Embed Size (px)
Citation preview

[CANCER RESEARCH56, 2488—2492.June 1. 19961
Advances in Brief
Genetic Progression Model for Head and Neck Cancer: Implications forField Cancerization1
Joseph Califano, Peter van der Riet, William Westra, Homaira Nawroz, Gary Clayman, Steven Piantadosi,Russell Corio, Daniel Lee, Benjamin Greenberg, Wayne Koch, and David Sidransk?Departments of Otolaryngology-Head and Neck Surgery Ii. C., P. v. d. R., H. N., D. L, B. G., W. K., D. S.], Oncology ID. S., S. P.], Biostatistics (S P.], and Pathology1W. W., R. C.]. Johns Hopkins Hospital, Baltimore. Maryland 21205-2195. and M. D. Anderson Cancer Center. Houston. Texas 77030 fG .C.]
Abstract
A genetic progression model ofhead and neck squamous cell cardnomahas not yet been elucidated, and the genetic basis for “fieldcancerization―of the aerodigestive tract has also remained obscure. EIghty-sevenlesionsof the head and neck, including premvasive lesions and benign lesionsassociated with carcinogen exposure, were tested using microsatelliteanalysis for allelic loss at 10 maJor chromosomal lod whIch have beendefined previously. The spectrum of chromosomal loss progressively increased at each histopathological step from benign hyperplasia to dysplasin to carcinoma in situ to invasIve cancer. Adjacent areas of tissue withdifferent histopathological appearance shared common genetic changes,but the more histopathologically advanced areas exhibited additionalgenetic alterations, Abnormal mucosal cells surrounding prelnvasIve andmicroinvaslve lesions shared common genetic alterations with those le
slons and thus appear to arise from a sIngle progenitor clone. Based onthese findings, the local clinical phenomenon of field cancerization seemsto involve the expansion and migration of clonally related preneoplasticcells
Introduction
Annually, there are approximately 500,000 new cases of head andneck squamous cell carcinoma worldwide and over 50,000 cases inthe United States (1). Patients with early stage cancer frequentlymanifest minimal physical findings and symptoms, resulting in delayed diagnosis and poor survival in many patients. Head and neckcancer is often associated with widespread epithelial histopathologicalalterations, and despite successful treatment of a primary head andneck cancer, there is a high likelihood of occurrence of a secondprimary tumor of the upper aerodigestive tract and lung (2—5).These
observations led Slaughter et aL (6) to propose the concept of “fieldcancerization―; the hypothesis that there are carcinogen-inducedchanges throughout the mucosa of the upper aerodigestive tract ofhead and neck cancerpatients.
It is now generally accepted that most sporadic solid tumors resultfrom a multistep process of accumulated genetic alterations (7). In thepast several years, a model for the initiation and progression ofcolorectal cancer has become a paradigm for other human solidtumors, including brain and bladder (8—12).Like colorectal cancer,HNSCC3 is thought to progress through a series of well-definedclinical and histopathological stages.
Areas of frequent chromosomal loss have recently been identified
Received 2/29/96; accepted 4/11/96.Thecostsof publicationof thisarticleweredefrayedin partby thepaymentof page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
I Supported by Lung Cancer Specialized Program of Research Excellence (SPORE)
Grant CA-58l84-Ol.2 To whom requests for reprints should be addressed, at the Head and Neck Cancer
Research Division, 818 Ross Research Building, 720 Rutland Avenue, Baltimore MD,21205.
3 The abbreviations used are: HNSCC, head and neck squamous cell carcinoma; LOH,
loss of heterozygosity; CIS, carcinoma in situ.
in head and neck cancer, but little is known about the timing of thesegenetic changes in malignant transformation (13). A variety of geneticchanges frequently found in primary head and neck cancer haverecently been described, including specific alterations of proto-oncogenes and tumor suppressor genes as well as chromosomal lossesthought to indicate inactivation of other critical tumor suppressorgenes (14—16).Ten tumor suppressor loci were chosen for this analysis based on the following criteria: (a) they have displayed a substantial proportion of loss (>40%) in invasive lesions by allelotypeanalysis and/or (b) they identify a minimal area of loss at a putativetumor suppressor locus (see “Materialsand Methods,―“SelectionofLoci―).
PCR-based microsatellite marker analysis enables analysis of microscopic lesions at different histopathological stages to establish ageneral order of progression for specific genetic changes. This studycorrelated genetic changes and histopathological progression withinindividual premalignant and malignant head and neck lesions, as wellas histopathologically benign lesions frequently observed in patientsat risk for head and neck cancer. Histopathologically distinct areaswithin single lesions were also analyzed and were particularly helpfulin defining molecular progression. Based on this information, we haveconstructed a preliminary genetic progression model for HNSCC.Moreover, we have examined the concept of field cancerization basedon the order of genetic changes established in this model.
