Embed Size (px)
Citation preview

Scientific American Surgery DOI 10.2310/7800.2182
05/15
© 2015 Decker Intellectual Properties Inc
gastrointestinal tract and abdomen
N e u r o e N d o c r i N e T u m o r s o f T h e P a N c r e a s
Katherine A. Morgan, MD, FACS
Pancreatic neuroendocrine tumors (PNeTs) are neoplasms of the endocrine pancreas, accounting for 1 to 2% of pancre-atic tumors and with a reported clinical incidence of one to five cases per million persons annually in the united states.1 interestingly, autopsy studies report PNeTs in 0.8 to 10% of cases,2,3 implying a significant incidence of subclinical disease. PNeTs appear to be increasing in incidence4 or at least in clinical detection. The understanding of the patho-physiology of these unpredictable tumors has evolved significantly over the past decade due to broadened clinical experience and developing cellular science.
PNeTs comprise a heterogeneous group of tumors with variable presentation and biologic behavior, including func-tional and nonfunctional tumors, as well as tumors associ-ated with known hereditary syndromes. The presentation of PNeTs is broad in spectrum, including small, asymptomatic, incidentally discovered, nonfunctional neoplasms, functiona l tumors (both localizable and unlocalizable) with associated clinical syndromes, and diffuse metastatic disease. Given this diversity, PNeTs are best considered broadly and then by category.
Clinical Presentation
PNeTs are categorized as functional or nonfunctional based on the presence or absence of clinical symptoms due to excess hormone production by the tumor. PNeTs present in a variety of ways largely related to the functional status and stage at presentation. functional PNeTs present with a distinct clinical syndrome associated with the oversecretion of enterohormonal peptides by the tumor, such as insulin or gastrin. Tumors are named after the overproduced hormone causing the symptoms and can be detected by elevated serum levels of the incriminated peptide [see Table 1].
conversely, nonfunctional PNeTs do not present with an associated clinical syndrome. Nonfunctional PNeTs may instead present with symptoms due to mass effect, including abdominal pain, early satiety, and weight loss. unlike pancreatic adenocarcinoma, jaundice is less common but can be present. historically, nonfunctional PNeTs were often locoregionally advanced or metastatic at diagnosis due to their nonspecific symptoms. increasingly, however, small, asymptomatic, incidentally discovered, nonfunctional PNeTs are being detected due to a broad increase in cross-sectional abdominal imaging for a variety of reasons.
most PNeTs are sporadic, but they can occur in the setting of several hereditary syndromes, including multiple endo-crine neoplasia type i (meN i), von hippel-Lindau disease (VhL), tuberous sclerosis, and neurofibromatosis type 1 (Nf-1). The association of PNeTs with meN i varies by functional tumor type, with gastrinomas being the most common. in addition, PNeTs have varying rates of malig-nancy based on functional status, ranging from mostly
benign (insulinoma) to more commonly malignant more than 50% of the time (gastrinoma, somatostatinoma). PNeTs have a varying predilection to occur in the different parts of the pancreas (pancreatic head or tail), with insulinomas most commonly occurring in the pancreatic tail and gastri-nomas in the pancreatic head and gastrinoma triangle. The common location, association with meN i, and malignancy rate are summarized by PNeT functional status and hormone production here [see Table 1].
Evaluation
laboratory
functional PNeTs can be detected by elevated serum lev-els of the incriminated peptide [see Table 1]. Nonfunctional PNeTs produce distinct gastrointestinal peptides as well, including chromogranin a, neurotensin, and pancreatic polypeptide. however, these peptides are not associated with clinical symptoms or syndromes. chromogranin a levels have been shown to correlate with tumor presence in both functional and nonfunctional PNeTs. similar to other biomarkers, chromogranin a is useful for both confirmation of the diagnosis in a patient with suspected PNeT on imag-ing and posttreatment surveillance for recurrence. it should be noted that chromogranin a levels can be elevated in patients on proton pump inhibitors, in patients with atrophic gastritis, and in patients with hepatic or renal insufficiency.
imaging
imaging of PNeTs is essential in diagnosis and manage-ment. Tumor location, size, and relationship to surrounding structures are evaluated, as well as the presence of nodal disease and distant metastases.
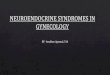
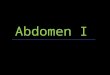
contrast-enhanced computed tomography (cT), with fine cuts and multiphase imaging, is the primary modality used for evaluation of PNeTs. on cT, PNeTs are hypervascular and typically enhance in the arterial phase [see Figure 1]. magnetic resonance imaging (mri) can also allow for assess-ment of local tumor extension and distant spread and has the advantage of elucidating pancreatic ductal anatomy. endoscopic ultrasonography (eus) has been increasingly used for tumor evaluation and can allow for fine-needle aspiration for cytologic examination [see Figure 2]. on eus, PNeTs appear as homogeneous, hypoechoic masses. The sensitivity and specificity of eus for the detection of PNeTs have been reported as 82 to 93% and 95%, respectively.5,6
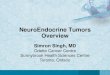
most PNeTs, with the notable exception of insulinomas, overexpress somatostatin receptors. Therefore, somatostatin receptor scintigraphy (srs) can be useful in the evaluation of PNeTs [see Figure 3]. srs has been shown to be more sensitive than conventional axial imaging in the detection of PNeTs, with the use of srs changing clinical management

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 2
tumor on other imaging modalities, calcium-stimulated angiography can be undertaken. selective mesenteric arterial infusion of calcium with simultaneous hepatic venous sam-pling for increased peptide levels can localize the region of the pancreas harboring the elusive tumor. although calcium-stimulated angiography is less often used in the modern
in 12 to 53% of patients with PNeTs, particularly in advanced disease.7–9 imaging algorithms vary with suspected tumor type, location, and association with meN i.
