Embed Size (px)
Citation preview

GW
Di1caftvecopMigo
ssf
G
SA
0d
enetics of Hereditary Colorectal Canceron-Seok Jo and Daniel C. Chung
Genetic factors can dramatically influence the risk of colorectal cancer, and the molecularbases of many hereditary colorectal cancer syndromes, including familial adenomatouspolyposis (FAP), attenuated FAP (AFAP), and hereditary nonpolyposis colorectal cancer(HNPCC) have been elucidated. Additional syndromes continue to be defined as newgenes, including MYH, are linked to the development of colonic polyps and cancer. Therisks of colorectal cancer are variable and depend on the specific germline alterations.Some mutations are associated with a 100% lifetime risk of developing cancer, while othersare associated with only a mild increase in risk. Although there are overlapping clinicalfeatures in many of these syndromes, they can be distinguished by the age at cancerdiagnosis, inheritance pattern, number and distribution of polyps, specific histologic fea-tures of the cancers, and the presence of distinctive extracolonic features. The introductionand refinement of genetic testing has provided a new and invaluable tool for the diagnosisand assessment of cancer risk for suspected cases of hereditary colon cancer.Semin Oncol 32:11-23 © 2005 Elsevier Inc. All rights reserved.
GCTtwwgoiteTosttgar
dgtsgaeg
ietary and lifestyle modifications can reduce the risk ofcolon cancer, but other risk factors are not easily mod-
fied. Epidemiologic studies have estimated a relative risk of.8 if one first-degree relative is diagnosed with colon can-er.1,2 As many as 25% of all colon cancers are associated withfamily history of the disease, indicating that a substantial
raction of cases may be attributable to inherited genetic fac-ors.3 Approximately 3% to 5% of these cases are seen in indi-iduals with the well-recognized genetic syndromes familial ad-nomatous polyposis (FAP) or hereditary nonpolyposisolorectal cancer (HNPCC) (Table 1).4 However, the numberf hereditary colon cancer syndromes has been rapidly ex-anding and now includes, for example, the newly identifiedYH polyposis syndrome. Nevertheless, most cases of hered-
tary colon cancer have not yet been defined genetically. Theoal of this review is to highlight our current understandingf the inherited forms of colon cancer.Recognition of these syndromes is crucial because of the
pecialized approach to cancer risk assessment and cancercreening that is required for affected individuals, as well asamily members.
astrointestinal Unit and Department of Medicine, Massachusetts GeneralHospital, Harvard Medical School, Boston, MA.
upported by NIH RO1 CA92594.ddress reprint requests to Daniel C. Chung, MD, Gastrointestinal Unit and
Department of Medicine, Massachusetts General Hospital, Harvard Med-ical School, 50 Blossom St, Boston, MA 02114. E-mail: chung.daniel@
smgh.harvard.edu
093-7754/05/$-see front matter © 2005 Elsevier Inc. All rights reserved.oi:10.1053/j.seminoncol.2004.09.034
enetic Model ofolorectal Tumorigenesis
he study of colon cancer genetics established a paradigm forhe molecular pathogenesis of solid tumors. In 1990, a step-ise model for colorectal tumorigenesis was proposed inhich sequential alterations in the key growth regulatoryenes APC, K-ras, and TP53 culminated in the developmentf a malignant tumor.5 This so-called chromosomal instabil-ty pathway underlies the development of 85% of colorectalumors.6 Nearly all colon cancers arise from pre-existing ad-nomatous polyps, but not all adenomas progress to cancer.hose that do have accumulated the necessary combinationf genetic mutations in a prescribed chronological order. Inome familial colorectal cancer syndromes, the progressiono cancer is accelerated due to a pre-existing germline muta-ion in one of these key regulatory genes. In other cases, aermline mutation in one of several DNA repair genes createshypermutable environment in which somatic mutations
apidly accumulate.The genes implicated in colorectal carcinogenesis can be
ivided into three categories: tumor-suppressor genes, onco-enes, and DNA-repair genes. In the most general sense,umor-suppressor genes function to downregulate growth-timulatory pathways. In colon cancer, the tumor-suppressorenes that are most frequently inactivated include APC, TP53,nd p16INK4a.6 Consistent with the Knudson “two-hit hypoth-sis,” mutations in both alleles are required to fully inactivateene function.7 In autosomal dominant hereditary cancer
yndromes, one allele is mutated in the germline. The second11

Table 1 Inherited Syndromes With an Increased Risk of Colorectal Cancer
Syndrome GenesLifetime Risk
of CRCInheritance
Pattern
Average Ageof Diagnosisof CRC (yr)
No. ofPolyps
PolypsHistology
PredominantLocation of
Polyps/Cancerin Colon Extracolonic Features
High riskClassic familial
adenomatouspolyposis (FAP)
APC 100% Autosomaldominant
39 Hundreds tothousands
Adenomatous Entire colon Fundic gland polypsDuodenal/ampullary adenomasDesmoid tumors, osteomas,
thyroid and brain tumorsCHRPE
Attenuated FAP(AFAP)
APC >80% Autosomaldominant
56 <100 Adenomatous Proximal colon Fundic gland polypsDuodenal/ampullary adenomas
Hereditary nonpolyposiscolorectalcancer (HNPCC)
MLH1MSH2MSH6
80% Autosomaldominant
45 Few Adenomatous Proximal colon Tumors of the uterus, ovary,stomach, kidney, urinarytract, biliary tree, smallintestine, and skin
MYH polyposis MYH �100%* Autosomalrecessive
5082 <100 Adenomatous Entire colon Undetermined
Moderate riskPeutz-Jegher’s
syndrome (PJS)LKB1 39%90 Autosomal
dominant4590 Few Hamartomatous Entire colon Mucocutaneous pigmentation
Tumors of the uterus, breast,lungs, reproductive organs,pancreas, and gallbladder
Juvenile polyposiscoli (JPC)
MADH4BMPR1A
10%-38%108-110 Autosomaldominant
34111 Few Hamartomatous Entire colon Tumors of the stomach andduodenum
Hyperplasticpolyposissyndrome (HPS)
Unknown 25%-35%†118,120 Unknown 66122 Many‡ Hyperplastic Entire colon None described
Low riskBloom’s syndrome BLM 8%128 Autosomal
recessive33128 Few Adenomatous Entire colon Leukemia
LymphomaCarcinomas of the head and
neck, respiratory tract,female reproductive organs,breast, and uppergastrointestinal tract
I1307K APCpolymorphism
APC 8%-11%134 Autosomaldominant
64-70136 Few Adenomatous Entire colon None described
Abbreviations: CRC, colorectal cancer; CHRPE, congenital hypertropy of the retinal pigmented epithelium.*Extrapolated from preliminary studies. Exact value remains to be determined.†These numbers represent prevalence of colorectal cancer among HPS patients. Lifetime risk has not been determined.‡See Table 6.
12W
.-S.Joand
D.C.Chung

aach
iltmga
cvrncepn“opmad
RCTb
fiya(cti
cibatcwmtnHetfico
itsctoadoiolcrpc
SRFPFw7wted
FgIppsc
Genetics of hereditary colorectal cancer 13
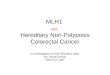
lteration is acquired somatically, and silencing of the secondllele can be achieved through a variety of mechanisms, in-luding chromosomal deletion, point mutation, or promoterypermethylation (Fig 1).Proto-oncogenes such as K-ras are components of signal-
ng pathways that normally promote cellular growth and pro-iferation. Oncogenic mutations result in a constitutively ac-ive gene product. In contrast to tumor-suppressor genes, autation in only one allele is sufficient to exhibit a tumori-
enic effect. To date, no colon cancer syndrome has beenttributed to an inherited mutation in a proto-oncogene.
Maintaining the integrity of the genome is a complex pro-ess essential for cellular homeostasis. Modification of indi-idual nucleotides can be introduced through biochemicaleactions that include UV cross-linking, alkylation, sponta-eous deamination, or oxidation. A highly orchestrated pro-ess called the “base excision repair system” corrects theserrors.8 A second way that errors are introduced is via mis-airing of nucleotides. Mismatch errors can occur duringormal DNA replication but are quickly repaired by theDNA mismatch-repair system.” When components of eitherf these DNA-repair systems are dysfunctional, a mutatorhenotype results in which deleterious mutations can accu-ulate in target genes that directly control cellular growth
nd proliferation. A dysfunctional DNA-repair process un-erlies the HNPCC, MYH polyposis, and Bloom’s syndromes.
ecognizing Hereditaryolon Cancer Syndromes
he recognition of a hereditary colon cancer syndrome first
igure 1 Knudson’s “two hit” hypothesis. For tumor-suppressorenes, inactivation of both alleles is required for cancer to develop.n autosomal dominant colon cancer syndromes, the “first hit” isrovided by the pre-existing germline mutation in one allele that isresent in every cell. The “second hit” occurs when an acquired, oromatic, mutation inactivates the other allele. In sporadic colonancer, both “hits” are acquired somatically.
egins with the astute clinician. In general, there are several C
eatures that should raise the suspicion of such a syndrome,ncluding (1) the diagnosis of colon cancer at an unusuallyoung age (�50 years), (2) the diagnosis of colonic polyps atn unusually young age (�45 years) or in large numbers�10 polyps), (3) the presence of distinctive extracolonicancers, or (4) a family history of any of the above. If any ofhese features is present, a more careful evaluation should benitiated.
