Embed Size (px)
Citation preview

Giovambattista DesideriUniversità degli Studi dell’Aquila
Dipartimento di Medicina Interna e Sanità Pubblica
Approccio terapeutico all’anziano iperteso:
quanto e come trattare
Approccio terapeutico all’anziano iperteso:
quanto e come trattare
Simposio SIGG-SIGGIpertensione arteriosa: gli
aspetti peculiari nell’anziano
Simposio SIGG-SIGGIpertensione arteriosa: gli
aspetti peculiari nell’anziano
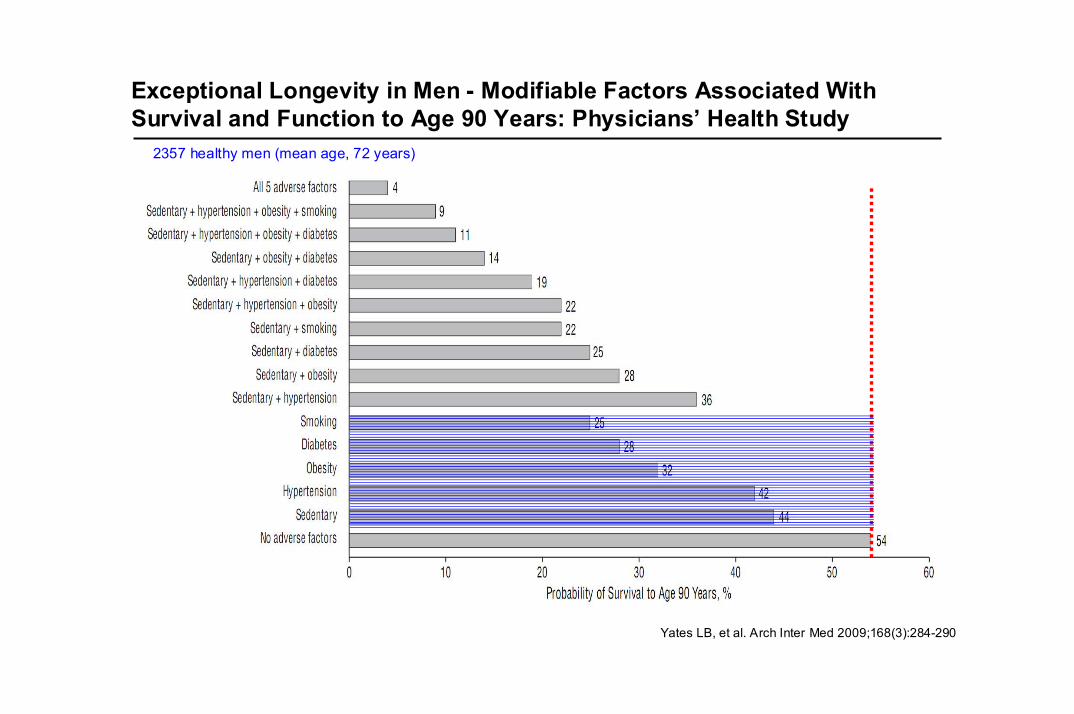
Exceptional Longevity in Men - Modifiable Factors Associated With Survival and Function to Age 90 Years: Physicians’ Health Study
Yates LB, et al. Arch Inter Med 2009;168(3):284-290
2357 healthy men (mean age, 72 years)
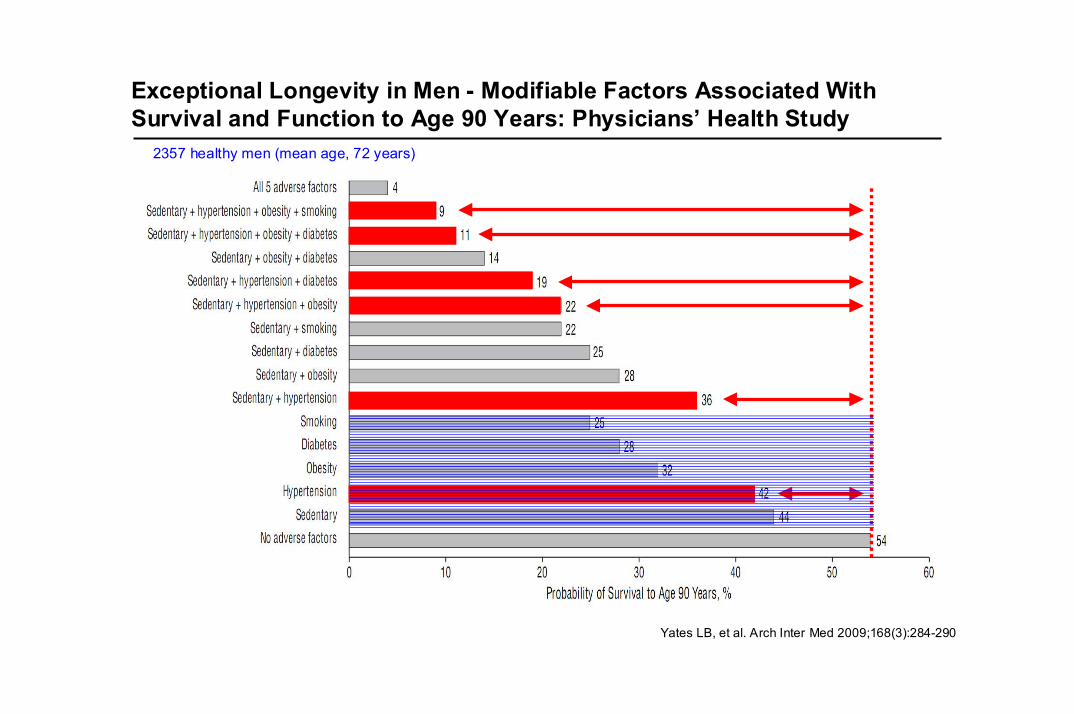
Yates LB, et al. Arch Inter Med 2009;168(3):284-290
2357 healthy men (mean age, 72 years)
Exceptional Longevity in Men - Modifiable Factors Associated With Survival and Function to Age 90 Years: Physicians’ Health Study
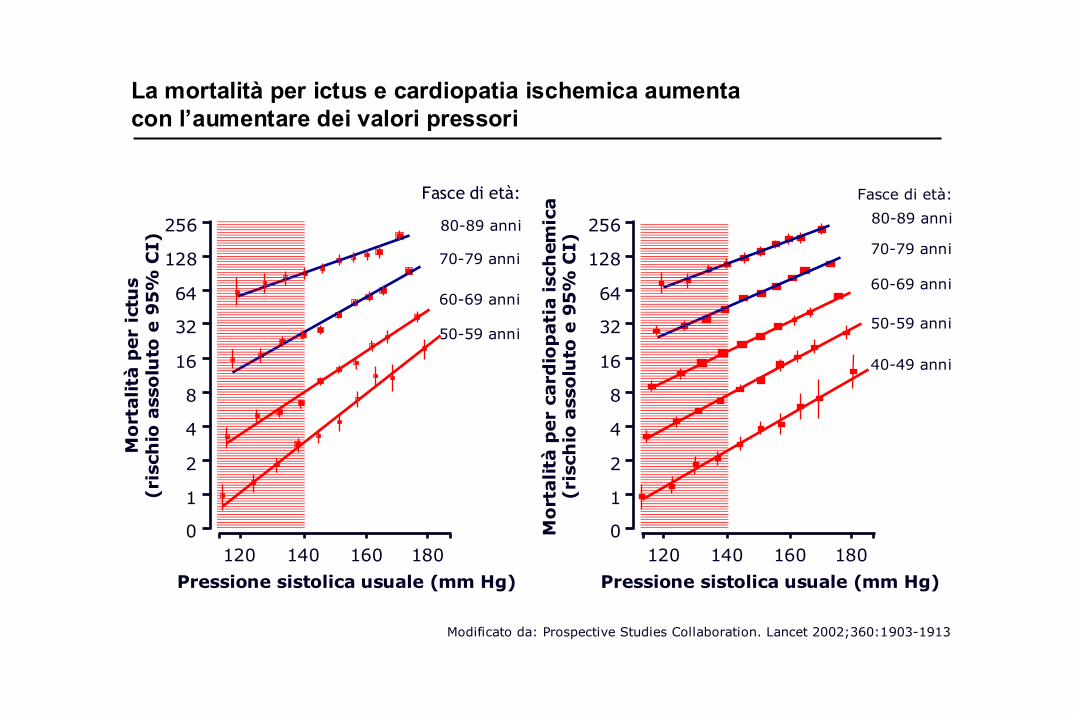
Modificato da: Prospective Studies Collaboration. Lancet 2002;360:1903-1913
Mo
rtalità
per
ictu
s(r
isch
io a
sso
luto
e 9
5%
CI)
Pressione sistolica usuale (mm Hg)
50-59 anni
60-69 anni
70-79 anni
80-89 anni
Fasce di età:
256
128
64
32
16
8
4
2
1
0120 140 160 180
Mo
rtalità
per
card
iop
ati
a isc
hem
ica
(ris
chio
ass
olu
toe 9
5%
CI)
Pressione sistolica usuale (mm Hg)
256
128
64
32
16
8
4
2
1
0120 140 160 180
50-59 anni
60-69 anni
70-79 anni
80-89 anni
Fasce di età:
40-49 anni
La mortalità per ictus e cardiopatia ischemica aumenta con l’aumentare dei valori pressori
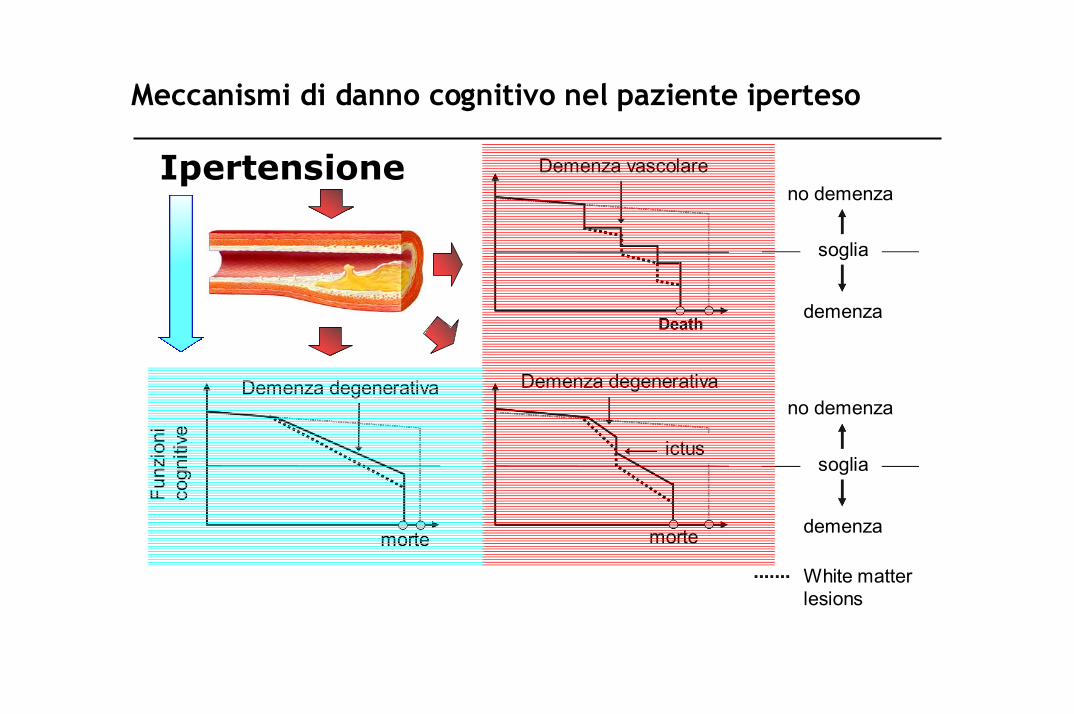
Ipertensione
Meccanismi di danno cognitivo nel paziente iperteso
Demenza vascolare
Demenza degenerativaDemenza degenerativa
Funz
ioni
cogn
itive
no demenza
demenza
soglia
no demenza
demenza
soglia ictus
morte morte
White matter lesions
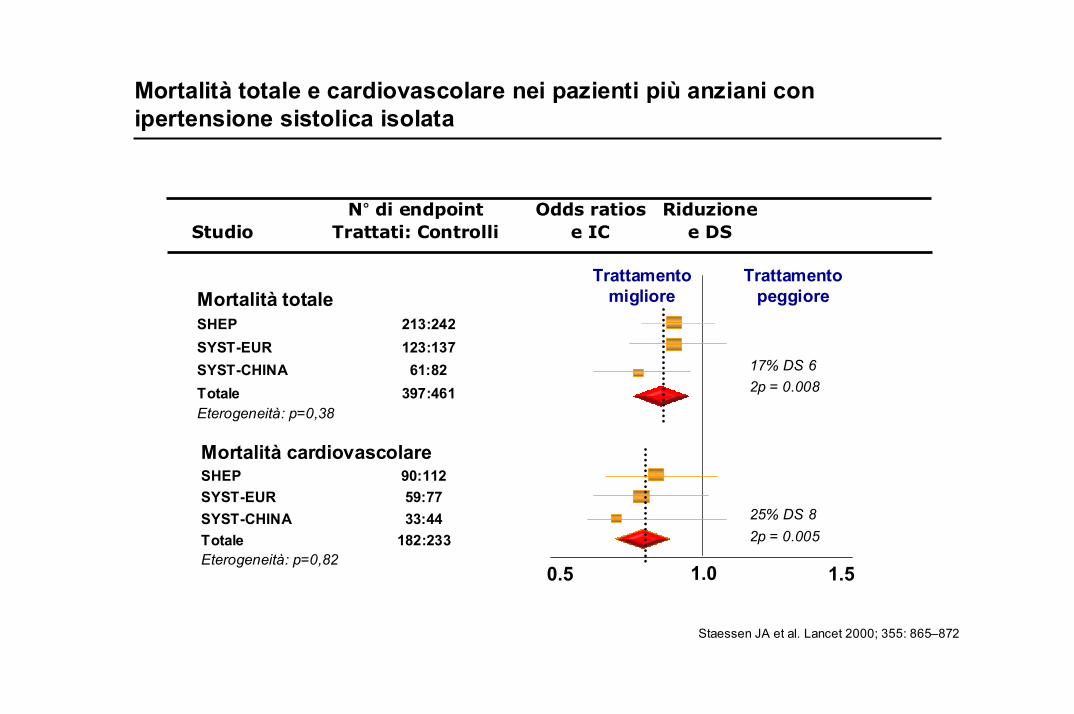
Mortalità totaleSHEP 213:242SYST-EUR 123:137SYST-CHINA 61:82Totale 397:461Eterogeneità: p=0,38
Mortalità cardiovascolareSHEP 90:112SYST-EUR 59:77SYST-CHINA 33:44Totale 182:233Eterogeneità: p=0,82