Materials and Methods
Selection of IMci. The 9p2l locus corresponds to an area of genetic losscommon to many solid tumors containing p16, a cyclin-dependent kinaseinhibitor involved in cell cycle regulation (17, 18). At this time, this area
demonstrates the locus with the most frequent LOH in HNSCC (16). llql3
includes the bcl-1/int-2 locus, an amplicon carrying the proto-oncogene cyclinD1 (19), one ofthe few proto-oncogenes implicated in HNSCC. Apparent LOH
at this locus actually represents amplification of cyclin D1, as confirmed bystudies using fluorescence in situ hybridization (20). The p53 gene locus iscommonly mutated in HNSCC (16). The p5.3 gene locus is located at l7pl3,which also corresponds to an area of frequent LOH in HNSCC (21). Weanalyzed both LOH at this locus and p53 sequence in those lesions thatdemonstrated LOH to describe the time course of p53 inactivation and llpl3loss in HNSCC progression. Chromosome 3p has been shown to contain atleast three putative HNSCC tumor suppressor loci (22, 23). We analyzedmarkers from each of these three loci for those specimens with histopathologically distinct areas and in lesions biopsied over time. For the sake of clarity,however, only data for the 3p2l locus is included the calculations for LOH inTable 2. 13q21 contains an area with frequent LOH near the retinoblastomalocus that is now thought to identify a second, novel tumor suppressor genelocus (24). Chromosomes 4q26—28and l4q3l—32.lcontain loci mapped bymicrosatellite analysis in our laboratory that are also lost at high rates inHN5 Chromosomes 8 and 6p contain loci thought to contain putativetumor suppressor genes that have not been precisely mapped and are as yet
4 D. Lee and D. Sidransky, submitted for publication.
3 B. Greenberg and D. Sidransky, submitted for publication.
2488
Research. on November 2, 2020. © 1996 American Association for Cancercancerres.aacrjournals.org Downloaded from

DiagnosisBenignsquamous
hyperplasiaDysplasiaCISInvasiveNo.
of lesionsMean loss/total loci ±SDLOH for at least one locus (%)35
0.7 ±1.311 (31)31
212.7 ±1.5 3.3 ±2.030 (97) 21 (100)30―
3.6 ±2.229 (97)
GENETIC PROGRESSION MODEL FOR HEAD AND NECK CANCER
unidentified, but these regions are included since they are lost at a high rate(—40%)in invasive tumors (13). Microsatellite markers included wereD3S1067, D3S1284, D3S1038, D3S1007 (chromosome 3p), D451613, FABP2(chromosome 4), D6S265, TCTE, D6S105 (chromosome 6p), D8S261,
D8S262, D8S273, D8S257, D8S167(chromosome 8), IFN-cs, D9S736, D9S171(chromosome 9p21), D11S873, JNT-2, PYGM (chromosome 11q13),D13S170, D13S133 (chromosome l3q2l), D14S81, D14S51 (chromosomel4q), TP53, and CHRNB-1 (chromosome 17pl3).
Tissue and DNA Extraction. Eighty-seven specimens from 83 patientswith head and neck lesions of the upper aerodigestive tract were analyzed. Fourpatients were biopsied twice at an interval of 1—12months. Thirty-four lesionswere diagnosed as benign squamous hyperplasia with no evidence of neoplastic transformation, 31 lesions were diagnosed as dysplasia, 21 lesions werediagnosed as squamous cell CIS, and 1 lesion was diagnosed as a small focusof squamous carcinoma with microscopic invasion arising in a background ofbenign squamous hyperplasia. Five of these lesions had sharp borders demarcating histopathologically distinct areas within a single biopsy. Tissue wasobtained from archival, paraffin-embedded blocks from the the Johns HopkinsDepartment of Surgical Pathology or from fresh-frozen tissue obtained withconsent from Johns Hopkins Hospital patients and from the M. D. AndersonCancer Center Head and Neck Cancer Tumor Bank. Tissue was chosen solelyon the basis of the initial histopathological diagnosis from the pathologydepartments of both institutions. Representative sections from tissue used forDNA extractionwerestainedwithH&E,anddiagnosiswas confirmedforeachlesion by two pathologists (R. C. and W. W.). Fresh-frozen tissue was meticulously dissected on a cryostat to ensure that the specimen contained at least75% epithelial cells. Approximately thirty-five l2-@am sections were thencollected and placed in 1% SDS/proteinase K (0.5 mg/ml) at 58°Cfor 24 h.Paraffin-embedded tissue was sectioned into twenty-five l4-@msections. Eachindividual section was placed on a glass slide and individually microdissectedusing a dissecting microscope to obtain >75% epithelial cells. The sampleswere placed in xylene overnight to remove the paraffin, pelleted in 70%ethanol, dried, and incubated in SDS/proteinase K at 58°Cfor 72 h. Digestedtissue from both sources was then subjected to phenol-chloroform extractionand ethanol precipitation as described previously. Normal control DNA wasobtained by either (a) venipuncture and isolation of lymphocyte DNA asdescribed previously (25); (b) microdissection of purely nonepithelial normal
tissue in the previously mentioned archival, paraffin-embedded biopsy specimens; or, if necessary, (c) isolation of DNA from distant (normal), nonepithehal, paraffin-embedded tissue from archival paraffin blocks other than thebiopsy specimen in the manner described above.
