Embed Size (px)
Citation preview

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 1/43
Gastrostomy and Jejunostomy

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 2/43
Gastrostomy
• Is a surgical procedurein which an openingis created into thestomach for thepurpose of
administering foodsand liquids via afeeding tube or forgastricdecompression in the
setting of intestinalobstruction.
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 3/43
• A gastrostomy is preferred over NGfeedings in the patient who iscomatose, because of
gastroesophaeal sphincter remainsintact, making regurgitation andaspiration less likely than with NG
feedings.
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 4/43
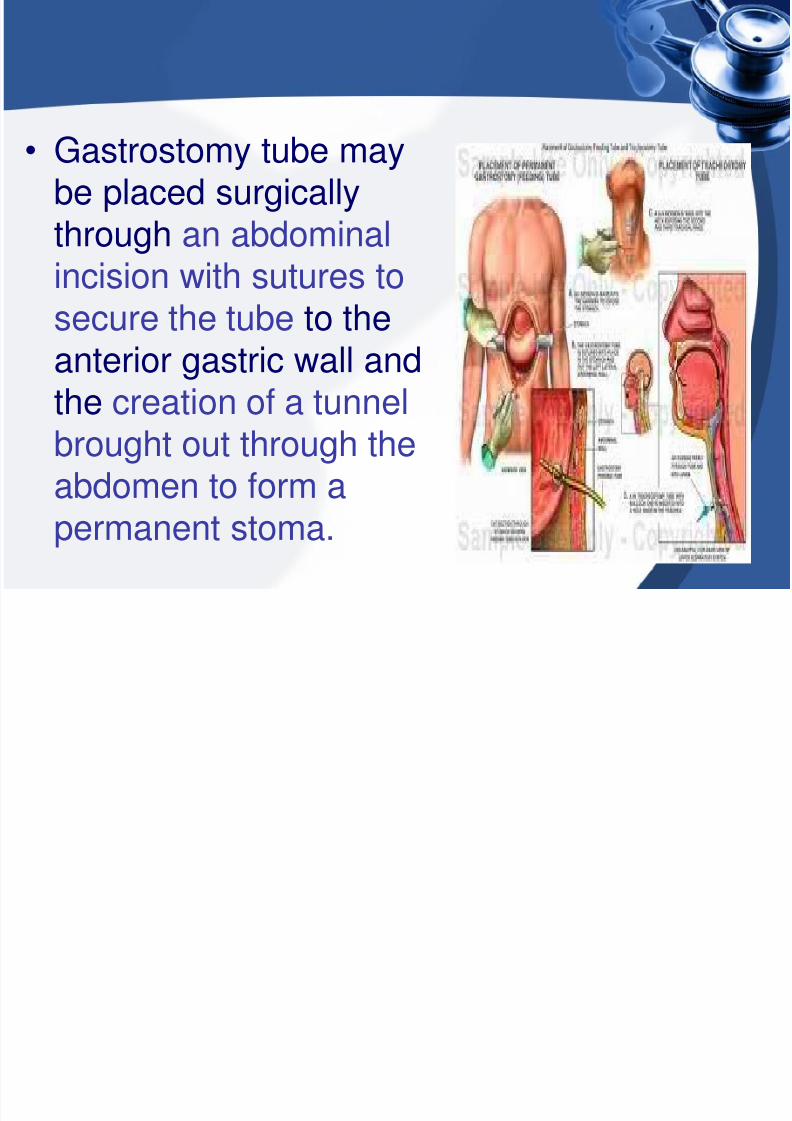
• Gastrostomy tube maybe placed surgicallythrough an abdominal
incision with sutures tosecure the tube to theanterior gastric wall and
the creation of a tunnelbrought out through theabdomen to form apermanent stoma.
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 5/43
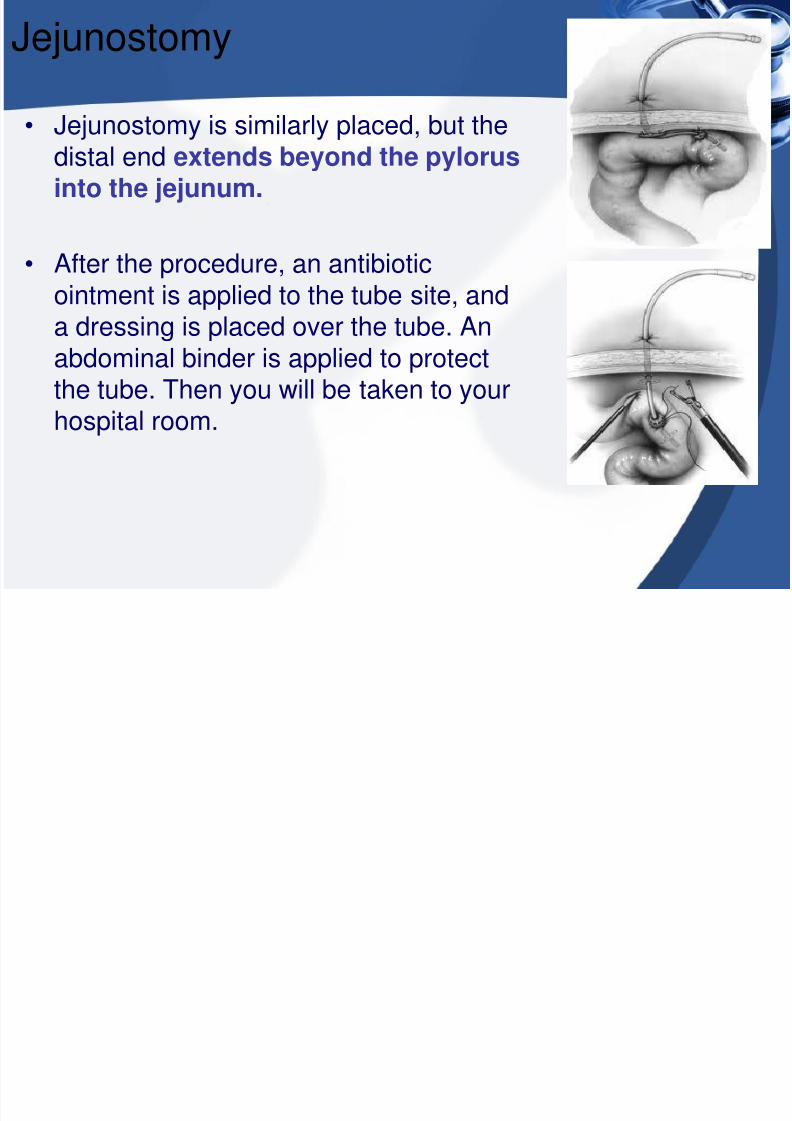
Jejunostomy
• Jejunostomy is similarly placed, but thedistal end extends beyond the pylorusinto the jejunum.
• After the procedure, an antibioticointment is applied to the tube site, anda dressing is placed over the tube. Anabdominal binder is applied to protectthe tube. Then you will be taken to your
hospital room.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 6/43
• Using the J-tube for feeding Feedings through a J-tube are always done using afeeding pump. A visiting nurse or home care
company will help arrange for your feeding pumpand instructions on how to use the pump at home.They will also be available to assist you in caring foryour tube at home.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 7/43
Insertion of a Percutaneous EndoscopicGastrostomy (PEG)
• Requires the service of a provider skilled endoscopyor interventional radiology.
• After local anesthetic is administered, a cannula is
inserted into the stomach through a small abdominalincision and an endoscope is inserted via thepatient's mouth and upper GIT.
• The PEG tube is guided down the esophagus, intothe stomach, and through the abdominal incision
• A mushroom catheter tip or internal fasteners secure
the tube against the stomach wall

