policy comparison
38
Pricing and reimbursement (Out-patient)
In Sweden, the cost of outpatient drugs is financed by the central government through designated government grants to the county councils, whereas in-patient care at hospitals, including any drugs used for the treatment, are carried by county councils directly. This leads to a split in the assessment process.
Source: European Observatory on Health Systems and Policies [74]
After market authorization, manufacturers apply with the Dental and Pharmaceutical Benefits Agency (Tandvårds-ochläkemedelsförmånsverket, TLV) for an assessment of the scientific evidence. The product is then categorized as either “general reimbursement”, “restricted reimbursement” or “no reimbursement”.
In case of reference drugs, there are two rules that the TLV applies to adjust costs.
• First, the “15 year rule” which gives TLV the right to reduce the price of specific pharmaceuticals which were approved for marketing more than 15 years ago. This method is mainly used for pharmaceuticals with low exposure to competition. [114]
• Second method is re-evaluation where the price is revaluated after looking in to how efficient and cost effective the use of the pharmaceutical is. [114]
Standard VAT in Sweden is 25%, but it is reduced to zero for prescription medicines.
Pricing and reimbursement (In-patient)
For hospital in-patient use, medicines are procured via a tendering process on the county level. Some counties use joint procurement. The lowest-price bidder is selected as the winner among all qualified bids. [115]
Co-payments
Patient co-payments are capped by a total yearly expenditure limit, with a decreasing share until the maximum. Patients pay the first SEK 1100 in full (100%); 50% until SEK 2100; 25% until SEK 3900 and 10% until SEK 5400. Thus, the maximum total co-payment for high-cost medicines by a patient is limited to SEK 2200 per year.
Patient co-payments are limited to outpatient use. [59]
Generic substitution and INN prescriptions
Generic substitution is generally mandatory at the doctor or pharmacist level. In 2014, Sweden revised the Act on Pharmaceutical Benefits and introduced a rule that mandates a 65% price decrease four months after generic entry if there has been a substantial price decrease in a given interchangeable group in the outpatient market. [116]
INN prescribing is not allowed in the country. The full product name needs to be on the prescription. If a generic drug have a product name that consists of the substance's generic name, then the company name must be included in the prescription. [117]
Reimbursement Out-Patient In-Patient
Involved Institution for decision, evidence assessment, appraisal and recommendation
Dental and Pharmaceutical Benefits Agency (TLV)
County councils
Interactions TLV determines prices, assesses drugs and decides on reimbursement status
Pricing mechanism Internal reference pricing, value-based pricing
Tendering process (joint or single council)
Type of reimbursement list Positive list Positive list (usually only one product per indication)
Reimbursement restrictions Product specification, patient group
Revision of decision Due to change of indication, linked to assessment of other medicine
1-2 years

Global biosimilar policy comparison
39
4.3. Market for biosimilars
4.3.1. Available biosimilars
The biopharmaceuticals market (comprising original biologics and their biosimilars) in Sweden exceeded SEK10 billion or one-fourth of the drug costs in 2015. [114]
While the first biosimilar was approved more than a decade ago, discussions around the drug category gained momentum only in the last few years in Sweden.
We have added a list of biosimilars approved for marketing in the EU in the Appendices section – List of biosimilars approved in EU to date. The table below highlights the biosimilars being reimbursed in the country. Until now, the country’s exposure to biosimilars has been limited to seven molecules — namely, etanercept, filgrastim, insulin glargine, infliximab, follitropin alfa, epoetin and somatropin. The cost of these seven substances constitutes nearly a fifth of the total costs of biological drugs in the country. [114]
Biosimilar brand name Active substance Company EMA
authorization date
Benepali etanercept Samsung Bioepis UK Limited (SBUK)
14/01/2016
Accofil filgrastim Accord Healthcare Ltd 18/09/2014
Abasaglar (previously Abasria) insulin glargine Eli Lilly Regional Operations GmbH
09/09/2014
Bemfola follitropin alfa Gedeon Richter Plc. 27/03/2014
Inflectra infliximab Hospira UK Limited 10/09/2013
Remsima infliximab Celltrion Healthcare Hungary Kft. 10/09/2013
Nivestim filgrastim Hospira UK Ltd
08/06/2010
Zarzio filgrastim Sandoz GmbH 06/02/2009
Ratiograstim filgrastim Ratiopharm GmbH 15/09/2008
Tevagrastim filgrastim Teva GmbH 15/09/2008
Retacrit epoetin zeta Hospira UK Limited 18/12/2007
Binocrit epoetin alfa Sandoz GmbH 28/08/2007
Omnitrope somatropin Sandoz GmbH 12/04/2006
Source: TLV’s drug database, accessed on 8 August 2017 [118]

Global biosimilar policy comparison
40
4.3.2. Biosimilars market share
The uptake of biosimilars in the country varies between regions. For example, as of March 2016, the uptake of biosimilar infliximab (Remicade) ranged from 0-90%. [119] It also needs to be noted that the choice of biosimilars also ranges between counties — 11 counties primarily used Remsima and eight used Inflectra as the biosimilar version of Remicade.
Additionally, there exists a variation in the use of biosimilars by their product class. Epoetin and filgrastim biosimilars have the highest percentage of use while biosimilar insulin glargine and somatropin have the lowest percentage of use in the country.
Captured below is the market share of biosimilars (in comparison with the reference product, accessible market and the total market) in the product classes of EPO, G-CSF, HGH, Anti-TNF and follitropin alpha. [10]
Source: The Impact of Biosimilar Competition in Europe, IMS (sourced from a publicly available report) [10]13
4.4. Legal framework for biosimilars
4.4.1. Market approval
The country follows a centralized regulatory pathway established by the European Medicines Agency (EMA) in 2006 (for details refer to the section on EMA’s regulatory framework on biosimilars). The national pathway for approval and regulation of new drugs in the country is defined by The Medical Products Agency (MPA). [120]
4.4.2. Pricing and reimbursement
As with all medicines, biologics for outpatient use are financed in part by subsidies from the central government to county councils, and in part by patient co-payments, whereas in-patient medicines are paid by county councils as part of the cost of treatment. [121]
Outpatient use
The TLV applies the same appraisal rules to determine price and reimbursement value for synthetic pharmaceuticals as well as biologics and biosimilars. A biosimilar must be priced at the same level or lower than the originator. [115] [122] [114]
Recent biosimilar approvals in the country show that biosimilars that provided similar benefits at a lower cost were approved for use in the country. While biosimilar products are usually priced at the same level or lower than the originator product, there does not exist any price linkage between the biosimilar and its reference drug. Based on the market trend, the country has witnessed stronger price competition for biosimilars that are used for short term treatment as against long term. [114]
Since 2014, the TLV, county councils and manufacturers have engaged in “trialogues” to decide on drug subsidies for some biosimilars (e.g. prescribed subcutaneous anti-TNFs) . In 2015/16, the TLV approved two new biosimilars Abasaglar (insulin glargine) and Benepali (etanercept) to be marketed in the counties. While both the drugs were granted subsidies to a list price lower than their respective reference products, the decision of using Benepali was made using the “trialogue” approach. The TLV
13
EPO: epoetin; G-CSF: Granulocyte-colony stimulating factor; HGH: Human Growth Hormone; TNF: Tumor Necrosis Factor; Biosimilar vs. reference product - TD biosimilars as % of TD reference products; Biosimilar vs. accessible market - TD biosimilars as % of TD accessible market; Biosimilar vs total market - TD biosimilars as % of TD total market
94%
51%
20%
94% 94%
56%
33%20% 20%
29% 29%
12%18% 15%
6%4% 2% 1%
Biosimilar vs. referenceproduct
Biosimilar vs. accessiblemarket
Biosimilar vs. total market
Biosimilar market share (% of treatment days)
EPO (2015) G-CSF (2016) HGH (2016)Anti-TNF (2016) Follitropin alfa (2016) Insulin glargine (2016)

Global biosimilar policy comparison
41
has the authority to initiate price changes to make drugs more cost effective and change re-imbursement status. [114] The “trialogue” system is not currently applied to all biosimilars, but its use is increasing.
Inpatient use
In case of inpatient use, biosimilars are financed through county tax and general government grants. County councils procure individually or jointly with other councils and negotiate prices and other terms with pharmaceutical companies through a tendering process. This involves price/ risk sharing agreements between county Councils and the manufacturers to decide on pricing and reimbursement. Contract duration and other conditions may vary between counties, making drug prices open to re-evaluation. [121] [115]
4.4.3. Switching and substitution
Interchangeability: Sweden does not have any national guidelines or recommendations on interchangeability [115]
Substitution and switching: Sweden does not have a national framework in place for switching of biosimilars. The stance varies in different counties. County councils have their individual views on treatment switching and some have instructed physicians to switch patients to cost effective biosimilar treatment options. [119]
Switching to biosimilars is the onus of the prescribing physician [114]
Automatic substitution of biosimilars is not allowed at the pharmacy level [119]
4.5. Additional factors and initiatives impacting the growth of biosimilars
4.5.1. Marketing or education initiatives regarding biosimilars
To increase awareness about biosimilar drugs in the region, some counties have special working groups that organize training courses for physicians on biosimilar treatment guidelines and follow-up treatment options. Counties also collaborate with each other to conduct training workshops for physicians on new biosimilars.
During the regulation planning for financial year 2016, the Swedish government commissioned the drug regulatory body, (TLV) to analyze development of the biological market in the presence of biosimilar competition. As part of this task, the TLV conducted a volume-based analysis of Swedish pharma prices relative to 19 European countries. [123] The report provides an understanding of effective price competition in Nordic countries for biologics and biosimilars. As part of this assessment, the TLV collaborated with representatives of industry associations, caregivers and authorities in individual meetings and seminars to propose policies that could further develop the biosimilars market in the country. [114]
4.5.2. Government incentives to increase biosimilar prescriptions
Incentives to doctors / hospitals / pharmacies
Incentives for prescribing biosimilars exist in the country. [124] [59]
Prescription quotas
Prescription budgets and quotas exist in the country for controlling prescription of expensive alternatives. These budgets and quotas may affect biosimilars in an indirect manner. [124]
Presence of prescription budgets and quotas has led to monitoring of drug prescriptions in the country. An example is the Southern Healthcare Region, where the introduction of biosimilar filgrastim led to an increased uptake in the G-CSF category on account of reduced treatment costs. Following these benefits, the authorities were forced to relax restrictions on prescriptions. Treating physicians can now prescribe biosimilar versions of the drug without obtaining a formal approval from three other physicians. [125]
4.5.3. Procurement policy
Sweden does not have any national and regional polices for the supply of biosimilars. The TLV as part of its annual assessment in 2016 has recommended increased use of dialogue with manufacturers as a procurement strategy at the national and regional level.
Some of the 21 County Councils have joint procurement of pharmaceuticals via a contract process (i.e. regional tenders): [114]
• 15 counties have procurement contracts for epoetin

Global biosimilar policy comparison
42
• 17 counties have procurement contracts for infliximab
4.5.4. Other country-specific issues that influence the introduction and adoption of biosimilars
The following local factors have led to a higher uptake of biosimilars in Sweden:
• Physicians’ level of knowledge and comfort with biosimilars • Counties’ constant efforts to introduce cost-effective biosimilars in their respective regions However, the level of biosimilar uptake is not as high as in Norway, Denmark and Finland due to greater level of decentralization owing to a lack of coordination between counties in Sweden. [114]
4.5.5. Industry position on biosimilars
Association for Generic Medicines and Biosimilars (Föreningen för Generiska läkemedel och Biosimilarer, FGL) — FGL, an industry organization with 20 member companies that actively pursues issues to protect and develop the system of generic drugs, is of the opinion that biosimilars are essential for creating downward pricing pressure on biologics in addition to reducing healthcare costs. Additionally, the body does not support automatic substitution at the pharmacy level. [114]

Global biosimilar policy comparison
43
5. Norway
5.1. Current healthcare landscape
5.1.1. Country Data
Indicator Value Year Source
Population (Mill) 5.2 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %) 1.25 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 0.85 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 16.35%
2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 59267 2016 OECD [14]
Doctors per 10,000 people 44.2 2014 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people
7.21 2014 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 37.6 2015 OECD [16]
Healthcare expenses (% of GDP) 10.5 2016 OECD [17]
Source: UN Dept. of Economic and Social Affairs, WHO and OECD
Thanks to abundant North Sea oil and gas resources, Norway enjoys one of the highest GDPs per capita in Europe, which is also reflected in its healthcare spending. Considered as a percentage of GDP, the yearly amount is in the average for Europe, but per capita, it is among the highest (with the other two big spenders, Switzerland and Luxembourg, not covered in this report). The high expenses generally translate into a high quality of service, with Norway scoring 3rd on the 2016 Euro Health Consumer Index. [111]
5.1.2. Healthcare system overview
The health system is semi-decentralized. Local municipalities are responsible for primary care, counties provide dental care14, while specialist care lies with four regional health authorities of the central government.
The Ministry of Health and its subordinate agencies are responsible for regulation and supervision of the system. The Norwegian Institute of Public Health and over 200 medical registries monitor health data and collect information on specific diseases.
The four regional health authorities (RHAs) administer delivery in their individual geographical areas in Norway (North, Middle, West and South-East). Each individual RHA is responsible for which services they wish to tender (outsource) and what services they wish their hospitals to keep in-house. They are financed by central government subsidies. [126]
GP’s are self-employed or hospital employees, and act as gatekeepers to specialist treatment. GP’s income is comprised of about 30% capitation payments, with fee-for-service as the remainder. [127]
5.1.3. Health insurance system
The healthcare system is mainly financed through municipal taxes and block grants from the central government. 85% of total health expenditure is covered by the central and local government as well as the National Insurance scheme. The remaining 15% are mostly out-of-pocket payments, including a small fixed co-payment for GP visits and expenses for pharmaceuticals and dental care. Out-of-pocket payments are limited by exemptions and ceilings. [127]
Private health insurance is additional to the coverage provided through the public national health system. However, despite this, approximately 20% of the Norwegian workforce held private insurances in 2015 – accumulating to approximately 480,000 policies in 2015. [128]
14
Free for children up to 18.

Global biosimilar policy comparison
44
5.1.4. Current issues in the healthcare system
Geographic access: With only 5 million inhabitants spread over a country with an extensive coast line of fjords and small islands, providing access to healthcare infrastructure is a major challenge that drives up costs. While GPs are fairly well-distributed, specialist care is often only available in major urban centers.
Long waiting times: The number of hospital beds is low in international comparison, and has been declining. Together with a high occupancy rate (93%), this has led to long waiting times for specialist consultation and elective treatment, which are almost as delayed as neighboring Sweden. [127]
5.2. Market for pharmaceuticals
5.2.1. Market statistics
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 2.8 BMI
World market share % 0.25 BMI
Pharmaceutical sales / capita USD 525 BMI
Pharmaceutical sales / GDP % 0.76 BMI
Pharmaceutical sales / health expenditure
% 7.2 BMI
Prescription drug sales USD bn 2.5 BMI
Patented drug sales USD bn 2.0 BMI
OTC medicine sales USD bn 0.3 BMI
Generic drug sales USD bn 0.4 BMI
Share of generics (value) % 16.0 OECD
Share of generics (volume) % 48.5 OECD
Source: BMI data tool, accessed on 25 July 2017; OECD 2014 [21]

Global biosimilar policy comparison
45
5.2.2. Market authorization and pricing
Market authorization
While Norway is not an EU member, it is part of the EEA, so marketing approval of pharmaceuticals is subject to the same regulations. They can either be approved EU-wide by the EMA in the Centralized Procedure, or locally in the Decentralized Procedure, Mutual Recognition Procedure, or National Procedure. [22]
The Norwegian Medicines Agency (NoMA) is in charge of regulations.
Pricing and reimbursement (Outpatient)
From January 2017, all medicines have to go through a HTA process for consideration from NoMA whether reimbursement should be granted or not. NoMA does not decide only based on budget impact (BI). There is a set of criteria that has to be fulfilled, and a HTA is mandatory. If BI is below 20 mill NOK NoMA may make the decision. If above the need to forward the decision to MOH. This BI-limit is to be increased to 100 mill NOK in 2018.
In the pre-approved case, NoMA requires all manufacturers to apply for a maximum pharmacy purchase price (PPP) for each prescription medicine, regardless of whether they seek reimbursement or not. Maximum prices in the retail setting are based on the average of the three lowest in 9 Northern and Western European countries (Austria, Belgium, Denmark, Finland, Germany, Ireland, the Netherlands, Sweden, and the UK). [129]
Manufacturer prices are not otherwise regulated and subject to negotiation between manufacturers and wholesalers.
Source: European Observatory on Health Systems and Policies [74]
NoMA is also responsible for evaluating and deciding whether a drug is reimbursable under the National Insurance Scheme (NIS). [130] For this, NoMA is mainly using a cost-effectiveness calculation based on QALY. Reimbursed medicines are included on a positive list called the “blue list”.
15
Includes H-prescriptions, which are initiated and prescribed in hospitals, procured and paid for by hospitals, but used outside of hospitals
Reimbursement Outpatient Inpatient15
Involved Institution for decision, evidence assessment, appraisal and recommendation
Norwegian Medicines Agency (NoMA)
NoMA, Regional Health Authority, Sykehusinnkjøp HF
Interactions - Sykehusinnkjøp HF is tasked with procurement
Pricing Free Pricing, External Reference Pricing
Tendering
Type of reimbursement list - Tender winner only
Reimbursement restrictions - -
Revision of decision - 1-2 years

Global biosimilar policy comparison
46
Pricing and reimbursement (Inpatient)
Since 2006, drugs are covered by the Regional Health Authorities (RHAs), as part of the overall treatment costs, and not charged to the National Insurance.
Some pharmaceuticals in in-patient setting are purchased through hospital tenders. Since December 2015, the four regional health authorities (RHAs) have been performing joint tenders. Conducted nationally, the tender system is a “winner takes it all” process, wherein, the medicine that wins the tender is given a “preferred use” status across the four RHAs. [131]
Hospital tenders are conducted for the following treatment areas — multiple sclerosis, tumor necrosis factor, contrast agents, hepatitis C treatment, oncology, coagulation factors, and human growth hormones. [131]
Since 2015, Sykehusinnkjøp HF, a company owned 25% by each of the regional health authorities, has been tasked with health-care related procurement for in-patient use, including drugs. [132]
• Any private company can participate in the tender (no restrictions) • Decision is not based solely on price, but also takes into account mentioned considerations such as
supply safety, quality, location of service provider, service portfolio, competence, experience etc. • The period of tenders are individual, but are usually 1-2 years, sometimes with an option for
extension of 1 year [131] [133]
Patient co-payments
The standard reimbursement rate is 62%. “Schedule 4” pharmaceuticals for serious contagious diseases (HIV, tuberculosis, syphilis etc.) are reimbursed 100%. The maximum co-payment is NKr 520 per prescription. [134]
In addition, there is a cost-sharing ceiling (egenandelstak) in place that limits total co-payments for physician treatments, including reimbursed medicines and transportation, per year. The amount is set by parliament every year (NKr 2205 in 2017). [127]
Generics and INN prescriptions
A step-system was launched in 2005 to reduce costs to the NIS. Following the patent expiry of an originator medicine, the same maximum price as for the originator is applied to generics that enter the market. This maximum price is then gradually reduced, based on a step scheme. The pre-tax maximum price of the drug is cut by a percentage in the following steps:
• Step 1: 35%, immediately after patent expiry and listing on the substitution list • Step 2: 81%, 6 months after Step 1 (if total sales revenues are over NKr 100M) • Step 3: 90%, 12 months after step 2 (if sales revenues are still over NKr 100M)
(smaller price cuts if sales revenues are lower) [135]
Since generics will have a lower manufacturer price, pharmacies can earn a higher markup on them. This acts as an indirect incentive to increase sales of generics. [136] [127] [137]
The Norwegian Medicines Agency (NoMA) compiles a pre-approved substitution list for drugs (generic substitution). This list includes original medicine and their pre-approved generics. If a physician has prescribed an original medicine, and not set any reservation in the prescription, a pharmacy is free to substitute the original medicine with a generic if either they do not have the original medicine in stock or a tender process advises them to do so. [138]
Pharmacists are required to inform the patient about available cheaper alternatives. If the patient refuses substitution, he or she has to pay the difference out of pocket, unless the prescriber has ruled out substitution. [136]
Substitution with parallel imports is allowed. Norway does not allow therapeutic substitution16. [136]
INN prescribing is allowed but it is not mandatory. Doctors are required to prescribe the cheapest alternative unless there is a serious medical reason for a more expensive alternative. For some therapeutic equivalent groups, a so-called “first choice” exists, usually a generic. [136]
16
Therapeutic substitution: Substitution with a different molecule with the same therapeutic effect

Global biosimilar policy comparison
47
5.3. Market for biosimilars
5.3.1. Available biosimilars
As of June 2017, the following biosimilars are actively marketed in the country:
Biosimilar brand name
Active substance
Company Authorization
date Status
Rixathon Rituximab Sandoz GmbH 15/06/2017 Marketed
Benepali Etanercept Samsung Bioepis UK Limited (SBUK) 14/01/2016 Marketed
Abasaglar (previously Abasria)
insulin glargine Eli Lilly Regional Operations GmbH 09/09/2014 Marketed
Bemfola follitropin alfa Gedeon Richter Plc. 27/03/2014 Marketed
Ovaleap follitropin alfa Teva Pharma B.V. 27/09/2013 Marketed
Inflectra infliximab Hospira UK Limited 10/09/2013 Marketed
Remsima infliximab Celltrion Healthcare Hungary Kft. 10/09/2013 Marketed
Nivestim filgrastim Hospira UK Ltd 08/06/2010 Marketed
Zarzio filgrastim Sandoz GmbH 06/02/2009 Marketed
Tevagrastim filgrastim Teva GmbH 15/09/2008 Marketed
Retacrit epoetin zeta Hospira UK Limited 18/12/2007 Marketed
Omnitrope somatropin Sandoz GmbH 12/04/2006 Marketed Source: Norwegian Medicines Agency Database, accessed on 8 August 2017 [139];
The following medicines have been approved, but they are not currently marketed [140]
Biosimilar brand name
Active substance
Status
Abseamed epoetin alfa Approved
Binocrit epoetin alfa Approved
Epoetin alfa Hexal epoetin alfa Approved
Silapo epoetin zeta Approved
Accofil filgrastim Approved
Filgrastim Hexal filgrastim Approved
Grastofil filgrastim Approved
Ratiograstim filgrastim Approved
Flixabi infliximab Approved

Global biosimilar policy comparison
48
5.3.2. Biosimilars market share
Captured below is the market share of biosimilars (in comparison with the reference product, accessible market and the total market) in the product classes of EPO, G-CSF, HGH, Anti-TNF and follitropin alpha. [10] The data shows that anti-TNFs have had a strong uptake in the country.
Source: The Impact of Biosimilar Competition in Europe, IMS (sourced from a publicly available report) [10]17
5.4. Legal Framework for biosimilars
5.4.1. Market approval
Approval pathway: The country follows a centralized regulatory pathway established by the European Medicines Agency (EMA) in 2006 (for details refer to the section on EMA’s regulatory framework on biosimilars) [141]
The national pathway for approval and regulation of new drugs in the country is defined by the Norwegian Medicines Agency (NoMA). [114] All drug manufacturers need to file for a market authorization to NoMA and once approved, the authorization lasts for five years. [142]
5.4.2. Pricing and reimbursement
The pricing and market access process for biosimilars is same as that for other pharmaceutical products. While cost effectiveness is the most important parameter for reimbursement of a drug, there are additional criteria that NoMA assesses in an application: [130]
• The drug is used in treatment of serious diseases (or risk factors that lead to a serious disease) that require a long treatment duration
• The clinical efficacy of the drug is well documented in a defined and appropriate patient population • NoMA rewards reimbursement status to a drug if fulfills the above criteria and its costs is below a
“bagatelle threshold”. In case the drug costs above the set threshold, NoMA forwards its recommendation to the Ministry of Health and Care Services (HOD) for political consideration and decision-making at the ministry or in parliament. [130]
Government regulation on biosimilars pricing and reimbursement (outpatient)
Pricing and reimbursement for outpatient biologics follows the process described in 5.2.2.2.
• Filgrastim, somatropin and epoetin were transferred from NHI to hospital funding for both hospital and home use. This puts their funding into the hands of the regional health authority, and opens the option of a national tender to also cover outpatient use. [143]
17
EPO: epoetin; G-CSF: Granulocyte-colony stimulating factor; HGH: Human Growth Hormone; TNF: Tumor Necrosis Factor; Biosimilar vs. reference product - TD biosimilars as % of TD reference products; Biosimilar vs. accessible market - TD biosimilars as % of TD accessible market; Biosimilar vs total market - TD biosimilars as % of TD total market
87%
44%
4%
86% 86%
5%
29%
15% 15%
82% 82%
53%
35%
21%
9%1% 1% 0%
Biosimilar vs. referenceproduct
Biosimilar vs. accessiblemarket
Biosimilar vs. total market
Biosimilar market share (% of treatment days)
EPO (2015) G-CSF (2016) HGH (2016)
Anti-TNF (2016) Follitropin alfa (2016) Insulin analog

