Embed Size (px)
DESCRIPTION
Project in Biology.
Citation preview

Angelman Syndrome
Angelman syndrome is a neuro-genetic disorder characterized by severe intellectual and developmental disability, sleep disturbance, seizures, jerky movements (especially hand-flapping), frequent laughter or smiling, and usually a happy demeanor.
AS is a classic example of genomic imprinting in that it is caused by deletion or inactivation of genes on the maternally inherited chromosome 15 while the paternal copy, which may be of normal sequence, is imprinted and therefore silenced. The sister syndrome, Prader-Willi syndrome, is caused by a similar loss of paternally inherited genes and maternal imprinting. AS
is named after a British pediatrician, Harry Angelman, who first described the syndrome in 1965. An older, alternative term for AS, "happy puppet syndrome", is generally considered pejorative and stigmatizing so it is no longer the accepted term. People with AS are sometimes known as "angels", both because of the syndrome's name and because of their youthful, happy appearance.
Treatment
There is currently no cure available. The epilepsy can be controlled by the use of one or more types
of anticonvulsant medications. However, there are difficulties in ascertaining the levels and types of
anticonvulsant medications needed to establish control, because AS is usually associated with having
multiple varieties of seizures, rather than just the one as in normal cases of epilepsy. Many families
use melatonin to promote sleep in a condition which often affects sleep patterns. Many individuals with
Angelman syndrome sleep for a maximum of 5 hours at any one time. Mild laxatives are also used
frequently to encourage regular bowel movements, and early intervention with physiotherapy is
important to encourage joint mobility and prevent stiffening of the joints. Speech and Language Therapy
is commonly employed to assist individuals with Angelman syndrome and their communicative issues.
Those with the syndrome are generally happy and contented people who like human contact and play.
People with AS exhibit a profound desire for personal interaction with others. Communication can be
difficult at first, but as a child with AS develops, there is a definite character and ability to make
themselves understood. People with AS tend to develop strong non-verbal skills to compensate for their
limited use of speech. It is widely accepted that their understanding of communication directed to them
is much larger than their ability to return conversation. Most afflicted people will not develop more than
5–10 words, if any at all.[9]
Seizures are a consequence, but so is excessive laughter,[10] which is a major hindrance to early
diagnosis.

Canavan Disease
Canavan disease, also called Canavan-Van Bogaert-Bertrand disease is an autosomal recessive degenerative disorder that causes progressive damage to nerve cells in the brain, and is one of the most common degenerative cerebral diseases of infancy. It is caused by a deficiency of the enzyme aminoacylase 2, and is one of a group of genetic diseases referred to as aleukodystrophies. It is characterized by degeneration of myelin in the phospholipid layer insulating the axon of a neuron and is associated with a gene located on human chromosome 17.
The signs and symptoms of this disease usually begin in early infancy; however, the course of the condition can be quite variable. Infants with Canavan disease typically appear normal for the first few months of life. By age 3 to 5 months, affected infants begin having problems with development, including a delay in
motor skills such as turning over, controlling head movement, and sitting without support. These infants typically also have weak muscle tone (hypotonia), unusually large head size (macrocephaly), abnormal posture, and intellectual disability. Feeding and swallowing difficulties, seizures, and sleep disturbances may also develop.
Treatment
There is no cure for Canavan disease, nor is there a standard course of treatment. Treatment is
symptomatic and supportive. There is also an experimental treatment using lithium citrate. When a
person has Canavan disease, his or her levels of N-acetyl aspartate are chronically elevated. The lithium
citrate has proven in a rat genetic model of Canavan disease to be able to significantly decrease levels
of N-acetyl aspartate. When tested on a human, the subject reversed during a two week wash-out
period after withdrawal of lithium.
The investigation revealed both decreased N-acetyl aspartate levels in regions of the brain tested and
magnetic resonance spectroscopic values that are more characteristic of normal development and
myelination. This evidence suggests that a larger controlled trial of lithium may be warranted as
supportive therapy for children with Canavan disease.[6]
In addition there are experimental trials of gene therapy, published in 2002, involving using a healthy
gene to take over for the defective one that causes Canavan disease. [7] In human trials, the results of
which were published in 2012, this method appeared to improve the life of the patient without long-
term adverse effects during a 5 year follow-up.