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 8/43
• If an endoscope cannot be passed throughesophagus , then the gastrostomy can be attemptedunder x-ray guidance through the abdominal wall.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 9/43
Removal of PEG
• The initial PEG device can be removed and replace once thetract is well established, typcally 3-6 weeks after insertion.
• Replacement of the PEG device is indicated for a clogged offractured tube.
• The PEG should be fitted securely to the stoma to prevent
leakage of gastric secretions and is maintained in place throughgentle traction between the internal and anchoring device.
• PEG tube no longer required (recovery of swallow
after stroke or surgery for laryngeal cancer)
• Persistent infection of PEG site
• Failure, breakage or deterioration of PEG tube (a new tube canbe sited along the existing track)
• "Buried bumper syndrome"

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 10/43
Alternative to PEG device
• An alternative to the PEG device is alow profile gastrostomy device(LPGD)
May be inserted 3-6 months afterintial gastrostomy tube placement.
• these device are inserted flush with
the skin; they eliminate the possibilityof tube migration and have antirefluxvalves to prevent gastric leakage.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 11/43
• Pt. requiring lifelong enternalsupport are able to conceal thefeeding access site under their
clothing.• However, it is not possible to assess
residual volumes w/ LPGDs(ie, they
have one way valve), they also requirea special adaptor to connect the deviceto the feeding container.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 12/43
The patient with a Gastrostomy orJejunostomy
• AssessmentDetermined the pt. ability both to understand and
cooperate with the procedure.
The nurse assesses the ability of both pt. and family toa change in a body image and to participate in selfcare.
the purpose of the procedure and expectedpostoperative course should be explain.
The feeding tube will bypass the mouth and esophagusso that liquid feeding can be administered directlyinto the stomach or intestines.
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 13/43
• If the tube is expected to be permanent, the patientshould be made aware of this.
• The procedure is being performed to relieve discomfort ,prolonged vomiting , debilitation of an ability to eat, thepatient may find it more acceptable.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 14/43
• In the postopreative period, the pt. fluid andnutritional needs to assessed to ensureproper intake and GI Function.
• Inspect the tube for proper maintenance and
incision for signs of infection.• Evaluate pt. responses to the change of body
image and their understanding of the feeding
method, interventions are identified to help themcope with the tube and learn self –caremeasures.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 15/43
Diagnosis
• Major diagnosis in the postoperative periodmay include the ff.
• Acute pain• Risk for infection related to presence of
wound and tube.
• Risk for impaired skin integrity at tubeinsertion site
• Disturbed body image related to thepresence of tube.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 16/43
Collaborative Problems/PotentialComplication
• Would infection, cellutitis, and leakage
• GI Bleeding
• Premature dislodgement of the tube.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 17/43
Planning and goals
• Minimizing pain
• Preventing infection
• Maintaining skin integrity
• Enhancing coping
• Adjusting to change in body image
• Preventing complication.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 18/43
Nursing Intervention
• Meeting nutritional needs
• Providing tube care and preventinginfection
• Providing skin integrity
• Enhancing body image
• Monitoring and managing potentialcomplication
• Promoting home and community-basedcare

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 19/43
Evaluation
1.Maintains adequate fluid balancea. Maintains or gains wg.
b. Has normal electrolyte values
c. Is adequately hydrated
2.Is free from infection and skin breakdown
a. Is afebrile
b. Has no drainage from the incisionc. Demonstrates intact skin surrounding the exit site.
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 20/43
3. Adjust to change in body imagea. Is able to discuss expected change
b. Verbalizes concerns
4. Demonstrate skill in tube care
a. Handles equipment competentlyb. Demonstrate how to maintain tube patency
c. Keeps an accurate record of I and O
5. Avoids complication
a. Inhibits adequate wound healingb. Has no abnormal bleeding from puncture site
c. Tube remains intact for the duration of therapy

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 21/43
Parenteral Nutrition
• PN is a method of providingnutrients to the body by an IV route.
• The nutrients are complex admixture
containing proteins, carbs, fats,electrolytes, vitamins, trace mineralsand sterile water in a single container.
• The goal of PN are to improvenutritional status, establish apositive nitrogen balance, maintainmuscle mass, promote wt. maintenanceor gain, and enhance the healingprocess.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 22/43
Establishing (+) nitrogen balance
• PN solution can provide enough calories andnitrogen to meet the patient daily nutritionalneeds.
• When highly concentrated Dextrose isadministered, caloric requirements are satisfiedand the body uses amino acid for proteinsynthesis rather than for energy.
• Electrolytes such as Ca,P, Mg, NaCl areadded to the solution to maintain properelectrolyte balance and to transport glucose
and amino acid across cell membranes.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 23/43
Clinical Indication
• The indication for PN include an inabilityto ingest adequate oral food or fluidsw/in 7days. Enteral nutrition should be
considered before parenteral supportbecause it assist in maintaining gutmucosal integrity and is typically
associated with fewer complication.
F l

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 24/43
Formulas
• A total of 1-3 L of solution isadministered over a 24-hrs period.Intravenous fat emulsion (IVFEs) may
be infused site and should not befiltered. Usually 500 Ml of a 10% IVFEis administered over 6-12 hrs, 1-3 timesa week. IVFEs can provide up to 30% of
the total daily calorie intake.
INDICATION FOR PARENTERAN NUTRITION

