Embed Size (px)
DESCRIPTION
understanding toxic multinodular goiter as well as general anaesthesia chosen for the operation.
Citation preview
CHAPTER 1
THEORY: NON-TOXIC MULTINODULAR GOITER
INTRODUCTION
Multinodular non-toxic goiter is the most prevalent thyroid pathology characterized by
unilateral or bilateral thyroid growth with morphologically and/or functionally transformed
follicles and euthyroidism. At thyroid sonography in unselected populations, 20 to 30 %
incidence of thyroid nodules has been reported. Beside morphologic variability, lack of
hyperstimulation in the majority of the multiplicated follicles is the hallmark of the disorder.
Most nodular goiters grow slowly and undergo different morphologic changes, encompassing
diffuse hyperplastic enlargement in the early phase, development of large follicles loaded with
abundant colloid and with increasing age, formation of functionally autonomous tissue. Annual
growth potential of approximately 20 % can be assumed.
The pathogenesis of nodular goiter is multifactorial and probably differs from patient to
patient. In contrast to the endemic goiter, iodine deficiency is not a primary causal factor.
Environmental factors such as natural goitrogens, iodine intake, malnutrition, drugs, stress,
pollution or infections, constitutional factors such as female gender and several genetic factors,
i.e. circulating thyroid growth factors contribute to different degree to the development of
nodular thyroid enlargement. Also controversially debated, thyroid-stimulating hormone (TSH)
presumably has an important role in the maintenance of thyroid growth and goitrogenesis. The
observation that TSH-suppressive treatment may cause a reduction of goiter volume underlines
the role of TSH as goitrogen factor.
1.1. Anatomy
1
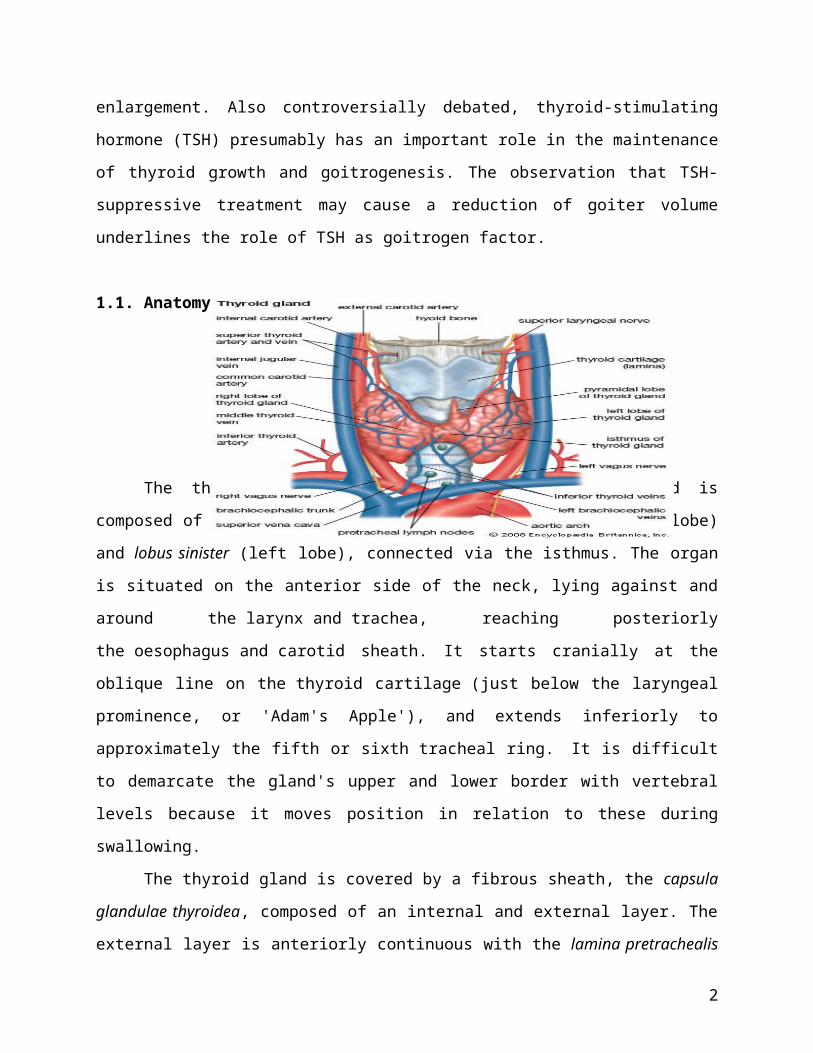
The thyroid gland is a butterfly-shaped organ and is composed of two cone-like lobes or
wings, lobus dexter (right lobe) and lobus sinister (left lobe), connected via the isthmus. The
organ is situated on the anterior side of the neck, lying against and around the larynx and trachea,
reaching posteriorly the oesophagus and carotid sheath. It starts cranially at the oblique line on
the thyroid cartilage (just below the laryngeal prominence, or 'Adam's Apple'), and extends
inferiorly to approximately the fifth or sixth tracheal ring. It is difficult to demarcate the gland's
upper and lower border with vertebral levels because it moves position in relation to these during
swallowing.
The thyroid gland is covered by a fibrous sheath, the capsula glandulae thyroidea,
composed of an internal and external layer. The external layer is anteriorly continuous with
the lamina pretrachealis fasciae cervicalis and posteriorolaterally continuous with the carotid
sheath. The gland is covered anteriorly with infrahyoid muscles and laterally with
the sternocleidomastoid muscle also known as sternomastoid muscle. On the posterior side, the
gland is fixed to the cricoid and tracheal cartilage and cricopharyngeus muscle by a thickening of
the fascia to form the posterior suspensory ligament of Berry. The thyroid gland's firm
attachment to the underlying trachea is the reason behind its movement with swallowing. In
variable extent, Lalouette's Pyramid, a pyramidal extension of the thyroid lobe, is present at the
most anterior side of the lobe. In this region, the recurrent laryngeal nerve and the inferior
thyroid artery pass next to or in the ligament and tubercle.
Between the two layers of the capsule and on the posterior side of the lobes, there are on
each side two parathyroid glands.
The thyroid isthmus is variable in presence and size, can change shape and size, and can
encompass a cranially extending pyramid lobe (lobus pyramidalis or processus pyramidalis),
remnant of the thyroglossal duct. The thyroid is one of the larger endocrine glands, weighing 2-
3 grams in neonates and 18-60 grams in adults, and is increased in pregnancy.
The thyroid is supplied with arterial blood from the superior thyroid artery, a branch of
the external carotid artery, and the inferior thyroid artery, a branch of the thyrocervical trunk, and
sometimes by the thyroid ima artery, branching directly from the brachiocephalic trunk. The
venous blood is drained via superior thyroid veins, draining in the internal jugular vein, and
via inferior thyroid veins, draining via the plexus thyroideus impar in the left brachiocephalic
vein.
2
Lymphatic drainage passes frequently the lateral deep cervical lymph nodes and the pre-
and parathracheal lymph nodes. The gland is supplied by parasympathetic nerve input from
the superior laryngeal nerve and the recurrent laryngeal nerve.
1.2. Histology
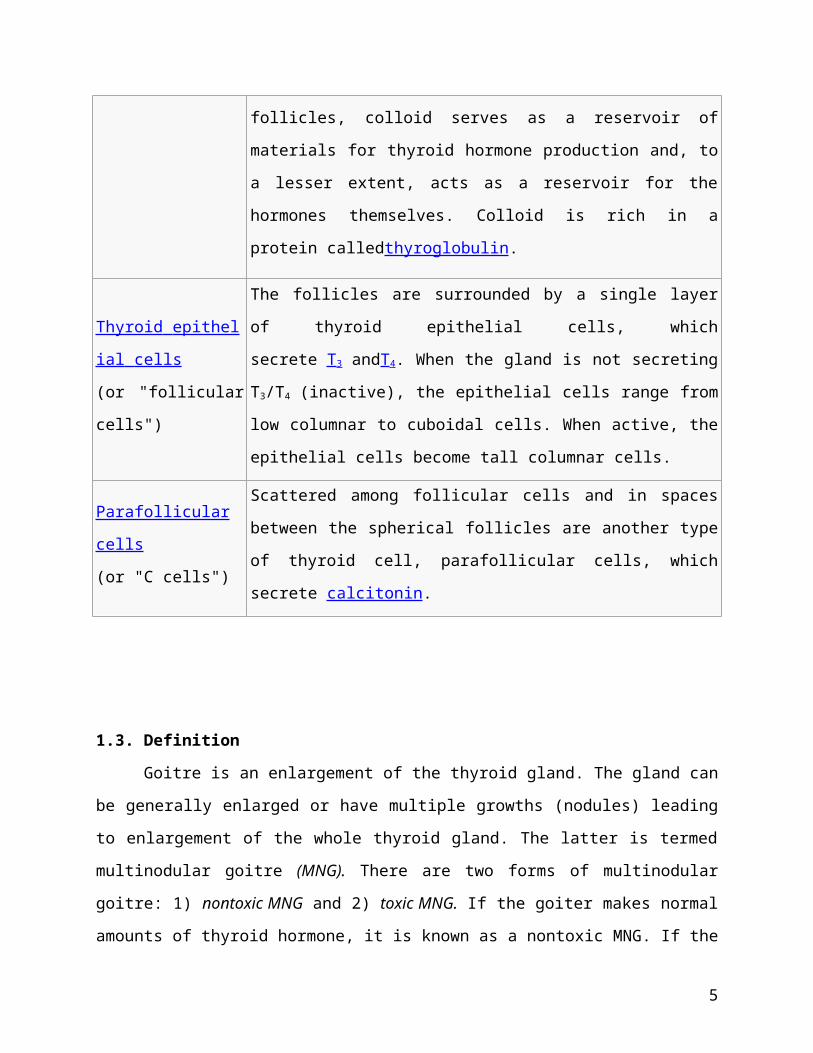
At the microscopic level, there are three primary features of the thyroid:
Feature Description
Follicles
The thyroid is composed of spherical follicles that selectively absorb
iodine (as iodide ions, I-) from the blood for production of thyroid
hormones, but also for storage of iodine in thyroglobulin, in fact iodine
is necessary for other important iodine-concentrating organs as breast,
stomach, salivary glands, thymus etc. (see iodine in biology).
Twenty-five percent of all the body's iodide ions are in the thyroid gland.
Inside the follicles, colloid serves as a reservoir of materials for thyroid
hormone production and, to a lesser extent, acts as a reservoir for the
hormones themselves. Colloid is rich in a protein calledthyroglobulin.
Thyroid epithelial cells
(or "follicular cells")
The follicles are surrounded by a single layer of thyroid epithelial cells,
which secrete T3 andT4. When the gland is not secreting T3/T4 (inactive),
the epithelial cells range from low columnar to cuboidal cells. When
active, the epithelial cells become tall columnar cells.
Parafollicular cells
(or "C cells")
Scattered among follicular cells and in spaces between the spherical
follicles are another type of thyroid cell, parafollicular cells, which
secrete calcitonin.
3
1.3. Definition
Goitre is an enlargement of the thyroid gland. The gland can be generally enlarged or
have multiple growths (nodules) leading to enlargement of the whole thyroid gland. The latter is
termed multinodular goitre (MNG). There are two forms of multinodular goitre: 1) nontoxic
MNG and 2) toxic MNG. If the goiter makes normal amounts of thyroid hormone, it is known as
a nontoxic MNG. If the goiter makes higher than normal amounts of thyroid hormone leading to
a suppressed TSH, it is known as a toxic MNG. The exact causes of thyroid nodules or
multinodular goitres are unknown. In general, the development of goitre is due to a complex mix
of genetic and environmental factors. Iodine deficiency as a cause of goitre is rare in North
America and most of Europe. However, even in areas of iodine deficiency most patients do not
develop goitres.
1.4. Etiology
The first comprehensive theory about the development of multinodular goitre was
proposed by David Marine and studied further by Selwyn Taylor, and can be considered one of
the classics in this field. Nodular goitre may be the result of any chronic low-grade, intermittent
stimulus to thyroid hyperplasia. In response to iodide deficiency, the thyroid first goes through a
period of hyperplasia as a consequence of the resulting TSH stimulation, but eventually, possibly
because of iodide repletion or a decreased requirement for thyroid hormone, enters a resting
phase characterized by colloid storage and the histologic picture of a colloid goitre. Repetition of
these two phases of the cycle would eventually result in the formation of nontoxic multinodular
goitre. Studies by Taylor of thyroid glands removed at surgery led him to believe that the initial
lesion is diffuse hyperplasia, but that with time discrete nodules develop.
