Embed Size (px)
Citation preview
Page 1/13
Associations Between Personality Traits and Adherenceto Treatment in Patients with Primary Open AngleGlaucoma in an African PopulationEbenezer Oduro Antiri
University of Cape CoastStephen Ocansey
University of Cape CoastMichael Ntodie
University of Cape CoastSamuel Abokyi
University of Cape CoastCarl Halladay Abraham
University of Cape CoastEmmanuel Kwasi Abu ( [email protected] )
University of Cape Coast, School of Allied Health Sciences https://orcid.org/0000-0003-2354-9170
Research Article
Keywords: Personality traits, Big Five Inventory, Glaucoma patients, Medication adherence, Africa.
Posted Date: June 7th, 2021
DOI: https://doi.org/10.21203/rs.3.rs-588275/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read FullLicense

Page 2/13
AbstractPurpose: There is poor adherence to medication among patients with glaucoma especially in people of Africanancestry. The present study assessed the in�uence of personality traits on adherence to glaucoma medicationamong patients living with primary open angle glaucoma (POAG) from an African population.
Methods: A clinic-based cross sectional study was conducted among patients with POAG attending a specialisteye care facility. Adapted and validated personality trait and medication adherence measures questionnaires wereused.
Results: Self-reported adherence to glaucoma medication was 60.8% but the overall mean adherence score was18.58±3.40, indicating slight non-adherence. The personality traits conscientiousness and agreeablenesssigni�cantly predicted medication adherence but accounted for only 30.3% and 13.3% of the variance respectively.Non-adherence to medication was signi�cantly predicted by the personality pro�les neuroticism, extraversion andopenness which respectively accounted for 61.7%, 20.3% and 13.3% of the variance in the personality traitassessment. Old age and longer use of glaucoma medications were also signi�cantly associated with non-adherence to glaucoma medication.
Conclusions: Glaucoma patients’ personality pro�les signi�cantly predicted their adherence to glaucomamedications. Assessment of the personality pro�les and appropriate psychotherapeutic approaches should beincluded in glaucoma diagnosis and management protocols in order to enhance medication adherence in patientsliving with glaucoma.
IntroductionGlaucoma is the leading cause of irreversible blindness worldwide and the commonest form of the disease is theprimary open-angle glaucoma (POAG) which is a chronic optic neuropathy often requiring lifelong treatment [1].The burden of POAG, relating to higher prevalence, earlier age of onset, and more blinding, disproportionatelyaffects people of African descent [2]. Ghana is known to have the highest prevalence of glaucoma in Africa andsecond globally, with St. Lucia reporting the highest prevalence [3, 4]. Lowering of intraocular pressure is the mainobjective of POAG management and this is often achieved through pharmacotherapy as the �rst line of choice,especially for newly diagnosed cases and in populations with low glaucoma surgery rates [5–7]. POAG as a non-life threatening, asymptomatic and gradual progressive disease offers little incentive for strict adherence to alifetime therapeutic regimen [1, 8]. Non-compliance with glaucoma treatment has been associated with increasedintraocular pressure, impaired visual acuity and worse visual �eld loss [8, 9]. There is considerable non-adherenceto glaucoma medication in Ghana and has been described as having a major impact on clinical outcomes [10].
Patients on one or more intraocular pressure lowering medications have been found to exhibit unique sets ofbarriers to optimal adherence including reduced self-e�cacy, di�culty instilling drops, forgetfulness, di�cultieswith medication schedule, suspicion that glaucoma will cause vision loss, mistrust that glaucoma medications areeffective, mistrust in the physician, and perceived life stress [11–13]. These barriers are perceived as physicalexpressions of personality traits which may underline poor health seeking behaviors like medication non-adherence. Previous studies on this subject were founded on the reasoning that psychic trauma and emotionalupsets could be a determinant in glaucoma aetiology and that comprehension of the psychology of the glaucomapatient could provide a foundation for a complete and successful treatment [14, 15]. Pappa et al found self-

Page 3/13
reported non-compliance with glaucoma treatment to be associated with depression and suggested thatassessment and treatment of depressive feelings could improve compliance in glaucoma patients [8]. In effect,practitioners could be managing the chronic condition well but the person’s personality can be a formidable barrierto achieving a better prognosis leading to needless medication changes or surgical interventions.
