Embed Size (px)
Citation preview
©2018 MFMER | slide-1
Get aHEAD of the ACHE: Monoclonal Antibodies in Migraine Prevention
Amanda Janisch, PharmDPGY2 Ambulatory Care Pharmacy ResidentMCHS SWMN, Mankato, MN

©2018 MFMER | slide-2
Disclosures
• No financial interest or conflicts of interest to disclose
• Discussion of off-label use for the following in migraine prevention: metoprolol, atenolol, amitriptyline, venlafaxine, lisinopril, candesartan, carbamazepine, clonidine, and guanfacine

©2018 MFMER | slide-3
Objectives
• Explain the pathophysiology and epidemiology of migraines
• Describe treatment guidelines for management of migraines
• Discuss novel monoclonal antibodies for migraine prevention

©2018 MFMER | slide-4
Definitions
• Headache- head pain without neurologic symptoms
• Migraine- head pain with neurologic symptoms such as aura, nausea, vomiting, aversion to light, sound, or smell
• Episodic migraine (EM)- headache ≤14 days/month
• Chronic migraine (CM)- headache >15 days/month for at least 3 months, with ≥ 8 migraine days/month
Katsarava Z. Curr Pain Headache Rep. 2012.

©2018 MFMER | slide-5
Epidemiology• Migraine affects ~14% of the population
• More common in women• Highest prevalence in age range of 40 to 49
• Associated cost >$13 billion• Loss in productivity
• Studies suggest that ~30% of patients with migraine need preventative therapy
• 3-13% use preventative therapy
AAN/AHS. Am Fam Physician. 2013.Katsarava Z. Curr Pain Headache Rep. 2012.

©2018 MFMER | slide-6
Pathophysiology• COMPLEX
• Activation & sensitization of trigeminovascularpathways
• Dysregulation of sensory processing leading to neurologic symptoms
• Associations• Comorbidities: depression, anxiety, chronic pain
disorders• Medication over-use• Environmental factors: caffeine use, stress
Katsarava Z. Curr Pain Headache Rep. 2012.

©2018 MFMER | slide-7
TRUE or FALSE
Chronic Migraine (CM) occurs more commonly than Episodic Migraine (EM).

©2018 MFMER | slide-8
a. Trueb. False

©2018 MFMER | slide-9
Patient Case• MK a 42 year old female, is diagnosed with EM.• PMH: hypertension and s/p kidney excision
(donor)• She currently takes sumatriptan 50 mg as needed
and is using more frequently (~8x/month) • Other medications include: losartan and oral
contraceptive

©2018 MFMER | slide-10
Acute Treatment• Non-Steroidal Anti-inflammatory (NSAIDs)
• 1st line for mild-moderate migraines• Triptans
• 1st line for moderate-severe migraines• Dopamine antagonist antiemetics
• 2nd line for migraine treatment• Refractory Migraines
• May use parenteral dihydroergotamine, magnesium sulfate, valproate, and opioids
Mayans L, et al. Am Fam Physician. 2018.

©2018 MFMER | slide-11
Preventative Therapy• Consider when:
• ≥ 2 migraine days per month with disability lasting ≥ 3 days/month
• Acute treatment failure, adverse effects, or contraindication
• Use of abortive therapy ≥ 2 times/week• Patient preference and cost
• Goals:• Reduce frequency, intensity, and duration
Modi S, et al. Am Fam Physician. 2006.

©2018 MFMER | slide-12
FDA Approved for Migraine Prevention
Level of evidence A: ≥2 Class I trials
Silberstein SD,et al. Neurology. 2012.
Medication Dosage Rangedivalproex (Depakote®) IR: 250 mg twice daily up to 1000 mg/day
ER: 500 mg-1000 mg/day
topiramate (Topamax®) IR: 25 mg-100 mg in two divided dosesER: 25 mg-100 mg once daily
propranolol (Inderal®) IR: 80 mg/day divided every 6-8 hours, maximum of 160-240 mg/dayER: 80 mg once daily initially, Effective range 160-240 mg once daily
OnabotulinumtoxinA(Botox®)
5 units/0.1 mL per site with total dose of 155 units divided between 31 IM sites every 12 weeks.