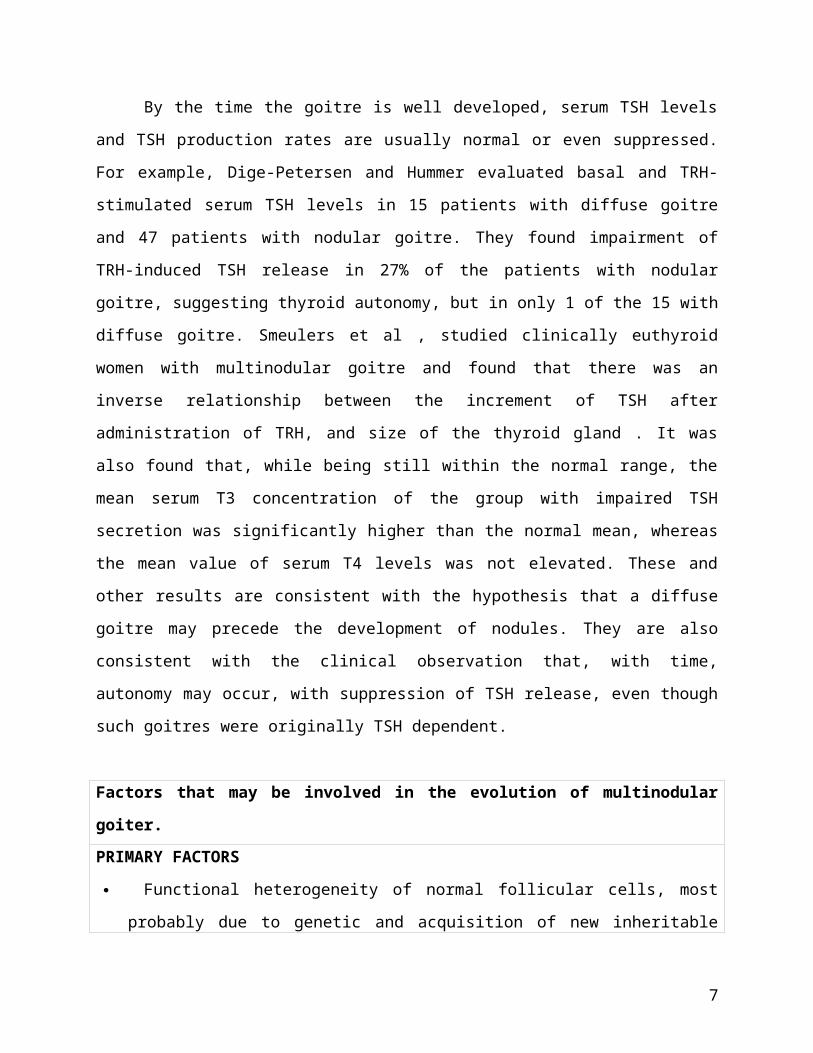
By the time the goitre is well developed, serum TSH levels and TSH production rates are
usually normal or even suppressed. For example, Dige-Petersen and Hummer evaluated basal
and TRH-stimulated serum TSH levels in 15 patients with diffuse goitre and 47 patients with
nodular goitre. They found impairment of TRH-induced TSH release in 27% of the patients with
nodular goitre, suggesting thyroid autonomy, but in only 1 of the 15 with diffuse goitre.
Smeulers et al , studied clinically euthyroid women with multinodular goitre and found that there
was an inverse relationship between the increment of TSH after administration of TRH, and size
of the thyroid gland . It was also found that, while being still within the normal range, the mean
4
serum T3 concentration of the group with impaired TSH secretion was significantly higher than
the normal mean, whereas the mean value of serum T4 levels was not elevated. These and other
results are consistent with the hypothesis that a diffuse goitre may precede the development of
nodules. They are also consistent with the clinical observation that, with time, autonomy may
occur, with suppression of TSH release, even though such goitres were originally TSH
dependent.
Factors that may be involved in the evolution of multinodular goiter.
PRIMARY FACTORS
Functional heterogeneity of normal follicular cells, most probably due to genetic and
acquisition of new inheritable qualities by replicating epithelial cells. Gender (women) is an
important factor.
Subsequent functional and structural abnormalities in growing goiters.
SECONDARY FACTORS
Elevated TSH (induced by iodine deficiency, natural goitrogens, inborn errors of thyroid
hormone synthesis)
Smoking, stress, certain drugs
Other thyroid-stimulating factors (IGF-1 and others)
Endogenous factor (gender)
1.5. Pathology
Although it is rare to obtain pathological examination of thyroid glands in the early phase
of development of multinodular goitres, such glands should show areas of hyperplasia with
considerable variation in follicle size. The more typical specimen coming to pathologists is the
goitre that has developed a nodular consistency. Such goitres characteristically present a
variegated appearance, with the normal homogeneous parenchymal structure deformed by the
presence of nodules. The nodules may vary considerably in size (from a few millimeters to
several centimeters); in outline (from sharp encapsulation in adenomas to poorly defined
margination for ordinary nodules); and in architecture (from the solid follicular adenomas to the
gelatinous, colloid-rich nodules or degenerative cystic structures). The graphic term
5
“Puddingstone goitre” has been applied. Frequently the nodules have degenerated and a cyst has
formed, with evidence of old or recent haemorrhage, and the cyst wall may have become
calcified. Often there is extensive fibrosis, and calcium may also be deposited in these septae.
Scattered between the nodules are areas of normal thyroid tissue, and often-focal areas of
lymphocytic infiltration. Radioautography shows a variegated appearance, with RAI localized
sometimes in the adenomas and sometimes in the paranodular tissue. Occasionally, most of the
radioactivity is confined to a few nodules that seem to dominate the metabolic activity of the
gland. If careful sections are made of numerous areas, 4-17% of these glands removed at surgery
will be found to harbor microscopic papillary carcinoma. The variable incidence can most likely
be attributed to the different criteria used by the pathologists and the basis of selection of the
patients for operation by their physicians.
1.6. Natural History of the Disease
Multinodular goitre is probably a lifelong condition that has its inception in adolescence
or at puberty. Minimal diffuse enlargement of the thyroid gland is found in many teenage boys
and girls, and is almost a physiologic response to the complex structural and hormonal changes
occurring at this time. It usually regresses, but occasionally (much more commonly in girls) it
persists and undergoes further growth during pregnancy. This course of events has not been
documented as well as might be desired in sporadic nodular goitre, but it is the usual evolution in
areas where mild endemic goitre is found.
Patients with multinodular goitre seek medical attention for many reasons. Perhaps most
commonly they consult a physician because a lump has been discovered in the neck, or because a
growth spurt has been observed in a goiter known to be present for a long time. Sometimes the
increase in the size of the goitre will cause pressure symptoms, such as difficulty in swallowing,
cough, respiratory distress, or the feeling of a lump in the throat. Rarely, an area of particularly
asymmetrical enlargement may impinge upon or stretch the recurrent laryngeal nerve.
Commonly the goitre is discovered by a physician in the course of an examination for some other
condition. An important scenario is for the patient to seek medical attention because of cardiac
irregularities or congestive heart failure, which proves to be the result of slowly developing
thyrotoxicosis. Many times the goitre grows gradually for a period of a few too many years, and
then becomes stable with little tendency for further growth. It is rare for any noteworthy
6
spontaneous reduction in the size of the thyroid gland to occur, but patients often describe
fluctuation in the size of the goitres and the symptoms they give. These are usually subjective
occurrences, and more often than not the physician is unable to corroborate the changes that the
patient describes. On the other hand, it could be that changes in blood flow through the enlarged
gland account for the symptoms.
Occasionally, a sudden increase in the size of the gland is associated with sharp pain and
tenderness in one area. This event suggests haemorrhage into a nodular cyst of the goiter, which
can be confirmed by ultrasound. Within 3-4 days the symptoms subside, and within 2-3 weeks
the gland may revert to its previous dimensions. In such a situation, acute thyrotoxicosis may
develop and subside spontaneously. Rarely, if ever, do the patients become hypothyroid and if
they do, the diagnosis is more probably Hashimoto’s thyroiditis than nodular goitre. If the goitre
is present for long time, thyrotoxicosis develops in a large number of patients. In a series
collected many years ago at the Mayo Clinic, 60% of patients with MNG over 60 were
thyrotoxic. The average duration of the goitre before the onset of thyrotoxicosis was 17 years;
the longer the goitre had been present the greater was the tendency for thyrotoxicosis to develop.
This condition appears to occur because with the passage of time, autonomous function of the
nodules develops. In a study of patients with euthyroid multinodular goitre, thyroid function was
autonomous in 64 and normal in 26. After a mean follow-up of 5.0 years (maximum 12 years) 18
patients with autonomous thyroid function became overtly hyperthyroid and in 6 patients with
primarily normal thyroid function autonomy develope. Thyroid function tests is illustrated in a
patient with multinodular goitre starting from complete euthyroidism on to overt thyrotoxicosis.
Occasionally a single discrete nodule in the thyroid gland becomes sufficiently active to cause
thyrotoxicosis and to suppress the activity of the rest of the gland. If these patients are given
thyroid hormone, continued function of nodules can be demonstrated by radioiodine scanning
techniques. Thus, these nodules have become independent of pituitary control. When patients
with euthyroid multinodular goiter are frequently tested, it appears that in some of them
occasional transient increases of serum T3 and / or T4 are seen. In several areas of the world
previously iodine deficiency the introduction of iodine supplementation lead to an increase of
hyperthyroidism (non-autoimmune) possibly by excessive thyroid hormone production by “hot”
thyroid nodules.
7
1.7. Diagnosis
1.7.1. Signs and Symptoms
Many of the symptoms of multinodular goitre have already been described. They
are chiefly due to the presence or an enlarging mass in the neck and its impingement
upon the adjacent structures. There may be dysphagia, cough, and hoarseness. Paralysis
of recurrent laryngeal nerve may occur when the nerve is stretched taut across the surface
of an expanding goiter, but this event is very unusual. When unilateral vocal cord
paralysis is demonstrated, the presumptive diagnosis is cancer. Pressure on the superior
sympathetic ganglions and nerves may produce a Horner’s syndrome.
As the gland grows it characteristically enlarges the neck, but frequently the
growth occurs in a downward direction, producing a substernal goitre. A history
sometimes given by an older patient where a goitre once present in the neck has
disappeared may mean that it has fallen down into the upper mediastinum, where its
upper limits can be felt by careful deep palpation. Hemorrhage into this goitre can
produce acute tracheal obstruction. Sometime substernal goitres are attached only by a
fibrous band to the goitre in the neck and extend downward to the arch of the aorta. They
have even been observed as deep in the mediastinum as the diaphragm. Occasionally the
skilled physician can detect a substernal goiter by percussion, particularly if there is a
hint from tracheal deviation, or the presence of a nodular mass in the neck above the
manubrial notch.
Symptoms suggesting constriction of the trachea are frequent, and displacement
of the trachea is commonly found on physical examination. Computer Tomography
examination is useful in defining the extent of tracheal deviation and compression.
Compression is frequently seen but rarely is functionally significant have expected to find
softened tracheal cartilage after the removal of some large goiters, but tracheomalacia has
been observed only on the rarest occasion. Patients may be remarkably tolerant of
nodular goiter even when the enlargement is striking. This finding is especially true in the
endemic goiter areas of the world.
It is generally agreed that, thyroid isotope or ultrasound scanning are of little or
no use in the diagnosis of carcinoma in a multinodular goiter. Two aspects are important
in the differentiation from malignancy. First, the clinical presentation, if the goiter is of
8
longstanding, showing little or no growth, absence of a dominant node, familial, while
there is no neck irradiation in the past, especially in childhood, no hoarse voice, and no
suspicious lymphnodes in the neck, there is little fear for carcinoma.
1.7.2. Laboratory investigation
The choice of tests to investigate the functional status of a patient with a simple
diffuse goitre or multinodular goitre may differ depending on the geographic areas of the
world. Recent surveys conducted in the American, European and Latin American
Thyroid Associations have indicated that the North American thyroidologists are quite
restrictive in the choice of laboratory tests. Most of the experts, however, would perform
a serum TSH and serum Free T4 test. In other settings Total T4 and Total T3 are also
included because of the preferential secretion of T3 over T4 in mild iodine deficiency.
Antibodies against thyro-peroxidase (anti-TPO) and thyroglobulin (anti-TG) are
measured, routinely, by most Europeans and Latin Americans thyroidologists. This seems
to be relevant because thyroid auto antibodies are found approximately in 10% of the
population and, consequently, autoimmunity may coexist with a goiter. Also diffuse or
focal lymphocytic infiltration in an enlarged gland may represent chronic autoimmune
thyroiditis.
Although serum TG correlates with the iodine status and the size of the enlarged
thyroid gland it has little or no value in the diagnosis of goiter.