Analysis for Allellc Loss. Microsatellite markers suitable for PCR analysiswere obtained from Research Genetics. Prior to amplification, 50 ng of oneprimer from each pair was end labeled with [y-32P]ATP (20 mCi; Amersham)and T4 kinase (New England Biolabs) in a total volume of 50 j.d. PCRreactions were carried out in a total volume of 12.5 pJ containing 10 nggenomic DNA, 0.2 ng labeled primer, and 15 ng ofeach unlabeled primer. ThePCR buffer included 16.6mi@iammonium sulfate, 67 mMTris (pH 8.8), 6.7 mMmagnesium chloride, 10 mM (3-mercaptoethanol, and 1% DMSO, to whichwere added 1.5 mM deoxynucleotide triphosphates and 1.0 units Taq DNApolymerase (Boehringer Mannheim). PCR amplifications of each primer setwere performed for 30 to 35 cycles consisting of denaturation at 95°Cfor 305, annealing at 50—60°C for 60 s, and extension at 70°C for 60 s as described.
One third of the PCR product was separated on 8% urea-formamide-polyacrylamide gels and exposed to film from 4 to 48 h as described. Forinformative cases, alleic loss (or possible allelic imbalance in the case of thellql3 locus; Refs. 19 and 20) was scored if one allele was significantlydecreased in tumor DNA (>50%) when compared to the same allele in normalcontrol DNA.
Lesions were initially analyzed for at least two microsatellite markers per
locus selected from the 10 major lcd displaying loss in primary invasive headand neck squamous cell tumors (13). Additional markers from the samechromosomal region were tested until at least 80% of the lesions displayed aninformative result in the region of interest.
Sequence Analysis. PurifiedDNA from primarylesions was subjectedtoPCR amplification of the coding portion of the p53 gene in two fragments asdescribed (26). The two PCR fragments including exons 5—6(500 bp) andexons 7—8(750 bp) were extracted using phenol-chloroform and precipitatedwith 70% ethanol. This DNA was then subjected to a direct sequence analysis
of the p53 gene using Taq-CS polymerase cycle sequencing (27, 28). Samplesdisplaying mutations were reamplified and resequenced to confirm mutations.
Statistical Analysis. The primary statistical outcome for the analysis ofthese data is the proportion of chromosomal loci showing LOH at differenthistopathological points in the progression to cancer. To make comparisonsbetween the different loci, it is convenient to model the proportion with LOHas a quantity which increases from benign squamous hyperplasia throughdysplasia, CIS, and reaching a maximum with invasive cancer. To accomplishthis, we used a simple model with the following characteristics: (a) the
diagnostic categories from benign to invasive cancer were represented on anordinal scale; (b) the proportion with LOH increases in a linear fashion acrossdiagnoses; and (c) the slopes and intercepts of these linearly increasingproportions can differ from locus to locus. This degree of structure permits usto quantify and test differences between loci using a familiar Poisson regression approach. It is true that the assumption of an ordinal scale acrossdiagnostic categories is arbitrary, as is the linear component of the Poissonmodel. However, the purpose of the analysis is to quantify and reveal structurein the data rather than to model them rigorously.
The results of this analysis demonstrate that the increase in LOH across thediagnostic categories (modelled as a linear trend) is significantly greater than0 (P < 0.0001). Pairwise tests comparing trend in different loci do not showstatistically significant differences.
Results
Timingof GeneticLoss Weexamined87 preinvasivelesionsandpaired normal samples using microsatellite analysis to establish thepresence of allelic loss at 10 critical loci frequently lost in HNSCC(see “Materialsand Methods―). The incidence of LOH at all loci(mean allelic loss) corresponding to each stage of histopathologicaldiagnosis is shown in Table 1. Nearly all samples ofdysplasia and CISand less than one third of benign epithelial hyperplastic lesionsdisplayed LOH in at least one of these specific loci. Calculation of themean number of loss events (maximum of 10) shows that LOH at anincreasing number of loci correlates with histopathological progression. As seen in Table 2, the highest frequency of LOH occurred inbenign squamous hyperplastic lesions at 9p21 (20%), followed by3p2l (16%) and l7pl3 (1 1%). This finding indicates that LOH atthese loci is an early event in HNSCC tumor progression. Dysplasia,considered to be an intermediate step in histopathological progression,showed additional loci with LOH at increased incidence at 11q13(29%), l3q2l (32%), and 14q31 (23%). As expected, there was anincrease in frequency for losses at 9p2l and 3p2l in the step frombenign hyperplasia to dysplasia, and then an additional increase in CISto a plateau level that was not greater in the invasive cancers. This isconsistent with the role of 9p2l and 3p2l as early loss events. Laterevents in progression are indicated by a significant rise in the frequency of LOH (at least 2-fold) from the CIS to the invasive stage.These loci included (Ip (19% and 38%, respectively), 8p (21% and40%), 8q (20% and 38%), and 4q26—28(21% and 47%). Statisticalanalysis shows that both the initial proportion of LOH and the rates ofprogression differ significantly among the loci (P < 0.0001, see“Materialsand Methods―).
a A @aiof 10 chromosomal loci were tested, minimal losses were initially defined in
30 invasive tumors (for 3p2l, 6p, 8, and llql3). Subsequently, the minimal region wasfurther mapped in at least 70 primary tumors at 9p21, Ylpl3, 13q2l, 4q26—28, andl4q3l—32.l.