Coeliac Disease
Coeliac disease is an autoimmune disorder of
the small intestine that occurs in genetically
predisposed people of all ages from middle infancy
onward. Symptoms include pain and discomfort in
the digestive tract, chronic constipation
and diarrhoea, failure to thrive (in
children), anaemia and fatigue, but these may be
absent, and symptoms in other organ systems have
been described. Vitamin deficiencies are often noted
in people with coeliac disease owing to the reduced
ability of the small intestine to properly absorb nutrients from food.
Coeliac disease is caused by a reaction to gliadin, a prolamin (gluten protein) found in wheat, and similar
proteins found in the crops of the tribe Triticeae (which includes other common grains such
as barley and rye). Upon exposure to gliadin, and specifically to three peptides found in prolamins, the
enzyme tissue transglutaminase modifies the protein, and the immune system cross-reacts with the
small-bowel tissue, causing an inflammatory reaction. That leads to a truncating of the villi lining the
small intestine (called villous atrophy). This interferes with the absorption of nutrients because
the intestinal villi are responsible for absorption. The only known effective treatment is a lifelong gluten-
free diet. While the disease is caused by a reaction to wheat proteins, it is not the same aswheat allergy.
Treatment
Diet
At present, the only effective treatment is a lifelong gluten-free diet. No medication exists that will
prevent damage or prevent the body from attacking the gut when gluten is present. Strict adherence to
the diet allows the intestines to heal, leading to resolution of all symptoms in most cases and, depending
on how soon the diet is begun, can also eliminate the heightened risk of osteoporosis and intestinal
cancer and in some cases sterility.[76] The diet can be cumbersome; failure to comply with the diet may
cause relapse.
Dietitian input is generally requested to ensure the person is aware which foods contain gluten, which
foods are safe, and how to have a balanced diet despite the limitations. In many countries, gluten-free
products are available on prescription and may be reimbursed by health insurance plans. Gluten-free
products are usually more expensive and harder to find than common gluten-containing foods. [77] Since
ready-made products often contain traces of gluten, some coeliacs may find it necessary to cook from
scratch.

Even while on a diet, health-related quality of life (HRQOL) may be lower in people with coeliac disease.
Studies in the United States have found that quality of life becomes comparable to the general
population after staying on the diet, while studies in Europe have found that quality of life remains
lower, although the surveys are not quite the same. Men tend to report more improvement than
women.[87] Some have persisting digestive symptoms or dermatitis herpetiformis, mouth ulcers,
osteoporosis and resultant fractures. Symptoms suggestive of irritable bowel syndrome may be present,
and there is an increased rate of anxiety, fatigue, dyspepsia and musculoskeletal pain.
Charcot-Marie Tooth Disease
Charcot–Marie–Tooth disease (CMT), also known as Charcot–Marie–Tooth neuropathy, hereditary motor and sensory neuropathy (HMSN) and peroneal muscular atrophy (PMA), is a genetically and clinically heterogeneous group of inherited disorders of the peripheral nervous system characterised by progressive loss of muscle tissue and touch sensation across various parts of the body. Currently incurable, this disease is one of the most common inherited neurological disorders affecting
approximately 1 in 2,500 people[1][2] equating to approximately 26,000 people in the United Kingdom and 128,000 people in the United States. CMT was previously classified as a subtype of muscular dystrophy.
Causes
Charcot–Marie–Tooth disease is caused by mutations that cause defects in neuronal proteins. Nerve
signals are conducted by an axon with a myelin sheath wrapped around it. Most mutations in CMT affect
the myelin sheath, but some affect the axon.
The most common cause of CMT (70-80% of the cases) is the duplication of a large region on the short
arm of chromosome 17 that includes the gene PMP22. Some mutations affect the gene MFN2, which
codes for a mitochondrial protein. Cells contain separate sets of genes in their nucleus and in
their mitochondria. In nerve cells, the mitochondria travel down the long axons. In some forms of CMT,
mutated MFN2 causes the mitochondria to form large clusters, or clots, which are unable to travel down
the axon towards thesynapses. This prevents the synapses from functioning.
Treatment