N° di endpoint Odds ratios RiduzioneStudio Trattati: Controlli e IC e DS
Trattamentopeggiore
1.00.5 1.5
17% DS 62p = 0.008
25% DS 82p = 0.005
Staessen JA et al. Lancet 2000; 355: 865–872
Trattamentomigliore
Mortalità totale e cardiovascolare nei pazienti più anziani con ipertensione sistolica isolata
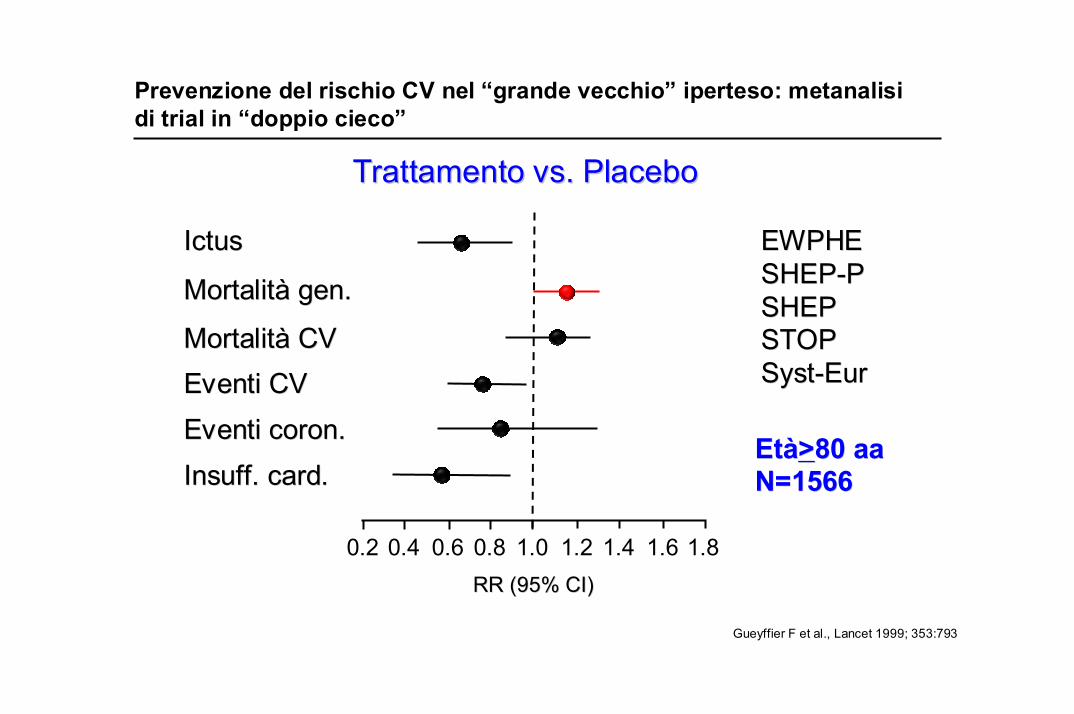
Gueyffier F et al., Lancet 1999; 353:793
MortalitMortalitàà gen.gen.
MortalitMortalitàà CVCV
Eventi coronEventi coron..
IctusIctus
InsuffInsuff. card.. card.
EventiEventi CVCV
EWPHEEWPHESHEPSHEP--PPSHEPSHEPSTOPSTOPSystSyst--EurEur
1.00.80.2 0.4 0.6 1.2 1.4 1.6 1.8RR (95% CI)RR (95% CI)
TrattamentoTrattamento vs. Placebovs. Placebo
EtEtàà>>8080 aaaaN=1566N=1566
Prevenzione del rischio CV nel “grande vecchio” iperteso: metanalisidi trial in “doppio cieco”
Gueyffier F et al., Lancet 1999; 353:793
MortalitMortalitàà gen.gen.
MortalitMortalitàà CVCV
Eventi coronEventi coron..
IctusIctus
InsuffInsuff. card.. card.
EventiEventi CVCV
EWPHEEWPHESHEPSHEP--PPSHEPSHEPSTOPSTOPSystSyst--EurEur
1.00.80.2 0.4 0.6 1.2 1.4 1.6 1.8RR (95% CI)RR (95% CI)
TrattamentoTrattamento vs. Placebovs. Placebo
EtEtàà>>8080 aaaaN=1566N=1566
Prevenzione del rischio CV nel “grande vecchio” iperteso: metanalisidi trial in “doppio cieco”
Keep Antihypertensive drugs away from very old people
….The instrument of geriatric assessment should be included in future biomedical trials with elderly patients.
Peter Oster, Gunter Schlierf - Lancet 1999
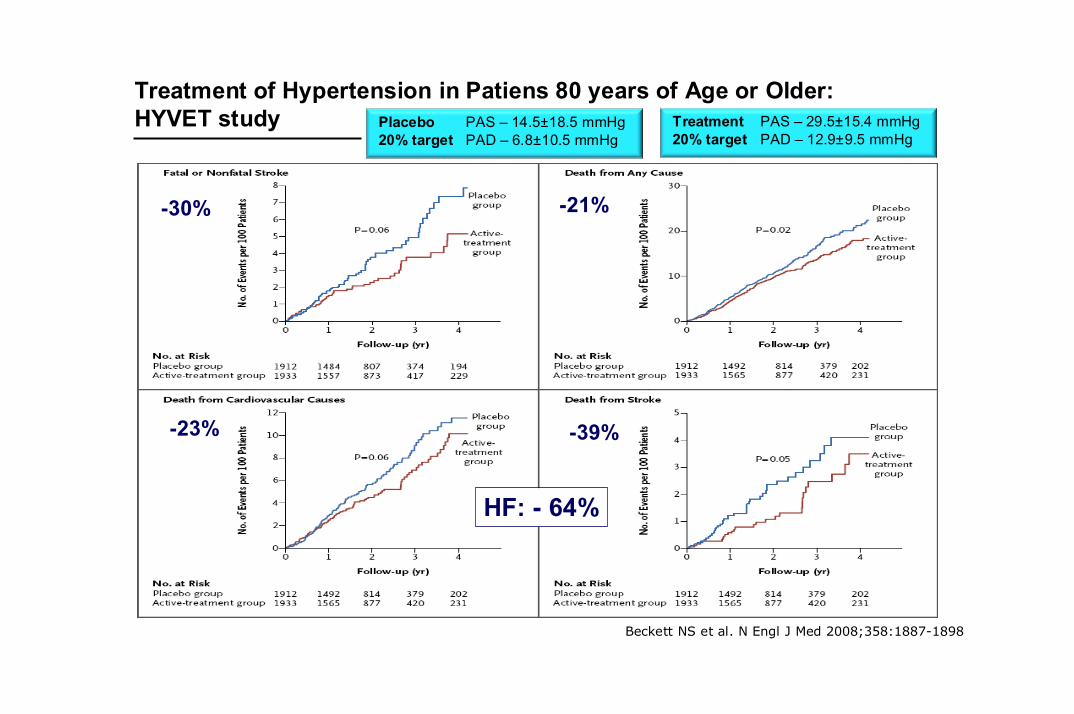
Beckett NS et al. N Engl J Med 2008;358:1887-1898
Treatment of Hypertension in Patiens 80 years of Age or Older: HYVET study
-30%
-39%-23%
HF: - 64%
-21%
PAS – 14.5±18.5 mmHgPAD – 6.8±10.5 mmHg
Placebo20% target
PAS – 29.5±15.4 mmHgPAD – 12.9±9.5 mmHg
Treatment20% target
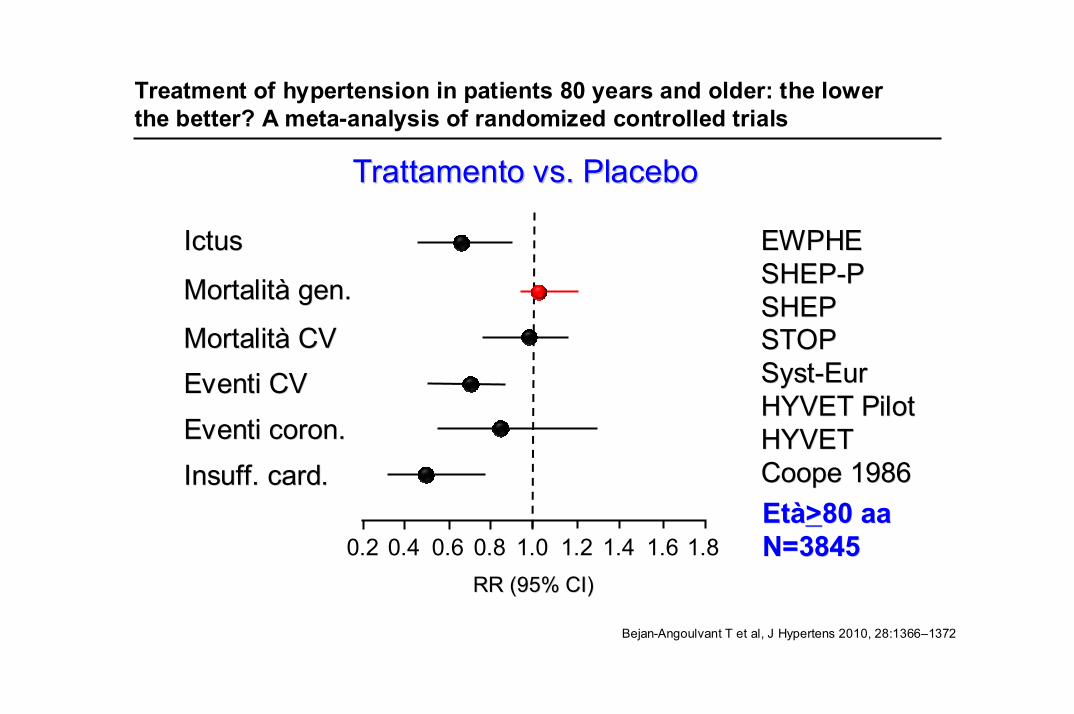
Bejan-Angoulvant T et al, J Hypertens 2010, 28:1366–1372
MortalitMortalitàà gen.gen.
MortalitMortalitàà CVCV
Eventi coronEventi coron..
IctusIctus
InsuffInsuff. card.. card.
