Embed Size (px)
Citation preview
General Debility General Debility The Palliative ResponseThe Palliative Response
F. Amos Bailey, M.D.F. Amos Bailey, M.D.
General DebilityGeneral DebilityDefinitionDefinition
Declining functional status with Declining functional status with
limited prognosislimited prognosis
Condition may include multiple medical Condition may include multiple medical problemsproblems
None of medical conditions necessarily None of medical conditions necessarily
terminal on its ownterminal on its own

Know Signs of Life’s Know Signs of Life’s EndEnd
While no one knows how long anyone will While no one knows how long anyone will live, live,
there are certain signs there are certain signs
that health is very poor and declining that health is very poor and declining
and time could be limitedand time could be limited
Palliative Evaluation of Palliative Evaluation of Suffering in DebilitySuffering in Debility
PhysicalPhysical – Poorly controlled physical symptomsPoorly controlled physical symptoms
(e.g., pain, anorexia, asthenia)(e.g., pain, anorexia, asthenia)
EmotionalEmotional – Distress in the face of physical declineDistress in the face of physical decline
Palliative Evaluation of Palliative Evaluation of Suffering in DebilitySuffering in Debility
Social Social – Distress from need for additional Distress from need for additional
supportive servicessupportive services
Spiritual/ExistentialSpiritual/Existential– Existential angst Existential angst – Feeling of hopelessnessFeeling of hopelessness

Palliative ResponsePalliative ResponseOverviewOverview
Symptom ManagementSymptom Management– Development of plan of care to palliate Development of plan of care to palliate
symptoms symptoms not relieved by disease-modifying treatment not relieved by disease-modifying treatment
Advance Directive DiscussionAdvance Directive Discussion– Document surrogate decision maker(s) Document surrogate decision maker(s) – Educate and guide about treatment preferencesEducate and guide about treatment preferences– Appropriate in any debilitating illnessAppropriate in any debilitating illness
Assess Eligibility for Hospice ReferralAssess Eligibility for Hospice Referral
Truth-Telling to Patient/FamilyTruth-Telling to Patient/Family
PrognosticationPrognosticationValue to Value to
Patient/FamilyPatient/Family
Aids in symptom managementAids in symptom management Allows time to access community resources Allows time to access community resources Fosters preparing and planning care Fosters preparing and planning care Helps avoid lurching from crisis to crisisHelps avoid lurching from crisis to crisis

Determining PrognosisDetermining Prognosis
Can be difficult in individual caseCan be difficult in individual case
““Would I be surprised if patient died Would I be surprised if patient died
in the next 6 months?”in the next 6 months?”
yields a more accurate answer thanyields a more accurate answer than
““Will this patient die in next 6 months?”Will this patient die in next 6 months?”
If you would not be surprised, If you would not be surprised,
assess palliative care needsassess palliative care needs
Language is ImportantLanguage is Important
““Because of the severity of your Because of the severity of your illness, illness,
you and your family are eligible for you and your family are eligible for
the assistance of hospice at home”the assistance of hospice at home”
is preferable tois preferable to
““You have a prognosis of less than six You have a prognosis of less than six months; months;
therefore, I am referring you hospice”therefore, I am referring you hospice”
Example of Example of Life-Limiting Illness Life-Limiting Illness
Combination of diagnoses in 84 year-oldCombination of diagnoses in 84 year-old– Moderately severe dementiaModerately severe dementia– Progressive heart failureProgressive heart failure– Chronic renal diseaseChronic renal disease
Status despite medical managementStatus despite medical management– Unintentional weight loss Unintentional weight loss – Confined to bedConfined to bed
Patient and/or family choose palliationPatient and/or family choose palliation– Relief of symptoms and suffering vs. cureRelief of symptoms and suffering vs. cure

Markers for Poor Markers for Poor Prognosis Prognosis in Debilityin Debility
Disease Progression Disease Progression – Of one or more of underlying diseasesOf one or more of underlying diseases– Although none yet considered terminalAlthough none yet considered terminal
Increased Dependence Increased Dependence
Need for Home Care ServicesNeed for Home Care Services
Markers for Poor Markers for Poor Prognosis Prognosis in Debilityin Debility
Multiple Emergency Room VisitsMultiple Emergency Room Visits Multiple Hospital AdmissionsMultiple Hospital Admissions
are signs thatare signs that
disease-modifying treatment disease-modifying treatment
is inadequate tois inadequate to
Control symptomsControl symptoms Relieve sufferingRelieve suffering Prevent decline in functionPrevent decline in function
Functional Decline Functional Decline Objective MeasuresObjective Measures
Activities of Daily Living (ADL) Activities of Daily Living (ADL)
Development of dependence in at least Development of dependence in at least three ADL’s in the last six months three ADL’s in the last six months – BathingBathing– DressingDressing– FeedingFeeding– TransfersTransfers– ContinenceContinence– Ability to walk unaided to the bathroomAbility to walk unaided to the bathroom
Functional Decline Functional Decline Objective MeasuresObjective Measures
Karnofsky Performance StatusKarnofsky Performance Status– Karnofsky Score 50% or less with declineKarnofsky Score 50% or less with decline
in score over last 6 monthsin score over last 6 months
– KS 70% KS 70% Cares for selfCares for self Unable to carry on normal activity or active Unable to carry on normal activity or active
workwork
– KS 50% KS 50% Requires considerable assistance Requires considerable assistance Requires frequent medical careRequires frequent medical care

Functional Decline Functional Decline Objective MeasuresObjective Measures
Unintentional Weight Loss Unintentional Weight Loss – Greater than or equal to 10% of body Greater than or equal to 10% of body
weightweight– In the last 6 monthsIn the last 6 months
Albumin Albumin – Less than 2.5 mg/dl Less than 2.5 mg/dl – Always combine this measure with other Always combine this measure with other
evidence of declineevidence of decline

Palliative Care Palliative Care ConsultConsult
IndicationsIndications
Unrelieved SufferingUnrelieved Suffering
Functional DeclineFunctional Decline– Any combinationAny combination of measures of decline of measures of decline
or or
markers for poor prognosismarkers for poor prognosis
Consideration of Hospice ReferralConsideration of Hospice Referral

Palliative Care ConsultPalliative Care ConsultValueValue
Symptom ControlSymptom Control– Assessment Assessment – PlanPlan
Treatment PlanningTreatment Planning– Assist to define goals of careAssist to define goals of care– Assist to develop plan that melds Assist to develop plan that melds
symptom management with disease-symptom management with disease-modifying treatmentmodifying treatment
Assist with Advance Care PlanningAssist with Advance Care Planning
Determine eligibility for hospice careDetermine eligibility for hospice care
Palliative Care inPalliative Care inGeneral DebilityGeneral Debility
Consult Often and EarlyConsult Often and Early
Dementia Dementia The Palliative ResponseThe Palliative Response
F. Amos Bailey, M.D.F. Amos Bailey, M.D.
Dementia Causes Dementia Causes SufferingSuffering
PhysicalPhysical EmotionalEmotional Social Social SpiritualSpiritual
Both the person afflicted with dementia Both the person afflicted with dementia and the person’s family and the person’s family will experience suffering will experience suffering
in any or all of these domainsin any or all of these domains

Dementia Dementia and Palliative Careand Palliative Care
Most patients and families living with Most patients and families living with dementia would benefit from the dementia would benefit from the Palliative Care approach to the Palliative Care approach to the assessment and treatment of their assessment and treatment of their sufferingsuffering
Suffering has multiple domains and is Suffering has multiple domains and is best addressed in an interdisciplinary best addressed in an interdisciplinary processprocess

Dementia Dementia and Hospice Care and Hospice Care
A select subset of all patientsA select subset of all patients
with dementia will qualifywith dementia will qualify
for services through the for services through the
Medicare Hospice BenefitMedicare Hospice Benefit

The Physician’s RoleThe Physician’s Role
Evaluation and diagnosis of dementiaEvaluation and diagnosis of dementia Search for reversible causes (rare)Search for reversible causes (rare) Management of current medical Management of current medical
problemsproblems Sensitive revelation of the diagnosis and Sensitive revelation of the diagnosis and
prognosisprognosis Assist in defining Goals of CareAssist in defining Goals of Care

The Physician’s RoleThe Physician’s RoleMedical ManagementMedical Management
Management of acute, often Management of acute, often recurrent and infectious illnessesrecurrent and infectious illnesses– PneumoniaPneumonia– UTIUTI
Management of co-morbid illnessManagement of co-morbid illness – Treatment may be more difficult, Treatment may be more difficult,
especially in the advanced stages of especially in the advanced stages of dementiadementia
The Physician’s Role The Physician’s Role Late-Stage DementiaLate-Stage Dementia
Evaluation of key markers of late-Evaluation of key markers of late-stage dementiastage dementia– Inability to walk independentlyInability to walk independently– Fewer than six intelligible wordsFewer than six intelligible words– Decline in oral intake and nutritional Decline in oral intake and nutritional
statusstatus– Frequent ER visits and hospital Frequent ER visits and hospital
admissionadmission
Management of late-stage dementiaManagement of late-stage dementia
Transition to hospice careTransition to hospice care
Dementia Dementia Physical SufferingPhysical Suffering
PainPain Pain from complications of dementia is Pain from complications of dementia is
often under-treated due to difficulty often under-treated due to difficulty with self-reportingwith self-reporting
InfectionsInfections Pneumonia Pneumonia
– Aspirations and atelectasis Aspirations and atelectasis UTI UTI
– Diapers and indwelling cathetersDiapers and indwelling catheters