POAG is a chronic condition which requires continues public health interventions. However, associations betweenpersonality traits and glaucoma medication adherence have not been extensively explored, especially in sub-Saharan Africa. Many studies have reported different personality pro�les among glaucoma patients whencompared to non-glaucoma controls [16–19]. It appears that certain personality pro�les have predispositions toglaucoma etiology or that these personality traits rather develop as a consequence to the onset of glaucoma.Since research has revealed differences in personality traits within and between countries [20, 21], this studysought to investigate how personality trait dimensions relate to medication adherence of glaucoma patientsattending a specialist eye clinic in Ghana. As glaucoma remains the commonest cause of irreversible blindness, itis envisaged that these �ndings will generate enough body of evidence to support public health interventions, andguide the development of patient speci�c treatment plans including assessment and treatment of personalityde�cits to enhance glaucoma treatment outcomes. To the best of our knowledge, no previous study has reportedthe associations between personality traits and adherence to treatment in POAG patients in sub-Saharan Africa,where glaucoma is most prevalent.
Materials And MethodsStudy setting
The study was conducted at the Archbishop Ackon Memorial Christian Eye Centre which is a specialist eye carefacility and a glaucoma referral centre in the Central Region of Ghana. The eye care workforce at this specialist eyecentre consisted of ophthalmologists, optometrists, ophthalmic nurses and opticians. The daily ophthalmic patientattendance to the facility averages one hundred, of which close to 30% are glaucoma patients [7].
Study design and sampling
A cross sectional survey of patients with POAG was conducted between February and May, 2019. The sample forthis study was 400 patients with POAG who were systematically sampled when they reported for routine reviews atthis specialist eye facility. The sample size was determined using the formula N = Z2 (1–p) (p)/b2, where N =minimum sample size, z = the standard normal deviation, set at 1.96 which corresponds to the 95% con�denceinterval, p = estimated prevalence of 30% [7], b = degree of accuracy desired, usually set at 5%. Per this equation,the sample size was determined to be 323 which was adjusted to 400 participants to account for attrition rate andine�ciencies associated with the small sample size.
Inclusion and exclusion criteria
Eligibility for participation in the study was all patients who had been diagnosed of POAG and were receivingtreatment at the specialist eye care facility for at least three months [22]. Diagnosis of glaucoma that met theinclusion criteria was based on a typical glaucomatous optic nerve head abnormalities on dilated fundoscopy(including notching, pallor, disc hemorrhages, vertical cup-to-disc ratio equal to or greater than 0.5 or difference incup disc ratio of more than 0.2 in the two eyes); abnormal glaucoma hemi�eld test or a pattern deviationconsistent with glaucoma (including temporal wedge, nasal step, altitudinal defect, partial arcuate defect etc.);

Page 4/13
gonioscopically con�rmed open anterior chamber angles [18, 23]. Further, patients were included if they had nohistory of psychotic illness, were not alcoholic or on drugs, and did not have dementia as indicated on theirmedical folders or through verbal responses. Participants were excluded if they were less than 18 years old, hadother kinds of glaucoma (closed-angle, congenital or other secondary glaucomas), had a history of cognitivecontra-indications like traumatic brain injury, seizure disorders, unstable ocular conditions (uveitis, cataract, recenttrauma, diabetic retinopathy) and chronic medical conditions (diabetes, sickle cell, hypertension) [8, 19].
Research tools and measures
The Big Five Inventory Questionnaire
The Big Five Inventory questionnaire is made up of 44 items measuring �ve trait dimensions of personality [24].These are extraversion (8 items), agreeableness (9 items), conscientiousness (9 items), neuroticism (8 items) andopenness to experience (10 items). The items were measured on a �ve point Likert scale ranging from 1 = disagreestrongly to 5 = agree strongly. Examples of items on the questionnaire include – I see myself as someone who:“tends to �nd fault with others”, “does a thorough job”, “is reserved”, “can be cold and aloof”. After the respondentsanswer the inventory, the options they choose on the Likert scale for the various items are summed for each traitdimension. Scores equal to or above the �ftieth percentile in a trait was graded high in that particular trait andscores below the �ftieth percentile were considered low. This classi�cation was made to show where personalitystrengths and weaknesses of the participants placed. The dimension with the highest score is considered as thedominant personality trait of the respondent [25].
Medication Adherence Report Scale 5
The Medication Adherence Report Scale 5 (MARS-5) was used to measure participants’ self-reported adherence totheir glaucoma medication regimens [26]. Each of the �ve items on the questionnaire was rated on a �ve pointLikert scale from 1= very often to 5 = never. Some items on the questionnaire include “I take less than instructed”and I stop taking it for a while”. Lower scores indicate lower levels of adherence and vice versa. Adherence wasmeasured by computing the �ve individual items into a composite one with a total score range between 5 and 25;a score of 18.75 ((i.e., 75% of total score)) or less was categorised as non-adherence and a score above 18.75 asadherence [26].