EventiEventi CVCV
EWPHEEWPHESHEPSHEP--PPSHEPSHEPSTOPSTOPSystSyst--EurEurHYVET PilotHYVET PilotHYVETHYVETCoopeCoope 19861986
1.00.80.2 0.4 0.6 1.2 1.4 1.6 1.8RR (95% CI)RR (95% CI)
TrattamentoTrattamento vs. Placebovs. Placebo
EtEtàà>>8080 aaaaN=3845N=3845
Treatment of hypertension in patients 80 years and older: the lowerthe better? A meta-analysis of randomized controlled trials
Turnbull F, et al. BMJ 2008;336:1121-1123
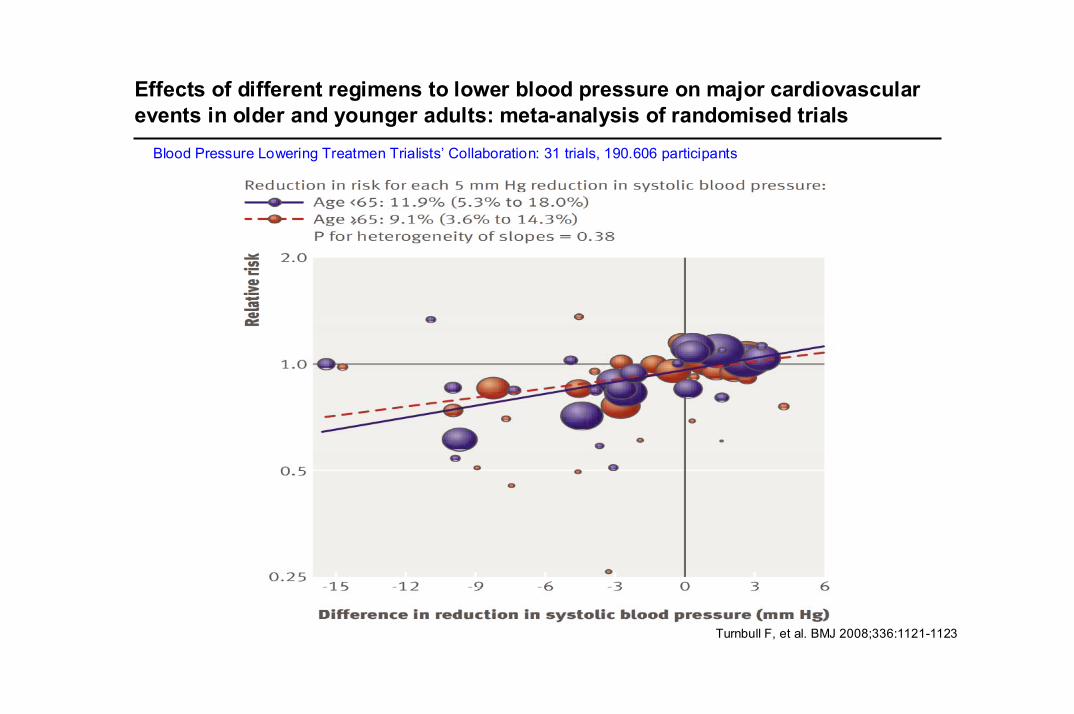
Effects of different regimens to lower blood pressure on major cardiovascular events in older and younger adults: meta-analysis of randomised trials
Blood Pressure Lowering Treatmen Trialists’ Collaboration: 31 trials, 190.606 participants
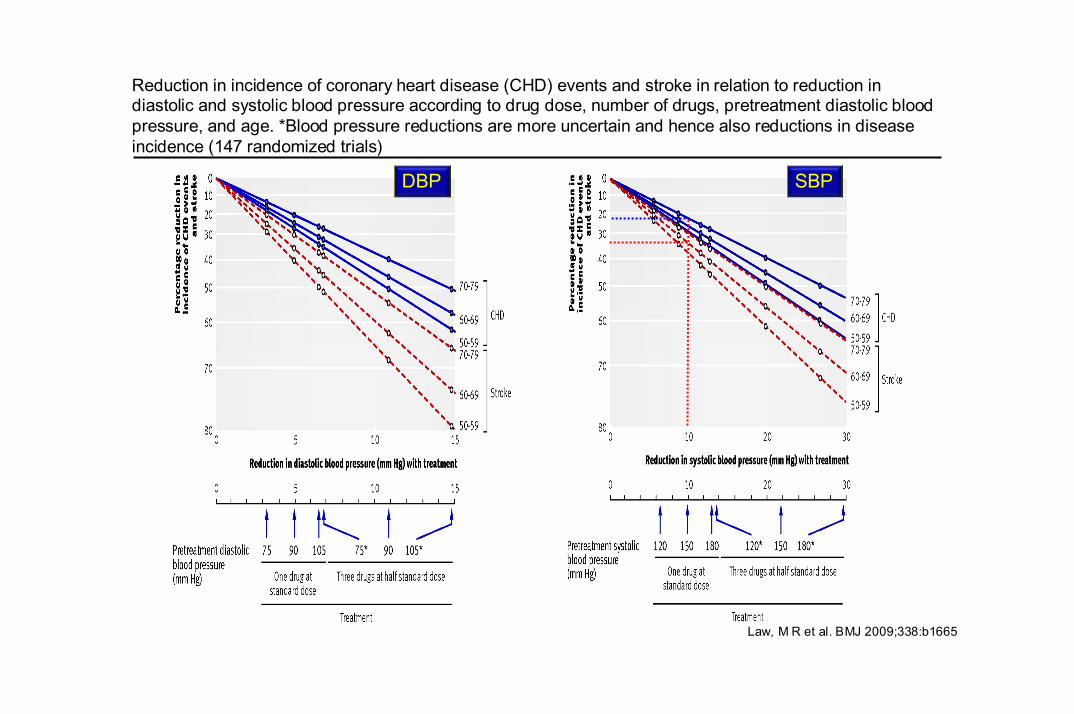
Law, M R et al. BMJ 2009;338:b1665
DBP SBP
Reduction in incidence of coronary heart disease (CHD) events and stroke in relation to reduction in diastolic and systolic blood pressure according to drug dose, number of drugs, pretreatment diastolic blood pressure, and age. *Blood pressure reductions are more uncertain and hence also reductions in disease incidence (147 randomized trials)
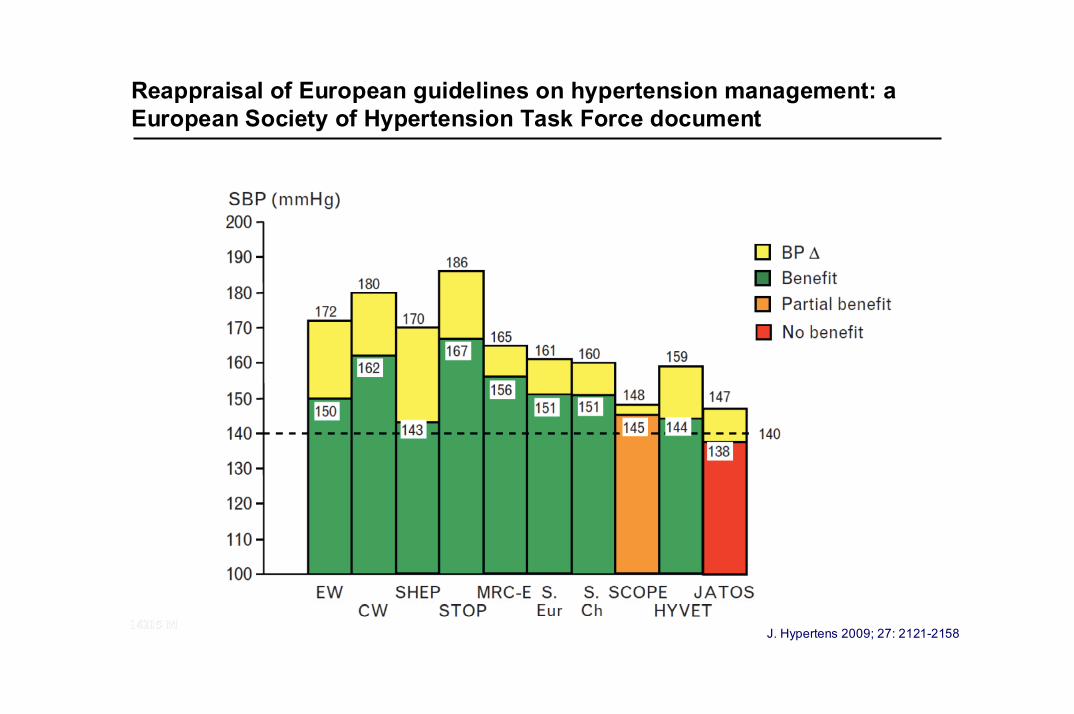
Reappraisal of European guidelines on hypertension management: aEuropean Society of Hypertension Task Force document
J. Hypertens 2009; 27: 2121-2158
In the elderly antihypertensive treatment is highly beneficial. Theproportional benefit in patients aged more than 65 years is no less than thatin younger patients.
In the elderly, outcome trials have only addressed patients with an entry SBP at least 160mmHg, and in no trial in which a benefit was shown achieved SBP averaged less than 140mmHg…. but common sense considerations suggest that also in the elderly drug treatment can be initiated when SBP is higher than 140mmHg, and that SBP can be brought to below 140mmHg, provided treatment is conducted with particular attention to adverse responses, potentially more frequent in the elderly.
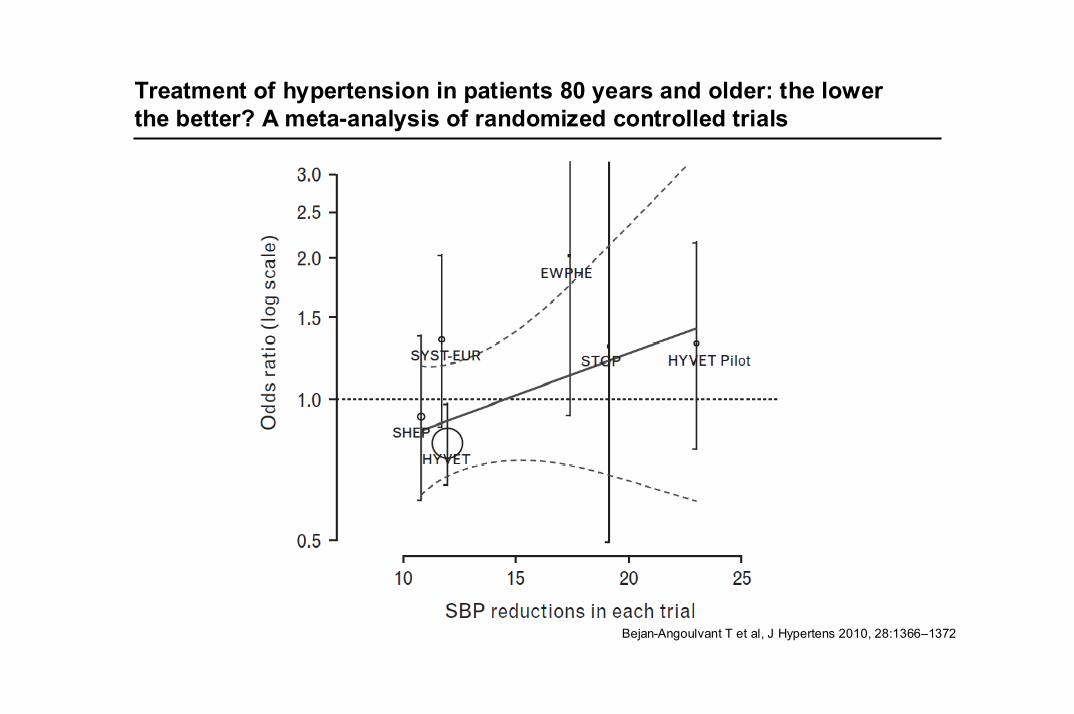
Treatment of hypertension in patients 80 years and older: the lowerthe better? A meta-analysis of randomized controlled trials
Bejan-Angoulvant T et al, J Hypertens 2010, 28:1366–1372
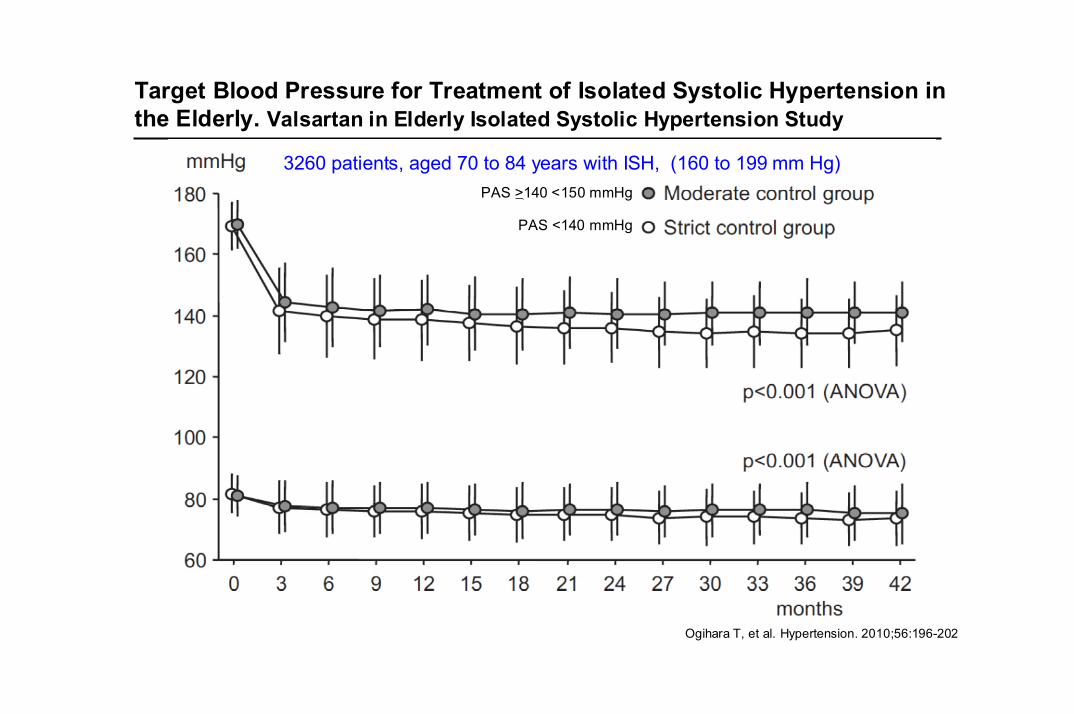
Target Blood Pressure for Treatment of Isolated Systolic Hypertension in the Elderly. Valsartan in Elderly Isolated Systolic Hypertension Study
Ogihara T, et al. Hypertension. 2010;56:196-202
3260 patients, aged 70 to 84 years with ISH, (160 to 199 mm Hg)PAS >140 <150 mmHg
PAS <140 mmHg
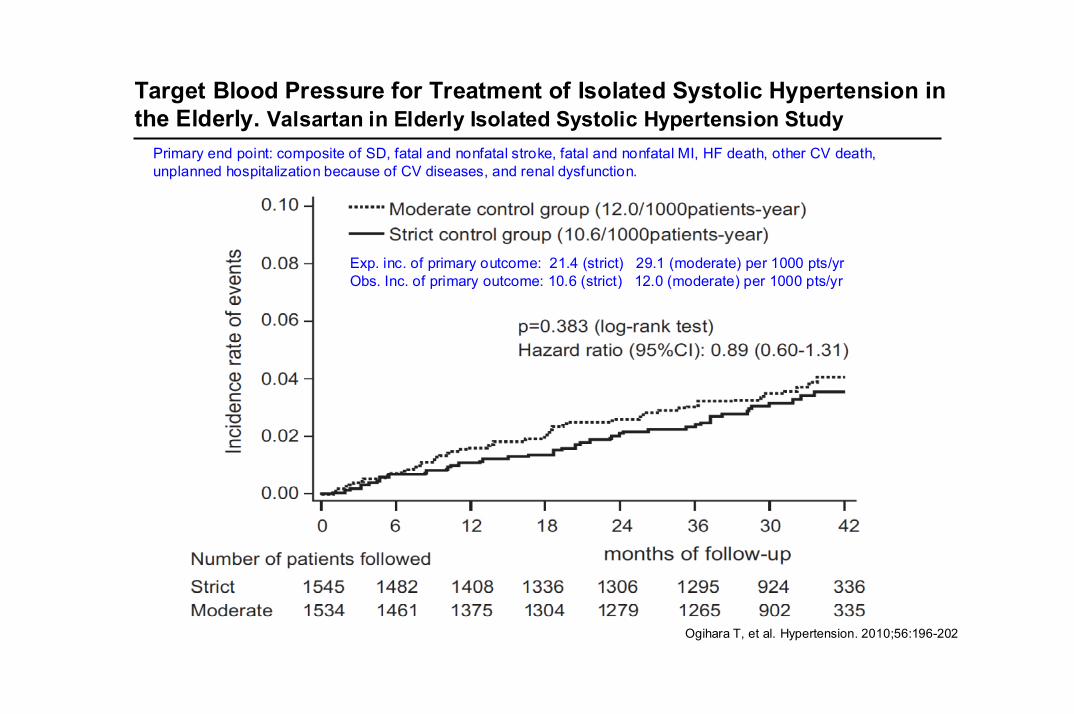
Target Blood Pressure for Treatment of Isolated Systolic Hypertension in the Elderly. Valsartan in Elderly Isolated Systolic Hypertension Study
Ogihara T, et al. Hypertension. 2010;56:196-202
Primary end point: composite of SD, fatal and nonfatal stroke, fatal and nonfatal MI, HF death, other CV death,unplanned hospitalization because of CV diseases, and renal dysfunction.