in rare cases, a PNeT cannot be localized with the afore-mentioned imaging studies. in patients with biochemical evidence of a functional PNeT, but without an identified
Table 1 Pancreatic Neuroendocrine Tumors
Tumor Clinical Presentation Laboratory DiagnosisCommon Location
in Pancreas
% Malig-nant
% Associated
with MEN I Incidence
insulinoma hypoglycemia, neuroglycopenia, symptoms relieved with eating
72 hr fast: glucose < 55 mg/dL, insulin > 3 uu/mL; insulin/glucose ratio > 0.3; c-peptide > 0.2 nmol/L; negative sulfonylureas
head = body/tail 5–15 5 0.7–4 per million per year
Gastrinoma refractory peptic ulcer disease, diarrhea
elevated fasting serum gastrin level; secretin stimulation test with paradoxical increase in gastrin > 200 pg/mL
Gastrinoma triangle
60–90 25–40 0.7–4 per million per year
ViPoma Watery diarrhea, hypokalemia, achlorhydria
diarrhea and serum ViP > 75 pg/mL
Body/tail >> head
40–70 5 0.7–4 per million per year
Glucagonoma Glucose intolerance, necrotizing migratory erythema, depression, venous thrombosis
elevated fasting serum glucagon > 500 pg/mL
Tail > body > head
50–80 10 0.7–4 per million per year
somatostati-noma
diabetes, steatorrhea, cholelithiasis
elevated fasting serum somatostatin > 160 pg/mL
duodenum; head > body/tail
70–80 45 0.7–4 per million per year
Nonfunctional None or symptoms of local invasion or metastasis
elevated chromogranin a (> 300 pg/mL), neurotensin, pancreatic polypeptide (> 200 pg/mL); typical radiographic characteristics, histopathologic confirmation
most in head of pancreas
60–90 20 0.7–4 per million per year
meN = multiple endocrine neoplasia; ViP = vasoactive intestinal polypeptide.
Contrast: CONTRASTGantry: 0°Fov: 400 mmTime: msSlice: 5 mmPos: 191.3FFS
F: B447 mA120 kVImage no: 33Image 33 of 94
Figure 1 Computed tomographic image of a nonfunctional pancre-atic neuroendocrine tumor (arrow) in the head of the pancreas. The tumor enhances with intravenous contrast.
Figure 2 Endoscopic sonogram demonstrating a 1.2 cm insulinoma in the uncinate process of a 47-year-old man who had negative or equivocal cross-sectional imaging. Because of the location of the tumor, the patient required pancreaticoduodenectomy.PD = pancreatic duct; SMA = superior mesenteric artery; SMV/PV CONF = superior mesenteric vein–portal vein confluence.

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 3
a b
c d
Figure 3 A gastrinoma in the head of the pancreas visualized on a computed tomography (CT) image (a) is well demonstrated on an octreotide single-photon emission CT/CT scan (b). Corresponding axial (c) and coronal (d) octreotide scan. The lesion is denoted by green linear markers.
era of sophisticated less invasive imaging modalities, it is an important technique in the occasional challenging case.
staging
The histologic evaluation of PNeTs for prognostic impli-cations is challenging and has been historically ill-defined. The World health organization (Who) [see Table 2]10 and the american Joint committee on cancer (aJcc) [see Table 3]11–13 have both recently proposed pathologic classifi-cation and staging systems for PNeTs. These systems have been validated clinically.
The Who classification is for all neuroendocrine tumors regardless of the site of origin, including PNeTs. in the Who classification system, neuroendocrine tumors are categorized as low (grade 1, G1), intermediate (grade 2, G2),
or high (grade 3, G3) grade. further classification is based on size, invasion of other organs, the Ki-67 proliferative index, presence of angioinvasion, and functional status [see Table 2]. more recently, the aJcc has applied the TNm staging system initially developed for pancreatic adenocarcinoma to pancreatic neuroendocrine tumors, and this staging system has become widely accepted for use [see Table 3].
Surgical Management
locoregional disease
for patients with locoregional disease, complete surgical resection is the primary therapeutic approach. surgical technique incorporates a formal oncologic resection with the goal of margin negativity and regional lymphadenectomy.

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 4
Table 3 aJcc TNm staging system for Pancreatic Neuroendocrine Tumors13
Primary Tumor (T) Description
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
Tis carcinoma in situ (includes Paniniii)
T1 Tumor limited to pancreas, ≤ 2 cm in size
T2 Tumor limited to pancreas, > 2 cm in size
T3 Tumor extends beyond the pancreas but without involvement of celiac axis or superior mesenteric artery
T4 Tumor involves the celiac axis or superior mesenteric artery
Regional Lymph Nodes (N) Description
NX regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 regional lymph node metastasis
Distant Metastasis (M) Description
m0 No distant metastasis
m1 distant metastasis
Anatomic Stage TNM Stage
0 Tis N0 m0
ia T1 N0 m0
iB T2 N0 m0
iia T3 N0 m0
iiB T1 N1 m0
T2 N1 m0
T3 N1 m0
iii T4 any N m0
iV any T any N m1
aJcc = american Joint committee on cancer.
Table 2 World health organization histologic classification system for Pancreatic Neuroendocrine Tumors10
FactorNeuroendocrine Tumor
(low grade, G1)Neuroendocrine Carcinoma
(intermediate grade, G2)Neuroendocrine Carcinoma
(high grade, G3)
mitotic rate per high-power field < 2 2–20 > 20
Ki-67 index < 3% 3–20% > 20
Necrosis absent — Present
size < 2 cm > 2 cm any size; invasion of adjacent organs, lymph node metastases
angioinvasion No No Yes
distant metastases No No Yes
for all PNeTs in aggregate, patients undergoing resection have a reported 5-year overall survival of 55 to 64%, with a median survival of 60 to 100 months.4,12,14–16
a notable exception to the requirement for oncologic resection is insulinomas. as they are usually benign [see Table 1], they can often be managed with enucleation. additionally, controversy exists over the potential manage-ment of small, incidentally discovered, nonfunctional PNeTs with limited resection or even observation.17 Both of these exceptional cases are considered in more detail below.
on the other end of the spectrum, PNeTs, most typically nonfunctional, can present with advanced localized disease. aggressive multivisceral resection can be undertaken in these patients, with reasonable expected morbidity and survival improvement similar to those of other patients with resected locoregional disease.16,18–20 recurrence after resection for locally advanced disease, however, is common, reported in 47 to 100% of patients in small series.16,19
metastatic disease
PNeTs often present late, with advanced disease, and have a propensity to recur after initial treatment with surgi-cal resection, with the most common site being the liver. Propensity to do so varies with initial tumor type, grade, and functional status. hepatic metastases occur in greater than half of patients with PNeTs, and liver metastases portend a significantly decreased 10-year survival.21,22 Given the relatively indolent behavior of this tumor even in the setting of metastatic disease, a variety of treatment options exist and continue to be developed to aggressively address metastatic liver disease. These entail surgical options as well as percutaneous radiologic techniques such as radiofre-quency ablation (rfa), which are best chosen with the involvement of a multidisciplinary care team.