Global biosimilar policy comparison
49
Government regulation on biosimilars pricing and reimbursement (hospital) Most biologics fall within the six specified treatment areas for national-level hospital tenders — multiple sclerosis, tumor necrosis factor, contrast agents, hepatitis C treatment, oncology, coagulation factors, and growth hormones. Therefore, some biosimilars are subject to tenders and can receive preferred status, e.g., filgrastim, while there are no tenders in other areas. [131]
Current market pricing As a trend, the country has witnessed relatively higher discounts when compared to other European nations. For example, Remsima offered 69% discount in the tender closed in February 2015. [144]
5.4.3. Switching and substitution Switching: Switching is permissible and is a common practice among physicians. [11]
Automatic substitution: The country has a national pre-approved substitution list, issued by the National Medicine Agency. Currently, biosimilars do not form part of this pre-approved list and hence cannot be automatically substituted. Since, June 2017, NoMA and the Norwegian Pharmacy Association have been considering the inclusion biosimilars on this list. [145]
5.4.4. INN prescribing INN prescribing for biosimilars is not allowed in the country.
5.5. Additional factors and initiatives impacting the growth of biosimilars
5.5.1. Marketing or education initiatives regarding biosimilars In its efforts to make data available and eliminate concerns pertaining to physician led switching of biosimilars, the Norwegian Health Ministry granted NOK20mn to conduct the ‘NOR-SWITCH’ study in 2014. The aim of NOR-SWITCH was to examine switching from originator infliximab to the less expensive biosimilar CT-P13 regarding efficacy, safety, and immunogenicity.
Results from the NOR-SWITCH trial have showcased that switching from Remicade to Remsima is non-inferior to continued treatment with Remicade. [146]
5.5.2. Government incentives to increase biosimilar prescriptions
Incentives to doctors / hospitals / pharmacies There are strong financial incentives in place for hospitals to promote the use of biosimilars. Procurement of drugs in a hospital setting is carried out by “Sykehusinnkjøp”, the national procurement company through multiple yearly tenders. Prescribing physicians are required to prescribe the tender winning drug. [147]
5.5.3. Procurement policy
Through the Norwegian drug procurement cooperation (Sykehusinnkjøp HF), the government replaced biologics with biosimilars as the official choice of medication in indications like rheumatoid arthritis, ankylosing spondylitis, Crohn’s disease, and ulcerative colitis.
5.5.4. Other country-specific issues that influence the introduction and adoption of biosimilars
• Patients usually follow the advice of the physicians when they are switched from a biologic to a biosimilar [11]
• Payers show least interest in engaging multiple biosimilar manufacturers as they prefer a single-winner tender process. Therefore, there is generally no market share for second or third lowest bidder in the tender process. [11]
• High acceptance of biosimilars among physicians [11]
5.5.5. Industry position on biosimilars Legemiddelindustrien (LMI) — The LMI which is the pharmaceutical industry association in Norway advocates the role of biosimilars in achieving healthcare savings and providing patients with access to innovative treatment options. LMI is of the opinion that switching should occur only if there exists strong scientific evidence to support interchangeability between a biosimilar and its reference product.
The association stresses the importance of pharmacovigilance, particularly those which fall under the “black triangle”18
category. [148]
18
A drug falling under this category requires surveillance of adverse drug reactions that may occur from its usage

Global biosimilar policy comparison
50
6. United States
6.1. Current healthcare landscape
6.1.1. Country data
Indicator Value Year Source
Population (Mill) 319.93 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %)
0.72 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 46.84 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 14.64% 2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 57325 2016 OECD [14]
Doctors per 10,000 people 25.54 2013 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people
8.87 2010 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 28.3 2014 OECD [16]
Healthcare expenses (% of GDP) 17.2 2016 OECD [17]
Source: UN Dept. of Economic and Social Affairs, WHO and OECD
The US has the highest spending on healthcare as part of GDP (17.2%) worldwide, as well as the highest per capita spending on pharmaceuticals (USD 1112). Meanwhile, a common criticism is that these high levels of spending do not translate into better health results.
6.1.2. Healthcare system overview
Unlike the other countries in covered in this report, the US does not have a universal healthcare system, opting instead for a mixed system of private, usually employer-based health insurance in combination with public health insurance schemes (Medicare, Medicaid, CHIP) for specific population groups as well as the Veterans Health Administration (VHA). A significant share of the population, 29 million people or 9.1% of the population, did not have health insurance in 2015. [149] [150]
Providers are a mix of public and private bodies. In 2017, of 5,564 US general hospitals, 2,845 (51.1%) were private non-profit community hospitals, 1,034 (18.6%) were for-profit, 17.7% were state or local government community hospitals, and 212 were federal hospitals (3.8%). [151]
6.1.3. Health insurance system
Overall, healthcare expenditures are split between 33.4% private health insurance, 20.2% Medicare, 17.0% Medicaid (10.7% federal and 6.3% state and local), 0.5% CHIP, 10.5% out-of-pocket expenses, and 18.4% other payers (defense and veteran affairs, other programs, public health, research and investment) [152]
Medicare
Medicare is a single-payer, national social insurance program administered by the US federal government, currently using about 30–50 private insurance companies across the United States under contract for administration. United States Medicare is funded by a 2.9% payroll tax, premiums and surtaxes from beneficiaries, and general revenue. It provides health insurance for Americans aged 65 and older who have worked and paid into the system through the payroll tax. It also provides health insurance to younger people with certain disabilities.
Medicaid
Medicaid is a social health care program for 68.9M low-income families and individuals (in 2017 [153]). It is a means-tested program that is jointly funded by the state and federal governments and managed by the states. Each state decides the criteria for categories of eligibility and the details of implementation. The model for roughly 80% of enrollees is a managed care program, under which Medicaid recipients are enrolled into a private health plan, which receives a fixed monthly premium from the state. The health plan is then responsible for providing for all or most of the recipient's healthcare needs. Other recipients are covered by a fee-for-service model.

Global biosimilar policy comparison
51
CHIP
CHIP is a US Department of Health program that in some states, matches state funds to provide healthcare to 5.6M children (in 2017 [153]) in families that do not qualify for Medicaid. In some states, it also covers pregnant women. [154]
VHA
The Veterans Health Administration (VHA) is the component of the United States Department of Veterans Affairs that implements the medical assistance program of the VA through the administration and operation of numerous VA Medical Centers, Outpatient Clinics and other institutions to provide healthcare to over 9M enrolled veterans. [155]
6.1.4. Current issues in the healthcare system
Chronic illness and obesity: More than one-third (36.5%) of U.S. adults have obesity, increasing rates of obesity-related conditions such as heart disease, stroke, type 2 diabetes and certain types of cancer. The estimated annual medical cost of obesity in the U.S. was $147 billion in 2008 USD; the medical costs for people who are obese were USD 1,429 higher than those of normal weight. [156]
Healthcare reform: As of the time of writing of this report, a replacement or repeal of the Affordable Care act is being discussed in both chambers of Congress. Depending on the outcome of the debate, there would be sweeping changes to the healthcare system.
Uninsured population: Reducing the number of uninsured was one of the main policy goals of the Patient Protection and Affordable Care Act. By 2015, this number had been reduced to 29 million. The impact of a repeal or reform of the act on that number remains a key question. [149] [150]
High drug prices: The US has the highest per-capita spending on prescription drugs in the world. In a 2016 report, researchers at Harvard Medical School listed the following reasons: the ability of pharmaceutical companies to set their own prices, patent protection and exclusivity, long delays in the approval of generics, and requirements for patient consent in pharmacy-level switching. [157] [158]
6.2. Market for pharmaceuticals
6.2.1. Market statistics
The US is the largest market for pharmaceuticals worldwide at a 33% share, way ahead of #2 Japan. Its total market size is a factor of high individual consumption, higher consumption of more expensive medicines, and high prices for individual drugs in international comparison.
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 362.1 BMI
World market share % 32.57 BMI
Pharmaceutical sales / capita USD 1117 BMI
Pharmaceutical sales / GDP % 1.95 BMI
Pharmaceutical sales / health expenditure
% 11.0 BMI
Prescription drug sales USD bn 342.4 BMI
Patented drug sales USD bn 270.2 BMI
OTC medicine sales USD bn 19.7 BMI
Generic drug sales USD bn 72.2 BMI
Share of generics (value) % 28% OECD
Share of generics (volume) % 86% OECD
Source: BMI data tool, accessed on 25 July 2017; OECD 2014 [21]

Global biosimilar policy comparison
52
6.2.2. Market authorization and pricing
Market authorization
Responsibility for the marketing approval of both prescription and OTC drugs lies with the Center for Drug Evaluation and Research (CDER) of the U.S. Food & Drug Administration (FDA). For some biologics, such as vaccines, the Center for Biologics Evaluation and Research (CBER) is responsible instead. As a result, regulation and oversight is shared between the two centers within the FDA. [159] [160]
Pricing
Pharmaceutical firms are able to set their own prices on the US market. They are subject to negotiation between manufacturers and wholesalers. Pricing between wholesalers and pharmacies / hospitals is also subject to negotiation.
Free pricing also extends to generics.
Medicare, medicaid, VHA
Medicaid and the US Veterans Health Administration have used their buyer power to cap drug prices. The VHA uses a formulary (positive list) to limit the number of reimbursed drugs. Products are categorized in therapeutic classes. To secure lower drug prices, the VHA has declared several classes as closed. Within a closed class, the VHA enters contracts with only a limited number of manufacturers and commits to a certain level of usage in exchange for volume discounts. A second, less restrictive policy applies to preferred classes, where certain brands are still purchased under a volume contract, but products other than the preferred products can still be used. [161]
For Medicaid, pricing policy is a lot more fractured, as the system is supported by the federal government but administered by individual states. All states have instituted a form of coverage for outpatient prescription drugs and some OTC drugs, but who is covered, what is covered and to what degree all varies. Manufacturers who wish their drugs to be reimbursed by Medicaid enter a national rebate agreement with the federal government, which requires a rebate from the average manufacturer price (AMP) between 13% for generics and 23.1% for innovator drugs. The AMP is the average price of the drug to wholesalers across the US, reported monthly. [161] [162]
On top of that, individual states (or pools of states) enter supplemental rebate agreements with individual manufacturers. [161]
Some of outpatient prescription drugs are included in Medicare Part B such as injectable drugs administered by a physician; oral anticancer drugs and immunosuppressive drugs; drugs used in conjunction with durable medical equipment; and some vaccines. It also mandated the Office of Inspector General (OIG) to compare ASPs with average manufacturer prices (AMPs) and instructed CMS to substitute amount of payment for drugs with ASPs that exceed 5 percent threshold above AMPs. OIG has completed 29 quarterly pricing comparisons since the ASP reimbursement methodology for Part B drugs was implemented in January 2005 to comply with its statutory mandate. In accordance with its published price substitution policy which currently applies to only certain codes with complete AMP data, CMS began substituting amount of payment in April 2013. [163]

Global biosimilar policy comparison
53
6.3. Market for biosimilars
6.3.1. Available biosimilars
Out of the seven approved biosimilars in the US under section 351(k) pathway, three have been launched in the market. Below is a list of biosimilars that are available for sale in the US market: [164] [165]
Biosimilar brand name Active substance Company
Date of licensure
Commercialization status
Inflectra infliximab-dyyb Celltrion and Pfizer 05/04/2016 Marketed [166]
Zarxio filgrastim-sndz Sandoz 06/03/2015 Marketed [167]
Renflexis infliximab-abda Samsung Bioepis and Merck Sharp & Dohme Corp
21/04/2017 Marketed [168]
Amjevita adalimumab-atto Amgen 23/09/2016 Market entry delayed until 2023 [169]
Erelzi etanercept-szzs Sandoz 30/08/2016 Not marketed until 2018 [170]
Cyltezo adalimumab-adbm Boehringer-Ingelheim 25/08/2017 Not marketed due to patent litigation [171]
Mvasi bevacizumab-awwb Amgen 14/09/2017 Not marketed (originator patent protected until 2019) [172]
Source: US FDA, NASDAQ, GlobalNewswire, accessed on 9 August 2017 [165] [164]
In the U.S., Lantus and other insulins are regulated under the Federal Food, Drug and Cosmetic Act like other drugs, and they are not treated specifically as biological products under the Public Health Service (PHS) Act, so they cannot act as the reference product for a biosimilar. Because of this, Eli Lilly’s Basaglar was approved through the 505(b)(2) regulatory pathway for follow-on drugs. [173]
6.3.2. Biosimilars market share
Currently, there are three biosimilars launched in the US market.
In the G-CSF / filgrastim field, Zarxio had achieved a market share (by volume) of 50% against its originator, Neupogen by the end of 2016. [174]
For TNF inhibitors / infliximab, Inflectra has managed to gain only 2.3% against the originator Remicade by end of June 2017, according to a Pfizer investor report. [175]
6.3.3. Market outlook
The biosimilars market in the US is expected to exhibit high growth and become the main driver for biosimilars growth globally. The market size (US$ million) of biosimilars in the US is as follows:
Source: Global biosimilars market (2016-2020), Technavio
145
1,348.30
2015 2020E
US$ millions
CAGR: 52.6%

Global biosimilar policy comparison
54
6.4. Legal framework for biosimilars
6.4.1. Market approval
The Patient Protection and Affordable Care Act (ACA) was signed into law in 2010. This Act paved the way for the creation of an abbreviated approval pathway for biologic products that are believed to be highly similar (biosimilar) or interchangeable with a reference biologic.
According to the New York Pharma Forum’s report, congress passed the Biologic Price Competition and Innovation Act (BPCIA), which is separate from ACA, in 2010. BPCIA created the pathway to biosimilars through an abbreviated Biologics License Application (“aBLA”), in which applicants show that its product is “biosimilar” and “interchangeable” and can receive an approval in a simplified pathway than a traditional Biologics License Application (“BLA”). [176]
In April 2015, the US FDA issued final guidelines on the key requirements for demonstrating biosimilarity under the section 351(k) pathway (also known as abbreviated licensure pathway for biosimilars).
The US FDA has released final versions of the following guidance documents to support the manufacturers:
• Scientific considerations in demonstrating biosimilarity to a reference product • Quality considerations in demonstrating biosimilarity of a therapeutic protein product to a
reference product • Clinical pharmacology data to support a demonstration of biosimilarity to a reference product • Biosimilars: questions and answers regarding implementation of the biologics price competition and
innovation act of 2009 guidance for industry
The below listed guidance are in a draft stage:
• Reference product exclusivity for biological products filed under section 351(a) of the Public Health Service (PHS) Act
• Biosimilars: additional questions and answers regarding implementation of the biologics price competition and innovation act of 2009
• Considerations in demonstrating interchangeability with a reference product guidance for industry [164]

Global biosimilar policy comparison
55
The table below gives a broad overview of the biosimilars regulatory approval landscape in the US:
Parameter Regulatory provision in US
Definition Biosimilars are biological products that are highly similar to the reference product, notwithstanding minor differences in clinically inactive components. There are no clinically meaningful differences between a biosimilar and its reference product in terms of the safety, purity, and potency. [177]
Reference product Reference product is the single biological drug which is licensed under section 351(a) of the PHS Act, against which a biosimilar is. [177]
Reference product exclusivity (draft guidance released in August 2014)
The Draft Exclusivity Guidance provides clarification on the following three provisions in Section 351(k)(7)(C): • “licensor, predecessor in interest, or other related entity” • “modification to the structure of the biological product” • “does not result in a change in safety, purity, or potency” [178]
General requirements
A 351(k) application must include the following information to demonstrate that the biological product: • �is a biosimilar to the reference product • �has the same mechanism of action for the proposed condition of use • condition of use proposed in labeling have been approved for the reference product • has the same route of administration, dosage form, and strength as the reference product • is manufactured, processed, packed, or held in a facility that meet standards that are
designed to assure that the biological product continues to be safe, pure, and potent The PHS Act requires that a 351(k) application must include the following information for demonstrating biosimilarity based upon data derived from: • Analytical studies — demonstrating that the biological product is “highly similar” to the
reference product, notwithstanding minor differences in clinically inactive components; • �Animal studies — including the assessment of toxicity • Clinical studies — including the assessment of immunogenicity and pharmacokinetics (PK)
or pharmacodynamics (PD) that are sufficient to demonstrate safety, purity, and potency in one or more appropriate conditions of use for which the reference product is licensed and for which licensure is sought for the biosimilar product [177]
In a nutshell, the US FDA considers the totality of the data and information submitted in the application which includes the structural and functional characterization, nonclinical evaluation, human PK and PD data, clinical immunogenicity data, and comparative clinical study data. [179]
Non-US-licensed comparator products
Non-US-licensed products can be used as a comparator for approving a biosimilar however, bridging studies are required. The type of bridging data needed would include the following: • Direct physico-chemical comparison of all three products (proposed biosimilar to US-
licensed reference product; proposed biosimilar to non-US-licensed comparator product; US-licensed reference product to non-US-licensed comparator product)
• Likely three-way bridging clinical PK and/or PD study �including all three pair-wise comparisons. These should meet the pre-specified acceptance criteria for analytical and PK and/or PD similarity. [177]
Naming (final guidance released in January 2017)
A four-letter (in lowercase) random suffix is required to be added to the International Nonproprietary Name (INN). This is done to differentiate between the originator and the biosimilar to aid pharmacovigilance. [180]
Labelling (draft guidance issued in March 2016)
The label should not include that there is no meaningful clinical difference between biosimilar and its reference biologic. Instead, the label should contain a description of data that supports the safety and efficacy of the reference biologic. [181]
180-day notice of commercial marketing is not mandatory
The ruling of US Supreme court in June 2017, will speed up the biosimilar approval process in the US so that the biosimilar manufacturing company will not have to wait to launch the biosimilar for an additional six months after the US FDA has approved the biosimilar. This ruling is a result of the case between Amgen (biologic manufacturer) and Sandoz (subsidiary and generic / biosimilar manufacturer of Novartis) [182]
Extrapolation of indications
The guidance of the US FDA outlines the following factors that should be considered while providing a scientific justification for extrapolation: • MOA(s) in each condition of use for which licensure is required • PK and bio-distribution of the product in different patient populations • immunogenicity of the product in different patient populations • differences in expected toxicities in each condition of use and patient population [177]
E.g. of extrapolation of indications: The US FDA has approved Zarxio for all the five indications for which Neupogen has been approved, even though Sandoz conducted clinical trials for Zarxio in only one approved indication of Neupogen. [183]

Global biosimilar policy comparison
56
6.4.2. Pricing and reimbursement
There are no specified guidelines on the pricing of biosimilars in the US, but the country has separate reimbursement policies in case of public payers. For payments and discounts, Centers for Medicare & Medicaid Services (CMS) sets the prices that serve as a base for private insurers. CMS has approved biosimilars into the Average Sales Price (ASP) payment methodology and has issued additional guidelines. [184] [185]
Both Zarxio and Inflectra were launched at 15% discount vs. their reference biologics [186] [187].
CMS expects that the biosimilars will be priced at 15-30% discount to the reference products. [185]
Medicare and medicaid
Medicare Part B — From January 2016 to 1 January 2018, biosimilars reimbursed under Medicare Part B, were set a coding policy by the CMS which grouped all the biosimilars of a single reference product under the same Healthcare Common Procedure Coding System (HCPCS) code, called a J-code. Payment of the biosimilars under Medicare Part B was based on products’ average sales price (ASP) for all biosimilars included within the same HCPCS code. [188] Additional amount of 6% of the ASP for the reference product is added. From January 1, 2018, newly approved biosimilar biological products with a common reference product will no longer be grouped into the same billing code.
The new policy ensures all biosimilars will have independent J-codes and will therefore rely on their individual ASPs for reimbursement. Once the ASP is established, each biosimilar will be reimbursed at its ASP plus 6% of the reference biologic’s ASP.
In response to the decision, CMS indicated that “a solution that increases provider and patient choice is superior to existing policy and may lead to additional cost savings over the long-term. By encouraging innovation and greater manufacturer participation in the marketplace, we believe that this policy change will result in the licensing of more biosimilar products, thus creating a stable and robust market, driving competition and decreasing uncertainty about access and payment. Carrying out this policy change as early as possible, rather than waiting, is expected to bring more certainty to the new and developing marketplace”. [189]
Medicare Part D — Under the Patient Protection and Affordable Care Act of 2010, pharmaceutical manufacturers should provide a 50% discount on branded drugs to patients in the coverage gap. However, under the CMS's biosimilars regulation for Part D rules sponsors published in March 2015, biosimilars are excluded from this obligation which may make them more expensive than the branded originals under Medicare Part D. The cost benefit that biosimilars are proposed to provide is likely to be cancelled by the 50% discounting policy for originator products under Medicare Part D.
Medicaid — Biosimilars are likely to be incorporated on the preferred drug lists of states' Medicaid programs. This would mean that they will not require prior authorization like non-preferred products. However, biosimilar manufacturers would most likely have to offer additional rebates on top of the statutory 23.1% rebate (rather than 13.1% rebate on generics) of the average manufacturer price that will be required for all biosimilar manufacturers according to CMS rules. [181]
Payment limits for biosimilars by CMS from 1 July 2017 to 30 September 2017 is as follows: [190]
HCPCS code Biosimilar HCPCS code dosage Payment limit (US$)
Q5101 Zarxio 1 microgram 0.73
Q5102 Inflectra 10 milligram 80.192 Source: US FDA, accessed on 9 August 2017 [190]
6.4.3. Switching and substitution
Interchangeability (draft guidance released in Jan 2017): The draft guidelines recommend a step-wise approach for interchangeability criteria which includes the following:
• Similar clinical results in any given patient • Similar risks in safety and efficacy if switched back and forth multiple times between biosimilar and
a reference biologic
This new guidance will assist sponsors in proving that a proposed therapeutic protein product is interchangeable with a reference product for the purposes of submitting a marketing application or supplement under section 351(k) of the Public Health Service Act (PHS Act). Interchangeable products may be substituted for the reference product without the intervention of the prescribing health care provider.
Switching: A physician can prescribe a biosimilar in place of the FDA-approved reference product. [191]

Global biosimilar policy comparison
57
Substitution: The policy on substitution is decided and implemented by the individual states in the US. The substitution is only allowed for biosimilars that are designated as interchangeable by the US FDA in the community setting. Currently, 35 of 50 US states and Puerto Rico support biosimilar substitution through state laws. [192] [177] In the hospital setting, substitution can take place without designation of interchangeability or physician notification based on advanced protocols that are commonly developed by institutional pharmacy and therapeutics committees. [193]
Legislation on biologics and biosimilar substitution, 2013-2017 [192]
Source (map): National Conference of State Legislatures, accessed on 10 August 2017 [192]
6.4.4. INN prescribing
INN prescribing of biologics is not allowed. A health care professional has to write the specific name of the brand on the prescription. [191]
6.5. Additional factors and initiatives impacting the growth of biosimilars
6.5.1. Marketing or education initiatives regarding biosimilars
The following steps have been taken by the US FDA to promote use of biosimilars in the US:
• Released “Purple Book” — this book lists biological products, including biosimilars and interchangeable biological products, licensed by the US FDA under the PHS Act. [194]
• Developed a free, continuing education course on biosimilars for health care professionals named, ‘FDA Overview of Biosimilar Products’ — the objective of this course is to increase the knowledge and understanding of biosimilars for health care professionals. [195]
• Organized two basic webinars (part 1 and part 2) on biosimilars and biological products in 2013. [196] [197]
Separately, the Biosimilars Forum (a nonprofit organization for increasing patient access to biosimilars in the US) launched a biosimilars education initiative ‘Partnership for Biosimilars Education and Access’ in 2016. The focus of this initiative is to increase awareness and encourage access of biosimilars. The Forum has released two educational guides on biosimilars for health professionals, media, and patient advocacy groups. These education guides provide background, insights, FAQs, and resources on biosimilars. [198] [199]
NY 2017
PA2016
ME
H VT
MI
ND 2013
KS 2017
SC2017
NC2015
ALMS
LA 2015
AR
TX 2015
NM AZ
2016
WY
MT 2017 ID
2016
WA 2015
OK
CO 2015
UT 2013, 2015
NV 2017
TN2015
OR 2013,
2016
CA 2015
IA2017
WI
MN 2017
## SD
MO 2016
IL 2015
NE 2017
GA 2015
WV VA
2013
FL 2013
KY2016
IN2014
OH2016
MA 2014 RI 2016
CT NJ 2015 DE 2014 MD 2017 DC
HI
Enacted law, 2013-17
Filed; failed/adjourned 2013-17 Don’t have a law, 2013-17
WV

Global biosimilar policy comparison
58
6.5.2. Government incentives to increase biosimilar prescriptions
Incentives to doctors / hospitals / pharmacies
Medicare Part B pricing rules provide an indirect incentive to prescribing physicians. As per Centers for Medicare & Medicaid Services (CMS) recommendation, a biosimilar will have unique HCPCS billing code as the reference biologic. The lower manufacturer sales price of the biosimilar is considered into the weighted average sales price (ASP) paid by a physician, thus increasing the margin on the lower-priced biosimilar and decreasing the margin on the reference product, giving an indirect incentive to prescribe the biosimilar. [200] [188]
Prescription quotas
There are no prescription quotas for physicians in the US for biosimilars.
6.5.3. Other country specific issues that influence the introduction and adoption of biosimilars
US payers are in favor of using biosimilars. This can be demonstrated from the following points:
• CVS Health (Pharmacy benefit manager) replaced Neupogen with its biosimilar Zarxio on the formulary in 2017. [201]
• According to a survey of 40 different payers conducted by Amgen (published in 2016) in the US, payers anticipate that biosimilars will decrease specialty drug prices and biosimilars represents a compelling opportunity [202]
• According to J P Morgan’s US payer survey (March 2017), biosimilars’ relative costs/ associated savings are the most likely drivers of formulary inclusion for the payers in the US [203]
The FY 2017 CMS budget includes proposals to increase the availability of generics and biologics as below:
• This proposal increases competition for biological products by reducing the number of years (from 12 to 7) that manufacturers have exclusivity or monopoly pricing power and prohibiting additional years of exclusivity due to minor formulation changes
• It also modifies how Part B pays for biosimilar and innovative biological products. For these products, reimbursement would be based on the weighted average sales price of the reference biological product and all of its biosimilars
• In both Medicare and Medicaid, it saves money (e.g. $6.9 billion in Medicare savings over 10 years) [204]
6.5.4. Industry position on biosimilars
Pharmaceutical Research and Manufacturers of America (PhRMA) According to PhRMA, patient safety is paramount concern when considering the naming of biosimilars. Use of different non-proprietary names will assist the attribution of potential adverse events to the correct biologics, which in turn will enable detection of any safety differences between the biologics. These names will also ensure that the physician decisions about the treatment choices for individual patients are respected, and prevent errors in the prescribing, dispensing and administration of biologics. To avoid confusion between and among biologics, an internationally consistent biological qualifier (BQ) should be added and should be used in all circumstances where the INN (e.g., “INN-BQ”) are used. [205]
Biosimilars Forum The body has disagreed with the recommendation of CMS to group all biosimilars of a single reference product under the same HCPCS code. [206] . The Forum issued a positive media release following the decision by the CMS to reverse the policy indicating that it is a huge win for patients and that it will ensure a robust and competitive biosimilars market. [207]
Institute for Patient Access The association is against the current state laws which allow pharmacist to substitute a biosimilar for a biologic product under circumstances without notifying to the physician. This is due to underlying difference between the biosimilar and biologic product which may cause an adverse event in the patient. [192]
America's Health Insurance Plans The body is in favor of removing the barriers that limit the uptake of biosimilar. E.g. the US FDA needs to finalize its guidelines that will determine when a biosimilar drugs is truly interchangeable with an already approved biologic. [192]