Exp. inc. of primary outcome: 21.4 (strict) 29.1 (moderate) per 1000 pts/yrObs. Inc. of primary outcome: 10.6 (strict) 12.0 (moderate) per 1000 pts/yr
14215 M14215 M
Does Evidence Support an Aggressive Systolic Blood Pressure Target in the Elderly?
Zanchetti A, et al. J. Hypertens 2009; 27: 923-934
(1) Not a single trial was specifically conducted in elderly hypertensive patients with systolic BP <160 mm Hg;
(2) In none of the available placebo-controlled trials did systolic BP fall below 140 mm Hg in the treated group
(3) In none of the available placebo-controlled trials was140 mm Hg the prespecified BP target of treatment.
14215 M14215 M
Reappraisal of European guidelines on hypertension management: aEuropean Society of Hypertension Task Force document
J. Hypertens 2009; 27: 2121-2158
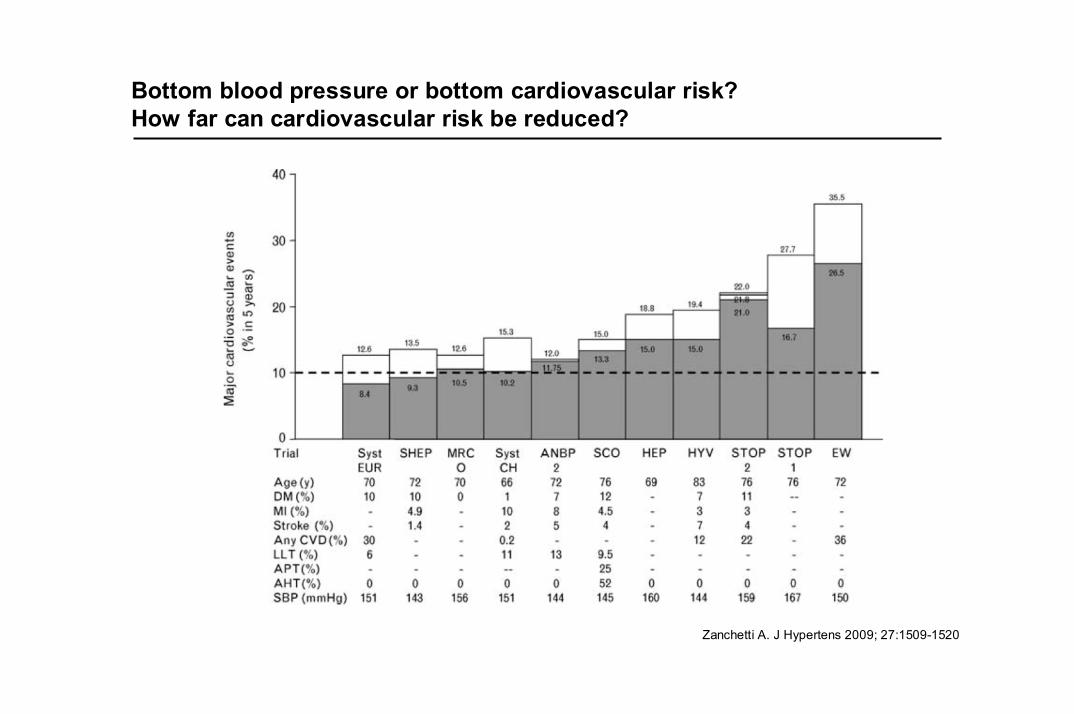
Bottom blood pressure or bottom cardiovascular risk?How far can cardiovascular risk be reduced?
Zanchetti A. J Hypertens 2009; 27:1509-1520
Elderly Hypertensive Patients
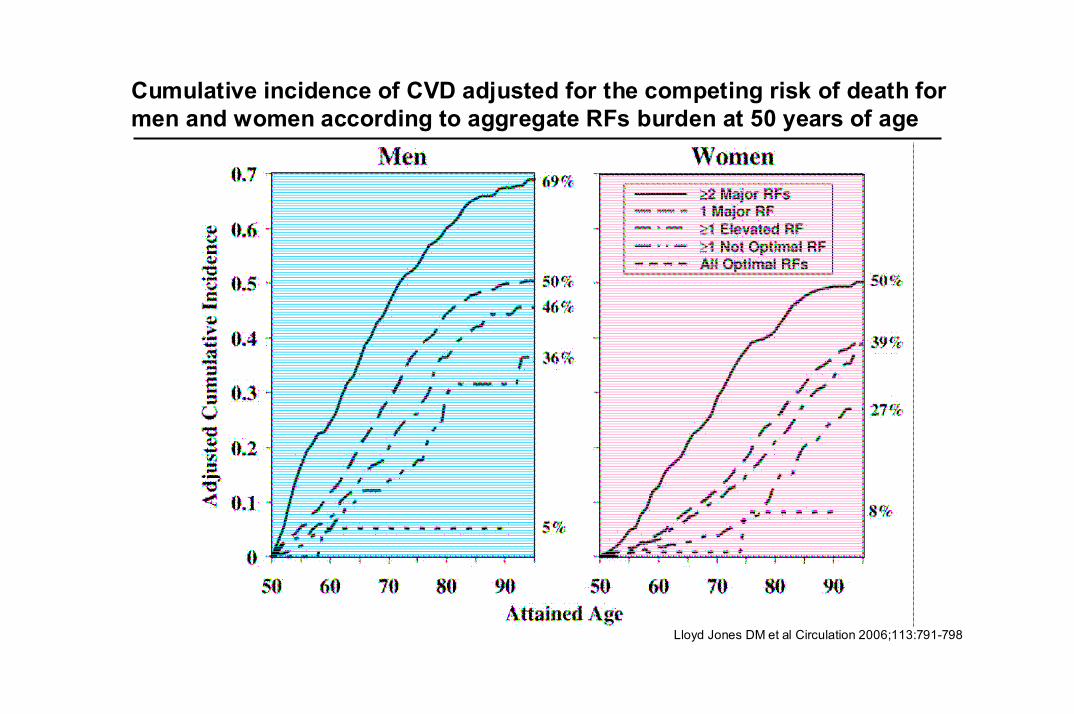
Cumulative incidence of CVD adjusted for the competing risk of death for men and women according to aggregate RFs burden at 50 years of age
Lloyd Jones DM et al Circulation 2006;113:791-798

Two-steps in hypertension induced vascular damage
Life: 0 10 20 30 40 50 60 70 80...years
Early step:Endothelial Abnormalities
Late step:Atherosclerotic plaque
Early step:Subclinical damage
Late step:Cardiovascular event

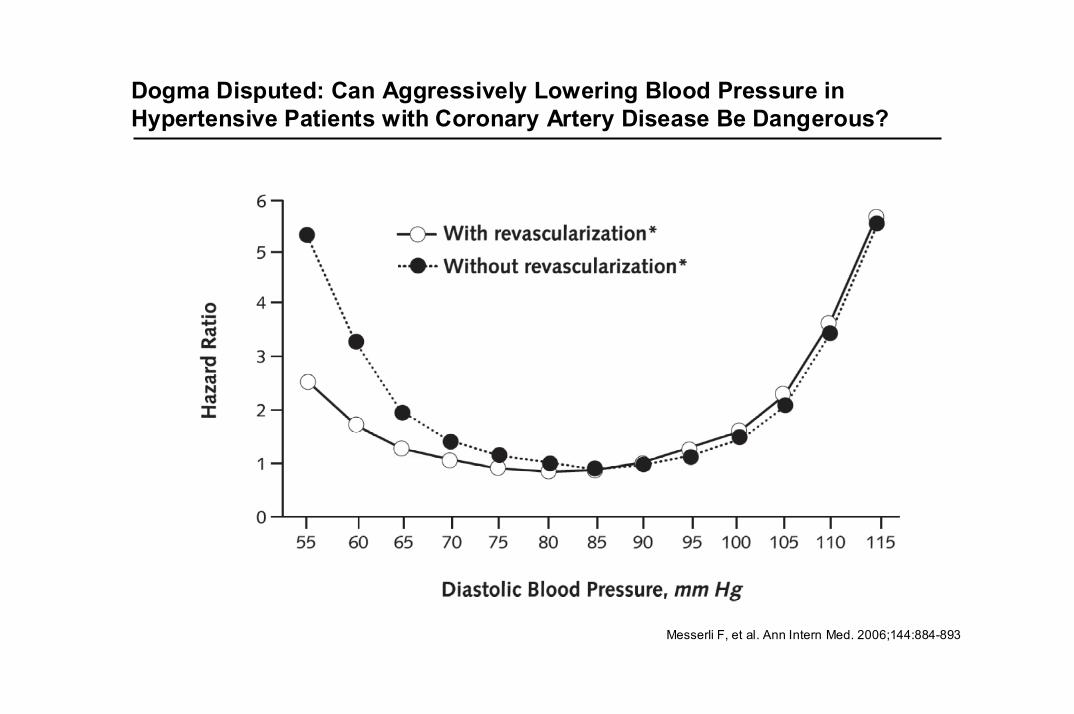
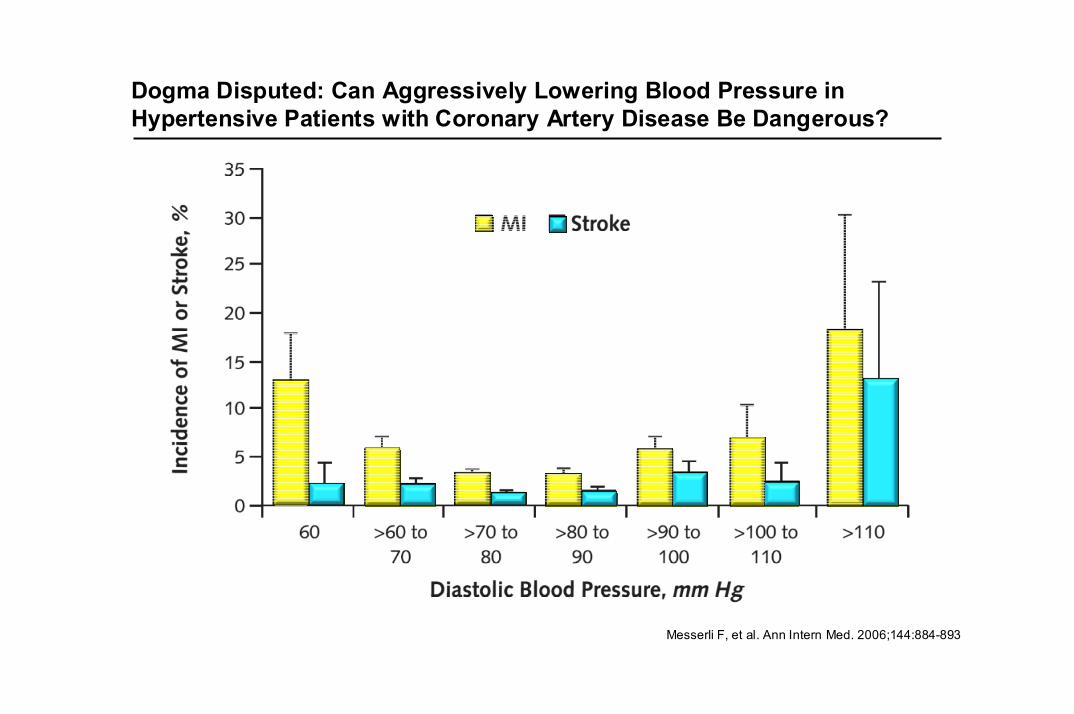
Dogma Disputed: Can Aggressively Lowering Blood Pressure inHypertensive Patients with Coronary Artery Disease Be Dangerous?
