Embed Size (px)
Citation preview

GIS-K-25
ACUTE APPENDICITIS
Appendiceal Mass / Abscess
Syahbuddin Harahap
Division of Digestive Surgery
Department of SurgeryDepartment of Surgery
Faculty of Medicine University of North Sumatera
Adam Malik Hospital

INTRODUCTION
The appendix is :
-Wormlike extension of the cecum (vermiform appendix).
-Length is 8-10 cm (ranging from 2-20 cm).
-Fifth month of gestation-Fifth month of gestation
-Several lymphoid follicles.

Etiology: Obstruction of the lumen appendix followed by infection
�Catarrhal appendicitis. -lymphoid hyperplasia (60% children)
-Gastro enteritis -Virus -Acute respiratory infection -Mononucleosis
�Obstructive appendicitis -fecalith 35% adults.
-foreign body / parasites (4%)
- tumors (1%)

Pathophysiology
�Wangensteen proposed1. Closed loop obstruction2. Increase in luminal pressure. 3. Exceeds capillary pressure causes mucosal ischemia4. Luminal bacterial overgrowth and translocation bacteria across the
appendiceal wall result :-Inflammation-Inflammation-Edema-Necrosis � perforation occur about 48 hours .
�If the body successfully walls off the perforation Appendiceal Mass
�If the perforation is not successfully walled off � Diffuse peritonitis will
develop.

Problem:
Appendicitis can mimic several abdominal conditions.
�Laboratory test�Imaging investigation
Statistics report�1 of 5 cases is misdiagnosed�1 of 5 cases is misdiagnosed
�Normal appendix is found in 15-40% Emergency appendectomy.(Negative Appendectomy)

Differential diagnosis of acute appendicitis
Surgical
• Acute Intestinal obstruction
• Intussusception
• Acute cholecystitis
• Perforated peptic ulcer
• Mesenteric adenitis
• Acute Meckel's diverticulitis
Urological
• Right ureteric colic
• Right pyelonephritis
• Urinary tract infection
• Right Acute epididymitis
Gynaecological
• Ectopic pregnancy• Acute Meckel's diverticulitis
• Acute Pancreatitis
Medical
• Gastroenteritis
• Basal Pneumonia dextra
• Terminal ileitis
• Ectopic pregnancy
• Ruptured ovarian follicle
• Torted ovarian cyst
• Salpingitis/pelvic inflammatory disease

Differential diagnosis of appendicitis appendicitis can mimic several abdominal conditions.

Lab Studies:
Complete blood cell countA mild elevation of WBCs (ie, >10,000/µL)
Urinalysis
�Mild pyuria �relationship of the appendix with the right �Mild pyuria �relationship of the appendix with the right
ureter.
�Severe pyuria �in UTI.
�For women of childbearing age,Ectopic pregnancy� test urin (beta-hCG)
On physical examination
•Lying down
•Flexing their hips
•The most common symptom of appendicitis is :- Acute abdominal pain.- Epigastric or Periumbilical pain migrating to the - Epigastric or Periumbilical pain migrating to the right lower quadrant (RLQ) of the abdomen.
- Vomiting, nausea, and anorexia- Afebrile or has a low-grade fever , 38 º C
•Higher fevers are associated with a perforated appendix

Special maneuvers
�McBurney sign
�McBurney's point
it is only the area
of greatest tenderness
�Blumberg sign
�Rovsing’s Sign
�Dunphy sign Cough Test
�Obturator sign
�Psoas sign
�Markle sign

Location appendix during pregnancy

INDICATIONS
Consider an appendectomy for patients with a history of :
•Persistent abdominal pain•Persistent abdominal pain•Fever•Clinical signs of localized or diffuse peritonitis•Especially if leukocytosis is present.

Imaging Studies
Abdomen plain film: Fecalith within the appendixUrolithiasis right middle third

MANTRELS SCORE
Characteristic Score
M = Migration of pain to the RLQ 1
A = Anorexia 1
N = Nausea and vomiting 1
T = Tenderness in RLQ 2
Alvarado score 1986
R = Rebound pain 1
E = Elevated temperature 1
L = Leukocytosis 2
S = Shift of WBC to the left 1
Total 10
A score of 7 or more is strongly predictive of acute appendicitis.

Sonography
Advantages of sonography
1. Noninvasiveness,2. Short acquisition time3. Lack of radiation exposure4. Potential for diagnosis of
normal less than 6 mm
4. Potential for diagnosis of other causes of abdominal pain
5. Pediatric patients6. Women of childbearing age. 7. Pregnant women

CT scan
-Oral contrast medium
-Rectal Gastrografin enema
�Reserved for patients -Uncertain diagnosis
more than 6 mm
-Uncertain diagnosis -Severe obesity.

If the clinical picture is unclear
�Short period (4-6 h) of watchful waiting
�USG / CT scan -May improve diagnostic accuracy
�Without a definite diagnosis - return for continued or recurrent symptoms - follow-up examination in 24 hours.