DementiaDementiaPhysical SufferingPhysical Suffering
Decubitis UlcersDecubitis Ulcers
IncontinenceIncontinence ImmobilityImmobility RestraintsRestraints Poor hygienePoor hygiene Decreasing nutritional statusDecreasing nutritional status
Dementia Dementia Physical SufferingPhysical Suffering
AstheniaAsthenia
FallsFalls
Bed or chair confinementBed or chair confinement
Medical interventions and iatrogenic injuryMedical interventions and iatrogenic injury– Nasogastric tubes and PEG tubesNasogastric tubes and PEG tubes– Foley cathetersFoley catheters– IV’sIV’s– Restraints to protect other interventions Restraints to protect other interventions
or to prevent attempts to get upor to prevent attempts to get up

Dementia Dementia Emotional SufferingEmotional Suffering
DepressionDepression
May benefit from treatment with SSRIMay benefit from treatment with SSRI
Cognitive LossCognitive Loss
May benefit from treatment with May benefit from treatment with medications like Aricept in early-to-medications like Aricept in early-to-moderate stagesmoderate stages
May cause unacceptable side effects May cause unacceptable side effects without benefitwithout benefit

Dementia Dementia Emotional SufferingEmotional Suffering
DeliriumDelirium
Wandering and sun-downingWandering and sun-downing Often worsened by even a minor illnessOften worsened by even a minor illness Disturbance of sleep-wake cycle disrupts Disturbance of sleep-wake cycle disrupts
homehome Usually less intense in familiar Usually less intense in familiar
environmentsenvironments

Dementia Dementia Caregiver SufferingCaregiver Suffering
DepressionDepression– Referral for treatmentReferral for treatment
FatigueFatigue– RespiteRespite
AngerAnger– Support groupsSupport groups
GuiltGuilt– Spiritual counsel/ support groupsSpiritual counsel/ support groups
Dementia Dementia Social SufferingSocial Suffering
Loss of independenceLoss of independence Family struggles with role reversalFamily struggles with role reversal Declining health or death of spouse Declining health or death of spouse
complicates carecomplicates care Loss of financial resourcesLoss of financial resources Need to change location of careNeed to change location of care
DementiaDementiaSocial SufferingSocial Suffering
Need to Change Location of Need to Change Location of CareCare
Nursing Home
Assisted Living Facility
Hospice Care
Home

Dementia Dementia Spiritual SufferingSpiritual Suffering
GuiltGuilt AngerAnger Inability to maintain relationship with Inability to maintain relationship with
faith communityfaith community Feelings of abandonment Feelings of abandonment
Advance Care PlanningAdvance Care PlanningIn Early DementiaIn Early Dementia
Patient can help make decisionsPatient can help make decisions
Surrogates for decision-makingSurrogates for decision-making Preferred locations of carePreferred locations of care Feeding tubesFeeding tubes Resuscitation and other aggressive Resuscitation and other aggressive
interventionsinterventions
Advance Care PlanningAdvance Care PlanningAdvanced DementiaAdvanced Dementia
Family and caregivers Family and caregivers
discuss decisionsdiscuss decisions
Transitions to other venues of careTransitions to other venues of care Response to complications and Response to complications and
progression of illnessprogression of illness Feeding tubesFeeding tubes Resuscitation attemptsResuscitation attempts

Prognosis and Care Prognosis and Care NeedsNeeds
Prediction by Fast ScoringPrediction by Fast Scoring
Development of incontinenceDevelopment of incontinence – Usually will require transfer from ALF to Usually will require transfer from ALF to
nursing homenursing home
FAST Score of 6 or 7 FAST Score of 6 or 7 – May predict a less than six-month May predict a less than six-month
survival survival – Qualifies patient for referral to hospiceQualifies patient for referral to hospice

Prognosis and Care Prognosis and Care NeedsNeeds
Key Indicators for Limited Key Indicators for Limited PrognosisPrognosis
Loss of ability to ambulate independentlyLoss of ability to ambulate independently Fewer than six intelligible wordsFewer than six intelligible words Declining oral intakeDeclining oral intake

Prognosis and Care Prognosis and Care NeedsNeeds
Key Indicators for Limited Key Indicators for Limited Prognosis Prognosis
Markers of advanced dementia Markers of advanced dementia predictpredict– Frequent ER visitsFrequent ER visits– Frequent hospital admissionsFrequent hospital admissions
Prognosis and Care Prognosis and Care NeedsNeeds
Key Indicators for Limited Key Indicators for Limited PrognosisPrognosis
Markers should prompt…Markers should prompt…– Discussion with surrogates of limited Discussion with surrogates of limited
prognosisprognosis– Review or development of Advance Care Review or development of Advance Care
PlanPlan– Consideration of hospice referralConsideration of hospice referral

The Palliative Response The Palliative Response Hepatic FailureHepatic Failure
F. Amos Bailey, M.D.F. Amos Bailey, M.D.
End-Stage Liver End-Stage Liver DiseasesDiseases
MarkersMarkers– Hepatic insufficiency Hepatic insufficiency – CirrhosisCirrhosis
EtiologyEtiology– Can arise from various specific Can arise from various specific
diagnosesdiagnoses SymptomsSymptoms
– Share many of the same symptomsShare many of the same symptoms PrognosisPrognosis
– Share general guidelines for predicting Share general guidelines for predicting prognosisprognosis

Palliative Care Palliative Care ResponseResponseEvaluationEvaluation
Physical Physical – Assess for poorly controlled symptoms Assess for poorly controlled symptoms
(e.g., pain, anorexia, asthenia)(e.g., pain, anorexia, asthenia) EmotionalEmotional
– Distress secondary to physical declineDistress secondary to physical decline Social Social
– Distress secondary to increased Distress secondary to increased debility debility
– Need for additional support servicesNeed for additional support services Existential/Spiritual AngstExistential/Spiritual Angst
– Hopelessness secondary to prognosisHopelessness secondary to prognosis
Palliative Care Palliative Care ResponseResponse
ManagementManagement Symptom ManagementSymptom Management
– Develop plan of care to palliate symptoms Develop plan of care to palliate symptoms not relieved by disease-modifying treatmentnot relieved by disease-modifying treatment
Advance Care PlanningAdvance Care Planning– Discuss choice of surrogate decision-maker(s)Discuss choice of surrogate decision-maker(s)– Inform and guide regarding treatment Inform and guide regarding treatment
preferences preferences – Any patient with end-stage liver disease Any patient with end-stage liver disease
needs to document surrogate(s) and needs to document surrogate(s) and preferencespreferences
Palliative Care Palliative Care ResponseResponse
Truth Telling and Truth Telling and ReferralReferral
Truth Telling/PrognosticationTruth Telling/Prognostication– Assists with symptom managementAssists with symptom management– Enables access of community resourcesEnables access of community resources– Facilitates preparing and planning care Facilitates preparing and planning care – Prevents lurching from crisis to crisisPrevents lurching from crisis to crisis
Assess Eligibility for Hospice Assess Eligibility for Hospice Care Care
Triggers for Triggers for PrognosticationPrognostication
Multiple Emergency Room visits Multiple Emergency Room visits
Multiple hospital admissionsMultiple hospital admissions
– Typical of patients with hepatic failureTypical of patients with hepatic failure– Indicate poorly controlled symptomsIndicate poorly controlled symptoms

Determining PrognosisDetermining Prognosis
Determining individual prognosis is difficultDetermining individual prognosis is difficult
Would I be surprised if this patient Would I be surprised if this patient died died
in next 6 months?in next 6 months?yields more accurate prognosisyields more accurate prognosis thanthan
Will this patient die in the next six months?Will this patient die in the next six months?
If you would not be surprised, assess palliative If you would not be surprised, assess palliative needsneeds
Sharing PrognosisSharing Prognosis
Important for people to know that Important for people to know that prognosis is limitedprognosis is limited
““While no one knows how long anyone While no one knows how long anyone
will live, there are certain signs that your will live, there are certain signs that your health is very poor and declining and health is very poor and declining and that time could be limited”that time could be limited”
““People are eligible for hospice when People are eligible for hospice when their illness is so severe that they might their illness is so severe that they might die in the next 6 months to a year”die in the next 6 months to a year”

Language is ImportantLanguage is Important
““Because of the severity of your Because of the severity of your disease, you and your family are disease, you and your family are eligible for the assistance of hospice eligible for the assistance of hospice at home”at home”
is preferable tois preferable to
““You have a prognosis of less than six You have a prognosis of less than six months; therefore, I am referring you to months; therefore, I am referring you to hospice”hospice”

Is Patient a CandidateIs Patient a CandidateFor Liver Transplant?For Liver Transplant?
If YESIf YES
Pursue aggressive treatment goalsPursue aggressive treatment goals