Measured variables
The outcome variable in this study was glaucoma medication adherence scores and the predictive variables werepersonality trait dimension scores, demographic characteristics (age, gender, educational level), and duration ofglaucoma drug use.
Procedures
Before the commencement of the data collection, a pilot study was carried out to ascertain the reliability andvalidity of the research questionnaires with a total of 40 conveniently sampled POAG patients. The outcome of thepilot study indicated that most of the participants found the questionnaire suitable, not stressful and easy tocomprehend. After the responses were reviewed, some modi�cations were made to the items the respondents sawas confusing or di�cult to comprehend. The Cronbach’s alpha (internal consistency) for all the personality

Page 5/13
subscales and MARS-5 ranged between 0.86 and 0.96. For participants who could read and write in the Englishlanguage, the questionnaires were self-administered but for those who could not read and write in English, it wasinterviewer-administered.
Ethical Considerations
The research was approved by the University of Cape Coast Institutional Review Board (UCCIRB/CHAS/2018/47)and the study procedures adhered to the prescribed guidelines in the Declaration of Helsinki for research involvinghuman subjects. Consent forms including local language versions were issued or read out to each participant tosign or thumb-print before enrolling them onto the study. Prior to issuance of consent forms, the rationale andpurpose of the study were explained to each participant in the language they understood best. Also, permissionwas obtained from the management of the eye care facility before the commencement of the study. The patientswere assured of con�dentiality and anonymity as no names were included in the data recording.
Statistical analysis
All data were analysed using IBM SPSS version 23.0. The data were summarised as counts and percentages forcategorical variables. Means adherence scores across demographic variables were initially explored using a one-way Analysis of Variance (ANOVA). Pearson’s correlations were used to ascertain the direction and strength ofrelationship between the various personality trait dimensions and medication adherence scores. Subsequently, aforced entry multiple linear regression model was run to assess how the various personality trait dimensions andother independent variables could predict adherence to glaucoma treatment. The level of signi�cance was set at p≤ 0.05.
ResultsA total of 400 glaucoma patients, with a mean age of 56.3 ± 16.2 (range: 19 to 89) years participated in the study.Most of the participants, 221 (52.8%) were females, but their ages did not differ signi�cantly from that of themales (t = 0.770, p = 0.442). Majority 171 (42.8%) of the participants had no formal education and the averageduration of glaucoma drug usage was 5.2 ± 3.8 years, ranging from 3 months to 18 years. Again, the majority ofpatients, 141 (35.3%) had their highest personality trait scores in the openness subscale, followed byconscientiousness 123 (30.8%), neuroticism 90(22.5%), agreeableness 38(9.5%), and extraversion 8 (2.0%). TheANOVA results showed that age and duration of medication usage had statistically signi�cant association withmedication adherence. The demographic characteristics with mean scores for medication adherence are presentedin Table 1.

Page 6/13
Table 1Demographic characteristics of patients with their mean (standard deviation) scores for
medication adherenceCharacteristics n(%) MARS-5
(Mean ± SD)
95% CI P-value
Gender 0.343
Male 189 (47.2) 18.75 ± 3.36 18.29–19.24
Female 211 (52.8) 18.44 ± 3.44 17.99–18.88
Age group (years) < 0.001
18–34 46(11.5) 19.78 ± 3.31 18.80-20.83
35–50 90(22.5) 19.42 ± 2.82 18.83–20.21
50–64 111(27.8) 18.86 ± 3.21 18.25–19.46
65–80 140(35.0) 17.69 ± 3.07 17.08–18.29
80 13(3.2) 15.92 ± 3.40 14.70-17.78
Duration of medication use (years) < 0.001
5 212(53.0) 19.52 ± 2.99 19.11–19.92
5–9 143(35.8) 17.84 ± 3.50 17.26–18.42
≥ 10 45(11.2) 16.56 ± 3.52 15.50-17.61
Level of formal education 0.054
None 171 (42.8) 18.19 ± 0.249 17.70-18.68
Primary 160 (40.0) 18.75 ± 0.269 18.22–19.28
Secondary 34 (8.5) 19.88 ± 0.586 18.69–21.07
Tertiary 35 (8.8) 18.49 ± 0.651 17.16–19.81
Medication AdherenceMost of the respondents 243 (60.75%) had a medication adherence score of more than 18.75 and so wereclassi�ed as adherent but the overall mean glaucoma medication adherence score was (18.58 ± 3.403) indicatingnon-adherence.