Hepatic Resection for Metastatic Disease
Given the indolent nature of PNeTs, debulking surgery, where resection is undertaken with the recognition that there will be residual tumor burden, has been undertaken in carefully selected patients with advanced and metastatic disease. This approach is controversial. some studies show that cytoreductive surgery does not result in improved

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 5
survival.23–25 however, the experience from the mayo clinic suggests that significant reduction of tumor burden (> 90%) can be beneficial. in that series, 5-year overall survival was 48%.26–28
however, when feasible, complete surgical resection of metastatic disease (most commonly hepatic) is the optimal treatment and can translate into prolonged overall survival (61 to 69%) and disease-free survival (11 to 24%) at 5 years.26–28
Locally Ablative Therapies
Locally ablative therapies of metastatic hepatic tumor foci are considered palliative treatments in patients with metastatic PNeTs that are limited to the liver or in liver- predominant disease associated with a functional hormonal syndrome. ablative techniques are best for patients who are not good surgical candidates. in the setting of bilobar, unre-sectable disease, the combined use of resection and ablative therapy addresses all disease and improves survival. abla-tive techniques include rfa, cryoablation, hepatic arterial embolization (hae), and ethanol ablation. The most com-monly used technique is rfa. rfa can be undertaken alone or in conjunction with surgical resection. it is best used in patients with smaller tumors (< 3.5 to 5 cm), few lesions (< 5 to 15), and lesions not abutting major vascular struc-tures (which acts as a heat sink, preventing achievement of necessary temperatures for ablation).
similar to locally ablative therapies, hae is undertaken in patients with confined hepatic metastases or with significant disease burden in the liver who are not amenable to surgical resection. hae draws on the premise that tumor blood supply is predominantly arterial, whereas the hepatic blood supply is primarily from the portal vein. Thus, hae selec-tively targets tumor foci over normal liver tissue. emboliza-tion can be performed with a hemostatic embolic agent (transarterial embolization [Tae]) or with a chemotherapeu-tic agent (transarterial chemoembolization [Tace]) such as doxorubicin, 5-fluorouracil, cisplatin, mitomycin c, and streptozocin. Tumor response rates of 25 to 86% are reported, with a duration of response of 6 to 45 months.29,30 in a study of 127 patients with metastatic neuroendocrine tumors, of whom 69 were treated with rfa whereas the others underwent resection or hae, rfa had the lowest morbidity and provided effective symptom relief in 91% of patients at a mean follow-up of 20 months.31 response rates of 80 to 95% with up to a 3-year follow-up are reported.32,33
hae with yttrium-90 microspheres is a relatively new treatment option for metastatic PNeTs. The response rate for patients treated with radioembolization for neuroendo-crine tumors is reported as 12.5 to 89%, with stable disease in 10 to 60%.34
few data are available on the less commonly performed ablative techniques.
Liver Transplantation
Liver transplantation is currently applied in selected patients with metastatic PNeT confined to the liver, although it is a controversial issue. an analysis of the united Network for organ sharing database in 2011 identified 185 liver transplantations for neuroendocrine tumors in the united states, with an overall 5-year survival of 58%.35 in a french multicenter review of 85 liver transplantations for metastatic neuroendocrine tumors, 5-year overall and disease-free
survival were 47% and 20%, respectively.36 The european Neuroendocrine Tumor society (eNeTs) 2012 consensus guidelines recognize that recurrence is significant; thus, transplantation should be reserved for selected patients who are refractory to other treatments and have favorable tumors, with a low Ki-67 index and normal e-cadherin, that are histologically well differentiated, have no extrahepatic disease, and are a young age (< 50 years).37
Medical Management
surgery is the primary treatment modality in the patient with PNeT. however, in patients with advanced disease, medical management plays a significant role. exciting new medical therapies have emerged over the past several years, with significant potential benefit for these patients.
biotherapy
PNeTs overexpress somatostatin receptors in 70 to 100% of cases. as such, somatostatin analogues act to ameliorate the hormonal excess state in patients with functional PNeTs to control symptoms and have been shown to have anti– tumor proliferation effects.38,39 somatostatin analogues are available in short-acting formulas, which are administered subcutaneously two to four times per day, and in long- acting preparations, which are administered intramuscularly every 4 weeks. in patients unresponsive to somatostatin analogue therapy or with somatostatin receptor–negative tumors, interferon can be used to decrease hormonal symp-toms and for tumoristatic effects. a median symptomatic response rate of 40 to 70% has been reported with interfer-on.40 This is also given as an injection and has significantly more side effects than somatostatin analogues, including fever, chills, headache, and muscle aches following each.