1.7.3. Diagnostic imaging
Neck palpation is notoriously imprecise with regard to thyroid morphology and
size estimation. Several imaging methods are available in most settings: scintilography
(with radioiodine, technetium), ultrasonography, computed tomography scans, magnetic
resonance imaging and, less frequently used, positron emission tomography (PET).
1.7.3.1. Ultrasonography of the thyroid
The main reasons for the widespread use of thyroid sonography are
availability (several portable models are widely available at a relatively affordable
price), the low cost of the procedure (if performed in the office or in the thyroid
clinic), limited discomfort for the patient, and the non ionizing nature of the
9
method. Ultrasonography may detect non palpable nodules cysts, will estimate
nodule and goiter size (volume), will monitor the changes following therapy and
will guide the Fine Needle Aspiration Biopsy (FNAB). After the introduction of
ultrasonography it has become clear that nodules in the thyroid gland are very
prevalent, ranging from 17% to 60% if older people are included in the study.
Hypoechogenicity, micro-calcifications, indistinct borders increased
nodular flow (visualized by DOPPLER) may have predictive value in
distinguishing malignant from benign nodules (even in Multinodular Goiters).
The possibility of measuring thyroid volume is another highly useful
feature of ultrasonographic studies particularly after therapy with L-T4 or
radioiodine ablation. The volume of the goiter is usually based on the ellipsoid
method (length, width depth X pi/6). This has an observer coefficient of variation
of more than 10%.When compared to CT planimetry the ellipsoid method
underestimate the goiter volume by 20%. Ultrasonography can not evaluate a
multinodular goiter that has partially migrated to the upper mediastinum.
1.7.4. Scintigraphy (isotope imaging)
It was used routinely in the past but at present has little place in the evaluation of
a multinodular goiter (101-105). It is helpful in the determination of the functionality of
the various nodules of a MNG. Thyroid scintigrams have been used through many years
for measurement of the thyroid volume but compared to other methods is very inaccurate.
1.7.5. Computed tomography (CT) and Magnetic resonance (MR)
CT and MR provide high-resolution visualization of the goiter (Simple diffuse,
multinodular). The major strength of CT and MR is their ability to diagnose and assess
the extent of substernal goiters. Another advantage of the CT is the possibility for
planimetric volume estimations, quite useful in irregularly enlarged multinodular goiter.
Recently the ionizing radiation delivered by a CT procedure has been source of
concern for both clinicians and radiologists. Therefore the use of CT as an imaging
method should be reserved for intra thoracic multinodular goiters, with tracheal
compression.
10
1.8. Differential Diagnosis
Adenoma
Cyst
Carcinoma
Multinodular goitre
Hashimoto’s thyroiditis
Subacute thyroiditis
Effect of prior operation or 131I therapy
Thyroid hemiagenesis
Metastasis
Parathyroid cyst or adenoma
Thyroglossal cyst
Nonthyroidal lesions
o Inflammatory or neoplastic nodes
o Cystic hygroma
o Aneurysm
o Bronchocele
o Laryngocele
1.9. Treatment
Unlike Graves disease, Multinodular goitre (MNG) is not an autoimmune disease and
rarely, if ever, remits. Therefore, patients who have autonomously functioning nodules should be
treated definitely with radioactive iodine or surgery. The American Thyroid Association and
American Association of Clinical Endocrinologists have released guidelines for the management
of hyperthyroid and other causes of thyrotoxicosis, including the use of radioactive iodine or
surgery to treat toxic multinodular goitre.
Patients with subclinical hyperthyroidism should be monitored closely for overt disease.
Some suggest that elderly patients, women with osteopenia, and patients with risk factors for
atrial fibrillation should be treated, even those who have subclinical disease.
11
1.9.1. Na131 I treatment
Radioactive iodine is considered the treatment of choice for Toxic MNG. Except
for pregnancy, there are no absolute contraindications to radioiodine therapy.
o A single dose of radioiodine therapy has a success rate of 85-100% in patients
with TNG. Radioiodine therapy may reduce the size of the goiter by up to 40%.
o Failure of initial treatment with radioactive iodine has been associated with
increased goiter size and higher T3 and free T4 levels, which suggests that these
factors may present a need for higher doses of Na131 I.
o A positive correlation exists between radiation dose to the thyroid and decrease in
thyroid volume. In patients with uptake of less than 20%, pretreatment with
lithium, PTU, or recombinant TSH can increase the effectiveness of iodine uptake
and treatment. This treatment may be valuable in elderly patients in whom
surgery is considered high risk.
o Complications
Hypothyroidism occurs in 10-20% of patients; this is similar to the
incidence rate after surgery and is substantially less than in the treatment
of Graves disease.
Tracheal compression due to thyroid swelling after radiation therapy is no
longer thought to be a risk.
Mild thyrotoxic symptoms after radioiodine occur in about one-third of
patients, and about 4% of patients develop a clinically significant
radiation-induced thyroiditis. These patients should be treated
symptomatically with beta blockers.
Elderly patients may have exacerbation of congestive heart failure and
atrial fibrillation. Pretreat elderly patients with antithyroid drugs.
Thyroid storm is a rare complication, particularly in patients with rapidly
enlarging goiters or high total T3 levels. Patients with these conditions
should receive pretreatment with antithyroid drugs.
12
1.9.2. Pharmacotherapy
Antithyroid drugs and beta blockers are used for short courses in the treatment of MNG;
they are important in rendering patients euthyroid in preparation for radioiodine or surgery and in
treating hyperthyroidism while awaiting full clinical response to radioiodine. Patients with
subclinical disease at high risk of complications (eg, atrial fibrillation, osteopenia) may be given
a trial of low dose methimazole (5-15 mg/d) or beta blockers and should be monitored for a
change in symptoms or for disease progression that requires definitive treatment.
o Thioamides - The role of therapy with thioamides (eg, PTU, methimazole) is to
achieve euthyroidism prior to definitive treatment with either surgery or
radioiodine therapy. Data suggest that pretreated patients have decreased response
to radioiodine. The general recommendation is to stop antithyroid agents at least 4
days prior to radioiodine therapy in order to maximize the radioiodine effect.
Antithyroid drugs and beta blockers have side effects, the most common
being pruritic rash, fever, gastrointestinal upset, and arthralgias. More
serious potential side effects include agranulocytosis, drug-induced lupus
and other forms of vasculitis, and liver damage.
PTU is considered to be a second-line drug therapy, except in patients who
are allergic to or intolerant of methimazole, or in women who are in the
first trimester of pregnancy. Rare cases of embryopathy, including aplasia
cutis, have been reported with methimazole during pregnancy. The FDA
recommends the following criteria be considered for prescribing PTU:
Reserve PTU use during first trimester of pregnancy, or in patients
who are allergic to or intolerant of methimazole.
Closely monitor PTU therapy for signs and symptoms of liver
injury, especially during the first 6 months after initiation of
therapy.
For suspected liver injury, promptly discontinue PTU therapy,
evaluate the patient for evidence of liver injury, and provide
supportive care.
13
PTU should not be used in pediatric patients unless the patient is
allergic to or intolerant of methimazole and no other treatment
options are available.
Counsel patients to promptly contact their health care provider for
the following signs or symptoms: fatigue, weakness, vague
abdominal pain, loss of appetite, itching, easy bruising, or
yellowing of the eyes or skin.
o Beta-adrenergic receptor antagonists - These drugs remain useful in the treatment
of symptoms of thyrotoxicosis; they may be used alone in patients with mild
thyrotoxicosis or in conjunction with thioamides for treatment of more severe
disease.
Propranolol, a nonselective beta blocker, may help to lower the heart rate,
control tremor, reduce excessive sweating, and alleviate anxiety.
Propranolol is also known to reduce the conversion of T4 to T3.
In patients with underlying asthma, beta-1 selective antagonists, such as
atenolol or metoprolol, would be safer options.
In patients with contraindications to beta blockers (eg, moderate to severe
asthma), calcium channel antagonists (eg, diltiazem) may be used to help
control the heart rate.
Surgical therapy is usually reserved for young individuals, patients with 1 or more large nodules
or with obstructive symptoms, patients with dominant nonfunctioning or suspicious nodules,
patients who are pregnant, patients in whom radioiodine therapy has failed, or patients who
require a rapid resolution of the thyrotoxic state.
Subtotal thyroidectomy results in rapid cure of hyperthyroidism in 90% of patients and
allows for rapid relief of compressive symptoms.
Restoring euthyroidism prior to surgery is preferable.
Complications of surgery include the following:
o In patients who are treated surgically, the frequency of hypothyroidism is similar
to that found in patients treated with radioiodine (15-25%).
14

o Complications include permanent vocal cord paralysis (2.3%), permanent
hypoparathyroidism (0.5%), temporary hypoparathyroidism (2.5%), and
significant postoperative bleeding (1.4%).
o Other postoperative complications include tracheostomy, wound infection, wound
hematoma, myocardial infarction, atrial fibrillation, and stroke.
o The mortality rate is almost zero.
1.10. Complications
Hyperthyroid complications
o The most important complications are related to the heart.
o Cardiomyopathy resulting in severely depressed function may be observed with
hyperthyroidism, possibly in relation to persistent tachycardia. Fortunately,
cardiomyopathy resolves remarkably with resolution of the hyperthyroid state.
o Using anticoagulants to treat patients exhibiting atrial fibrillation remains
controversial, although it is recommended by many authorities. Atrial fibrillation
of long duration that is associated with other anatomical defects of the heart
should be treated with warfarin or another suitable anticoagulant.
1.11. Prognosis
Most treated patients have a good prognosis. A worse prognosis is related to untreated
hyperthyroidism. If left untreated, hyperthyroidism may lead to osteoporosis, arrhythmia, heart
failure, coma, and death. Regular assessment of thyroid function is important in monitoring
disease.
Na131 I ablation may result in continued hyperthyroidism, with some patients (up to 73%
in some studies, depending on the size of the goiter and the dosing of radioiodine) requiring
repeated treatment or surgical removal of the gland. Hypothyroidism after radioiodine ablation
has been reported in 0-35% of individuals. .
Surgical treatment usually consists of a lobectomy of the hyperfunctioning nodule. The
rate of hypothyroidism associated with this procedure is very low. Rates of hyperthyroidism
recurrence with surgery have been reported to be as low as 0-9%. Larger, multinodular goiters
may require total thyroidectomy.
15
CHAPTER 2
THEORY: GENERAL ANESTHESIA
INTRODUCTION
Anesthesia is an important field of medicine that has made complicated surgeries
possible. It involves the administration of substances or drugs to patients which causes loss of
consciousness, loss of verbal ability, absence of recall and loss of protective reflexes e.g. cough,
gag and withdrawal from pain.
Anesthesia means “without feeling” (no sensation), whereas analgesia means “without
pain”. Although a patient is anesthetized but without proper analgesia, there will be evidence of
pain such as tachycardia and hypertension. Thus, one must not think that a person will not feel
pain when he is anesthetized.
General anesthesia (GA) is the state produced when a patient receives medications for
amnesia, analgesia, muscle paralysis, and sedation. An anesthetized patient can be thought of as
being in a controlled, reversible state of unconsciousness. Anesthesia enables a patient to tolerate
surgical procedures that would otherwise inflict unbearable pain, potentiate extreme physiologic
exacerbations, and result in unpleasant memories.
The combination of anesthetic agents used for general anesthesia often leaves a patient with
the following clinical constellation:
1. Unarousable even secondary to painful stimuli
2. Unable to remember what happened (amnesia)
3. Unable to maintain adequate airway protection and/or spontaneous ventilation as a result
of muscle paralysis
4. Cardiovascular changes secondary to stimulant/depressant effects of anesthetic agents.
2.1. General Anesthesia
General anesthesia uses intravenous and inhaled agents to allow adequate surgical access
to the operative site. A point worth noting is that general anesthesia may not always be the best
choice; depending on a patient’s clinical presentation, local or regional anesthesia may be more
appropriate.