The key clinical features of the known hereditary colonancer syndromes are described in detail below. The mostmportant advance in their diagnosis and management haseen the introduction of genetic testing for germline DNAlterations. There are two major implications. First, diagnos-ic criteria for these syndromes are no longer based purely onlinical features but now include genetic test results. In caseshere the phenotypic expression of a condition is pathogno-onic, such as the diffuse polyposis observed in FAP, genetic
esting may simply confirm the straightforward clinical diag-osis. However, when clinical features are more protean as inNPCC, genetic testing can provide an invaluable means of
stablishing a diagnosis. The second major implication is thathe accuracy of cancer risk assessment for potentially affectedamily members has substantially improved. This permitsntensive cancer screening to be targeted only to those whoarry a germline alteration and spares noncarriers from thesetherwise necessary measures.Genetic testing for cancer predisposition is a rapidly evolv-
ng area of medicine. One facet that can present a challenge ishe interpretation of test results. Although most cases aretraightforward, there are times when test results can be in-onclusive. For example, the absence of an identifiable mu-ation does not necessarily rule out the disorder. The absencef a mutation is a true “negative” result only when a clinicallyffected family member also tests “positive.” A particularlyifficult result to explain is the so-called missense mutationf uncertain significance. In contrast to mutations that resultn a prematurely truncated protein, a missense alteration mayr may not be associated with the disorder. Finally, althoughegislation has been passed in 47 states banning genetic dis-rimination for health insurance,9 some apprehension sur-ounding genetic testing lingers. Because of the many com-lexities inherent in the testing process, formal geneticounseling is recommended.
yndromes With a Highisk of Colorectal Cancer
amilial Adenomatousolyposis and Attenuated FAPAP is the most common adenomatous polyposis syndrome,ith an estimated prevalence between one in 5,000 to,500.10 It is inherited in an autosomal dominant mannerith a penetrance of 100%. Classic FAP is characterized by
he development of multiple colonic adenomas during thearly teenage years with progressive increases so that hun-reds to thousands of polyps are recognized by adulthood.
olonic adenocarcinomas are observed approximately 10 to
1bai
nniiumm6F
tmcydbhtwH
s(cchtpacpersAc
icchtgt�lpaots
g
tutttwloAiftAt
pDtqma
FsctiWnafai
14 W.-S. Jo and D.C. Chung
5 years after the appearance of polyposis, and almost alwaysy the age of 40 years. FAP-associated adenomas and cancersre distributed throughout the entire colon and are histolog-cally identical to those found in the general population.
Multiple gastric polyps can develop and are typically be-ign fundic gland polyps. Gastric adenomas and adenocarci-omas have also been documented, particularly in FAP fam-
lies from Japan and Korea, where there is an overall twofoldncreased risk of gastric cancer compared to the general pop-lation.11,12 Duodenal, peri-ampullary, or ampullary adeno-as eventually develop in nearly all FAP patients. Approxi-ately 10% will develop duodenal adenocarcinoma by age
0,13 making it the second most common malignancy inAP.14
Extraintestinal features include follicular and papillaryhyroid cancers, congenital hypertrophy of the retinal pig-ented epithelium (CHRPE), desmoid tumors, epidermoid
ysts, and osteomas. Rarely, hepatoblastomas are seen inoung children. Desmoid tumors typically develop after ab-ominal surgery and rank second as a cause of mortalityehind metastatic carcinoma.15 Turcot’s syndrome refers toereditary colon cancer families with central nervous systemumors. Medulloblastomas have been associated with FAP,hereas glioblastomas are the brain tumors primarily seen inNPCC kindreds.16
An attenuated version of FAP (AFAP) differs from the clas-ic form in that there are substantially fewer colonic polyps�100); these polyps tend to develop on the right side of theolon, and the average ages at which colorectal polyps andancer occur are delayed approximately 15 years. There are,owever, no appreciable differences in upper gastrointestinalract lesions, as multiple fundic gland polyps are invariablyresent and there is a similar risk of duodenal adenomas anddenocarcinomas.17 In some cases, fundic gland polyposisan actually precede the onset of colonic polyposis.17 Theresence of thousands of colonic polyps makes classic FAPasy to diagnose, but the attenuated form can be difficult toecognize when the polyp burden is very low or the onset isignificantly delayed (ie, after age 60 years). The features ofFAP can also overlap with HNPCC,18 and genetic testingan distinguish between the two syndromes.
The gene responsible for both FAP and AFAP was firstdentified in 1991 through linkage analysis and positionalloning.19-21 The adenomatous polyposis coli (APC) gene lo-ated on chromosome 5q21 is a tumor-suppressor that in-ibits the Wnt signaling pathway.6 The key component inhis pathway is �-catenin, which activates the transcription ofrowth-regulatory genes through its interaction with theranscription factor T-cell factor 4 (TCF4). APC targets-catenin for degradation, thereby acting as a negative regu-
ator of Wnt signaling (Fig 2). When APC is mutated, thehysical interaction between APC and �-catenin is impaired,nd excess �-catenin is translocated to the nucleus. The piv-tal role of APC in colorectal tumorigenesis is highlighted byhe fact that more than 70% of sporadic colon cancers harboromatic mutations in the APC gene.
Germline mutations are located throughout the entire APC
ene, and more than 90% of mutations introduce a prema- hure stop codon that results in a truncated protein prod-ct.22,23 There are fascinating genotype-phenotype correla-ions (Fig 3). Classic FAP is seen with mutations located inhe central region between codons 169 and 1393,24 and mu-ations between codons 1250 and 1464 have been associatedith particularly severe polyposis.25 In contrast, mutations
ocated at the 5= end (proximal to codon 157)26 or the 3= endf the gene (distal to codon 1596)27 are associated withFAP. One potential explanation for the delayed phenotype
s that mutations in AFAP give rise to a truncated but stillunctional APC protein.28 Thus, two additional somatic mu-ations are required to inactivate both the wild-type and theFAP allele, which would be predicted to require a longer
ime to occur.Genetic tests for FAP were one of the first cancer predis-
osition tests available commercially. The options includeNA sequencing, conformation strand gel electrophoresis,
he protein truncation test, and linkage analysis.29 Direct se-uencing of the entire APC gene is now considered to be theost accurate.30 In up to 20% of cases, genetic testing reveals
n APC mutation in an affected individual without a family
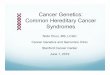
igure 2 The Wnt signaling pathway. The activation of the Wntignaling pathway involves the translocation of �-catenin from theell membrane into the nucleus where it interacts with the TCF4ranscription factor to promote transcription of TCF target genes,ncluding cyclin D1, myc, PPAR�, and VEGF. APC downregulates the
nt signaling pathway by preventing �-catenin from entering theucleus. When �-catenin is bound to a complex containing APC,xin, and GSK3�, GSK3� phosphorylates �-catenin and targets itor degradation. When APC is mutated, the Wnt pathway becomesctivated because phosphorylation of �-catenin does not occur, andt can then translocate to the nucleus.
istory of polyposis in either parent, indicating a de novo, or

sum
coateoambs
iyimscwmucnpbbgcq
HAcbr
turfiuttcsaddtTc
Httiibsb(bs
cataHmpets2
m(
Ffmi1ap
TH
CEGOSBBK
Genetics of hereditary colorectal cancer 15
pontaneously acquired, germline mutation.29 These individ-als can pass on the disorder to their offspring in an autoso-al dominant manner.Annual flexible sigmoidoscopy in classic FAP or colonos-
opy in AFAP should be initiated by the age of 10 to 12 yearsr by age 25 years, respectively. Upper endoscopy using bothforward- and side-viewing instrument31 should be started at
he time of colectomy or by age 30 years and then repeatedvery 1 to 3 years. Annual thyroid ultrasounds should bebtained beginning at the age of 10 to 12 years. Annuallpha-fetoprotein levels and liver ultrasound are also recom-ended during the first decade of life to screen for hepato-
lastoma. Individuals in families with Turcot’s syndromehould also undergo periodic brain imaging.