chemotherapy
chemotherapy is indicated for patients with advanced metastatic PNeTs. independent of their tissue of origin, poorly differentiated PNeTs are generally responsive to cisplatinum in combination with etoposide therapy.41 more well-differentiated PNeTs are classically treated with streptozocin, 5-fluorouracil, and doxorubicin. response rates of 20 to 45% are reported.42 more recently, temozolo-mide combined with capecitabine has been used in patients with metastatic PNeTs, with response rates reported as high as 70%.43
targeted therapies
everolimus is a mammalian target of rapamycin (mTor) inhibitor that has antitumor effects on PNeTs. The rad001 in advanced Neuroendocrine Tumors (radiaNT-3) trial demonstrated a significant improvement in progression-free survival over placebo in patients with advanced disease who were treated with everolimus (11 versus 4.6 months; p < .0001).44 Tyrosine kinase inhibitors have also been incor-porated in the treatment of patients with advanced PNeTs. most notably, sunitinib has been shown to be clinically effective. in a placebo-controlled prospective trial, sunitinib demonstrated benefit in progression-free (11.4 versus 5.5 months; p < .001) and overall survival.45
Peptide receptor radionuclide therapy (PrrT) entails yttrium-90 and lutetium-177 radioisotopes conjugated with

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 6
in a review by researchers at massachusetts General hospi-tal of their experience with 139 patients with incidentally discovered nonfunctional PNeTs, 28% were found to be malignant. in their study, even tumors less than 2 cm were associated with disease recurrence and progression. The investigators concluded that incidentally detected PNeTs can display aggressive behavior, even when small; there-fore, all should be resected.47 however, the group at moffitt cancer center reviewed their experience with 143 PNeTs, of which 56 (40%) were incidental findings. They found a 5-year progression-free survival rate of 86% for incidentally discovered tumors versus 59% for symptomatic tumors (p = .007) and concluded that more selective criteria for resection may be in order.48 in a review of their experience at the mayo clinic, 77 patients with small, asymptomatic, nonfunctional PNeTs did not undergo resection and were observed.49 in this group, the median tumor size (1 cm, range 0.3 to 3.2 cm) did not change over the mean 45-month follow-up, and there was no disease progression or disease-specific mortality. additionally, in the operative group (median tumor size 1.8 cm, range 0.5 to 3.6 cm), 46% had a complication, most due to a clinically significant pancreatic leak. The authors advocate nonoperative management and close radiographic surveillance in selected patients with small asymptomatic nonfunctional PNeTs. Given the limit-ed data and potential malignant nature of small, incidental, nonfunctional PNeTs, management remains controversial. if observed, there are no clear guidelines regarding the frequency of surveillance.
Minimally Invasive Surgery
significant technical advances have evolved over the past decade in pancreatic surgery, including laparoscopic and robotic pancreatic resection. in an effort to minimize perioperative morbidity, pancreatic surgeons have applied minimally invasive techniques to PNeTs. Laparoscopic pan-creatic resections are well described [search the publication for minimally invasive pancreatectomy], including anatomic resection (laparoscopic distal pancreatectomy, pancreato-duodenectomy) and nonanatomic resections (laparoscopic enucleation, middle segment pancreatectomy). in experi-enced hands, the minimally invasive approach has been shown to be feasible and advantageous over the open approach, with decreased blood loss, morbidity, and hospi-tal stay. at the same time, equivalent operative times and margin status have been demonstrated.50,51
Parenchyma-Sparing Techniques
in an effort to preserve pancreatic parenchyma and endocrine/exocrine function, several parenchyma-sparing techniques have been applied to PNeTs. The parenchyma-sparing techniques entail obtaining a negative local margin but notably do not allow for regional lymphadenectomy and therefore are best reserved for benign or low-grade PNeTs. enucleation involves removing or shelling out the PNeT in its entirety, with a negative perilesional margin but no sur-rounding pancreatic parenchyma. it has become standard in insulinoma management and is becoming increasingly applied in nonfunctional PNeTs, particularly those that are small, located in the head of the pancreas, and at least 3 mm from the main pancreatic duct and with a presumed benign
somatostatin analogues for targeted radiotherapy. PrrT appears to be effective in stabilization of tumor growth, with some tumoricidal effect.46
controversy exists regarding the exact role and timing of the various medical therapies in the management of patients with advanced PNeTs. Generally, biotherapy is favored due to the low side-effect profile. in more aggressive, faster-growing tumors with poor prognostic indicators, chemo-therapy is undertaken. The targeted therapies have more recently gained favor with growing science and experience in the treatment of advanced PNeTs.
Nonfunctional Pancreatic Neuroendocrine Tumors
general considerations
Nonfunctional PNeTs comprise the majority of PNeTs and 2% of pancreatic malignancies. They occur with an annual incidence of one to three per million population. Nonfunctional PNeTs are typically sporadic (20% associated with meN i), and more than 60% are malignant [see Table 1].4 despite their malignant characteristics, nonfunctional PNeTs are characterized by slow progression and a reasonable prognosis, particularly with resection (median 4.8 to 8.4 years). surgical resection with proper oncologic technique, includ-ing margin negativity and lymphadenectomy, is currently the primary therapeutic approach to nonfunctional PNeTs. an algorithm for the management of nonfunctional PNeTs is shown here [see Figure 4]. Typically, patients present with symptoms prompting cross-sectional imaging. once a pan-creatic mass is identified, it may have characteristic radio-graphic features (hypervascular [see Figure 1]) that suggest PNeT. chromogranin and pancreatic polypeptide levels can be sent, and patients should be asked about associated hormonal symptoms to rule out functional tumor. When necessary, a definitive tissue diagnosis can be obtained via eus and biopsy (for localized disease) or percutaneous liver biopsy in the case of metastatic disease. Treatment depends on the presence or absence of metastatic disease [see Figure 4]. in general, if complete resection is possible, even with metastatic disease, this should be the first-line therapy in patients who present a reasonable surgical risk.
current controversies
classically, nonfunctional PNeTs present late in disease due to the lack of clinical symptomatology, with as many as 50% of patients presenting with metastatic disease.22 more recently, a seeming epidemic of incidentally discovered pancreatic neoplasms, including PNeTs, has occurred due to the technological advances in axial imaging as well as the increased use of axial imaging in medical evaluation. small, asymptomatic lesions are now being detected at a higher rate and have brought forth new clinical controversies in the management of PNeT, including indications for surgery and goals of resection. importantly, clinical outcomes data are essential in understanding the biologic behavior and prog-nosis of small lesions and in understanding the morbidity and appropriateness of modern surgical approaches.
Incidentalomas
Nonfunctional PNeTs are incidentally discovered with increasing frequency, and some controversy exists regard-ing the management of these pancreatic “incidentalomas.”