Is Patient a CandidateIs Patient a CandidateFor Liver Transplant?For Liver Transplant?
If NOIf NO
Due to ineligibility or choice Due to ineligibility or choice
Patient and/or family may elect Palliative Patient and/or family may elect Palliative CareCare– After discussion with physiciansAfter discussion with physicians– Direct Goals of Care and treatment to Direct Goals of Care and treatment to
relief of symptoms and suffering rather relief of symptoms and suffering rather than to cure of underlying diseasesthan to cure of underlying diseases
Markers for Poor Markers for Poor PrognosisPrognosis
Synthetic Function Synthetic Function ImpairmentImpairment
Severe synthetic function impairmentSevere synthetic function impairment – Serum Albumin less than 2.5gm/dlSerum Albumin less than 2.5gm/dl– Prolonged INR greater than 2.0Prolonged INR greater than 2.0
Indications to assess improvementIndications to assess improvement– Acute illness resolvesAcute illness resolves– Abstinence from alcoholAbstinence from alcohol
Markers for Poor Markers for Poor PrognosisPrognosis
Clinical Indicators Clinical Indicators
Refractory AscitesRefractory Ascites– Lack of response to diuretics Lack of response to diuretics – Non-adherence to treatmentNon-adherence to treatment
Spontaneous Bacterial PeritonitisSpontaneous Bacterial Peritonitis
Hepatorenal SyndromeHepatorenal Syndrome
Markers for Poor Markers for Poor PrognosisPrognosis
Clinical Indicators Clinical Indicators Recurrent Hepatic EncephalopathyRecurrent Hepatic Encephalopathy
– Decreased response to treatmentDecreased response to treatment– Non-adherence to treatmentNon-adherence to treatment
Recurrent Variceal BleedingRecurrent Variceal Bleeding– Despite medical intervention and Despite medical intervention and
managementmanagement

Other Markers forOther Markers for Poor Prognosis Poor Prognosis
Unintentional weight loss Unintentional weight loss – Greater than or equal to 10% of body Greater than or equal to 10% of body
weightweight– In the last 6 monthsIn the last 6 months
Muscle wasting/reduced strengthMuscle wasting/reduced strength
Continued alcohol useContinued alcohol use
HBsAg positivityHBsAg positivity
Multiple ER and hospital admissionsMultiple ER and hospital admissions

ConsiderConsiderPalliative Care ConsultPalliative Care Consult
Any combinationAny combination of markers for poor of markers for poor prognosisprognosis
Not necessary for patient to have all Not necessary for patient to have all signs or symptomssigns or symptoms

Palliative Care ConsultPalliative Care Consult
Unrelieved SufferingUnrelieved Suffering– Assess symptom controlAssess symptom control– Advise about Goals of CareAdvise about Goals of Care– Assist to meld symptom management Assist to meld symptom management
with disease- modifying treatmentwith disease- modifying treatment
Advance Care PlanningAdvance Care Planning
Evaluate for Hospice ReferralEvaluate for Hospice Referral– Help establish life-expectancyHelp establish life-expectancy– Determine eligibility for hospice careDetermine eligibility for hospice care
Palliative Care andPalliative Care andProgressive Liver Progressive Liver
DiseaseDisease
Consult Often and EarlyConsult Often and Early
Pulmonary Disease Pulmonary Disease The Palliative ResponseThe Palliative Response
F. Amos Bailey, M.D.F. Amos Bailey, M.D.

Suffering in Pulmonary Suffering in Pulmonary DiseaseDisease
Patients with advanced pulmonary Patients with advanced pulmonary diseasedisease
often suffer extensively despite often suffer extensively despite
maximum disease-modifying therapiesmaximum disease-modifying therapies

Palliative Care Palliative Care EvaluationEvaluation
Pulmonary DiseasePulmonary DiseasePhysical DiscomfortPhysical Discomfort
Poorly controlled symptomsPoorly controlled symptoms
(e.g., dyspnea and asthenia)(e.g., dyspnea and asthenia)
Emotional DistressEmotional Distress
Secondary to physical declineSecondary to physical decline
Palliative Care Palliative Care EvaluationEvaluation
Pulmonary DiseasePulmonary DiseaseSocial DistressSocial Distress
Secondary to debility and need for Secondary to debility and need for additional support and servicesadditional support and services
Spiritual DistressSpiritual Distress
Existential angst and hopelessnessExistential angst and hopelessness

Palliative Care Palliative Care ResponseResponse
Manage SymptomsManage Symptoms Develop plan to palliate symptoms unrelieved Develop plan to palliate symptoms unrelieved
by disease-modifying treatmentby disease-modifying treatment
Discuss Advance DirectiveDiscuss Advance Directive Discuss choice of surrogate decision maker(s)Discuss choice of surrogate decision maker(s) Discuss treatment preferences Discuss treatment preferences Appropriate in any advanced pulmonary Appropriate in any advanced pulmonary
diseasedisease
Evaluate for Hospice ReferralEvaluate for Hospice Referral
Palliative Care Palliative Care ResponseResponse
PrognosticationPrognosticationValue of Truth TellingValue of Truth Telling
Assists with symptom managementAssists with symptom management Enables patient and family to access Enables patient and family to access
community resources community resources Fosters preparing and planning careFosters preparing and planning care Helps family avoid lurching from crisis to Helps family avoid lurching from crisis to
crisiscrisis
Aids to Aids to PrognosticationPrognostication
Determining individual prognosis is difficultDetermining individual prognosis is difficult
Would I be surprised if this patient Would I be surprised if this patient died Idied Iin the next six months?in the next six months?
yields more accurate answer thanyields more accurate answer than
Will this patient die in the next six months?Will this patient die in the next six months?
If you would not be surprised, If you would not be surprised, assess for palliative care needsassess for palliative care needs
Language is ImportantLanguage is Important
““Because of the severity of your lung Because of the severity of your lung disease, you and your family are disease, you and your family are eligible for the assistance of hospice eligible for the assistance of hospice at home”at home”
is preferable tois preferable to
““You have a prognosis of less than six You have a prognosis of less than six months. Therefore, I am referring you to months. Therefore, I am referring you to hospice”hospice”
Language is ImportantLanguage is Important
““While no one knows how long anyone While no one knows how long anyone will live, there are certain signs that will live, there are certain signs that your lung disease is very severe and your lung disease is very severe and that time could be limited”that time could be limited”
““People are eligible for hospice when People are eligible for hospice when their illness is so severe that they might their illness is so severe that they might die in the next six months to a year”die in the next six months to a year”

Markers for Poor Markers for Poor PrognosisPrognosis
Disabling DyspneaDisabling Dyspnea Dyspnea at rest despite maximum medical Dyspnea at rest despite maximum medical
managementmanagement
Patients may be very limited Patients may be very limited
(e.g., bed-to-chair or mostly bed confined)(e.g., bed-to-chair or mostly bed confined)
Other problems often presentOther problems often present
(e.g., cough, profound fatigue)(e.g., cough, profound fatigue)
Consider co-morbid illnessesConsider co-morbid illnesses

Poor Prognosis Poor Prognosis Functional Markers Functional Markers
Multiple emergency room visitsMultiple emergency room visits
Multiple hospital admissionsMultiple hospital admissions
Declining functional status Declining functional status (based on assessment of Activities of Daily (based on assessment of Activities of Daily Living)Living)
Inability to live independentlyInability to live independently(necessitating move to live with family or in a (necessitating move to live with family or in a residential care facility)residential care facility)
Poor Prognosis Poor Prognosis 5 Key Clinical Markers 5 Key Clinical Markers
1. Unintentional Weight Loss1. Unintentional Weight Loss
Greater than 10% of body weight Greater than 10% of body weight Over six monthsOver six months
Poor Prognosis Poor Prognosis 5 Key Clinical Markers5 Key Clinical Markers
2. Resting Tachycardia2. Resting Tachycardia
Resting heart beat >100/ minuteResting heart beat >100/ minute Unrelated to recent breathing treatmentUnrelated to recent breathing treatment Unrelated to atrial fibrillation Unrelated to atrial fibrillation Unrelated to MATUnrelated to MAT
Poor Prognosis Poor Prognosis 5 Key Clinical Markers5 Key Clinical Markers
3. Hypoxemia at Rest3. Hypoxemia at Rest
Despite supplemental oxygen, such as Despite supplemental oxygen, such as 2l NP, 2l NP, pO2 less than or equal to pO2 less than or equal to 55mm HG55mm HG
4. Hypercapnia 4. Hypercapnia
pCO2 greater than or equal to 50mm HGpCO2 greater than or equal to 50mm HG

Poor Prognosis Poor Prognosis 5 Key Clinical Markers5 Key Clinical Markers
5. Evidence of Right Heart 5. Evidence of Right Heart FailureFailure
Physical Signs of RHFPhysical Signs of RHF EchocardiogramEchocardiogram ElectrocardiogramElectrocardiogram

Palliative Care Palliative Care EvaluationEvaluationIndicationIndication
Any combination of markers of poor Any combination of markers of poor prognosis warrants referral for prognosis warrants referral for Palliative Care evaluation Palliative Care evaluation
Not necessary or appropriate for Not necessary or appropriate for
patient to exhibit all markers to patient to exhibit all markers to warrant palliative evaluationwarrant palliative evaluation
Palliative Care ConsultPalliative Care ConsultReview of ContributionReview of Contribution
Unrelieved SufferingUnrelieved Suffering– Assess symptom controlAssess symptom control– Assist to develop treatment plan that Assist to develop treatment plan that
melds symptom management with melds symptom management with disease-modifying treatmentdisease-modifying treatment
Goals of CareGoals of Care
Advance Care PlanningAdvance Care Planning
Assess for Hospice ReferralAssess for Hospice Referral
Palliative Care andPalliative Care andPulmonary DiseasePulmonary Disease
Consult Often and EarlyConsult Often and Early

Renal DiseaseRenal DiseaseThe Palliative ResponseThe Palliative Response
F. Amos Bailey, M.D.F. Amos Bailey, M.D.