Colectomy is the only definitive treatment and becomesnevitable once the colon is carpeted with adenomatous pol-ps. The preferred approach is a total proctocolectomy withleostomy or ileo-anal anastomosis. In select cases of FAP and
ost cases of AFAP where the rectal polyp burden is low, aubtotal colectomy with an ileorectal anastomosis can beonsidered.32,33 If the rectum is left intact, rigorous follow-upith sigmoidoscopy every 6 to 12 months is required. Che-opreventive agents may play an adjunctive role in individ-als with a residual rectum. Sulindac and the more selectiveyclooxygenase-2 inhibitors can significantly reduce theumber and size of colonic adenomas.34-36 However, a com-arable benefit for upper gastrointestinal adenomas has noteen convincingly demonstrated. Ampullary adenomas cane managed initially with endoscopic ampullectomy, butiven the risk of residual or recurrent adenomatous tissue,37
lose endoscopic surveillance or surgical management is re-uired.
ereditary Nonpolyposis Colorectal Cancermong the colon cancer syndromes, HNPCC is the mostommon and accounts for close to 1% of the colon cancerurden in the United States4 and nearly 2% in Europe.38 Also
igure 3 Genotype-phenotype correlations in FAP. Certain clinicaleatures in the FAP syndrome are correlated with the location of the
utation within the APC gene. There are 15 exons and 2843 codonsn the APC gene. Mutations that occur between codons 169 and393 have been associated with the classic FAP phenotype. AFAP,ttenuated familial adenomatous polyposis; CHRPE, congenital hy-ertrophy of the retinal pigmented epithelium.
eferred to as the Lynch syndrome, HNPCC exhibits an au- B
osomal dominant inheritance pattern, and affected individ-als carry an 80% lifetime risk of colorectal cancer.39 Colo-ectal cancers are diagnosed at an average age of 45 years. Thenite number (�10 to 20) of adenomas that develop aresually located in the right colon (�70% occur proximal tohe splenic flexure40) and appear flat endoscopically. Al-hough HNPCC-associated colorectal cancers have a signifi-antly greater depth of invasion at diagnosis compared withporadic tumors, their natural history is typically more favor-ble.41,42 Histologically, these tumors are described as poorlyifferentiated with mucinous and signet cell features. In ad-ition, there can be a Crohn’s-like inflammatory reaction athe periphery with dense tumor-infiltrating lymphocytes.43,44
he progression of adenomas to cancer is accelerated, witharcinomas emerging within as short a period as 2 years.
A unique set of extracolonic tumors is associated with theNPCC syndrome (Table 2). Type I HNPCC is defined by
he occurrence of only colorectal cancer, while families withype II HNPCC also display extracolonic tumors. The uteruss the most common site outside of the colon, but other sitesnclude the stomach, ovary, renal pelvis and urinary tract,iliary tract, and small intestine.45 Turcot’s and Muir-Torreyndromes are variants of HNPCC defined by the presence ofrain tumors (primarily glioblastomas16) and skin tumorskeratoacanthomas, squamous and basal cell carcinomas, se-aceous adenomas, or sebaceous adenocarcinomas46), re-pectively.
Clinical criteria for the diagnosis of HNPCC take into ac-ount the age of diagnosis of colon cancer, the number offfected family members, and the presence of extracolonicumors (Table 3). The original Amsterdam I criteria of 199047
re considered to be highly specific for the diagnosis ofNPCC. In order to develop less stringent guidelines, theodified Amsterdam and Amsterdam II criteria48 were pro-osed. In 1996, the Bethesda guidelines49 were formulated toncompass an even broader spectrum of at-risk patients,hereby maximizing sensitivity but necessarily reducingpecificity. These criteria were updated and simplified in004.50
The observation that HNPCC tumors exhibited a distinctolecular abnormality called DNA microsatellite instability
MSI) led to the identification of DNA mismatch-repair
able 2 Lifetime Risks for Cancer Associated WithNPCC148,149
Types of Cancer
Persons WithHNPCC
(%)
GeneralPopulation
(%)
olorectal 80-82 5-6ndometrial 50-60 2-3astric 13 1varian 12 1-2mall bowel 1-4 0.01ladder 4 1-3rain 4 0.6idney, renal, pelvis 3 1
iliary tract 2 0.6
(pamhfsfiqMrcrsg(g
rt
gnmhMMf(mvoit
hmcsmBfthtlclrthc
Fb(
TN
*
16 W.-S. Jo and D.C. Chung
MMR) genes as the underlying basis for HNPCC.51-60 MMRroteins recognize and then correct the base pair mismatchesnd small insertions or deletions that can occur during nor-al DNA replication. Multiple genes from the mutS (hMSH2,
MSH3, hMSH6) and mutL (hMLH1, hMLH3, hPMS1, hPMS2)amilies interact to repair these mismatched DNAequences.61,62 Microsatellite DNA sequences, which are de-ned as short repetitive mononucleotide or dinucleotide se-uences, are particularly susceptible to errors of replication.ost microsatellite sequences are located in the noncoding
egions of the genome. However, microsatellite sequencesan be found within the coding regions of certain growth-egulatory genes, and loss of MMR proofreading activity re-ults in the accumulation of frameshift mutations in theseenes. These target genes include receptors for growth factorstransforming growth factor-� receptor II,63 insulin-like
able 3 Clinical Guidelines for the Diagnosis of Hereditaryonpolyposis Colorectal Cancer
Amsterdam I criteria1. Three relatives with colorectal cancer, one a first-
degree relative of the other two2. Cases that span at least two generations3. At least one colorectal cancer case diagnosed before
age 50 yearsAmsterdam II criteria
1. Three relatives with an HNPCC-associated cancer(colorectal, endometrial, small bowel, ureter, or renalpelvis), one a first-degree relative of the other two
2. Cases that span at least two generations3. At least one cancer case diagnosed before age 50
yearsModified Amsterdam criteria
1. In very small families, two colon cancer cases in first-degree relatives spanning at least two generations,one case diagnosed before age 55 years
2. In families with two first-degree relatives with coloncancer, a third relative with an unusual early-onsetcancer or endometrial cancer
Bethesda criteria (revised 2004)50
1. Colorectal cancer before age 50 years2. Synchronous or metachronous colorectal cancer or
other HNPCC-related cancer* regardless of age3. Colorectal cancer with MSI-H morphology
(characterized by the presence of tumor infiltratinglymphocytes, mucinous differentiation/signet ring cellcarcinoma, peritumoral Crohn’s-like lymphocyticreaction, medullary growth pattern) before age 60years
4. Colorectal cancer with one or more first-degreerelatives with colorectal cancer or other HNPCC-related cancer,* one of the cancers before age 50years
5. Colorectal cancer with two or more relatives withcolorectal cancer or other HNPCC-related cancer*regardless of age
Includes endometrial, ovarian, gastric, small bowel, urinary tract,biliary tract, pancreas, brain, and sebaceous gland.
rowth factor II receptor64), cell cycle regulators (E2F465), M
egulators of apoptosis (BAX66), and some of the MMR geneshemselves (hMSH3 and hMSH667).
More than 90% of HNPCC cases are accounted for byermline mutations in hMSH2 or hMLH139 (see www.fdht.nl). A broad spectrum of truncating, frameshift, andissense mutations has been observed. Inactivation of
MSH2 or hMLH1 results in tumors that exhibit a high level ofSI. The US National Cancer Institute defines tumors asSI-high (MSI-H) when two of five microsatellite markers
rom a standard panel are found to be unstable and MSI-lowMSI-L) when only one of five displays instability.68 Germlineutations in hMSH6 have been associated with an attenuated
ersion of HNPCC69 that is characterized by a delayed onsetf colorectal cancer (median age of 61 years),69,70 a higherncidence of endometrial cancer,71 and tumors that displayhe MSI-L phenotype.
Commercial genetic testing is currently available forMLH1, hMSH2 and hMSH6. A suggested algorithm for theolecular diagnosis of HNPCC is illustrated in Fig 4. If the
linical suspicion is high based on the fulfillment of the Am-terdam I criteria, then one can proceed directly to germlineutational analysis. If the diagnosis is suggested by the looserethesda criteria, testing for MSI in archived tumor tissuerom an affected individual should be performed first. Forumors that display the MSI-H phenotype, hMLH1 andMSH2 germline mutational analysis is then indicated. If theumor does not exhibit MSI; then hMLH1 and hMSH2 germ-ine testing is not warranted. hMSH6 germline testing can beonsidered for tumors that are MSI-L. Currently, the corre-ation between clinical criteria for HNPCC and genetic testesults is suboptimal. If all Amsterdam I criteria are fulfilled,here is only a 39% to 86% chance of identifying a germlineMLH1 or hMSH2 mutation.72-74 Between 6.5% and 20% ofases in which no mutation can be identified may be ac-
igure 4 Suggested algorithm for genetic testing of an affected pro-and from a suspected HNPCC kindred. MSI-H, high level of MSIMSI-H phenotype); MSI-L, low level of MSI (MSI-L phenotype);
SS, microsatellite stable; IHC, immunohistochemistry.149
cmD
esbtttvrTtine3gus
MThtbcap1tacdtiaoobFptecr
eoeirip
e
tmwhfdtdo
fib
SRPPhtttmfttlcmtncdhtbTw4n
sAatpompgetar
Genetics of hereditary colorectal cancer 17
ounted for by large chromosomal deletions or rearrange-ents in hMLH1 or hMSH2 that are not routinely detected byNA sequencing.75-77
Once the diagnosis of HNPCC has been established byither clinical or molecular criteria, an aggressive cancercreening program should be initiated. Colonoscopy shouldegin between ages 20 and 25 years, or 10 years earlier thanhe age of diagnosis of the youngest case in the family, andhen repeated every 1 to 2 years.78 Annual colonoscopies arehen recommended after the age of 40 years. Annual trans-aginal ultrasounds and endometrial aspiration biopsies areecommended due to the high risk of endometrial cancer.here are no standardized guidelines for other extracolonic
umors, and screening is generally based on the specific fam-ly history. Screening for ovarian cancer would include an-ual transvaginal ultrasound and pelvic examination. Upperndoscopy can be considered every 2 years starting from age0 to 35 years, or 5 years earlier than the youngest case ofastric cancer. One approach to screening for tumors of theroepithelial tract would incorporate annual renal ultra-ound, urinalysis and urine cytology.