2489
Research. on November 2, 2020. © 1996 American Association for Cancercancerres.aacrjournals.org Downloaded from

ChromosomallocusBenign
squamoushyperplasiaDysplasiaCISInvasive@'9p2l8/35(20)17/30(57)17/21
(80)54/74(73)3p2l5/31(16)15/29(52)12/20(60)18/27(67)llpl34/35(11)10/30(33)9/17(47)34/62(55)llql32/34(6)9/31
(29)8/20(40)14/23(61)l3q211/32(3)9/28 (32)7/20 (35)31/60(52)l4q31—32.l1/31(3)7/30 (23)6/19 (32)32/73(44)6p3/34(8)6/29(20)4/21
(19)9/24(38)8q1/31(3)6/28(21)4/20(20)10/26(38)8p4/28(14)3/24(13)4/19(21)8120(40)4q26—281/26(4)2/23(9)4/19(21)30/64(47)
GENETIC PROGRESSION MODEL FOR HEAD AND NECK CANCER
Table 2 LOHfor histopathological diagnosis and chromosomal locus― changes with histopathological progression. The identification of allelic losses in tumors within the context of a tumor progression modelhas led to the identification of critical putative tumor suppressorgenes. The initial description of molecular progression proposed byFearon and Vogelstein (8) indicated that (a) tumors progress via theactivation of oncogenes and the inactivation of tumor suppressorgenes, each producing a growth advantage for a clonal population ofcells; (b) specific genetic events generally occur in a distinct order of
progression; but (c) the order of progression is not necessarily thesame for each individual tumor, and thus it is the accumulation ofgenetic events that determines tumor progression.
In the HNSCC progression model derived in this study, allelic losshas been used as a molecular marker for inactivation of putative tumorsuppressor genes. However, allelic imbalance may also occur from
oncogene amplification (e.g., cyclin D1 on 11q13). In the case ofHNSCC, chromosomal loss and amplification at these 10 loci havebeen confirmed by other complementary methods (29). A preliminarymolecular progression model developed from this work is presented inFig. 3. This model supports the initial observations of the colorectalmolecular progression model, in that (a) both oncogenes and tumorsuppressor genes are involved in tumor progression; (b) specificevents in head and neck cancer generally occur in a distinct order ofprogression, with loss at 9p2l or 3p among the earliest detectableevents; and (c) it is the accumulation and not necessarily the order of
.v_ D351038@3p K D351067@
@ D351284
D4S1613‘q26-28< FABP-2
V D651056p@ TCTE
8i@ D85261
k@1;@çj L@N'N1
LNIJ L:wr-i@ .-@
@@ c:@i@
t@N@@@\] __ ____ ____
— Lfffl‘@‘@N@@ ____
L@ c@D E@tJ
@ L@N@
—@
Diagnosis
‘IValues given in loss/informative cases (% loss).
b From previously published and unpublished data in 30—70 tumors for each locus.
LOH of l7pl3 is thought to result in the loss of a second p53 alleleafter the first allele has been inactivated by a mutational event.
However, our previous work indicated that p53 mutation was uncommon in preinvasive lesions, occurring in only 25% of CIS lesions andrarely in dysplastic lesions (16). In invasive tumors, LOH of l'7poccurs in 80% of lesions with a p.53 mutation. To test specifically forp53 inactivation, every lesion with Ylpl3 loss was sequenced. Wefound that none of the benign squamous hyperplastic lesions, onlythree of nine dysplastic lesions, and three of nine CIS lesions withVlpl3 loss had detectable p53 mutations. This observation is consistent with other reports indicating the presence of a second tumorsuppressor gene or amplification indicating a putative proto-oncogeneat Yip (21 , 29, 30). The high frequency of 17pl 3 LOH in early lesionsunaccompanied by p53 mutation also implies that Yip loss may heralda separate, earlier event in head and neck cancer progression.