©2018 MFMER | slide-13
Off-label use for Migraine Prevention
Medication Dosage Range Level of Evidence
metoprolol (Lopressor®, Toprol XL®)
n/a A
atenolol (Tenormin®) n/a B
amitriptyline (Elavil®) 10 mg-150 mg daily B
venlafaxine (Effexor®) ER: 37.5 mg- 150 mg daily B
Silberstein SD,et al. Neurology. 2012.Micromedex Database.

©2018 MFMER | slide-14
Off-label use for Migraine Prevention
Medication Level of Evidence
lisinopril (Zestril®, Prinivil®) C
candesartan (Atacand®) C
carbamazepine (Tegretol®) C
clonidine (Catapres®) C
guanfacine (Tenex®, Intuniv®) C
Silberstein SD,et al. Neurology. 2012.

©2018 MFMER | slide-15
NOT Recommended or Effective for Migraine Prevention
• lamotrigine (Lamictal®)• clomipramine (Anafranil®)• clonazepam (Klonopin®)• nabumetone (Relafen®)• oxcarbazepine (Trileptal®)• telmisartan (Micardis®)
Silberstein SD,et al. Neurology. 2012.

©2018 MFMER | slide-16
Drug Induced Headache
Mayo Clinic. 2018.
• Overuse of acute headache medications (>10 days/month)
• Butalbital products, acetaminophen, caffeine, NSAIDs, codeine, triptans
• Stimulants• Hormone therapy• Nitrates

©2018 MFMER | slide-17
Patient CaseWhich of the following products should NOT be recommended for MK as a first-line agent for migraine prevention?
©2018 MFMER | slide-18
a. topiramateb. butalbital/acetaminophen/caffeinec. propranolold. divalproex
©2018 MFMER | slide-19
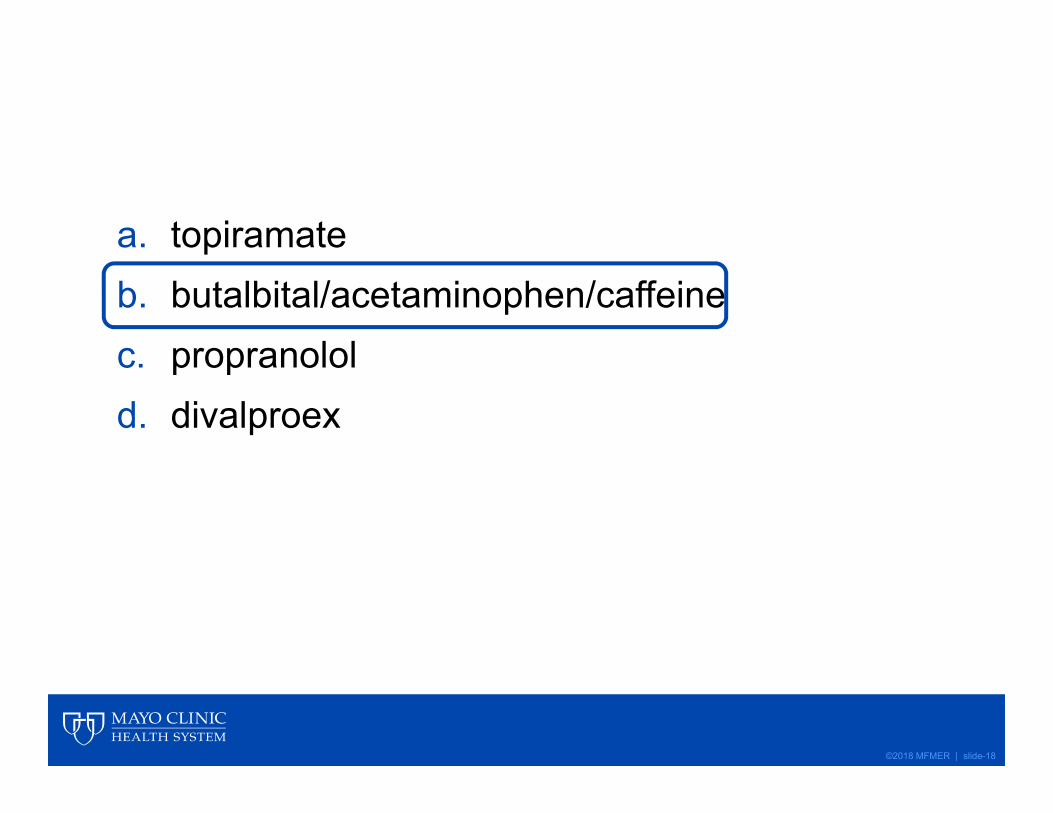
Erenumab-aooe (Aimovig®)
Lauritsen CG, Silberstein SD. Pract Neurology. 2016.DailyMedGoodRx
Approval• Approved 5/17/2018 for EM and CM prevention
Mechanism
• Monoclonal antibody• Binds to calcitonin gene-related peptide (CGRP)
receptor
Product
• 70 mg monthly Sub-Q injection• Cost: $600- 700/carton of two SureClick®
Autoinjectors (8 week supply)