There is no cure for CMT, but physical therapy, occupational therapy, braces and other orthopedic devices, and even orthopedic surgery can help individuals cope with the disabling symptoms of the disease. In addition, pain-killing drugs can be prescribed for individuals who have severe pain.
Physical and occupational therapy, the preferred treatment for CMT, involves muscle strength training, muscle and ligament stretching, stamina training, and moderate aerobic exercise. Most therapists recommend a specialized treatment program designed with the approval of the person's physician to fit individual abilities and needs. Therapists also suggest entering into a treatment program early; muscle strengthening may delay or reduce muscle atrophy, so strength training is most useful if it begins before nerve degeneration and muscle weakness progress to the point of disability.
Stretching may prevent or reduce joint deformities that result from uneven muscle pull on bones. Exercises to help build stamina or increase endurance will help prevent the fatigue that results from performing everyday activities that require strength and mobility. Moderate aerobic activity can help to maintain cardiovascular fitness and overall health. Most therapists recommend low-impact or no-impact exercises, such as biking or swimming, rather than activities such as walking or jogging, which may put stress on fragile muscles and joints.
Many CMT patients require ankle braces and other orthopedic devices to maintain everyday mobility and prevent injury. Ankle braces can help prevent ankle sprains by providing support and stability during activities such as walking or climbing stairs. High-top shoes or boots can also provide support for weak ankles. Thumb splints can help with hand weakness and loss of fine motor skills. Assistive devices should be used before disability sets in because the devices may prevent muscle strain and reduce muscle weakening. Some individuals with CMT may decide to have orthopedic surgery to reverse foot and joint deformities.
Color Blindness
Color blindness, or color vision deficiency, is the inability or decreased ability to see color, or perceive color differences, under normal lighting conditions. Color blindness affects a significant percentage of the population. There is no actual blindness but there is a deficiency of color vision. The most usual cause is a fault in the development of one or more sets of retinal cones that perceive color in light and transmit that information to the optic nerve. This type of color blindness is usually a sex-
linked condition. The genes that produce photopigments are carried on the X chromosome; if some of these genes are missing or damaged, color blindness will be expressed in males with a higher probability than in females because males only have one X chromosome (in females, a functional gene on only one of the two X chromosomes is sufficient to yield the needed photopigments).
Treatment

Inherited color vision problems cannot be treated or corrected. For the most common type of color blindness—red-green color deficiency—no treatment is needed, because you function normally. You may not be aware that you do not see colors the way they are seen by others.
Some acquired color vision problems can be treated, depending on the cause. For example, if a cataract is causing a problem with color vision, surgery to remove the cataract may restore normal color vision.
You can find ways to help make up for a color vision problem, such as:
Wearing colored contact lenses. These may help you see differences between colors. But these lenses don't provide normal color vision and can distort objects.
Wearing glasses that block glare. People with severe color vision problems can see differences between colors better when there is less glare and brightness.
Learning to look for cues like brightness or location, rather than colors. For example, you can learn the order of the three colored lights on a traffic signal.
Cri Du Chat Syndrome
Cri-du-chat (cat's cry) syndrome, also known as 5p- (5p minus) syndrome, is a chromosomal condition that results when a piece of chromosome 5 is missing. Infants with this condition often have a high-pitched cry that sounds like that of a cat. The disorder is characterized by intellectual disability and delayed development, small head size (microcephaly), low birth weight, and weak muscle tone (hypotonia) in infancy. Affected individuals also have distinctive facial features, including widely set eyes (hypertelorism), low-set ears, a small jaw, and a rounded face. Some children with cri-du-chat syndrome are born with a heart defect.
Treatment
Care is supportive. No treatment is available for cri-du-chat syndrome. Genetic counseling is indicated:
o Female patients are fertile and can deliver viable affected offspring, with an estimated recurrence risk of 50%.
o Recurrence risk for a de novo case is 1% or less. Rare recurrences in chromosomally healthy parents are probably the result of gonadal mosaicism for the 5p deletion in one of the parents.
o If a parent is a balanced carrier of a structural rearrangement, the risk is substantially high. The risk should be assessed based on the type of structural rearrangement and its pattern of segregation.
Chronic medical problems such as upper respiratory tract infections, otitis media, and severe constipation require appropriate treatment.Use the relatively good receptive skills to encourage language and communicative development rather than relying on traditional verbal methods. Early stimulation and introduction to sign language are effective means of developing communication skills (50% of children are able to use sign language to communicate). Behavior modification programs may be successful in managing hyperactivity, short

attention span, low threshold for frustration, and self-stimulatory behaviors (eg, head-banging, hand-waving). Visual-motor coordination computerized training improves the visuospatial performance in a child affected by cri-du-chat syndrome.
Cystic Fibrosis
Cystic fibrosis (CF), also known as mucoviscidosis, is a genetic disorder that affects mostly the lungs but also the pancreas, liver,kidneys and intestine. Long-term issues include difficulty breathing and coughing up sputum as a result of frequent lung infections. Other symptoms include sinus infections, poor growth, fatty stool, clubbing of the finger and toes, and infertility in males among others. Different
people may have different degrees of symptoms.
CF is an autosomal recessive disorder. It is caused by the presence of mutations in both copies of the gene for the protein cystic fibrosis transmembrane conductance regulator (CFTR). Those with a single working copy are carriers and otherwise mostly normal. CFTR is involved in production of sweat, digestive fluids, and mucus. When not functional usually thin secretions become thick. The condition is diagnosed by a sweat test and genetic testing.[1] Screening of infants
at birth take place in some areas of the world.
There is no cure for cystic fibrosis. Lung infections are treated with antibiotics which may be given intravenously, inhaled, or by mouth. Sometimes the antibiotic azithromycin is used long term. Inhaled hypertonic saline and salbutamol may also be useful. Lung transplantation may be an option if lung function continues to worsen. Pancreatic enzyme replacement and fat soluble vitaminsupplementation are important, especially in the young. While not well supported by evidence, many people use airway clearance techniques such as chest physiotherapy. The average life expectancy is between 37 and 50 years in the developed world. Lung problems are responsible for death in 80% of
people.
Down Syndrome