Suffering in Suffering in End-Stage Renal End-Stage Renal
DiseaseDisease
Patients with End-Stage Renal DiseasePatients with End-Stage Renal Disease
often suffer extensively often suffer extensively
despite despite
maximum disease-modifying maximum disease-modifying therapiestherapies
Dialysis TherapyDialysis Therapy
Some patients Some patients declinedecline
Some patients Some patients inappropriateinappropriate – Co-morbid diseases Co-morbid diseases – Quality-of-life issuesQuality-of-life issues
Some patients decide to Some patients decide to discontinuediscontinue– Progressive decline Progressive decline – Co-morbid illness Co-morbid illness – Appropriate for hospice referralAppropriate for hospice referral

Palliative EvaluationPalliative Evaluation
PhysicalPhysicalUncontrolled symptomsUncontrolled symptoms
(e.g., Dyspnea, Asthenia, Delirium)(e.g., Dyspnea, Asthenia, Delirium)
EmotionalEmotional
Distress in the face of physical declineDistress in the face of physical decline

Palliative EvaluationPalliative Evaluation
SocialSocial
Distress from increased debility and Distress from increased debility and need for additional servicesneed for additional services
SpiritualSpiritual
Existential angst and hopelessnessExistential angst and hopelessness
The Palliative The Palliative ResponseResponse
Symptom ManagementSymptom Management– Develop plan of care to palliate symptoms Develop plan of care to palliate symptoms
not relieved by disease-modifying treatmentnot relieved by disease-modifying treatment
Advance Directive DiscussionAdvance Directive Discussion– Discuss surrogate decision maker(s) Discuss surrogate decision maker(s) – Discuss treatment preferencesDiscuss treatment preferences– Document result of discussionDocument result of discussion
Hospice ReferralHospice Referral for advanced patients for advanced patients
Truth-TellingTruth-Telling
Value of Truth Telling Value of Truth Telling and Prognosticationand Prognostication
Assists with symptom managementAssists with symptom management Enables accessing community resourcesEnables accessing community resources Fosters preparing and planning careFosters preparing and planning care Helps avoid lurching from crisis to crisisHelps avoid lurching from crisis to crisis
Establishing PrognosisEstablishing Prognosis
Ask…Ask…
Would you be surprised if this Would you be surprised if this patient patient died in next six months?died in next six months?
Yields more accurate prognosis than…Yields more accurate prognosis than…
Will this patient die in the next six Will this patient die in the next six months?months?
If you would not be surprised…If you would not be surprised…
assess for palliative care needsassess for palliative care needs
Sharing PrognosisSharing Prognosis
Important for people to know Important for people to know that prognosis is limitedthat prognosis is limited
““Because of the severity of your kidney Because of the severity of your kidney disease, you and your family are eligible disease, you and your family are eligible for the assistance of hospice at home”for the assistance of hospice at home”
preferable to…preferable to… ““You have a prognosis of less than six You have a prognosis of less than six
months; therefore, I am referring you to months; therefore, I am referring you to hospice”hospice”
Language is ImportantLanguage is Important
““While no one knows how long anyone While no one knows how long anyone will live, there are certain signs that will live, there are certain signs that your kidney disease is very severe and your kidney disease is very severe and that time could be limited”that time could be limited”
““People are eligible for hospice when People are eligible for hospice when their illness is so severe that they might their illness is so severe that they might die in the next six months to a year”die in the next six months to a year”

Markers for Poor Markers for Poor PrognosisPrognosis
Co-Morbid IllnessesCo-Morbid Illnesses
StrokesStrokes
Advanced DementiaAdvanced Dementia
Congestive Heart Failure Congestive Heart Failure despite control of fluid overloaddespite control of fluid overload
Markers for Poor Markers for Poor PrognosisPrognosis
Co-Morbid IllnessesCo-Morbid Illnesses
Chronic Lung Disease Chronic Lung Disease Oxygen Dependence Oxygen Dependence
Diabetes Mellitus Diabetes Mellitus Manifestations of long-term Manifestations of long-term
complicationscomplications

Poor PrognosisPoor PrognosisKey Clinical MarkersKey Clinical Markers
Unintentional Weight LossUnintentional Weight Loss– Greater than 10% of body weight over Greater than 10% of body weight over
six months six months
Resting TachycardiaResting Tachycardia– Resting heartbeat greater than Resting heartbeat greater than
100/minute100/minute– Unrelated to recent breathing Unrelated to recent breathing
treatment, atrial fibrillation or MATtreatment, atrial fibrillation or MAT

Poor PrognosisPoor PrognosisKey Clinical MarkersKey Clinical Markers
Poor Prognostic Markers Poor Prognostic Markers
for patient who will not be receiving for patient who will not be receiving dialysisdialysis
Serum Creatinine >8mg/dlSerum Creatinine >8mg/dl Creatinine Clearance <10cc/minuteCreatinine Clearance <10cc/minute

Poor Prognosis Poor Prognosis Functional MarkersFunctional Markers
Multiple emergency room visitsMultiple emergency room visits
Multiple hospital admissionsMultiple hospital admissions
Declining functional status based on Declining functional status based on assessment of Activities of Daily Livingassessment of Activities of Daily Living
Need to move from living independently Need to move from living independently to living with family or in a residential to living with family or in a residential care facilitycare facility

Palliative Response to Palliative Response to Markers for Poor Markers for Poor
PrognosisPrognosis Any combination of markers for poor Any combination of markers for poor
prognosis might prompt evaluation by prognosis might prompt evaluation by palliative care for unrelieved suffering or palliative care for unrelieved suffering or for hospice referralfor hospice referral
It is not necessary or appropriate for a It is not necessary or appropriate for a patient to exhibit all of the markers patient to exhibit all of the markers before being evaluated by palliative carebefore being evaluated by palliative care

Palliative Care ConsultPalliative Care Consult
Symptom ControlSymptom Control
Treatment Plan Treatment Plan Assist to develop plan that melds Assist to develop plan that melds symptom management with disease-symptom management with disease-modifying treatmentmodifying treatment
Goals of Care Goals of Care Advance Care PlanningAdvance Care Planning Assess for Hospice Care Assess for Hospice Care