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 25/43
INDICATION FOR PARENTERAN NUTRITION
CONDITION OR NEED EXAMPLESInsufficient oral or enteral intake severe burns, malnutrition,short
bowel syndrome, AIDS,sepsis, cancer
Impaired ability to ingest or absorb paralytic ileus, Crohndisease,food orally or enterally short gut, postradiation
enteritishigh-output
enteroculataneousfistula
The pt. Is unwilling or unable to ingest major psychiatric illness
Adequate nutrients orally or enterally
Preoperative and postopetative nutritional extensive bowel surgery,nutritional needs are prolonged acute pancreatitis.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 26/43
Initiating therapy
• PN solution are initiated slowly andadvanced gradually each day to thedesired rate as the patient’s fluid and
dextrose tolerance permits.
• A 24 hrs urine nitrogen determinationmay be prformed for analysis of
nitrogen balance
Ad i i t ti th d

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 27/43
Administration methods
1. Peripheral Method(PPN)
is administered through a peripheral vein; this ispossible because the solution is less hypertonic thanfull-calorie parenteral nutrition solution
lipids are administered simultaneously to buffer thePPN and to protect the peripheral veins fromirritation.
the usual length of therapy using PPN is 5-7 days

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 28/43

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 29/43
• Central method (CPN)• CPN have 5-6 times the solute concentration of
blood (and exert an osmotic pressure of about 2000mOsm/L), they are administered in to the vascular
sysytem through a catheter inserted into a high-flow,large, large blood vessel (eg, the subclavian vein).Concentrated solution are then very rapidly diluted toisotonic levels by the blood in this vessel.
Four types of central venous