Down syndrome is a chromosomal condition that is associated with intellectual disability, a characteristic facial appearance, and weak muscle tone (hypotonia) in infancy. All affected individuals experience cognitive delays, but the intellectual disability is usually mild to moderate.
People with Down syndrome may have a variety of birth defects. About half of all affected children are born with a heart defect. Digestive abnormalities, such as a blockage of the intestine, are less common.
Individuals with Down syndrome have an increased risk of developing several medical conditions. These include gastroesophageal reflux, which is a backflow of acidic stomach contents into the esophagus, and celiac disease, which is an intolerance of a wheat protein called gluten. About 15 percent of people with Down syndrome have an underactive thyroid gland (hypothyroidism). The thyroid gland is a butterfly-shaped organ in the lower neck that produces hormones. Individuals with Down syndrome also have an increased risk of hearing and vision problems. Additionally, a small percentage of children with Down syndrome develop cancer of blood-forming cells (leukemia).
Delayed development and behavioral problems are often reported in children with Down syndrome. Affected individuals' speech and language develop later and more slowly than in children without Down syndrome, and affected individuals' speech may be more difficult to understand. Behavioral issues can include attention problems, obsessive/compulsive behavior, and stubbornness or tantrums. A small percentage of people with Down syndrome are also diagnosed with developmental conditions called autism spectrum disorders, which affect communication and social interaction.
People with Down syndrome often experience a gradual decline in thinking ability (cognition) as they age, usually starting around age 50. Down syndrome is also associated with an increased risk of developing Alzheimer disease, a brain disorder that results in a gradual loss of memory, judgment, and ability to function. Approximately half of adults with Down syndrome develop Alzheimer disease. Although Alzheimer disease is usually a disorder that occurs in older adults, people with Down syndrome usually develop this condition in their fifties or sixties
Causes
Down syndrome is caused by having three copies of the genes on chromosome 21, rather than the usual two. The parents of the affected individual are typically genetically normal. Those who have one child with Down syndrome have about a 1% risk of having a second child with the syndrome, if both parents are found to have normal karyotypes.
The extra chromosome content can arise through several different ways. The most common cause (about 92–95% of cases) is a complete extra copy of chromosome 21, resulting in trisomy 21. In 1.0 to 2.5% of cases, some of the cells in the body are normal and others have trisomy 21, known as mosaic Down syndrome. The other common mechanisms that can give rise to Down syndrome include: a Robertsonian translocation, isochromosome, or ring chromosome. These contain additional material from chromosome 21 and occur in about 2.5% of cases. An isochromosome results when the two long arms of a chromosome separate together rather than the long and short arm separating together during egg or sperm development.
Treatment
Although there is no cure for Down syndrome, children born with the condition can lead productive
lives. Everyone born with Down syndrome exhibits some level of cognitive impairment, but this usually

falls within the mild to moderate range. Just like other children, babies with Down syndrome will learn
basic skills -- such as sitting, walking, talking, and self-care (such as toilet training and bathing) -- but they
will do so at a delayed pace. Early intervention programs, including physical therapy, begun shortly after
birth, can help strengthen muscles for these basic motor skills.
Regular medical care to treat the chronic health problems associated with Down syndrome is also
important. Children with Down syndrome should receive regular vision and hearing testing, be
evaluated forthyroid dysfunction, and receive the regular childhood immunizations.
Over the years, a variety of laws have been passed to provide people with disabilities, including Down
syndrome, equal protection under the law. These laws include Section 504 of The Rehabilitation Act of
1973, the Education for All Handicapped Children Act of 1975, and the Americans with Disabilities Act of
1991. Children with Down syndrome can attend school, and many join regular classes. They are able to
participate in recreational, vocational, and social activities in their communities.
Some adults with Down syndrome live with their families; some live in group homes with other
individuals with Down syndrome; and others live independently. Many people with Down syndrome
hold jobs. The opportunities for people with Down syndrome are great, and there is no reason not to
expect these individuals to make lasting, positive contributions to society.
Duchenne Muscular Dystrophy
Duchenne muscular dystrophy (DMD) is a recessive X-
linked form of muscular dystrophy, affecting around 1 in
3,600 males, which results in muscle degeneration and
eventual death.[1] The disorder is caused by a mutation
in the dystrophin gene, located on the human X
chromosome, which codes for the protein dystrophin.
Dystrophin is an important structural component within
muscle tissue that provides structural stability to
the dystroglycan complex (DGC) of the cell membrane.
While both sexes can carry the mutation, females rarely
exhibit signs of the disease.
Symptoms usually appear in male children between the
age of 2 and 3 and may be visible in early infancy. Even though symptoms do not appear until early
infancy, laboratory testing can identify children who carry the active mutation at birth. Progressive
proximal muscle weakness of the legs and pelvis associated with a loss of muscle mass is observed first.
Eventually this weakness spreads to the arms, neck, and other areas. Early signs may
include pseudohypertrophy (enlargement of calf and deltoid muscles), low endurance, and difficulties in
standing unaided or inability to ascend staircases. As the condition progresses, muscle tissue