Evidencefrom IntralesionalProgression.To furtherdeterminethe general order of progression of early genetic events, areas ofintralesional histopathological progression were evaluated. Five lesions with histopathologically distinct areas were analyzed by micro
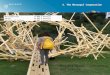
dissecting each area separately and comparing patterns of genomicmicrosatellite loss. Allelograms (diagrams showing the pattern ofLOH at multiple tumor suppressor gene loci) for two of these lesionsare shown in Fig. 1, along with representative autoradiographs in Fig.2. In these cases, the histopathologically advanced area displayed thesame pattern of LOH (i.e. , the same genetic events) as the lessadvanced area (Fig. lb). However, in four of the five cases (includingFig. la), the histopathologically advanced area demonstrated addi
tional LOH at one or more loci. We were also able to map the locationof identical boundaries between an area of loss and retention at one ormore loci in four of five of these pairs of lesions, including thoseshown in Fig. 1. If two samples from one patient share concordantlosses of identical alleles with identical boundaries between loss and
retention, this provides strong evidence that the cells in the two areasare clonally related. This finding is consistent with the hypothesis thatmore benign-appearing, histopathologically distinct areas adjacent tomore malignant regions in aerodigestive mucosa arise from a commonclonal progenitor. Progression, therefore, is thought to involve clonaloutgrowth of a subpopulation of cells with yet additional geneticalterations. Although the number of lesions examined in this fashionwas not sufficient for a statistical analysis, we noted frequent LOH ateither 9p2 I or 3p21 shared by both histopathologically early andadvanced regions, supporting the role of these loci as important earlyevents in tumor progression.
Discussion
In the past several years, tumor progression models have beenconstructed for a few tumor types by correlating specific genetic
a bd@pJa@ia CL5@ B@bT d@pJasia
L@fffl
L@MIIi
@INfll@@N1@]
L N1@@1
LJ{LjF N1@1
al @@D8S273D85167
9p21< IFN-xD95736D95171
11q13< PYGMINT-2D115873
1@21 .@zz:I:D13S170D135133
14124@zz::1D14S256D14551
17p13@z::::I:CHRNB-1TP -53
Fig. I. Genetic analysis of lesions undergoing histopathological progression. a, microdissected lesion shows genetic progression with loss at tip and I 1q13 accompanyinghistopathological progression from dysplasia to CIS within the biopsy sample. Noteidentical boundaries between LOH () and retention (@) at 3p, 8q, and 9p2l. Similargenetic progression was noted in three other biopsy samples with histopathologicalprogression. b, microdissected lesion showing identical genetic changes despite histopathological progression from benign squamous hyperplasia (BSH) to dysplasia. Again,note identical boundaries of LOH (U) and retention (@) at 3p and 11q13. NI, noninformative.
2490
Research. on November 2, 2020. © 1996 American Association for Cancercancerres.aacrjournals.org Downloaded from

GENEFIC PROGRESSION MODEL FOR HEAD AND NECK CANCER
genetic “pathway―to malignancy. However, the natural clinical history of benign squamous hyperplasia is not usually associated with
progression to carcinoma (although Fig. lb is consistent with a benignhyperplasia undergoing progression to dysplasia). This is consistentwith statistical models based on age-specific incidence of head andneck cancer that this malignancy requires multiple (perhaps 10 ormore) genetic alterations to develop an invasive phenotype (10).Therefore, it might be expected that lesions with only a few geneticevents would display a rather benign morphological phenotype. It isalso a reasonable, although an untested hypothesis, that other subclinical lesions or histopathologically normal mucosa may contain similargenetic alterations and may be placed early on the progression pathway.
Genetic changes in areas of differing histopathology containedwithin individual lesions have also been examined, similar to recentinvestigations of genetic progression in dysplastic colonic crypts (32).These lesions quite possibly provide snapshots of tumor progression,demonstrating common early genetic events, the common (clonal)
origin of these histopathologically distinct areas, and the associationof additional genetic loss with progression to a more malignantphenotype.
Our observations provide insight into a possible mechanism forfield cancerization. This term was originally coined by Slaughter et a!.(6) in a studyof oralcancer.Theyexaminedresectionspecimensofinvasive squamous cell carcinoma of the oral cavity and found his
topathological abnormalities in the epithelium surrounding the invasive cancer. These abnormalities included additional areas of invasivecancer, CIS, dysplasia, hyperkeratosis, and epithelial hyperplasia withfrequent multiple foci of the more aggressive lesions. Both Slaughteret a!. (6) and, more recently, other investigators have reported anincreased incidence of second primary head and neck, pulmonary, andesophageal cancers in patients with head and neck cancer (33). Basedon these observations, field cancerization was used to describe thephenomenon by which an entire field of tissue developed malignant orpremalignant change in response to a carcinogen.