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 30/43
Four types of central venousaccess devices (CVADs)
1. Nontunneled Central Catheters
-used for short term (less than 6 weeks)
-subclavian vein is the most common vessel
used-the jugular vein should only be used as a last
resort and then only for 1-2 days
-single lumen, double lumen, triple lumen central
catheters are available for central lines-distal lumen can be used for administration
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 31/43
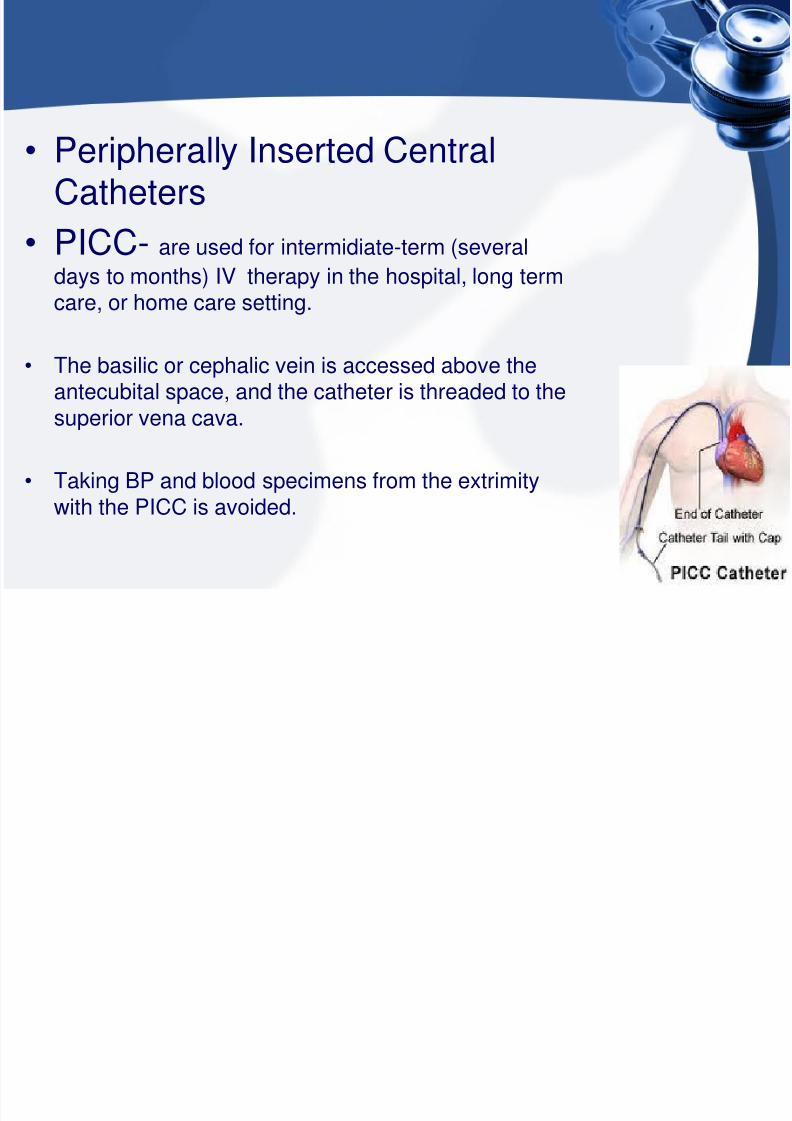
• Peripherally Inserted CentralCatheters
• PICC- are used for intermidiate-term (several
days to months) IV therapy in the hospital, long termcare, or home care setting.
• The basilic or cephalic vein is accessed above theantecubital space, and the catheter is threaded to the
superior vena cava.
• Taking BP and blood specimens from the extrimitywith the PICC is avoided.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 32/43
• Tunneled Central Catheters• Are for long term use and may remain in place for many
years.
• These catheters are cuffed and can have single or double
lumens; examples are the Hickmans, Groshong, andPermacath.
• There catheter are inserted surgically.
• They are threaded under the skin ( reducing the risk forascending infection) to the subclavian vein and advanced
into the superior vena cava.
implanted ports
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 33/43
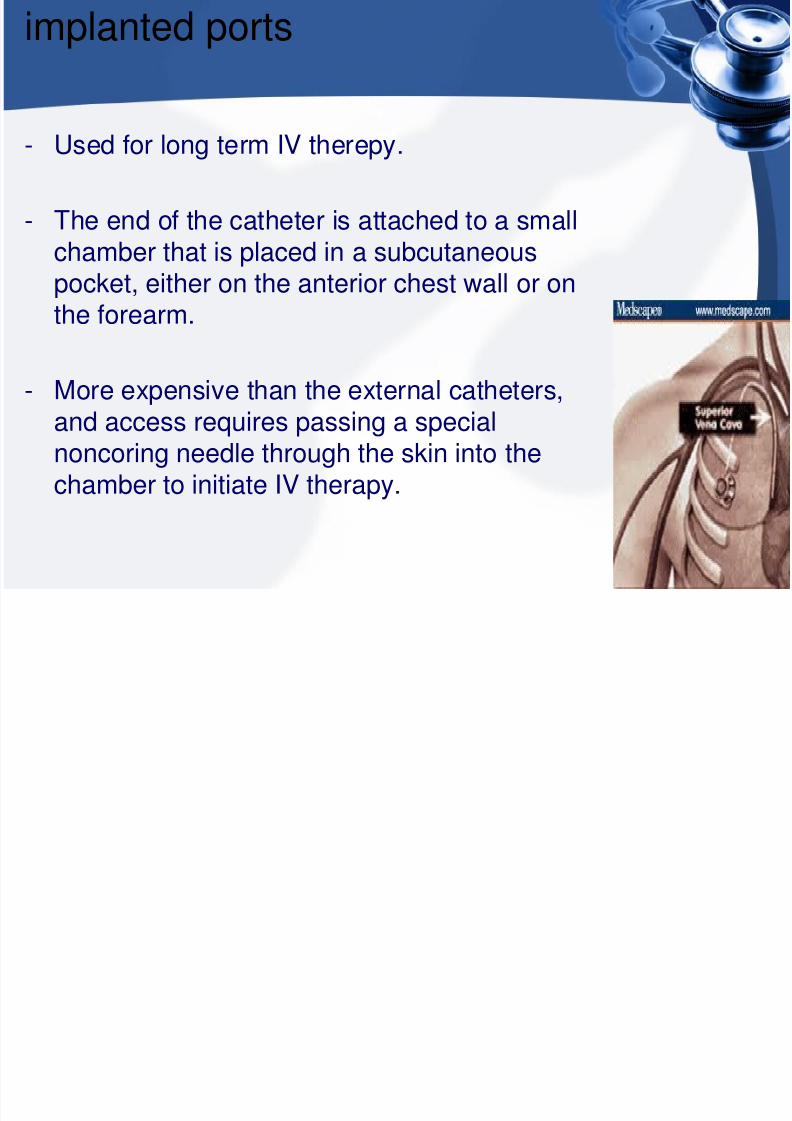
implanted ports
- Used for long term IV therepy.
- The end of the catheter is attached to a smallchamber that is placed in a subcutaneous
pocket, either on the anterior chest wall or onthe forearm.
- More expensive than the external catheters,