Global biosimilar policy comparison
59
7. Canada
7.1. Current healthcare landscape
7.1.1. Country data
Indicator Value Year Source
Population (Mill) 35.95 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %)
1.02 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 5.81 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 16.16% 2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 44025 2016 OECD [14]
Doctors per 10,000 people 24.77 2012 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people
9.25 2013 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 25.8 2016 OECD [16]
Healthcare expenses (% of GDP) 10.3 2016 OECD [17]
Source: UN, Dept. of Economic and Social Affairs, WHO/Europe, HlthResDB, OECD, BMI
7.1.2. Healthcare system overview
Health services in Canada are mostly administered, provided and funded by the 10 provinces and 3 territories. Each regional government offers a universal health insurance plan in accordance with the Canada Health Act.
The federal government sets national principles and provides funding support. It also provides direct healthcare services to certain groups of people, such as First Nations, Inuit, armed service members and veterans.
Healthcare delivery is two-tiered. Primary care is provided either by doctors in private practice, paid through fee-for-service schedules that are negotiated between each regional government and the medical professions in their jurisdictions, or by salaried doctors in clinics, community health centers and group practices.
Secondary services include specialized care at a hospital. The majority of Canadian hospitals are operated by community boards of trustees, voluntary organizations or regional health authorities established by provincial/territorial governments. Hospitals are generally funded through annual, global budgets that set overall expenditure targets or limits (as opposed to fee-for-service arrangements) negotiated with the provincial and territorial ministries of health, or with a regional health authority or board. Although global funding continues to be the principal approach for hospital reimbursement in Canada, a number of provinces have been experimenting with supplementary funding approaches. [208]
7.1.3. Health insurance system
Each Canadian territory and province provides its own health insurance plan. In total, the system is known as Medicare. Each health insurance plan covers medically necessary hospital and doctor services, pre-paid, without charges at the point of service.
The Canada Health Act requires these plans to cover: hospital services provided to in-patients or out-patients, if the services are medically necessary for the purpose of maintaining health, preventing disease or diagnosing or treating an injury, illness, or disability; and medically required physician services rendered by medical practitioners. Note that the definition of “medically necessary” services is decided by the province or territory, leading to regional differences in service levels and expenses.
In addition, different provinces have chosen cover other services, either to the entire population or specific groups (e.g. children, seniors, social assistance recipients), either partially or fully. Examples include prescription drugs, dental care, optometric, chiropractic, and ambulance services.
Each province and territory chooses the method of financing its health insurance plan, through the payment of premiums (as in British Columbia), payroll taxes, sales taxes, other provincial or territorial revenues, or by a combination of methods. Health insurance premiums are permitted as long as residents are not denied coverage for medically necessary hospital and physician services because of an inability to pay such premiums. [209]

Global biosimilar policy comparison
60
7.1.4. Current issues in the healthcare system
Wait times: Long wait times, especially for specialist treatment, have become an issue. Healthcare authorities have started addressing the issue with measures such as training and hiring more health professionals; clearing backlogs of patients requiring treatment; building capacity for regional centers of excellence; expanding ambulatory and community care programs; and developing and implementing tools to better manage wait times. [208]
Drug Pricing: The Canadian Minister of Health has stated that “Canadians are paying too much for prescription drugs” in a May 16, 2017 press release and announced the launch of a process to modernize price regulations. [210]
7.2. Market for pharmaceuticals
7.2.1. Market statistics
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 19.5 BMI
World market share % 1.75 BMI
Pharmaceutical sales / capita USD 537 BMI
Pharmaceutical sales / GDP % 1.29 BMI
Pharmaceutical sales / health expenditure
% 12.0 BMI
Prescription drug sales USD bn 15.5 BMI
Patented drug sales USD bn 11.3 BMI
OTC medicine sales USD bn 4.0 BMI
Generic drug sales USD bn 4.2 BMI
Share of generics (value) % 33.1% OECD
Share of generics (volume) % 64.3% OECD
Source: BMI data tool, accessed on 25 July 2017; OECD 2014 [21]
7.2.2. Market authorization and pricing
Market authorization
Marketing authorization for OTC and prescription drugs is performed by Health Canada. [211]
Pricing and reimbursement
Pricing Mechanism Yes / No Comment
Free Pricing Yes Off-patent drugs only
External Reference Pricing Yes Patent drugs; use median of 7 countries to set comparison to set Maximum Average Potential Price
The Patented Medicine Prices Review Board (PMPRB), a federal agency, establishes a Maximum Average Potential Price for each patented medicine that enters the market based on guidelines. The main reference is the median its price in France, Italy, Sweden, Switzerland, Germany, the UK and the U.S. If no references for the product are available, the regulator looks at comparable products, including a comparison of therapeutic benefit. Prices are allowed to rise yearly, at a maximum of 1.5 times the increase of the consumer price index. If a drug price is found to be in violation of the guidelines, the PMPRB can require the manufacturer to lower its prices and repay excessive profits to the government. [212]
Historically, Canada has been a fragmented market with the decision on drug reimbursements resting with the provinces. Authorization of sale in Canada does not guarantee funding through the drug benefits program. The Canadian Agency for Drugs and Technologies in Health (CADTH) is responsible for drug assessment and providing recommendations for reimbursing drugs in all formulary plans. It is the prerogative of each of the provincial, territorial and private plans to reimburse drugs in general. [213]

Global biosimilar policy comparison
61
In 2010, the pan-Canadian Pharmaceutical Alliance (pCPA) was established by the provinces to conduct joint provincial/territorial negotiations for brand name drugs in Canada to achieve greater value for publicly funded drug programs and patients. Federal health plans joined the scheme in 2016. All brand name drugs coming forward for funding through the national review processes Common Drug Review (CDR) or Pan-Canadian Oncology Drug Review (pCODR) are considered for negotiation through the pCPA. As of 2016, the alliance had completed negotiations for 89 brand name and 14 generic drugs. [214] [215]
Co-payments
Co-payments exist in the country particularly in drug plans that are based on price ceilings. Co-payments vary by provinces (in case of public insurance) and by health plans (in case of private insurance)
Generics
Off-patent drugs and generics can be priced freely. Pricing is subject to market competition and can differ between individual provincial health-care systems. [216]
Starting in 2013, the Value Price Initiative of the pan-Canadian Pharmaceutical Alliance (pCPA) has fixed the pricing of a number of generics at 18% of price of the originator brand. [214]
7.3. Market for biosimilars
7.3.1. Available biosimilars
As of May 2017, seven biosimilars have been approved in the country. All of these drugs except Erelzi* are being reimbursed in the country.
Biosimilar brand name Active substance
Company Authorization year
Erelzi19 etanercept Sandoz GmbH 2017
Brenzys etanercept Merck Canada 2016
Grastofil filgrastim Apotex 2015
Basaglar insulin glargine Eli Lilly 2015
Inflectra infliximab Hospira 2014
Remsima infliximab Celltrion 2014
Omnitrope somatropin Sandoz 2009 Source: Government of Canada Drug Product Database, accessed on 9 August 2017 [217]
19
*Note: Erelzi is available by prescription and recently received a positive recommendation by Health Canada for reimbursement

Global biosimilar policy comparison
62
7.3.2. Biosimilars market Share
The figure below gives the quarterly trends of biosimilar market share by molecule. [218]
Source: IMS Midas Database (data from sourced from a publicly available report) [218] *Note: The data labels in the box represent the market share of biosimilars as a % of molecule and for 4Q16
7.3.3. Market outlook
According to IMS estimates, biosimilars in the country will be more impactful beyond 2016 prior to which they would continue to have limited impact in the market. [219]
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1 2 3 4 1 2 3 4
Bio
sim
ilar
sale
s (C
AD
mill
ion)
Biosimilar sales (in CAD million) and market share (in %*) in Canada by molecule type, quarterly trends ending 4Q16
Infliximab Insulin Glargine Filgrastim
First year of launch Second year of launch
1.0%
0.9%
3.5%
BS market share (%)

Global biosimilar policy comparison
63
7.4. Legal framework for biosimilars
7.4.1. Market approval
According to guidelines issued by the drug regulatory body, Health Canada in 2010, biosimilars (initially known as Subsequent Entry Biologics (SEBs)) are treated as new drugs under the Food and Drugs Act and the Food and Drug Regulations. These guidelines were established in harmonization with EMA’s stringent framework for biosimilar approval and later revised in 2017 and the term “biosimilars” was officially adopted in alignment with international nomenclature.
Biosimilars are approved in a manner similar to other biologics. Health Canada’s Biologics and Genetic Therapies Directorate (BGTD) in collaboration with the Regulatory Operations and Regions Branch (RORB) and the Marketed Health Products Directorate (MHPD) regulates biosimilars in the country. [220]
The table below describes overarching guidelines as defined by Health Canada for market authorization of biosimilar products in Canada: [221]
Parameter Regulatory provision in Canada
Definition (revised in 2016)
A drug which is similar to a biologic (known as the reference product) which has already been authorized for sale. A biosimilar cannot gain market authorization until Health Canada establishes non-infringement of originator’s patents
Reference biologic An originator biologic authorized in Canada can be used as the basis for comparative studies to demonstrate similarity with the biosimilar. It is advised that sponsors consult with the BGTD early in the process to discuss suitability of the reference biologic. Following should be kept in mind when considering a non-Canadian reference biologic drug: • Non-Canadian reference drug should have the same medical ingredient, dosage form
and route of administration as the version approved in Canada • The drug should be marketed in a country that adopts the International Council for
Harmonization (ICH) guidelines • In case the non-Canadian drug is used in clinical studies in Canada, data must be
provided to satisfy chemistry and manufacturing (quality) information as per the local regulations
Labelling Product monograph should include: • A statement indicating that the product is a biosimilar to the reference biologic drug • A statement that indications have been granted on the basis of similarity between the
biosimilar and the reference biologic drug • A summary in tabular format of comparative data generated by the biosimilar sponsor
on which the decision for market authorization was made • Relevant safety and efficacy information from the product monograph of the biologic
drug authorized in Canada to which a reference is made, including warnings and precautions, Adverse Drug Reactions/Adverse Drug Effects and key post-market safety information for all indications that are authorized for the biosimilar
Comparative non-clinical studies
Non-clinical studies include established structural and functional studies with extensive in vitro studies. In vivo studies may not be necessary
Comparative clinical studies
Clinical studies should begin with comparative Pharmacokinetic (PK) studies and Pharmacodynamic (PD) studies. Comparative clinical trial is important to rule out clinically meaningful differences in efficacy and safety between the biosimilar and the reference product
Extrapolation of indications
A sponsor can ask for authorization of the biosimilar for all indications held by a Canadian reference biologic drug. In case the clinical indication being sought is not authorized for the reference biologic drug, then the indication falls outside the scope of the guidance document issued by Health Canada
Pharmacovigilance A risk management plan (RMP) should be submitted as part of the drug submission and it should be designed to monitor and detect both known inherent safety concerns and potentially unknown safety signals that may result from the impurity profile and other characteristics of the biosimilar
Manufacturing (revised in 2017)
Biosimilars manufactured through methods different from reference biologics may be considered for approval
Source: Health Canada, accessed on 27 July 2017 [221]

Global biosimilar policy comparison
64
7.4.2. Pricing and reimbursement
Biosimilars have had low penetration into the local market. To improve biosimilar uptake, the pan-Canadian Pharmaceutical Alliance (pCPA), which negotiates medicine prices for provincial and federal drug plans, introduced a national negotiation process for purchasing biosimilars to replace the approval system at provincial level in April 2016. This was issued as the First Principles for Subsequent Entry Biologics to guide pricing negotiations. This newly introduced centralized purchasing process will ensure that products that add value to drug plans, without raising expenditures, are part of the national drug list. Consequently, this regulation has promoted pricing competition between biosimilars and their reference products. Manufacturers of reference products are now required to provide similar or greater price reductions, for their reference products vis-a-vis the biosimilar drug for all payers, including private drug plans, to gain equivalent listing on provincial drug formularies. [214] [222] [223]
The impact of pCPA’s guidelines can be seen in the price of Inflectra, which due to the organization’s negotiations, is now being provided at 47% of the price of Remicade across public plans. [224]
Drug plans in Canada can encourage their plan members who are new to biologics to start using biosimilars using any of the following plan designs: [225]
• Step therapy: Plan members can try less expensive medicines on an ad-hoc basis with the option of using the brand name biologic in case they face tolerance issues
• Preferential listing: In this plan design, new patients are required to use biosimilars and not the branded biologic drug. This is a restrictive plan design
• Price ceiling: This particular plan design involves a co-payment option. In case plan members prefer to use the branded biologic over the biosimilar, they are required to pay the difference
• Listing agreements: This arrangement ensures that the price of the reference product is at par with the biosimilar allowing plan members to choose from either of the options
There are no fixed price discounts mandated by the law. Currently, the market trend is that biosimilars are priced at an average discount of 15%-23% to their reference products. [226]
7.4.3. Switching and substitution
Interchangeability: As Health Canada stresses in its biosimilars fact sheet, the decision on interchangeability (defined by the body as equivalent to pharmacy-level subsitution) rests with the provincian authorities. [227] The interchangebility of drugs is listed on the provincial Drug Benefits List.
Switching: According to Health Canada, the decision to switch a patient from an originator biologic to its biosimilar drug “should be made by the treating physician in consultation with the patient and taking into account available clinical evidence and any policies of the relevant jurisdiction”. [227] The pCPA too wishes to explore switching, which can be observed from a recent HTA recommendation on filgrastim that included a comment supporting patient discussions with prescribing physicians on switching. [228]
Substitution: Health Canada does not promote substitution at the pharmacy level. However, its position is only a recommendation, as the decision on biosimilar substitution rest with each province. As of January 2017, no province has published such guidelines yet. [225]
7.5. Additional factors and initiatives impacting the growth of biosimilars
7.5.1. Marketing or education initiatives regarding biosimilars
Besides issuing a guidance document and a factsheet, the regulatory body in the country hasn’t made much effort to improve physician acceptance. Hence, one of the industry associations, the Canadian Generic Pharmaceutical Association (CGPA) established “First Voice”, a biosimilars board, in April 2015, aimed at educating patients, prescribing physicians and drug plan sponsors. [229]
Furthermore, in September 2015, Health Canada announced a three year pilot program for offering scientific advice to sponsors on a “step-wise” review approach. As part of the program, when the sponsor submits data to establish similarity between biosimilars and their reference products, to the BGTD, the organization holds a series of meetings with the sponsor. After the meetings, the BGTD issues one of the three recommendations on the drug under review: [230]
• Drug to continue as a biosimilar • Drug to continue as a conventional drug • Seek additional data, after which the drug may be classified as either a biosimilar or a conventional
drug

Global biosimilar policy comparison
65
The BGTD and Health Canada encourage this step wise review process and have given comprehensive guidelines on their webpage on how sponsors may request Scientific Advice Meetings with BGTD early in the development process.
7.5.2. Government incentives to increase biosimilar prescriptions
Incentives to doctors / hospitals / pharmacies
There are no incentives specific to biosimilars in the country.
Prescription quotas
There are no prescription quotas specific to biosimilars in the country.
7.5.3. Procurement policies
Early this year, the Canadian Generic Pharmaceutical Association announced that domestic generic and biosimilar manufacturers will be eligible for an export waiver to mitigate negative effects of Comprehensive Economic and Trade Agreement (CETA), a trade deal between Canada and the EU. [231]
7.5.4. Other country-specific issues that influence the introduction and adoption of biosimilars
Market access issues • Delays between authorization and formulary listing — this can be attributed to an extensive HTA and
price negotiations. One such example is Inflectra which received authorization in 2014 only to be listed in public formularies in the year 2016 [225] [232]
• Variations in provincial formularies resulting in high degree of market fragmentation — Canada is the only industrialized nation that provides universal coverage to its citizens but does not cover prescription drug costs by that system. As a consequence, Canadians face varying drug costs between provinces. After a drug’s approval by Health Canada, it is the responsibility of each jurisdiction to include it in their provincial formularies. Such variations have been known to cause delays in access to urgently required medicines in the country [233]
• There has been reluctance to assign biosimilars with a “preferred status” in public and private drug plan designs, creating a barrier for the establishment of a biosimilars market [224]
Low physician acceptance for biosimilars • There exists a discrepancy between patient support programs for biosimilars and those targeting
reference products
Lack of information on biosimilars • Biosimilar uptake in Canada has been relatively low in the country due to a dearth of information
about the drug class. A country wide patient survey conducted by Consumer Advocare Network, a not-for-profit umbrella organization of patient groups between May-June 2016 showed that patients have to make efforts to search for information on biosimilars. More than 60% of the patients had learnt about biosimilars from online resources while 25% had knowledge about the drugs from their physicians. [234]
Budget constraints at provincial levels Provinces are looking to tap into cost savings associated with biosimilars by encouraging the use of these drugs.
• For instance, Quebec and Ontario have recently delisted Remicade from its formulary to encourage the prescription of Inflectra [235]
• Quebec’s Bill 92 – The proposed bill is expected to bring transparency into drug pricing.20 One of the provisions in the bill requires pharmacists and wholesalers to provide more details on drug margins leading to greater transparency and competition among pharmacists while reducing costs for insurers and drug plan members. [236]
20
Quebec is the only province in Canada that does not require pharmacists to disclose their fees.

Global biosimilar policy comparison
66
7.5.5. Industry position on biosimilars
Public Policy Forum (PPF) In 2014, the PPF, an independent not-for-profit organization in Canada, in collaboration with Roche, published a research paper advocating the case for multi-sector collaboration in the industry. According to the roundtable summary report, to counter the lack of information in the country, there is a need to identify the best possible methods to share responsibilities and costs that are associated with an education campaign or strategy. According to the body, it is desirable for all stakeholders to work together around roles and responsibilities to spread information about the drug class. [237]
BIOTECanada The Canadian biotech industry body published the guide “Demystifying Biosimilars” in 2012 to educate science writers and the public on the topic. [238]
Canadian Generic Pharmaceutical Association (CGPA) The CGPA represents generics manufacturers who are active in the Canadian market. It advocates for a higher share of generics prescriptions, educates the public on topics such as bioequivalence. They oppose the 2-year patent term extension for originators that has been part of the CETA agreement between Canada and the EU. [239]
Biosimilars Canada This Canadian industry body is affiliated with the International Generic and Biosimilar Medicines Association (IGBA) and represents its positions, such as promotion of switching and substitution.
In January 2017, it issued a statement welcoming the Revised Canadian Guidance for Sponsors of Biosimilars as the convergence towards international standards reduced the cost of entry to the Canadian market. [240]
Canadian Institute for Health Information (CIHI) In 2015, the CIHI in collaboration with the Canadian Generic Pharmaceutical Association (CGPA) published a report to highlight the importance of cost-savings of generics and biosimilars for the ongoing sustainability drug plans in the country. [241]

Global biosimilar policy comparison
67
8. Australia
8.1. Current healthcare landscape
8.1.1. Country data
Indicator Value Year Source
Population (Mill) 23.8 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %)
1.46 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 3.56 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 14.96% 2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 47770 2016 OECD [14]
Doctors per 10,000 people 33.74 2013 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people
8.27 2013 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 37.9 2014 OECD [16]
Healthcare expenses (% of GDP) 9.6 2016 OECD [17]
Source: UN, Dept. of Economic and Social Affairs, WHO/Europe, HlthResDB, OECD, BMI
8.1.2. Healthcare system overview
Health care in Australia is provided by both private and government organizations. Medicare is the publicly funded universal health care system for Australian residents. It coexists with a private health system.
The federal government, through the Department of Health, sets healthcare policy and funds Medicare.
Health sector infrastructure is a responsibility of the state, but they are limited in their ability to raise funds. In response, many hospitals have been subjected to privatization initiatives. One such model is co-location, where a private hospital is established next to, or within a public hospital, with sharing of facilities, staff and services. Another model is build-own-operate-transfer, where the private sector establishes a new hospital which is later transferred to the public sector. About 70% of hospital beds are in the public sector. [242]
General practitioners act as the first point of medical contact and gatekeepers to the system. A referral from a GP is required by Medicare to reimburse specialist consultation and outpatient care at hospitals.
Pharmaceuticals are typically dispensed through private community-based pharmacies, but very high-cost drugs are mostly available through hospital pharmacies. Medicines are subsidized under the Pharmaceutical Benefits Scheme (PBS) as discussed below. The private market for pharmaceuticals is relatively small in Australia.
8.1.3. Health insurance system
Medicare is funded by the federal government from general tax income, as well as the Medicare levy, which is currently 2% of taxable income. The levy is reduced or waived for low-income earners. On the other hand, the levy is increased by an additional 1% to 1.5% surcharge for high-income earners without private insurance to encourage switching into the private system. [243]
Medicare sets a “scheduled fee” for different goods and services. Medicare gives patients access to a range of medical services for free or at a lower cost including general practitioners, specialists and optometrists. Patients can also get a 75% rebate of the set Medicare Schedule fee for services and procedures received as a private patient. Medical practitioners are allowed to charge higher fees than the scheduled fee. Patient co-payments amount to the part of the scheduled fee not covered by Medicare, plus the difference between the practitioner fee and the scheduled fee. An additional safety net is in place to limit yearly out-of-pocket expenses for families that pays 80% of out-of-pocket costs past a certain threshold. [244]
All Australian residents are automatically covered by Medicare. Australians have the option to also purchase private health insurance. Over 30 “health funds” offer a wide variety of policies at different price and service levels. The largest health fund is Medibank, at roughly 30% market share, which used to be a government-owned non-profit alternative but was privatized in 2014.

Global biosimilar policy comparison
68
About 47% of Australians have a private insurance, with the government providing different incentives for signing up, such as a tax rebate of up to 33%.
A major difference between private and public health plans is that public patients must seek treatment with a specific provider within the public system. Private health plans, however, offer free choice of provider, and the insured can seek treatment in both public and private hospitals and allied health. [242]
The Australian Prudential Regulation Authority (APRA) has oversight over private health insurance providers.
8.1.4. Current issues in the healthcare system
Healthcare for indigenous people: Australia spends about AUD 7995 per person / year on healthcare for indigenous people, around 1.5 times of the AUD 5437 spent on non-indigenous Australians. One reason is that a large part of this population lives in remote areas, which increases the cost of providing goods and services. [245]
Preferential treatment of privately insured patients: Studies have shown shorter waiting times for privately insured patients, with the debate still going on as to how prevalent the effect is and what the incentives are. Cost shifting has increasingly become an issue with private patients in public hospitals. Public hospitals may encourage their patients to “go private” because it allows cross charging the patient’s health insurance and Medicare for costs incurred, rather than having to dip into their own limited budgets.
8.2. Market for pharmaceuticals
8.2.1. Market statistics
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 11.1 BMI
World market share % 1.0 BMI
Pharmaceutical sales / capita USD 455 BMI
Pharmaceutical sales / GDP % 0.88 BMI
Pharmaceutical sales / health expenditure
% 8.8 BMI
Prescription drug sales USD bn 8.9 BMI
Patented drug sales USD bn 7.3 BMI
OTC medicine sales USD bn 2.2 BMI
Generic drug sales USD bn 1.6 BMI
Share of generics (value) % 18.80% OECD
Share of generics (volume) % 36.80% OECD
Source: BMI data tool, accessed on 25 July 2017; OECD 2014 [21]
8.2.2. Market authorization and pricing
Market authorization
The key agency involved with the market assessment of medicines is the Therapeutic Goods Administration (TGA), which tests the safety and efficacy.
Pricing and reimbursement
Once market approval has been granted on the Australian Register of Therapeutic Goods (ARTG), the manufacturer may apply for government subsidization under a fixed price in the Pharmaceutical Benefits Scheme (PBS), a government-financed reimbursement system that is separate from Medicare. [242]
A new medicine cannot be listed on the PBS unless the Pharmaceutical Benefits Advisory Committee (PBAC) makes a positive recommendation for its listing. Under the National Health Act, the PBAC must take into account both the cost and clinical effectiveness of the medicine when compared with other treatments for the same condition. [242]

Global biosimilar policy comparison
69
If a positive recommendation is given by the PBAC, the sponsor must still negotiate the final arrangements for listing on the PBS, including pricing with the Department of Health. Final approval can be granted by the Minister for Health, unless the net cost of the medicine to the PBS is more than $20 million per year, in which case Cabinet approval is required for PBS listing.
If an application is rejected by the PBAC, sponsors can resubmit products at a lower price point or with new clinical data. [246]
Under the PBS, new originator products are listed in the F1 formulary. Products in F1 currently take price cuts after 5 years (5%) from the listing date. They will also take further price cuts at 10 years (10%) and 15 years (5%) from 1 June 2018. The details are set in a Strategic Agreement between the Commonwealth of Australia and Medicines Australia Limited (the industry association of the innovative pharmaceutical industry). These agreements usually have a 5-year term, with the second such agreement signed on April 27, 2017. [247] They can also be subjected to post market reviews, reference price changes and also risk share agreements with the Government which could impact price.
When the first generic enters the market, a one-time minimum price reduction is mandated on the originator’s price. The price reduction will be increased from 16% to 25% as part of the 2017 Strategic Agreement. [242] [247]
The products are moved to the F2 formulary, where they are subject to price disclosure. The price disclosure program progressively reduces the price of some PBS medicines which are subject to competition. As part of the price disclosure provisions, pharmaceutical manufacturers submit sales information and, based on this information, the price the Australian Government pays is adjusted to more closely reflect the actual market price. [248]
The PBS reimbursement price of a medicine is paid to the pharmacy. The price is set at the level of the cheapest available brand by molecule. Manufacturers are allowed to set a higher price and charge a so-called “brand premium” above the reimbursement price. The difference is paid by the patient. In 2008, the average brand premium was around AUD 3.03. [249]
Some private health insurers will cover medicines not subsidized by the PBS. [250]
The PBS lists expensive, specialized medicines for rare and chronic diseases in a separate category of Highly Specialised Drugs (HSDs). Large or repeated prescriptions of these drugs require a written authorization as so-called Written Authority Required Drugs. The list includes a range of biologics, such as trastuzumab for breast cancer and etanercept for �severe chronic plaque psoriasis. Patient eligibility is regulated by strict requirements that are determined for each individual condition and / or drug. [251] [252]
Co-payment
Co-payments are tiered by group. General consumers pay AUD 38.80 per prescription, while pensioners and other holders of entitlement cards pay AUD 6.30.
The co-payments are reduced/eliminated for patients and their families who have spent an amount equivalent to the PBS safety net threshold
21 on their co-payments in a calendar year (AUD 1,494.90
for general consumers and AUD 378 for benefits card holders). [253]
Generic substitution and INN prescriptions
Pharmacy substitution of generics and biosimilars is permitted if the brand is denoted by an “a-flag” in the PBS. A-flagging is common for generics but has only recently been applied to biosimilars (and is done so on a case by case basis only).
The doctor can prevent substitution by ticking a “no brand substitution permitted” box on the prescription. If a pharmacy sells a generic with a cheaper manufacturer price than the reimbursement price, the difference is kept by the pharmacy.
The 2017 Strategic Agreement introduced a policy for default INN prescribing. Prescribing software will be enhanced to default to the INN in producing a prescription (for both small molecule and biological medicines), while retaining physician choice. There will be consultation with stakeholder groups prior to implementation (most likely in 2018). [254] [249] [253] [255]
21 Safety net threshold is reached by accruing patient contributions for PBS prescriptions supplied by community pharmacies and private hospitals and for out-patient
medicine provided by public hospitals. [350]