Relationship Between Personality Trait Dimensions AndMedication AdherenceTable 2 presents Pearson’s correlation between medication adherence, the �ve personality trait dimensions andsome patient characteristics. There was a strong but negative relationship between neuroticism and medicationadherence (r = -0.77, ρ 0.001). On the other hand, a signi�cantly strong positive relationship was realised between

Page 7/13
conscientiousness and medication adherence (r 0.71, ρ < 0.001). There was a signi�cantly moderate positiveassociation between adherence to glaucoma medication regimen and the personality pro�le agreeableness (r = 0.419, ρ 0.001). Age of patient signi�cantly and negatively correlated with medication adherence and allpersonality subscales except for neuroticism. Similarly, duration of drug use negatively correlated with adherenceand all the personality subscales except for neuroticism. A signi�cantly moderate positive correlation wasobserved between duration of glaucoma medication use and neuroticism trait(r = 0.419, ρ 0.001), indicating thatthe longer neurotic patients continued to use their medications the more they exhibited neurotic tendencies. Again,older patients and longer use of glaucoma medications were associated with non-compliance.
Table 2Pearson’s correlation between the Big Five personality traits and glaucoma medication adherence
Variables MARS-5 Extraversion Agreeableness Conscientious Neuroticism Openness
MARS-5 -
Extraversion 0.215** -
Agreeableness 0.419** 0.266** -
Conscientiousness 0.719** 0.273** 0.209** -
Neuroticism -0.770** -0.486** -0.531** -0.814** -
Openness 0.180** 0.185** 0.337** 0.348** -0.426**
Age of patient -0.282** -0.115* -0.114* -0.392** 0.373** -0.216**
Duration of druguse
-0.349** -0.093ns -0.182** -0.439** 0.419** -0.208**
**Correlation is signi�cant at the 0.01 level (2-tailed)
*Correlation is signi�cant at the 0.05 level (2-tailed)
ns non-signi�cant association
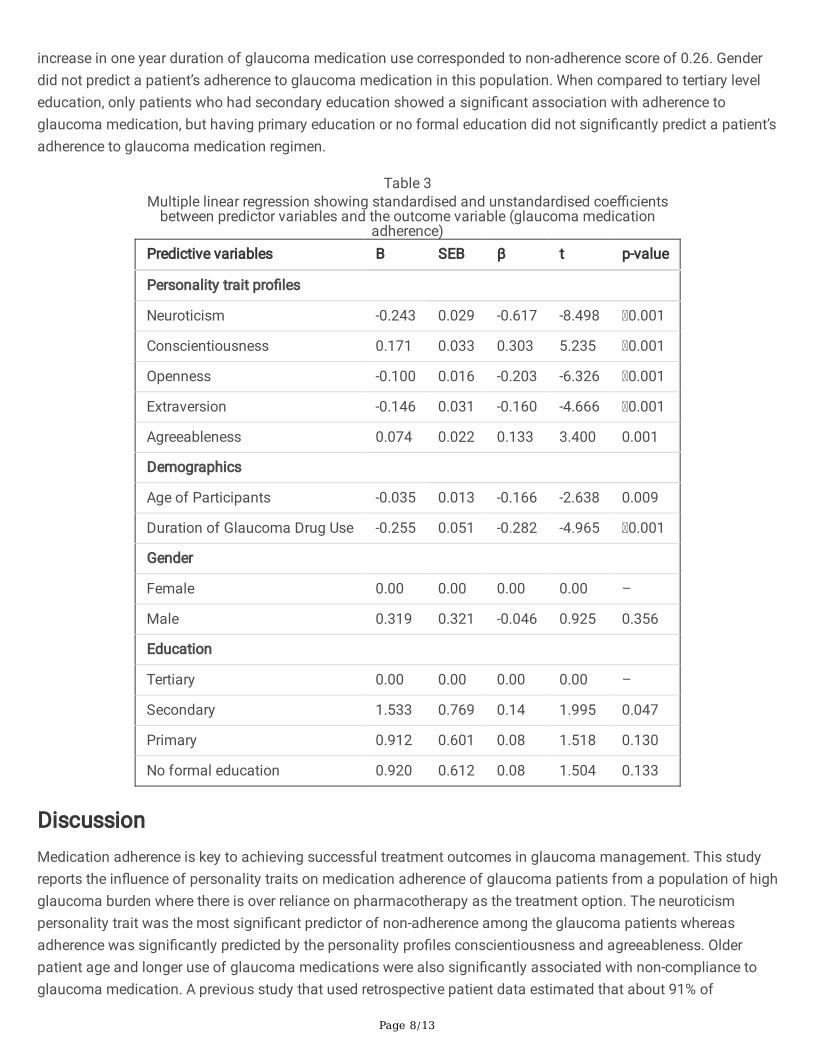
Multiple Linear Regression Between Predictive And The OutcomeVariablesWe performed a multiple linear regression to evaluate how personality traits could predict medication adherenceamong the glaucoma patients. A forced-entry regression was run to assess the contribution of all predictorvariables at the same time, and the overall regression model could explain 67.3% of the variance in the data (R2 = 0.673, F (5, 394) = 165.5, p < 0.001). As shown in Table 3, all the personality trait dimensions signi�cantly predictedthe patients’ adherence to glaucoma medication regimen. The highest predictor of non-adherence was thepersonality trait neuroticism, accounting for 61.7% of the variance in glaucoma medication non-adherence (β = 0.617, t = -8.45, ρ < 0.001), where a unit increase in neuroticism score corresponded to a non-adherence score of0.24. Conscientiousness was the most signi�cant personality dimension associated with glaucoma medicationadherence which accounted for 30.3% of the variance in glaucoma medication adherence. A unit increase in thescore of conscientiousness corresponded to an adherence score of 0.17. Again, as the age of a glaucoma patientincreased by one year, he/she became non-adherent to glaucoma medication by a score of 0.04. Similarly, an
Page 8/13
increase in one year duration of glaucoma medication use corresponded to non-adherence score of 0.26. Genderdid not predict a patient’s adherence to glaucoma medication in this population. When compared to tertiary leveleducation, only patients who had secondary education showed a signi�cant association with adherence toglaucoma medication, but having primary education or no formal education did not signi�cantly predict a patient’sadherence to glaucoma medication regimen.
Table 3Multiple linear regression showing standardised and unstandardised coe�cients
between predictor variables and the outcome variable (glaucoma medicationadherence)