YH Polyposis Syndromehus far, the high risk colon cancer syndromes discussedave displayed an autosomal dominant pattern of inheri-ance. However, the discovery that biallelic mutations in thease excision repair gene, MYH, result in an increased risk ofolorectal adenomas and cancer led to the first description ofn autosomal recessive colon cancer syndrome.79 In Euro-ean populations, 22% to 29% of individuals with more than0 adenomatous polyps carried biallelic germline MYH mu-ations.79-84 The precise colon cancer risk has not yet beenscertained, but it is likely to approach the 100% level appre-iated in FAP. The mean ages of colon polyp and canceriagnosis are 46 and 49.7 years, respectively.82 The pheno-ype of MYH polyposis resembles AFAP in that patients typ-cally present with less than 100 polyps.85 However, there issubset that displays features of classic FAP. A total of 7.5%f individuals who exhibited diffuse colonic polyposis with-ut a detectable germline APC mutation were found to carryiallelic MYH mutations. These individuals resemble cases ofAP with de novo APC mutations, as there is no evidence ofolyposis in either parent. Although some extracolonic fea-ures such as congenital hypertrophy of the retinal pigmentpithelium, duodenal adenomas, osteomas, and gastric can-er have been observed rarely in these patients, a direct causalelationship has not yet been established.81-83
MYH is a DNA glycosylase that participates in the basexcision repair process.86 8-Oxo-guanine is a byproduct ofxidative DNA damage and it inappropriately pairs with ad-nines, leading to G:C3T:A mutations.87-89 The role of MYHs to excise the mispaired adenines. Dysfunction of MYHesults in the accumulation of somatic G:C3T:A mutationsn specific growth-regulatory genes, and APC appears to be areferred target.79,80
Genetic testing is now available, and analysis is focused on
xons 7 and 13 of the MYH gene. Two specific mutations in mhese exons (Y165C and G382D) account for 87% of all MYHutations in the Northern European population.81 Patientsho display a phenotype suggestive of attenuated FAP butave tested negative for APC mutations can be offered testingor germline MYH mutations. Recognizing that the MYH syn-rome has important implications for genetic counseling, ashe cancer risk is limited primarily to siblings but not chil-ren. Thus far, there does not appear to be an increased riskf polyps or cancer in MYH heterozygote carriers.Until official guidelines are established, it is reasonable to
ollow the recommendations for colorectal cancer screeningn attenuated FAP. The role of chemoprevention has not yeteen studied.
yndromes With a Moderateisk of Colorectal Cancereutz-Jegher’s Syndromeeutz-Jegher’s syndrome (PJS) is an autosomal dominantamartomatous polyposis syndrome that carries a 39% life-ime risk of colon cancer.90 There is a striking 93% cumula-ive risk of developing any type of malignancy. The charac-eristic clinical feature in PJS is mucocutaneous pigmentedacules on the lips, perioral area, buccal mucosa, hands, and
eet. Patients also develop multiple hamartomatous polypshroughout the gastrointestinal tract, most prominently inhe small intestine. PJS polyps are unique hamartomatousesions characterized by glandular epithelium with a centralore of arborizing smooth muscle bands contiguous with theuscularis mucosae. These polyps cause intestinal obstruc-
ion and hemorrhage. Carcinomas of the stomach, duode-um, jejunum, ileum, and colon have been reported.90 Theseancers are believed to arise from adenomatous tissue thatevelops within PJS polyps.91 Extraintestinal tumors thatave been associated with PJS include melanoma, sex cordumors, uterine, breast, lung, pancreatic, gallbladder, andiliary cancer.92-98 The clinical diagnosis of PJS is outlined inable 4. The average age of PJS diagnosis is 23 to 26 years,hile the mean age of any cancer diagnosis is approximately0 to 50 years.91,99 The mean age of colorectal cancer diag-osis is 45.8 years.90
PJS has been linked to germline mutations of LKB1, aerine-threonine kinase located on chromosome 19p.100,101
mong its many functions, LKB1 can regulate p53-mediatedpoptosis.102 Recently, adenosine monophosphate (AMP) ac-ivated protein kinase has been identified as a direct phos-horylation target for LKB1, implicating LKB1 in the controlf cellular metabolism.103,104 Genetic testing for germlineutations in LKB1 is available, but only 50% to 60% ofatients with classic features of PJS will have identifiableermline mutations, suggesting there may be additional dis-ase loci yet to be identified.105 This observation reinforceshe general principle that the absence of a mutation in anffected individual must be viewed as an inconclusive testesult.
Because of the colon cancer risk, colonoscopy is recom-
ended every 3 years starting at age 18 years. In addition,
uasce
JLidt1
yi
pt
etfdfyau
Mtfeodpi
1Uy
HSttiymsddh
ysfrhdT
hpme
TG
D
S
Ts
TS
18 W.-S. Jo and D.C. Chung
pper endoscopy should be performed every 3 years startingt age 25 years,106,107 and screening for small bowel cancerhould also be undertaken with a small bowel series or videoapsule endoscopy every 2 years. Screening guidelines forxtraintestinal cancers are outlined in Table 4.
uvenile Polyposis Syndromeike PJS, the juvenile polyposis syndrome (JPS) is inherited
n an autosomal dominant pattern and characterized by theevelopment of hamartomatous intestinal polyps. JPS pa-ients exhibit a 10% to 38% lifetime risk of colon cancer,108-
10 and the average age of colon cancer diagnosis is 34ears.111 A clinical diagnosis of JPS is made when the criterian Table 5 have been fulfilled.
Juvenile polyps are characterized by a prominent laminaropria compartment with dilated cystic glands rather thanhe excessive number of epithelial cells that are seen in ad-
able 4 Diagnostic Criteria150 and Recommended Screeninguidelines107 for Peutz-Jegher’s Syndrome
iagnostic criteria1. Two or more PJS polyps in the gastrointestinal tract,
or2. One or more PJS polyp in conjunction with
characteristic mucocutaneous pigmentation, or3. One or more PJS polyp in conjunction with a family
history of PJS
creening guidelinesOrgan Recommendations
Colon Colonoscopy every 3 years startingat age 18 years
Stomach Upper endoscopy every 3 yearsstarting at age 25 years
Small bowel Small bowel series or video capsuleendoscopy every 2 years startingat age 25 years
Pancreas Endoscopic or abdominalultrasound every 1-2 yearsstarting at age 30 years
Breast Annual breast examination withmammogram every 2-3 yearsstarting at age 25 years
Uterus, ovaries Annual pelvic examination, PAPsmear, pelvic ultrasound startingat age 20 years
Testes Annual testicular examinationstarting at age 10 years; testicularultrasound if feminizing featuresare present
able 5 Clinical Diagnostic Criteria for Juvenile Polyposisyndrome111,151
1. Greater than 3 to 10 juvenile polyps in the colon, or2. Any juvenile polyp in the gastrointestinal tract outside
of the colon, or
3. Any juvenile polyp with a family history of JPSnomatous polyps. Juvenile polyps can cause bleeding, in-ussusception, and obstruction, which are typically mani-ested during childhood. The average age at which symptomsevelop is 9.5 years.112 Like PJS, cancer is believed to arise
rom adenomatous tissue that develops within juvenile pol-ps.108 Patients also have a 15% to 21% lifetime risk of gastricnd duodenal cancers that arise from juvenile polyps in thepper gastrointestinal tract.108,109
Two genes, MADH4 and BMPR1A, have been linked to JPS.ADH4, located on chromosome 18q, encodes the Smad4 pro-
ein that regulates intracellular signaling of transforming growthactor-� (TGF-�).113 The BMPR1A gene on chromosome 10qncodes a receptor for bone morphogenetic protein, a memberf the TGF-� superfamily.114 Genetic testing for JPS consists ofirect sequencing for mutations in MADH4 and BMPR1A. Aathogenic mutation in one of these two genes will be detected
n only 40% to 50% of all JPS cases.115-117
Patients with JPS should have their first colonoscopy at age5 to 18 years, and this should be repeated every 1 to 2 years.pper endoscopy is recommended starting at the age of 25ears and then every 1 to 2 years.