Global biosimilar policy comparison
70
8.3. Market for biosimilars
8.3.1. Available biosimilars
At present, the following nine biosimilars are approved for use in Australia. Seven of these drugs are listed on Pharmaceutical Benefits Scheme (PBS):
#Listed on Australian Pharmaceutical Benefits Scheme (PBS)
Biosimilar brand name Active substance Company Authorization date
Renflexis infliximab Merck Sharpe and Dohme November 2016
Brenzys # etanercept Merck Sharpe and Dohme July 2016
Bemfola # follitropin alfa Finox Biotech November 2015
Inflectra # infliximab Hospira (Pfizer) August 2015
Basaglar insulin glargine Eli Lilly November 2014
Zarzio # filgrastim Sandoz May 2013
Tevagrastim # filgrastim Aspen Pharmacare August 2011
Nivestim # filgrastim Hospira (Pfizer) September 2010
Novicrit # epoetin lambda Sandoz January 2010 Source: The Department of Health, Australia, accessed on 2 August 2017 [256]
Various brands of human growth hormone (somatropin) are also available in Australia. Most of these brands were approved before the biosimilar regulatory pathway was implemented. Below are the somatropin approved in Australia:
Zomacton (Ferring Pharmaceuticals), Norditropin (Novo Nordisk Pharmaceuticals), Saizen (Merck Serono Australia), Humatrope (Eli Lilly Australia), Genotropin (Pfizer Australia), Nutropin AQ (Ipsen), Omnitrope (Sandoz), Scitropin A (Sandoz) [256]
8.3.2. Biosimilars market share
(No recent public data available)
8.3.3. Market outlook
Biosimilars are expected to gain a strong market share because of price sensitivity in Australian market. [257] The government of Australia plans to save AUD 880 million from 2015-20. [258]
8.4. Legal framework for biosimilars
8.4.1. Market approval
Biosimilars in Australia are approved by the Therapeutic Goods Administration (TGA) which is part of the Australian Government Department of Health. TGA first officially published biosimilar regulations in 2013 (based on EMA pathway) and then released a revised version in 2015. [259]
The following table highlights the key guidelines to ensure similarity in terms of physicochemical, biological, immunological, efficacy and safety between biosimilar and reference product.
Parameter Regulatory provision in Australia
Definition Biosimilars are highly similar to the ‘reference biological medicine’. The reference biological medicines are the first brand to come into the market. [260]
Reference medicine
For a biosimilar medicine to be registered in Australia, the reference biological medicine must be registered in Australia or a similarly regulated country (e.g. EMA and US FDA). [261]
In case of a reference medicine that has not been registered in Australia, a bridging study must be provided to demonstrate that the comparability studies are relevant to the Australian reference medicine. [262]
Non-clinical studies
Data requirements for comparability studies are similar to that of EMA [262]
Clinical studies Data requirements for comparability studies are similar to that of EMA [262]

Global biosimilar policy comparison
71
Parameter Regulatory provision in Australia
Quality comparability studies
The following points are followed for comparability studies of quality aspects:
• Studies are conducted according to CPMP/ICH/5721/03 ICH Topic Q 5 E guideline
• In-house reference standard, reference medicine and the biosimilar medicine are always included
• Direct comparison between the reference standard, reference medicine and the biosimilar
• Batches of drug substance of the biosimilars should be from a single process for both clinical trials and commercial distribution
In the case that the biosimilar manufacturing process is changed significantly due to inevitable circumstances between clinical trial and commercial stages, then either:
• Reference medicine in a second comparability study is included together with the clinical trial and commercial medicines
• A linked comparability study showing that the clinical trial and commercial medicine is similar should be provided
Not to use more than two linked bridging comparability studies, as it will not be possible to make robust comparison between the reference and batches of biosimilars. If a direct comparison of the biosimilar and reference material is not possible, then an extraction or concentration techniques may be used, but these must be:
• Declared in the dossier
• Described in full
• Validated for use [262]
Extrapolation of indications
Australia follows EMA’s guidelines for assessing non-clinical and clinical issues in extrapolation of indications [262]
Risk management plan (RMP)
It should include the following:
• outline of the pharmacovigilance procedures which will be implemented
• specifically address immunogenicity
• potential risks that are associated with the reference product, as well as with biosimilarity
• pharmacovigilance and risk minimization activities for the reference medicine, or provide an explanation for these not being relevant for biosimilars [262]
Adverse event reporting
Adverse event report must include the following points:
• trade name of the biosimilar
• non-proprietary name of the biosimilar (currently, the Australian biological name)
• AUST R number22
• batch number and expiry date
• dosage form [262]
Naming Biosimilar medicines are required to have a trade name clearly distinguishable from all other products, especially the reference medicine and other biosimilar medicines. The use of the active ingredient ABN in the trade name of a biosimilar is not acceptable. [262] TGA has recently closed a consultation on naming of biological medicines. The options include retain the same INN, take the EU approach using barcodes or FDA approach with a unique identifier. [263] [264] The TGA decided to retain the same INN for both biologics and biosimilars and strengthen pharmacovigilance provisions. [263]
Product information
The following words are used under the description section:
• <Biosimilar product name> is a biosimilar medicine to <Reference medicine name>. The evidence for comparability supports the use of <Biosimilar product name> for the listed indication[s].
In addition, clearly identified information on clinical trials and adverse drug effects must be mentioned in separate sections. [262]
22
AUST R medicines are assessed for safety and efficacy. AUST R medicine include all the prescription only medicines and many over-the-counter products (e.g. pain relief, coughs and colds and antiseptic creams).

Global biosimilar policy comparison
72
In addition, TGA has also taken EMA’s product-specific guidelines for recombinant granulocyte colony stimulating factor, low molecular weight heparins, recombinant human insulin and insulin analogues, interferon beta, monoclonal antibodies, recombinant erythropoietins, recombinant human follicle stimulating hormone, somatropin and recombinant interferon alfa.
The following are the ‘Guiding principles for the governance of biological and biosimilar medicines in Australian hospitals’ from Council of Australian Therapeutic Advisory Groups (CATAG):
• Guiding principle 1: The rules for biologics/biosimilars within the hospital system should be same as that of any other medicine.
• Guiding principle 2: The choice of a biologic/biosimilar in the first-line therapy for treatment-naïve patients must be based on evidence of safety, efficacy and cost-effectiveness.
• Guiding principle 3: Biologics/biosimilars must be prescribed with both the active ingredient name and the brand name.
• Guiding principle 4: Biologic can be interchanged with its biosimilar at dispensing only when it has been determined to be substitutable by the drug and therapeutics committee (DTC).
• Guiding principle 5: Patients should be informed when they are receiving the treatment with a biologic/biosimilar.
• Guiding principle 6: Switching between a biologic and a biosimilar should be as per the drug and therapeutics committee–approved treatment protocol which includes a monitoring plan.
• Guiding principle 7: Selection of a biologic/biosimilar for the second-line therapy should be as per the treatment pathway which is approved by the drug and therapeutics committee.
• Guiding principle 8: A patient-centered pharmacovigilance framework within each hospital must be there to monitor and report adverse effects due to administration of a biologic/biosimilar.
• Guiding principle 9: Active ingredient and brand name of the biologic/biosimilar must be specifically communicated to the patient at the time of transition of care. [265] [266] [267]
8.4.2. Pricing and reimbursement
Once the TGA has approved a medicine, the biosimilar company may apply to the Pharmaceutical Benefits Advisory Committee (PBAC) to list their medicine on the Pharmaceutical Benefits Scheme (PBS) for national use. In deciding whether a medicine should be recommended for subsidy, the PBAC considers the patient benefits and cost-effectiveness of the medicine compared with alternative medicines. [261]
The PBAC will only recommend a biosimilar medicine for PBS listing if it is satisfied that it will deliver the same health outcomes as the reference biological medicine. [261]
A mandatory 25% price reduction will be applied to all medicines within a therapeutic category when the first biosimilar enters the market. This price was increased from 16% in the latest agreement between the industry body Medicines Australia and the government. This is the same as for generics. [268] [269] [247]
As with biologic originators, PBS reimbursement for biosimilar prescriptions can be subject to the Highly Specialised Drugs (HSDs) rules. [251] [252]
8.4.3. Switching and substitution
Originator drugs are listed in the F2 formulary together with their biosimilar competition as a therapeutic group. However, to be substituted at the pharmacy level, without informing the physician, a drug must be given the “a” flag.
Under PBS, the “a” flag is used to indicate that different pharmaceutical products are similar for the purposes of substitution by the pharmacist during dispensing of the drug. Products with the “a” flag have been determined by the PBAC on a case by case basis that they can be interchanged without alterations in clinical effect. [270] [271]
Guidelines on choice between biosimilar and biologic are as follows:
• The choice for the medicine to be used for treatment is made by the physician in discussion with the patient
• Pharmacists can substitute the biologics in discussion with the patient, and informing the physician regarding substitution is not mandatory provided there is no clinical evidence to the contrary
• Pharmacist can’t substitute a biosimilar for a biologic if the physicians tick the box ‘brand substitution not permitted’ (even if a medicine is substitutable) while writing a prescription [272]
The incentive to substitute depends on whether the biosimilar manufacturer sells into pharmacy at a discount. The difference between the discounted price and the reimbursed price is kept by the pharmacy.

Global biosimilar policy comparison
73
Originally, the PBAC declined to give biologics the “a” flag to allow substitution. However, that stance was reversed in 2015. [273]
Currently, the following products are flagged as schedule equivalent “a” flagged brands to their respective reference products, for pharmacy level substitution): [274]
• Etanercept: Brenzys as substitute for Enbrel • infliximab: Inflectra and Renflexis for Remicade
In 2017, as part of the Strategic Agreement, the government and industry agreed that further uptake drivers, including recommended treatment naïve prescribing and streamlined authority for biosimilars, could be recommended by PBAC on a case by case basis. [254]
8.4.4. INN prescribing
As part of the Strategic Agreement in 2017, a policy for default INN prescribing was proposed. The Australian government plans to introduce a prescribing software that will be enhanced to default to the INN while producing a prescription (for both small molecule and biological medicines) while maintaining the physician’s choice.
The proposed plan will come into effect post consultation with stakeholder groups which is expected to occur most likely in the year 2018. [275]
8.5. Additional factors and initiatives impacting the growth of biosimilars
8.5.1. Marketing or education initiatives regarding biosimilars
The Australian government has taken steps to encourage the prescription of generics, including education campaigns aimed at pharmacists and consumers.
Biosimilar Awareness Initiative – This initiative was announced in May 2015 and is a part of PBS Access and Sustainability Package. Under this package, a fund of AUD 20mn has been allocated to be spent over three years (2015-16 to 2017-18) to educate clinicians and the general public on biosimilars.
The main objective of this initiative are as follows:
• Increase the awareness of PBS and the potential of biosimilars in the future across the community • Convey advantages and information required to overcome obstacles in the use of biosimilars • Provide education to healthcare professionals to meet the clinical and information needs of
patients • Assist in specific communication requirements of stakeholders, including the PBAC.
This initiative is further divided into the following three stages:
Stage 1 Stage 2 Stage 3
• Initial Awareness • Research • Plan
• Implementation • Monitor • Review • Refine
• Evaluate • Finalize • Recommend
The main communication channels used under this initiative are as follows:
• Fact sheets and frequently asked questions (FAQs) • Brochure • Accredited education/training module (online) • Articles in medical/pharmacy journals and industry association newsletters • Information on websites of the Ministry of Health and pharmacy organizations • Online videos • Broadcast emails from the Ministry of Health [260] [276]
The Generic and Biosimilar Medicines Association (GBMA) secured a grant under the initiative in May 2017.

Global biosimilar policy comparison
74
8.5.2. Government incentives to increase biosimilar prescriptions
Incentives to doctors / hospitals / pharmacies
The government has strict guidelines for PBS-subsidized biologics that fall under Highly Specialised Drugs (HSD) rules — depending on the condition, only those patients who have failed on other therapies are eligible. [247] [251] [252]
While there are no direct Government incentives to pharmacists for biosimilar substitution, they are allowed to keep the difference when dispensing medicines cheaper than the reimbursement price. With some biosimilars recently flagged for substitution, there is the potential for an indirect incentive. [277]
Following the 2017 Agreement, the Government intends to implement policy changes that will promote greater use of biosimilars, in consultation with stakeholders including Medicines Australia. Such changes are intended to apply to new PBS listings only.
The following biosimilar uptake drivers may be considered by the PBAC on a case-by-case basis:
• Encouraging prescribing of a biosimilar brand rather than the reference biological brand for treatment naïve patients
• Providing for a simpler and faster approval process for prescribing biosimilar brands (e.g. streamlined authority) while maintaining an existing higher level authority requirement for the reference biological brand (e.g. written authority). [278]
These uptake drivers are designed to supplement existing activities by the Department of Health to improve awareness of, and confidence in, biosimilars for both healthcare professionals and consumers.
The uptake drivers will be implemented with the following principles in mind:
Doctors and other prescribers will retain, in consultation with their patient, the ability to choose which brand to prescribe. Prescribers can also continue to tick the ‘no substitution’ box on a prescription which means the prescribed brand must be dispensed when an equivalent brand could otherwise be substituted by the pharmacist
• The uptake drivers will be considered by the PBAC on a case by case basis, with regard to the evidence for, and context of the particular medicine and the clinical setting in which it will be used
• Existing authority requirements to prescribe reference brands will not be increased • Greater use of biosimilars is beneficial for supporting access to clinically and cost effective
medicines in Australia [278]
Government is currently engaging with stakeholders on an appropriate implementation framework for the new uptake drivers.
Prescription quotas
There are no prescribing quotas for the physicians in Australia. [272] The 2017 agreement between the government and Medicines Australia specifically states that physicians will retain prescriber choice with regards to biologics and biosimilars. [247]
8.5.3. Other country specific issues that influence the introduction and adoption of biosimilars
• Prescription choice is clinician-driven with limited influence from other stakeholders [247] • Majority of pharmacists are comfortable in substituting biologic for biosimilar when the products
have identical non-proprietary name [279]
8.5.4. Industry position on biosimilars
Pharmaceutical Society of Australia (PSA)23 — the following are the prominent views expressed by the body in September 2015:
• Urgent need to develop a consensus document on definitions relating to biological medicines (including biosimilars) to support accurate and common understanding
• Need for a coordinated method, focused on outcomes, to implement a strong pharmacovigilance program
• Carry out a national awareness campaign on biosimilars, based around consistent communication messages [270]
23
These views are as of September 2015 and the policy for biosimilars in Australia was revised in December 2015.

Global biosimilar policy comparison
75
Generic and Biosimilar Medicines Association (GBMA) — In January 2017, GBMA has made the following two recommendations to increase the uptake of biosimilars: [280]
• Introduce measures to increase the use of generic and biosimilar medicine, e.g. INN prescribing and incentives for prescribing/dispensing/purchasing biosimilars and generics
• Reform Australia’s pharmaceutical intellectual property system to support market entry for affordable generic and biosimilar medicines
AusBiotech — the association identified the following points that need to be addressed in future: [281]
• Build stakeholder confidence and undertake shared decision-making through high quality information
• Develop more comprehensive pharmacovigilance systems and reporting processes for biologic and biosimilar medicines
• Improve evidence-based data collection to support the uptake of biosimilars and to increase patient confidence in biosimilars
Medicines Australia (MA) — In May 2015, the association expressed its views over substitution and monitoring of biosimilars in the country: [282]
• MA is of the opinion that biosimilars are similar to but not the same as their reference products and therefore, all policies involving biosimilars should be made keeping patient safety into consideration
• MA urged the TGA to play an active role in post market surveillance of biosimilars • MA supports switching of biosimilars at the physician level

Global biosimilar policy comparison
76
9. South Korea
9.1. Current healthcare landscape
9.1.1. Country data
Indicator Value Year Source
Population (Mill) 50.59 2015 UN, Dept. of Economic and Social Affairs [13]
Population growth / year (2010-2015, %)
0.52 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (Mill) 6.56 2015 UN, Dept. of Economic and Social Affairs
Population over 65 (%) 12.97% 2015 UN, Dept. of Economic and Social Affairs
GDP per capita (USD) 35921 2016 OECD [14]
Doctors per 10,000 people 22.31 2014 WHO/Europe, HlthResDB; OECD [15]
Pharmaceutical Personnel per 10,000 people
6.52 2015 WHO/Europe, HlthResDB; OECD [15]
Hospital beds per 10,000 people 115.3 2015 OECD [16]
Healthcare expenses (% of GDP) 7.7 2016 OECD [17]
Source: UN, Dept. of Economic and Social Affairs, WHO/Europe, HlthResDB, OECD, BMI
9.1.2. Healthcare system overview
Overall responsibility for the health policy, the healthcare system and health insurance is held by the Ministry for Health and Welfare (MOHW). The Health Insurance Review and Assessment Service (HIRA) reviews healthcare services provided by medical institutions with respect to their costs and benefits. NHIS (National Health Insurance Service) takes change of overall operations of public health insurance system.
Patient have free choice of practitioner. However, specialized hospitals in secondary care require a referred slip from a primary care practitioner, except for cases such as childbirth, emergency care, dental care etc.
Healthcare providers are predominantly privately owned, with over 90% of beds provided by private hospitals and clinics. [283]
9.1.3. Health insurance system
South Korea has a compulsory National Health Insurance (NHI) with universal coverage. The system was introduced in 1977 for corporate employees, and gradually expanded to cover the entire population. Several not-for-profit health insurers that had been founded to cover different groups were merged into a single National Health Insurance Corporation (NHIC) in 2000 and is currently known as the NHIS.
A small minority of the population (3-4%) are covered by the Medical Aid Programme (MAP) for low-income households instead.
The NHI contribution rate is 6.12% of salary or income, paid half by employee and employer each.
The government subsidizes the National Health Insurance with 14% of its projected income from premiums. Another 6% is provided by a surcharge on tobacco.
The NHI requires comparatively high co-payments, at 5-20% for inpatient care (General: 20%, Rare: 10% such as Hemophilia, Chronic renal failure, Serious: 5% such as Cancer, Cardiovascular disease, Cerebrovascular disease, Tuberculosis, and severe burn injuries), 30%-60% for outpatient care (Tertiary hospital: 60%, General Hospital: 50%, Hospital: 40%, and Clinic: 30%), and 30% for pharmaceuticals. To prevent patients with high-cost diseases from facing bankruptcy, total co-payments over a period of 6 months are limited to a ceiling of 1.22-5.14 million Won, depending on income. [284]
In addition to NHI, over 60% of the population also have some form of complementary private health insurance, either individually or from their employer.
Healthcare providers enter a contract with the NHI to offer their services to the insured. Payments are mainly made on a fee-for-service level, based on a negotiated unit price per point. Points represent the relative value of a service or procedure. Some payments are based on diagnosis-related group (DRG). [283] [285]

Global biosimilar policy comparison
77
9.1.4. Current issues in the healthcare system
Ageing society: The Republic of Korea has one of the lowest fertility rates in the world (1.2 in 2015 [286]) and one of the fastest ageing societies. This has led to additional strain on the healthcare system, with increased costs for chronic degenerative diseases.
Alcohol and Tobacco: Korea has the highest alcohol consumption in Asia, with an average daily intake of 54.9 grams of pure alcohol [287], and 39.3% of the male population smoke (according to KHANES, 2015). [288]
Rural access to healthcare: Korea is highly urbanized, with 79.7% of the population in urban areas, but medical facilities are even more concentrated, with 92.1% of physicians and 90.8% of hospital beds. The government has created a system of public health centers and health posts in underserved areas to address the issue. [285]
9.2. Market for pharmaceuticals
9.2.1. Market statistics
Source: BMI data tool, accessed on 25 July 2017
9.2.2. Market authorization and pricing
Market approval
Market approval is granted by the MFDS (Ministry of Food and Drug Safety).
Pricing and reimbursement
With the NHI as the single payer, a prescription drug has to be included in the reimbursable drug list (positive list) to gain any market share.
Korea follows a 2-step system to set the NHI price. First, a HTA assessment looking at clinical need and cost effectiveness is performed by the Health Insurance Review and Assessment service (HIRA) whether to include a drug on the reimbursement list. Then, National Health Insurance Service (NHIS) negotiates price and expected sales volume with the manufacturer, taking into account factors such as the therapeutic benefit, budget impact, the serverity of the disease and available alternatives. [289]
If it is, a price is negotiated between the NHI and the manufacturer, while taking into account factors such as the therapeutic benefit, budget impact, the severity of the disease and available alternatives.
Keeping industry sentiments in mind, the South Korean government recently announced changes to its pricing policy for biologics. It will provide preferential price to the local biopharma industry for a global innovative drug and bio-product which contributes to local healthcare promotion, such as being locally developed or providing social contribution. [290] [291]
24
Share of generics (% of Value) = (Generic drug sales in USD bn*100)/ Prescription drug sales in USD bn
Market in 2016 Unit Size Source
Pharmaceutical sales USD bn 15.2 BMI
World market share % 1.37 BMI
Pharmaceutical sales / capita USD 301 BMI
Pharmaceutical sales / GDP % 1.08 BMI
Pharmaceutical sales / health expenditure
% 14.2 BMI
Prescription drug sales USD bn 12.2 BMI
Patented drug sales USD bn 5.1 BMI
OTC medicine sales USD bn 3.0 BMI
Generic drug sales USD bn 7.2 BMI
Share of generics (value)24
% 58.5% BMI
Share of generics (volume) % N/A -

Global biosimilar policy comparison
78
Generics and INN prescriptions
For generics, limited to small-molecule medicines, the reimbursement price is set by the Drug Price Reimbursement Scheme, at maximum 59.5% of the original branded drug price for the first entrant while pricing the original at 70% of one before LOE. Then, under the policy to offer the same reimbursement price for generic as the originator instituted in 2012, price ceiling for generic and LOE originator sets at 53.55% of the original price after 1yr of patent expiry when the more than 3 generics are launching in the market. [285] [292]
This has led to a price decrease for originators, while at the same time increasing their market share. [293]
The NHI has implemented an incentive system that allows pharmacists to substitute generics, and provides financial incentives to do so. When a pharmacist exchanges a prescribed drug for a generic, 30% of the price difference between the actual drug price and the substitute is retained by the pharmacist. After substitution, pharmacists must report to the doctor who wrote prescription within one business day. However, this incentive system carried out only 0.12%, because pharmacists does not want any conflict with doctors about changing prescription, the procedure of reporting was inconvenient, and pharmacists’ reliability of generics’ bioequivalence test was relatively low. [294]
In Korea, physicians can only prescribe by a specific brand name, not by an INN. [295]
Co-payments
The NHI charges a 30% co-payment for pharmaceuticals in ambulatory care and 20% in hospitals. The co-payment is reduced to 5% for cancer patients and 10% for special disease codes (usually rare diseases). A majority of the population has supplementary private health insurance to cover co-payments. [293]
9.2.3. Industry policy
The domestic South Korean pharmaceutical industry has traditionally focused on generics, OTC medicines and traditional Chinese medicine. The Korean government has recently invested heavily into promoting R&D and manufacturing capacity to move the industry towards more original medicines, including biologics.
The 2012 Korea-US FTA has put additional pressure on the domestic industry by allowing US multinationals better access to the market.
9.3. Market for biosimilars
9.3.1. Available biosimilars
South Korea is one of the world’s most advanced biosimilar markets and witnessed the approval of world’s first biosimilar monoclonal antibody. While historically, domestic players have dominated the market for biosimilars, several foreign players have recently started conducting research in the country. Ministry of Food and Drug Safety (MFDS) data in 2015 showed that 40% of biosimilar trials underway in the country were sponsored by overseas companies. [296]
The table below shows that as of June 2017, eight biosimilars have been approved in the country.
Biosimilar brand name Active substance Company Authorization year
Truxima rituximab Celltrion 2016
Renflexis infliximab Yuhan/ Samsung Bioepis 2015
Brenzys etanercept Yuhan/ Samsung Bioepis 2015
Basaglar insulin glargline Eli Lilly/ Boehringer Ingelheim 2015 [297]
Omnitrope somatropin Sandoz 2014
Herzuma trastuzumab Celltrion 2014
Remsima infliximab Celltrion 2012 Source: GaBI, accessed on 13 July 2017 [296]
For example, Remsima is the world first approved biosimilar which is now available in 71 countries. In Korea, Remsima was exported 737.7 billion Won (2016) which is 44.7% higher than 2015 (497 billion Won). [298]

Global biosimilar policy comparison
79
9.3.2. Biosimilars market share
(No data available)
9.3.3. Market outlook
According to the Pharmaceutical Manufacturers Association (PMA) of Korea, the biosimilar market is expected to double in size in the coming years. [299]
Source: First Word Pharma, accessed on 13 July 2017 [299]
80
150
2013 2019E
Korean biosimilar market outlook, KRW billion
CAGR: 11.06%