Predictive variables B SEB β t p-value
Personality trait pro�les
Neuroticism -0.243 0.029 -0.617 -8.498 0.001
Conscientiousness 0.171 0.033 0.303 5.235 0.001
Openness -0.100 0.016 -0.203 -6.326 0.001
Extraversion -0.146 0.031 -0.160 -4.666 0.001
Agreeableness 0.074 0.022 0.133 3.400 0.001
Demographics
Age of Participants -0.035 0.013 -0.166 -2.638 0.009
Duration of Glaucoma Drug Use -0.255 0.051 -0.282 -4.965 0.001
Gender
Female 0.00 0.00 0.00 0.00 –
Male 0.319 0.321 -0.046 0.925 0.356
Education
Tertiary 0.00 0.00 0.00 0.00 –
Secondary 1.533 0.769 0.14 1.995 0.047
Primary 0.912 0.601 0.08 1.518 0.130
No formal education 0.920 0.612 0.08 1.504 0.133
DiscussionMedication adherence is key to achieving successful treatment outcomes in glaucoma management. This studyreports the in�uence of personality traits on medication adherence of glaucoma patients from a population of highglaucoma burden where there is over reliance on pharmacotherapy as the treatment option. The neuroticismpersonality trait was the most signi�cant predictor of non-adherence among the glaucoma patients whereasadherence was signi�cantly predicted by the personality pro�les conscientiousness and agreeableness. Olderpatient age and longer use of glaucoma medications were also signi�cantly associated with non-compliance toglaucoma medication. A previous study that used retrospective patient data estimated that about 91% of

Page 9/13
glaucoma patients in Ghana did not fully adhere to their medication regimens [10]. Using the MedicationAdherence Report Scale 5, the present study found self-reported adherence to glaucoma medication to be 60.8%among a cohort of glaucoma patients.
Varying levels of adherence to glaucoma medication have been reported globally, ranging from 61.4% in Ethiopia[27], 63.2% in Nigeria [28], 73.0% in the USA [13], and 77% in Hungary [29]. Apart from population-speci�c factorssuch as income levels, urbanisation and health insurance coverage [10, 27, 28], the diversity of methodologicalapproaches may also account for the differing reported adherence levels by the various studies. Glaucomapatients have been particularly described as non-adherence to their medications when compared to patients withother chronic diseases. Yeaw et al. have documented that persistence and adherence to glaucoma medicationswere signi�cantly lower than that for hyperlipidemia, osteoporosis, diabetes, overactive bladder, and hypertension[30]. Other barriers including African ancestry [22] and personality pro�les have been documented to account forthe signi�cant medication non-adherence among glaucoma patients. The current study revealed that theneuroticism personality trait was the highest predictor of non-adherence accounting for the highest variance(61.7%) in the analysis of all the personality subscales (β = 0.617, t = -8.45, ρ < 0.001). Similar trends have alsobeen described among glaucoma patients across many populations [16, 17, 19, 31]. Again, a review of literature onpsycho-ophthalmology suggests a greater level of psychopathology amongst glaucoma patients such as hysteria,hypochondriasis, depression, stress and anxiety [8, 18, 19, 32–35]. Mabuchi et al reported that patients withglaucoma recorded signi�cantly higher scores for neuroticism than patients with cataracts [17]. All these �ndingssuggest that there is something characteristic of a glaucoma diagnosis that is associated with medication non-adherence or feelings of ill health. For instance, a glaucoma diagnosis may ignite worries of blindness andconsequent loss of physical and �nancial independence [36]. Again, there is evidence of psychophysiologicalreactivity to ocular hypertension where high levels of anxiety were found to increase intraocular pressure (IOP) toclinically signi�cantly degrees [34, 37]. The physiological basis for this phenomenon may be related to thesympathetic and parasympathetic regulation of aqueous humor dynamics [34, 38].