Messerli F, et al. Ann Intern Med. 2006;144:884-893
Dogma Disputed: Can Aggressively Lowering Blood Pressure inHypertensive Patients with Coronary Artery Disease Be Dangerous?
Messerli F, et al. Ann Intern Med. 2006;144:884-893
Dogma Disputed: Can Aggressively Lowering Blood Pressure inHypertensive Patients with Coronary Artery Disease Be Dangerous?
Messerli F, et al. Ann Intern Med. 2006;144:884-893
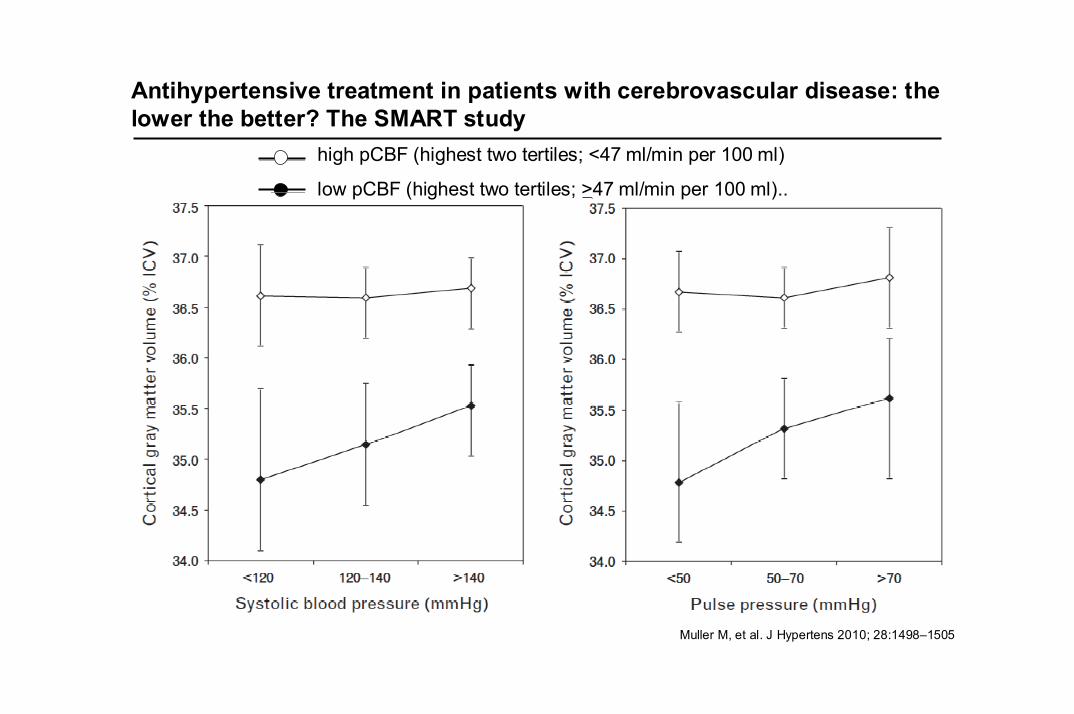
Antihypertensive treatment in patients with cerebrovascular disease: thelower the better? The SMART study
Muller M, et al. J Hypertens 2010; 28:1498–1505
high pCBF (highest two tertiles; <47 ml/min per 100 ml)
low pCBF (highest two tertiles; >47 ml/min per 100 ml)..
Reappraisal of European guidelines on hypertension management: aEuropean Society of Hypertension Task Force document
J. Hypertens 2009; 27: 2121-2158
In the elderly antihypertensive treatment is highly beneficial. Theproportional benefit in patients aged more than 65 years is no less than thatin younger patients.
In the elderly, outcome trials have only addressed patients with an entry SBP at least 160mmHg, and in no trial in which a benefit was shown achieved SBP averaged less than 140mmHg…. but common sense considerations suggest that also in the elderly drug treatment can be initiated when SBP is higher than 140mmHg, and that SBP can be brought to below 140mmHg, provided treatment is conducted with particular attention to adverse responses, potentially more frequent in the elderly.
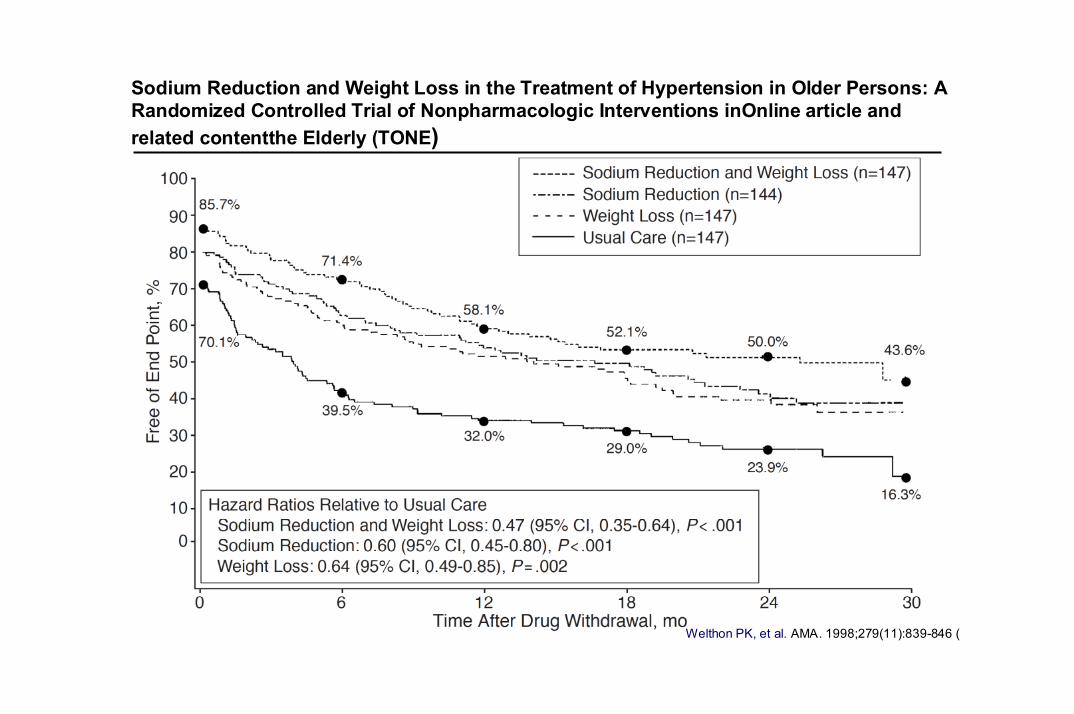
Sodium Reduction and Weight Loss in the Treatment of Hypertension in Older Persons: ARandomized Controlled Trial of Nonpharmacologic Interventions inOnline article andrelated contentthe Elderly (TONE)
Welthon PK, et al. AMA. 1998;279(11):839-846 (
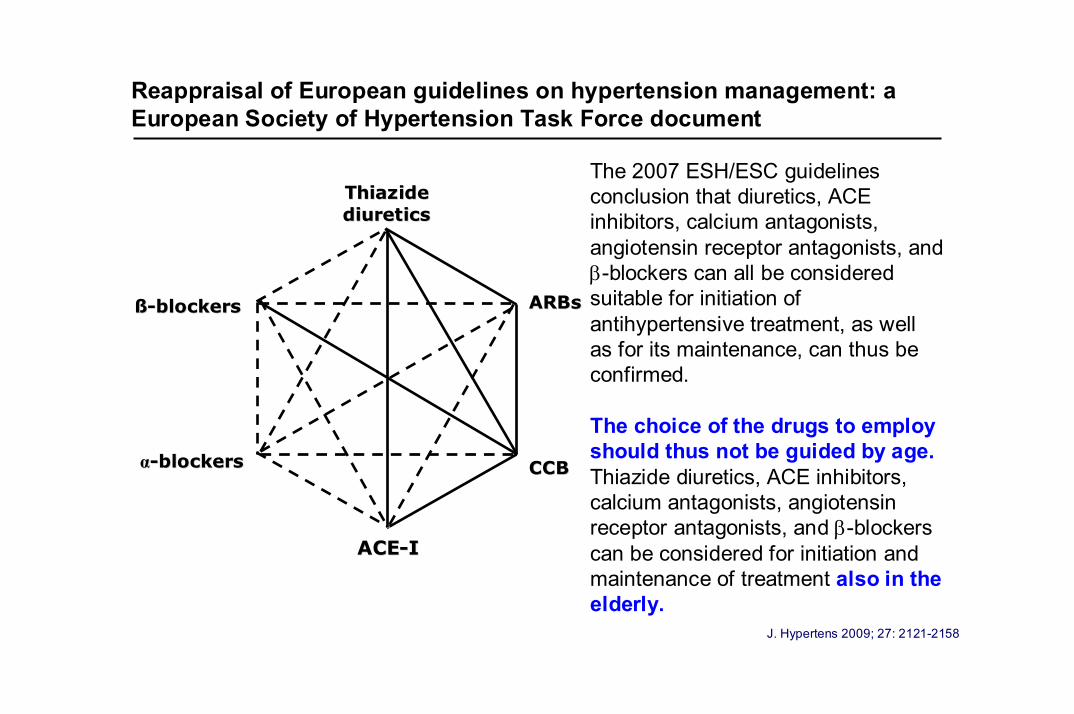
The 2007 ESH/ESC guidelines conclusion that diuretics, ACEinhibitors, calcium antagonists,angiotensin receptor antagonists, and β-blockers can all be considered suitable for initiation ofantihypertensive treatment, as well as for its maintenance, can thus be confirmed.
The choice of the drugs to employ should thus not be guided by age.Thiazide diuretics, ACE inhibitors,calcium antagonists, angiotensin receptor antagonists, and β-blockerscan be considered for initiation andmaintenance of treatment also in theelderly.