Our analysis of lesions with areas of apparently benign mucosaadjacent to premalignant lesions demonstrate that early genetic eventsmay be shared by cells in a local anatomical area, which are apparently derived from a common clone. Other studies of areas of histopathological abnormality surrounding lung carcinomas show allelespecific loss in both chromosome 3p and 9p loci, consistent with acommon clonal origin of these cells (34, 35). The original observations of Slaughter et a!. (6) may be interpreted in the context of thesedata, suggesting that areas of histopathological abnormality surrounding malignant and premalignant lesions are all generally derived froma common single progenitor clone. In fact, Slaughter et a!. (6) notedthat “forty-threeof these eighty-eight patients [with] two separatetumors occurred in the same anatomical area of the oral cavity.―Subsequent genetic events in various subclones produce differentphenotypic alterations, resulting in a variety of histopathologicallydiverse regions in a local anatomical area and possible outgrowth of
Fig. 3. Genetic progression of HNSCC. Genetic changes associated with the histopathological progression of HNSCC based on loss of chromosomal material (allelic loss). Geneticalterations have been placed prior to the lesion where the frequency of the particular event plateaus. It is the accumulation and not necessarily the order of genetic events that determinesprogression. A small fraction of benign squamous hyperplastic lesions contain 9p2l or 3p2l loss, suggesting that an unidentified precursor lesion (or cells) may also give rise todysplasia. Candidate tumor suppressor genes include p16 (9p2l), p53 (lip), and retinoblastoma (13q), and a candidate proto-oncogene includes cyclin D1 (I 1q13).
2491
NDCLY'
55
S..
D8S273 I
,tFig. 2. Representative autoradiographs from genetic analysis of lesion shown in Fig.
Ia. Autoradiographs show concordant loss of the top allele for microdissected areas ofdysplasia (DYS) and CIS compared to retained normal genomic control (NL) for markerD9S171 (top), concordant loss of the bottom allele for marker D85273 (bottom), andselective loss of the bottom allele in the area of CIS for marker D11S873 (middle),demonstrating genetic progression from dysplasia to CIS at this locus.
genetic events that determines progression. This model is certainly notcomplete, and the temporal placement of two closely occurring eventsin progression may in fact be arbitrary. Our data support the notionthat events spaced at greater intervals in the model are likely to occurin the indicated order in most tumors. Progression by accumulation ofgenetic events is also supported by the fact that generally “late―genetic events occasionally occur as the only detectable change inearly lesions (e.g., one benign hyperplastic lesion showed loss solelyat the 8p locus). In many tumor types, including HNSCC, p53 mactivation apparently occurs in the transition from the preinvasive to theinvasive state (16). A second Ylpl3 locus may be altered earlier inprogression. Existence of an alternate gene in this region has beenimplied in the genetic progression of brain and breast cancer (30, 31).
The finding that 30% of histopathologically benign squamous hyperplastic lesions already consist of a clonal population of cells withshared genetic alterations characteristic of those seen in head and neckcancer suggests that a substantial proportion of these lesions are on a
D9S171
Dl 1S873
Research. on November 2, 2020. © 1996 American Association for Cancercancerres.aacrjournals.org Downloaded from

GENETIC PROGRESSION MODEL FOR HEAD AND NECK CANCER
16. Boyle, J. 0., Hakim, J., Koch, W., van der Riet, P., Hruban, R. H., Roa, R. A., Correo,R., Eby, Y. J., Ruppert, J. M., and Sidransky, D. The incidence of p53 mutationsincreases with progression of head and neck cancer. Cancer Res., 53: 4477-4480,1994.
17. Kamb, A., Gruis, N., Weaver-Feldhaus, J., Liu, 0., Harshman, K., Tavtigian, S. V.,Stockert, E., Day, R. S., III, Johnson, B. B., and Skolnick, M. H. A cell cycle regulatorpotentially involved in genesis of many tumor types. Science (Washington DC), 264:436—440,1994.
18. Nabori, T., Miura, K., Wu, D. J., Lois, A., Takahayasbi, K., and Carson, D. A.Deletions of the cydin-dependent kinase-4 inhibitor gene in multiple human cancers.Nature (Lend.), 368: 753—756,1994.
19. Callender, T., El-Naggar, A. K., Lee, M., Frankenthaler, R., Luna, M. A., andBatsakis, 3. G. PRAD-l (CCND1)/cyclin Dl oncogene amplification in primary headand neck squamous cell carcinoma. Cancer (Phila.), 74: 152—158,1994.
20. Lese, C. M., Rossie, K. M., Appel, B. N., Reddy, J. K., Johnson, J. T., Myers, E. N.,and Gollin, S. M. Visualization of Int2 and Hstl amplification in oral squamous cellcarcinomas. Genes Chromosomes & Cancer, 12: 288—295,1995.
21. Soder, A. I., Hopman, A. H. N., Ramaekers, F. C. S., Conradt, C., and Bosch, F. X.Distinct nonrandom patterns of chromosomal aberrations in the progression of squamous cell carcinomas of the head and neck. Cancer Res., 55: 5030—5037,1995.
22. Wu, C. L., Sloan, P., Read, A. P., Harris, R., and Thakker, N. Deletion mapping onthe short arm of chromosome 3 in squamous cell carcinoma of the oral cavity. CancerRes., 54: 6484—6488,1994.
23. Maestro, R., Gasparotto, D., Vuksavljevic, 1., Barzan, L., Sulfaro, S., and Biocchi, M.Three discrete regions of deletion in head and neck cancers. Cancer Rca., 53:5775—5779,1993.