Next to neuroticism, the conscientiousness trait had the second highest variance (30.3%) in the personality traitregression analysis. Conscientiousness, however, had a positive outlook, predicting adherence with glaucomamedication. Conscientious individuals often exhibit positive life tendencies such as self-discipline, self-control,determination, and hardworking which are associated with positive health outcomes [17, 39]. Scores in theagreeableness subscale also predicted patients’ adherence to glaucoma medication regimes in this study but thistrait accounted for only 13.3% of the variance in the data. Relatedly, Chen et al. and Mabuchi et al. in case-controlstudies among glaucoma cases and non-glaucoma controls, found that glaucoma patients recorded signi�cantlyhigher levels of neuroticism but lower scores for openness and extraversion [17, 19]. Chen et al. actually found apositive relation between openness and agreeableness and positive health seeking behavior in a Chineseglaucoma population [19]. In contrast to these previous �ndings, the present results indicated that extraversionand openness traits predicted non-adherence. Though both extraversion and openness trait dimensions havesome positive facets like sociability, optimism, creativity and enthusiasm they have been reported to associatewith health-risk behaviors while agreeableness and conscientiousness where less associated with such riskyendeavours [17, 40, 41]. It therefore clear that personality trait assessment in respect of medication compliance inthis study presented a more negative outlook as the highest variance in the analysis was accounted for by non-adherence tendencies. To achieve successful treatment outcomes in patients with glaucoma, protocols forglaucoma management could include the assessment of patient’s personality pro�les in order to tailor care andtreatment to the individual and personal levels. For patients with high scores in neuroticism, psychotherapeutic

Page 10/13
management should also be sought in order to enhance medication adherence. Nakano et al. [31] have advocatedthat since individuals with high neuroticism are sensitive to negative emotions, glaucoma prognostic informationcould be provided to them from an optimistic viewpoint such as “this medication will prevent 80% of patients withglaucoma from going blind”. On the other hand, for individuals with low neuroticism, prognostic informationshould be formulated from a pessimistic perspective like “20% of patients will go blind whether or not they receivethis medication”. These approaches will enhance compliance.
The burden of glaucoma is known to be high among the aged due to the di�culty in diagnosing glaucoma earlyand the fact that age related tissue changes contribute to the progression of glaucoma [42]. Our �nding thatmedication adherence reduced with increasing age and that old age also correlated with high scores forneuroticism could portend a double jeopardy for the older glaucoma population. Results of the present studyfurther revealed that older patients and longer use of glaucoma medications were associated with non-compliance. The development of age speci�c treatment plans, taking into account the individuals’ personalitieswill improve adherence among this at risk population. In addition to what has been mentioned earlier, practitionerscould adopt some recommended adherence strategies like enforcing regular reviews, patient education, givingwritten instructions to patients and the inclusion of such patients in national health insurance schemes [10, 43,44].
A limitation for this study was the use of self-report to measure personality traits and medication adherence,making it susceptible to social desirability bias especially for medication adherence and a tendency for a recallbias.
ConclusionGlaucoma patients’ personality pro�les signi�cantly predicted their adherence to glaucoma medications. Theneuroticism domain was associated with non-adherence and accounted for the highest variance in the analysis ofall the personality traits. This was followed by the conscientiousness subscale which signi�cantly predictedadherence. Extraversion and agreeableness respectively contributed 20.2 and 1.16 to the variance and were bothassociated with non-adherence. Glaucoma diagnosis and management protocols should include assessment ofpersonality pro�les and psychotherapy as appropriate.