Global biosimilar policy comparison
80
9.4. Legal framework for biosimilars
9.4.1. Market approval
The MFDS, through the National Institute of Food and Drug Safety Evaluation, is responsible for scientifically evaluating biosimilars in the country. In 2009, the Ministry issued detailed guidelines for development, approval and commercialization of biosimilars. These guidelines were co-developed with the WHO and harmonized with those issued by the EMA in terms of requiring a demonstration of similarity, comprehensive characterization and comparative quality studies.
The guidelines have been designed in such a manner that products approved in South Korea stand a chance of obtaining market authorizations in Japan, US and Europe.
The table below describes overarching guideline on the evaluation of biosimilar products in South Korea [300] [301]
Parameter Regulatory provision in South Korea
Definition Defined as biological products that are comparable to an already marketed reference product in South Korea in terms of quality, safety and efficacy
Reference product Defined as a biological product already approved by a regulatory authority on the basis of full registration dossier (licensed based on full quality, safety, and efficacy data).
The regulatory body does not advocate the use of a biosimilar as a reference drug. In situations of non-availability of a Korean reference product, a reference product from another country is acceptable only on demonstration of similarity between the biosimilar under investigation and the non-Korean reference drug. [302]
Comparability studies
Conducted to demonstrate comparable characterization, physicochemical properties, biological activity and immunological properties between the biosimilar and its reference product through quality, non-clinical and clinical studies. Post-marketing safety studies are needed to track adverse reactions
Comparative non-clinical studies
Designed to detect differences between reference products and biosimilars using both in vitro and in vivo studies
Comparative clinical studies
• Phase II dosage trials are not needed
• Comparable pharmacokinetic and pharmacodynamics studies are required
• In some cases, comparative PK/PD study may be alternatively demonstrate the efficacy of biosimilar products
• Equivalence design is recommended and equivalence margins should be pre-specified and justified
• Detailed antibody testing strategy is required in addition with post-marketing safety studies
Extrapolation of indications
Allowed for indications where post-marketing surveillance has ended and the following conditions are met:
• Use of sensitive clinical models to detect potential differences
• Sufficient characterization of safety and immunogenicity
• The mechanism of action and receptor(s) is the same
Pharmacovigilance Post marketing surveillance should last four years. It is mandatory to submit a post-marketing surveillance study plan to the MFDS. The sponsor should also report data from the post-marketing surveillance study to the MFDS on a periodic basis. [303]
Source: GaBI, accessed on 13 July 2017 [300]
In addition to the revision of base guidelines in 2014, the MFDS has also issued product-specific guidelines for somatropins, erythropoietins, filgrastims, mAbs, and insulin analogs. [304]
In 2015, Korea introduced new IP rules in which a qualified biosimilar manufacturer is granted nine months of market exclusivity. To qualify for exclusivity, a company must be the first to file for the approval and file an invalidation or scope action against the relevant patent. The rule was brought to encourage challenges to originator patents, favoring biosimilar developers. [305]

Global biosimilar policy comparison
81
9.4.2. Pricing and reimbursement
As part of efforts to bolster international competitiveness of domestic biopharmaceuticals, the Korean the Ministry of Health and Welfare announced the “Reform Plan for Reimbursement Prices of Biopharmaceuticals and Global Innovative Pharmaceuticals” in July 2016. As part of this reform, the Ministry of Health and Welfare increased the list price of biosimilars which qualify for certain criteria, such as conducting a local clinical trial, being developed by innovation-certified pharma, etc., from the usual 70% to 80% of the originator’s pre-LOE price for a maximum of 3 years. [294] [306] [307]
As a current trend, regardless of pricing and reimbursement regulation, there is approximately 5% difference between the NHI price of the originator biologic and the biosimilar, according to the reimbursement price list from Health Insurance Review and Assessment Service (HIRA). The small 5% price gap is based on the biosimilar companies’ decision, considering their market competitiveness. For example, the price of Janssen’s Remicade injection 100mg (infliximab) is 383,051 won, and this is 5% more expansive than both Remsima from Celltrion and Renflexis from Samsung Bioepis which is 363,530 won. (Both prices are currently in effect (as of 17th Oct. 2017) but they are subject to change according to post-launch cost containment measures.) [308] [309]
9.4.3. Switching and substitution
Substitution: Automatic substitution of biosimilars at pharmacy level is prohibited. [310]
9.5. Additional factors and initiatives impacting the growth of biosimilars
9.5.1. Marketing or education initiatives regarding biosimilars
The MFDS releases approval documents on its website. In August 2016, it also released approval evaluation results in English for the first time and has pledged to continue publishing these documents on its portal.25
Keeping up with its pledge of developing an internationally competent domestic biopharmaceutical industry, the Korean Drug Ministry chaired the International Pharmaceutical Regulators Forum in 2016 that witnessed participation from the world’s major drug regulators such as the US FDA and EMA. [311]
The South Korean government has been investing heavily in domestic biopharmaceutical companies through capital provision and regulatory assistance since 2011. The government launched a consulting program codenamed “Columbus” for local biopharma companies to understand the regulatory process for biosimilar approval in South Korea and abroad. [312] [313]
9.5.2. Government incentives to increase biosimilar prescriptions
There is no specific government incentive to increase biosimilar prescriptions. In general, the Korean government provides an incentive to hospitals to procure pharmaceuticals at a lower cost compared to previous year’s expenditure or comparable institution’s expenditure. [293].
9.5.3. Procurement policies
Although the patient market for biosimilars in Korea was slow to develop, as of 2014, Korea possessed the largest production capacity for biologics in the world at 11.2%, according to a NH Investments & Securities study. [314] The government has always been a strong supporter of domestic production with roll-outs of industry friendly policies. The South Korean government has a stated goal of providing 22% of the global biosimilar supply under “Pharma Vision 2020”. [315]
To support this goal, the government has consistently invested in domestic biopharma companies:
• As part of Project Columbus, in addition to consulting services, the government has also been sharing the burden of high-risk investments such as construction of cGMP facilities. To date, 21 South Korean biopharma companies have participated and benefited from the initiative [316]
• In 2012, the government invested 35% of the national medical R&D budget for development of biosimilars in the country [317]
• The government has further been actively involved in the roll-out of tax benefits, creation of a “biomedical fund” and strategic planning, according to a BNP Paribas report. [318]
• The MFDS has shown further support to the industry by showing a keenness to reduce approval times. According to a BMI Research trend analysis, this move would be beneficial to both local and foreign biosimilar manufacturers. [319]
25
The documents can be found by clicking “Pharmaceutical Information” under the “Category Information” tab at www.mfds.go.kr.

Global biosimilar policy comparison
82
9.5.4. Other country-specific issues that influence the introduction and adoption of biosimilars
• The pricing policy in South Korea favors local production with generous price ceilings for locally developed biosimilars [290]
• A multinational firm producing a biosimilar must also fulfil a number of conditions, such as joint development with a Korean company and then conducting the clinical trials in Korea. [320]
9.5.5. Industry position on biosimilars
Korea Pharmaceutical and Bio-Pharma Manufacturers Association (KPBMA)
In April 2014, KPBMA criticized and recommended how to develop pharmaceutical industry in Korea: [321]
• Competitiveness in global, investment in R&D, export rate is insufficient. The rate of R&D expenses in pharmaceutical industry is getting more important, but it is only 8% average (2013) while global shows 20%.
• Moreover, the Government uniformly reduced drug price in 2011, and it causes 2500 billion Won loss every year.
• In 2014, the challenge of domestic pharmaceutical industry is to find a new drug (including biosimilar) with more R&D investment from Government, transparency in drug logistics, and expansion towards globalization at the end. Especially, developing biologics (including biosimilar) needs proper supportive scheme from the Government in the long term.
Korean Research-based Phama Industry Association (KRPIA)
KRPIA, representing 36 foreign drug companies in Korea, criticized the country's reimbursement rate for new drugs, currently at 44% of the OECD member country average, and asked for an increase to 60%. [322]

Global biosimilar policy comparison
83
III. Appendices
1. Glossary The table below defines some commonly occurring terms in the document:
Terminology Explanation Defined by
Abbreviated pathway
The pathway created under the Biologics Price Competition and Innovation (BPCI) Act of 2009 for the biological products shown to be biosimilar to the US FDA licensed reference product
US FDA [177]
Accessible category
Includes products within the same ATC4 code with the following categories:
• Referenced product: It is the original product which is granted market exclusivity at the start of its life. Exclusivity of it has now expired and the product is now categorized as referenced.
• Non-Referenced product: It is the original product which is granted market exclusivity at the start of its life. Exclusivity of it has now expired and the product has never been categorized as a Referenced Medicinal product.
• Biosimilar product: It is a product which is granted regulatory approval and demonstrates similarity to the reference product in terms of quality characteristics, biological activity, safety and efficacy
IMS [10]
Adverse drug reaction (ADR)
An unwanted medical event following the use of a medicine. Suspected ADRs are those that have been reported to authorities but which are not necessarily caused by the medicine
EMA [323]
Anatomical Therapeutic Chemical Classification System (ATC level 4 code)
A classification system in which active substances are divided under different groups according to the organ system they act on in addition to their pharmacological and chemical properties. The drugs are further classified into five levels: Level 1: anatomical main group Level 2: therapeutic subgroup Level 3: pharmacological subgroup Level 4: chemical subgroup Level 5: chemical substance
WHO [324]
Anti-Tumor Necrosis Factor (Anti-TNF)
Anti-TNFs are used the treatment of severe, active and progressive rheumatoid arthritis in adults.
NICE [325]
Bioequivalence Comparison of medicines based on the rate and extent of active substances released in the body
EMA [323]
Biosimilarity Demonstration of high similarity between a biosimilar and its reference drug in terms of chemical structure, biological activity, efficacy, safety and immunogenicity profile
EMA [323]
Centralized procedure in the EU
Approval process of medicines with a single application, a single evaluation and, for successful applications, a single authorization valid throughout the European Union. It is mandatory for certain types of medicines, including all medicines produced by biotechnology and medicines for specific conditions such as cancer, neurodegeneration and auto-immune diseases
EMA [323]
Co-payment A fixed amount that the patient pays for a covered health care service after he/she has paid a deductible
US health-care [326]
Defined Daily Dose (DDD)
The assumed average maintenance dose per day for a drug used for its main indication in adults
WHO [327]
Diagnosis Related Group (DRG)
A statistical system which classifies inpatient stay into groups for the purposes of reimbursement.
CMS [328]
Disability-Adjusted Life Year (DALY)
Quantifies the burden of disease from mortality and morbidity. One DALY is one lost year of healthy life
WHO [329]
Erythropoiesis‑stimulating agents (epoetin and darbepoetin)
These agents are approved for the treatment of anemia resulting from chronic kidney disease, chemotherapy etc.
NICE [330]

Global biosimilar policy comparison
84
Terminology Explanation Defined by
European Medicines Agency (EMA)
A decentralized agency of the European Union and accountable for the scientific evaluation and safety monitoring of medicines
EMA [331]
Extrapolation of indications
Extension of approved therapeutic indications of a biosimilar to include indications of the reference drug
EMA [323]
Gainsharing Agreements between hospitals and physicians, or hospitals and payers, whereby both parties share the benefit of any reduction in the treatment costs from a measure
Health lawyers [332]
General physician
Physicians who provide a wide range of non-surgical health care to adult patients
IMSANZ [333]
Good manufacturing practice (GMP)
A system which ensures that the products are consistently produced and controlled according to quality standards.
WHO [334]
Granulocyte-colony stimulating factor (G-CSF)
A factor that stimulates bone marrow to produce granulocytes and stem cells
NHS [335]
Health technology assessment (HTA)
A process to assess the social, economic, organizational and ethical issues of a health intervention or health technology
WHO [336]
Human Growth Hormone (HGH)
A hormone that stimulates growth, cell reproduction and cell regeneration NHS [337]
Inpatient care Refers to medical services that require admission into a hospital. CMS [338]
Interchangeability
The possibility of exchanging one medicine for another medicine and expected to have the same clinical effect
EMA [323]
International Non-proprietary Name (INN)
A unique name that identifies active pharmaceutical ingredients and is globally recognized
WHO [339]
Market access A process to ensure that all the appropriate patients receive the medicine at the right time and right price
PMlive [340]
Market authorization
A document issued by the drug regulatory authority for the purpose of marketing of a product after evaluation for safety, efficacy and quality.
WHO [341]
Mechanism of Action
The pharmacologic action of the drug at the receptor, membrane, or tissue level
US FDA [342]
National authorization procedures
Each EU country has its own national authorization procedures and the drug manufacturer can proceed for market authorization by the following way under national authorization procedure:
• Mutual-recognition procedure: when a marketing authorization granted in one member country can be recognized in other EU countries
• Decentralized procedure: when a medicine that has not yet been authorized in the EU can be at the same time authorized in several EU Member States
EMA [343]
Non-accessible category
The products within the same ATC4 code as the accessible category products; however, they are typically second generation products. The products in this category may have different dosing schedules and / or route of administration to those in the accessible category
IMS [10]
Outpatient care Medical services that do not require a prolonged stay at the hospital CMS [338]
Over-the-counter drugs
Drugs that are safe for use without the supervision of a health care professional and they can be purchased without a prescription.
US FDA [344]
Pharmacovigilance
Detecting and assessing adverse drug reactions EMA [323]

Global biosimilar policy comparison
85
Terminology Explanation Defined by
Quality-Adjusted Life Year (QALY)
Measure for the benefit of a treatment in terms of additional length of life, adjusted to reflect the quality of life. QALYs are calculated by estimating the years of life remaining for a patient following a particular treatment or intervention and weighting each year with a quality-of-life score (on a 0 to 1 scale), reflecting the person’s ability to carry out the activities of daily life, and freedom from pain and mental disturbance
NICE [345]
Reference medicine
Biologic chosen by the biosimilar developer to use as a reference for head-to-head comparison of quality, safety and efficacy
EMA [323]
Reference pricing
A means of controlling expenditure on the reimbursement of drugs by making use of equivalent drugs in the market and setting a reimbursement tariff (reference price) for the drugs which are considered to be “interchangeable”.
WHO [346]
Risk Management Plan (RMP)
Companies applying for marketing authorization in the EU must submit an RMP for each new medicine, including biologic medicines. The RMP, which is tailored for each product, includes a pharmacovigilance plan and risk minimization measures
EMA [347]
Specialist care Specialized medical services which are provided by a specialist physician Dignity Health [348]
Substitution The practice of dispensing one medicine instead of another equivalent and interchangeable medicine at the pharmacy level, usually without consulting the prescriber
EMA [323]
Switching Occurs when the prescriber decides to exchange one medicine for another medicine with the same therapeutic intent
EMA [323]
Total market Includes both the accessible and the non-accessible product markets IMS [10]
Universal healthcare coverage
It refers to a healthcare system that provides health care protection to all the citizens of a particular country
WHO [349]

Global biosimilar policy comparison
86
IV. References
[1] D. Kent, S. Rickwood and S. Di Blase, "Disruption and Maturity: The next phase of biologics," 2017. [Online]. Available: http://www.imshealth.com/files/web/Global/white%20paper/QI_Disruption_and_maturity_The_next_phase_of_biologics.pdf. [Accessed 15 August 2017].
[2] A. V. Klein, J. Wang and P. Bedford, "Subsequent entry biologics (biosimilars) in Canada: approaches to interchangeability and the extrapolation of indications and uses," 2014. [Online]. Available: http://gabi-journal.net/subsequent-entry-biologics-biosimilars-in-canada-approaches-to-interchangeability-and-the-extrapolation-of-indications-and-uses.html#T1.
[3] EY Knowledge - Life Sciences Team, "Your guide to understand Biosimilars - includes market performance and competitive landscape," EYGM Limited, 2017.
[4] D. M. Coory, "Extrapolation of indications for biosimilars - Regulatory perspective," Australian Government - Department of Health - Therapeutic Goods Administration, 2015.
[5] I. Royzman and A. D. Cohen, "United States: Biobetters: The Advantages And Challenges Of Being Better," 1 July 2015. [Online]. Available: http://www.mondaq.com/unitedstates/x/408998/Patent/Biobetters+The+Advantages+And+Challenges+Of+Being+Better. [Accessed 16 August 2017].
[6] S. B. Dusetzina, "Cost Sharing and Adherence to Tyrosine Kinase Inhibitors for Patients With Chronic Myeloid Leukemia," February 2014. [Online]. Available: http://ascopubs.org/doi/abs/10.1200/jco.2013.52.9123. [Accessed 30 10 2017].
[7] S. Milmo, "Labeling of Biosimilars," 1 February 2015. [Online]. Available: http://www.biopharminternational.com/labeling-biosimilars-0. [Accessed 18 August 2017].
[8] L. Christl, "FDA - From our perspective: Biosimilar product labeling," 15 June 2016. [Online]. Available: https://www.fda.gov/Drugs/NewsEvents/ucm493240.htm. [Accessed 18 August 2017].
[9] Medicines, Diagnostics and Personalised Medicine Policy Team, National Medical Directorate, NHS England, "Commissioning framework for biological medicines," 12 September 2017. [Online]. Available: https://www.england.nhs.uk/wp-content/uploads/2017/09/biosimilar-medicines-commissioning-framework.pdf. [Accessed 13 October 2017].
[10] QuintilesIMS, "The Impact of Biosimilar Competition in Europe," May 2017. [Online]. Available: http://www.medicinesforeurope.com/wp-content/uploads/2017/05/IMS-Biosimilar-2017_V9.pdf. [Accessed 18 July 2017].
[11] Simon Kucher and Partners, "Payer's price & market access policies supporting a sustainable biosimilar medicines market," Simon Kucher & Partners, September 2016. [Online]. Available: http://www.medicinesforeurope.com/wp-content/uploads/2016/09/Simon-Kucher-2016-Policy-requirements-for-a-sustainable-biosimilar-market-FINAL-report_for-publication.pdf. [Accessed 10 July 2017].
[12] Australian Government - The Department of Health, "Who chooses whether the biosimilar medicine or the reference biological medicine is used?," 23 March 2017. [Online]. Available: http://www.health.gov.au/internet/main/publishing.nsf/Content/biosimilar-hp-who-chooses-whether-biosimilar-medicine-or-reference-biological-medicine-is-used. [Accessed 20 September 2017].
[13] UN, Department of Economic and Social Affairs, Population Division, "World Population Prospects," [Online]. Available: https://esa.un.org/unpd/wpp/.
[14] OECD Stat, "Level of GDP per capita and productivity," [Online]. Available: https://stats.oecd.org/Index.aspx?DataSetCode=PDB_LV. [Accessed 14 7 2017].
[15] OECD Data, "Doctors," [Online]. Available: https://data.oecd.org/healthres/doctors.htm. [Accessed 14 7 2017].
[16] OECD Data, "Hospital beds," [Online]. Available: https://data.oecd.org/healtheqt/hospital-beds.htm. [Accessed 14 7 2017].
[17] OECD Data, "Health Spending," [Online]. Available: https://data.oecd.org/healthres/health-spending.htm. [Accessed 14 7 2017].
[18] NHS Clinical Commissioners, "About CCGs," [Online]. Available: https://www.nhscc.org/ccgs/. [Accessed 18 August 2017].
[19] NHS, "The NHS in England," 13 April 2016. [Online]. Available: http://www.nhs.uk/NHSEngland/thenhs/about/Pages/overview.aspx. [Accessed 18 August 2017].
[20] National Audit Office, "Healthcare across the UK: A comparison of the NHS in England, Scotland, Wales and Northern Ireland," 2012. [Online]. Available: https://www.nao.org.uk/report/healthcare-across-the-uk-a-comparison-of-the-nhs-in-england-scotland-wales-and-northern-ireland/. [Accessed 30 October 2017].
[21] OECD Stat, "Pharmaceutical Market: Generic market," [Online]. Available: http://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_PHMC. [Accessed 14 7 2017].
[22] Gov.uk, "Guidance - Apply for a licence to market a medicine in the UK," [Online]. Available: https://www.gov.uk/guidance/apply-for-a-licence-to-market-a-medicine-in-the-uk. [Accessed 18 7 2017].
[23] European Observatory on Health Systems and Policies, "Pharmaceutical regulation in 15 European countries," 2016. [Online]. Available: http://www.euro.who.int/__data/assets/pdf_file/0019/322444/HiT-pharmaceutical-regulation-15-European-countries.pdf.
[24] National Institute for Health and Care Excellence, "Technology appraisal guidance," 2017. [Online]. Available: https://www.nice.org.uk/About/What-we-do/Our-Programmes/NICE-guidance/NICE-technology-appraisal-guidance. [Accessed 30 October 2017].
[25] Department of Health, "The Pharmaceutical Price Regulation Scheme 2014," [Online]. Available: https://www.gov.uk/government/publications/pharmaceutical-price-regulation-scheme-2014. [Accessed 10 7 2017].
[26] Gov.uk, "PPRS: payment percentage 2017," [Online]. Available: https://www.gov.uk/government/publications/pprs-payment-percentage-2017. [Accessed 25 7 2017].
[27] GaBI, "Policies and Legislation," 2011. [Online]. Available: http://www.gabionline.net/Country-Focus/United-Kingdom/Policies-and-Legislation. [Accessed 17 July 2017].
[28] L. Taylor, "NICE to help develop local drug formularies," 7 February 2012. [Online]. Available: http://www.pharmatimes.com/news/nice_to_help_develop_local_drug_formularies_975780. [Accessed 15 August 2017].
[29] "Regional Medicines Optimisation Committees," [Online]. Available: https://www.england.nhs.uk/wp-content/uploads/2016/08/rmoc-proposals-for-establishment.pdf.
[30] SMC, "Home page," [Online]. Available: https://www.scottishmedicines.org.uk/. [Accessed 4 August 2017].

Global biosimilar policy comparison
87
[31] NHS England, "Get help with prescription costs," [Online]. Available: http://www.nhs.uk/NHSEngland/Healthcosts/Pages/Prescriptioncosts.aspx. [Accessed 24 July 2017].
[32] NHS National Statistics., Prescriptions Dispensed in the Community Statistics for 1998 to 2008, England: The Information Centre (Health Care), 2009.
[33] NHS England, "What is a biosimilar medicine?," 24 September 2015. [Online]. Available: https://www.england.nhs.uk/wp-content/uploads/2015/09/biosimilar-guide.pdf. [Accessed 30 October 2017].
[34] S. d. C. Steven Simoens, "Sustaining Generic Medicines Markets in Europe," 2006. [Online]. Available: http://journals.sagepub.com/doi/abs/10.1057/palgrave.jgm.4940128.
[35] NICE British Formulary, "Benepali," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/10-musculoskeletal-and-joint-diseases/101-drugs-used-in-rheumatic-diseases-and-gout/1013-drugs-that-suppress-the-rheumatic-disease-process/cytokine-modulators/etanercept/benepali. [Accessed 4 August 2017].
[36] Boehringer Ingelheim, "European Commission grants Lilly and Boehringer Ingelheim's insulin glargine product marketing authorisation in Europe," 10 September 2014. [Online]. Available: https://www.boehringer-ingelheim.com/press-release/european-commission-grants-lilly-and-boehringer-ingelheims-insulin-glargine-product. [Accessed 30 October 2017].
[37] NICE British formulary, "Follitropin-alfa," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/6-endocrine-system/65-hypothalamic-and-pituitary-hormones-and-anti-oestrogens/651-hypothalamic-and-anterior-pituitary-hormones-and-anti-oestrogens/anterior-pituitary-hormones/gonadotrophins/follitropin-alf. [Accessed 4 August 2017].
[38] NICE British Formulary, "Inflectra," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/10-musculoskeletal-and-joint-diseases/101-drugs-used-in-rheumatic-diseases-and-gout/1013-drugs-that-suppress-the-rheumatic-disease-process/cytokine-modulators/infliximab/inflectra. [Accessed 4 August 2017].
[39] NICE British formulary, "Remsima," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/10-musculoskeletal-and-joint-diseases/101-drugs-used-in-rheumatic-diseases-and-gout/1013-drugs-that-suppress-the-rheumatic-disease-process/cytokine-modulators/infliximab/remsima. [Accessed 4 August 2017].
[40] NICE British Formulary, "Nivestim," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/9-nutrition-and-blood/91-anaemias-and-some-other-blood-disorders/916-drugs-used-in-neutropenia/filgrastim/nivestim. [Accessed 4 August 2017].
[41] NICE British Formulary, "Zarzio," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/9-nutrition-and-blood/91-anaemias-and-some-other-blood-disorders/916-drugs-used-in-neutropenia/filgrastim/zarzio. [Accessed 4 August 2017].
[42] NICE British Formulary, "Ratiograstim," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/9-nutrition-and-blood/91-anaemias-and-some-other-blood-disorders/916-drugs-used-in-neutropenia/filgrastim/ratiograstim. [Accessed 4 August 2017].
[43] NICE British Formulary, "Retacrit," july 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/9-nutrition-and-blood/91-anaemias-and-some-other-blood-disorders/913-drugs-used-in-hypoplastic-haemolytic-and-renal-anaemias/erythropoietins/epoetin-alfa-beta-and-zeta/epoetin-zeta/retacrit. [Accessed 4 August 2017].
[44] NICE British Formulary, "Binocrit," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/9-nutrition-and-blood/91-anaemias-and-some-other-blood-disorders/913-drugs-used-in-hypoplastic-haemolytic-and-renal-anaemias/erythropoietins/epoetin-alfa-beta-and-zeta/epoetin-alfa/binocrit. [Accessed 4 August 2017].
[45] NICE British formulary, "Omnitrope," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/6-endocrine-system/65-hypothalamic-and-pituitary-hormones-and-anti-oestrogens/651-hypothalamic-and-anterior-pituitary-hormones-and-anti-oestrogens/anterior-pituitary-hormones/growth-hormone/somatropin/omni. [Accessed 4 August 2017].
[46] Technavio, "Global cardiovascular and metabolic disorders biosimilars market," August 2016. [Online]. Available: https://www.technavio.com/report/global-cardiovascular-and-metabolic-disorders-biosimilars-market. [Accessed 3 August 2017].
[47] Medicines and Healthcare products Regulatory Agency , "Reporting suspected adverse drug reactions to vaccines and biological medicines," November 2012. [Online]. Available: https://www.gov.uk/drug-safety-update/reporting-suspected-adverse-drug-reactions-to-vaccines-and-biological-medicines. [Accessed 30 October 2017].
[48] NICE, "Biosimilar medicines," January 2017. [Online]. Available: https://www.nice.org.uk/advice/ktt15/chapter/evidence-context. [Accessed 11 July 2017].
[49] ISPOR, "Are EU Payers Adapting Biosimilar Pricing and Reimbursement Approval Processes to Optimize Healthcare Savings?," 2015. [Online]. Available: https://www.ispor.org/research_pdfs/49/pdffiles/PHP106.pdf. [Accessed 17 July 2017].
[50] Gov.uk, "Guidance - Pharmaceutical price regulation scheme 2014," 21 December 2015. [Online]. Available: https://www.gov.uk/government/publications/pharmaceutical-price-regulation-scheme-2014. [Accessed 4 August 2017].
[51] Scottish Medicines Consortium, "About SMC," May 2015. [Online]. Available: https://www.scottishmedicines.org.uk/About_SMC/Policy_statements/Biosimilar_Medicines. [Accessed 4 August 2017].
[52] https://www.scottishmedicines.org.uk/SMC_Advice/Advice/1007_14_infliximab_Inflectra/Briefing_note_infliximab_Inflectra, "Briefing note infliximab Inflectra," 9 March 2015. [Online]. Available: https://www.scottishmedicines.org.uk/SMC_Advice/Advice/1007_14_infliximab_Inflectra/Briefing_note_infliximab_Inflectra. [Accessed 4 August 2017].
[53] Scottish Medicines Consortium, "Infliximab Remicade RESUBMISSION," 12 May 2014. [Online]. Available: https://www.scottishmedicines.org.uk/SMC_Advice/Advice/374_07_infliximab_100mg_powder_for_intravenous_infusion_Remicade/infliximab_Remicade_RESUBMISSION. [Accessed 4 August 2017].
[54] SMC, "Infliximab Remicade," 11 March 2013. [Online]. Available: https://www.scottishmedicines.org.uk/SMC_Advice/Advice/854_13_infliximab_Remicade/infliximab_Remicade. [Accessed 4 August 2017].
[55] SMC, "Infliximab Remicade," 10 October 2011. [Online]. Available: https://www.scottishmedicines.org.uk/SMC_Advice/Advice/739_11_infliximab_Remicade/infliximab_Remicade. [Accessed 4 August 2017].
[56] SMC, "Infliximab (Remicade)," 10 March 2008. [Online]. Available: https://www.scottishmedicines.org.uk/SMC_Advice/Advice/448_08_infliximab_100mg_powder__Remicade_/infliximab__Remicade_. [Accessed 4 August 2017].