J. Hypertens 2009; 27: 2121-2158
Reappraisal of European guidelines on hypertension management: aEuropean Society of Hypertension Task Force document
Thiazide Thiazide diuretics diuretics
ACEACE--II
CCBCCB
ARBsARBsßß--blockersblockers
αα--blockersblockers
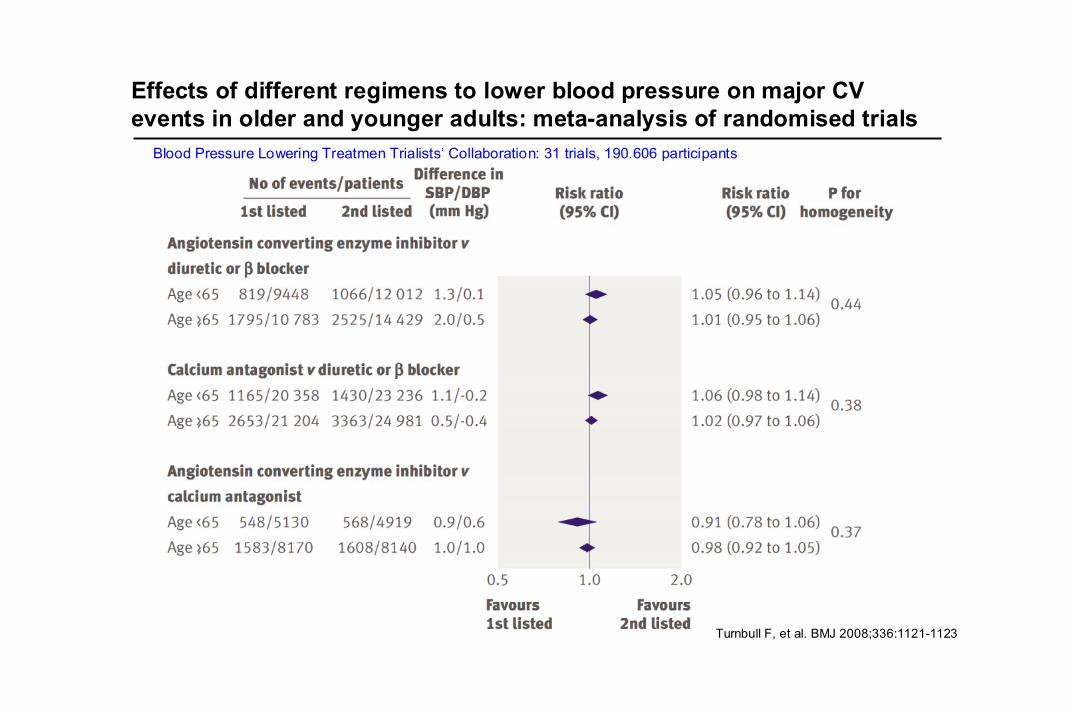
Effects of different regimens to lower blood pressure on major CVevents in older and younger adults: meta-analysis of randomised trials
Turnbull F, et al. BMJ 2008;336:1121-1123
Blood Pressure Lowering Treatmen Trialists’ Collaboration: 31 trials, 190.606 participants
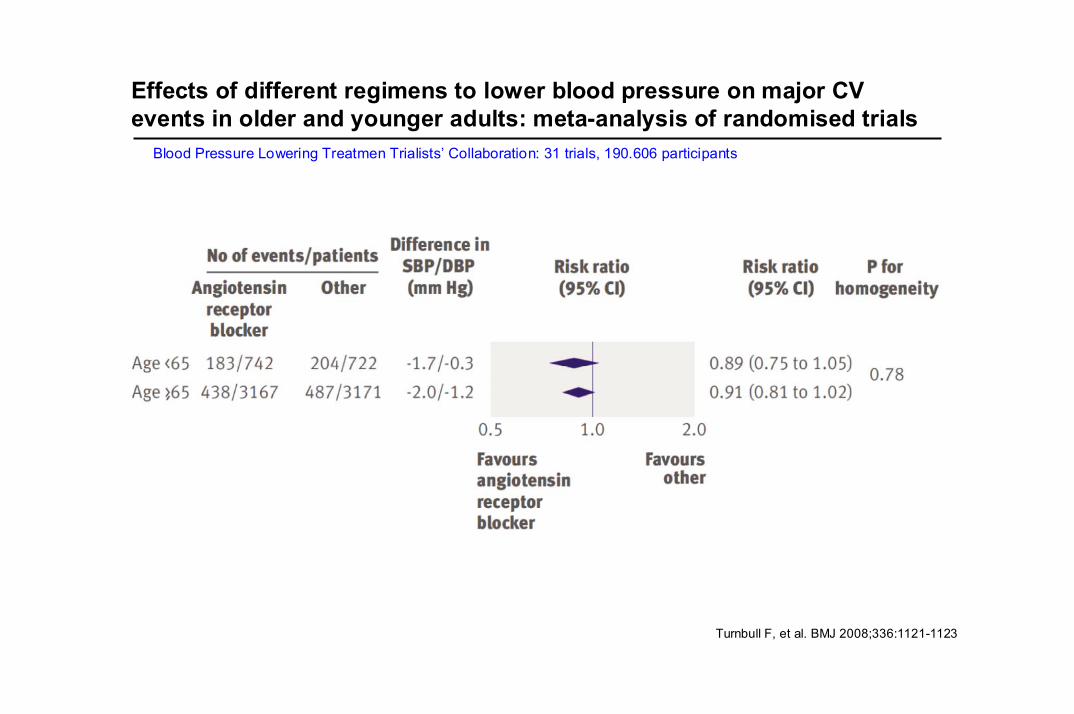
Effects of different regimens to lower blood pressure on major CVevents in older and younger adults: meta-analysis of randomised trials
Turnbull F, et al. BMJ 2008;336:1121-1123
Blood Pressure Lowering Treatmen Trialists’ Collaboration: 31 trials, 190.606 participants
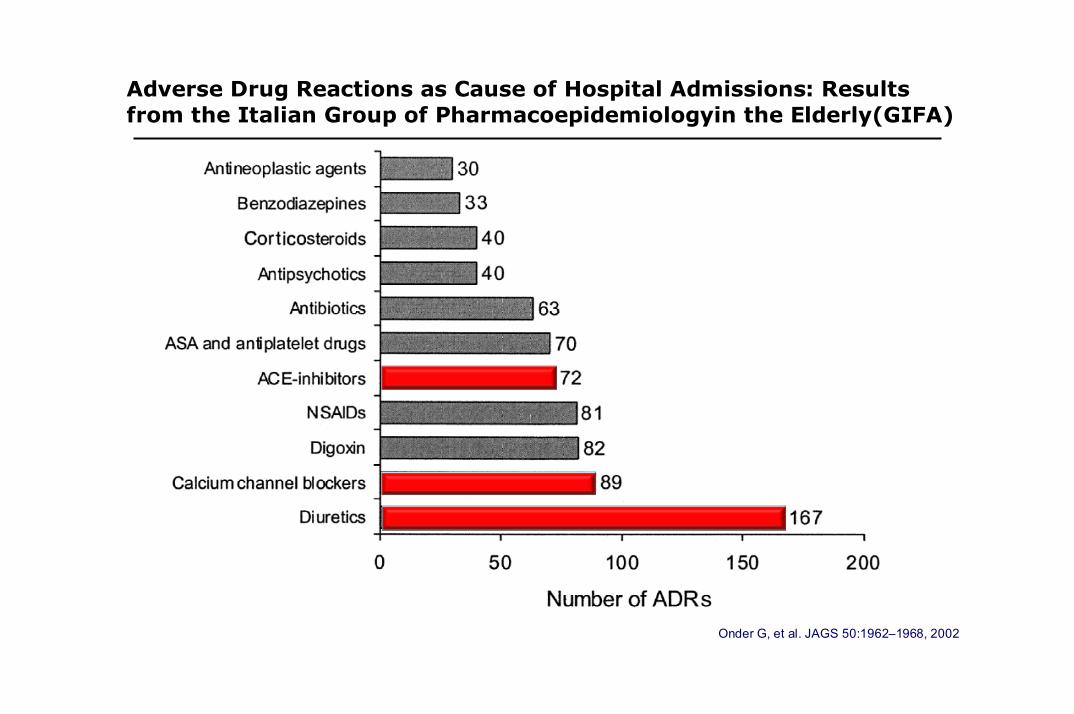
Onder G, et al. JAGS 50:1962–1968, 2002
Adverse Drug Reactions as Cause of Hospital Admissions: Results from the Italian Group of Pharmacoepidemiologyin the Elderly(GIFA)
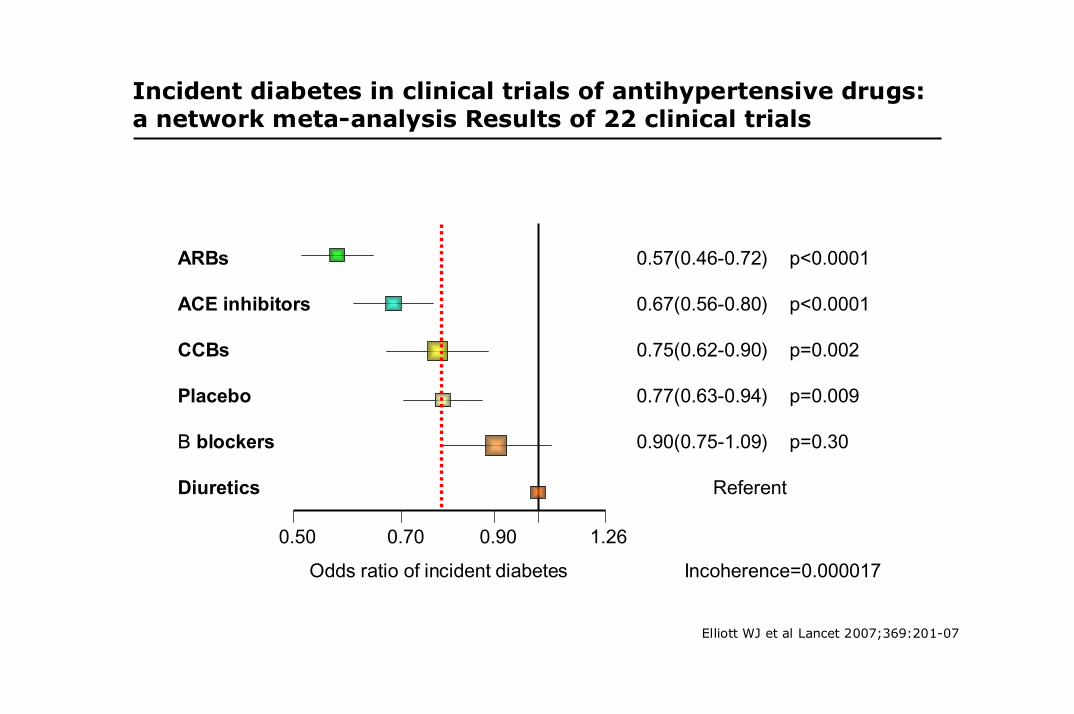
ARBs 0.57(0.46-0.72) p<0.0001
ACE inhibitors 0.67(0.56-0.80) p<0.0001
CCBs 0.75(0.62-0.90) p=0.002
Placebo 0.77(0.63-0.94) p=0.009
Β blockers 0.90(0.75-1.09) p=0.30
Diuretics Referent
0.50 0.70 0.90 1.26
Odds ratio of incident diabetes Incoherence=0.000017
Elliott WJ et al Lancet 2007;369:201-07
Incident diabetes in clinical trials of antihypertensive drugs: a network meta-analysis Results of 22 clinical trials
Diff
eren
ces
inH
azar
d R
atio
s(H
R)
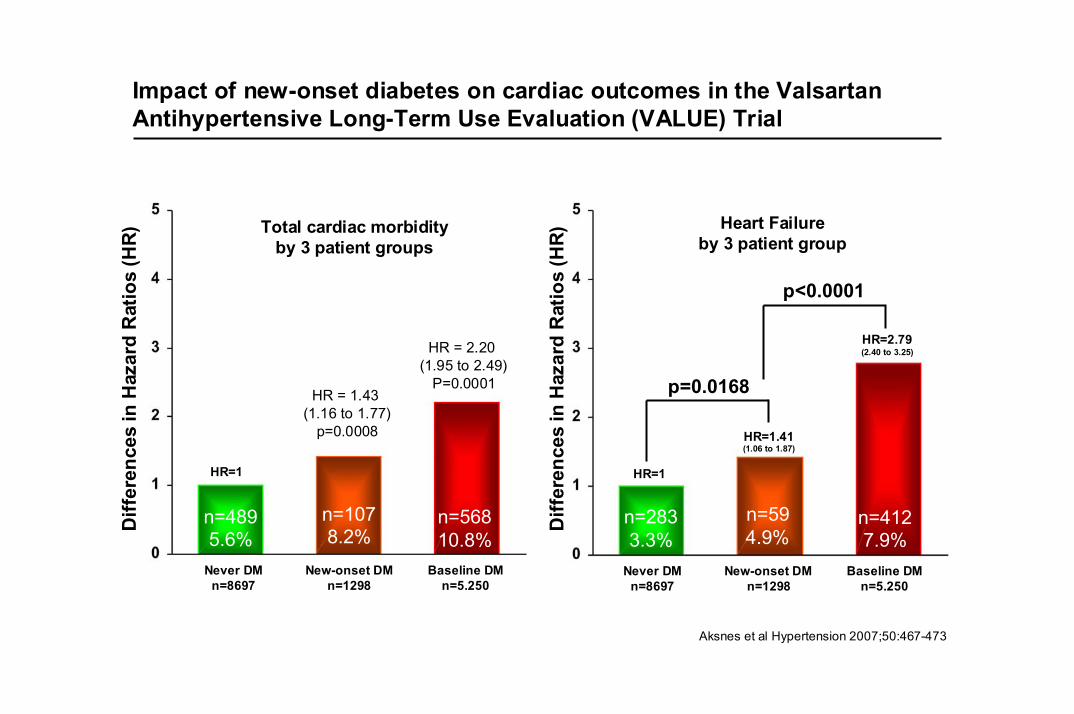
p=0.0168
HR=1
Aksnes et al Hypertension 2007;50:467-473
Never DMn=8697
New-onset DMn=1298
Baseline DMn=5.250
Heart Failureby 3 patient group
HR=1.41(1.06 to 1.87)
HR=2.79(2.40 to 3.25)
Total cardiac morbidityby 3 patient groups
p<0.0001
HR = 1.43 (1.16 to 1.77)
p=0.0008
HR = 2.20 (1.95 to 2.49)
P=0.0001
HR=1
Diff
eren
ces
inH
azar
d R
atio
s(H
R)
n=2833.3%
n=594.9%
n=4127.9%
Never DMn=8697
New-onset DMn=1298
Baseline DMn=5.250
n=4895.6%
n=1078.2%
n=56810.8%
Impact of new-onset diabetes on cardiac outcomes in the Valsartan Antihypertensive Long-Term Use Evaluation (VALUE) Trial
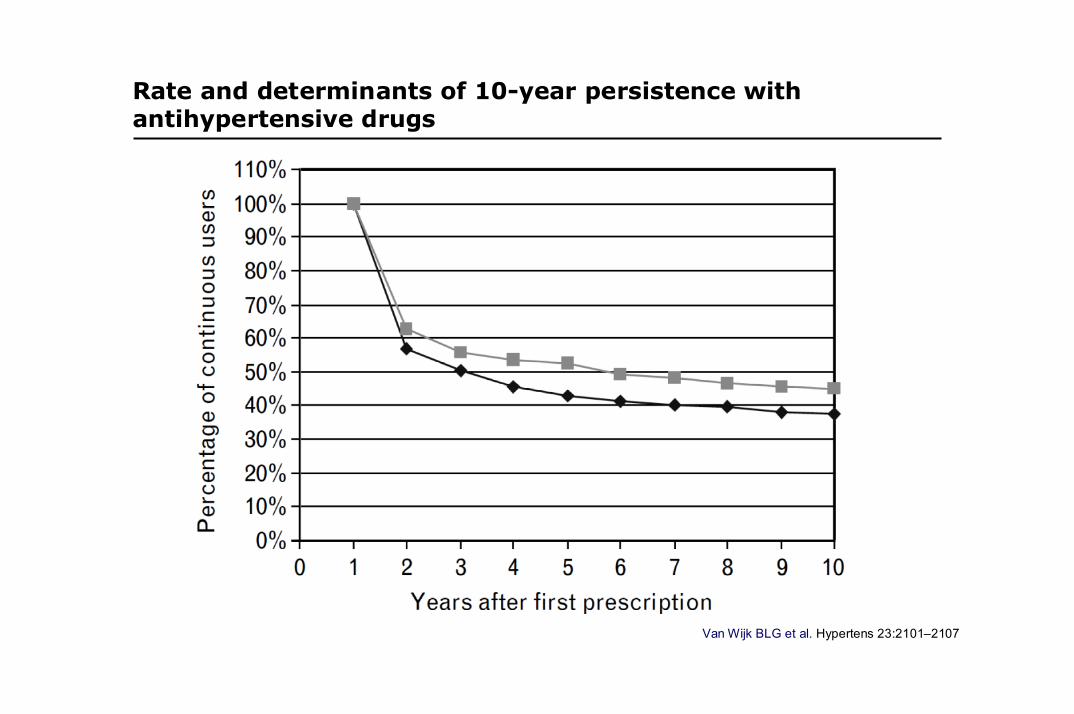
Van Wijk BLG et al. Hypertens 23:2101–2107
Rate and determinants of 10-year persistence withantihypertensive drugs
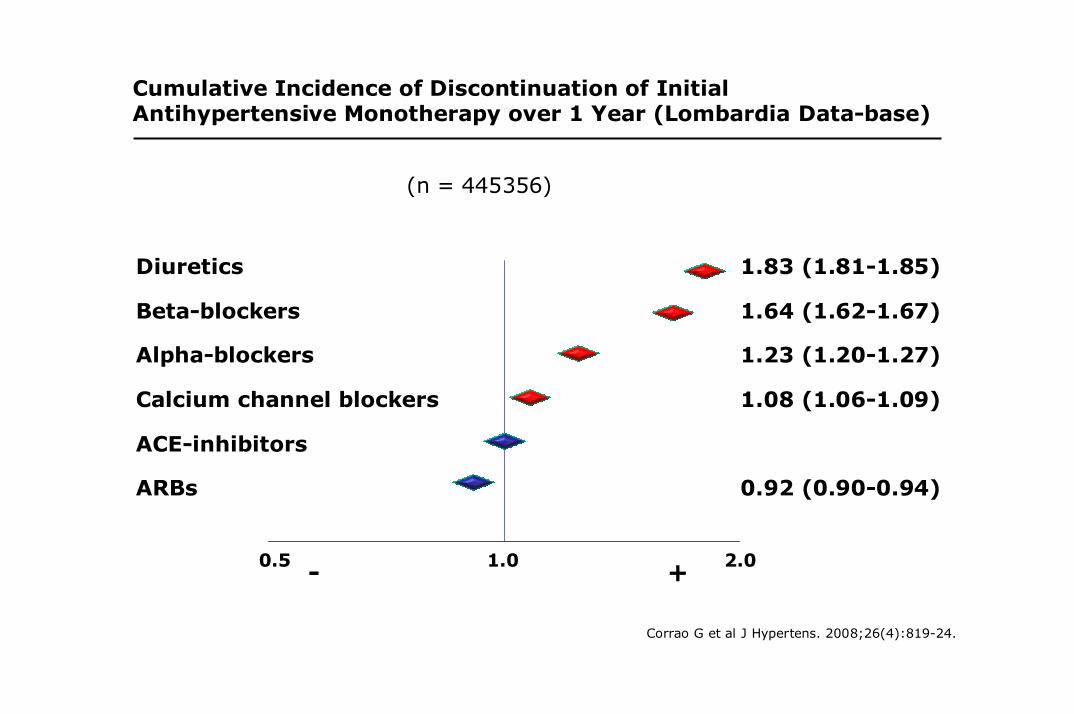
0.5 1.0 2.0
Diuretics
Beta-blockers
Alpha-blockers
Calcium channel blockers
ACE-inhibitors
ARBs
1.83 (1.81-1.85)
1.64 (1.62-1.67)
1.23 (1.20-1.27)
1.08 (1.06-1.09)
0.92 (0.90-0.94)
- +
(n = 445356)
Corrao G et al J Hypertens. 2008;26(4):819-24.