16

Anesthesia providers are responsible for assessing all factors that influence a patient's
medical condition and selecting the optimal anesthetic technique accordingly. Attributes of
general anesthesia include the following:
Advantages
o Reduces intraoperative patient awareness and recall
o Allows proper muscle relaxation for prolonged periods of time
o Facilitates complete control of the airway, breathing, and circulation
o Can be used in cases of sensitivity to local anesthetic agent
o Can be administered without moving the patient from the supine position
o Can be adapted easily to procedures of unpredictable duration or extent
o Can be administered rapidly and is reversible
Disadvantages
o Requires increased complexity of care and associated costs
o Requires some degree of preoperative patient preparation
o Can induce physiologic fluctuations that require active intervention
o Associated with less serious complications such as nausea or vomiting, sore
throat, headache, shivering, and delayed return to normal mental functioning
o Associated with malignant hyperthermia, a rare, inherited muscular condition in
which exposure to some (but not all) general anesthetic agents results in acute and
potentially lethal temperature rise, hypercarbia, metabolic acidosis, and
hyperkalemia
With modern advances in medications, monitoring technology, and safety systems, as
well as highly educated anesthesia providers, the risk caused by anesthesia to a patient
undergoing routine surgery is very small. Mortality attributable to general anesthesia is said to
occur at rates of less than 1:100,000. Minor complications occur at predicable rates, even in
previously healthy patients. The frequency of anesthesia-related symptoms during the first 24
hours following ambulatory surgery is as follows:
Vomiting - 10-20%
Nausea - 10-40%
Sore throat - 25%
Incisional pain - 30%
17

2.2. Preparation for General Anesthesia
Safe and efficient anesthetic practices require certified personnel, appropriate
medications and equipment, and an optimized patient.
Minimum infrastructure requirements for general anesthesia include a well-lit space of
adequate size; a source of pressurized oxygen (most commonly piped in); an effective suction
device; standard ASA (American Society of Anesthesiologists) monitors, including heart rate,
blood pressure, ECG, pulse oximetry, capnography, temperature; and inspired and exhaled
concentrations of oxygen and applicable anesthetic agents.
Beyond this, some equipment is needed to deliver the anesthetic agent. This may be as
simple as needles and syringes, if the drugs are to be administered entirely intravenously. In most
circumstances, this means the availability of a properly serviced and maintained anesthetic gas
delivery machine.
An array of routine and emergency drugs, including Dantrolene sodium (the specific
treatment for malignant hyperthermia), airway management equipment, a cardiac defibrillator,
and a recovery room staffed by properly trained individuals completes the picture.
2.3. Preparing the patient
Preoperative evaluation allows for proper laboratory monitoring, attention to any new or
ongoing medical conditions, discussion of any previous personal or familial adverse reactions to
general anesthetics, assessment of functional cardiac and pulmonary states, and development of
an effective and safe anesthetic plan. It also serves to relieve anxiety of the unknown surgical
environment for patients and their families. Overall, this process allows for optimization of the
patient in the perioperative setting.
Physical examination associated with preoperative evaluations allow anesthesia providers
to focus specifically on expected airway conditions, including mouth opening, loose or
problematic dentition, limitations in neck range of motion, neck anatomy, and Mallampati
presentations. By combining all factors, an appropriate plan for intubation can be outlined and
extra steps, if necessary, can be taken to prepare for fiberoptic bronchoscopy, video
laryngoscopy, or various other difficult airway interventions.
18
Airway management
Possible or definite difficulties with airway management include the following:
Small or receding jaw
Prominent maxillary teeth
Short neck
Limited neck extension
Poor dentition
Tumors of the face, mouth, neck, or throat
Facial trauma
Interdental fixation
Hard cervical collar
Halo traction
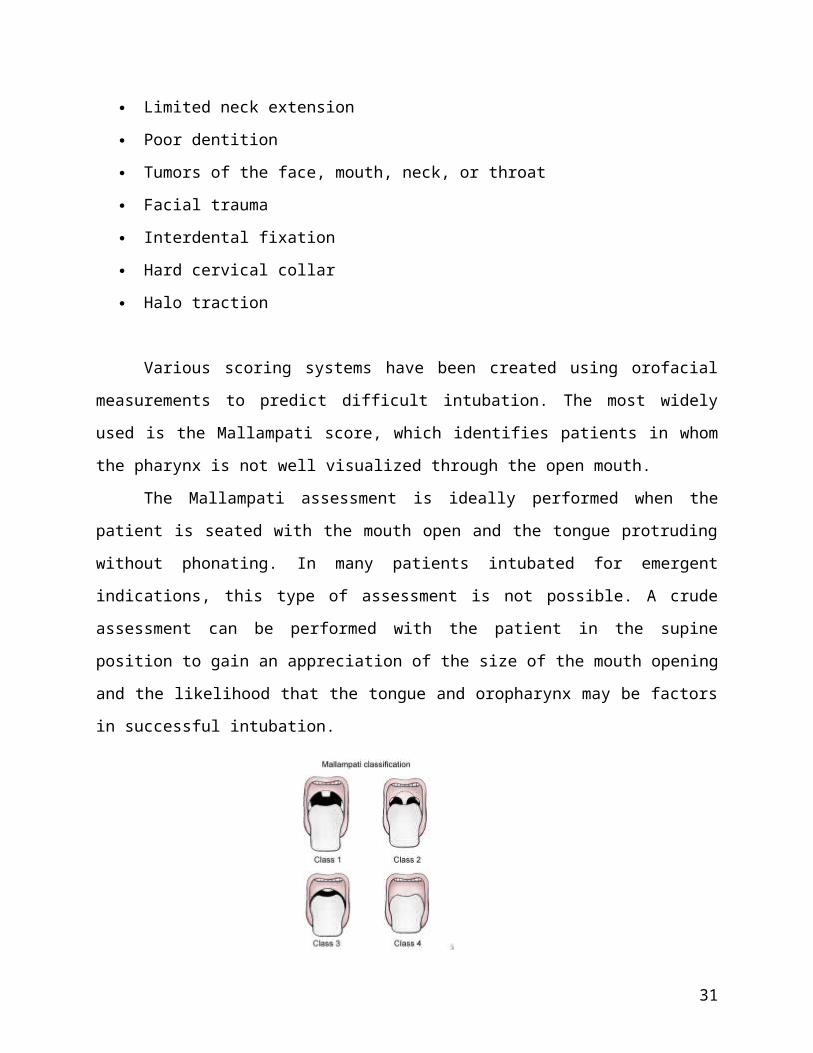
Various scoring systems have been created using orofacial measurements to predict
difficult intubation. The most widely used is the Mallampati score, which identifies patients in
whom the pharynx is not well visualized through the open mouth.
The Mallampati assessment is ideally performed when the patient is seated with the
mouth open and the tongue protruding without phonating. In many patients intubated for
emergent indications, this type of assessment is not possible. A crude assessment can be
performed with the patient in the supine position to gain an appreciation of the size of the mouth
opening and the likelihood that the tongue and oropharynx may be factors in successful
intubation.
Mallampati classification.
19
High Mallampati scores have been shown to be predictive of difficult intubations.
However, no one scoring system is near 100% sensitive or 100% specific. As a result,
practitioners rely on several criteria and their experience to assess the airway.
When suspicion of an adverse event is high but a similar anesthetic technique must be
used again, obtaining records and previous anesthetic records from previous operations or from
other institutions may be necessary.
Other requirements
The need for coming to the operating room with an empty stomach is to reduce the risk of
pulmonary aspiration during general anesthesia when a patient loses his or her ability to
voluntarily protect the airway.
Patients should continue to take regularly scheduled medications up to and including the
morning of surgery. Exceptions may include the following:
Anticoagulants to avoid increased surgical bleeding
Oral hypoglycemics (For example, metformin is an oral hypoglycemic agent that is
associated with the development of metabolic acidosis under general anesthesia.)
Monoamine oxidase inhibitors
Beta blocker therapy (However, beta blocker therapy should be continued perioperatively
for high-risk patients undergoing major noncardiac surgery)
2.4. The process of anesthesia
2.4.1. Premedication
This is the first stage of a general anesthetic and usually conducted in the surgical
ward or in a preoperative holding area. The goal of premedication is to have the patient arrive
in the operating room in a calm, relaxed frame of mind.
Most patients do not want to have any recollection of entering the operating room.
The most commonly used premedication is midazolam, a short-acting benzodiazepine. For
example, midazolam syrup is often given to children to facilitate calm separation from their
parents prior to anesthesia. In anticipation of surgical pain, nonsteroidal anti-inflammatory
drugs or acetaminophen can be administered preemptively. When a history of
20
gastroesophageal reflux exists, H2 blockers and antacids may be administered. Drying agents
(eg, atropine, scopolamine) are now only administered routinely in anticipation of a
fiberoptic endotracheal intubation.
2.4.2. Induction
This is the critical part of the anesthesia process. Usually, the mnemonic DAMMIS
can be used to remember what to check ( D rugs, A irway equipment, M achine, M
onitors, I V, S uction).
This stage can be achieved by intravenous injection of induction agents (drugs that
work rapidly, such as propofol), by the slower inhalation of anesthetic vapors delivered into a
face mask, or by a combination of both.
For the most part, contemporary practice dictates that adult patients and most children
aged at least 10 years be induced with intravenous drugs, this being a rapid and minimally
unpleasant experience for the patient. However, sevoflurane, a well-tolerated anesthetic
vapor, allows for elective inhalation induction of anesthesia in adults.
In addition to the induction drug, most patients receive an injection of an opioid
analgesic, such as fentanyl (a synthetic opioid many times more potent than morphine).
Many synthetic and naturally occurring opioids with different properties are available.
Induction agents and opioids work synergistically to induce anesthesia. In addition,
anticipation of events that are about to occur, such as endotracheal intubation and incision of
the skin, generally raises the blood pressure and heart rate of the patient. Opioid analgesia
helps control this undesirable response.
The next step of the induction process is securing the airway. This may be a simple
matter of manually holding the patient's jaw such that his or her natural breathing is
unimpeded by the tongue, or it may demand the insertion of a prosthetic airway device such
as a laryngeal mask airway or endotracheal tube. Various factors are considered when
making this decision. The major decision is whether the patient requires placement of an
endotracheal tube. Potential indications for endotracheal intubation under general anesthesia
may include the following:
o Potential for airway contamination (full stomach, gastroesophageal [GE] reflux,
gastrointestinal [GI] or pharyngeal bleeding)
21
o Surgical need for muscle relaxation
o Predictable difficulty with endotracheal intubation or airway access (eg, lateral or
prone patient position)
o Surgery of the mouth or face
o Prolonged surgical procedure
Not all surgery requires muscle relaxation. If surgery is taking place in the abdomen
or thorax, an intermediate or long-acting muscle relaxant drug is administered in addition to
the induction agent and opioid. This paralyzes muscles indiscriminately, including the
muscles of breathing. Therefore, the patient's lungs must be ventilated under pressure,
necessitating an endotracheal tube.
Persons who, for anatomic reasons, are likely to be difficult to intubate are usually
intubated electively at the beginning of the procedure, using a fiberoptic bronchoscope or
other advanced airway tool. This prevents a situation in which attempts are made to manage
the airway with a lesser device, only for the anesthesia provider to discover that oxygenation
and ventilation are inadequate. At that point during a surgical procedure, swift intubation of
the patient can be very difficult, if not impossible.
2.4.3. Maintenance phase
At this point, the drugs used to initiate the anesthetic are beginning to wear off, and
the patient must be kept anesthetized with a maintenance agent. For the most part, this refers
to the delivery of anesthetic gases (more properly termed vapors) into the patient's lungs.
These may be inhaled as the patient breathes spontaneously or delivered under pressure by
each mechanical breath of a ventilator.
The maintenance phase is usually the most stable part of the anesthesia. However,
understanding that anesthesia is a continuum of different depths is important. A level of
anesthesia that is satisfactory for surgery to the skin of an extremity, for example, would be
inadequate for manipulation of the bowel.
As the procedure progresses, the level of anesthesia is altered to provide the minimum
amount of anesthesia that is necessary to ensure adequate anesthetic depth. Traditionally, this
has been a matter of clinical judgment, but new processed EEG machines give the anesthesia
22
provider a simplified output in real time, corresponding to anesthetic depth. These devices
have yet to become universally accepted as vital equipment.
If muscle relaxants have not been used, inadequate anesthesia is easy to spot. The
patient moves, coughs, or obstructs his airway if the anesthetic is too light for the stimulus
being given. If muscle relaxants have been used, then clearly the patient is unable to
demonstrate any of these phenomena. In these patients, the anesthesia provider must rely on
careful observation of autonomic phenomena such as hypertension, tachycardia, sweating,
and capillary dilation to decide whether the patient requires a deeper anesthetic. This requires
experience and judgment.
The specialty of anesthesiology is working to develop reliable methods to avoid cases
of awareness under anesthesia. Excessive anesthetic depth, on the other hand, is associated
with decreased heart rate and blood pressure, and, if carried to extremes, can jeopardize
perfusion of vital organs or be fatal. Short of these serious misadventures, excessive depth
results in slower awakening and more adverse effects.
As the surgical procedure draws to a close, the patient's emergence from anesthesia is
planned. Experience and close communication with the surgeon enable the anesthesia
provider to predict the time at which the application of dressings and casts will be complete.