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 7
SRS
Localized disease
Metastatic disease
Complete resection not possible
Large (> 2 cm)
Small (< 2 cm)
Resection
Octreotide
Complete (or near- complete > 90%) resection possible
Body/tail: distal pancreatectomy
Immunotherapy (everolimus, sunitinib)
Hepatic-directed therapies (hepatic arterial embolization, chemoembolization)
Head: pancreatoduodenectomy
Head: pancreatoduodenectomy or enucleation (if > 3 mm from main pancreatic duct)
Cytotoxic chemotherapy (streptozotocin, 5-FU, doxorubicin; temozolomide, capecitabine; cisplatinum, etoposide )
< 1 cm, asymptomatic, poor surgical risk: consider observation
Body/tail: distal pancreatectomy with splenectomy
Contrast-enhanced multiphase CT or MRI
Chromogranin A level and pancreatic polypeptide level
± EUS
Figure 4 Management algorithm for nonfunctional pancreatic neuroendocrine tumors. CT = computed tomography; EUS = endoscopic ultrasonography; 5-FU = 5-fluorouracil; MRI = magnetic resonance imaging; SRS = somatostatin receptor scintigraphy.
or low-grade biology. crippa and colleagues described their experience with enucleation in 61 patients, the majority of whom had nonfunctional PNeTs, and found reasonable operative times and estimated blood loss.52 however, enu-cleation was associated with a 38% postoperative pancreatic
fistula rate. interestingly, in the long term, no patient devel-oped new-onset exocrine failure and only 3% developed new-onset diabetes.
middle segment pancreatectomy has also been applied in PNeT management. middle segment pancreatectomy

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 8
involves resection of a segment of the pancreas over the portal vein with a pancreaticojejunal anastomosis fashioned to the preserved pancreatic body and tail segment. a multi-center comparative study of middle segment pancreatectomy (N = 100) with extended distal pancreatectomy for benign or low-grade pancreatic neck lesions showed an increased operative time and decreased blood loss in the middle segment pancreatectomy group but equivalent morbidity, including pancreatic fistula. importantly, the rates of post-operative new exocrine and endocrine failure were signifi-cantly lower in the middle segment pancreatectomy group.53 several investigators have evaluated their experience collec-tively with parenchyma-sparing techniques and have found decreased operative times,54,55 blood loss,54,55 morbidity,54 and hospital stay,55,56 as well as decreased postoperative pancreatic exocrine and endocrine insufficiency.55 impor-tantly, similar long-term survival has been reported between parenchyma-sparing surgery and conventional resection.4,54 Larger experience with long-term clinical outcomes is important to fully elucidate the role of these techniques in the management of PNeTs as the above studies included varying types of benign and low-grade lesions.
Insulinoma
epidemiology
insulinomas are the most common of the functional PNeTs, with an incidence of one to two per million popula-tion. most tumors are solitary and low grade, exhibiting benign behavior in 85 to 95% of cases. although the major-ity of insulinomas are sporadic, 5% are associated with meN i, and these are more likely to be multiple and malignant.57 The management algorithm for suspected insulinoma is shown here [see Figure 5].
clinical presentation and diagnosis
insulinomas present with the classic “Whipple triad” of symptoms of hypoglycemia and neuroglycopenia (diapho-resis, confusion) and resolution of symptoms with eating. Patients have often gained weight as they eat more frequently to prevent hypoglycemic episodes. diagnosis can be estab-lished classically with a 72-hour monitored fast, with glu-cose, insulin, c-peptide, proinsulin, and b-hydroxybutyrate tested at 6-hour intervals and immediately when a patient becomes symptomatic. Glucose and insulin levels are evaluated to determine the inappropriate release of insulin in the face of hypoglycemia. c-peptide and proinsulin levels can help exclude the administration of exogenous insulin, and b-hydroxybutyrate levels or urine sulfonylureas exclude the use of oral hypoglycemic agents. a plasma glucose level less than 55 mg/dL, a simultaneous insulin level greater than or equal to 3 uu/mL, c–peptide of 0.2 nmol/mL or greater, proinsulin of 5 pmol/L or greater, and negative sulfonylureas constitute a positive fast. alternatively, an insulin-to-glucose ratio greater than 0.3 is diagnostic.58 it is critical to monitor patients during the fast to promptly obtain levels and treat hypoglycemia at the time symptoms occur.
localization of tumor
insulinomas typically present as solitary, small, well- defined lesions and are distributed equally throughout the pancreas [see Table 1]. initial imaging is with contrast-enhanced multiphase cT or mri. These modalities are very sensitive for insulinomas greater than 1 cm in size. eus is more sensitive than conventional axial imaging and can be very useful in elusive cases or in cases associated with meN i. Because insulinomas, unlike other PNeTs, do not typically overexpress somatostatin receptors, srs is not very helpful in localizing insulinomas.
± EUS
Chromogranin A level
Insulin to glucose ratio 72 hr fast
Unlocalized: calcium-stimulated angiography
Contrast-enhanced multiphase CT or MRI
Locoregional disease
Medical managementBody/tail lesion: distal pancreatectomy
Head lesion: pancreatoduodenectomy
Head lesion, < 3 cm, > 3 mm from the pancreatic duct: enucleation, consider laparoscopic
Glucose control, diazoxide
Metastatic disease
Figure 5 Management algorithm for insulinomas. CT = computed tomography; EUS = endoscopic ultrasonography; MRI = magnetic resonance imaging.

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 9
crippa and colleagues of 198 patients with resected insuli-noma reported that 88% were low grade and 7% had lymph node or distant metastases.57 Postoperative morbidity included a pancreatic fistula rate of 18%, which is consistent with other groups.54,55,60 With a median follow-up of 65 months, 3% of patients developed recurrence and 2% died of disease.57
Gastrinoma
epidemiology
Gastrinoma is the other relatively common functional PNeT, occurring with an annual incidence of 0.3 to 5 cases per million population. Gastrinomas cause gastric acid hypersecretion through stimulation by an overproduction of gastrin, resulting in intractable peptic ulcer disease. especially in the era of proton pump inhibitors, in patients with refractory peptic ulcer disease or ulcers in uncommon locations (third and fourth portions of the duodenum or jejunum), the diagnosis of gastrinoma should be considered. Gastrinoma is malignant in 60 to 90% of cases. it is the most common PNeT found in meN i, but the majority of cases are sporadic, with only 25 to 40% of cases occurring in the setting of meN i [see Table 1]. Gastrinoma has also been reported in association with neurofibromatosis.61
clinical presentation and diagnosis
Gastrinoma classically presents with abdominal pain and diarrhea (70%) in the presence of refractory peptic ulcer dis-ease. The management algorithm for gastrinoma is detailed here [see Figure 6]. diagnosis is corroborated by an elevated serum gastrin level. however, hypergastrinemia can be related to multiple other causes shown here [see Table 4]. as such, these things must be ruled out to make the diagnosis of gastrinoma. Proton pump inhibitors should be stopped
if the insulinoma is unable to be localized with cT, mri, and eus, then calcium-stimulated selective mesenteric angiography with hepatic venous sampling for insulin can help localize the region of the tumor within the pancreas, with a reported sensitivity of 88%. regional portal venous sampling for insulin can also be used, with a reported sensitivity of 81%.59 if the tumor is not localized preopera-tively, intraoperative ultrasonography is undertaken to find the tumor and guide surgical management. however, this should happen very infrequently with modern imaging technology.