24. Yoo, G. H., Xu, H. J., Brennan, J. A., Westra, W., Hruban, R. H., Koch, W., Benedict,W. F., and Sidransky, D. Infrequent inactivation of the retinoblastoma gene despitefrequent loss of chromosome l3q in head and neck squamous cell carcinoma. CancerRes., 54: 4603-4606, 1994.
25. Baker, S. J., Preisinger, A. C., Jessup, J. M., Paraskeva, C., Markowitz, S., Wilson,J. K., Hamilton, S., and Vogelstein, B. p53 gene mutations occur in combination withl7p alleic deletions as late events in colorectal tumongenesis. Cancer Res., 50:7717—7722, 1990.
26. van 6cr Riet, P., Karp, D., Farmer, E.,Wei, Q.. Grossman, L, Tokino, K., Ruppert,J. M., and Sidransky, D. Progression of basal cell carcinoma through loss of chromosome 9q and inactivation of a single p53 allele. Cancer Res., 54: 25—27,1994.
27. Snvastava, A. K., Montanaro, V., and Kere, J. Simplified template preparation andimproved direct sequencing using Taq polymerase. PCR Methods Appl., 1: 255-256,1992.
28. Lawyer, F. C, Stoffel, S., Saiki, R. K., Chang, S. Y., Landre, P. A., Abramson, R. D.,and Gelfand, D. H. High-level expression, purification, and enzymatic characterization of full-length Thermusaquaticus DNA polymerase and a truncated form deficientin 5' to 3' exonuclease activity. PCR Methods Appl., 2: 275—287,1993.
29. Speicher, M. R., Howe, C., Crony, P., du Manoir, S., Costa, J., and Ward, D. C.Comparative genomic hybridization detects novel deletions and amplifications inhead and neck squamous cell carcinomas. Cancer Res., 55: 1010-1013, 1995.
30. Saxena, A., Clark, W. C., Robertson, J. T., Ikejiri, B., Oldfield, E. H., and All, I. U.Evidence for the involvement of a potential second tumor suppressor gene onchromosome 17 distinct from p53 in malignant astrocytomas. Cancer Res., 52:6716—6721, 1992.
31. Merlo, G. R., Venesio, T., Bernardi, A., Cropp, C. S., Diella, F., Cappa, A. P.,Callahan, R., and Uscia, D. S. Evidence for a second tumor suppressor gene on l'lplinked to high S-phase index in primary human breast carcinomas. Cancer Genet.Cytogenet., 76: 106—111, 1994.
32. Boland, C. R., Sato, J., Appelman, H. D., Bresalier, R. S., and Feinberg, A. P.Microallelotyping defines the sequence and tempo of allelic losses at tumor suppressor gene loci during colorectal cancer progression. Nat. Med., 1: 902—909.1995.
33. Shikhani, A. H., Matanoski, G. M., Jones, M. M., Kashima, H. K., and Johns, M. E.Multiple primary malignancies in head and neck cancer. Arch. Otolaryngol. Head &NeckSurg.. 112: 1172—1179.1986.
34. Hung, J., Kushimoto, Y., Sugio, K., Virmani, A., Mclntire, D. D., Minna, J. D., andGazdar, A. F. Allele-specific chromosome 3p deletions occur at an early stage in thepathogenesis of lung carcinoma. J. Am. Med. Assoc., 273: 558—563,1995.
35. Kushimoto, Y., Sugio, K., Hung, J. Y., Virmani, A. K., Mclntire, D. D., Minna, J. D.,and Gazdar, A. F. Allele-specific loss in chromosome 9p loci in preneoplastic lesionsaccompanying non-small-cell lung cancers. J. Nail. Cancer Inst., 87: 1224—1229,1995.
36. Bedi, G., Westra, W., Gabrielson, E., Koch, W., and Sidransky, D. Multiple head andneck tumors: evidence for clonal origin. Cancer Res., 56: 2484—2487,1996.
37. Brennan, J. A., Mao, L., Hniban, R., Boyle, J. 0., Eby, Y. J., Koch, W. M., Goodman,S. N., and Sidransky, D. Molecular assessment of histopathological staging insquamous-cell carcinoma of the head and neck. N. EngI. J. Med., 332: 429—435,1995.
38. Mao, L., Schoenberg, M. P., Scicchitano, M., Erozan, Y. S., Merlo, A., Schwab, D.,and Sidransky, D. Molecular detection of primary bladder cancer by microsatelliteanalysis. Science (Washington DC), 271: 659—662, 1996.
2492
a subclone that has acquired a particular selective growth advantage.Findings in our laboratory related to the origin of these multipleprimary tumors are discussed by Bedi et a!. (36).