In advance of that time, anesthetic vapors have been decreased or even switched off entirely
to allow time for them to be excreted by the lungs. Excess muscle relaxation is reversed
using specific drugs and an adequate long-acting opioid analgesic to keep the patient
comfortable in the recovery room. If a ventilator has been used, the patient is restored to
breathing by himself, and, as anesthetic drugs dissipate, the patient emerges to consciousness.
Removal of the endotracheal tube or other artificial airway device is only performed
when the patient has regained sufficient control of his or her airway reflexes.
2.4.4. Reversal
It is a process of discontinuation of anesthetic agents at the end of surgery to allow
return of consciousness and recovery from muscle paralysis while maintaining analgesia.
Volatile agents are discontinued first and later the nitrous oxide. Patient is given
100% oxygen. Wait for return of spontaneous breathing; this can be observed on
capnography and can also be felt with reservoir bag if patient is manually ventilated.
23

Administer reversal agent such as neostigmine (anticholinesterase) or glycopyrrolate
to counteract non-depolarizing muscle relaxant; atropine is usually given to counteract the
parasympathetic effects of anticholinesterase.
Reversal agent is given when there is evidence of spontaneous breathing effort.
Patient’s tidal volume has to be ensured that it is adequate and able to control own airway
before attempting extubation.
2.5. Postoperative Care
The anesthesia should conclude with a pain-free awakening and a management plan for
postoperative pain relief. This may be in the form of regional analgesia, oral, transdermal or
parenteral medication. Minor surgical procedures are amenable to oral pain relief medication
such as paracetamol and NSAIDs such as ibuprofen. Moderate levels of pain require the addition
of mild opiates such as tramadol. Major surgical procedures may require a combination of
modalities to confer adequate pain relief.
Parenteral methods include patient-controlled analgesia (PCA) involving a strong opiate
such as morphine, fentanyl or oxycodone. To activate a syringe device, patient will press a
button and receive a preset dose or bolus of the drug (eg: 1mg of morphine). The PCA device
then locks out for a preset period to allow drug to take effect. If the patient becomes too sleepy or
sedated, they make no more morphine requests. This confers a fail safe aspect which is lacking in
continuous opiate infusion techniques.
Shivering is a frequent occurs in the post operative period. Apart from causing discomfort
and exacerbating post operative pain, shivering has been shown to increase oxygen consumption,
cathecolamine release, cardiac output, heart rate, blood pressure and intra ocular pressure. There
are number of techniques used to reduce this occurrence, such as increasing the ambient
temperature in theatre, using conventional or forced warm air blankets and using warmed
intravenous fluids.
2.6. Common Anesthetic Drugs
The main group of drugs commonly used in general anesthesia are broadly classified into
induction agents, muscle relaxants, analgesics and reversal agents. Induction agents then are
24
further classified into inhalational and parenteral while the muscle relaxants can be divided into
depolarizers and non depolarizers.
2.6.1. Inhalational Anaesthetic Agents
It exists as gaseous form (nitrous oxide) or volatile liquids (isoflurane).
Halothane is a halogenated alkane derivative. Other modern volatile agents are
halogenated methyl ether derivatives (enflurane, isoflurane). Controllability is by
pulmonary administration and is delivered via vaporizers. The commonly used
inhalational agents are liquids at room temperature and therefore they need to be
converted to the gaseous state for administration to patients. Vaporizers is a
device for producing a clinically useful and stable concentration of an anesthetic
vapour in a carrier gas ( oxygen and nitrous oxide). The aim of inhalational
anaesthesia is the development of an appropriate tension or partial pressure of
anesthetic agent within the brain.
- Gaseous anaesthetic agents
Nitrous oxide
o It is stored in steel cylinders as a liquid under pressure in equilibrium
with the gas phase at normal room temperature.
o N2O is a colorless gas without appreciable odour or taste and non
explosive.
o It is a potent analgesic but a weak anaesthetic agents
o It cause depress hematopoietic function ( megaloblastic anemia,
thrombocytopenia and leucopenia), thus not advisable for
administration of more than 24 hours.
o It is widely used as an adjuvant to lower the MAC of volatile
anesthetics. With inhalation of 70% N2O / 30% O2 MAC value are
reduced (~35%- 45%)
- Volatile Anesthetic agents
Halothane
Halothane is a haloalkane and has a MAC value of 70%. It can be used
for induction of anesthesia in children. Halothane is a non specific Ca2+ influx
inhibitor and it may cause bradycardia. It increases the automaticity of the heart
25

and when combined with adrenaline it may cause tachyarrythmias. One of the
important side effects is ha;othane hepatotoxicity. The diagnosis of halothane
hepatitis is by exclusion. This may progress into fulminant hepatic failure with a
high mortality. Obese middle aged women having repeat halothane exposures are
at risk. Halothane hepatitis may occur following a single exposure.
Isoflurane
It causes a dose dependent reduction in blood pressure. The decrease in
blood pressure is due to vasodilatation and decreased total peripheral resistance.
The heart rate is increased via reflex mechanisms but arrhythmias are uncommon.
Isoflurane does not affect ventricular conduction and does not increase the
excitability of ventricular myocardium. Induction of anesthesia is difficult with
isoflurane due to its pungent odour and preanesthetic concentration of isoflurane
may cause an airway reflex stimulation, with increased secretions and/or
coughing and laryngospasm.
Sevoflurane
It is a new inhalational agent and more expensive than others. It has
pleasant odour and can be used as induction agents in paediatric and adult
patients. It has rapid onset of induction and recovery of anesthesia because it is
less soluble in blood than isoflurane. It has a mild negative inotropic effect. It also
decreases systemic vascular resistance but does not cause reflex tachycardia.
Sevoflurane is less arrythmogenic when compared to halothane and it is suitable
for daycare surgery.
2.6.2. Intravenous induction agents
Criteria for ideal intravenous anesthetic agents:
Induction of anesthesia should be rapid, smooth and safe
It should have limited effects on cardiovascular and respiratory systems
It should possess analgesic activity.
Consciousness should return rapidly, smoothly and predictably.
26
a. Sodium thiopental (Pentothal)
Thiopental is the only intravenous barbiturate being used today and is
classified under an ultra short acting barbiturate. It is prepared as a 2.5% solution,
water soluble, pH of 10.5 and stable for up to 1-2 weeks if refrigerated.
Mechanism of action: Depress the reticular activating system, reflecting the
ability of barbiturates to decrease the rate of dissociation of the inhibitory
neurotransmitter GABA from its receptors
Pharmacokinetics
Short duration of action (5-10 minutes) following IV bolus reflects high lipid
solubility and redistribution from the brain to inactive tissues.
Protein binding parallels lipids solubility, decreased protein binding increases
drug sensitivity.
Fat is the only compartment in which thiopental continues to accumulate 30
minutes after injection
Thiopental is metabolized in the liver slowly. Its hepatic excretion ratio is 0.15
It has an anticonvulsant effect and is a useful drug for cerebral protection
in head injury. It also has an analgesics effect. In the presence of inadequate
anaesthesia, airway manipulation may result in bronchospasm and laryngospasm.
Cardiovascular effects of barbiturate include decrease in blood pressure due to
vasodilatation and direct myocardial depression. There is a compensatory
increased in heart rate.
It should be used cautiously in haemodynamically unstable patients and is
contraindicated in hypovolaemia and hypotensive patients. Induction dose is 3-
5mg/kg in a healthy adult.
b. Propofol
It is 2,6- diisopropyl-phenol, under group of hindered phenol, an
alkylphenol derivative. Formulated in a solution with 10% soy bean oil,
27
hydrophobic nature. It has rapid onset and short duration of action. Emergence
and awakening are prompt and complete after even prolonged infusions.
Mechanism of action: Propofol increases the inhibitory neurotransmission
mediated by gammaaminobutyric acid.
It has extensive metabolism by hepatic and extrahepatic. It has no
cumulative effects, has antiemetic property and suitable for daycare surgery. It
does not has antianalgesic activity.
Propofol is an ideal drug for total intravenous anesthesia. The target
controlled induction (TCI) and maintenance of anesthesia can be achieved
nowadays with propofol by a special TCI pump. Propofol also can be used to
provide sedation in ICU, for minor procedures or in combination with regional
anesthesia.
Effects on organ system
Cardiovascular : decrease in arterial blood pressure secondary to a drop in
systemic vascular resistance, contractility, and preload. Hypotension is more
pronounced than with thiopental. Propofol markedly impairs the normal arterial
baroreflex response to hypotension.
Respiratory: propofol causes profound respiratory depression. Propofol
induced depression of the upper airway reflexes exceeds that of thiopental
Cerebral: decreases cerebral blood flow and intracranial pressure.
Induction dose: 1.5-3 mg/ kg in a healthy adult.
c. Ketamine
It is a phenicyclidine derivative. It produces dissociative anesthesia
resulting in catatonia, amnesia and analgesia. Patient may appear awake and
reactive but does not response to sensory stimuli
Mechanism of action: It acts on NMDA receptor. It blocks polysynaptic
reflexes in the spinal cord, inhibiting excitatory neurotransmitter effects. It has
both anesthetic and analgesic properties. It causes postoperative psychic
phenomena- emergence delirium, vivid dreams, hallucination. Therefore it is not
28
suitable for adults. These effects can be minimized by combination with
benzodiazepines.
Clinical usage:
Induction of anesthesia in poor risk patients (eg: hypotension or bronchial
asthma)
As sole agent in dressing of burns, radiological procedures in children,
mass casualties in the field.
In the management of unresponsive severe bronchospasm
It is contraindicated in raised intracranial pressure, perforating eye
surgery, hypertension, heart failure, recent myocardial infarction, aneurysm and
valvular heart disease.
Dosage:
o IV 1.5-2 mg/kg, onset 30 sec. duration 5-10min.
o IM 10 mg/kg, onset 3-8min, duration 10-20min
Systemic effects:
Increase intracranial and intraocular pressures
Postoperative nausea and vomiting
Increased salivation. An antisialagogue is recommended before used
Preservation of airway reflexes and produces brochodilatation
Increased in cathecolamines secretion
Ketamine has cardiovascular effects: increases heart rate, blood pressure
and pulmonary arterial pressure. It is most likely due to direct stimulation of the
sympathetic nervous system.
2.6.3. Neuromuscular blocking agents
Muscle relaxants are generally classified into two groups, depending on
their mechanism of action.
1. Depolarizing muscle relaxants.
a. Example: succinylcholine
2. Non depolarizing muscle relaxants
a. Intermediate acting: vecuronium, atracurium, rocuronium
b. Long acting: pancuronium
29

1. Depolarizing muscle relaxants
Used to provide skeletal muscle relaxation to facilitate tracheal intubation
and optimal surgical condition. Ventilation must be provided as the diaphragmatic
muscle would also be paralysed. There is no CNS activity and the problem of
awareness begin with introduction induction of muscle relaxants.
Factors that influence inclusion of muscle relaxants in general anesthesia
are types of surgical procedures (anatomic location and patient position),
anesthetic techniques and patient factors (ASA class, obese, exreme of age).
Succinylcholine
The only depolariser drug that is used clinically. It consists of two
molecules of acetylcholine linked together. It acts on nicotinic receptors at
neuromuscular junction (NMJ) to cause sustained depolarization that
prevents propagation of action potential. The net effect of SCh induced
depolarization is uncoordinated skeletal muscle activity that is seen as
fasciculation.
It remains a useful muscle relaxants because of its rapid onset and
short duration of muscular relaxation that cannot be achieved by any other
available nondepolarising muscle relaxants.
A dose of 1-2 mg/kg produces profound muscle relaxation within
one minute. Full recovery is 10-12 minutes. It is used in emergency
surgery as rapid sequence induction technique and in situation of difficult
airway management.
Side effects
It may cause cardiac dysarryhmias such as bradycardia especially in
children.
Hyperkalemia – at risk patients (burns, extensively trauma, unrecognized
muscular dystrophy and denervation injuries.