Palliative CarePalliative CareEnd-Stage Renal End-Stage Renal
DiseaseDisease
Consult Often and EarlyConsult Often and Early
Congestive Heart Congestive Heart FailureFailure
The Palliative ResponseThe Palliative Response
F. Amos Bailey, M.D.F. Amos Bailey, M.D.
Dying from Heart Dying from Heart Disease Disease
Physical Suffering at Life’s Physical Suffering at Life’s EndEnd
PAINPAIN was one of was one of the most common the most common problemsproblems
78% report pain in 78% report pain in the last yearthe last year
63% report pain the 63% report pain the last weeklast week
50% say pain is 50% say pain is ““very distressing”very distressing”
DYSPNEADYSPNEA was the was the second most second most common problemcommon problem
61% report dyspnea 61% report dyspnea in the last yearin the last year
51% report dyspnea 51% report dyspnea in the last weekin the last week
43% say dyspnea is 43% say dyspnea is “very distressing”“very distressing”
McCarthy et. al., 1996
Dying from Heart Dying from Heart Disease Disease
Physical Suffering at Life’s Physical Suffering at Life’s EndEnd
Loss of appetite 43%Loss of appetite 43%
Nausea/Vomiting 32%Nausea/Vomiting 32%
Constipation 37%Constipation 37%
Fecal incontinence 16%Fecal incontinence 16%
McCarthy et. al., 1996
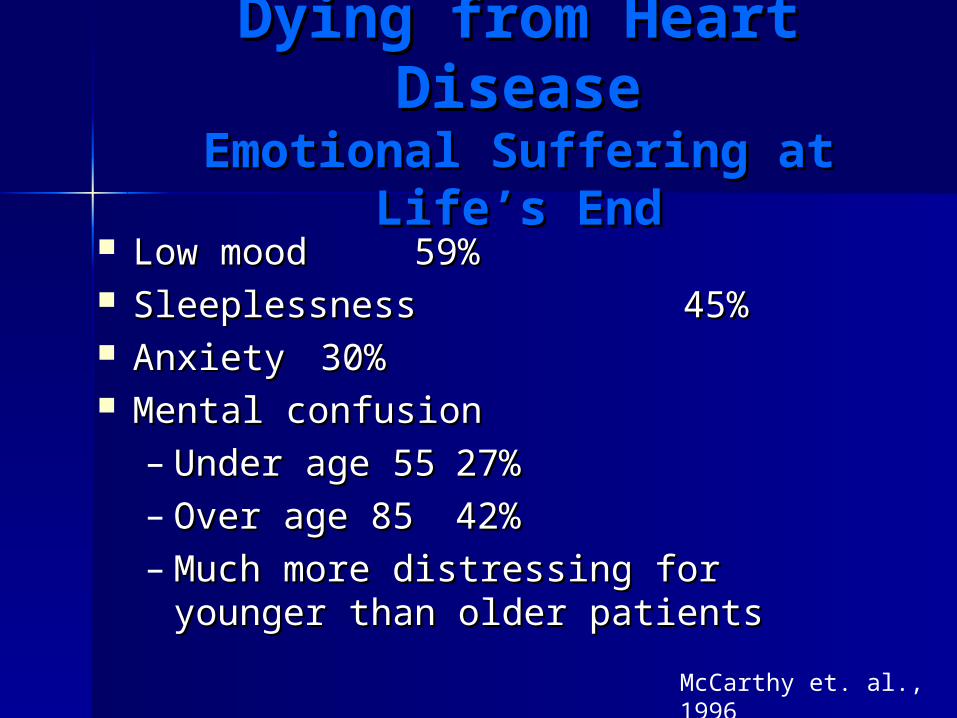
Dying from Heart Dying from Heart DiseaseDisease
Emotional Suffering at Life’s Emotional Suffering at Life’s EndEnd
Low mood Low mood 59%59% Sleeplessness Sleeplessness 45% 45% Anxiety Anxiety 30%30% Mental confusionMental confusion
– Under age 55Under age 55 27%27%– Over age 85Over age 85 42%42%– Much more distressing for Much more distressing for
younger than older patientsyounger than older patients
McCarthy et. al., 1996

Social and Spiritual Social and Spiritual Suffering at Life’s EndSuffering at Life’s End
Dying in setting other than home (70%)Dying in setting other than home (70%) Declining functional statusDeclining functional status Social isolationSocial isolation Depletion of financial resourcesDepletion of financial resources Caregiver fatigueCaregiver fatigue Questions of meaning – Why?Questions of meaning – Why?
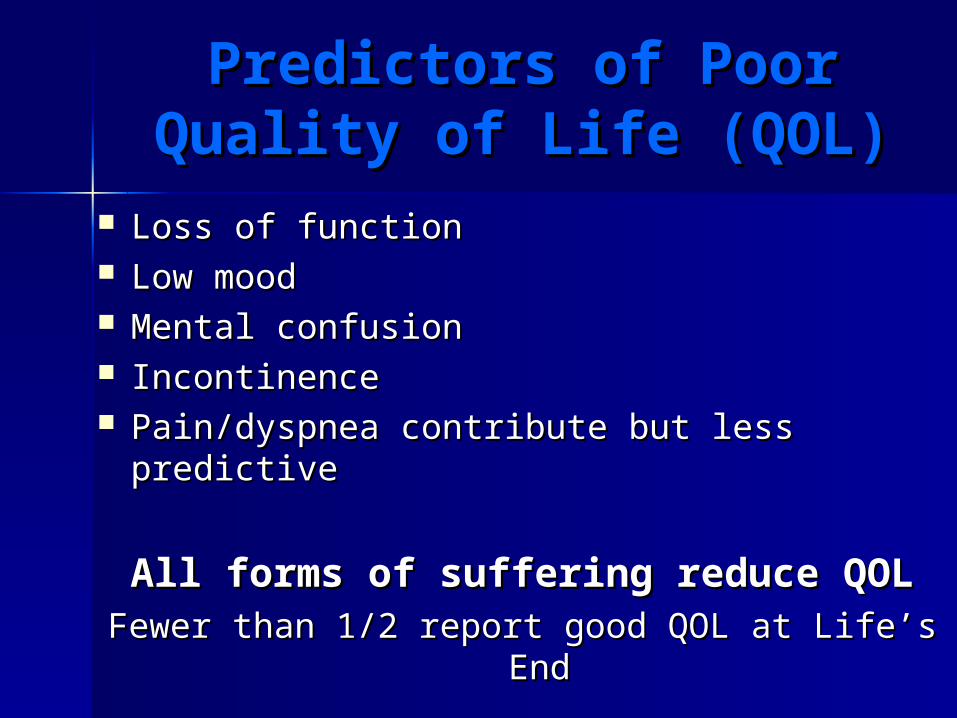
Predictors of PoorPredictors of PoorQuality of Life (QOL)Quality of Life (QOL)
Loss of functionLoss of function Low moodLow mood Mental confusionMental confusion Incontinence Incontinence Pain/dyspnea contribute but less predictivePain/dyspnea contribute but less predictive
All forms of suffering reduce QOLAll forms of suffering reduce QOLFewer than 1/2 report good QOL at Life’s EndFewer than 1/2 report good QOL at Life’s End