Global biosimilar policy comparison
88
[57] SMC, "Infliximab 100mg powder for intravenous infusion (Remicade)," 7 May 2007. [Online]. Available: https://www.scottishmedicines.org.uk/SMC_Advice/Advice/infliximab_100_mg_powder_for_intravenous_infusion__Remicade_/infliximab__Remicade__318_06. [Accessed 4 August 2017].
[58] SMC, "Infliximab 100mg vial of powder for intravenous infusion," 12 July 2004. [Online]. Available: https://www.scottishmedicines.org.uk/SMC_Advice/Advice/Infliximab_100mg_vial_of_powder_for_intravenous_infusion__Remicade__174__/Infliximab__Remicade_. [Accessed 4 August 2017].
[59] C. Rémuzat, A. Kapuśniak, A. Caban, D. Ionescu, G. Radière, C. Mendoza and M. Toumi, "Supply-side and demand-side policies for biosimilars: an overview in 10 European member," 28 April 2017. [Online]. Available: http://www.tandfonline.com/doi/pdf/10.1080/20016689.2017.1307315. [Accessed 25 July 2017].
[60] Health Improvement Scotland, "Biosimilar Medicines: A national prescribing framework," May 2015. [Online]. Available: http://www.healthcareimprovementscotland.org/our_work/technologies_and_medicines/programme_resources/biosimilar_medicines_framework.aspx. [Accessed 18 August 2017].
[61] BioPharma Reporter, "NHS England rules on biosimilar interchangeability," 2015. [Online]. Available: http://www.biopharma-reporter.com/Markets-Regulations/NHS-England-rules-on-biosimilar-interchangeability. [Accessed 11 July 2017].
[62] isdscotland, "Health-Topics/Prescribing-and-Medicines," [Online]. Available: https://www.isdscotland.org/Health-Topics/Prescribing-and-Medicines/Publications/2016-07-12/2016-07-12-Prescribing-PrescriptionCostAnalysis-Report.pdf.
[63] NHS UK, "Biosimilar Medicines," [Online]. Available: https://www.england.nhs.uk/ourwork/pe/mo-dash/biosimilar-medicines/. [Accessed 17 July 2017].
[64] British Biosimilars Association, "About Us," [Online]. Available: http://britishbiosimilars.co.uk/about-us. [Accessed 11 July 2017].
[65] UK Medicines Information, "Medicines Information Update," June 2017. [Online]. Available: https://www.sps.nhs.uk/wp-content/uploads/2017/06/MI-update-Jun-2017-national.pdf. [Accessed 18 August 2017].
[66] NHS England, "GE3: Hospital medicines optimisation," [Online]. Available: https://www.england.nhs.uk/wp-content/uploads/2016/11/ge3-hospital-medicines-optimisation.pdf. [Accessed 13 October 2017].
[67] NHS England, "Commissioning for Quality and Innovation (CQINN) - Guidance for 2017-2019," November 2016. [Online]. Available: https://www.england.nhs.uk/wp-content/uploads/2016/11/cquin-2017-19-guidance.pdf. [Accessed 13 October 2017].
[68] Precision Medicine Group, "Impact of market access factors in the adoption of biosimilar anti-TNFs across Europe," 2017, 2017. [Online]. Available: https://www.precisionmedicinegrp.com/pfv/wp-content/uploads/sites/2/2017/03/Impact-of-market-access-factors-in-the-adoption-of-biosimilar-anti-TNFs.pdf. [Accessed 17 July 2017].
[69] ABPI, "ABPI position on biosimilar medicines," 2 May 2015. [Online]. Available: http://www.abpi.org.uk/our-work/library/Documents/ABPI%20position%20on%20biosimilar%20medicines.pdf. [Accessed 3 August 2017].
[70] WHO - European Observatory on Health Systems and Policies, "Germany - Health system review," 2014. [Online]. Available: http://www.euro.who.int/__data/assets/pdf_file/0008/255932/HiT-Germany.pdf?ua=1. [Accessed 7 August 2017].
[71] Bundesministerium für Gesundheit, "Demographischer Wandel," [Online]. Available: https://www.bundesgesundheitsministerium.de/themen/krankenversicherung/herausforderungen/demografischer-wandel.html. [Accessed 29 6 2017].
[72] Bundesministerium für Gesundheit, "Wettbewerb im Gesundheitswesen," [Online]. Available: https://www.bundesgesundheitsministerium.de/themen/krankenversicherung/herausforderungen/wettbewerb.html. [Accessed 29 6 2017].
[73] Association of Research-Based Pharmaceutical Companies (vfa), "Arzneimittelmarkt Deutschland," [Online]. Available: https://www.vfa.de/de/wirtschaft-politik/strukturdaten/statistics-am-deutschland. [Accessed 29 6 2017].
[74] European Observatory on Health Systems and Policies, "Pharmaceutical regulation in 15 European countries," 2016. [Online]. Available: http://www.euro.who.int/__data/assets/pdf_file/0019/322444/HiT-pharmaceutical-regulation-15-European-countries.pdf.
[75] Stiftung Warentest, "Test.de - Arzneimittelpreise," [Online]. Available: https://www.test.de/medikamente/begriffe/arzneimittelpreise/. [Accessed 29 June 2017].
[76] P. J. Fuhr and A. Chandra, "Product naming, pricing, and market uptake of biosimilars," 2015. [Online]. Available: http://gabi-journal.net/product-naming-pricing-and-market-uptake-of-biosimilars.html. [Accessed 10 July 2017].
[77] BPI: German Pharmaceutical Industry Association, "Pharma-Data 2016," 2016. [Online]. Available: http://www.bpi.de/fileadmin/media/bpi/Downloads/Internet/Publikationen/Pharma-Daten/Pharmadaten_2016_EN.pdf. [Accessed 2 August 2017].
[78] Pro Biosimilars, "Brochure: Biosimilars In Figures - The Year 2016 At A Glance," 11 May 2017. [Online]. Available: http://probiosimilars.de/tag/daten-und-zahlen/. [Accessed 2 August 2017].
[79] Visiongain, "Visiongain biosimilars in Germany," 17 June 2015. [Online]. Available: https://www.visiongain.com/Report/1462/Biosimilars-and-Follow-On-Biologics-World-Industry-and-Market-Prospects-2015-2025. [Accessed 7 July 2017].
[80] G. Foxon, G. Fox and P. Craddy, "Are EU Payers Adapting Biosimilar Pricing and Reimbursement Approval Processes to Optimize Healthcare Savings?," 16 May 2015. [Online]. Available: https://www.ispor.org/research_pdfs/49/pdffiles/PHP106.pdf. [Accessed 4 August 2017].
[81] Gesetze im Internet, "Gesetz über den Verkehr mit Arzneimitteln (Arzneimittelgesetz - AMG)," [Online]. Available: http://www.gesetze-im-internet.de/amg_1976/__24b.html. [Accessed 8 August 2017].
[82] BfArM, "Zulassung von Biosimilars," [Online]. Available: http://www.bfarm.de/DE/Arzneimittel/zul/zulassungsarten/biosimilars/_node.html. [Accessed 8 August 2017].
[83] Value in Health Journal, "Biosimilars And Reference Price Groups In Germany," 2016. [Online]. Available: http://www.valueinhealthjournal.com/article/S1098-3015(16)32071-X/fulltext. [Accessed 2 August 2017].
[84] Gemeinsamer Bundesausschuss, "Arzneimittel-Richtlinie/Anlage IX: Einleitung eines Stellungnahmeverfahrens – Festbetragsgruppenbildung Infliximab, Gruppe 1, in Stufe 1," 6 December 2016. [Online]. Available: https://www.g-ba.de/informationen/beschluesse/2787/. [Accessed 30 October 2017].
[85] GKV-Spitzenverband, "Rahmenvertrag über die Arzneimittelversorgung nach § 129 Absatz 2 SGB V," 30 September 2016. [Online]. Available: https://www.gkv-

Global biosimilar policy comparison
89
spitzenverband.de/media/dokumente/krankenversicherung_1/arzneimittel/rahmenvertraege/apotheken/AM_20160930_Rahmenvertrag_129_Absatz-2_SGB-V.pdf. [Accessed 4 August 2017].
[86] GaBI, "Product naming, pricing, and market uptake of biosimilars," 2015. [Online]. Available: http://gabi-journal.net/product-naming-pricing-and-market-uptake-of-biosimilars.html#R36. [Accessed 2 August 2017].
[87] GKV-SV, "Rahmenverträge zur Arzneimittelversorgung," 30 September 2016. [Online]. Available: https://www.gkv-spitzenverband.de/krankenversicherung/arzneimittel/rahmenvertraege/rahmenvertraege.jsp. [Accessed 8 August 2017].
[88] Pharma Voice, "Germany Puts Focus on Pharma Innovation," September 2016. [Online]. Available: http://www.pharmavoice.com/article/2016-09-germany/. [Accessed 2 August 2017].
[89] Medicines for Europe, "What you need to know about Biosimilar Medicinal Products," European Commission, 2013. [Online]. Available: http://www.medicinesforeurope.com/wp-content/uploads/2016/03/biosimilars_report_en.pdf. [Accessed 10 July 2017].
[90] ISPOR, "Biologic Brands and Biosimilars for Rheumatoid Arthritis in the EU5," 2016. [Online]. Available: https://www.ispor.org/research_pdfs/49/pdffiles/PMS77.pdf. [Accessed 4 August 2017].
[91] VfA, "vfa-Positionspapier Biosimilars english," December 2016. [Online]. Available: https://www.vfa.de/download/biosimilars-en.pdf. [Accessed 7 August 2017].
[92] Pro Generika, "Effects of tendering on the generics industry in Germany," [Online]. Available: http://www.progenerika.de/wp-content/uploads/2014/02/ENGLISH_FINAL-Stn-BMWi_Anfrage_Auswirkung-von-RVausschreibungen-auf-die-Generikaindustrie_Stand-15.2.2013.pdf. [Accessed 2 August 2017].
[93] APM Health Europe, "Fixed-price group for biosimilars 'problematic' - German lobby," 19 January 2017. [Online]. Available: http://www.apmhealtheurope.com/Fixed-price-group-for-biosimilars-%27problematic%27---German-lobby-FS_51404.html. [Accessed 2 August 2017].
[94] C. L. Pen, "ISPOR - The French Health Care System," [Online]. Available: https://www.ispor.org/news/articles/November09/tfhcs.asp. [Accessed 7 7 2017].
[95] French Property, "Hidden Costs of Healthcare in France," [Online]. Available: https://www.french-property.com/news/french_health/medical_treatment_charges/. [Accessed 7 7 2017].
[96] K. B. B. I. D.-Z. C. H.-Q. (. Karine Chevreul, "France: Health System Review 2015," 2015. [Online]. Available: http://www.euro.who.int/__data/assets/pdf_file/0011/297938/France-HiT.pdf. [Accessed 31 October 2017].
[97] Smart Pharma, "Global Biosimilar Drugs Market Outlooks," February 2015. [Online]. Available: http://www.smart-pharma.com/uploads/files/Rapport_Biosimilars_2015_Excerpts-3.pdf. [Accessed 8 August 2017].
[98] Santé, French Government : Ministère des Solidarités et de la, «Médicaments - Professionnels de la santé,» September 2016. [En ligne]. Available: http://solidarites-sante.gouv.fr/soins-et-maladies/medicaments/professionnels-de-sante/prescription-et-dispensation/article/prescription-en-denomination-commune-internationale-dci. [Accès le 31 July 2017].
[99] HAS, "Assessment and Recommendation," [Online]. Available: https://www.has-sante.fr/portail/jcms/c_2567683/en/portail-english-assessment-recommendation?portal=c_2567683. [Accessed 3 August 2017].
[100] LinkedIn, "Les medicaments biosimilaires en France : Quelles perspectives de croissance a l’horizon 2020 ?," 10 July 2017. [Online]. Available: https://fr.linkedin.com/pulse/les-medicaments-biosimilaires-en-france-quelles-de-charrondi%C3%A8re. [Accessed 8 August 2017].
[101] ISPOR, "Are EU Payers Adapting Biosimilar Pricing and Reimbursement Approval Processes to Optimize Healthcare Savings?," May 2015. [Online]. Available: https://www.ispor.org/research_pdfs/49/pdffiles/PHP106.pdf. [Accessed 17 July 2017].
[102] Decision Resources, "Is France's Biosimilar Pharmacy-Level Substitution a Harbinger of Change?," 8 April 2014. [Online]. Available: https://decisionresourcesgroup.com/drg-blog/drug-watch/is-frances-biosimilar-pharmacy-level-substitution-a-harbinger-of-change/. [Accessed 3 August 2017].
[103] Ministère de l’économie et des finances / Ministère des affaires sociales et de la santé, "Projet de Loi de financement de financement de la sécurité sociale pour 2014," 2014. [Online]. Available: http://www.securite-sociale.fr/IMG/pdf/plfss_2014_expose_motifs_cm_09.10.2013.pdf. [Accessed 31 October 2017].
[104] AFMPS, "Biosimilaires," [Online]. Available: https://www.fagg-afmps.be/fr/humain/medicaments/medicaments/procedures_damm/Procedures_enregistrement/Biosimilaires. [Accessed 31 July 2017].
[105] France Foundation, "Avoiding the Path of Least Resistance," 27 June 2017. [Online]. Available: http://www.francefoundation.com/avoiding-the-path-of-least-resistance. [Accessed 5 July 2017].
[106] France Foundation, "How Can We Engage Learners if They are Unaware of Their Own Educational Gaps?," 15 November 2016. [Online]. Available: http://www.francefoundation.com/how-can-we-engage-learners-if-they-are-unaware-of-their-own-educational-gaps. [Accessed 5 July 2017].
[107] the Ministry of Health, "Instruction DGOS/DSS/DGS/CAMTS 2017-244," 12 October 2017. [Online]. Available: http://circulaire.legifrance.gouv.fr/pdf/2017/10/cir_42638.pdf. [Accessed 11 December 2017].
[108] LEEM, "Economic challenges: restructuring healthcare expenditure regulation," 8 January 2014. [Online]. Available: http://www.leem.org/sites/default/files/Voeux%202014%20ang%20-%20ConstatsPropositions%20DEF.pdf. [Accessed 1 August 2017].
[109] A. Annell, "The Public–Private Pendulum — Patient Choice and Equity in Sweden (New England Journal of Medicine)," 1 January 2015. [Online]. Available: http://www.nejm.org/doi/full/10.1056/NEJMp1411430.
[110] A. Anell, "The Swedish Health Care System," February 2008. [Online]. Available: http://www.commonwealthfund.org/~/media/files/resources/2008/health-care-system-profiles/sweden_country_profile_2008-pdf.pdf.
[111] Health Consumer Powerhouse, "Euro Health Consumer Index 2016," 2016. [Online]. Available: http://www.healthpowerhouse.com/files/EHCI_2016/EHCI_2016_report.pdf.
[112] C. Guibourg, "Private Health Insurance in Sweden - A clash of cultures," October 2011. [Online]. Available: https://www.thelocal.se/20111010/36648.
[113] The Local, "Swedes buy insurance to skip long health queues," January 2014. [Online]. Available: https://www.thelocal.se/20140117/hospital-queues-tied-to-insurance-trend.
[114] TLV, "Analys av marknaden för biologiska läkemedel med konkurrens av biosimilarer," June 2016. [Online]. Available: https://www.tlv.se/Upload/Ovrigt/Rapport_160615_biosimilarer.pdf. [Accessed 12 July 2017].

Global biosimilar policy comparison
90
[115] TLV / PPRI / WHO, "Sweden - Recent and planned developments in pharmaceutical policies 2016," [Online]. Available: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationPosters/SE_Poster_PPRI_Meeting_Lisbon_Apr2016.pdf. [Accessed 16 August 2017].
[116] TLV, "International price comparison of pharmaceuticals 2016," 2016. [Online]. Available: https://www.tlv.se/Upload/English/Report_international_price_comparison_pharmaceuticals_2016.pdf. [Accessed 20 December 2017].
[117] LV, "Therapeutic recommendations / Factoring exercises etc.," [Online]. Available: https://lakemedelsboken.se/kapitel/regelverket_och_it-stod/receptskrivningsregler.html. [Accessed 10 August 2017].
[118] TLV, "TLV Database," [Online]. Available: https://www.tlv.se/beslut/sok/lakemedel/. [Accessed 1 August 2017].
[119] WHO, "Sweden: Recent and planned developments in pharmaceutical policies 2016," WHO, [Online]. Available: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationPosters/SE_Poster_PPRI_Meeting_Lisbon_Apr2016.pdf. [Accessed 11 July 2017].
[120] Medical Products Agency, "Welcome to the Medical Products Agency - Sweden," [Online]. Available: https://lakemedelsverket.se/english/. [Accessed 8 August 2017].
[121] PPRI and TLV, "PPRI Pharma Profile: Sweden 2017," 2017. [Online]. Available: https://www.tlv.se/Upload/English/PPRI_Pharma_Profile_Sweden_2017.pdf. [Accessed 11 July 2017].
[122] G. Foxon, G. Fox and P. Craddy, "Are EU payers adopting biosimilar pricing and reimbursement approval processes to optimize healthcare savings?," May 2015. [Online]. Available: https://www.ispor.org/research_pdfs/49/pdffiles/PHP106.pdf. [Accessed 16 August 2017].
[123] TLV, "International price comparison of pharmaceuticals 2016," TLV, December 2015. [Online]. Available: https://www.tlv.se/Upload/English/Report_international_price_comparison_pharmaceuticals_2016.pdf. [Accessed 11 July 2017].
[124] N. Swartenbroekx, M.-I. Farfan-Portet, J. Espín and S. Gerkens, "Incentives for market penetration of biosimilars in Belgium and in five European countries," 2014. [Online]. Available: https://www.researchgate.net/profile/Jaime_Espin/publication/273955449_Incentives_for_market_penetration_of_biosimilars_in_Belgium_and_in_five_European_countries/links/5612ae1308ae4f0b65159810/Incentives-for-market-penetration-of-biosimilars-in-Belgium-an. [Accessed 25 July 2017].
[125] QuintilesIMS, "Delivering on the Potential of Biosimilar Medicines," IMS Quintiles, March 2016. [Online]. Available: http://www.imshealth.com/files/web/IMSH%20Institute/Healthcare%20Briefs/Documents/IMS_Institute_Biosimilar_Brief_March_2016.pdf. [Accessed 25 July 2017].
[126] Statens legemiddelverk, "The Norwegian health care system and pharmaceutical system," [Online]. Available: https://legemiddelverket.no/english/about-us/the-norwegian-health-care-system-and-pharmaceutical-system. [Accessed 17 August 2017].
[127] WHO, "Health Systems in Transition - Norway," 2013. [Online]. Available: http://www.euro.who.int/__data/assets/pdf_file/0018/237204/HiT-Norway.pdf.
[128] Finans Norge, "Statistics - Non-life insurance," 2016. [Online]. Available: https://www.finansnorge.no/en/statistics1/non-life-insurance/. [Accessed 10 October 2017].
[129] LIS, "Bisimilars, purchasing systems and impact of tenders in Norway," 11 May 2015. [Online]. Available: http://www.piperska.org/sites/default/files/Mack_Biosimilars_purchasing_tenders_in_Norway.pdf. [Accessed 14 August 2017].
[130] Statens Iegemiddelverk, "General reimbursement - preapproved medicines," [Online]. Available: https://legemiddelverket.no/english/price-and-reimbursement/general-reimbursement-preapproved-medicines. [Accessed 14 August 2017].
[131] LIS, "Oversikt LIS anbud og avtaleperioder," [Online]. Available: http://sykehusinnkjop.no/wp-content/uploads/2017/07/Oversikt-LIS-anbud-og-avtaleperiode-fra-juli-2017.pdf. [Accessed 14 August 2017].
[132] Sykehusinnkjøp HF, "Sykehusinnkjøp," [Online]. Available: http://sykehusinnkjop.no/. [Accessed 17 August 2017].
[133] Sykehusinnkjøp HF, "Legemidler," [Online]. Available: http://sykehusinnkjop.no/legemidler/. [Accessed 17 August 2017].
[134] European Observatory on Health and Policies, "Norway - Health System Review," 2013. [Online]. Available: http://www.euro.who.int/__data/assets/pdf_file/0018/237204/HiT-Norway.pdf. [Accessed 20 7 2017].
[135] Statens Legemiddelverk, "Trinnpris," 2 August 2017. [Online]. Available: https://legemiddelverket.no/refusjon-og-pris/pris-pa-legemidler/trinnpris#-oversikt-over-trinnpriser-og-virkestoff-inkludert-i-trinnprissystemet. [Accessed 17 August 2017].
[136] WHO, "Norway," February 2017. [Online]. Available: http://www.who.int/health-laws/countries/nor-en.pdf?ua=1. [Accessed 1 August 2017].
[137] Apotekforeningen, "The medicines market in Norway," 2008. [Online]. Available: http://www.apotek.no/Files%2fFiler%2fNAF-bibliotek%2fPDF_Aktuelt_kolonne%2fPrisbrosjyre_engelsk2008.pdf. [Accessed 14 August 2017].
[138] Statens leggemiddelverk, "Byttelisten per 1.august 2017," 1 August 2017. [Online]. Available: https://legemiddelverket.no/nyheter/byttelisten-per-1august-2017. [Accessed 17 August 2017].
[139] NoMA, "NoMA medicine database," [Online]. Available: https://www.legemiddelsok.no/. [Accessed 8 August 2017].
[140] S. Madsen, "Bruk av biotilsvarende i Norge og andre land," 26 January 2017. [Online]. Available: https://www.dagensmedisin.no/contentassets/d7222d8e3e9d4dc9bcdbf31d1c9fd422/2_bruk-av-biotilsvarende-i-norge-og-andre-land-2017-01-26.pdf. [Accessed 17 August 2017].
[141] European Medicines Agency, "Authorisation of medicines," [Online]. Available: http://www.ema.europa.eu/ema/index.jsp?curl=pages/about_us/general/general_content_000109.jsp. [Accessed 13 July 2017].
[142] WHO, "Norway: European Region," February 2017. [Online]. Available: http://www.who.int/health-laws/countries/nor-en.pdf. [Accessed 8 August 2017].
[143] GaBI, "Norway biosimilars in different funding systems - what works," March 2015. [Online]. Available: http://gabi-journal.net/norway-biosimilars-in-different-funding-systems-what-works.html. [Accessed 16 October 2017].
[144] BioPharma Reporter, "Biosimilar discounts and switching will wipe-out J&J's Remicade in Norway says regulator," 16 October 2015. [Online]. Available: http://www.biopharma-reporter.com/Markets-Regulations/Biosimilar-discounts-will-wipe-out-Janssen-s-Remicade-sales-in-Norway. [Accessed 8 August 2017].