operative management
Preoperative preparation includes proper glucose man-agement. somatostatin analogues and diazoxide (inhibits insulin release and enhances glycogenolysis) are used to aid in medical control of blood glucose.
operative conduct is dictated by the size and location of the tumor, with particular note of its relationship to the main pancreatic duct, which can be evaluated on preopera-tive cT, mri/magnetic resonance cholangiopancreatogra-phy, or eus. The goals of surgery are complete tumor extirpation with parenchyma preservation and minimal morbidity. small, solitary, well-circumscribed (sporadic) tumors with some distance from the pancreatic duct are well suited to enucleation, which can be performed openly or laparoscopically. Tumors in the body or tail may be as safely managed with open or laparoscopic distal pancreatec-tomy. anatomic resection is favored in cases with close ductal proximity. Those tumors that are large or malignant in appearance should be treated with formal resection, including lymphadenectomy.
outcomes
insulinomas are benign in 85 to 95% of cases [see Table 1], with an excellent long-term prognosis. a recent review by
± EUS
± SRS
Secretin- or Ca- stimulated gastrin level
Fasting gastrin level
Contrast-enhanced multiphase CT or MRI
Locoregional disease
Not localized
Resection
ResectionLocalized
Not localized
Body/tail (rare): distal pancreatectomy
Head/duodenal (most common): anatomic resection with pancreatoduodenectomy; small < 2 cm without LAD, consider enucleation
Medical management
Exploration with intraoperative ultrasonography
Ca-stimulated angiography and/or portal venous sampling
Metastatic disease
Figure 6 Management algorithm for gastrinomas. CT = computed tomography; EUS = endoscopic ultrasonography; LAD = lymphadenopathy; MRI = magnetic resonance imaging; SRS = somatostatin receptor scintigraphy.

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 10
Table 4 differential diagnosis of hypergastrinemia
Gastrinomaantral G cell hyperplasiaconditions associated with achlorhydria or reduced gastric acid
secretionPernicious anemiachronic atrophic gastritisProton pump inhibitor therapy
conditions associated with gastric acid hypersecretionHelicobacter pylori infectionGastric outlet obstruction
Truncal vagotomyretained gastric antrum (in patients who have undergone prior
antrectomy)short bowel syndromerenal failure
for 2 weeks prior to serum gastrin testing. a fasting serum gastrin greater than 1,000 pg/mL is considered diagnostic of gastrinoma, but this degree of hypergastrinemia is present in less than a third of cases.62 in cases where serum gastrin levels do not provide a definitive diagnosis, a secretin or calcium stimulation test is done [see Table 5]. The test entails giving 2 units/kg secretin intravenously and then measur-ing serum gastrin at serial intervals over the ensuing half hour. an increase in serum gastrin of greater than 200 pg/mL over baseline is considered diagnostic. alternatively, a cal-cium stimulation test entails infusion of calcium gluconate followed by serial measurement of serum gastrin over 3 hours, with an increase in serum gastrin of greater than 400 pg/mL considered diagnostic. it is essential to ensure that patients are not achlorhydric as this can lead to significantly elevated serum gastrin levels.
localization of tumor
Gastrinomas are classically located in the gastrinoma triangle, which is bordered by the neck of the pancreas, the
Table 5 secretin and calcium Provocative Testing for Gastrinoma
Withdraw patient from PPis for at least 3 days, possibly up to 7 days
Withdraw patient from h2 blocker for at least 30 hoursovernight fastsecretin stimulation test
administer 2 u/kg secretin iV bolusmeasure serum gastrin levels at 0, 2, 5, 10, 20, 30 minan increase in serum gastrin by more than 200 pg/mL over
baseline levels is diagnostic of gastrinoma73; new criterion using 120 pg/mL has been found to have increased sensitivity and specificity (sensitivity 94%, specificity 100%)62
calcium infusion testadminister 54 mg/kg/hr of 10% calcium gluconate
(5 mg/kg/hr of calcium) by continuous iV infusion for 3 hours
measure serum calcium and serum gastrin levels every 30 min for 3 hours
an increase in serum gastrin level by more than 395 pg/mL over baseline levels is diagnostic of gastrinoma73
iV = intravenous; PPi = proton pump inhibitor.
junction of the second and third portions of the duodenum, and the junction of the cystic and common bile ducts. Lymph node–only primary gastrinomas are reported in 4 to 13% of cases, which may represent true primary tumors or occult metastases from unidentified primary lesions.63 sporadic gastrinomas are usually solitary and located with equal fre-quency in the pancreas and duodenum. meN i–associated gastrinomas are often multiple and more frequently located in the duodenum.
initial localizing studies include axial imaging with contrast-enhanced multiphase cT, including water as oral contrast to enhance duodenal imaging, or mri. as gastrino-mas overexpress somatostatin receptors, srs can be helpful in their detection (sensitivity 53 to 72%). eus is useful in the localization of pancreatic and duodenal gastrinomas, with a sensitivity of 67 to 100% reported. srs or eus should be routinely considered in meN i patients to enhance lesion detection given the high rate of multiple lesions. in addition, srs is useful in monitoring for recurrence in these patients.
similar to insulinoma, if these primary modalities do not locate the tumor, more invasive techniques, including calcium-stimulated angiography with hepatic venous sam-pling or selective portal venous sampling, can be undertaken.64
operative management
Preoperative optimization of the gastrinoma patient comprises proton pump inhibitors to normalize gastric hyperacidity. additionally, all patients with meN i should be screened for hypercalcemia and parathyroid adenoma/hyperplasia. When present, hypercalcemia and parathyroid disease should be treated prior to surgery as calcium stimulates gastrin secretion.