yperplastic Polyposis Syndromeporadic hyperplastic polyps are encountered incidentally inhe distal sigmoid and rectum and have traditionally beenhought to not possess malignant potential. However, rarendividuals and families exhibit numerous hyperplastic pol-ps distributed throughout the colon,118,119 and approxi-ately 25% to 35% of these cases have been associated with
ynchronous colorectal cancers.118,120,121 This genetically un-efined entity has been termed hyperplastic polyposis syn-rome (HPS). A set of clinical criteria for the diagnosis of HPSas been proposed (Table 6).HPS patients typically have more than 20 hyperplastic pol-
ps in the colon, with some polyps greater than 1 cm inize.119,120 Large hyperplastic polyps are more commonlyound in the right colon and are associated with an increasedisk of proximal colon cancer. There may be a history ofyperplastic polyps and colorectal cancer in first- or second-egree family members, but this is not consistently observed.he mean age of colorectal diagnosis is 66 years.122
The molecular mechanisms responsible for this syndromeave not yet been elucidated. It has been proposed that hy-erplastic polyps may progress to cancer through an adeno-atous intermediate, either the admixed hyperplastic- ad-
nomatous polyp or the serrated adenoma.123 The genetic
able 6 Clinical Diagnostic Criteria for Hyperplastic Polypo-is Syndrome (HPS)152
1. Greater than five histologically diagnosed hyperplasticpolyps proximal to the sigmoid colon, two of whichmeasure greater than 10 mm in diameter, or
2. Any number of hyperplastic polyps proximal to thesigmoid colon in an individual with a first-degreerelative with HPS, or
3. Greater than 20 hyperplastic polyps of any size
distributed throughout the colon
coatpfm
Httu
SRBBdtsnstakrgctTci
olttqDt
cri
Asim
srlt
IArapcdtcthtrbrsc
BTwctdpBmmsScHpadc
CTicdtlsihtcgllea
Genetics of hereditary colorectal cancer 19
hanges in polyps from individuals with hyperplastic polyp-sis have been rather heterogeneous. For example, both MSInd chromosomal instability have been observed.119 An al-ernative pathway of colorectal tumorigenesis has been pro-osed in which the initiation of hyperplastic polyps resultsrom the inactivation of DNA-repair genes by promoter
ethylation.123
Cancer screening guidelines have not yet been established.owever, one strategy is to repeat a colonoscopy 1 year after
he diagnosis is made and then every 2 to 3 years.120 Colec-omy may be appropriate in cases where the polyp burden isnmanageable endoscopically.
yndromes With a Lowisk of Colorectal Cancerloom’s Syndrome
loom’s syndrome is an extremely rare autosomal recessiveisorder primarily seen in the Ashkenazi Jewish popula-ion.124,125 Affected individuals display short stature, photo-ensitive facial erythema, diabetes mellitus, infertility, immu-odeficiency, and a predisposition to cancer in multipleites.126 As of 1996, approximately 42% of the 168 patients inhe Bloom’s Syndrome Registry had developed cancer, oftent more than one primary site.127 The cancers included leu-emia, lymphoma, and carcinomas of the head and neck,espiratory tract, female reproductive organs, breast, upperastrointestinal tract, and colon. As of 2001, colorectal can-er had been observed in approximately 8% of the patients inhe registry, with a mean age of diagnosis of 33.2 years.128
he presence of multiple colonic adenomas in the proximalolon reminiscent of the AFAP phenotype has been describedn a single individual with Bloom’s syndrome.128
The gene underlying Bloom’s syndrome (BLM) is locatedn chromosome 15q and encodes a homologue of recQ he-icase.129 The 3= to 5= DNA helicase activity of BLM is essen-ial for chromosomal stability,130 as cells deficient in this pro-ein show a high frequency of sister chromatid exchanges anduadriradial configuration.126 BLM plays a role in repairingNA damage at stalled replication forks, thus maintaining
he fidelity of DNA replication.131
A provocative study in 2002 suggested that heterozygotearriers of the BLM mutation appeared to have an increasedisk (odds ratio, 2.76) of colorectal cancer.132 However, anndependent study failed to confirm this association.133
The diagnosis can be confirmed by cytogenetic analysis.lternatively, DNA can be probed with an oligonucleotidepecific for the BlmAsh mutation, a 6-bp deletion and 7-bpnsertion at nucleotide position 2281. This is the most com-
on mutation observed in Ashkenazi Jewish carriers.125
There are currently no guidelines for colorectal cancercreening in Bloom’s syndrome. It is reasonable to begin pe-iodic screening with colonoscopy early in the third decade ofife. The significance of heterozygous BLM mutations remains
o be determined. c1307K APC Polymorphismpproximately 6% of the Ashkenazi Jewish population car-ies a variant in codon 1307 of the APC gene that substituteslysine for an isoleucine. I1307K carriers do not display
olyposis but do exhibit a small increase in the risk of colonancer (odds ratio, 1.4 to 1.9).134,135 The mean age of canceriagnosis is 64 to 70 years,135,136 which is not different fromhe general population. Family history is not predictive ofarrier status. The I1307K alteration does not directly alterhe function of the APC gene product but creates a region ofypermutability within the APC gene itself. The accumula-ion of additional somatic mutations in this hypermutableegion of APC then inactivates gene function. Genetic testingy direct analysis of codon 1307 is available. However, theelatively low odds ratio and the late onset of colon canceruggest that genetic test results may have little impact uponlinical management.
RCA1he co-occurrence of breast and colorectal cancers in manyomen has raised the possibility of an underlying “breast–
olon cancer” syndrome. Indeed, the relative risk of colorec-al cancer in women with a history of breast cancer has beenemonstrated to be between 1.1 and 3.0.137,138 BRCA1 wasroposed as a candidate gene because deletions near theRCA1 locus on chromosome 17 have been detected in al-ost 50% of sporadic colorectal cancers.139 BRCA1 is a tu-or-suppressor gene that plays a role in the repair of double-
trand DNA breaks through homologous recombination.140
ome have estimated the relative risk of BRCA1 mutationarriers for colorectal cancer to lie between 2 and 4.11.141,142
owever, the preponderance of the evidence does not sup-ort an association between BRCA1 germline mutation andn increased colon cancer risk.143-147 Until further studiesemonstrate otherwise, enhanced screening for colorectalancer is not recommended.
onclusionhere is a rapidly growing appreciation for the role of inher-
ted genetic factors and the development of cancer. In colonancer, a wide spectrum of genes can increase the risk of theisease when altered in the germline. The vast majority ofhese genes display a pattern of high penetrance but relativelyow prevalence in the population. Recognizing these geneticyndromes is the essential first step to appropriately manag-ng these individuals and their families, and a careful familyistory is a necessary component of this evaluation. The in-roduction of genetic testing has revolutionized the field ofancer risk assessment, and cancer prevention is a realisticoal for affected individuals who adhere to screening guide-ines. The next major challenge is the identification of germ-ine mutations or polymorphisms that may have low pen-trance but high prevalence, as these are the geneticlterations that are likely to have an even greater impact on
olon cancer risk in the population as a whole.