and access requires passing a specialnoncoring needle through the skin into thechamber to initiate IV therapy.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 34/43
Discontinuing Parenteral Nutrition
• PN solution is discontinued gradully to allow the patent to adjustto decrease level of glucose.
• If PN solution is abrupt terminated, isotonic dextrose can beadministered for 1-2 hrs to prevent rebound hypoglycemia.
• Once all IV therapy is completed, the nontunneled centralvenous catheter of PICC is removed and an occlusive dressingis applied to the exit site
• Tunneled catheters and implanted ports are removed only bythe physician.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 35/43
Nursing Process:Patient Recieving PN
• ASSESSMENT• Nurse assist in identifying pt. unable to tolerate oral and enteral
feeding who may be candidates for PN
• Indicators include significant wg. loss (10% or morethan ofusual wg.),
• The nurse carefully monitors the pt. hydration status, electrolytelevels, and calorie intake.
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 36/43
DIAGNOSIS
• The major nursing diagnosis may include the ff.• Imbalanced nutrition, less than body requirements, related to
inadequate oral intake of nutrients
• Risk for infection related to contamination of the centralcatheter site of or infusion line
• Risk for imbalanced fluid volume related to altered infusion rate
• Anxiety related to catheter care and securement
Collaborative Problems/Potential
8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 37/43
Collaborative Problems/PotentialComplication
Most common complication are:1.Pneumothorax
2.Embolism
3.Clotted cathter line
4.Catheter displacement and contamonation
5.Sepsis
6.Hyperglycemia
7.Fluid overload8.Rebound hypoglycemia.