A genetic progression model for head and neck cancer has severalimportantimplications.From a scientificviewpoint,identificationoftargeted tumor suppressor genes and proto-oncogenes at these locimay be critical for understanding the biological initiation, behavior,and progression of head and neck cancer. Determination of the geneticstatus of a primary tumor or of the tissues surrounding invasive cancer
may have prognostic significance for tumor recurrence and/or progression of remaining clonal epithelial populations toward a moremalignant phenotype. For example, the presence of transformingclonal events in surrounding normal epithelium at the time of cancerresection may predict late local recurrence in some patients. Identification of early genetic events would also provide the best targets forscreening of saliva or sputum to identify premalignant transformation.Knowledge of early events could also be used to identify residualclonal populations by molecular margin analysis to more accuratelyassess the success of surgical resections (37). A recent molecularanalysis of urine sediment identified microsatellite alteration or LOHin 95% of cancer patients in our laboratory, similar strategies could beadopted for screening of saliva specimens (38). Moreover, prevalentand early events such as 9p2l loss offer attractive targets for therapeutic strategies based on pharmacological or genetic modification inlesions of all stages.
References
1. Vokes, E. E., Weichselbaum, R. R., Lippman, S. M., and Hong, W. K. Head and neckcancer. N. Engl. J. Med., 328: 184—194,1993.
2. Cooper, J. S., Pajak, T. F.. Rubin, P., Tupchong, L., Brady, L. W., Leibel, S. A.,Laramore, G. E., Marcial, V. A., Davis, L. W., and Cox, J. D. Second malignanciesin patients who have head and neck cancer; incidence, effect on survival andimplications for chemoprevention based on the RTOG experience. Int. J. Radiat.Oncol. Biol. Phys., 17: 449—456,1989.
3. Liciardello, J. T.. Spitz, M. R., and Hong, W. K. Multiple primary cancer in patientswith cancer of the head and neck: second cancer of the head and neck, esophagus, andlung. Lot.J. Radiat. Oncol. Biol. Phys., 17: 467—476,1989.
4. Christensen, P., Joergensen, K., Munk, J., and Oesterlind, A. Hyperfrequency ofpulmonary cancer in a population of 415 patients treated for laryngeal cancer.Laryngoscope, 97: 612-6124, 1987.
5. Tepperman, B. S., and Fitzpatrick, P. J. Second respiratory and upper digestive tractcancers after oral cancer. Lancet, 2: 547—549,1981.
6. Slaughter, D. P., Southwick, H. W., and Smejkal, W. “Fieldcancetizmion@'in oralstratified squamous epithelium: clinical implications of multicentric origin. Cancer(Phila.), 6: 963—968,1953.
7. Renan, M. J. How many mutations are required for tumorigenesis? Implications fromhuman cancer data. Mol. Carcinog., 7: 139—146,1993.
8. Fearon, E. R., and Vogelstein, B. A genetic model for colorectal tumorigenesis. Cell,61: 759—767,1990.
9. Vogelstein, B., Fearon, E. R., Hamilton, S. R., Kern, S. E., Preisinger, A. C., Lepport,M., Nakamura, Y., White, R., Smits, A. M., and Bos, J. L. Genetic alterations duringcolorectal tumor development. N. Engl. J. Med., 319: 525—532,1988.
10. Sidransky, D., Mikkelsen, T., Schwechheimer, K., Rosenblum, M. L., Cavanee, W.,and Vogelstein, B. Clonal expansion of p53 mutant cells is associated with braintumor progression. Nature (Lond.), 355: 846—847,1992.
11. Simoneau, A. R., and Jones, P. A. Bladder cancer the molecular progression toinvasive disease. World J. Urol., 12: 89—95,1994.
12. Dalbagni, G., Presti, J., Reuter, V., Fair, W. R., and Cordon-Casio, C. Geneticalterations in bladder cancer. Lancet, 342: 469—471, 1993.
13. Nawroz, H.. van der Riet, P., Hruban, R. H., Koch, W. M., Ruppert, J. M., andSidransky, D. Allelotype of head and neck squamous cell carcinoma. Cancer Res., 54:1152—1155,1994.
14. Cowan, J. M., Becken, M. A., Ahmed-Swan, S., and Weichselbaum, R. R. Cytogenetic evidence of the multistep origin of head and neck squamous cell carcinomas. J.Nail. Cancer Inst., 84: 793—797,1992.
15. Ishitoya, J., Toriyama, M., Oguchi, N., Kitamura, K., Oshina, M., Asano, K., andYamamoto, T. Gene amplification and overexpression of EGF receptor in squamouscell carcinoma of the head and neck. Br. J. Cancer, 59: 559—562,1989.
Research. on November 2, 2020. © 1996 American Association for Cancercancerres.aacrjournals.org Downloaded from

1996;56:2488-2492. Cancer Res Joseph Califano, Peter van der Riet, William Westra, et al. Implications for Field CancerizationGenetic Progression Model for Head and Neck Cancer:
Updated version
http://cancerres.aacrjournals.org/content/56/11/2488
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/56/11/2488To request permission to re-use all or part of this article, use this link
Research. on November 2, 2020. © 1996 American Association for Cancercancerres.aacrjournals.org Downloaded from