surgical resection should be the primary approach to resectable gastrinoma in the modern era. historically, controversy existed over the best surgical approach to gas-trinoma, whether to perform a total gastrectomy to relieve symptomatology or to attempt tumor resection. This contro-versy shifted in the 1980s when effective acid suppression therapy emerged to whether gastrinoma should be managed medically altogether. With the evolving understanding of the natural history of gastrinoma and with the accumulation of clinical outcomes data, it is clear that surgical resection increases survival in gastrinoma due to control of the primary tumor and prevention of disease progression.65
operative management of sporadic small noninvasive gastrinomas that are located in the head entails enucleation. small tumors in the body and tail can be managed with either enucleation or distal pancreatectomy.64 in invasive or large tumors, formal anatomic resection with lymphade-nectomy is undertaken. management of the sporadic gastri-noma that is not localized preoperatively is controversial in the modern era of proton pump inhibitor therapy, but consensus still favors exploration. Norton and colleagues recently reported experience with 58 patients with sporadic gastrinoma who underwent exploration without preopera-tive localization.66 Tumors were located in 57 of the 58 patients and were mostly less than a centimeter in size. at a mean follow-up of 9.4 years, 46% were disease free and three had died of disease. in patients with unlocalized disease, operation entails mobilization of the duodenum

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 11
The diagnosis is established with an elevated serum glucagon level. The fasting serum glucagon level should be greater than 1,000 pg/mL. The differential diagnosis of hyperglucagonemia includes prolonged fasting, diabetic ketoacidosis, liver disease, malabsorption, danazol therapy, renal failure, and sepsis [see Table 6].67
localization of tumor
most glucagonomas are large in size and located in the tail of the pancreas [see Table 1].67 most are malignant. cross-sectional imaging, including contrast-enhanced multiphase cT or mri, is well used to identify the tumor. srs is also beneficial, as well as eus. in elusive cases, which are rare, selective portal venous sampling can localize the region of the tumor within the pancreas where the tumor is located.
operative management
Preoperative optimization includes somatostatin analogue therapy. Blood glucose should be tightly controlled, and nutrition should be optimized. Zinc deficiency is common and should be corrected in these patients. administration of amino acids and correction of malnutrition lead to resolution of the characteristic skin rash. Because of the hypercoagulable state, anticoagulation therapy should be considered.
operative management entails formal anatomic resection with margin negativity and lymphadenectomy. due to its high rate of malignancy, glucagonoma is not treated with enucleation. cholecystectomy is recommended to prevent gallstone-related complications.67 Glucagonomas are rare; thus, outcomes data are lacking. The majority are malignant but, like other PNeTs, indolent in progression.
Somatostatinoma
epidemiology
somatostatinomas are rare PNeTs, with an incidence of 0.1 persons per million population. They are often malig-nant, representing 70 to 80% of cases. They are associated with meN i in 45% of cases and are also found in neurofi-bromatosis [see Table 1].69
and pancreas with palpation and intraoperative ultrasonog-raphy. duodenal transillumination and duodenotomy for exploration are important operative localization maneu-vers. a small duodenal tumor should be enucleated with periduodenal lymphadenectomy.
Patients with meN i are more likely to have multiple lesions that are malignant; thus, management of these persistent yet elusive tumors differs from that of sporadic gastrinoma and is controversial. medical management only with proton pump inhibitor therapy can control symptoms effectively, whereas surgical exploration with resection can be the only opportunity for cure of this potentially malig-nant disease. Patients are best managed on an individual basis, with consideration of organ involvement, potential for morbidity, and chance of disease clearance. These patients often require multiple operations, and the presence of nodal metastases in the absence of a primary tumor can sometimes occur.
outcomes
The prognosis of patients with gastrinoma depends on tumor size and location, the presence of liver metastases, and meN i association. Liver metastases are the most impor-tant determinant of survival, and lymph node metastases over long-term follow-up decrease survival with an increas-ing number of positive nodes.21 after resection, 41 to 46% of patients are disease free long term. fifteen-year disease-specific survival is 98% for operated patients and 74% for unoperated patients [see Figure 6].65,66 meN i–associated gastrinomas, despite their tendency for multiplicity and regional lymph node spread, often behave in a more indo-lent fashion than sporadic tumors and can be associated with a more favorable prognosis.
Glucagonoma
epidemiology
Glucagonoma is a rare tumor, occurring in 0.1 persons per million population. it is marked clinically by hyperglu-cagonemia, diabetes, and necrolytic migratory erythema. Glucagonomas are malignant in 50 to 80% of cases, with metastases (most commonly to liver but also to bone, adre-nal glands, and lung) at initial presentation in 78 to 90% of patients. most cases are sporadic, but up to 10% may be associated with meN i [see Table 2].67,68
clinical presentation and diagnosis
Glucagonomas present with diabetes, necrolytic migratory erythema (a blistering rash typically on the lower abdomen, groin, and buttocks and the perioral region occurring in 70% of patients), and deep vein thrombosis. Patients also often experience weight loss and malnutrition (hypoaminoacide-mia) due to the catabolic effects of glucagon. Glucagon also suppresses the bone marrow; thus, patients are often anemic. in addition, patients may develop neuropsychiatric disturbances, most notably depression. The hypercoagulable state that results in venous thromboembolism is thought to be due to a factor X–like mediator released by the tumor. Glucagonomas may also secrete other gut hormones, including gastrin, vasoactive intestinal polypeptide (ViP), pancreatic polypeptide, and somatostatin.
Table 6 differential diagnosis of hyperglucagonemia
GlucagonomaProlonged fasting/starvationdiabetic ketoacidosis/hyperosmotic nonketotic stateother endocrine causes
familial hyperglucagonemiacushing syndrome
Liver disease associated with decreased degradation of glucagonhepatitiscirrhosishemachromatosis
conditions associated with a malabsorptive statePancreatic diseaseceliac diseaseinflammatory bowel disease
renal failuredanazol therapyTrauma/burns/sepsis

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 12
outcomes
Patients with ViPomas can expect 5-year survival of 68% after resection, with the presence of metastatic disease representing a poor predictive factor.72
Conclusions
PNeTs are fascinating tumors increasingly encountered in the modern era. They represent a heterogeneous group of tumors and require careful evaluation and thoughtful clinical consideration. PNeTs are often malignant but also often indolent in progression and thus are ripe for benefit from a variety of interventions. significant progress in both the medical and surgical management of these tumors has occurred over the past decade and is ongoing.