DeclarationsFunding
This study received no funding
Compliance with ethical standards
Con�ict of interest
None of the authors has any proprietary interests or con�icts of interest related to this submission
Ethical approval
The research was approved by the University of Cape Coast Institutional Review Board and the study proceduresadhered to the prescribed guidelines in the Declaration of Helsinki for research involving human subjects.
Page 11/13
Informed consent
Informed consent was obtained from all individual participants included in the study
References1. Kulkarni SV, Damji KF, Buys YM (2008) Medical management of primary open-angle glaucoma: Best practices
associated with enhanced patient compliance and persistency. Patient Prefer Adherence 2:303–314
2. Resnikoff S, Pascolini D, Etya'Ale D et al (2004) Global data on visual impairment in the year 2002. Bull WorldHealth Organ 82:844–851
3. Ntim-Amponsah CT, Amoaku WM, Ofosu-Amaah S et al (2004) Prevalence of glaucoma in an Africanpopulation. Eye 18:491–497
4. Mason RP, Kosoko O, Wilson MR et al (1989) National survey of the prevalence and risk factors of glaucomain St. Lucia, West Indies: Part I. Prevalence �ndings. Ophthalmology 96:1363–1368
5. Gupta SK, Niranjan GD, Agrawal SS, Srivastava S, Saxena R (2008) Recent advances in pharmacotherapy ofglaucoma. Indian J Pharmacol 40:197–208
�. Mansouri K, Medeiros FA, Weinreb RN (2013) Global rates of glaucoma surgery. Graefes Arch Clin ExpOphthalmol 251:2609–2615
7. Kyei S, Obeng PA, Kwarteng MA, Assiamah F (2021) Epidemiology and clinical presentation of glaucoma in areferral facility in Ghana: any lessons for public health intervention? PLoS One 16:e0245486
�. Pappa C, Hyphantis T, Pappa S et al (2006) Psychiatric manifestations and personality traits associated withcompliance with glaucoma treatment. J Psychosom Res 61:609–617
9. Konstas AG, Maskaleris G, Gratsonidis S, Sardelli C (2000) Compliance and viewpoint of glaucoma patients inGreece. Eye 14:752–756
10. Ocansey S, Kyei S, Diafo A, Darfor KN, Boadi-Kusi SB, Aglobitse PB (2016) Cost of the medical managementand prescription pattern for primary open angle glaucoma (POAG) in Ghana–a retrospective cross-sectionalstudy from three referral facilities. BMC Health Serv Res 16:1–8
11. Tsai JC, McClure CA, Ramos SE, Schlundt DG, Pichert JW (2003) Compliance barriers in glaucoma: asystematic classi�cation. J Glaucoma 12:393–398
12. Gellad WF, Grenard JL, Marcum ZA (2011) A systematic review of barriers to medication adherence in theelderly: looking beyond cost and regimen complexity. Am J Geriatr Pharmacother 9:11–23
13. Newman-Casey PA, Robin AL, Blachley T et al (2015) The most common barriers to glaucoma medicationadherence: a cross-sectional survey. Ophthalmology 122:1308–1316
14. Hibbeler HL (1947) Personality patterns of white adults with primary glaucoma. Am J Ophthalmol 30:181–186
15. Shaheen O, Labib MA, Abboud I, el-Rifai M (1970) Some ophthalmological factors affecting the personalitypatterns in primary glaucoma patients as determined by the Minnesota Multiphasic Personality Inventory. BullOphthalmol Soc Egypt 63:139–140
1�. Çakmak H, Altinyazar V, Yilmaz SG et al (2015) The temperament and character personality pro�le of theglaucoma patient. BMC Ophthalmol 15:1–8

Page 12/13
17. Mabuchi F, Yoshimura K, Kashiwagi K et al (2005) Personality assessment based on the �ve-factor model ofpersonality structure in patients with primary open-angle glaucoma. Jpn J Ophthalmol 49:31–35
1�. Lim MC, Shiba DR, Clark IJ et al (2007) Personality type of the glaucoma patient. J Glaucoma 16:649–654
19. Chen J, Lin ZN, Tao YT et al (2019) In�uences of personality characteristics and coping modes on anxiety inprimary glaucoma patients. Int J Ophthalmol 12:1163–1169
20. Bartram D (2013) Scalar equivalence of OPQ32: Big Five pro�les of 31 countries. J Cross Cult Psychol 44:61–83
21. Rentfrow PJ, Jokela M, Lamb ME (2015) Regional personality differences in Great Britain. PloS One10:e0122245
22. Dreer LE, Girkin C, Mansberger SL (2012) Determinants of medication adherence to topical glaucoma therapy.J Glaucoma 21:234–240