Cumulative Incidence of Discontinuation of Initial Antihypertensive Monotherapy over 1 Year (Lombardia Data-base)
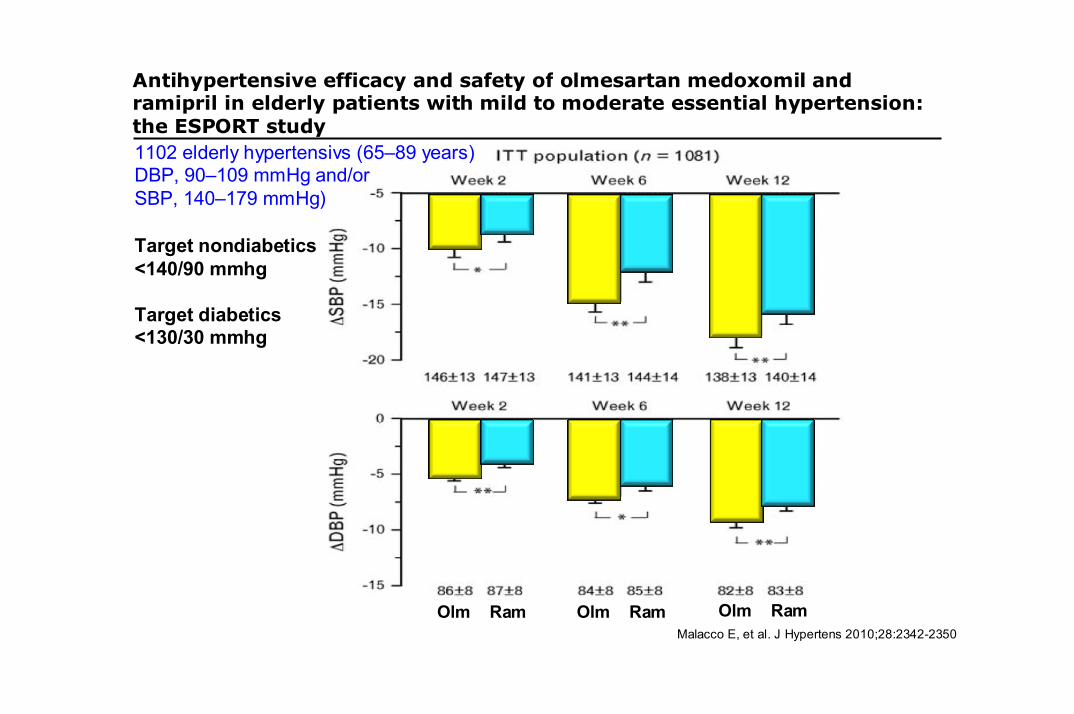
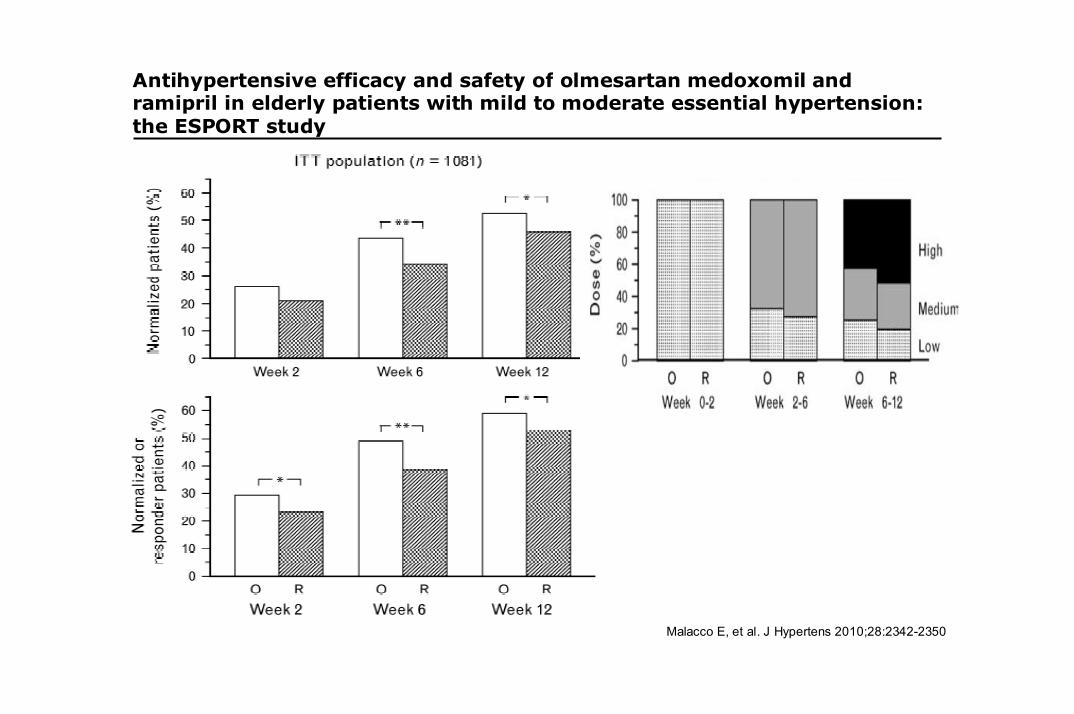
Antihypertensive efficacy and safety of olmesartan medoxomil andramipril in elderly patients with mild to moderate essential hypertension: the ESPORT study
Malacco E, et al. J Hypertens 2010;28:2342-2350
1102 elderly hypertensivs (65–89 years)DBP, 90–109 mmHg and/or SBP, 140–179 mmHg)
Target nondiabetics<140/90 mmhg
Target diabetics<130/30 mmhg
Olm Ram Olm Ram Olm Ram
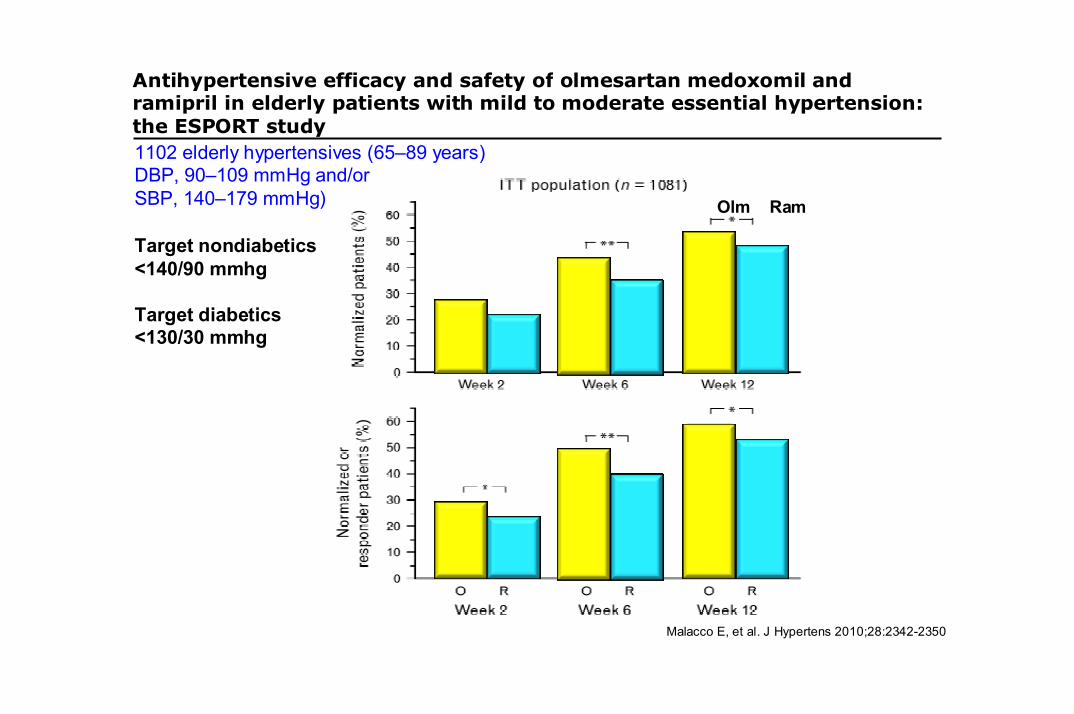
Antihypertensive efficacy and safety of olmesartan medoxomil andramipril in elderly patients with mild to moderate essential hypertension: the ESPORT study
Malacco E, et al. J Hypertens 2010;28:2342-2350
1102 elderly hypertensives (65–89 years)DBP, 90–109 mmHg and/or SBP, 140–179 mmHg)
Target nondiabetics<140/90 mmhg
Target diabetics<130/30 mmhg
Olm Ram
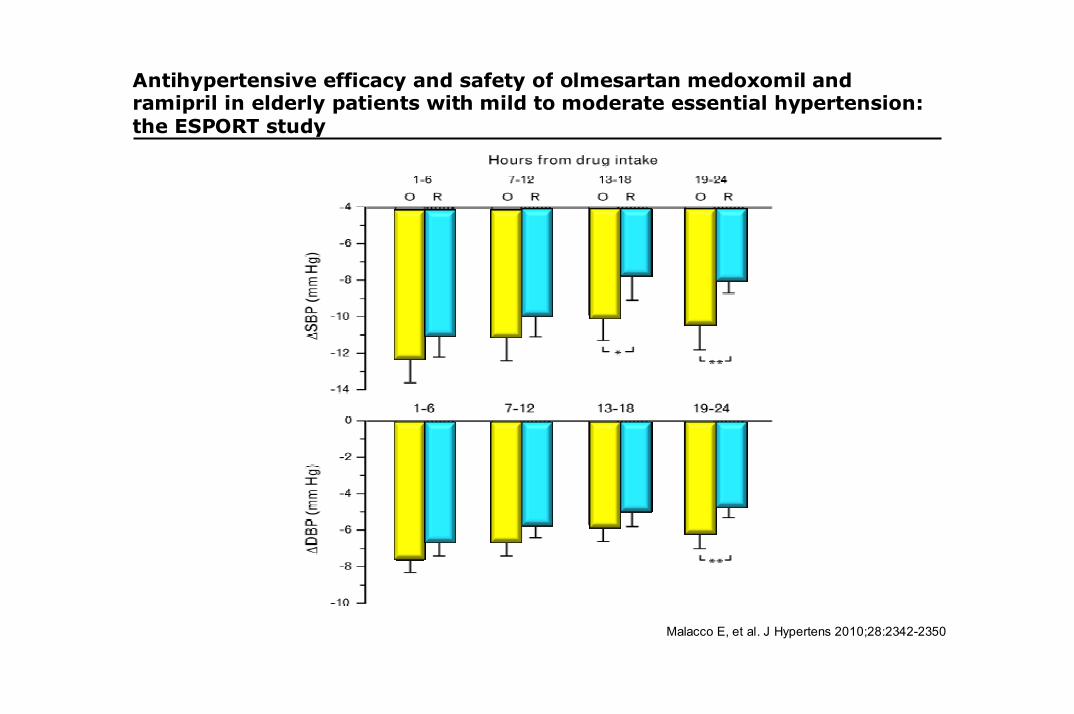
Antihypertensive efficacy and safety of olmesartan medoxomil andramipril in elderly patients with mild to moderate essential hypertension: the ESPORT study
Malacco E, et al. J Hypertens 2010;28:2342-2350
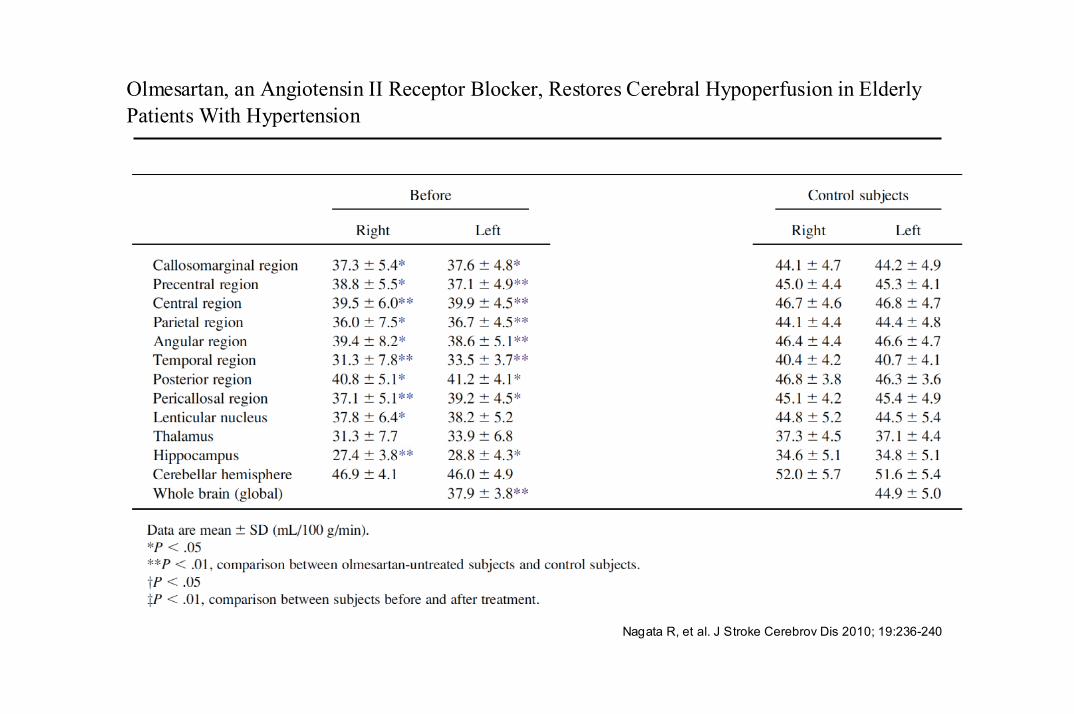
Olmesartan, an Angiotensin II Receptor Blocker, Restores Cerebral Hypoperfusion in Elderly Patients With Hypertension
Nagata R, et al. J Stroke Cerebrov Dis 2010; 19:236-240