Complications
• Perforation
• General Secondary Peritonitis
• Appendiceal Mass
• Appendiceal Abscess
• Pylephlebitis is suppurative thrombophlebitis of the • Pylephlebitis is suppurative thrombophlebitis of the
portal venous system
• Hepatic absces
• Chills
• High fever
• Jaundice

TREATMENTMedical therapy
�Resuscitated adequately with fluids .
�Preoperative prophylactic antibiotics-Acute Appendicitis single agent second-generation cephalosporin.
-Perforated appendix triple antibiotic therapy -Perforated appendix triple antibiotic therapy Ampicillin , gentamycin , metronidazol
�Antibiotic prophylaxis should be administered before every appendectomy.
�Antibiotic treatment may be stopped. -Becomes afebrile -WBC count normalizes

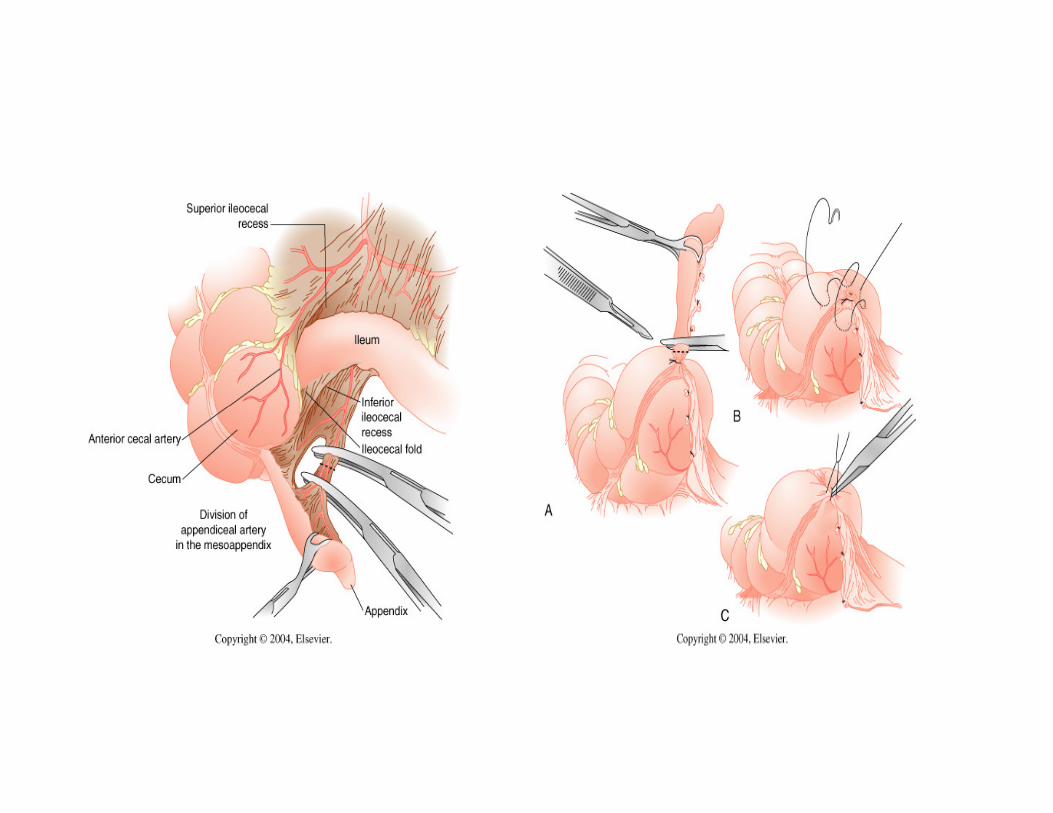
Two approaches to appendectomy
1. Open Emergency Appendicectomy ( Appendectomy)
2. Laparoscopic appendectomy
� If normal appendix removed need to look for:
Meckel's diverticulum-Meckel's diverticulum
- Acute salpingitis
- Crohn's disease

�If the body successfully walls off the localized perforation
Appendiceal Mass
�RLQ mass�The pain may actually improve. �Symptoms do not completely resolve. �Still have right lower quadrant pain�Still have right lower quadrant pain�Decreased appetite�Change in bowel habits (eg, diarrhea, constipation)�Intermittent low-grade fever.

Treatment of
�Appendiceal Mass Nonoperative management Becomes walled off by omentum and ajacent viscera.Initially treated with intravenous broad-spectrum antibiotic
�Appendiceal Abscess � USG or CT scan
-Percutaneous aspiration-Drain placement
Intravenous antibiotics are continued until the patient Intravenous antibiotics are continued until the patient - afebrile for 24 hours- return of normal gastrointestinal function- normal WBC count with a normal differential.
At this time, patients are switched to oral antibiotics for a total antibiotic course of 10-14 days.
Traditionally, interval appendectomy is performed 6-8 weeks later.

Acute Appendicitis Appendicitis Perforation




















![Acute Appendicitis[1]](https://img.dokumen.tips/doc/110x75/577cd3341a28ab9e7896e8e0/acute-appendicitis1.jpg)