Status and Status and Symptoms Symptoms
at Life’s Endat Life’s End 55% conscious in the last three days55% conscious in the last three days 4 of 10 had severe pain most of the time4 of 10 had severe pain most of the time 8 of 10 had severe asthenia8 of 10 had severe asthenia 1 of 4 had severe dysphoria1 of 4 had severe dysphoria 2 of 3 had one or more difficult-to-tolerate 2 of 3 had one or more difficult-to-tolerate
physical or emotional symptomsphysical or emotional symptoms
SUPPORT Study Lynn et. al., 1997
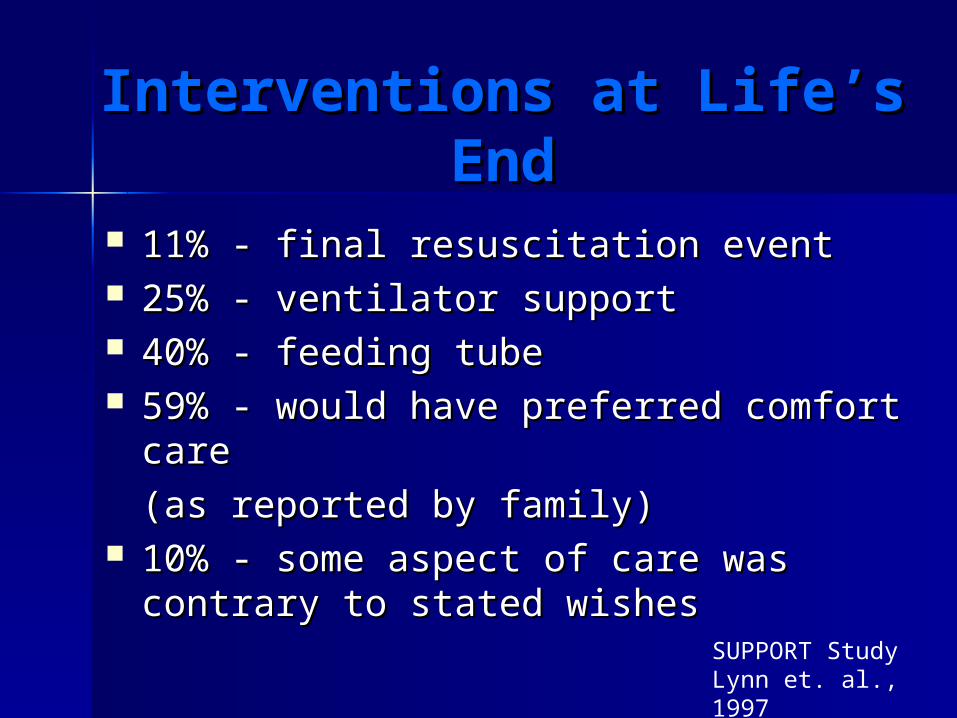
Interventions at Life’s Interventions at Life’s EndEnd
11% - final resuscitation event11% - final resuscitation event 25% - ventilator support25% - ventilator support 40% - feeding tube40% - feeding tube 59% - would have preferred comfort care59% - would have preferred comfort care
(as reported by family)(as reported by family) 10% - some aspect of care was contrary to 10% - some aspect of care was contrary to
stated wishesstated wishes
SUPPORT Study Lynn et. al., 1997
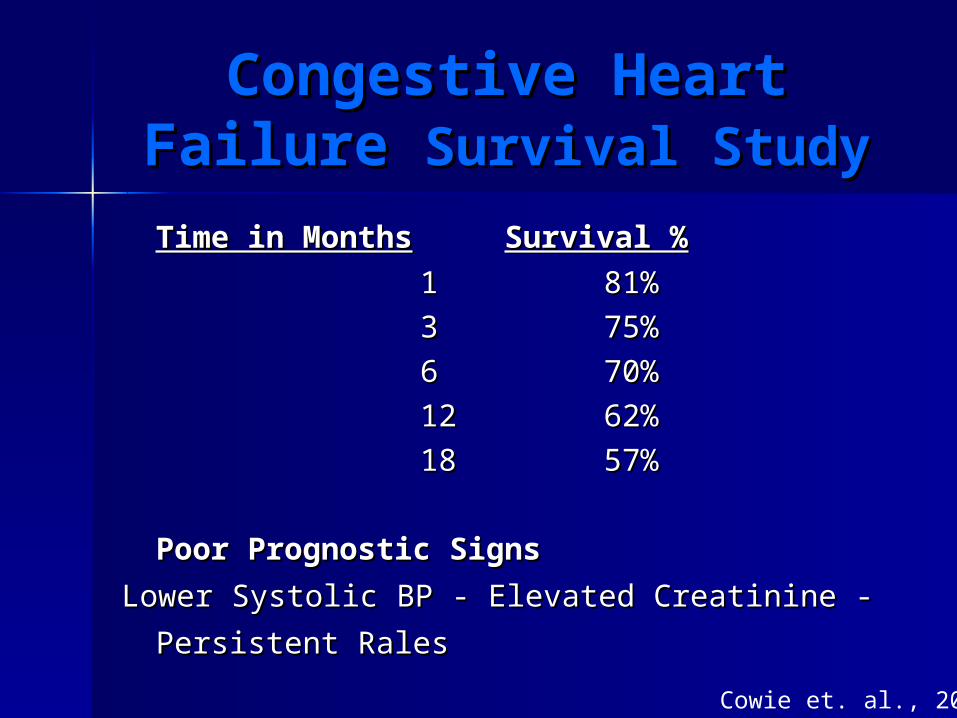
Congestive Heart Congestive Heart Failure Failure Survival StudySurvival Study
Time in MonthsTime in Months Survival %Survival %
11 81% 81%
33 75% 75%
66 70% 70%
1212 62% 62%
1818 57% 57%
Poor Prognostic SignsPoor Prognostic Signs
Lower Systolic BP - Elevated Creatinine - Lower Systolic BP - Elevated Creatinine -
Persistent RalesPersistent Rales Cowie et. al., 2000
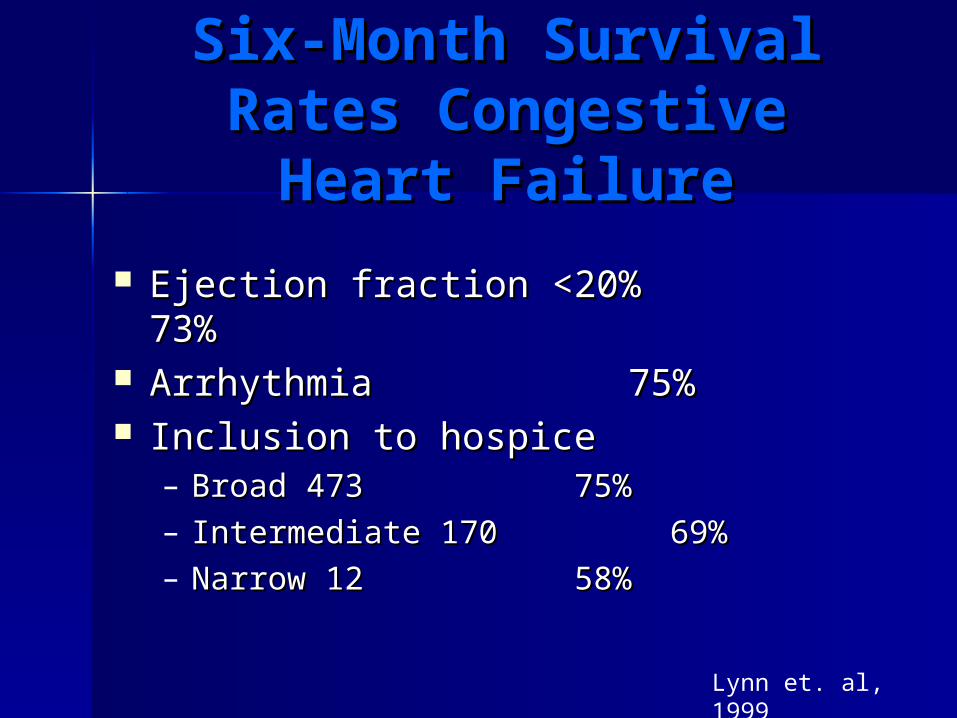
Six-Month Survival Six-Month Survival Rates Congestive Rates Congestive
Heart FailureHeart Failure
Ejection fraction <20%Ejection fraction <20% 73%73% ArrhythmiaArrhythmia 75%75% Inclusion to hospiceInclusion to hospice
– Broad 473Broad 473 75%75%– Intermediate 170Intermediate 170 69%69%– Narrow 12Narrow 12 58%58%
Lynn et. al, 1999
Congestive Heart FailureCongestive Heart FailureResearch ResultsResearch Results
High Death Risk/Low Prognostic AccuracyHigh Death Risk/Low Prognostic AccuracySurvival can be unpredictably very shortSurvival can be unpredictably very short
Impossible to predict accurately which Impossible to predict accurately which congestive heart patients will die in given congestive heart patients will die in given periodperiod
Many patients die before judged “eligible” for Many patients die before judged “eligible” for hospice care by their predicted life hospice care by their predicted life expectancyexpectancy
Thus, many patients amenable to palliative Thus, many patients amenable to palliative care instead experience unrelieved sufferingcare instead experience unrelieved sufferingSUPPORT Study
Lynn et. al, 1999

Congestive Heart Congestive Heart FailureFailure
The Palliative The Palliative ResponseResponse Symptom management Symptom management
(vs. disease modification)(vs. disease modification) Psychological, emotional and bereavement Psychological, emotional and bereavement
supportsupport Care of the family unitCare of the family unit Access to community resourcesAccess to community resources Interdisciplinary assistance Interdisciplinary assistance Home servicesHome services Advance Care PlanningAdvance Care Planning
Doctor-Patient Doctor-Patient Communication About Communication About
Death and DyingDeath and DyingEvidence of Communication DifficultyEvidence of Communication Difficulty
MMany patients realized were dying, but without any input from physician about this reality
Patients queried researchers about condition, prognosis and likely manner of death
Etiology of Communication DifficultyEtiology of Communication Difficulty Patients – Confusion, memory lossPatients – Confusion, memory loss Physicians – Discomfort/unwillingness to Physicians – Discomfort/unwillingness to
provide informationprovide information Rogers & Addington-Hall, 2000
Optimum Optimum Medical TreatmentMedical Treatment
Ace inhibitors Digoxin Loop diuretics Beta-blockers Spironolactone Anticoagulant therapy Nitrates

BreathlessnessBreathlessness
KEEP DRY, reposition, reassure, provide a KEEP DRY, reposition, reassure, provide a fanfan
OxygenOxygen Morphine or another opioid in short-acting Morphine or another opioid in short-acting
form form Ms 10mg/5ml 5-10mg q1-2 hour for dyspneaMs 10mg/5ml 5-10mg q1-2 hour for dyspnea Mild anxiolytic Mild anxiolytic
LLorazepam 0.5-1mg q2-4 hoursorazepam 0.5-1mg q2-4 hours
Relief of dyspnea is more important than Relief of dyspnea is more important than determining the creatinine level determining the creatinine level

Diuretic Treatment is Diuretic Treatment is Key Key
in Breathlessnessin BreathlessnessGoals Goals
Minimal rales and patient comfortMinimal rales and patient comfort Weight controlWeight control
– Weigh and chart dailyWeigh and chart daily– Increase: increase diuretics/reduce fluid Increase: increase diuretics/reduce fluid
intakeintake– Decrease: risk of hypotension or renal Decrease: risk of hypotension or renal
failure secondary to overshootingfailure secondary to overshooting
Possible Unavoidable Side EffectsPossible Unavoidable Side Effects HypotensionHypotension Elevated creatinine and BUNElevated creatinine and BUN Dry mouthDry mouth
Home Nursing RoleHome Nursing Role
Assist with medicinesAssist with medicines Assist with dietAssist with diet Assist with memory Assist with memory Assess patient safety and comfortAssess patient safety and comfort
– Bed or recliner with raised head? Bed or recliner with raised head? – Easy access to toiletEasy access to toilet– Family supportFamily support– Need for additional assistanceNeed for additional assistance
(home health aides, homemaker, meals)(home health aides, homemaker, meals)
Fatigue and Fatigue and LightheadednessLightheadedness
Reassess drug therapyReassess drug therapy Consider depressionConsider depression Recommend energy conservationRecommend energy conservation Check for postural hypotensionCheck for postural hypotension If dyspnea is controlled, may be able to If dyspnea is controlled, may be able to
titrate fluid intake to increase titrate fluid intake to increase intravascular volume with oral hydrationintravascular volume with oral hydration
Nausea and AnorexiaNausea and Anorexia
EtiologyEtiology Complications of drug therapyComplications of drug therapy Constipation secondary to medicines or Constipation secondary to medicines or
decreased fluid intakedecreased fluid intake
InterventionsInterventions Frequent small meals to accommodate Frequent small meals to accommodate
fatiguefatigue Appetite stimulant (e.g., alcohol or decadron)Appetite stimulant (e.g., alcohol or decadron) Metoclopramide for decreased emptying Metoclopramide for decreased emptying