23. Keltner JL, Johnson CA, Cello KE et al (2003) Ocular Hypertension Treatment Study Group. Classi�cation ofvisual �eld abnormalities in the ocular hypertension treatment study. Arch Ophthalmol 121:643–650
24. Intiful FD, Oddam EG, Kretchy I, Quampah J (2019) Exploring the relationship between the big �ve personalitycharacteristics and dietary habits among students in a Ghanaian University. BMC Psychol 7:1–7
25. De Raad B, Mlačić B (2015) Big Five Factor Model, theory and structure. Int Encycl Soc Behav Sci 2:559–566
2�. Adeniran A, Akinyinka M, Wright KO et al (2015) Personality traits, medication beliefs & adherence tomedication among diabetic patients attending the diabetic clinic in a teaching hospital in southwest Nigeria. JDiabetes Mellitus 5:319–329
27. Anbesse DH, Yibekal BT, Assefa NL (2019) Adherence to topical glaucoma medications and associatedfactors in Gondar University Hospital Tertiary Eye Care Center, northwest Ethiopia. Eur J Ophthalmol 29:189–195
2�. Onwubiko SN, Nwachukwu NZ, Eze B (2020) Glaucoma medications: issues with adherence in a tertiaryhospital in Nigeria. Fam Med Prim Care Rev Review 22:302–306
29. Holló G, Kóthy P, Géczy A, Vargha P (2009) Personality traits, depression, and objectively measured adherenceto once-daily prostaglandin analog medication in glaucoma. J Glaucoma 18:288–292
30. Yeaw J, Benner JS, Walt JG, Sian S, Smith DB (2009) Comparing adherence and persistence across 6 chronicmedication classes. J Manag Care Pharm 15:728–740
31. Nakano T, Kodaka F, Tsuneoka H (2016) Differences in neuroticism between patients with glaucoma whohave discontinued visits to ophthalmologists and those who make regular visits: implications for adherenceto topical glaucoma medications. Ophthalmol Ther:207–214
32. Mabuchi F, Yoshimura K, Kashiwagi K et al (2008) High prevalence of anxiety and depression in patients withprimary open-angle glaucoma. J Glaucoma 17:552–557
33. Bubella RM, Bubella DM, Cillino S (2014) Type A behavior pattern: is it a risk factor for open-angle chronicglaucoma? J Glaucoma 23:199–201
34. Méndez-Ulrich JL, Sanz A, Feliu-Soler A, Álvarez M, Borràs X (2018) Could white coat ocular hypertensionaffect to the accuracy of the diagnosis of Glaucoma? Relationships between anxiety and intraocular pressurein a simulated clinical setting. Appl Psychophysiol Biofeedback 43:49–56
35. Mabuchi F, Yoshimura K, Kashiwagi K et al (2012) Risk factors for anxiety and depression in patients withglaucoma. Br J Ophthalmol 96(6):821–825

Page 13/13
3�. Odberg T, Jakobsen J, Hultgren S (2001) The impact of glaucoma on the quality of life of patients in Norway.Acta Ophthalmol Scand 79:116–120
37. Méndez-Ulrich JL, Casas N, Sanz A (2013) Ocular white coat hypertension: A pilot study. Ansiedad y Estrés19:41–51
3�. Chiquet C, Denis P (2004) The neuroanatomical and physiological bases of variations in intraocular pressure.J Fr Ophtalmol 27:2S11–2S18
39. Warrian KJ, Spaeth GL, Lankaranian D, Lopes JF, Steinmann WC (2009) The effect of personality on measuresof quality of life related to vision in glaucoma patients. Br J Ophthalmol 93:310–315
40. Breivik G, Sand TS, Sookermany AM (2020) Risk-taking attitudes and behaviors in the Norwegian population:the in�uence of personality and background factors. J Risk Res 23:1504–1523
41. McGhee RL, Ehrler DJ, Buckhalt JA, Phillips C (2012) The relation between �ve-factor personality traits andrisk-taking behavior in preadolescents. Psychology 3:558–561
42. Leskea MC, Heijl A, Hyman L, Bengtsson B, Komaroff E (2004) Factors for progression and glaucomatreatment: the Early Manifest Glaucoma Trial. Curr Opin Ophthalmol 15:102–106
43. Kharod BV, Johnson PB, Nesti HA, Rhee DJ (2006) Effect of written instructions on accuracy of self-reportingmedication regimen in glaucoma patients. J Glaucoma 15:244–247
44. Jampel HD, Parekh P, Johnson E, Miller R (2005) Chart documentation by general physicians of the glaucomamedications taken by their patients. Am J Ophthalmol 140:344–345





