Increased intragastric pressure (offset by even greater increase in lower
oesophageal sphincter)
Increased intraocular pressure (due to cycloplegic action of
succinylcholine)
30
Prolonged response in presence of atypical cholinesterase
Increased intracranial pressure
Muscle pain and myoglobinuria
2 Non depolarizing muscle relaxant
Acts on nicotinic receptors in a competitive fashion to produce
neuromuscular blockade- absence od depolarization. Can be antagonized by
anticholinesterase drugs. They are used to facilitate endotracheal intubation,
controlled ventilation and maintenance of muscle relaxation during surgical
procedures.
a. Atracurium
It is an intermediate acting benzyliso-quinolinium type NDMR. The
intubation dose is 0.5-0.6mg/kg. It presents as 10mg/ml solution in 25mg or 50mg
glass ampoules and is stored at 4 °C. Histamine release may occur in susceptible
patients but anaphylactoid reaction is very rare.
b. Vecuronium
It is an aminosteroid group and presents as freezed dried powder and
diluted with sterile water before used. There is no histamine release and devoid of
cardiovascular side effects. It does not antagonize fentanyl induced bradycardia. It
is metabolized by liver and also excreted unchanged in bile. The intubation dose
is 0.08-0.1 mg/kg.
c. Rocuronium
It is an aminosteroid group. Its rapid onset of action makes it a potential
replacement for SCh when rapid tracheal intubation is needed. Its duration of
action is similar to vecuronium and has similar pharmacokinetic characteristic. It
has minimal cardiovascular side effects and very low potential for histamine
release. Dosage for endotracheal intubation is 0.6 mg/kg.
d. Pancuronium
It is a long acting NDMR with a steroid structure (Bisaminoquaternary
steroid). It increases heart rate and blood pressure and cardiac output due to
31
cardiac vagal blockade. Histamine release is very rare and bronchospasm is
extremely uncommon.
Assessment of neuromuscular blockade
1. Clinical assessment
a. Ability to lift up head for 5 second
b. Hand grip for 5 second
c. Ability to produce vital capacity breath > 10 ml/kg
d. Tongue protrusion
2. Responses to electrical stimulation of a peripheral nerve stimulator
Anticholinesterase
Anticholinesterase is used to reverse non depolarizers. It inhibits the action of
acetylcholinesterase and increase the concentration of acetylcholine at the neuromuscular
junction. It also acts at parasympathetic nerve endings.
In excessive doses, acetylcholineesterase inhibitors can paradoxically potentiate a
nondepolarizing neuromuscular blockade and prolong the depolarization blockade of
succinylcholine. Anticholinesterase increases acetylcholine at both nicotinic and muscarinic
receptors. Muscarinic effects can be blocked by administration of atropine or glycopyrolate.
2.6.4. Opioid analgesics
Few examples of this drugs are morphine, pethidine, fentanyl and nalbuphine.
This drugs act on opioid receptors and classified as full agonist, antagonist, or mixed
agonist-antagonist depending on the actions on the opioid receptors. Three main receptors
are mu, kappa and delta.
Classification of opioid receptors
Mu receptors: morphine is the prototype exogenous ligand.
Mu-1: the main action at this reseptors is analgesia, but also responsible for
miosis, nausea/vomiting, urinary retention and pruritus. The endogenous ligands
are enkephalins.
32
Mu-2: respiratory depression, euphoria, bradycardia, ileus and physical
dependence are elicited by binding at this receptor.
Kappa: Ketocyclazocine and dynorphin are the prototype exogenous and endogenous
ligands respectively. Analgesia, sedation, dysphoria and psychomimetic effects are
produced by this receptor. Binding to kappa receptor can inhibit release of vasopressin
and thus promote dieresis.
Delta: It is a modulation of Mu receptor. Has high selective for the endogenous
enkephalins, but opioid drugs still bind (leuenkephalin and beta-endorphin).
Morphine pharmacokinetics:
Elimination halftimes for morphine following bolus administration is about 1.7-4.5
hours. Following bolus administration onset time is relatively slow (15-30 minutes)
because:
1. morphine exhibits relatively low lipid solubility about 2.5% of fentanyl
(Sublimaze)
2. at physiological pH, morphine, a weak base with the pKa of about 8.0, is
primarily ionized. The ionized form does not favor passage through the lipid
membrane; accordingly, only about 10%-20% of molecules are un-ionized.
Relatively high plasma clearance (15-40 ml/kg/minute) has implicated extrahepatic
clearance mechanisms, most likely renal.
Fentanyl (Sublimaze) pharmacokinetics:
Fentanyl (Sublimaze) is significantly more lipid-soluble, compared morphine and,
relative to morphine, has a more rapid onset of action (fentanyl (Sublimaze) is also a
weak base and at physiological pH only about 10% of molecules are un-ionized).
Clearance of about 10-20 ml/kg/minute is consistent with a primary hepatic mechanism.
Fentanyl (Sublimaze)'s short duration of action following bolus administration is
explained by rapid redistribution from brain to other compartments such as skeletal
muscle and fat. If, however, fentanyl (Sublimaze) is administered by continuous IV
infusion or multiple IV dosing, other non-CNS compartments will saturated and
remaining CNS fentanyl will contribute to postoperative ventilatory depression.
33
Action of opioid drugs:
A. Central nervous system: Analgesia, sedation, euphoria, nausea, vomiting, miosis,
depression of ventilation, pruritus and skeletal muscle rigidity.
B. Respiratory system: bronchospasm in susceptible patients and depressed cough reflex
C. Cardiovascular system: bradycardia (fentanyl) or tachycardia ( pethidine)
D. Skin: pruritus may be due to histamine release or action on opioid receptor.
E. Gastrointestinal tract: constipation, delays gastric emptying, increased tone of the
common bile duct and sphincter of Oddi.
F. Urinary tract: increased sphincter tone and retention of urine.
Use of opioids in anesthesias
Premedication drugs
Induction of anaesthesia
Blunt haemodynamic reactions to noxious stimulation
Intraoperative analgesia
Postoperative analgesia
Used in ICU as analgesia to facilitate mechanical ventilation
Drug Doses
Morphine 2.5 - 5 mg (IV), 15 - 30 mg (oral)
Pethidine 50 to 100 mg S.C., I.M or in reduced doses I.V.
repeated every 3 to 4 hours
Fentanyl 25 - 50 µg (IV), 150 - 300 µg (oral)
Naloxone
It is an antagonist at all opioid receptors of pure opioid antagonist. It reverse all opioid
actions including analgesia. It has short duration of action ( 1-4 hours) and has limited action
against partial or mixed actions opioids. Abrupt reversal of opioid analgesia can result in
sympathetic stimulation (tachycardia, ventricular irritability, hypertension and pulmonary
oedema).
34
Dosage :
Bolus:
o Adult: 0.04 mg IV in titrated bolus every 23 minutes until the desired
effects
o Child: 1-4mcg/kg titrated
Continuous infusion: 5mcg/kg/hr IV will prevent respiratory depression without
altering the analgesia produced by neuraxial opioids.
Tramadol
It is an opioid agonist at mu receptor and inhibits noradrenaline reuptake and release of 5-
hydroxytryptamine (monoaminergic pathways). It is given intravenously with the dose of 1-2
mg/kg and also can be given orally (good bioavailability). It produces less respiratory
depression in equivalent dose if compared with morphine.
Non opioids
Use of non steroidal anti-inflammatory drugs as analgesics (eg: Ketorolac, Diclofenac). It
block synthesis of prostaglandins by inhibiting cyclooxygenase enzyme. It reduces pain by
peripheral action and centrally by reducing input of nociceptive information in spinal cord.
Ketorolac and Ketoprufen has opioid sparing effects.
Side effects:
Reduced platelet aggregation may increase bleeding – it is not advisable for neurosurgical
and ophthalmic surgery.
It may cause damage to gastric mucosa causing ulceration and bleeding.
Bronchospasm – patients with asthma have an increased incidence of sensitivity to
aspirin
Renal failure- inhibition of renal prostaglandin synthesis may interfere with maintenance of
renal blood flow.
Drug Doses
Voltaren (Diclofenac) 100-200 mg daily
Paracetamol 2 x 500mg 4-6 hourly
Synflex Initially 550 mg then 275 mg
6-8 hrly
35
CHAPTER 3
CASE: PERIOPERATIVE ASSESSMENT
3.1. Preoperative Assessment
3.1.1. Case History
IDENTIFICATION DATA
Name : Anita binti Yahaya
Sex : Female
Age : 39 years old
Nationality/Tribe : Malaysian/Malay
Religion : Islam
Address : Kangar, Perlis
Marital Status : Married
Occupation : Housewife
Admission Date :17th May 2012, 11.15 am
CHIEF COMPLAINT
This 39-year old Malay lady was admitted to surgical ward of Hospital Tuanku Fauziah
with a chief complaint of right anterior neck swelling associated with shortness of breath since
one week ago.
HISTORY OF PRESENTING ILLNESS
Patient is a known case of goitre for the past two years. The goitre, which is a right sided
anterior neck swelling, painless, and gradually increases in size. Sometimes, the patient
experienced hand tremor, palpitation and heat intolerance. Now, she was having obstructive
symptoms such as shortness of breath and occasionally orthopnoea since 1 week ago.
Ultrasound was done on 4th May 2011, with the impression of Multinodular Goitre. Fine
Needle Aspiration Cytology (FNAC) was also done on 2nd June 2011, with the impression of
nodular goitre with cystic degeneration.
36

Otherwise, she has no dysphagia, no diarrhea, no constipation, no abdominal pain, no
upper respiratory tract infection or urinary tract infection, and no stridor.
PAST MEDICAL HISTORY
She has no known of other medical condition.
PAST ANAESTHETIC HISTORY
Patient has never gone through any surgical or anaesthetic procedures.
DRUG HISTORY
Patient is not on any medication. There’s no history of drug or food allergy. Patient
claimed she’s not taking any traditional medication or over the counter drug.
PAST OBSTETRIC & GYNECOLOGY HISTORY
Patient has never had any problem regarding obstetric and gynecology. She had her
menarche at the age of 13 years old and claimed to have a regular menstrual cycle, around 7 to 8
days every month. However, she has mild dysmenorrhea.
FAMILY HISTORY
The patient’s father has thyroid cancer. Mother is healthy.
SOCIAL HISTORY
Patient is a housewife, married, and having 4 children. Currently, she’s living with her
husband and children. She’s a non-smoker and non-alcoholic. She denied of any high-risk
behavior.
3.1.2. Physical Examination
GENERAL EXAMINATION
Patient was conscious and alert, lying comfortably on the bed. She doesn’t look ill, not in
pain, and not in respiratory distress. Her nutritional status is obesity, and her hydrational status is
37
fair. There’s no gross deformity, no any involuntary or abnormal movement, and there’s a
brannula attached at her left wrist.
VITAL SIGNS
HEAD, NECK & EXTREMITIES EXAMINATION
On the general examination (extremities), the palm was moist, no pallor, no palmar
erythema and the temperature was normal. There’s no clubbing finger, and no bluish
discolouration of the nail. No leuconychia or koilonychia noted. There’s no fine tremor or
flapping tremor. There’s also no pedal edema at both lower extremities.
Examination of the head did not reveal pallor of the conjunctiva, no jaundice of the
sclera, no exophthalmus, no arcus senilis and no xanthelasma. There’s also no bluish
discoloration of the lips and the tongue. The dental hygiene was fair.
For neck examination, on inspection, there’s a right anterior neck swelling that moves
upon deglutition, but does not move with tongue protrusion. Otherwise, there’s no redness, no
skin changes, no discharge, no surgical scar and no prominent vein. On palpation, it’s a non-
tender swelling with normal temperature. The size is 3x2 cm. The swelling has a smooth surface,
firm in consistency, round in shape, mobile and has a well-defined margin. The lower border of
the swelling can be felt upon deglutition. There is a tracheal deviation towards the left side.
Otherwise, the swelling is not attached to underlying structures or overlying skin, no fluctuation
Vital signs Value Interpretation
Temperature 37°C Afebrile
Blood pressure 135/70 mmHg Normal
Pulse rate 72 bpm Normal
Respiratory rate 18x/minute Normal
Pain score 0/10 Not in pain
Height 162 cm -
Weight 84 kg -
Body Mass Index 32 kg/m2 Obesity
38
and there’s no pulsation can be appreciated. On percussion, there’s no retrosternal extension of
the swelling, and on auscultation, there’s no bruit can be heard.
RESPIRATORY SYSTEM EXAMINATION
From airway assessment, patient was classified as Mallampati class II, and the
thyromental distance was more than 6.5 cm or three fingers wide.
Patient has no history or symptoms of upper respiratory tract infection. On examination;
on inspection, the chest moved symmetrically with respiration, with thoraco-abdominal breathing
pattern. The chest shape was normal and there was no deformity or scar noted on both anterior
and posterior chest wall. There were also no signs of respiratory distress. On palpation, the chest
expansion and tactile vocal fremitus were symmetrical on both anterior and posterior chest. On
percussion, it was a symmetrical resonance sounds, and there’s no retrosternal extension of the
goiter. On auscultation, no wheezing or crepitation heard. Air entry was equal on both sides.
CARDIOVASCULAR SYSTEM EXAMINATION
The peripheral pulses were palpable, equal and regular. There was no surgical scar seen
on the chest. There was neither heave nor thrill can be palpated. Apex beat was palpable at left
midclavicular line between 4th and 5th intercostal space. Normal 1st and 2nd heart sounds were
heard and there were no additional sounds or murmurs heard in the mitral, tricuspid, aortic and
pulmonary area.