EdemaEdema
InterventionsInterventions Diuretic therapyDiuretic therapy Fluid restrictionFluid restriction ElevationElevation Salt restrictionSalt restriction ReassuranceReassurance
Consider EtiologyConsider Etiology AnasarcaAnasarca Decreased albumin levelDecreased albumin level
Emotional SufferingEmotional Suffering
ManifestationsManifestations DeliriumDelirium DepressionDepression AnxietyAnxiety
InterventionsInterventions Medical management Medical management Supportive home environment Supportive home environment Openly address fears to help regain Openly address fears to help regain
sense of controlsense of control

Social SufferingSocial Suffering
EtiologyEtiology Loss of incomeLoss of income Cost of treatmentCost of treatment Difficulty with transportation and errandsDifficulty with transportation and errands Necessity for residential care vs. home Necessity for residential care vs. home
carecare Time limits and lack of defined prognosisTime limits and lack of defined prognosis
InterventionsInterventions Access community resourcesAccess community resources
Spiritual SufferingSpiritual Suffering
EtiologyEtiology Uncertainty about timing/manner of deathUncertainty about timing/manner of death Guilt and angerGuilt and anger Sense of isolation and abandonment due Sense of isolation and abandonment due
to fatigue of caregivers and other to fatigue of caregivers and other supporterssupporters
InterventionIntervention Improve symptom control Improve symptom control Reconnect with communityReconnect with community

Programmatic ResponseProgrammatic Response
Hospice Care in advanced and difficult Hospice Care in advanced and difficult cases for intensive supportcases for intensive support
Congestive Heart Home Health SpecialistCongestive Heart Home Health Specialist
(offered by some insurances)(offered by some insurances)
Medicaring Demonstration ProjectMedicaring Demonstration Project
(supportive services for CHF and COPD)(supportive services for CHF and COPD)
HIV/AIDS HIV/AIDS and Palliative Careand Palliative Care
F. Amos Bailey, M.D.F. Amos Bailey, M.D.
Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSEarly 1980’s Early 1980’s
Clusters of PCP Pneumonia Clusters of PCP Pneumonia
Identification of high-risk groups in USIdentification of high-risk groups in US– Gay menGay men– Injecting drug usersInjecting drug users– HemophiliacsHemophiliacs

Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSMid 1980’sMid 1980’s
Identification of HIV as the causative Identification of HIV as the causative agentagent
Screening and testing of at-risk groupsScreening and testing of at-risk groups Identification of the routes of infectionIdentification of the routes of infection Development of education/prevention Development of education/prevention
campaignscampaigns Mounting numbers of deaths from AIDSMounting numbers of deaths from AIDS

Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSMid 1980’sMid 1980’s
Understanding of natural history of Understanding of natural history of infectioninfection
Acute infection (usually not recognized)Acute infection (usually not recognized) Long period of time during which infected Long period of time during which infected
person is asymptotic (infectious)person is asymptotic (infectious) ARC (AIDS Related Complex)ARC (AIDS Related Complex) Opportunistic infection and/or certain types Opportunistic infection and/or certain types
of cancers leading to deathof cancers leading to death
Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSMid 1980’sMid 1980’s
Understanding of the natural history of Understanding of the natural history of infectioninfection
Lose about 100 CD4’s/yearLose about 100 CD4’s/year Relationship to CD4 lymphocyte depletionRelationship to CD4 lymphocyte depletion
– ~ 500-1000/dl Normal~ 500-1000/dl Normal– 200-500/dl ARC200-500/dl ARC– <200/dl PCP<200/dl PCP– <100/dl Other opportunistic <100/dl Other opportunistic
infections (OI) and infections (OI) and deathdeath
Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSLate 1980’s Late 1980’s
TreatmentTreatment
TMP/Sulfa for PCPTMP/Sulfa for PCP AZT trialAZT trial DDI trial DDI trial People living longer develop other OI’sPeople living longer develop other OI’s
– CMVCMV– MAIMAI
Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSEarly 1990’sEarly 1990’s
Recognition that the medicines Recognition that the medicines developed developed
could be toxic and lose effectivenesscould be toxic and lose effectiveness
Development of other NRTI’sDevelopment of other NRTI’s Development of NNRTI’sDevelopment of NNRTI’s HIV/AIDS hospice programs in larger citiesHIV/AIDS hospice programs in larger cities
– San FranciscoSan Francisco– New York New York – ChicagoChicago
Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSEarly 1990’sEarly 1990’s
Beginning to appreciate the crisis Beginning to appreciate the crisis developing in Sub-Saharan Africa, Asia and developing in Sub-Saharan Africa, Asia and other developing countriesother developing countries
Hospice programs in smaller communities Hospice programs in smaller communities begin to have more referrals as local begin to have more referrals as local infection occurs and persons living with infection occurs and persons living with AIDS (PWA) return to live with their familiesAIDS (PWA) return to live with their families

Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSEarly 1990’sEarly 1990’s
Finding Expression for the CrisisFinding Expression for the Crisis
AIDS QuiltAIDS Quilt Red RibbonsRed Ribbons Angels in AmericaAngels in America (play) (play) RENTRENT (musical) (musical) The Band Played OnThe Band Played On (book and movie) (book and movie) PhiladelphiaPhiladelphia (movie) (movie)
Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSMid 1990’sMid 1990’s
New TreatmentsNew Treatments
PI Protease Inhibitors introducedPI Protease Inhibitors introduced HAART (Highly Active Anti-Retroviral HAART (Highly Active Anti-Retroviral
Therapy) 2NRTIs and a PITherapy) 2NRTIs and a PI People with AIDS on their death beds got People with AIDS on their death beds got
up and walked out of hospicesup and walked out of hospices Irrational exuberance (possible cure) Irrational exuberance (possible cure)

Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSLate 1990’s to Present Late 1990’s to Present
PI Protease Inhibitors widely used in both PI Protease Inhibitors widely used in both newly infected and established patientsnewly infected and established patients
HIV/AID specialty hospice programs closeHIV/AID specialty hospice programs close New side effects and toxicity identifiedNew side effects and toxicity identified COST of treatment over $1000 a monthCOST of treatment over $1000 a month Patients begin to fail treatment because Patients begin to fail treatment because
of the development of resistanceof the development of resistance
Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSLate 1990’ to PresentLate 1990’ to Present
Infection Escalates in Developing Infection Escalates in Developing CountriesCountries
HIV/AIDS infection rate in some South African HIV/AIDS infection rate in some South African countries reaches 25% of the populationcountries reaches 25% of the population
Protest about the inability to afford or access Protest about the inability to afford or access treatment in developing countriestreatment in developing countries
Development of HIV/AIDS hospice care in Development of HIV/AIDS hospice care in developing worlddeveloping world
Changing Natural Changing Natural HistoryHistory
of HIV/AIDSof HIV/AIDSLate 1990’s to PresentLate 1990’s to Present
View HIV/AIDS in USA as chronic illness View HIV/AIDS in USA as chronic illness such as DM or HTNsuch as DM or HTN
Hospice referral of patients with Hospice referral of patients with HIV/AIDS resumesHIV/AIDS resumes
The future…..The future…..

The Experience of The Experience of Dying from HIV/AIDSDying from HIV/AIDS
PhysicalPhysical EmotionalEmotional
SufferingSuffering
SocialSocial SpiritualSpiritual
Palliative CarePalliative Care
““Palliative care seeks to prevent, relieve, Palliative care seeks to prevent, relieve, reduce or soothe the symptoms of disease reduce or soothe the symptoms of disease or disorder without effecting a cure…or disorder without effecting a cure…
Palliative care in this broad sense is not Palliative care in this broad sense is not restricted to those who are dying or those restricted to those who are dying or those enrolled in hospice programs…enrolled in hospice programs…
It attends closely to the emotional, It attends closely to the emotional, spiritual, and practical needs and goals of spiritual, and practical needs and goals of patients and those close to them.”patients and those close to them.”
Institute of Medicine 1998Institute of Medicine 1998
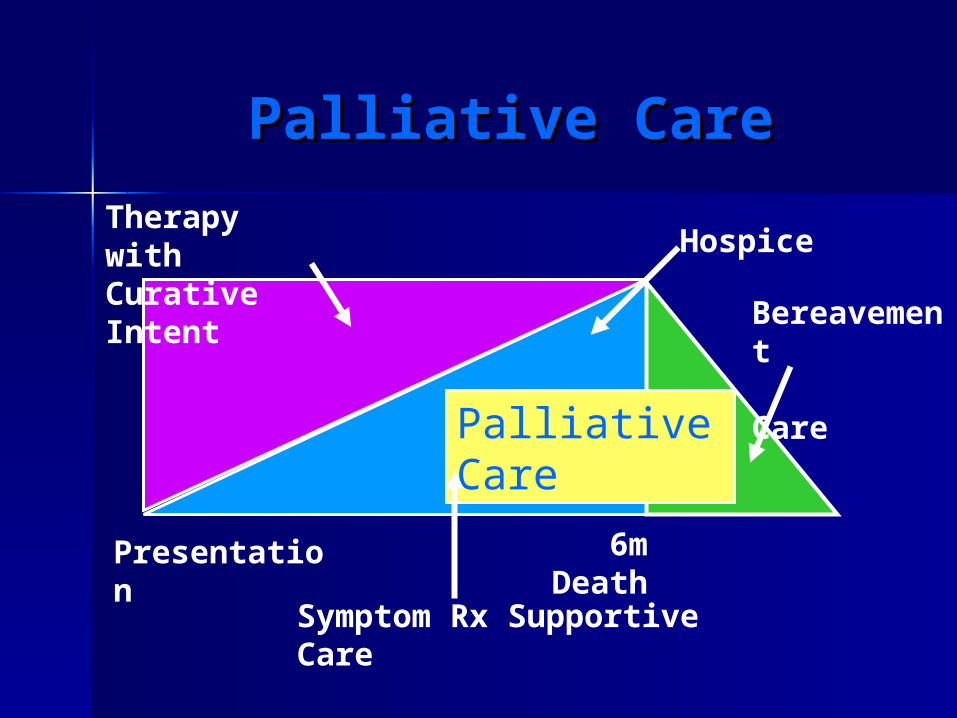
Palliative CarePalliative Care
Palliative Care
HospiceTherapy with Curative Intent
Symptom Rx Supportive Care
Bereavement Care
Presentation 6m Death