experiences wasting and is eventually replaced by fat and fibrotic tissue (fibrosis). By age 10, braces may
be required to aid in walking but most patients are wheelchair dependent by age 12. Later symptoms
may include abnormal bone development that lead to skeletal deformities, including curvature of the
spine. Due to progressive deterioration of muscle, loss of movement occurs, eventually leading to
paralysis. Intellectual impairment may or may not be present but if present, does not progressively
worsen as the child ages. The average life expectancy for individuals afflicted with DMD is around 25.
Treatment
There is no current cure for DMD, and an ongoing medical need has been recognized by regulatory
authorities. Phase 1-2a trials with exon-skipping treatment for certain mutations have halted decline
and produced small clinical improvements in walking.
Treatment is generally aimed at controlling the onset of symptoms to maximize the quality of life, and
include the following:
Corticosteroids such as prednisolone and deflazacort increase energy and strength and defer
severity of some symptoms.
Randomised control trials have shown that beta2-agonists increase muscle strength but do not
modify disease progression. Follow-up time for most RCTs on beta2-agonists is only around 12
months and hence results cannot be extrapolated beyond that time frame.
Mild, non-jarring physical activity such as swimming is encouraged. Inactivity (such as bed rest) can
worsen the muscle disease.
Physical therapy is helpful to maintain muscle strength, flexibility, and function.
Orthopedic appliances (such as braces and wheelchairs) may improve mobility and the ability for
self-care. Form-fitting removable leg braces that hold the ankle in place during sleep can defer the
onset of contractures.
Appropriate respiratory support as the disease progresses is important.
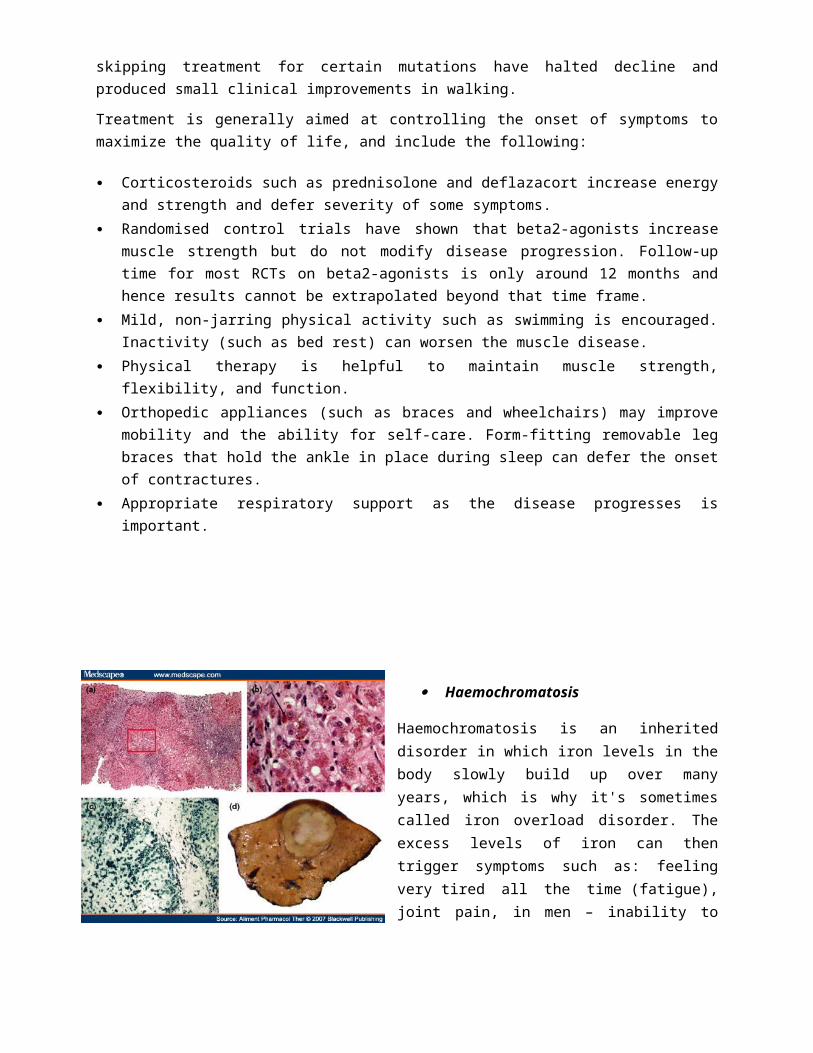
Haemochromatosis
Haemochromatosis is an inherited disorder in which iron levels in the body slowly build up over many years, which is why it's sometimes called iron overload disorder. The excess levels of iron can then trigger symptoms such as: feeling very tired all the