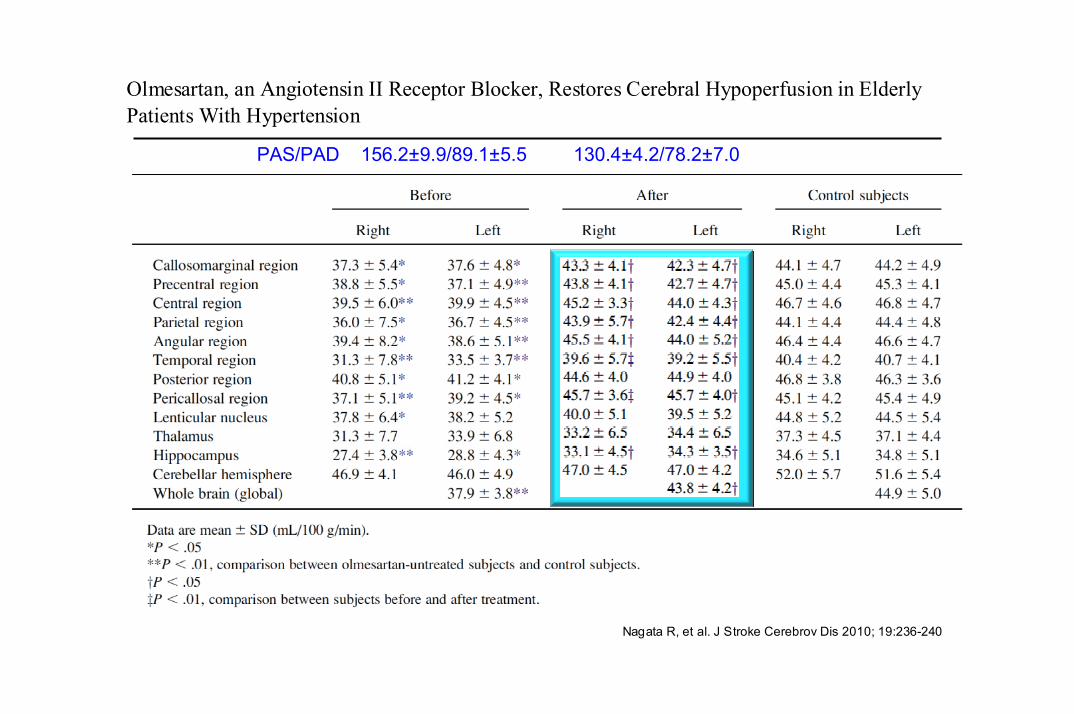
Olmesartan, an Angiotensin II Receptor Blocker, Restores Cerebral Hypoperfusion in Elderly Patients With Hypertension
Nagata R, et al. J Stroke Cerebrov Dis 2010; 19:236-240
PAS/PAD 156.2±9.9/89.1±5.5 130.4±4.2/78.2±7.0
Death
Terminal HFDementia
ESRD
Endothelialdysfunction and
activation
Micro-albuminuria
CHFSecondary stroke
Nefrotic proteinuria
Macro-proteinuria
MI and Stroke
ATS, IVS
LV dilationCognitive
impairment
LV remodelling
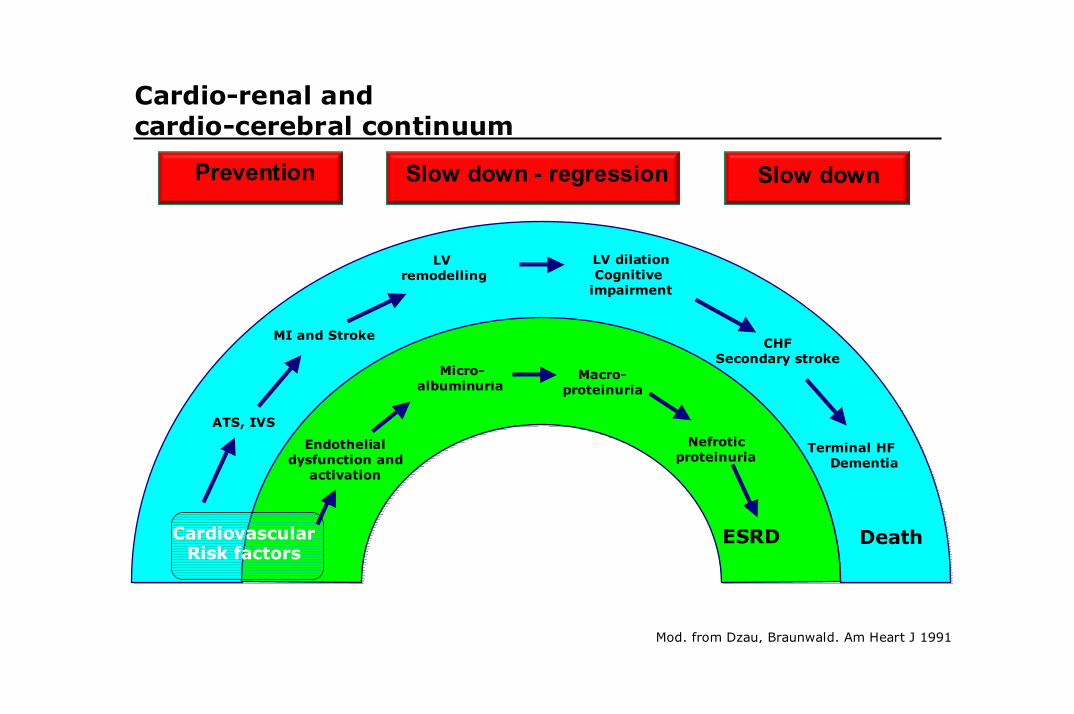
Cardio-renal and cardio-cerebral continuum
CardiovascularRisk factors
Mod. from Dzau, Braunwald. Am Heart J 1991
Slow downSlow down - regressionPrevention
Antihypertensive efficacy and safety of olmesartan medoxomil andramipril in elderly patients with mild to moderate essential hypertension: the ESPORT study
Malacco E, et al. J Hypertens 2010;28:2342-2350
J. Hypertens 2009; 27: 2121-2158
olivus
J. Hypertens 2009; 27: 2121-2158
IPOTENSIONE E CADUTE
J. Hypertens 2009; 27: 2121-2158
J. Hypertens 2009; 27: 2121-2158
OLIVUS
Valish ha fallito
VEDI GILL NEJM 2010 SU FRAGILITA
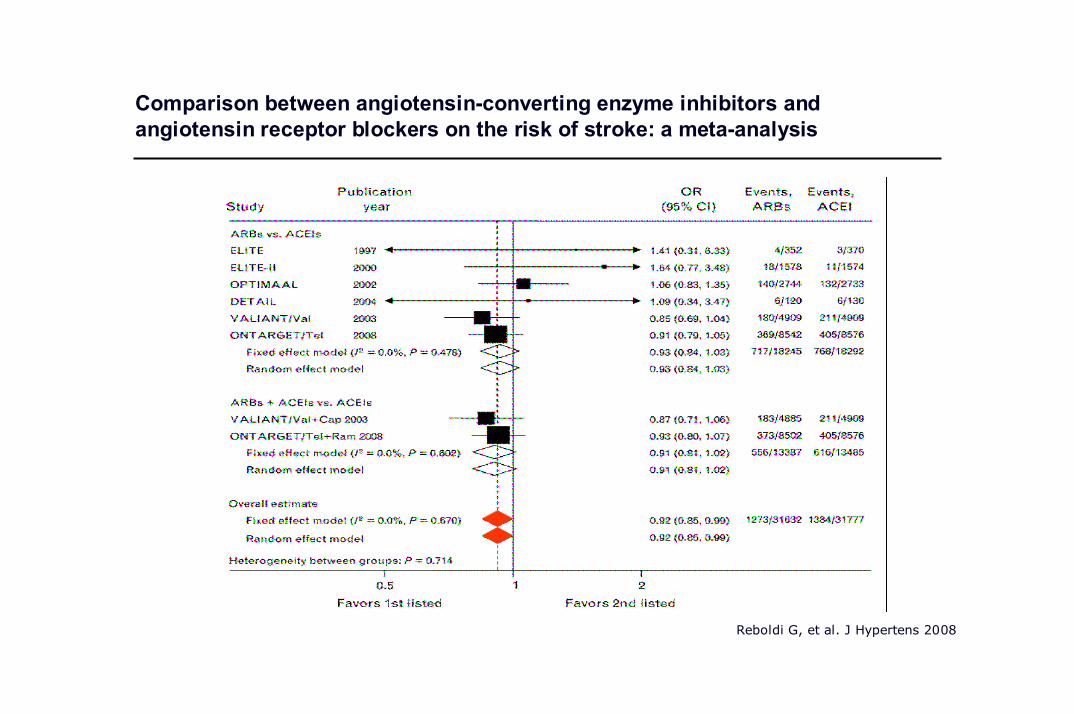
Comparison between angiotensin-converting enzyme inhibitors andangiotensin receptor blockers on the risk of stroke: a meta-analysis
Reboldi G, et al. J Hypertens 2008
J. Hypertens 2009; 27: 2121-2158
MAZZAGLIA
E STAY ON TREATMENT
E noi di AQ





