Physical SufferingPhysical Suffering
Opportunistic infectionOpportunistic infection MalignancyMalignancy Treatment toxicityTreatment toxicity Organ FailureOrgan Failure
Physical SufferingPhysical SufferingOpportunistic InfectionOpportunistic Infection
Opportunistic infection may developOpportunistic infection may developwhen immune competency when immune competency cannot be restored due tocannot be restored due to
Lack of response (resistance)Lack of response (resistance) Non-compliance with treatmentNon-compliance with treatment Lack of availability of treatment Lack of availability of treatment
(developing countries)(developing countries)

Physical SufferingPhysical SufferingOpportunistic InfectionOpportunistic Infection
Opportunistic infection may lead toOpportunistic infection may lead todeath within 12 months of onsetdeath within 12 months of onset
MAC 74%MAC 74% CMV 70%CMV 70% Toxoplasmosis 73%Toxoplasmosis 73% CMV and MAC 99%CMV and MAC 99% CMV and wasting 88%CMV and wasting 88%

Physical SufferingPhysical SufferingComplicationsComplications
Complications when immune-Complications when immune-competencycompetency
cannot be restored may lead to deathcannot be restored may lead to death
within 12 months of onsetwithin 12 months of onset
Progressive multifocal Progressive multifocal
leukoencephalopathy 100%leukoencephalopathy 100% Dementia 79%Dementia 79% Cancers such as B cell lymphoma, primary Cancers such as B cell lymphoma, primary
CNS lymphoma and cervical cancer in womenCNS lymphoma and cervical cancer in women
Physical SufferingPhysical SufferingComplications of Complications of
TreatmentTreatment
Diabetes mellitusDiabetes mellitus PancreatitisPancreatitis Lipid dystrophy with stroke or heart Lipid dystrophy with stroke or heart
diseasedisease Hepatic injuryHepatic injury Bone marrow suppressionBone marrow suppression
Physical SufferingPhysical SufferingComplications & Organ Complications & Organ
FailuresFailures
Renal failureRenal failure Liver failure with Hepatitis B and/or CLiver failure with Hepatitis B and/or C CardiomyopathyCardiomyopathy Co-morbid risk of injury from drug and Co-morbid risk of injury from drug and
alcohol abusealcohol abuse

Palliative CarePalliative Careand Hospice Referralsand Hospice Referrals
Indications for ReferralIndications for Referral
HAART therapy ineffectiveHAART therapy ineffective HAART therapy not tolerated wellHAART therapy not tolerated well PWA declines treatment for HIVPWA declines treatment for HIV Complications such as dementia, PMLComplications such as dementia, PML HIV may be secondary diagnosis with the HIV may be secondary diagnosis with the
primary diagnosis being hepatic failure primary diagnosis being hepatic failure or canceror cancer

Palliative and Hospice Palliative and Hospice CareCare
Physical symptoms may be similar to those Physical symptoms may be similar to those of other patients referred to hospice of other patients referred to hospice although may have larger numberalthough may have larger number
Special issuesSpecial issues– Pain control in patients with history of Pain control in patients with history of
past or current drug usepast or current drug use– Decisions about continuing some OI or Decisions about continuing some OI or
HIV treatmentsHIV treatments– Management of specific OI/HIV problems Management of specific OI/HIV problems
in concert with HIV specialistin concert with HIV specialist
Emotional Suffering Emotional Suffering and HIV/AIDSand HIV/AIDS
Depression and suicideDepression and suicide Cognitive impairment Cognitive impairment
– Dementia or PMLDementia or PML Substance abuseSubstance abuse AnxietyAnxiety Mental illness and homelessnessMental illness and homelessness Gender and sexuality issuesGender and sexuality issues
Social Suffering Social Suffering and HIV/AIDSand HIV/AIDS
Relative youth of infected individualsRelative youth of infected individuals
Infection of multiple members of family or Infection of multiple members of family or community groupcommunity group
Estrangement from family and society Estrangement from family and society
Loss of incomeLoss of income
Lack of insurance - Medicaid and Lack of insurance - Medicaid and Medicare issuesMedicare issues

Social Suffering Social Suffering and HIV/AIDSand HIV/AIDS
Unstable living environmentUnstable living environment
LonelinessLoneliness
Dissatisfaction with available supportDissatisfaction with available support
Lack of recognized long-term Lack of recognized long-term relationshiprelationship
Need for Advance Care PlanningNeed for Advance Care Planning
Need for residential careNeed for residential care
Spiritual Suffering Spiritual Suffering and HIV/AIDSand HIV/AIDS
Perceived and Actual Discrimination Perceived and Actual Discrimination
HomosexualityHomosexuality RaceRace EthnicityEthnicity ClassClass
Spiritual Suffering Spiritual Suffering and HIV/AIDSand HIV/AIDS
Perceived and actual rejection by faith Perceived and actual rejection by faith communitycommunity
Fear of divine judgment and retributionFear of divine judgment and retribution
Lack of time to process life events and Lack of time to process life events and develop sources of meaning and develop sources of meaning and transcendencetranscendence
Unmet need for grace and mercyUnmet need for grace and mercy

Palliative Care Palliative Care for HIV/AIDSfor HIV/AIDS
Many HIV/AIDS primary care providers Many HIV/AIDS primary care providers have recognized the importance of have recognized the importance of incorporating nursing, social work, incorporating nursing, social work, pastoral care and mental health in a pastoral care and mental health in a coordinated holistic model of care coordinated holistic model of care
New service models have developed New service models have developed because of fear, prejudice and because of fear, prejudice and discrimination by community providersdiscrimination by community providers

Hospice Care Hospice Care for HIV/AIDSfor HIV/AIDS
Late Hospice Referrals are CommonLate Hospice Referrals are Common
Difficult for patients to accept hospiceDifficult for patients to accept hospice Difficult for providers determine Difficult for providers determine
appropriateness because of appropriateness because of effectiveness of HAART treatmenteffectiveness of HAART treatment
Lack of stable home environment and Lack of stable home environment and primary caregiverprimary caregiver

Hospice Care Hospice Care for HIV/AIDSfor HIV/AIDS
Persons with HIV/AIDS Persons with HIV/AIDS
frequently receive EOL care frequently receive EOL care
in “non-traditional” hospice settingsin “non-traditional” hospice settings
Acute care hospitalsAcute care hospitals Residential care facilitiesResidential care facilities Prisons Prisons
Hospice Care Hospice Care for HIV/AIDSfor HIV/AIDS
There is an international need for hospice There is an international need for hospice and palliative care as primary treatment and palliative care as primary treatment because of lack of infrastructure for because of lack of infrastructure for medical treatmentmedical treatment
HAART is unlikely to become widely HAART is unlikely to become widely available because of expense and available because of expense and difficulty of treatment management in difficulty of treatment management in poor and developing countriespoor and developing countries
Palliative Care Palliative Care for HIV/AIDSfor HIV/AIDS
Needs to be available to patients and their Needs to be available to patients and their medical providersmedical providers
Could become a model for the incorporation Could become a model for the incorporation of palliative care into other chronic illnessesof palliative care into other chronic illnesses
Care needs to be flexible and responsive to Care needs to be flexible and responsive to patient and caregiver needspatient and caregiver needs
Providers need to learn from each other Providers need to learn from each other about management of HIV/AIDS throughout about management of HIV/AIDS throughout the course of the diseasethe course of the disease

Palliative Care Palliative Care for HIV/AIDSfor HIV/AIDS
Offers Possibility for GrowthOffers Possibility for Growth
IndividualIndividual CommunityCommunity ProfessionProfession
HIV/AIDS HIV/AIDS and Palliative Careand Palliative Care
Consult Early and OftenConsult Early and Often