ABDOMINAL EXAMINATION
On inspection, the abdomen was not distended, moves with each respiration. The
umbilicus is centrally located. Otherwise, there is no surgical scar, no visible peristalsis or
pulsation, no skin discolouration and no cough impulse.
On palpation, the abdomen is soft and non-tender. No mass can be appreciated and no
hepatomegaly or splenomegaly. The kidney was non-ballotable.
The percussion gives tympanic sound, and there’s no shifting dullness. On auscultation,
the bowel sound was present and no renal bruit heard.
39

CENTRAL NERVOUS SYSTEM EXAMINATION
Patient was alert, and well oriented to person, time and place. Glasgow Coma Scale was
15/15. Facial expression was symmetry. All cranial nerves were intact.
MUSCULOSKELETAL SYSTEM EXAMINATION
Patient has a normal muscle bulk, strength, tone and power for both upper and lower
extremities. The shape of vertebral spine is normal. No deformities noted. Gait was normal.
PHYSICAL STATUS
ASA score is 1. Patient was healthy with no systemic disease, and the surgery was an
elective surgery.
3.1.3. Investigation
o Full blood count:
Components Value Normal Range Interpretation
White blood cell 8.8 (109/L) 4.0 – 11.0 Normal
Red blood cell 4.7 (106/L) 3.8 – 4.8 Normal
Haemoglobin 12.0 (g/dL) 12.0 – 15.0 Normal
Haematocrit 37.8 (%) 36.0 – 46.0 Normal
Mean cell volume 80.1 (fL) 83.0 – 101.0 Low
Mean cell
haemoglobin
25.4 (pg) 27.0 – 32.0 Low
MCHC 31.7 (g/dL) 31.5 – 34.5 Normal
Platelet 298 (103/uL) 150 – 450 Normal
Differential:
Neutrophils
Lymphocytes
Monocytes
Eosinophils
Basophils
4.75 (103/uL)
2.90 (103/uL)
0.35 (103/uL)
0.70 (103/uL)
0.00 (103/uL)
2.0 – 7.0
1.0 – 3.0
0.2 – 1.0
0.02 – 0.50
0.02 – 0.10
Normal
Normal
Normal
High
Low
40
o Renal profile
Components Value Normal Range Interpretation
Sodium 138 (mmol/L) 135 – 145 Normal
Potassium 3.7 (mmol/L) 3.3 – 5.3 Normal
Urea 3.7 (mmol/L) 1.7 – 8.3 Normal
Creatinine 61 (umol/L) <97 Normal
o Coagulation:
Components Value Normal Range Interpretation
Prothrombin time 11.7 (sec) 10.4 – 13.2 Normal
INR 0.99 0.9 – 1.1 Normal
APTT test 28.5 (sec) 20.1 – 34.9 Normal
APTT ratio 1.0
o Thyroid function test:
41
Components Value Normal Range Interpretation
TSH 1.720 (uIU/mL) 0.27 – 4.20 Normal
Free T4 15.96 (pmol/L) 12 - 22 Normal
o Urine FEME:
Components Value Interpretation
Urine glucose Normal Normal
Bilirubin Negative Normal
Ketone Negative Normal
Specific gravity 1.000 Normal
Blood Negative Normal
Urine pH 5.0 Normal
Protein Negative Normal
Urobilinogen 3.2 Normal
Nitrite Negative Normal
Leucocyte Negative Normal
Color Light yellow Normal
Turbidity Clear Normal
Urine PT Negative Normal
EKG:
o Sinus rhythm
o No ischemic changes
o Interpretation: Normal
Chest X-Ray:
o Tracheal deviated to the left side
o Lung: Normal
o No cardiomegaly
o Bones: Intact
42
o Soft tissues: Normal
Indirect Laryngoscope:
o Both vocal fold mobile equally
o No anterior compression
o Impression: Normal vocal cord
3.1.4. Summary
A 39 years old malay lady, a known case of multinodular goitre diagnosed in 2010,
presented with right anterior neck swelling associated with shortness of breath since 1 week
before her admission to the hospital. Occasionally she has tremor, palpitation and heat
intolerance. On physical examination, patient is clinically euthyroid and not in respiratory
distress. From the chest X-ray, there’s a tracheal deviation to the left side. Otherwise, there’s no
any significant finding in any other system.
3.1.5. Preoperative Diagnosis
o Bilateral multinodular goitre
3.1.6. Plan
o Right hemithyroidectomy KIV total thyroidectomy
o To keep nil by mouth by 12 midnight (8 hours prior to surgery)
o To inquire informed consent for the surgery and anaesthetic procedures
o Send blood for blood crossmatch
o To plan for general anaesthesia/intermittent positive pressure volume
3.2. Intraoperative Assessment
Anaesthesia : Balanced general anaesthesia with intermittent positive pressure ventilation
(IPPV).
Fasting : Patient was kept nil by mouth 8 hours prior to operation.
43
Premedication : Not given to patient
3.2.1. Anaesthesia Procedures :
I. Preoperative assessment was done and consent was taken from the patient.
II. GA machine was checked and anaesthetic drug was prepared before patient was
entered into the operation room.
III. Intravenous assessed was established by inserting IV catheter 18G and patient was
preloaded with normal saline.
IV. Procedures were done in a full aseptic technique, scrubbed, gloved and gowned.
V. Patient neck was fully extended and given sand bag to get the better view for the
surgery.
VI. Patient was preoxygenated with 100% oxygen for 3 minutes at 8am.
VII. Administration of intravenous Fentanyl 100mcg and intravenous sodium thiopentan
2.5% 175mg.
VIII. Loss of consciousness was assessed by loss of eyelash reflex.
IX. Test ventilate before give muscle relaxant.
X. Then, IV atracurium 30mg was given and mask ventilate with oxygen and volatile
for 3minutes.
XI. Laryngoscopy and intubation were then performed by using ‘armored’ ETT tube.
XII. ETT cuff of 7.5 cm and angle at 15cm was inflates and connected to breathing
circuit.
XIII. ETT positioned was confirmed by auscultation and end tidal volume CO2.
XIV. The vital sign which are oxygen saturation, brain tissue carbon dioxide, respiratory
rate, blood pressure, heart rate, any blood loss and urine output was monitored during
the operation.
XV. No blood transfusion was done during the operation.
XVI. Anaesthesia was maintained with Sevoflurane and top up atracurium infusion
3ml/hour and morphine 3mg /hour.
XVII. Reversal with intravenous Atropine 1mg and Neostigmine 2.5mg.
XVIII. ETT was removed and mouth was cleared under direct vision once patient
spontaneously breathing.
44
XIX. Oxygen was administered by face mask and patient was transferred to recovery room
to be reassessed.
3.2.2. Drugs :
3.2.2.1. Intravenous :
a. Fentanyl 100mcg
b. Sodium thiopentate 2.5% 175mg
c. Atracorium 30g
d. Morphine 3mg
e. Atrocorium infusion 3ml/hour
f. Atropine 1mg
g. Neostigmine 2.5mg
3.2.2.2. Gases : 8.20 am 8.50am 9.20am 9.50am
1. Oxygen / air (L/min) 1:1 1:1 1:1 1:1
2. Volatile : Sevoflurane (MAC %)1.7 1.7 1.7 1.7
3.2.3. Monitoring :
Time 8.20am 8.50am 9.20am 9.50am
Saturation O2 (100%) 100 % 100% 99% 100%
Respiratory rate (x/min) 18x/min 18/min 16x/min 18x/min
Pbt CO2 34 34 34 36
Blood Pressure and Heart Rate :
Blood pressure was monitored every 5 minutes during the whole operation
procedure. The systole reading range was between 140 – 180 mmHg and diastolic
pressure was between 60 – 180mmHg.
Heart rate was monitored every 5minutes and noted to be in normal range which
was within 90 – 100 beats per minutes.
45

Blood Pressure monitoring :
Heart rate monitoring
3.2.4. Summary :
Patient was hemodynamically stable with minimal blood loss during the operation
thus no blood transfusion was needed. Upon operation, the surgeon only did right
hemithyroidectomy and not done total thyroidectomy because the nodule at the left side is
small (1cm) near the recurrent laryngeal nerve and not removed. Both recurrent laryngeal
nerve identified and preserved and parathyrois gland identifiend and preserved. Skin closed
with subcuticular. Patient reversed with atropine and neostigmine and was transferred to
recovery ward before discharging to ward.
3.3. Post Operative Assessment
After extubation, patient was stable and began to breathe spontaneously with
supplemental oxygen via face mask (5L/min).
46
Patient was transferred to the recovery area after the surgery was done. Patient was still
drowsy lethargic but there was no sign of respiratory distressed seen.
Non-invasive blood pressure (NIBP) monitor, ECG monitoring and pulse oximeter were
set-up.
Patient was put below radiant warmer to prevent hypothermia.
Pain was minimal and there were no complaints of headache, nausea or vomiting.
Otherwise, no other post-operative complications noted.
Vital Signs Reading Interpretation
Blood pressure 119/80 mmHg Normal
Pulse rate 81 x/min Normal
Respiratory rate 20x/ min Normal
Temperature 37°C Afebrile
SpO2 100% Normal
Pain score 2/10 Mild pain
Post-operative anaesthesia recovery score
Parameters Signs Score
Activity Able to lift the head or has a good hand grip
None of the above
1
0
Respiration Able to breathe and cough easily
Dyspnoeic or apnoeic
1
0
Circulation BP within 20% of pre-operative level
BP above or below 20% of pre-operative
level
Pulse regular rate, within 20% of pre-
operative level
Pulse irregular, above or below 20% of pre-
operative level
1
0
1
0
Consciousness Arousable 1
47
Not responding 0
Colour Pink
Dusky
1
0
Total score 6/6
Note:
Score 5 or more may be coming home with the conditions of operation/ action possible
Score 4 to the treatment room when the breathing value is 1
Score 3 or less to ICU
Operative findings:
Multinodular goitre, right lobe is larger than the left lobe
Only 1 small nodule is noted, measuring about 1cm on the left side, situated near the
recurrent laryngeal nerve, not removed
Both recurrent laryngeal nerves are identified and preserved
Parathyroid glands are identified and preserved
Plan:
(i) To transfer patient to the surgical ward after 30 minutes and regularly monitor the vital
signs in the ward
(ii) Continue to give supplemental oxygen (5L/min) via face mask
(iii) Infuse 3 pints of dextrose 5% and 2 pints normal saline 0.9% in 24 hours
(iv) Keep nil by mouth for 6-8 hours
(v) To give C. Tramal 50mg PRN
(vi) To give tab. Paracetamol 1g QID
3.3.1. Follow-up
18th of May 2012 (12.00 pm)
Subjective Patient complain of pain over the incision site and throat
discomfort, pain score 3/6
Patient was able to speak, can tolerate small volume of liquid
(2-3 spoonful) orally
Otherwise, there is no numbness, hoarseness of voice, shortness
48
of breath, tremor or palpitation
Objective Patient is alert, conscious but mildly lethargic
Skin is pink, hydration is adequate
BP: 118/80 mmHg
Pulse rate: 80x/min
Respiratory rate: 20x/min
Temperature: 37°C
Surgical scar: clean, no discharge is seen, not infected
Lungs: Vesicular breath sound, no additional sound
CVS: Dual rhythm no murmur
Abdomen: soft non tender
Analysis Post- right hemithyroidectomy for multinodular goitre
Plan Continue vital signs monitoring every 4 hours
Keep nil by mouth for about 6-8 hours, then encourage fluid
intake orally (set an intake/ output chart)
Give C. Tramal 50mg PRN and T. Paracetamol QID for pain
To complete IV drip: 2 pints of normal saline and 3 pints of
Dextrose 5% in 24 hours
19th of May 2012 (2.00 pm)
Subjective Patient complain of pain over the incision site and throat
discomfort, pain score 2/6
Patient was able to speak with slight hoarseness, can tolerate
small volume of liquid orally
Otherwise, there is no numbness, shortness of breath, tremor
or palpitation
Objective Patient is alert, conscious and comfortable
Skin is pink, hydration is adequate
BP: 116/80 mmHg
Pulse rate: 76x/min
Respiratory rate: 17x/min
Temperature: 37°C
Surgical scar: clean and healing, no discharge is seen, not
infected
Lungs: Vesicular breath sound, no additional sound
CVS: Dual rhythm no murmur
Abdomen: soft non tender
Analysis Post- right hemithyroidectomy for multinodular goitre
Plan Continue vital signs monitoring every 4 hours
Encourage fluid intake orally (set an intake/ output chart)
Give C. Tramal 50mg PRN and T. Paracetamol QID for pain
Off IV drip when completed and adequate oral intake
To discharge patient when no complication and condition is
stable. Plan for follow-up in SOPD
49

CHAPTER 4
PERIOPERATIVE DISCUSSION (CASE)
4.1. Pre-operative Discussion
There are few criteria that need to be considered in the pre-operation before a patient
undergone surgery, which are:
o To access the condition of the patient from the history and physical examination. From
physical examination, it is important to make a thorough assessment of airway,
cardiovascular system, and respiratory system. Since this patient has no problem in her
cardiovascular and respiratory system, the assessment would be focused more on her
airway, to determine if there would be any difficulty when the intubation is performed.
o To decide the anaesthetic plan for the patient either by general or regional anaesthesia.
o The need of informed consent for both surgery and anaesthetic procedures.