R
20 W.-S. Jo and D.C. Chung
eferences1. St John DJ, McDermott FT, Hopper JL, et al: Cancer risk in relatives of
patients with common colorectal cancer. Ann Intern Med 118:785-790, 1993
2. Fuchs CS, Giovannucci EL, Colditz GA, et al: A prospective study offamily history and the risk of colorectal cancer. N Engl J Med 331:1669-1674, 1994
3. Johns LE, Houlston RS: A systematic review and meta-analysis offamilial colorectal cancer risk. Am J Gastroenterol 96:2992-3003,2001
4. Samowitz WS, Curtin K, Lin HH, et al: The colon cancer burden ofgenetically defined hereditary nonpolyposis colon cancer. Gastroenterol-ogy 121:830-838, 2001
5. Vogelstein B, Fearon ER, Hamilton SR, et al: Genetic alterations duringcolorectal-tumor development. N Engl J Med 319:525-532, 1988
6. Chung DC: The genetic basis of colorectal cancer: Insights into criticalpathways of tumorigenesis. Gastroenterology 119:854-865, 2000
7. Knudson AG Jr: Mutation and cancer: statistical study of retinoblas-toma. Proc Natl Acad Sci U S A 68:820-823, 1971
8. Chung DC, Rustgi AK: DNA mismatch repair and cancer. Gastroen-terology 109:1685-1699, 1995
9. Clayton EW: Ethical, legal, and social implications of genomic medi-cine. N Engl J Med 349:562-569, 2003
10. Bussey HJ, Veale AM, Morson BC: Genetics of gastrointestinal polyp-osis. Gastroenterology 74:1325-1330, 1978
11. Park YJ, Shin KH, Park JG: Risk of gastric cancer in hereditary non-polyposis colorectal cancer in Korea. Clin Cancer Res 6:2994-2998,2000
12. Iwama T, Mishima Y, Utsunomiya J: The impact of familial adenoma-tous polyposis on the tumorigenesis and mortality at the several or-gans. Its rational treatment. Ann Surg 217:101-108, 1993
13. Bjork J, Akerbrant H, Iselius L, et al: Periampullary adenomas andadenocarcinomas in familial adenomatous polyposis: Cumulativerisks and APC gene mutations. Gastroenterology 121:1127-1135,2001
14. Chung DC, Mino M, Shannon KM: Case records of the MassachusettsGeneral Hospital. Weekly clinicopathological exercises. Case 34-2003. A45-year-old woman with a family history of colonic polyps and cancer.N Engl J Med 349:1750-1760, 2003
15. Gurbuz AK, Giardiello FM, Petersen GM, et al: Desmoid tumours infamilial adenomatous polyposis. Gut 35:377-381, 1994
16. Hamilton SR, Liu B, Parsons RE, et al: The molecular basis of Turcot’ssyndrome. N Engl J Med 332:839-847, 1995
17. Lynch HT, Smyrk T, McGinn T, et al: Attenuated familial adenoma-tous polyposis (AFAP). A phenotypically and genotypically distinctivevariant of FAP. Cancer 76:2427-2433, 1995
18. Cao Y, Pieretti M, Marshall J, et al: Challenge in the differentiationbetween attenuated familial adenomatous polyposis and hereditarynonpolyposis colorectal cancer: Case report with review of the litera-ture. Am J Gastroenterol 97:1822-1827, 2002
19. Kinzler KW, Nilbert MC, Su LK, et al: Identification of FAP locusgenes from chromosome 5q21. Science 253:661-665, 1991
20. Nishisho I, Nakamura Y, Miyoshi Y, et al: Mutations of chromosome5q21 genes in FAP and colorectal cancer patients. Science, 253:665-669, 1991
21. Groden J, Thliveris A, Samowitz W, et al: Identification and charac-terization of the familial adenomatous polyposis coli gene. Cell 66:589-600, 1991
22. Miyaki M, Konishi M, Kikuchi-Yanoshita R, et al: Characteristics ofsomatic mutation of the adenomatous polyposis coli gene in colorectaltumors. Cancer Res 54:3011-3020, 1994
23. Miyoshi Y, Nagase H, Ando H, et al: Somatic mutations of the APCgene in colorectal tumors: Mutation cluster region in the APC gene.Hum Mol Genet 1:229-233, 1992
24. Dobbie Z, Spycher M, Mary JL, et al: Correlation between the devel-opment of extracolonic manifestations in FAP patients and mutationsbeyond codon 1403 in the APC gene. J Med Genet 33:274-280, 1996
25. Nagase H, Miyoshi Y, Horii A, et al: Correlation between the location
of germ-line mutations in the APC gene and the number of colorectalpolyps in familial adenomatous polyposis patients. Cancer Res52:4055-4057, 1992
26. Spirio L, Olschwang S, Groden J, et al: Alleles of the APC gene: Anattenuated form of familial polyposis. Cell 75:951-957, 1993
27. Hernegger GS, Moore HG, Guillem JG: Attenuated familial adenoma-tous polyposis: an evolving and poorly understood entity. Dis ColonRectum. 45:127-134, 2002
28. Heppner Goss K, Trzepacz C, Tuohy TM, et al: Attenuated APC allelesproduce functional protein from internal translation initiation. ProcNatl Acad Sci U S A 99:8161-8166, 2002
29. Grady WM: Genetic testing for high-risk colon cancer patients. Gas-troenterology 124:1574-1594, 2003
30. Giardiello FM, Brensinger JD, Petersen GM: AGA technical review onhereditary colorectal cancer and genetic testing. Gastroenterology121:198-213, 2001
31. Burke C: Risk stratification for periampullary carcinoma in patientswith familial adenomatous polyposis: Does Theodore know what todo now? Gastroenterology 121:1246-1248, 2001
32. Harvey JC, Quan SH, Stearns MW: Management of familial polyposiswith preservation of the rectum. Surgery 84:476-482, 1978
33. Bulow C, Vasen H, Jarvinen H, et al: Ileorectal anastomosis is appro-priate for a subset of patients with familial adenomatous polyposis.Gastroenterology 119:1454-1460, 2000
34. Waddell WR, Loughry RW: Sulindac for polyposis of the colon. J SurgOncol 24:83-87, 1983
35. Giardiello FM, Hamilton SR, Krush AJ, et al: Treatment of colonic andrectal adenomas with sulindac in familial adenomatous polyposis.N Engl J Med 328:1313-1316, 1993
36. Labayle D, Fischer D, Vielh P, et al: Sulindac causes regression of rectalpolyps in familial adenomatous polyposis. Gastroenterology 101:635-639, 1991
37. Norton ID, Geller A, Petersen BT, et al: Endoscopic surveillance andablative therapy for periampullary adenomas. Am J Gastroenterol 96:101-106, 2001
38. Aaltonen LA, Salovaara R, Kristo P, et al: Incidence of hereditarynonpolyposis colorectal cancer and the feasibility of molecular screen-ing for the disease. N Engl J Med 338:1481-1487, 1998
39. Lynch HT, de la Chapelle A: Genetic susceptibility to non-polyposiscolorectal cancer. J Med Genet 36:801-818, 1999
40. Lynch HT, de la Chapelle A: Hereditary colorectal cancer. N EnglJ Med 348:919-932, 2003
41. Gryfe R, Kim H, Hsieh ET, et al: Tumor microsatellite instability andclinical outcome in young patients with colorectal cancer. N EnglJ Med 342:69-77, 2000
42. Sankila R, Aaltonen LA, Jarvinen HJ, et al: Better survival rates inpatients with MLH1-associated hereditary colorectal cancer. Gastro-enterology 110:682-687, 1996
43. Smyrk TC, Watson P, Kaul K, et al: Tumor-infiltrating lymphocytesare a marker for microsatellite instability in colorectal carcinoma.Cancer 91:2417-2422, 2001
44. Alexander J, Watanabe T, Wu TT, et al: Histopathological identifica-tion of colon cancer with microsatellite instability. Am J Pathol 158:527-535, 2001
45. Watson P, Lynch HT: The tumor spectrum in HNPCC. Anticancer Res14:1635-1639, 1994
46. Lynch HT, Fusaro RM: The Muir-Torre syndrome in kindreds withhereditary nonpolyposis colorectal cancer (Lynch syndrome): A clas-sic obligation in preventive medicine. J Am Acad Dermatol 41:797-799, 1999
47. Vasen HF, Mecklin JP, Khan PM, et al: The International CollaborativeGroup on Hereditary Non-Polyposis Colorectal Cancer (ICG-HNPCC). Dis Colon Rectum 34:424-425, 1991
48. Vasen HF, Watson P, Mecklin JP, et al: New clinical criteria for hered-itary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) pro-posed by the International Collaborative group on HNPCC. Gastro-enterology 116:1453-1456, 1999
49. Rodriguez-Bigas MA, Boland CR, Hamilton SR, et al: A National Can-
cer Institute Workshop on Hereditary Nonpolyposis Colorectal Can-
Genetics of hereditary colorectal cancer 21
cer Syndrome: Meeting highlights and Bethesda guidelines. J NatlCancer Inst 89:1758-1762, 1997
50. Umar A, Boland CR, Terdiman JP, et al: Revised Bethesda Guidelinesfor hereditary nonpolyposis colorectal cancer (Lynch syndrome) andmicrosatellite instability. J Natl Cancer Inst 96:261-268, 2004
51. Fishel R, Lescoe MK, Rao MR, et al: The human mutator gene homologMSH2 and its association with hereditary nonpolyposis colon cancer.Cell 75:1027-1038, 1993