Global biosimilar policy comparison
91
[145] Statens legemiddelverk, "Oppdatert informasjon om bytte av biologiske legemidler i apotek," 31 May 2017. [Online]. Available: https://legemiddelverket.no/Documents/Import%20og%20salg/Apotek%C3%B8konomi/17-06581-1%20Oppdatert%20informasjon%20om%20bytte%20av%20biologiske%20legemidler%20i%20apotek%2020170531.pdf. [Accessed 17 August 2017].
[146] I. C. O. G. L. G. M. L. N. B. E. A. H. K. E. A. L. M. P. J. J. T. K. K. Kristin K Jørgensen, "Switching from originator infliximab to biosimilar CT-P13 compared with maintained treatment with originator infliximab (NOR-SWITCH): a 52-week, randomised, double-blind, non-inferiority trial," 11 May 2017. [Online]. Available: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)30068-5/abstract.
[147] Statens Legemiddelverk, "Nytt Om Legemidler," August 2017. [Online]. Available: https://legemiddelverket.no/Documents/Bivirkninger%20og%20sikkerhet/R%C3%A5d%20til%20helsepersonell/NYL/2017/2017_NYL%20nr%207-8_lavoppl%C3%B8slig.pdf. [Accessed 14 August 2017].
[148] LMI, "Biosafety: Is safe and exchangeable the same?," 2 February 2017. [Online]. Available: http://www.lmi.no/2017/02/02/biotilsvarende-er-trygg-og-byttbar-det-samme/. [Accessed 8 August 2017].
[149] US Census Bureau, "Health Insurance Coverage in the United States: 2015," [Online]. Available: https://www.census.gov/library/publications/2016/demo/p60-257.html. [Accessed 13 7 2017].
[150] DPE-AFLCIO, "The U.S. Health Care System: An International Perspective," [Online]. Available: http://dpeaflcio.org/programs-publications/issue-fact-sheets/the-u-s-health-care-system-an-international-perspective/. [Accessed 13 7 2017].
[151] American Hospital Association, "Fast Facts on US Hospitals," [Online]. Available: http://www.aha.org/research/rc/stat-studies/fast-facts.shtml. [Accessed 13 7 2017].
[152] Centers for Medicare and Medicaid Services, "National Health Expenditure Data - Historical," [Online]. Available: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.html. [Accessed 13 7 2017].
[153] Medicaid, "April 2017 Medicaid and CHIP Enrollment Data Highlights," [Online]. Available: https://www.medicaid.gov/medicaid/program-information/medicaid-and-chip-enrollment-data/report-highlights/index.html. [Accessed 13 7 2017].
[154] Healthcare.gov, "The Children's Health Insurance Program (CHIP)," [Online]. Available: https://www.healthcare.gov/medicaid-chip/childrens-health-insurance-program/. [Accessed 13 7 2017].
[155] Congressional Research Services, "The Number of Veterans that Use VA Health Care Services," [Online]. Available: https://fas.org/sgp/crs/misc/R43579.pdf. [Accessed 13 7 2017].
[156] Centers for Disease Control and Prevention, "Adult Obesity Facts," 1 September 2016. [Online]. Available: https://www.cdc.gov/obesity/data/adult.html. [Accessed 18 August 2017].
[157] A. S. Kesselheim, J. Avorn and A. Sarpatwari, "The High Cost of Prescription Drugs in the United States," 23 August 2016. [Online]. Available: http://jamanetwork.com/journals/jama/article-abstract/2545691. [Accessed 18 August 2017].
[158] S. Lupkin, "5 Reasons Prescription Drug Prices Are So High in the U.S.," 23 August 2016. [Online]. Available: http://time.com/money/4462919/prescription-drug-prices-too-high/. [Accessed 18 August 2017].
[159] FDA, "About the Center for Biologics Evaluation and Research (CBER)," [Online]. Available: https://www.fda.gov/AboutFDA/CentersOffices/OfficeofMedicalProductsandTobacco/CBER/default.htm. [Accessed 21 7 2017].
[160] FDA, "New Drugs at FDA: CDER’s New Molecular Entities and New Therapeutic Biological Products," [Online]. Available: https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DrugInnovation/ucm20025676.htm. [Accessed 21 7 2017].
[161] OECD Health Policy Studies, "Pharmaceutical Pricing - Policies in a global market," 2008. [Online]. Available: http://apps.who.int/medicinedocs/documents/s19834en/s19834en.pdf.
[162] Medicaid, "Medicaid Drug Rebate Program," [Online]. Available: https://www.medicaid.gov/medicaid/prescription-drugs/medicaid-drug-rebate-program/index.html. [Accessed 21 7 2017].
[163] Department of Health and Human Services - Office of Inspector General, "COMPARING AVERAGE SALES," March 2014. [Online]. Available: https://oig.hhs.gov/oei/reports/oei-03-13-00570.pdf. [Accessed 14 December 2017].
[164] US FDA, "Guidances: Biosimilars," [Online]. Available: https://www.fda.gov/drugs/guidancecomplianceregulatoryinformation/guidances/ucm290967.htm. [Accessed 18 July 2017].
[165] Globe Newswire, "United States Biosimilars Market Access Analysis Report 2017: The Need For Biosimilars, Regulatory Pathway, Substitution & Naming Policy, Legal Issues, Pricing Reimbursement & Access," 30 May 2017. [Online]. Available: https://globenewswire.com/news-release/2017/05/30/999780/0/en/United-States-Biosimilars-Market-Access-Analysis-Report-2017-The-Need-For-Biosimilars-Regulatory-Pathway-Substitution-Naming-Policy-Legal-Issues-Pricing-Reimbursement-Access.html. [Accessed 18 July 2017].
[166] Pfizer, "Pfizer Announces The U.S. Availability Of Biosimilar INFLECTRA® (infliximab-dyyb)," 17 October 2016. [Online]. Available: https://www.pfizer.com/news/press-release/press-release-detail/pfizer_announces_the_u_s_availability_of_biosimilar_inflectra_infliximab_dyyb. [Accessed 30 October 2017].
[167] Novartis, "Sandoz launches ZarxioTM (filgrastim-sndz), the first biosimilar in the United States," 3 September 2015. [Online]. Available: https://www.novartis.com/news/media-releases/sandoz-launches-zarxiotm-filgrastim-sndz-first-biosimilar-united-states. [Accessed 30 October 2017].
[168] Merck, "Merck Announces U.S. Launch of RENFLEXIS™ (infliximab-abda), a Biosimilar of Remicade, for All Eligible Indications," 24 July 2017. [Online]. Available: http://www.mrknewsroom.com/news-release/corporate-news/merck-announces-us-launch-renflexis-infliximab-abda-biosimilar-remicade-. [Accessed 30 October 2017].
[169] Amgen, "Amgen And AbbVie Agree To Settlement Allowing Commercialization Of AMGEVITA™," 28 September 2017. [Online]. Available: http://www.amgen.com/media/news-releases/2017/09/amgen-and-abbvie-agree-to-settlement-allowing-commercialization-of-amgevita/. [Accessed 30 October 2017].
[170] Reuters, "Novartis says court battle will delay its Enbrel copy until 2018 at least," 25 January 2017. [Online]. Available: http://uk.reuters.com/article/us-novartis-results-biosimilars/novartis-says-court-battle-will-delay-its-enbrel-copy-until-2018-at-least-idUKKBN1591KN. [Accessed 30 October 2017].
[171] Boehringer Ingelheim, "Boehringer Ingelheim Pharmaceuticals, Inc. receives FDA approval for CyltezoTM (adalimumab-adbm), a biosimilar to Humira®, for the treatment of multiple chronic inflammatory diseases," 29 August 2017. [Online]. Available:

Global biosimilar policy comparison
92
https://www.boehringer-ingelheim.com/press-release/adalimumab-biosimilar-cyltezo-receives-fda-approval. [Accessed 30 October 2017].
[172] J. Overley, "FDA Clears Amgen-Allergan Biosimilar Of Genentech's Avastin," 14 September 2017. [Online]. Available: https://www.law360.com/articles/963986/fda-clears-amgen-allergan-biosimilar-of-genentech-s-avastin. [Accessed 30 October 2017].
[173] Lilly, "BASAGLAR® (insulin glargine injection 100 units/mL), A Long-Acting Basal Insulin, Is Now Available in U.S.," 15 December 2016. [Online]. Available: https://investor.lilly.com/releasedetail.cfm?ReleaseID=1004325. [Accessed 30 October 2017].
[174] Leerink, "HCIT & Distribution, sourced via ThomsonOne," Leerink, 2017.
[175] D. Stanton, "Biosimilar boost for Pfizer but Inflectra just takes 2.3% of US infliximab market," 4 August 2017. [Online]. Available: http://www.biopharma-reporter.com/Markets-Regulations/Biosimilar-boost-for-Pfizer-but-Inflectra-share-just-2.3-of-US-market. [Accessed 17 August 2017].
[176] N. T. a. E. W. Dittman, "The First Supreme Court Review of a Biosimilar Case," 10 April 2017. [Online]. Available: http://dialogues.nypharmaforum.org/blog/the-first-supreme-court-review-of-a-biosimilar-case. [Accessed 12 December 2017].
[177] US FDA, "FDA’s Overview of the Regulatory Guidance for the Development and Approval of Biosimilar Products in the US," [Online]. Available: https://www.fda.gov/downloads/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/therapeuticbiologicapplications/biosimilars/ucm428732.pdf. [Accessed 9 August 2017].
[178] US FDA, "Reference Product Exclusivity for Biological Products Filed Under Section 351(a) of the PHS Act," August 2014. [Online]. Available: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM407844.pdf. [Accessed 9 August 2017].
[179] US FDA, "Scientific Considerations in Demonstrating Biosimilarity to a Reference Product," April 2015. [Online]. Available: https://www.fda.gov/downloads/drugs/guidances/ucm291128.pdf. [Accessed 9 August 2017].
[180] US FDA, "Nonproprietary Naming of Biological Products," January 2017. [Online]. Available: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM459987.pdf. [Accessed 9 August 2017].
[181] DataMonitor, "Biosimilars Market Access in the US," DataMonitor, March 2017.
[182] RAPS, "US Supreme Court: No Six-Month Wait for Biosimilars After FDA Approval," 12 June 2017. [Online]. Available: http://www.raps.org/Regulatory-Focus/News/2017/06/12/27881/US-Supreme-Court-No-Six-Month-Wait-for-Biosimilars-After-FDA-Approval/. [Accessed 9 August 2017].
[183] U.S. Food & Drug Administration, "Guidance for Industry on Biosimilars: Q & As Regarding Implementation of the BPCI Act of 2009: Questions and Answers Part I," 3 February 2016. [Online]. Available: https://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm259809.htm#Q11. [Accessed 30 October 2017].
[184] DCAT connect, "US Sets Course for Biosimilar Pricing and Use," 2015. [Online]. Available: http://connect.dcat.org/blogs/patricia-van-arnum/2015/04/06/us-sets-course-for-biosimilar-pricing-and-use#.WXXL54SGOM8. [Accessed 24 July 2017].
[185] Z. Brennan, "US CMS releases new info around biosimilar pricing uptake," 2 April 2015. [Online]. Available: http://www.biopharma-reporter.com/Markets-Regulations/US-CMS-releases-new-info-around-biosimilar-pricing-uptake. [Accessed 8 August 2017].
[186] Bio-Pharma Report, "Zarxio one year on: US biosimilars market still riddled with uncertainty," 9 March 2016. [Online]. Available: http://www.biopharma-reporter.com/Markets-Regulations/Zarxio-one-year-on-Questions-remain-around-US-biosimilar-market. [Accessed 19 July 2017].
[187] Rheumatologist, "Pfizer Announces Medicare Reimbursement for Inflectra (infliximab-dyyb), the First Biosimilar Monoclonal Antibody Available in the United States," January 2017. [Online]. Available: http://www.the-rheumatologist.org/article/pfizer-announces-medicare-reimbursement-inflectra-infliximab-dyyb-first-biosimilar-monoclonal-antibody-available-united-states/. [Accessed 21 July 2017].
[188] Centers for Medicare & Medicaid Services, "Part B Biosimilar Biological Product Payment and Required Modifiers," 26 July 2017. [Online]. Available: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Part-B-Drugs/McrPartBDrugAvgSalesPrice/Part-B-Biosimilar-Biological-Product-Payment.html. [Accessed 30 October 2017].
[189] C. f. M. &. M. Services, "Final Policy, Payment, and Quality Provisions in the Medicare Physician Fee Schedule for Calendar Year 2018," 2 11 2017. [Online]. Available: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2017-Fact-Sheet-items/2017-11-02.html. [Accessed 23 2 2018].
[190] CMS, "HCPCS Quarterly Update," 18 May 2017. [Online]. Available: https://www.cms.gov/Medicare/Coding/HCPCSReleaseCodeSets/HCPCS-Quarterly-Update.html. [Accessed 21 July 2017].
[191] US FDA, "Information for Consumers (Biosimilars)," 27 August 2015. [Online]. Available: https://www.fda.gov/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/therapeuticbiologicapplications/biosimilars/ucm241718.htm. [Accessed 9 August 2017].
[192] NCSL, "State Laws And Legislation Related To Biologic Medications And Substitution Of Biosimilars," 1 July 2017. [Online]. Available: http://www.ncsl.org/research/health/state-laws-and-legislation-related-to-biologic-medications-and-substitution-of-biosimilars.aspx. [Accessed 9 August 2017].
[193] S. Jarrett and T. Dingermann, "Biosimilars Are Here: A Hospital Pharmacist’s Guide to Educating Health Care Professionals on Biosimilars," 19 November 2015. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5057195/. [Accessed 12 December 2017].
[194] US FDA, "Purple Book: Lists of Licensed Biological Products with Reference Product Exclusivity and Biosimilarity or Interchangeability Evaluations," July 24 2017. [Online]. Available: https://www.fda.gov/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/therapeuticbiologicapplications/biosimilars/ucm411418.htm. [Accessed 9 August 2017].
[195] US FDA Blog, "FDA Taking New Steps to Better Inform Physicians about Biosimilars Through Education about these Potentially Cost-Saving Options," [Online]. Available: https://blogs.fda.gov/fdavoice/index.php/tag/biosimilars/. [Accessed 24 07 2017].
[196] US FDA, "About FDA Transparency Basics," [Online]. Available: https://www.fda.gov/AboutFDA/Transparency/Basics/ucm355978.htm. [Accessed 9 August 2017].
[197] US FDA, "FDA Basics Webinar August 19, 2013: Biological Products, Part 2: Biosimilar Biological Products," [Online]. Available: https://www.fda.gov/AboutFDA/Transparency/Basics/ucm364686.htm. [Accessed 9 August 2017].

Global biosimilar policy comparison
93
[198] Biosimilar development, "Biosimilars Forum Launches ‘Partnership For Biosimilars Education And Access'," February 2016. [Online]. Available: https://www.biosimilardevelopment.com/doc/biosimilars-partnership-for-biosimilars-education-and-access-0001. [Accessed 18 July 2017].
[199] BioPharm International, "Biosimilars Forum Launches Education Initiative," 1 February 2016. [Online]. Available: http://www.biopharminternational.com/biosimilars-forum-launches-education-initiative. [Accessed 24 July 2017].
[200] Lexology, "Biosimilars coding and reimbursement significance under Medicare Part B," 22 July 2015. [Online]. Available: http://www.lexology.com/library/detail.aspx?g=56a8b209-5661-48f3-91a0-93fe324125cb. [Accessed 8 August 2017].
[201] CVS Health, "2017 Formulary Management Strategy," 2016. [Online]. Available: http://investors.cvshealth.com/~/media/Files/C/CVS-IR-v3/documents/02-aug-2016/2017-standard-formulary-list-of-removals-and-updates.pdf. [Accessed 31 October 2017].
[202] Amgen, "How Do US Payers View Biosimilars From a Cost Perspective?," December 2016. [Online]. Available: http://www.centerforbiosimilars.com/news/how-do-us-payers-view-biosimilars-from-a-cost-perspective. [Accessed 24 July 2017].
[203] JP Morgan, "US Payor Survey, sourced via ThomsonOne," JP Morgan, 2017.
[204] U. D. o. H. &. H. Services, "HHS FY 2017 Budget in Brief - CMS - Medicare," 22 June 2017. [Online]. Available: https://www.hhs.gov/about/budget/fy2017/budget-in-brief/cms/medicare/index.html#. [Accessed 12 December 2017].
[205] PhRMA, "Biosimilars Naming: Why Terminology Matters and Where It Stands," 2015. [Online]. Available: http://phrma-docs.phrma.org/sites/default/files/pdf/biosimilars-101-naming.pdf. [Accessed 9 August 2017].
[206] Biosimilars Forum, "Biosimilars Forum Issues Comments for CMS Proposed Rule on Biosimilar Payment and Coding," 8 September 2015. [Online]. Available: http://www.biosimilarsforum.org/news/biosimilars-forum-issues-comments-cms-proposed-rule-biosimilar-payment-and. [Accessed 31 October 2017].
[207] B. Forum, "Biosimilars Forum Applauds CMS Decision to Reverse Existing Rule on Biosimilar Reimbursement Policy," 2 11 2017. [Online]. Available: http://www.biosimilarsforum.org/news/biosimilars-forum-applauds-cms-decision-reverse-existing-rule-biosimilar. [Accessed 23 2 2018].
[208] Government of Canada, "Canada's Health Care System," [Online]. Available: https://www.canada.ca/en/health-canada/services/health-care-system/reports-publications/health-care-system/canada.html. [Accessed 13 7 2017].
[209] Government of Canada, "Canada Health Act - Frequently Asked Questions," [Online]. Available: https://www.canada.ca/en/health-canada/services/health-care-system/canada-health-care-system-medicare/canada-health-act-frequently-asked-questions.html#a3. [Accessed 13 7 2017].
[210] Government of Canada, "Government of Canada taking action to protect Canadians from high prescription drug prices," 16 May 2017. [Online]. Available: https://www.canada.ca/en/health-canada/news/2017/05/government_of_canadatakingactiontoprotectcanadiansfromhighprescr.html. [Accessed 18 August 2017].
[211] Health Canada, "How Drugs are Reviewed in Canada," 12 February 2015. [Online]. Available: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/fact-sheets/drugs-reviewed-canada.html. [Accessed 30 October 2017].
[212] Patented Medicine Prices Review Board, "Compendium of Policies, Guidelines and Procedures – Updated February 2017," [Online]. Available: http://www.pmprb-cepmb.gc.ca/view.asp?ccid=492#1636. [Accessed 24 7 2017].
[213] CADTH, "CADTH Common Drug Review (CDR)," [Online]. Available: https://www.cadth.ca/about-cadth/what-we-do/products-services/cdr. [Accessed 30 October 2017].
[214] Canada's Premiers, "The pan-Canadian Pharmaceutical Alliance," [Online]. Available: http://www.pmprovincesterritoires.ca/en/initiatives/358-pan-canadian-pharmaceutical-alliance. [Accessed 18 8 2017].
[215] H. B.-N. (. Canada), "Private insurers want in as governments boost bulk-buying power," 6 May 2016. [Online]. Available: http://www.benefitscanada.com/uncategorized/what-plan-sponsors-should-know-about-the-drug-price-gap-80617. [Accessed 31 October 2017].
[216] Patented Medicine Prices Review Board, "Regulatory Process," [Online]. Available: http://www.pmprb-cepmb.gc.ca/en/regulating-prices/regulatory-process. [Accessed 21 7 2017].
[217] Government of Canada, "Drug Product Database online query," 2016. [Online]. Available: https://health-products.canada.ca/dpd-bdpp/newSearch-nouvelleRecherche.do?lang=en. [Accessed 9 August 2017].
[218] G. Warwick, "Potential Savings from Biosimilars in Canada," CADTH, April 2017. [Online]. Available: https://www.cadth.ca/sites/default/files/symp-2017/presentations/april24-2017/Concurrent-Session-B4-Gary-Warwick.pdf. [Accessed 24 July 2017].
[219] Government of Canada, "Canada’s pharmaceutical industry and prospects," 2014. [Online]. Available: https://www.ic.gc.ca/eic/site/lsg-pdsv.nsf/eng/hn01768.html. [Accessed 27 July 2017].
[220] QuintilesIMS, "Canada: Biosimilars by region," [Online]. Available: http://www.quintiles.com/microsites/biosimilars-knowledge-connect/biosimilars-by-region/canada. [Accessed 17 July 2017].
[221] Health Canada, "Guidance Document: Information and Submission Requirements for Biosimilar Biologic Drugs," 14 November 2016. [Online]. Available: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/dhp-mps/alt_formats/pdf/brgtherap/applic-demande/guides/seb-pbu/seb-pbu-2016-eng.pdf. [Accessed 27 July 2017].
[222] Biosimilar Development, "Health Canada's Unique Approach To Biosimilar Regulation," 16 December 2017. [Online]. Available: https://www.biosimilardevelopment.com/doc/health-canada-s-unique-approach-to-biosimilar-regulation-0001. [Accessed 24 July 2017].
[223] Scrip, "Canada Ups Pricing Pressure on Biosimilars And Originators," April 2016. [Online]. Available: https://scrip.pharmamedtechbi.com/SC065021/Canada-Ups-Pricing-Pressure-on-Biosimilars-And-Originators. [Accessed 24 July 2017].
[224] Greenshield Canada, "The Drug Landscape is Changing: Say Hello to Subsequent Entry Biologics," December 2016. [Online]. Available: http://www.greenshield.ca/en-ca/news/stories/the-drug-landscape-is-changing. [Accessed 27 July 2017].
[225] Benefits Canada, "What to do about biosimilars?," January 2017. [Online]. Available: http://www.benefitscanada.com/wp-content/uploads/2017/01/BECA0117_Biosimilars.pdf. [Accessed 27 July 2017].
[226] G. W. (PMPRB), "Potential Savings from Biosimilars in Canada," April 2017. [Online]. Available: https://www.cadth.ca/sites/default/files/symp-2017/presentations/april24-2017/Concurrent-Session-B4-Gary-Warwick.pdf. [Accessed 24 July 2017].

Global biosimilar policy comparison
94
[227] Health Canada, "Fact Sheet: Biosimilars," 3 August 2017. [Online]. Available: https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/applications-submissions/guidance-documents/fact-sheet-biosimilars.html. [Accessed 31 October 2017].
[228] F. Bruce, "Canada Attempts Biosimilar Balancing Act," February 2017. [Online]. Available: http://morseconsulting.ca/wp-content/uploads/2017/03/Biosimilar-Balancing-Act-Article-February-17%5EJ-2017.pdf. [Accessed 24 July 2017].
[229] Biosimilars Canada, "Canadian Generic Pharmaceutical Association (CGPA) Establishes First Voice for Biosimilars In Canada," 7 April 2015. [Online]. Available: http://biosimilarscanada.ca/news/April172015.html. [Accessed 27 July 2017].
[230] Mondaq, "Canada: Health Canada Releases Revised Guidance Document On Approval Pathway For Biosimilars," 12 January 2017. [Online]. Available: http://www.mondaq.com/canada/x/559468/Life+Sciences+Biotechnology/Health+Canada+Releases+Revised+Guidance+Document+On+Approval+Pathway+For+Biosimilars+Formerly+SubsequentEntry+Biologics. [Accessed 21 July 2017].
[231] Scrip, "Canada To Have Patent Term Extensions Soon – And An Export Waiver," Scrip, 28 March 2017. [Online]. Available: https://pink.pharmamedtechbi.com/PS120323/Canada-To-Have-Patent-Term-Extensions-Soon--And-An-Export-Waiver. [Accessed 24 July 2017].
[232] Government of Canada, "Health Canada’s 2017 Biosimilars Workshop: Summary Report," March 2017. [Online]. Available: https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/applications-submissions/guidance-documents/biosimilars-workshop.html?=undefined&wbdisable=true. [Accessed 27 July 2017].
[233] S. Morgan and K. Boothe, "Universal prescription drug coverage in Canada," October 2016. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5094297/. [Accessed 27 July 2017].
[234] Cision, "Canadian Patients Speak Out on Biosimilars," October 2016. [Online]. Available: http://www.newswire.ca/news-releases/canadian-patients-speak-out-on-biosimilars-595611611.html. [Accessed 21 July 2017].
[235] Express Scripts, "Express Scripts Canada Drug Trend Report 2016," 2017. [Online]. Available: http://www.express-scripts.ca/sites/default/files/2016-Drug-Trend-Report.pdf. [Accessed 10 August 2017].
[236] Morneau Shepell, "Quebec: Bill 92 a game-changer for prescription drugs," December 2016. [Online]. Available: http://www.morneaushepell.com/permafiles/80768/news-and-views-december-2016.pdf. [Accessed 8 August 2017].
[237] Canada's Public Policy Forum, "Subsequent entry biologics in Canada: The case for multi-sector collaboration," 2014. [Online]. Available: https://www.ppforum.ca/sites/default/files/SEB%20report%20-%20FINAL.pdf. [Accessed 28 July 2017].
[238] BIOTECanada, "Demystifying Biosimilars," 2012. [Online]. Available: http://www.biotech.ca/wp-content/uploads/2016/03/Demystifying-Biosimilars-Guide-English-.pdf. [Accessed 30 October 2017].
[239] CGPA, "CGPA Statement on the Provisional Application of CETA and New Pharmaceutical Intellectual Property Measures for Canada," 21 September 2017. [Online]. Available: http://canadiangenerics.ca/news-release6/cgpa-statement-on-the-provisional-application-of-ceta-and-new-pharmaceutical-intellectual-property-measures-for-canada/. [Accessed 31 October 2017].
[240] Biosimilars Canada, "Biosimilars Canada Statement on Revised Canadian Guidance for Sponsors of Biosimilars," 9 January 2017. [Online]. Available: http://www.biosimilarscanada.ca/news/jan92017.html. [Accessed 30 October 2017].
[241] Canadian Generic Pharmaceutical Association , "New Report on Drug Spending in Canada Highlights Importance of Generics and Biosimilars for Future Affordability of Drug Benefit Plans," 29 May 2015. [Online]. Available: http://canadiangenerics.ca/news-release2/june_01_15/. [Accessed 28 July 2017].
[242] European Observatory on Health Systems and Policies, "Australia - Health System review," 2006. [Online]. Available: http://www.euro.who.int/__data/assets/pdf_file/0007/96433/E89731.pdf.
[243] Australian Taxiation Office, "Medicare Levy," [Online]. Available: https://www.ato.gov.au/Individuals/Medicare-levy/. [Accessed 12 7 2017].
[244] Australian Government - Department of Human Services, "Medicare services," 27 August 2017. [Online]. Available: https://www.humanservices.gov.au/individuals/subjects/medicare-services#a1. [Accessed 20 September 2017].
[245] A. I. o. H. a. Welfare, "Australia's health system," [Online]. Available: http://www.aihw.gov.au/australias-health/2014/health-system/#content. [Accessed 12 7 2017].
[246] Australian Government - Department of Health, "Procedure guidance for listing medicines on the Pharmaceutical Benefits Scheme," September 2017. [Online]. Available: http://www.pbs.gov.au/industry/listing/procedure-guidance/files/procedure-guidance-listing-medicines-on-the-pbs.pdf. [Accessed 11 December 2017].
[247] Australian Government, "Strategic Agreement," 27 April 2017. [Online]. Available: https://medicinesaustralia.com.au/wp-content/uploads/sites/52/2017/05/09-May-2017-Strategic-Agreement-with-Commonwealth-Signed.pdf. [Accessed 16 August 2017].
[248] Australian Government - Department of Health - The Pharmaceutical Benefits Scheme, "FAQ – EAPD for Pharmacies and Wholesalers," [Online]. Available: http://www.pbs.gov.au/info/industry/pricing/eapd/faq-for-pharmacies-and-wholesalers. [Accessed 20 September 2017].
[249] H. Löfgren, "Generic Medicines in Australia: Business dynamics and recent policy reform," 2009. [Online]. Available: http://apps.who.int/medicinedocs/documents/s16383e/s16383e.pdf. [Accessed 7 August 2017].
[250] Australian Government - Private Health Insurance Ombudsman, "What is covered?," [Online]. Available: http://www.privatehealth.gov.au/healthinsurance/whatiscovered/. [Accessed 20 September 2017].
[251] Australian Government - Department of Human Services, "Highly specialised drugs," 27 August 2017. [Online]. Available: https://www.humanservices.gov.au/organisations/health-professionals/services/medicare/highly-specialised-drugs. [Accessed 31 October 2017].
[252] Australian Government - Department of Health Services, "Written Authority Required Drugs," 1 October 2017. [Online]. Available: https://www.humanservices.gov.au/organisations/health-professionals/services/medicare/written-authority-required-drugs. [Accessed 31 October 2017].
[253] Parliament of Australia, "Budget Review 201718 PBS," May 2017. [Online]. Available: http://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/rp/BudgetReview201718/PBS. [Accessed 26 July 2017].