time (fatigue), joint pain, in men – inability to get or maintain an erection (erectile dysfunction), in women – absent periods
Haemochromatosis is an inherited condition caused by a faulty gene called HFE, that allows a person to absorb too much iron from food. Normally, the body only absorbs as much as it needs. The excess iron starts building up in the body and causing problems.
Treatment
Haemochromatosis responds well to treatment, which aims to remove excess iron from the body.
The usual treatment is quite simple. Blood is removed from the body on a regular basis – about the same amount taken in a blood donation, around 500ml (roughly a pint).
This leads to an overall drop in iron levels. For people unable to use phlebotomy for medical reasons, a medication called deferasirox can be used as an alternative. This is known as chelation therapy.
Haemophilia
Hemophilia is a group of inherited blood disorders in which the blood does not clot properly.
Bleeding disorders are due to defects in the blood vessels, the coagulation mechanism, or the blood platelets. An affected individual may bleed spontaneously or for longer than a healthy person after injury or surgery. The blood
coagulation mechanism is a process which transforms the blood from a liquid into a solid, and involves several different clotting factors. The mechanism generates fibrin when it is activated, which together with the platelet plug, stops the bleeding. When coagulation factors are missing or deficient the blood does not clot properly and bleeding continues. Patients with Hemophilia A or B have a genetic defect which results in a deficiency in one of the blood clotting factors.
Causes
o Haemophilia A is a recessive X-linked genetic disorder involving a lack of functional clotting
Factor VIII and represents 80% of haemophilia cases.o Haemophilia B is a recessive X-linked genetic disorder involving a lack of functional clotting
Factor IX. It comprises approximately 20% of haemophilia cases.[11]
o Haemophilia C is an autosomal genetic disorder (i.e. not X-linked) involving a lack of functional
clotting Factor XI. Haemophilia C is not completely recessive, as heterozygousindividuals also
show increased bleeding.
Treatments

o Most cases of haemophilia are severe and require preventative treatment (prophylaxis). This
involves regular injections of clotting factor medication.o When your child is young, you will be trained to give them the injections. They will be taught
how to inject themselves when they are older. This will avoid the need for regular hospital
appointments.o In some cases, injections may be given into a device called an implantable port, which can be
surgically placed under the skin. This port is connected to a blood vessel near the heart,
meaning you don't need to try to find a vein for every injection.o If you're having preventative treatment, you'll need regular follow-up appointments with your
care team so your progress can be monitored.o Preventative treatment is usually continued until you're fully grown. After this point it may be
possible to change to on-demand treatment, but you may be advised to switch back to
preventative treatment if you experience any episodes of significant bleeding.
Klinefelter Syndrome
Klinefelter syndrome is a chromosomal condition that affects male physical and cognitive development. Its signs and symptoms vary among affected individuals.
Affected individuals typically have small testes that do not produce as much testosterone as usual. Testosterone is the hormone that directs male sexual development before birth and during puberty. A shortage of testosterone can lead to delayed or incomplete puberty, breast enlargement (gynecomastia), reduced facial and body hair, and an inability to have biological children (infertility). Some affected individuals also have genital differences including undescended testes (cryptorchidism), the opening of the urethra on the underside of the penis (hypospadias), or an unusually small penis (micropenis).
Older children and adults with Klinefelter syndrome tend to be taller than their peers. Compared with unaffected men, adults
with Klinefelter syndrome have an increased risk of developing breast cancer and a chronic inflammatory disease called systemic lupus erythematosus. Their chance of developing these disorders is similar to that of women in the general population.
Children with Klinefelter syndrome may have learning disabilities and delayed speech and language development. They tend to be quiet, sensitive, and unassertive, but personality characteristics vary among affected individuals.
Causes
The extra chromosome is retained because of a nondisjunction event during meiosis I (gametogenesis).
Nondisjunction occurs when homologous chromosomes, in this case the X and Y sex chromosomes, fail
to separate, producing a sperm with an X and a Y chromosome. Fertilizing a normal (X) egg with this
sperm produces an XXY offspring where this sperm could have yielded either XX or XY.