52. Palombo F, Hughes M, Jiricny J, et al: Mismatch repair and cancer.Nature 367:417, 1994
53. Bronner CE, Baker SM, Morrison PT, et al: Mutation in the DNAmismatch repair gene homologue hMLH1 is associated with heredi-tary non-polyposis colon cancer. Nature 368:258-261, 1994
54. Leach FS, Nicolaides NC, Papadopoulos N, et al: Mutations of a mutShomolog in hereditary nonpolyposis colorectal cancer. Cell 75:1215-1225, 1993
55. Papadopoulos N, Nicolaides NC, Wei YF, et al: Mutation of a mutLhomolog in hereditary colon cancer. Science 263:1625-1629, 1994
56. Nicolaides NC, Papadopoulos N, Liu B, et al: Mutations of two PMShomologues in hereditary nonpolyposis colon cancer. Nature 371:75-80, 1994
57. Liu B, Parsons RE, Hamilton SR, et al: hMSH2 mutations in hereditarynonpolyposis colorectal cancer kindreds. Cancer Res 54:4590-4594,1994
58. Parsons R, Li GM, Longley MJ, et al: Hypermutability and mismatchrepair deficiency in RER� tumor cells. Cell 75:1227-1236, 1993
59. Peltomaki P, Aaltonen LA, Sistonen P, et al: Genetic mapping of alocus predisposing to human colorectal cancer. Science 260:810-812,1993
60. Lindblom A, Tannergard P, Werelius B, et al: Genetic mapping of asecond locus predisposing to hereditary non-polyposis colon cancer.Nat Genet 5:279-282, 1993
61. Fishel R, Ewel A, Lee S, et al: Binding of mismatched microsatelliteDNA sequences by the human MSH2 protein. Science 266:1403-1405, 1994
62. Prolla TA, Pang Q, Alani E, et al: MLH1, PMS1, and MSH2 interac-tions during the initiation of DNA mismatch repair in yeast. Science265:1091-1093, 1994
63. Markowitz S, Wang J, Myeroff L, et al: Inactivation of the type IITGF-beta receptor in colon cancer cells with microsatellite instability.Science 268:1336-1338, 1995
64. Souza RF, Appel R, Yin J, et al: Microsatellite instability in the insulin-like growth factor II receptor gene in gastrointestinal tumours. NatGenet 14:255-257, 1996
65. Yoshitaka T, Matsubara N, Ikeda M, et al: Mutations of E2F-4 trinu-cleotide repeats in colorectal cancer with microsatellite instability.Biochem Biophys Res Commun 227:553-557, 1996
66. Rampino N, Yamamoto H, Ionov Y, et al: Somatic frameshift muta-tions in the BAX gene in colon cancers of the microsatellite mutatorphenotype. Science 275:967-969, 1997
67. Malkhosyan S, Rampino N, Yamamoto H, et al: Frameshift mutatormutations. Nature 382:499-500, 1996
68. Boland CR, Thibodeau SN, Hamilton SR, et al: A National CancerInstitute Workshop on Microsatellite Instability for cancer detectionand familial predisposition: Development of international criteria forthe determination of microsatellite instability in colorectal cancer.Cancer Res 58:5248-5257, 1998
69. Wu Y, Berends MJ, Mensink RG, et al: Association of hereditary non-polyposis colorectal cancer-related tumors displaying low microsatel-lite instability with MSH6 germline mutations. Am J Hum Genet 65:1291-1298, 1999
70. Kolodner RD, Tytell JD, Schmeits JL, et al: Germ-line msh6 mutationsin colorectal cancer families. Cancer Res 59:5068-5074, 1999
71. Wijnen J, de Leeuw W, Vasen H, et al: Familial endometrial cancer infemale carriers of MSH6 germline mutations. Nat Genet 23:142-144,1999
72. Syngal S, Fox EA, Li C, et al: Interpretation of genetic test results forhereditary nonpolyposis colorectal cancer: Implications for clinical
predisposition testing. JAMA 282:247-253, 199973. Moslein G, Tester DJ, Lindor NM, et al: Microsatellite instability andmutation analysis of hMSH2 and hMLH1 in patients with sporadic,familial and hereditary colorectal cancer. Hum Mol Genet 5:1245-1252, 1996
74. Nystrom-Lahti M, Wu Y, Moisio AL, et al: DNA mismatch repair genemutations in 55 kindreds with verified or putative hereditary non-polyposis colorectal cancer. Hum Mol Genet 5:763-769, 1996
75. Wijnen JT, Vasen HF, Khan PM, et al: Clinical findings with implica-tions for genetic testing in families with clustering of colorectal cancer.N Engl J Med 339:511-518, 1998
76. Charbonnier F, Olschwang S, Wang Q, et al: MSH2 in contrast toMLH1 and MSH6 is frequently inactivated by exonic and promoterrearrangements in hereditary nonpolyposis colorectal cancer. CancerRes 62:848-853, 2002
77. Wang Y, Friedl W, Sengteller M, et al: A modified multiplex PCR assayfor detection of large deletions in MSH2 and MLH1. Hum Mutat19:279-286, 2002
78. Winawer S, Fletcher R, Rex D, et al: Colorectal cancer screening andsurveillance: clinical guidelines and rationale—Update based on newevidence. Gastroenterology 124:544-560, 2003
79. Al-Tassan N, Chmiel NH, Maynard J, et al: Inherited variants of MYHassociated with somatic G:C3T:A mutations in colorectal tumors.Nat Genet 30:227-232, 2002
80. Jones S, Emmerson P, Maynard J, et al: Biallelic germline mutations inMYH predispose to multiple colorectal adenoma and somaticG:C3T:A mutations. Hum Mol Genet 11:2961-2967, 2002
81. Sieber OM, Lipton L, Crabtree M, et al: Multiple colorectal adenomas,classic adenomatous polyposis, and germ-line mutations in MYH.N Engl J Med 348:791-799, 2003
82. Sampson JR, Dolwani S, Jones S, et al: Autosomal recessive colorectaladenomatous polyposis due to inherited mutations of MYH. Lancet362:39-41, 2003
83. Enholm S, Hienonen T, Suomalainen A, et al: Proportion and pheno-type of MYH-associated colorectal neoplasia in a population-basedseries of Finnish colorectal cancer patients. Am J Pathol 163:827-832,2003
84. Halford SE, Rowan AJ, Lipton L, et al: Germline mutations but notsomatic changes at the MYH locus contribute to the pathogenesis ofunselected colorectal cancers. Am J Pathol 162:1545-1548, 2003
85. Cheadle JP, Sampson JR: Exposing the MYtH about base excisionrepair and human inherited disease. Hum Mol Genet 12:R159-R165,2003 (suppl 2)
86. Slupska MM, Baikalov C, Luther WM, et al: Cloning and sequencing ahuman homolog (hMYH) of the Escherichia coli mutY gene whosefunction is required for the repair of oxidative DNA damage. J Bacte-riol 178:3885-3892, 1996
87. Nghiem Y, Cabrera M, Cupples CG, et al: The mutY gene: a mutatorlocus in Escherichia coli that generates G.C3T.A transversions. ProcNatl Acad Sci U S A 85:2709-2713, 1988
88. Michaels ML, Miller JH: The GO system protects organisms from themutagenic effect of the spontaneous lesion 8-hydroxyguanine (7,8-dihydro-8-oxoguanine). J Bacteriol 174:6321-6325, 1992
89. Moriya M, Grollman AP: Mutations in the mutY gene of Escherichiacoli enhance the frequency of targeted G:C3T:a transversions in-duced by a single 8-oxoguanine residue in single-stranded DNA. MolGen Genet 239:72-76, 1993
90. Giardiello FM, Brensinger JD, Tersmette AC, et al: Very high risk ofcancer in familial Peutz Jeghers syndrome. Gastroenterology 119:1447-1453, 2000
91. Burdick D, Prior JT: Peutz-Jeghers syndrome. A clinicopathologicstudy of a large family with a 27-year follow-up. Cancer 50:2139-2146, 1982
92. Rowan A, Bataille V, MacKie R, et al: Somatic mutations in the Peutz-Jeghers (LKB1/STKII) gene in sporadic malignant melanomas. J InvestDermatol 112:509-511, 1999
93. Su GH, Hruban RH, Bansal RK, et al: Germline and somatic mutationsof the STK11/LKB1 Peutz-Jeghers gene in pancreatic and biliary can-cers. Am J Pathol 154:1835-1840, 1999
94. Wang ZJ, Churchman M, Campbell IG, et al: Allele loss and mutation

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
22 W.-S. Jo and D.C. Chung
screen at the Peutz-Jeghers (LKB1) locus (19p13.3) in sporadicovarian tumours. Br J Cancer 80:70-72, 1999
95. Wilson DM, Pitts WC, Hintz RL, et al: Testicular tumors with Peutz-Jeghers syndrome. Cancer 57:2238-2240, 1986
96. Cantu JM, Rivera H, Ocampo-Campos R, et al: Peutz-Jeghers syn-drome with feminizing sertoli cell tumor. Cancer 46:223-228, 1980
97. Trau H, Schewach-Millet M, Fisher BK, et al: Peutz-Jeghers syndromeand bilateral breast carcinoma. Cancer 50:788-792, 1982
98. Rebsdorf Pedersen I, Hartvigsen A, Fischer Hansen B, et al: Manage-ment of Peutz-Jeghers syndrome. Experience with patients from theDanish Polyposis Register. Int J Colorectal Dis 9:177-179, 1994
99. Foley TR, McGarrity TJ, Abt AB: Peutz-Jeghers syndrome: A clinico-pathologic survey of the “Harrisburg family” with a 49-year follow-up.Gastroenterology 95:1535-1540, 1988