50
o Patient is not given any premedication such as:
- Antibiotic: Thyroidectomy is considered as a clean surgery, prophylactic
antibiotic is not needed.
- Anxiolytic: Patient’s anxiety is not severe enough to be treated using medication.
- Antiemetic: Risk of aspiration is reduced by keeping patient NBM before surgery.
- Analgesic: Not given to our patient because she is not in pain prior to the surgery
o To keep the patient nil by mouth 8 hours prior to surgery
1. For this patient, she does not have any past medical history such as asthma, or any
evidence of recent upper respiratory tract infection, which suggesting the use of general
anaesthesia is not contradicting. However, this is her first surgical experience, thus
there’s no any record of allergy to anaesthetic agents. From assessment of Mallampati
class, this patient is in class II, and the thyromental distance is 3 finger breadth, which
suggesting the difficulty of airway for intubation is not present.
2. In this patient whom undergone right hemithyroidectomy surgery, which involves the
upper airway region; general anaesthesia is the best option. It is unethical to use regional
anaesthesia and keeps the patient awake for this type of surgery.
3. Based on American Society of Anaesthesiology grade, the patient classified into class I
(with the mortality rate of 0.06%-0.08%), because she is perfectly healthy and thus, the
operation risk is minimal. However, there are also other predictors which play roles in
determining the risk and mortality of an operation, such as operation type and surgical
skill of the operator.
4. The patient gave her consent to go through hemithyroidectomy surgery. The consent
given after the anaesthesia and surgical teams explained about the nature of surgical and
anaesthetic procedures. Their consent is taken and is documented in the anaesthesia and
surgery consent forms. All questions asked by the patient, answered by anaesthesiologist.
51

5. The patient was keep nil by mouth by 12 midnight, 8 hours before she undergone the
surgery, to allow sufficient time for gastric emptying of ingested food and liquid at the
time of induction of anaesthesia. It is believed that fasting can limit the severity of
aspiration pneumonitis syndrome in the event of aspiration of gastric content. The gastric
emptying of fluid is very rapid; 95% of ingested liquids are emptied in 1 hour, while
solids are emptied only when it is transformed into a liquefied form, which requires
unpredictable time (up to 12 hours).
4.2. Intraoperative Discussion
1. Patient was given balanced general anaesthesia with intermittent positive airway pressure
ventilation not by spontaneous ventilation. Balanced anaesthesia mean that 3 component
of anaesthesia was given which mean hypnotic, analgesia, and muscle relaxant. It is safer
to use 3 types of drug in safety doses than 1 type that require higher dose to get other
effect but can harm the patient. IPPV was chosen because the surgery involves the
airway, at the neck region, and requires endotracheal intubation. Spontaneous ventilation
was not chosen for this patient because it usually for superficial surgeries and surgery that
doesn’t involve the airway.
2. Patient was given special type of endotracheal tube which is ‘armored’ endotracheal tube
that are cuffed, wire- reinforced silicone rubber tubes that are much more flexible than
polyvinyl chloride tube, but they are difficult to compress or kink. This type of
endotracheal tube is useful when the trachea is anticipated to remain intubated for a
prolonged duration and the neck to remain flexed during surgery. ETT is indicated for
surgery that used IPPV and muscle relaxant, to secure the airway, and for unusual
surgical position.
3. Patient was given 2 types of opioid for the surgery which are IV Fentanyl and IV
morphine. Fentanyl was given 1-2mcg/kg, so for this patient is 80 – 160mcg. Patient was
given 100mcg which is 1 ampoule. Fentanyl was used as an induction agent because the
onset of action of fentanyl is almost immediately when given intravenously than
52
morphine. Fentanyl is more potent than morphine due to its high lipophilicity, which
make it penetrates the CNS more easily. It binds to mu opioid G protein couple receptor
which inhibits pain neurotransmitter released by decreasing intracellular Ca2+ levels.
Morphine is used as maintenance for analgesia during the intraoperation period because it
is long acting. Morphine is used than ketorolac because it is a gold standard drug and
patient does not have contraindication to it. Ketorolac may not improve analgesia due to
its ceiling effect but may increase the unfavorable effect. Furthermore, ketorolac
increased the risk of surgical bleeding and increased GI bleeding.
4. Patient was given with sodium thiopental (STP) which is an intravenous barbiturate (3-
5mg/kg), but for this patient was given 175mg. STP was given to sedate the patient so it
is given slowly with other volatile gas which can give synergistic effect and is stopped
when the patient has been sedated. That is why patient it is only given 175mg. STP is
cost effective compared to propofol. Unlike propofol, STP induces histamine release
which will be dangerous in asthmatic patient. STP is considered to be safe for our patient
since she doesn’t have asthma. STP causes less pain when it’s injected compared to
propofol. STP is an ultra-short acting barbiturate due to its rapid distribution which is
used as an induction that acts directly to GABA receptor and causes sedative effect. After
STP was given, ventilation test needs to be done to make sure that we can ventilate the
patient by monitoring the capnograph.
5. Atracurium is a muscle relaxant given to the patient after test ventilate was done. For this
patient was given 30 mg. It is non depolarizing muscle relaxant that acts on nicotinic
receptor in competitive fashion to produce neuromuscular blockade so that depolarization
not occur. It is used to facilitate endotracheal intubation, and controlled ventilation. It is
spontaneously degraded by Hofmann elimination. As maintenance, atracurium sustains
muscle relaxation during surgical. Usually atracurium not given as infusion for thyroid
surgery but for this patient, atracurium infusion was given because the anaesthesiologist
predicted that the surgery will be long, but the operation is not complicated and tends to
be short surgery, so it is stopped within ½ hour before the surgery was done. After the
53
atracurium was given, mask ventilation has to be done for 3 minutes to allow the onset of
action of atracurium.
6. Sevoflurane is a volatile anaesthetic agent that is used for this patient. It is used because it
is less soluble in blood which will cause patient to gain her consciousness faster from
anaesthesia. Furthermore, it is preferred agent for mask delivery due to its less irritation
to mucous membrane. It causes immobility that is measured by minimum alveolar
concentration (MAC) of anaesthesia required to suppress movement to a surgical incision
in 50% of patient. It has mild negative inotropic effect which can lower the blood
pressure in this patient during surgery.
7. Patient was given IV atropine 1mg and IV neostigmine 2.5mg for reversal after
operation. Neostigmine is an anticholinesterase that inhibits acethylcholinesterase so that
the enzyme can no longer break down the acethycholine molecules before they reach the
postsynaptic membrane receptor. Atropine is given to counteract the parasympathetic
effects of anticholinesterase.
8. Monitoring of intraoperative is to see any rapid changes in patient status during
anaesthesia. The patient’s oxygenation, ventilation, circulation and temperature are
continuously monitored. Clinical signs like colour, pulse rate and volume, rate and depth
of respiration, blood pressure, fluid status, temperature, urine output, blood transfusion
are also monitored. All the important vital sign are documented. For this patient all the
vital sign are in the normal state except that her blood pressure which is higher than
normal. Sevoflurane can reduce the blood pressure during the operation. Furthermore, it
is normal for blood pressure to elevate during intubation and extubation because of body
response and it will reduce later.
9. Fluid replacement is divided into 3 components, which are: for maintenance, deficit, and
the fluid loss (insensible & bleeding). Intraoperative fluid administration has to be given
to maintain adequate oxygen delivery, normal electrolyte concentration, and to normal
blood glucose level.
54
For the maintenance:
1st 10kg of BW : 100ml/kg/24h 4ml/kg/h Patient :80kg (10kg x4 = 40ml)
2nd 10kg of BW : 50ml/kg/24h 2ml/kg 10kg (10 kg x2= 20ml)
Each kg above 20kg : 20ml/kg/24h 1ml/kg/h 60kg (60kg x1= 60ml)
Maintenance – 40 ml + 20ml + 60ml = 120ml/hour
Preexisting deficit: maintenance x numbers of hour of fasting. Replace half in the 1 st
hour, quarter in 2nd and 3rd hours – 8hour x 120ml = 960ml (replace 480 in 1st hour,
240 in 2nd and 3rd hours )
Ongoing loss : from the blood loss and the evaporative loss from the surgical field
( minor = 1- 2ml/kg/h, moderate = 3- 4ml/kg/h, major = 6- 8 ml/kg/h)
Patient = minor – 1 x 80 = 80ml/h
1st hour = 120 ml + 480 ml + 80ml = 680 ml/h
2nd and 3rd hour = 120ml + 240ml + 80 ml = 440ml/h
4th hour onward = 120ml +80 = 200ml/h
The choice of fluid given is crystalloid because it is rapidly distributed into the
extracellular fluid component. It is useful to provide maintenance water and electrolytes
and for intravascular volume expansion . For this patient, normal saline was chosen
(0.9% NaCl) .
4.3. Post-operation discussion
1. Patient should not leave the operation room unless they have a stable and patent airway
(indicated by the presence of cough and gag reflex along with spontaneous breathing),
adequate ventilation and oxygenation, and are hemodynamically stable.
2. Continuing care in the recovery room:
3. Phase 1: Gained consciousness with intact pharyngeal reflexes. Able to sustain a 5
seconds head lift, cough and deep breath.
4. Phase 2: Recovers the ability to think clearly and movement returns. Can be transferred
to the ward.
5. Phase 3: At the end of this phase all the effects of anaesthetics should disappear.
6. The most frequent problems in the recovery room are:
55
7. Nausea and vomiting (might be the effect of opioids analgesics, which will cause
increased intracranial pressure, resulting in headache, altered consciousness. Fluid and
electrolyte loss can also happen).
8. Inadequate pain relief (pain will activate the sympathetic activity vasoconstriction
less perfusion to the tissue delayed wound healing)
9. shivering due to hypothermia (patient should be placed near a warmer and covered with
blanket)
10. Hypoxemia (to prevent this, pre-oxygenation via face mask should be continued
immediately after extubation)
11. Bleeding from the surgical site or wound infection (bleeding and swelling can
compromise the airway. If this occurs, remove skin clips/sutures and strap muscle sutures
and call for help.
12. Hoarseness of voice might post thyroidectomy might be due to iatrogenic injury to the
recurrent laryngeal nerve, or simply due to swelling around the nerves (this will resolve
with time). Patient should be warned that their voice will be different for a few days post-
op because of intubation and local edema.
13. Most patients who have mild to moderate pain following surgery can be managed with
oral COX inhibitors, opiods, or a combination. Our patient was given Paracetamol (1g
QID) tablet and Tramadol hydrochloride capsule (50mg PRN) as soon as patient was able
to tolerate orally.
Paracetamol (acetaminophen) has the fewest side effects but is a hepatotoxin at very
high doses. Isoniazid, zidovudine, and barbiturates can potentiate acetaminophen
toxicity.
Tramadol is a synthetic oral opioid that also blocks neuronal reuptake of
norepinephrine and serotonin. It appears to have the same efficacy as the combination
of codeine and acetaminophen but is associated with significantly less respiratory
depression and has little effect on gastric emptying.
56
REFERENCES
Basri, M., Ariff, Lukman, M., Hadi, A., Azrina, 2009. General Anaesthesia. Anaesthesiology for
Medical Undergraduates; 37-50.
Desai, A.M., Macario, A., Green, R., Talavera, F., Krugman, M., Raghavendra, M., 2011.
General Anaesthesia. Available from: http://emedicine.medscape.com/article/1271543-
overview [ Assessed 19 May 2012]
Frilling, A., Liu, C., Weber, F., 2004. Benign Multinodular Goiter. Scandinavian Journal of
Surgery, Vol.93: 278-281
Neto, G.M., 2010. Multinodular Goiter, Thyroid Disease Manager. Available from:
57
http://www.thyroidmanager.org/chapter/multinodular-goiter/ [Assessed 18 May
2012].
The American Association of Endocrine Surgeons, 2007. Benign Thyroid Enlargement (non-
toxic multinodular goiter). Available from:
http://endocrinediseases.org/thyroid/goiter_symptoms.shtml [ Assessed 18 May 2012]
58