Another mechanism for retaining the extra chromosome is through a nondisjunction event
during meiosis II in the female. Nondisjunction will occur when sister chromatids on the sex
chromosome, in this case an X and an X, fail to separate. (meiosis) An XX egg is produced which, when
fertilized with a Y sperm, yields XXY offspring. This XXY chromosome arrangement is one of the most
common genetic variations from the XY karyotype, occurring in about 1 in 500 live male births. [5] See
also Triple X syndrome
Variations
48,XXYY and 48,XXXY occur in 1 in 18,000–50,000 male births. The incidence of 49,XXXXY is 1 in 85,000
to 100,000 male births.[26]These variations are extremely rare. Additional chromosomal material can
contribute to cardiac, neurological, orthopedic and other anomalies.
Males with Klinefelter syndrome may have a mosaic 47,XXY/46,XY constitutional karyotype and varying
degrees of spermatogenic failure. Mosaicism 47,XXY/46,XX with clinical features suggestive of Klinefelter
syndrome is very rare. Thus far, only about 10 cases have been described in literature.[27]
Analogous XXY syndromes are known to occur in cats—specifically, the presence
of calico or tortoiseshell markings in male cats is an indicator of the relevant abnormal karyotype. As
such, male cats with calico or tortoiseshell markings are a model organism for Klinefelter syndrome.
Treatment
The genetic variation is irreversible. Often individuals that have noticeable breast tissue
or hypogonadism experience depression and/or social anxiety because they are outside of social norms.
This is academically referred to as psychosocial morbidity. At least one study indicates that planned and
timed support should be provided for young men with Klinefelter syndrome to ameliorate current poor
psychosocial outcomes. By 2010 over 100 successful pregnancies have been reported
using IVF technology with surgically removed sperm material from males with Klinefelter syndrome.
Neurofibromatosis
Neurofibromatosis (NF) refers to a number of inherited conditions that are clinically and genetically distinct and carry a high risk of tumor formation, particularly in the brain.[1] Neurofibromatosis is an autosomal dominant disorder, which means only one copy of the affected gene is needed for the disorder to develop. Therefore, if only one parent has
neurofibromatosis, his or her children have a 50% chance of developing the condition as well (it is rarely
the case that one person has the mutated gene twice, which would imply a 100% chance of their children developing NF). The severity in affected individuals can vary; this may be due to variable expressivity. Approximately half of cases are due to de novo mutations and no other affected family members are seen. It affects males and females equally. In addition, some individuals may have mosaic NF, in which some but not all cells of the body carry the mutation. The neurofibromatoses are as follows:
Neurofibromatosis type I, in which the nerve tissue grows tumors (neurofibromas) that may be benign and may cause serious damage by compressing nerves and other tissues.
Neurofibromatosis type II, in which bilateral acoustic neuromas (tumors of the vestibulocochlear nerve or cranial nerve 8 (CN VIII) also known as schwannoma) develop, often leading to hearing loss.
Schwannomatosis, in which painful schwannomas develop on cranial, spinal and peripheral nerves.
Treatment
For individuals diagnosed with neurofibromatosis type 1 (NF1), routine examinations should focus on the potential complications.
Annual examinations permit early detection of problems, decreasing morbidity and improving quality of life.
Annual eye examinations are important in early detection of optic nerve lesions.Cutaneous examination performed at each visit should look for new neurofibromas or progression of preexisting lesions. Plexiform neurofibromas may be locally invasive, therefore clinical evaluation should be directed at determining the extent of involvement and detecting evidence of bony erosion or nerve entrapment.
Skeletal involvement, including scoliosis, hemihypertrophy, or long-bone modeling defects, should be documented.
Blood pressure should be checked at each visit and hypertension treated promptly if detected. Hypertension workup should include evaluation for pheochromocytoma (ie, measurement of urinary catecholamines and metanephrines) and testing for renal artery stenosis. Percutaneous transluminal renal artery angioplasty may, in some cases, effectively treat renal artery stenosis secondary to fibromuscular dysplasia.
Interval history should focus on subtle sensory or motor symptoms such as paresthesia, radiculopathy, weakness, or muscle atrophy.
Patients should be asked about incontinence. At each visit, minor changes in the sensory or motor examination should be documented carefully.
Symptoms of spinal cord neurofibromas may be subtle and slowly progressive; prompt identification and early surgical intervention allow for optimal outcome.
Removal of neurofibromas for medical or cosmetic indications is one of the most common procedures on individuals with NF1.
Recent advances in laser technology have permitted nonsurgical removal of small, cutaneous neurofibromas.
However, careful surgical resection of small or large neurofibromas may leave an even smaller, less prominent scar.