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 38/43
Planning
• Major goals for the pt.• Optimal level of nutrition
• Absence of infection
• Adequate fluid volume• Optimal level of activity
• Knowledge of and skill in self-care
• Absence of complication
Nursing intervention

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 39/43
Nursing intervention
• Maintaining Optimal Nutrition
• Continuous, uniform infusion of PN solution over 24 hrs periodis desired
• The time periods for infusion are sufficient to meet the ptnutritional and pharmacologic needs
• Pt is initially weighted daily at the same of the day under thesame condition for accurate comparison
• Important to keep accurate I and O records and calcutaion offluid balance
• Calorie count is kept of any oral nutrients
• Trace elements are included in PN solution and areindividualized for each pt

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 40/43
Preventing Infection
• High dextrose and fat content of PN solution makes them anideal culture medium for bacterial and fungal growth andCVADs provide port of entry
• Meticulous aseptic technique is essential to prevent infection
any time the IV line setup is manipulated
• The primary source of microorganism for catheter related tobloodstream infections are the skin and the catheter
• The catheter site is covered w/ an occlusive gauze dressingthat is usually changed using sterile technique every 24-72 hrs

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 41/43
Maintaining Fluid
• To maintain an accurate rate of PN administration, an infusionpump is necessary
• Designed rate is set in mL/hr, and the rate is checked every 3-4hrs.
• If the rate is too rapid, hyperosmolar duiresis can occur
• If the flow rate is too slow , the pt does not receive the maximalbenefit of calorie and nitrogen.
• I and O are recorded q8

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 42/43
• Encourage Activity• With a catheter in the subclavian vein, the pt is free to move the
extremities, and normal activity should be encourage tomaintain a good muscle tone
Evaluation

8/3/2019 Gastrostomy and Jejunostomy
http://slidepdf.com/reader/full/gastrostomy-and-jejunostomy 43/43
Evaluation
• Expected Pt Outcomes• Attains or maintains nutritional balance
• Is free of catheter-related infection
a. is afebrile
b. Has no purulent drainage from the catheter insertion site• Is hydrated, as evidenced by good skin turgor
• achieve an optimal level of activity, within limitations
• demonstrates skill in managing PN regimen
• prevent complication a. Maintains proper catheter and equipment function
b. Maintains metabolic balance within normal limits





