©2018 MFMER | slide-20
Erenumab-aooe Properties
• 4 letter abbreviation- naming convention for biologic agents
• “Fully Human” monoclonal antibody• ~90% human derived, ~10% murine
• IgG2 type antibody

©2018 MFMER | slide-21
Calcitonin Gene-Related Peptide (CGRP) Pathway
Edvinsson L. Headache. 2018.
• CGRP serum levels increase during migraine attack
• Trigeminal nerve stimulation increases CGRP
• CGRP concentration correlates to headache intensity

©2018 MFMER | slide-22
Efficacy and safety of erenumab (AMG334) in chronic migraine patients with prior preventive treatment failure: A subgroup analysis of a randomized, double-blind, placebo-controlled study
Ashina M, Tepper S, Brandes JL, et al. Cephalalgia. 2018.

©2018 MFMER | slide-23
Objectives• Primary Endpoint: Change from baseline in
monthly migraine days (MMD)
• Secondary Endpoints: • Achievement of ≥50% and ≥75% reduction from
baseline in MMD
• Change from baseline in monthly acute migraine-specific medication days (MSMD) based on use of acute medications (triptans/ergots)
Ashina M., et al. Cephalalgia. 2018.

©2018 MFMER | slide-24
Study Methods• Multicenter, randomized, double-blind, placebo-
controlled, 12-week, parallel-group study• Subgroup analysis in CM
• placebo• erenumab 70 mg monthly• erenumab 140 mg monthly
Ashina M., et al. Cephalalgia. 2018.

©2018 MFMER | slide-25
Enrollment
Ashina M., et al. Cephalalgia. 2018.
Inclusion
Adult patients with CM (≥ 15 headache days/month; ≥8 migraine days/month)
Exclusion
No therapeutic response to >3 preventative treatment categories

©2018 MFMER | slide-26
Subgroup Baseline Characteristics
Characteristic Placebon= 286
Erenumab70 mgn= 191
Erenumab140 mgn= 190
Age, years 41-42.9 40.7-42.9 41.4-44.2
Female, % 79 80-90 78-89
MMD 17.5-18.5 17.1-18.2 17.2-18.8
Monthly MSMD 6.3-11.4 6.9-10.5 6.2-12.4
Ashina M., et al. Cephalalgia. 2018.MMD- Monthly Migraine DaysMSMD- Migraine-Specific Medication Days