00. Hemminki A, Markie D, Tomlinson I, et al: A serine/threonine kinasegene defective in Peutz-Jeghers syndrome. Nature 391:184-187, 1998
01. Jenne DE, Reimann H, Nezu J, et al: Peutz-Jeghers syndrome is causedby mutations in a novel serine threonine kinase. Nat Genet 18:38-43,1998
02. Yoo LI, Chung DC, Yuan J: LKB1—A master tumour suppressor of thesmall intestine and beyond. Nat Rev Cancer 2:529-535, 2002
03. Hawley SA, Boudeau J, Reid JL, et al: Complexes between the LKB1tumor suppressor, STRADalpha/beta and MO25alpha/beta are up-stream kinases in the AMP-activated protein kinase cascade. J Biol2:28, 2003
04. Woods A, Johnstone SR, Dickerson K, et al: LKB1 is the upstreamkinase in the AMP-activated protein kinase cascade. Curr Biol 13:2004-2008, 2003
05. Scott RJ, Crooks R, Meldrum CJ, et al: Mutation analysis of the STK11/LKB1 gene and clinical characteristics of an Australian series of Peutz-Jeghers syndrome patients. Clin Genet 62:282-287, 2002
06. Dunlop MG: Guidance on gastrointestinal surveillance for hereditarynon-polyposis colorectal cancer, familial adenomatous polypolis, ju-venile polyposis, and Peutz-Jeghers syndrome. Gut 51:V21-V27,2002 (suppl 5)
07. McGarrity TJ, Kulin HE, Zaino RJ: Peutz-Jeghers syndrome. Am JGastroenterol 95:596-604, 2000
08. Howe JR, Mitros FA, Summers RW: The risk of gastrointestinal carci-noma in familial juvenile polyposis. Ann Surg Oncol 5:751-756, 1998
09. Scott-Conner CE, Hausmann M, Hall TJ, et al: Familial juvenile pol-yposis: Patterns of recurrence and implications for surgical manage-ment. J Am Coll Surg 181:407-413, 1995
10. Desai DC, Murday V, Phillips RK, et al: A survey of phenotypic fea-tures in juvenile polyposis. J Med Genet 35:476-481, 1998
11. Jass JR, Williams CB, Bussey HJ, et al: Juvenile polyposis—A precan-cerous condition. Histopathology 13:619-630, 1988
12. Grotsky HW, Rickert RR, Smith WD, et al: Familial juvenile polyposiscoli. A clinical and pathologic study of a large kindred. Gastroenter-ology 82:494-501, 1982
13. Howe JR, Roth S, Ringold JC, et al: Mutations in the SMAD4/DPC4gene in juvenile polyposis. Science 280:1086-1088, 1998
14. Howe JR, Bair JL, Sayed MG, et al: Germline mutations of the geneencoding bone morphogenetic protein receptor 1A in juvenile polyp-osis. Nat Genet 28:184-187, 2001
15. Woodford-Richens K, Bevan S, Churchman M, et al: Analysis of ge-netic and phenotypic heterogeneity in juvenile polyposis. Gut 46:656-660, 2000
16. Houlston R, Bevan S, Williams A, et al: Mutations in DPC4 (SMAD4)cause juvenile polyposis syndrome, but only account for a minority ofcases. Hum Mol Genet 7:1907-1912, 1998
17. Friedl W, Uhlhaas S, Schulmann K, et al: Juvenile polyposis: Massivegastric polyposis is more common in MADH4 mutation carriers thanin BMPRIA mutation carriers. Hum Genet 111:108-111, 2002
18. Hawkins NJ, Gorman P, Tomlinson IP, et al: Colorectal carcinomasarising in the hyperplastic polyposis syndrome progress through thechromosomal instability pathway. Am J Pathol 157:385-392, 2000
19. Rashid A, Houlihan PS, Booker S, et al: Phenotypic and molecularcharacteristics of hyperplastic polyposis. Gastroenterology 119:323-
332, 200020. Renaut AJ, Douglas PR, Newstead GL: Hyperplastic polyposis of thecolon and rectum. Colorectal Dis 4:213-215, 2002
21. Leggett BA, Devereaux B, Biden K, et al: Hyperplastic polyposis: as-sociation with colorectal cancer. Am J Surg Pathol 25:177-184, 2001
22. Place RJ, Simmang CL: Hyperplastic-adenomatous polyposis syn-drome. J Am Coll Surg 188:503-507, 1999
23. Jass JR, Whitehall VL, Young J, et al: Emerging concepts in colorectalneoplasia. Gastroenterology 123:862-876, 2002
24. German J, Bloom D, Passarge E, et al: Bloom’s syndrome. VI. Thedisorder in Israel and an estimation of the gene frequency in theAshkenazim. Am J Hum Genet 29:553-562, 1977
25. Li L, Eng C, Desnick RJ, et al: Carrier frequency of the Bloom syn-drome blmAsh mutation in the Ashkenazi Jewish population. MolGenet Metab 64:286-290, 1998
26. German J: Bloom’s syndrome: A mendelian prototype of somatic mu-tational disease. Medicine (Baltimore) 72:393-406, 1993
27. German J: Bloom’s syndrome. XX. The first 100 cancers. Cancer GenetCytogenet 93:100-106, 1997
28. Lowy AM, Kordich JJ, Gismondi V, et al: Numerous colonic adenomasin an individual with Bloom’s syndrome. Gastroenterology 121:435-439, 2001
29. Ellis NA, Groden J, Ye TZ, et al: The Bloom’s syndrome gene productis homologous to RecQ helicases. Cell 83:655-666, 1995
30. Neff NF, Ellis NA, Ye TZ, et al: The DNA helicase activity of BLM isnecessary for the correction of the genomic instability of bloom syn-drome cells. Mol Biol Cell 10:665-676, 1999
31. Thompson LH, Schild D: Recombinational DNA repair and humandisease. Mutat Res 509:49-78, 2002
32. Gruber SB, Ellis NA, Scott KK, et al: BLM heterozygosity and the riskof colorectal cancer. Science 297:2013, 2002
33. Cleary SP, Zhang W, Di Nicola N, et al: Heterozygosity for theBLM(Ash) mutation and cancer risk. Cancer Res 63:1769-1771, 2003
34. Laken SJ, Petersen GM, Gruber SB, et al: Familial colorectal cancer inAshkenazim due to a hypermutable tract in APC. Nat Genet 17:79-83,1997
35. Strul H, Barenboim E, Leshno M, et al: The I1307K adenomatouspolyposis coli gene variant does not contribute in the assessment ofthe risk for colorectal cancer in Ashkenazi Jews. Cancer EpidemiolBiomarkers Prev 12:1012-1015, 2003
36. Gryfe R, Di Nicola N, Lal G, et al: Inherited colorectal polyposis andcancer risk of the APC I1307K polymorphism. Am J Hum Genet64:378-384, 1999
37. Rozen P, Fireman Z, Figer A, et al: Colorectal tumor screening inwomen with a past history of breast, uterine, or ovarian malignancies.Cancer 57:1235-1239, 1986
38. Schoen RE, Weissfeld JL, Kuller LH: Are women with breast, endo-metrial, or ovarian cancer at increased risk for colorectal cancer? Am JGastroenterol 89:835-842, 1994
39. Garcia-Patino E, Gomendio B, Lleonart M, et al: Loss of heterozygosityin the region including the BRCA1 gene on 17q in colon cancer.Cancer Genet Cytogenet 104:119-123, 1998
40. Venkitaraman AR: Cancer susceptibility and the functions of BRCA1and BRCA2. Cell 108:171-182, 2002
41. Ford D, Easton DF, Bishop DT, et al: Risks of cancer in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Lancet 343:692-695, 1994
42. Brose MS, Rebbeck TR, Calzone KA, et al: Cancer risk estimates forBRCA1 mutation carriers identified in a risk evaluation program.J Natl Cancer Inst 94:1365-1372, 2002
43. Johannsson O, Loman N, Moller T, et al: Incidence of malignanttumours in relatives of BRCA1 and BRCA2 germline mutation carriers.Eur J Cancer 35:1248-1257, 1999
44. Chen-Shtoyerman R, Figer A, Fidder HH, et al: The frequency of thepredominant Jewish mutations in BRCA1 and BRCA2 in unselectedAshkenazi colorectal cancer patients. Br J Cancer 84:475-477, 2001
45. Peelen T, de Leeuw W, van Lent K, et al: Genetic analysis of a breast-ovarian cancer family, with 7 cases of colorectal cancer linked toBRCA1, fails to support a role for BRCA1 in colorectal tumorigenesis.
Int J Cancer 88:778-782, 2000
1
1
1
1
1
1
1
Genetics of hereditary colorectal cancer 23
46. Niell BL, Rennert G, Bonner JD, et al: BRCA1 and BRCA2 foundermutations and the risk of colorectal cancer. J Natl Cancer Inst 96:15-21, 2004
47. Kirchhoff T, Satagopan JM, Kauff ND, et al: Frequency of BRCA1 andBRCA2 mutations in unselected Ashkenazi Jewish patients with colo-rectal cancer. J Natl Cancer Inst 96:68-70, 2004
48. Vasen HF, Wijnen JT, Menko FH, et al: Cancer risk in families withhereditary nonpolyposis colorectal cancer diagnosed by mutationanalysis. Gastroenterology 110:1020-1027, 1996
49. Chung DC, Rustgi AK: The hereditary nonpolyposis colorectal cancer
syndrome: Genetics and clinical implications. Ann Intern Med138:560-570, 2003
50. Tomlinson IP, Houlston RS: Peutz-Jeghers syndrome. J Med Genet34:1007-1011, 1997
51. Jarvinen H, Franssila KO: Familial juvenile polyposis coli; increasedrisk of colorectal cancer. Gut 25:792-800, 1984
52. Jass JR, Burt R: Hyperplastic polypsosis, in Hamilton SR, Aaltonen LA(eds): WHO international Classification of Tumors: Pathology andGenetics of Tumors of the Digestive System (ed 3). Berlin, Germany,
Springer-Verlag, 2000, pp 135-136