Although laser treatment has been used for various cutaneous, hyperpigmented lesions (eg, port-wine stains, tattoos), it has not yet proven successful in permanent removal of café-au-lait spots.
Use of chemotherapy to treat malignant peripheral nerve sheath tumors (MPNSTs) that are unresectable or metastatic has been debated for a number of years, with less than optimal outcomes using a variety of combinations of agents. More recently, in vitro studies looking at a broader range of agents targeting the Ras and/or other relevant pathways have shown some promising results.
Farnesyl transferases used in combination with lovastatin have shown synergistic effects in growth inhibition of MPNST cell lines in vitro.[23]
Sorafenib also appears to inhibit MPNST cell growth in vitro.[24]
A rapamycin complex 1 inhibitor (RAD001) demonstrated decreased tumor cell growth when used alone, and, when used in combination with erlotinib (an epidermal growth factor receptor tyrosine kinase inhibitor), showed even further growth inhibition and tumor cell apoptosis.[25]
Hyaluronan oligomers, another promising agent, has shown efficacy in slowing growth of MPNSTs in animal models. These small molecules, when used in combination with a traditional chemotherapy agent (doxorubicin), substantially inhibit tumor growth.[26]
In the near future, studies such as these will likely lead to preclinical and then clinical trials for patients with unresectable MPNSTs.
The use of chemotherapy, especially with carboplatin and vincristine have been shown to be effective in controlling the progression of optic nerve gliomas.
Phenylketonuria
Phenylketonuria (commonly known as PKU) is an inherited disorder that increases the levels of a substance called phenylalanine in the blood. Phenylalanine is a building block of proteins (an amino acid) that is obtained through the diet. It is found in all proteins and in some artificial sweeteners. If PKU is not treated, phenylalanine can build up to harmful levels in the body, causing intellectual disability and other serious health problems.
Less severe forms of this condition, sometimes called variant PKU and non-PKU hyperphenylalaninemia, have a smaller risk of brain damage. People with very mild cases may not require treatment with a low-phenylalanine diet.
Babies born to mothers with PKU and uncontrolled phenylalanine levels (women who no longer follow a low-phenylalanine diet) have a significant risk of intellectual disability because they are exposed to very high levels of phenylalanine before birth. These infants may also have a low birth weight and grow more slowly than other children. Other characteristic medical problems include heart defects or other heart problems, an abnormally small head size (microcephaly), and behavioral problems. Women with PKU and uncontrolled phenylalanine levels also have an increased risk of pregnancy loss.
CausesA genetic mutation causes phenylketonuria. In a person with PKU, this defective gene causes a lack of or deficiency of the enzyme that's needed to process an amino acid called phenylalanine. A dangerous buildup of phenylalanine can develop when a person with PKU eats foods that are high in protein, such as milk, cheese, nuts or meat.

For a child to inherit PKU, both the mother and father must have and pass on the defective gene. This pattern of inheritance is called autosomal recessive. It's possible for a parent to have the defective gene, but not have the disease. This is called being a carrier. If only one parent has the PKU gene, there's no risk of passing PKU to a child, but it is possible for the child to be a carrier.
Most often, PKU is passed to children by two parents who are carriers of the disorder, but don't know it.
Treatment
There is no cure for PKU, but treatment can prevent intellectual disabilities and other health problems. A person with PKU should receive treatment at a medical center that specializes in the disorder.
The PKU Diet
People with PKU need to follow a diet that limits foods with phenylalanine. The diet should be followed carefully and be started as soon after birth as possible. In the past, experts believed that it was safe for people to stop following the diet as they got older. However, they now recommend that people with PKU stay on the diet throughout their lives for better physical and mental health.1,2It is especially important for a pregnant woman with PKU to strictly follow the low-phenylalanine diet throughout her pregnancy to ensure the healthy development of her infant.3People with PKU need to avoid various high-protein foods, including: Milk and cheese, Eggs, Nuts, Soybeans, Beans, Chicken, beef, or pork, Fish, Peas, Beer.People with PKU also need to avoid the sweetener aspartame, which is in some foods, drinks, medications, and vitamins. Aspartame releases phenylalanine when it is digested, so it raises the level of phenylalanine in a person's blood.1Often, people with PKU also have to limit their intake of lower-protein foods, such as certain fruits and vegetables. However, a PKU diet can include low-protein noodles and other special products.The amount of phenylalanine that is safe to consume differs for each person. Therefore, a person with PKU needs to work with a health care professional to develop an individualized diet. The goal is to eat only the amount of phenylalanine necessary for healthy growth and body processes but not any extra. Frequent blood tests and doctor visits are necessary to help determine how well the diet is working. Some relaxation of the diet may be possible as a child gets older, but the recommendation today is lifelong adherence to the diet.2,4 Following the diet is especially important during pregnancy. However, the PKU diet can be very challenging. Getting support from friends and family or a support group can help. Sticking with the diet ensures better functioning and improved overall health.

