©2018 MFMER | slide-27
ResultsNo Prior Treatment
≥1 Prior Treatment Failure
≥2 Prior Treatment Failure
70 mg 140mg 70mg 140mg 70mg 140mgChange in MMD
-2.2 (-4.1,-0.3)*
-0.5 (-2.4, 1.5)
-2.5 (-3.8,-1.2)**
-3.3 (-4.6,-2.1)**
-2.7 (-4.2, -1.2)**
-4.3(-5.8, -2.8)**
≥ 50% reduction in MMD
1.8(0.9, 3.4)
1.3(0.7, 2.7)
2.6**(1.6, 4.5)
3.3**(2.0, 5.5)
3.5**(1.8, 6.6)
4.2** (2.2, 7.9)
≥ 75% reductionin MMD
2.0(0.8, 4.8)
1.9(0.8, 4.6)
3.1*(1.2, 10.9)
4.6**(2.1, 10.0)
3.6* (1.2, 10.9)
8.0** (2.8, 23.0)
Ashina M., et al. Cephalalgia. 2018.**p<0.001 *p<0.05 treatment groups compared to placebo

©2018 MFMER | slide-28
Results
Ashina M., et al. Cephalalgia. 2018.
38.1
17.3 14.2
50
34.7 35.641.9 40.8 41.3
0
10
20
30
40
50
60
No Prior Treatment >1 Prior Treatment Failure >2 Prior Treatment Failures
Proportion of Patients Reaching ≥50% Reduction in MMD over 3 Months
Placebo Erenumab 70mg Erenumab 140mg

©2018 MFMER | slide-29
Results
14.3
5.13.5
23.4
13.711.1
22.620
21.7
0
5
10
15
20
25
No Prior Treatment Failure > 1 Prior Treatment Failure >2 Prior Treatment Failures
Proportion of Patients Reaching ≥75% Reduction in MMD over 3 Months
Placebo Erenumab 70mg Erenumab 140mg
Ashina M., et al. Cephalalgia. 2018.

©2018 MFMER | slide-30
Strengths• 1st trial to evaluate
erenumab in CM in patients with prior preventative treatment failures
• Subgroup analysis• Not powered to detect
differences within each subgroup
• Statistical testing was not pre-specified or adjusted for multiplicity
• Exclusion criteria limited patients with higher treatment failures
Ashina M., et al. Cephalalgia. 2018.
Limitations

©2018 MFMER | slide-31
Conclusions• Erenumab was effective and well tolerated in
patients with previous treatment failures
• Further studies need for long-term safety/ efficacy and in patients exhibiting no therapeutic response to >3 classes of preventative therapy.

©2018 MFMER | slide-32
Treatment with erenumab resulted in ≥50% reduction in monthly migraine days in CM for ~_____% of patients.

©2018 MFMER | slide-33
a. 10-25%b. 35-50%c. 55-70%d. 75-90%
©2018 MFMER | slide-34
ARISE: A Phase 3 randomized trial of erenumab for episodic migraine
Dodick DW, Ashina M, Brandes JL, et al. Cephalalgia. 2018.

©2018 MFMER | slide-35
Objectives• Primary Endpoint: Change in monthly migraine days
(MMD)• Secondary Endpoints:
• ≥50% reduction in monthly migraine days (MMD)• Change in acute migraine-specific medication
treatment days (MSMD)• 5-point reduction in Physical Impairment and
Impact on Everyday Activities domain scores measured by the Migraine Physical Function Impact Diary (MPFID)
Dodick DW, et al. Cephalalgia. 2018.

©2018 MFMER | slide-36
Migraine Physical Function Impact Diary (MPFID)
13 item patient reported outcome measure
Demonstrated reliability and validity in two domains in prospective, observational study
Not used in clinical practice Developed by Amgen Inc.
Kawata AK, et al. Headache. 2017.

©2018 MFMER | slide-37
Study Methods
• Multicenter, randomized, double-blind, placebo-controlled, parallel-group, phase 3 trial
• Randomized 1:1 to placebo or erenumab 70 mg monthly subcutaneous injection
• 577 patients randomized
Dodick DW, et al. Cephalalgia. 2018.