Global biosimilar policy comparison
95
[254] Commonwealth of Australia, "Strategic Agreement," 2017. [Online]. Available: https://www.health.gov.au/internet/main/publishing.nsf/Content/CC4088EE246D44BFCA25811B002759EE/$File/Medicines%20Australia%20-%20Strategic%20Agreement.pdf. [Accessed 20 September 2017].
[255] Australian Government, Department of Human Services, "Pharmaceutical Benefits Scheme (PBS) Safety Net," 7 July 2017. [Online]. Available: https://www.humanservices.gov.au/customer/services/medicare/pharmaceutical-benefits-scheme-pbs-safety-net. [Accessed 3 August 2017].
[256] Department of Health - Australia, "What are biosimilar medicines," July 2017. [Online]. Available: http://www.health.gov.au/internet/main/publishing.nsf/Content/biosimilar-what-are-biosimilar-medicines. [Accessed 26 July 2017].
[257] GaBI, "Australian approval for infliximab biosimilar," 21 August 2015. [Online]. Available: http://www.gabionline.net/Biosimilars/General/Australian-approval-for-infliximab-biosimilar. [Accessed 31 July 2017].
[258] GaBI, "Australian approval for infliximab biosimilar," August 2015. [Online]. Available: http://www.gabionline.net/Biosimilars/General/Australian-approval-for-infliximab-biosimilar. [Accessed 27 July 2017].
[259] Therapeutic Goods Administration, "Evaluation biosimilars," December 2015. [Online]. Available: https://www.tga.gov.au/publication/evaluation-biosimilars. [Accessed 26 July 2017].
[260] The Deparment of Health - Australia, "Biosimilar awareness initiative," April 2017. [Online]. Available: http://www.health.gov.au/internet/main/publishing.nsf/Content/biosimilar-awareness-initiative. [Accessed 26 July 2017].
[261] The Department of Health - Australia, "Biosimilar how are biosimilar medicines assessed and monitored," 23 March 2017. [Online]. Available: http://www.health.gov.au/internet/main/publishing.nsf/Content/biosimilar-how-are-biosimilar-medicines-assessed-and-monitored. [Accessed 2 August 2017].
[262] TGA, "Evaluation-biosimilars," 17 December 2015. [Online]. Available: https://www.tga.gov.au/publication/evaluation-biosimilars. [Accessed 31 July 2017].
[263] Australian Government - Department of Health - Therapeutic Goods Adminstration, "Consultation: Nomenclature of Biological Medicines," 28 July 2017. [Online]. Available: https://www.tga.gov.au/consultation/consultation-nomenclature-biological-medicines. [Accessed 13 October 2017].
[264] TGA, "Evaluation biosimilars," December 2015. [Online]. Available: https://www.tga.gov.au/publication/evaluation-biosimilars. [Accessed 27 July 2017].
[265] Council of Australian Therapeutic Advisory Groups, "Overseeing biosimilar use Version 2," September 2016. [Online]. Available: http://www.catag.org.au/wp-content/uploads/2012/08/OKA10798-CATAG-Overseeing-biosimilar-use-Version-2-final.pdf. [Accessed 26 July 2017].
[266] D. A. Power, "Licensing and prescribing biosimilars in Australia," 2013. [Online]. Available: http://gabi-journal.net/licensing-and-prescribing-biosimilars-in-australia.html. [Accessed 7 August 2017].
[267] B. Shaw, "Biosimilars naming and prescribing policy in Australia," 25 November 2013. [Online]. Available: http://gabi-journal.net/biosimilars-naming-and-prescribing-policy-in-australia.html. [Accessed 7 August 2017].
[268] The Pharmaceutical Benefits Scheme - Australia, "Fact sheet pricing a new brand," [Online]. Available: http://www.pbs.gov.au/info/industry/pricing/pbs-items/fact-sheet-pricing-a-new-brand. [Accessed 27 July 2017].
[269] AJP, "Innovative medicines prices drop," May 2017. [Online]. Available: https://ajp.com.au/news/innovative-medicines-prices-drop/. [Accessed 2017 July 2017].
[270] Pharmaceutical Society of Australia, "Biosimilar medicines position statement," September 2015. [Online]. Available: http://www.psa.org.au/downloads/ent/uploads/filebase/policies/biosimilar-medicines-position-statement.pdf. [Accessed 27 July 2017].
[271] GaBi, "Licensing and prescribing biosimilars in Australia," 21 June 2013. [Online]. Available: http://gabi-journal.net/licensing-and-prescribing-biosimilars-in-australia.html. [Accessed 2 August 2017].
[272] The department of health - Australia, "Who chooses whether biosimilar medicine or reference biological medicine is used," March 2017. [Online]. Available: http://www.health.gov.au/internet/main/publishing.nsf/Content/biosimilar-hp-who-chooses-whether-biosimilar-medicine-or-reference-biological-medicine-is-used. [Accessed 27 July 2017].
[273] GaBI Online, "Australia’s PBAC recommends substitution of biosimilars," 19 June 2015. [Online]. Available: http://gabionline.net/Biosimilars/General/Australia-s-PBAC-recommends-substitution-of-biosimilars. [Accessed 7 August 2017].
[274] The Pharmaceutical Benefits Scheme, "Listed on PBS," June 2017. [Online]. Available: http://www.pbs.gov.au/info/browse/biological-medicines-currently-listed-on-the-pbs. [Accessed 26 July 2017].
[275] Medicines Australia Limited, "Strategic Agreement," 2017. [Online]. Available: https://www.health.gov.au/internet/main/publishing.nsf/Content/CC4088EE246D44BFCA25811B002759EE/$File/Medicines%20Australia%20-%20Strategic%20Agreement.pdf. [Accessed 9 September 2017].
[276] The Department of Health - Australia, "Biosimilar project management plan," June 2016. [Online]. Available: http://www.health.gov.au/internet/main/publishing.nsf/content/0CE13CDB4B59ACB0CA2580810077E68F/$File/biosimilar-project-management-plan.pdf. [Accessed 26 July 2017].
[277] AusBiotech, "Biologic And Biosimilar Medicines 2020: Making The Most Of The Opportunities," 2016. [Online]. Available: https://www.ausbiotech.org/documents/item/48. [Accessed 31 July 2017].
[278] Australian Government - Department of Health, "Biosimilar Uptake Driver," 1 December 2017. [Online]. Available: http://www.pbs.gov.au/general/biosimilars/biosimilar-uptake-drivers-q-and-a.pdf . [Accessed 11 December 2017].
[279] L. S. R. S. K. Ward Michael, "Biosimilars literature review," 26 September 2016. [Online]. Available: https://www.health.gov.au/internet/main/publishing.nsf/Content/48CEE4710816DAC8CA2580810077372D/$File/biosimilars-literature-review-09-2016.pdf. [Accessed 31 July 2017].
[280] GBMA, "Making Medicines Affordable A Pre-Budget Submission," January 2017. [Online]. Available: https://www.treasury.gov.au/~/media/Treasury/Consultations%20and%20Reviews/Consultations/2016/2017%20PreBudget%20submissions/Submissions/PDF/Generic%20and%20Biosimilar%20Medicines%20Association.ashx. [Accessed 10 August 2017].
[281] AusBiotech, "Biologic and Biosimilar Medicines 2020: Making The Most Of The Opportunities," 2016. [Online]. Available: https://www.ausbiotech.org/documents/item/48. [Accessed 10 August 2017].
[282] Medicines Australia, "MEDICINES AUSTRALIA SUBMISSION," 2015. [Online]. Available: https://medicinesaustralia.com.au/wp-content/uploads/sites/52/2010/02/20150618-sub-NHA-Inquiry-Medicines-Australia-submission-FINAL_.pdf. [Accessed 18 September 2017].

Global biosimilar policy comparison
96
[283] K. S.-Y. L. J.-Y. L. S.-Y. (. Chun C-B, "Health Systems in Transition: Republic of Korea," 2009. [Online]. Available: http://www.euro.who.int/__data/assets/pdf_file/0019/101476/E93762.pdf.
[284] National Health Insurance Service, "2014 National Health Insurance System of Korea: Universal Health Coverage for the World," May 2014. [Online]. Available: http://www.coopami.org/en/countries/countries/south_korea/social_protection/pdf/social_protection05.pdf. [Accessed 14 August 2017].
[285] S. Y-J, "The South Korean Health Care System," 2009. [Online]. Available: https://www.med.or.jp/english/journal/pdf/2009_03/206_209.pdf.
[286] OECD, "Fertility Rates," [Online]. Available: https://data.oecd.org/pop/fertility-rates.htm. [Accessed 12 7 2017].
[287] WHO, "Global Status Report on Alcohol and Health 2014," 2014. [Online]. Available: http://apps.who.int/iris/bitstream/10665/112736/1/9789240692763_eng.pdf?ua=1.
[288] KCDC, "Korea National Health and Nutrition Examination Survey," 2015. [Online]. Available: https://knhanes.cdc.go.kr/knhanes/intro.html. [Accessed 17 October 2017].
[289] ISPOR, "The Health Technology Assessment Environment in Mainland China, Japan, South Korea, and Taiwan—Implications for the Evaluation of Diabetes Mellitus Therapies," 2014. [Online]. Available: https://www.ispor.org/vihri/HTA-Asia-diabetes.pdf. [Accessed 4 August 2017].
[290] Scrip, "Korean Pro-Innovation Pricing Steps Draw Mixed Responses," 12 July 2016. [Online]. Available: https://pink.pharmamedtechbi.com/PS118732/Korean-ProInnovation-Pricing-Steps-Draw-Mixed-Responses. [Accessed 4 August 2017].
[291] The Korea Bizwire, "Korea’s Biosimilar Market on the Rise," The Korea Bizwiz, May 2016. [Online]. Available: http://koreabizwire.com/koreas-biosimilar-market-on-the-rise/55297. [Accessed 13 July 2017].
[292] Y. B-M, "Drug Pricing and Reimbursement in South Korea," 2012. [Online]. Available: http://www.pp.u-tokyo.ac.jp/HTA/events/2012-09-06/documents/hta20120906-yang.pdf.
[293] GaBI, "Impact of South Korea’s new drug–pricing policy on market competition," 2016. [Online]. Available: http://www.gabionline.net/Generics/Research/Impact-of-South-Korea-s-new-drug-pricing-policy-on-market-competition. [Accessed 4 August 2017].
[294] National Health Insurance Service, "한국의 의약품 가격결정 및 상환 정책," June 2017. [Online]. Available: http://www.nhis.or.kr/bbs7/boards/B0039/24123. [Accessed 14 August 2017].
[295] S. G. L. S. P. T. H. K. J. A. M.-H. C. E.-C. P. Ki-Bong Yoo, "Effects of drug price reduction and prescribing restrictions on expenditures and utilisation of antihypertensive drugs in Korea," 15 July 2015. [Online]. Available: http://bmjopen.bmj.com/content/5/7/e006940. [Accessed 16 August 2017].
[296] GaBI, "Biosimilars approved in South Korea," December 2016. [Online]. Available: http://gabionline.net/Biosimilars/General/Biosimilars-approved-in-South-Korea. [Accessed 13 July 2017].
[297] Biosimilar News, "Basaglar challenges Sanofi’s insulin drug Lantus in S.Korea," 17 April 2017. [Online]. Available: http://www.biosimilarnews.com/basaglar-challenges-sanofis-insulin-drug-lantus-in-s-korea . [Accessed 11 August 2017].
[298] Ministry of Food and Drug Safety, "지난해 국내 의약품 시장규모 첫 20조원 대 돌파," 6 July 2017. [Online]. Available: http://www.mfds.go.kr/index.do?mid=675&seq=37889&sitecode=1&cmd=v. [Accessed 15 August 2017].
[299] First Word Pharma, "Korea’s Biosimilar Market on the Rise," May 2016. [Online]. Available: https://www.firstwordpharma.com/node/1386008?tsid=33. [Accessed 13 July 2017].
[300] GaBI, "Regulations for biosimilars in South Korea," 2015, [Online]. Available: http://www.gabionline.net/Guidelines/Regulations-for-biosimilars-in-South-Korea. [Accessed 13 July 2017].
[301] HIndawi, "Biosimilars in Developed and Developing East and Southeast Asian Countries: Japan, South Korea, and Malaysia—Overview, Evolution, and Regulations Assessment," 2016. [Online]. Available: https://www.hindawi.com/journals/bmri/2016/5910403/. [Accessed 14 July 2017].
[302] S. Suh Kyung and Y. Park, "Regulatory guideline for biosimilar products in Korea," 2011. [Online]. Available: http://ac.els-cdn.com/S104510561100073X/1-s2.0-S104510561100073X-main.pdf?_tid=7660c8e6-7917-11e7-8a12-00000aab0f01&acdnat=1501852914_c2be7aac193f59bc931426eebe167b5f. [Accessed 4 August 2017].
[303] GaBI, "Korean regulations for biosimilars," 2015. [Online]. Available: http://gabi-journal.net/korean-regulations-for-biosimilars.html . [Accessed 4 August 2017].
[304] T. W. (Informa), "Hot Topic: Biosimilars in Emerging Markets," 20 April 2017. [Online]. Available: https://pharmastore.informa.com/product/biosimilars-in-emerging-markets/.
[305] IAM , "Recent developments in pharmaceutical patent law," 2016. [Online]. Available: http://www.iam-media.com/intelligence/IAM-Yearbook/2016/Country-by-country/Recent-developments-in-pharmaceutical-patent-law. [Accessed 4 August 2017].
[306] Lexology, "Expected Implementation of Reform Plan for Biopharmaceutical Price System," 14 July 2016. [Online]. Available: http://www.lexology.com/library/detail.aspx?g=51a596b1-ae38-4f79-b5cb-8b1dd307f2e4. [Accessed 19 July 2017].
[307] BMI Rearch , "Industry Trend Analysis - Higher Reimbursements To Benefit Celltrion And Samsung Bioepis - OCT 2016," 2016. [Online]. Available: http://www.pharmaceuticalsinsight.com/industry-trend-analysis-higher-reimbursements-benefit-celltrion-and-samsung-bioepis-oct-2016. [Accessed 19 July 2017].
[308] Health Insurance Review and Assessment Service, "건강보험심사평가원 급여기준별분류 (청구관련기준자료)," 26 July 2017. [Online]. Available: http://www.hira.or.kr/co/searchCms.do?catid=5h_43050&collection=cms&startCount=&pgmid=HIRAA030069000100&selPayStnd=%EC%B2%AD%EA%B5%AC%EA%B4%80%EB%A0%A8%EA%B8%B0%EC%A4%80%EC%9E%90%EB%A3%8C&startDate=&endDate=&search_word=%EC%95%BD%EA%B0%80. [Accessed 16 August 2017].
[309] D.-i. Lee, "Samsung Bioepis to launch second biosimilar by June," 1 April 2016. [Online]. Available: http://pulsenews.co.kr/view.php?sc=30800021&year=2016&no=241965. [Accessed 16 August 2017].
[310] ISPOR, "The Ispor Scientific Presentations Database," November 2015. [Online]. Available: https://www.ispor.org/ScientificPresentationsDatabase/Presentation/60530. [Accessed 4 August 2017].
[311] The Korean Herald, "Korean Drug Ministry releases more biosimilar approval results in English," December 2016. [Online]. Available: http://www.koreaherald.com/view.php?ud=20161214000711. [Accessed 13 July 2017].

Global biosimilar policy comparison
97
[312] Deallus Consulting, "South Korea: An Eye Towards the Biobetter," [Online]. Available: http://www.deallusconsulting.com/south-korea-eye-towards-biobetter/. [Accessed 27 July 2017].
[313] Big Molecule Watch, "South Korea’S Biosimilars Industry Poised To Grow Domestically And Abroad," Big Molecule Watch, 16 June 2016. [Online]. Available: http://www.bigmoleculewatch.com/2016/06/16/south-koreas-biosimilars-industry-poised-to-grow/. [Accessed 27 July 2017].
[314] "Biosimilars to become new trend in bio industry," NH Investments & Securities, 2015.
[315] Big Molecule Watch, "South Korea’s biosimilars industry poised to grow domestically and abroad," 2016 June 2016. [Online]. Available: http://www.bigmoleculewatch.com/2016/06/16/south-koreas-biosimilars-industry-poised-to-grow/. [Accessed 4 August 2017].
[316] PM Live, "An eye towards the biobetter in South Korea," 12 March 2013. [Online]. Available: http://www.pmlive.com/pharma_intelligence/an_eye_towards_the_biobetter_in_south_korea_466459. [Accessed 14 July 2017].
[317] Big Molecule Watch, "South Korea’S Biosimilars Industry Poised To Grow Domestically And Abroad," 16 June 2016. [Online]. Available: http://www.bigmoleculewatch.com/2016/06/16/south-koreas-biosimilars-industry-poised-to-grow/. [Accessed 14 July 2017].
[318] BNP Paribas, "Biosimilars – The next Korean Wave, Sourced via ThomsonOne," BNP Paribas, 2016.
[319] Pharmaceutical Insight, "Industry Trend Analysis - Biosimilars To Drive Domestic Industry Growth - FEB 2015," January 2015. [Online]. Available: http://www.pharmaceuticalsinsight.com/industry-trend-analysis-biosimilars-drive-domestic-industry-growth-feb-2015. [Accessed 25 July 2017].
[320] Pacific Bridge Medical, "Korea Drug Market Update 2017," 11 July 2017. [Online]. Available: http://www.pacificbridgemedical.com/publication/korea-drug-market-update-2017/. [Accessed 4 August 2017].
[321] Korea Pharmaceutical and Bio-Pharma Manufacturers Association, "한국 제약산업의 글로벌 도전과 과제," 29 April 2014. [Online]. Available: http://www.kpbma.or.kr/sub/select/00000000034/00000000038/160061. [Accessed 15 August 2017].
[322] P. S.-s. (. Times), "Foreign drug firms call for easing rules on pricing, reimbursement," 17 February 2015. [Online]. Available: http://www.koreatimes.co.kr/www/news/biz/2015/02/123_173777.html. [Accessed 31 October 2017].
[323] European Medicines Agency, "Biosimilars in the EU Information guide for healthcare professionals," 2017. [Online]. Available: http://www.ema.europa.eu/docs/en_GB/document_library/Leaflet/2017/05/WC500226648.pdf. [Accessed 8 August 2017].
[324] WHO, "ATC: Structure and principles," [Online]. Available: https://www.whocc.no/atc/structure_and_principles/. [Accessed 14 August 2017].
[325] NICE, "NICE Guidance: Conditions and diseases: Musculoskeletal conditions: Arthritis," February 2009. [Online]. Available: https://www.nice.org.uk/donotdo/use-of-the-tumor-necrosis-factor-a-tnf-inhibitors-for-the-treatment-of-severe-active-and-progressive-rheumatoid-arthritis-in-adults-not-previously-treated-with-methotrexate-or-other-diseasemodifying. [Accessed 14 August 2017].
[326] US government, "Glossary: co-payment," [Online]. Available: https://www.healthcare.gov/glossary/co-payment/. [Accessed 14 August 2017].
[327] WHO, "Safety and Vigilance - Medicines," [Online]. Available: http://www.who.int/medicines/regulation/medicines-safety/toolkit_ddd/en/. [Accessed 14 August 2017].
[328] CMS, "Design and development of the Diagnosis," [Online]. Available: https://www.cms.gov/ICD10Manual/version34-fullcode-cms/fullcode_cms/Design_and_development_of_the_Diagnosis_Related_Group_(DRGs)_PBL-038.pdf. [Accessed 14 August 2017].
[329] WHO, "Health statistics and information systems: Global Health Estimates," [Online]. Available: http://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/. [Accessed 14 August 2017].
[330] NICE, "Erythropoiesis-stimulating agents (epoetin and darbepoetin) for treating anaemia in people with cancer having chemotherapy," 26 November 2014. [Online]. Available: https://www.nice.org.uk/guidance/ta323. [Accessed 14 August 2017].
[331] EMA, "About us," [Online]. Available: http://www.ema.europa.eu/ema/index.jsp?curl=pages/about_us/document_listing/document_listing_000426.jsp&mid=. [Accessed 14 August 2017].
[332] Health Lawyers, "Gainsharing," [Online]. Available: https://www.healthlawyers.org/hlresources/Health%20Law%20Wiki/Gainsharing.aspx. [Accessed 14 August 2017].
[333] IMSANZ, "WHAT IS A GENERAL PHYSICIAN?," [Online]. Available: https://www.imsanz.org.au/about-us/what-is-a-general-physician. [Accessed 14 August 2017].
[334] WHO, "Medicines and health products: Areas of work Norms and Standards: Quality, safety and efficacy of medicines: Medicines quality assurance," [Online]. Available: http://www.who.int/medicines/areas/quality_safety/quality_assurance/gmp/en/. [Accessed 14 August 2017].
[335] NHS, "Guidelines for the Use of Granulocyte Colony Stimulating Factors (G-CSF) in Adult Haematology/Oncology Patients ACN CO5/1," February 2013. [Online]. Available: http://www.arden.nhs.uk/mf.ashx?ID=8817fd0e-e263-431a-90d1-b2fdb8732260. [Accessed 14 August 2017].
[336] WHO, "Medical devices: Health technology assessment," [Online]. Available: http://www.who.int/medical_devices/assessment/en/. [Accessed 14 August 2017].
[337] NHS, "Restricted growth (dwarfism) - Treatment," 5 March 2015. [Online]. Available: http://www.nhs.uk/Conditions/Restricted-growth/Pages/Treatment.aspx. [Accessed 14 August 2017].
[338] CMS, "Are You a Hospital Inpatient or Outpatient? - If You Have Medicare – Ask!," May 2014. [Online]. Available: https://www.medicare.gov/Pubs/pdf/11435.pdf. [Accessed 14 August 2017].
[339] WHO, "Guidance on INN," [Online]. Available: http://www.who.int/medicines/services/inn/innquidance/en/. [Accessed 14 August 2017].
[340] C. Wight, "The true meaning of market access?," 26 September 2012. [Online]. Available: http://www.pmlive.com/pharma_intelligence/the_true_meaning_of_market_access_422511. [Accessed 14 August 2017].
[341] WHO, "Marketing Authorization of Pharmaceutical Products with Special Reference to Multisource (Generic) Products: A Manual for Drug Regulatory Authorities - Regulatory Support Series No. 005," 1988. [Online]. Available: http://apps.who.int/medicinedocs/en/d/Js2273e/10.html. [Accessed 14 August 2017].
[342] US FDA, "Labeling for Human Prescription Drug and Biological Products — Determining Established Pharmacologic Class for Use in the Highlights of Prescribing Information," October 2009. [Online]. Available: https://www.fda.gov/downloads/Drugs/Guidances/ucm186607.pdf. [Accessed 14 August 2017].

Global biosimilar policy comparison
98
[343] EMA, "Authorisation of medicines," [Online]. Available: http://www.ema.europa.eu/ema/index.jsp?curl=pages/about_us/general/general_content_000109.jsp. [Accessed 14 August 2017].
[344] US FDA, "What are over-the-counter (OTC) drugs and how are they approved?," [Online]. Available: https://www.fda.gov/aboutfda/transparency/basics/ucm194951.htm. [Accessed 14 August 2017].
[345] National Institute for Health and Care Excellence (NICE), "Glossary - Q," [Online]. Available: https://www.nice.org.uk/glossary?letter=q. [Accessed 18 July 2017].
[346] WHO, "Drugs and Money - Prices, Affordability and Cost Containment," 2003. [Online]. Available: http://apps.who.int/medicinedocs/en/d/Js4912e/3.3.html. [Accessed 14 August 2017].
[347] European Medicines Agency, "Biosimilars in the EU: Information guide for healthcare professionals," 2017. [Online]. Available: http://www.ema.europa.eu/docs/en_GB/document_library/Leaflet/2017/05/WC500226648.pdf. [Accessed 6 July 2017].
[348] Dignity Health, "Primary Care vs. Specialty Care Physicians," 5 April 2015. [Online]. Available: http://dhmgblog.dignityhealth.org/primary-vs-specialty-care. [Accessed 14 August 2017].
[349] WHO, "Health financing for universal coverage," [Online]. Available: http://www.who.int/health_financing/universal_coverage_definition/en/. [Accessed 14 August 2017].
[350] The Pharmaceutical Benefits Scheme, "Section 1 5 Explanatory Notes," January 2017. [Online]. Available: http://www.pbs.gov.au/info/healthpro/explanatory-notes/section1/Section_1_5_Explanatory_Notes. [Accessed 27 July 2017].
[351] NICE, "Prices in the BNF," July 2017. [Online]. Available: https://www.evidence.nhs.uk/formulary/bnf/current/general-information-and-changes/how-to-use-the-bnf/prices-in-the-bnf. [Accessed 4 August 2017].

EY | Assurance | Tax | Transactions | Advisory
About EYEY is a global leader in assurance, tax, transaction and advisory services. The insights and quality services we deliver help build trust and confidence in the capital markets and in economies the world over. We develop outstanding leaders who team to deliver on our promises to all of our stakeholders. In so doing, we play a critical role in building a better working world for our people, for our clients and for our communities.EY refers to the global organization, and may refer to one or more, of the member firms of Ernst & Young Global Limited, each of which is a separate legal entity. Ernst & Young Global Limited, a UK company limited by guarantee, does not provide services to clients. For more information about our organization, please visit ey.com.
About EY JapanEY Japan refers to the member firms of EY in Japan. EY Japan includes Ernst & Young ShinNihon LLC, Ernst & Young Tax Co., Ernst & Young Transaction Advisory Services Co., Ltd. and EY Advisory & Consulting Co., Ltd. Each of these firms is a separate legal entity. For more information, please visit ey.com/jp/en/.
About EY Advisory & Consulting Co., Ltd.EY Advisory & Consulting is a member firm of EY Japan. Collaborating with EY professionals of diverse expertise from around the world, we provide comprehensive advisory services optimized to meet our clients’ business challenges using an innovative, global perspective and a commitment and capability to deliver, go to www.eyjapan.jp/advisory/.
© EY Advisory & Consulting Co., Ltd. All Rights Reserved.
ED None
This material has been prepared for general informational purposes only and is not intended to be relied upon as accounting, tax, or other professional advice. Please refer to your advisors for specific advice.











![[Product Monograph Template - Standard]€¦ · Web view is a biosimilar biologic drug (biosimilar) to](https://img.dokumen.tips/doc/110x75/5ed9c1d0fa48703dd5136997/product-monograph-template-standard-web-view-is-a-biosimilar-biologic-drug-biosimilar.jpg)