©2018 MFMER | slide-38
Enrollment
Dodick DW, et al. Cephalalgia. 2018.
Inclusion
Adults with EM (≥4 to 15 MMD and <15 headache days per month)
Exclusion
History of no therapeutic response to >2 preventative medication classes
Use of preventative medications during trial (washout period required)

©2018 MFMER | slide-39
Baseline CharacteristicsCharacteristic Placebo
n= 291Erenumab 70 mgn= 286
Age, years 42 ±12 42 ± 11Female sex, no (%) 247 (84.9) 245 (85.7)Age at migraine onset 22 ± 11 21 ± 10Prior Prophylactic Therapy, no (%) 125 (43) 123 (43)No Previous Prophylactic Therapy, no (%)
174 (59.8) 178 (62.2)
MMD 8.4 ± 2.6 8.1 ± 2.7MSMD 3.4 ± 3.6 3.7 ± 3.6MPFID impact on everyday activities score
13.2 ± 8.9 12.6 ± 8.6
MPFID physical impairment score 11.5 ± 9.2 10.8 ± 9.1Dodick DW, et al. Cephalalgia. 2018.MMD- Monthly Migraine Days
MSMD- Migraine-Specific Medication Days

©2018 MFMER | slide-40
Results
Endpoint Placebo Erenumab 70 mgChange in MMD -1.8 days -2.9 days
-1.0 (-1.6, -0.5) p< 0.001*≥50% reduction in MMD 29.5% 39.7%
OR: 1.59, (1.12,2.27) p=0.01*Change in MSMD -0.6 days -1.2 days
OR: -0.6, (-1.0,-0.2) p=0.002*MPFID impact on everyday activities score(≥5-point reduction)
35.8% 40.4%OR: 1.22, (0.87, 1.71) p=0.26
MPFID physical impairment score(≥5-point reduction)
27.1% 33.0%OR: 1.33, (0.92, 1.90) p=0.13
Dodick DW, et al. Cephalalgia. 2018.* statistically significantMMD- Monthly Migraine Days

©2018 MFMER | slide-41
Strengths• Endpoints measured • Excluded patients on
preventative treatment
Dodick DW, et al. Cephalalgia. 2018.
Limitations

©2018 MFMER | slide-42
Conclusion• Erenumab reduced MMD and MSMD in patients
with EM
• Further studies in combination with other migraine preventative treatments and in cardiovascular disease

©2018 MFMER | slide-43
Safety• Adverse effects similar between treatment and
placebo groups within both studies• Common Adverse Effects (≥2%)
• injection site pain• influenza• fatigue• nausea• constipation
• sinusitis• upper respiratory
tract infection (URI)• nasopharyngitis

©2018 MFMER | slide-44
Place in Therapy-Erenumab-aooe (Aimovig®)
• May be appropriate for patients with CM or EM that have had prior treatment failures
• Cost will likely limit use until more market competition
• Reports of prior authorization and restricted prescribing

©2018 MFMER | slide-45
Patient Case• MK established care with a neurologist after
failing an adequate trial of divalproex, nortriptyline, and gabapentin. She developed flank pain with topiramate.
• Which of the following is an appropriate option for this patient?

©2018 MFMER | slide-46
a. erenumab (Aimovig®)b. onabotulinumtoxinA (Botox®)c. propranolol (Inderal®)d. all of the above

©2018 MFMER | slide-47
Future Considerations with CGRP Antagonists
Tso AR, Goadsby PJ. Curr Treat Options Neurol. 2017.
Phase III trials
completed
fremanezumab Phase II trials completed
eptinezumab
Phase II trials completed
glacanezumab telcagepant & MK-3207 Trials stopped due to hepatotoxicity
ubrogepant (oral) Phase III trial underway for acute treatment
atogepant (oral)Under development for prevention

©2018 MFMER | slide-48
Summary
• Migraine preventative medications are often underutilized
• First-line agents include divalproex, topiramate, propranolol, and onabotulinumtoxinA
• CGRP antagonists will likely find a place in treatment after patients have failed multiple first-line agents
©2018 MFMER | slide-49
Questions