Financial Disclosures: Katherine A. Morgan, MD, FACS, has no relevant financial relationships to disclose.
References
1. halfdanarson Tr, rabe KG, rubin J, Petersen Gm. Pancre-atic neuroendocrine tumors (PNeTs): incidence, prognosis, and recent trend toward improved survival. ann oncol 2008;19:1727–33.
2. Grimelius L, hultquist GT, stenkvist B. cytological differ-entiation of asymptomatic pancreatic islet cell tumours in autopsy material. Virchows arch a Pathol anat histol 1974;365:275–88.
3. Kimura W, Kuroda a, morioka Y. clinical pathology of endocrine tumors of the pancreas. analysis of autopsy cases. dig dis sci 1991;36:933–42.
4. franko J, feng W, Yip L, et al. Nonfunctional neuroendo-crine carcinoma of the pancreas: incidence, tumor biology, and outcomes in 2,158 patients. J Gastrointest surg 2010;14: 541–8.
5. rosch T, Lightdale cJ, Botet Jf, et al. Localization of pancre-atic endocrine tumors by endoscopic ultrasonography. N engl J med 1992;326:1721–6.
6. anderson ma, carpenter s, Thompson NW, et al. endoscopic ultrasound is highly accurate and directs management in patients with neuroendocrine tumors of the pancreas. am J Gastroenterol 2000;95:2271–7.
7. ruf J, heuck f, schiefer J, et al. impact of multiphase 68Ga-doTaToc-PeT/cT on therapy management in patients with neuroendocrine tumors. Neuroendocrinology 2010;91: 101–9.
8. Termanini B, Gibril f, reynolds Jc, et al. Value of somatostatin receptor scintigraphy: a prospective study in gastrinoma of its effect on clinical management. Gastroen-terology 1997;112:335–47.
9. schillaci o, spanu a, scopinaro f, et al. somatostatin receptor scintigraphy with 111in-pentetreotide in nonfunc-tioning gastroenteropancreatic neuroendocrine tumors. int J oncol 2003;23:1687–95.
10. Kloppel G, Perren a, heitz Pu. The gastroenteropancreatic neuroendocrine cell system and its tumors: the Who classification. ann N Y acad sci 2004;1014:13–27.
11. rindi G, cloppel G, alhman h, et al. TNm staging of fore-gut neuroendocrine tumors: a consensus proposal includ-ing a grading system. Virchows arch 2006;449:395–401.
clinical presentation and diagnosis
somatostatinomas present with diabetes, cholelithiasis, malabsorption, and steatorrhea. Patients often complain of abdominal pain (39%) and may have jaundice (28%) or gastrointestinal bleeding (22%).69 diagnosis is made with an elevated fasting serum somatostatin level, with a level greater than 160 pg/mL considered diagnostic.
localization of tumor
most somatostatinomas are located in the head of the pan-creas or duodenum.69axial imaging with contrast-enhanced cT or mri is a good localizing study, along with srs and, finally, eus.
operative management
as most somatostatinomas are malignant, formal onco-logic resection with margin negativity and lymphadenectomy is recommended. most often this is a pancreatoduodenec-tomy given the tumor location, commonly in the head of the pancreas or the duodenum. cholecystectomy is performed as well.70 Given their rare nature, outcomes data are lacking, but 5-year survival is reported as 100% in benign disease and 30 to 60% for those with metastatic disease after resection.71
VIPoma
epidemiology
ViPomas are rare PNeTs with an annual incidence of less than 0.1 persons per million population. They are marked clinically by the Verner-morrison syndrome, also known as Wdha syndrome (watery diarrhea, hypokalemia, achlor-hydria). ViPomas are malignant in 40 to 70% of cases. on initial presentation, as many as half are noted to have liver metastases. most are sporadic, with only 5% associated with meN i.68,72
clinical presentation and diagnosis
ViPomas present with profuse secretory diarrhea (greater than 5 L of watery stool per day that persists despite fast-ing). Patients have hypokalemia and achlorhydria as a result of the gastrointestinal losses. diagnosis is confirmed with an elevated serum ViP level.68
localization of tumor
ViPomas are most often located in the body and tail of the pancreas but can be found in the head as well. extrapancre-atic tumors can be found in the adrenals, retroperitoneum, mediastinum, small intestine, kidney, or colon.68,72 contrast-enhanced multiphase cT or mri with srs can help locate the tumor. eus is also useful to identify small tumors.
operative management
Preoperative preparation entails temporizing the diarrheal syndrome with a somatostatin analogue and normalizing electrolytes. in protracted cases, nutritional optimization should be ensured.
Given the high rate of malignant disease, current recom-mendations for the operative management of ViPoma are for a formal anatomic resection with negative margins and including lymphadenectomy. cholecystectomy is also recommended to avoid gallstone-related complications.72

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 13
12. Bilimoria KY, Bentrem dJ, merkow rP, et al. application of the pancreatic adenocarcinoma staging system to pancre-atic neuroendocrine tumors. J am coll surg 2007;205: 558–63.
13. edge sB, Byrd dr, compton cc, et al. aJcc cancer staging manual. New York: springer; 2010.
14. Bilimoria KY, Tomlinson Js, mrekow rP, et al. clinicopath-ologic features and treatment trends of pancreatic neuroen-docrine tumors: analysis of 9821 patients. J Gastrointest surg 2007;11:1460–9.
15. ito h, abramson m, ito K, et al. surgery and staging of pancreatic neuroendocrine tumors: a 14 year experience. J Gastrointest surg 2010;14:891–8.
16. schurr PG, strate T, rese K, et al. aggressive surgery improves long-term survival in neuroendocrine pancreatic tumors. an institutional experience. ann surg 2007;245: 273–81.
17. fernandez-cruz L, molina V, Vallejos r, et al. outcome after laparoscopic enucleation for nonfunctional neuroen-docrine pancreatic tumors. hPB (oxford) 2012;14:171–6.
18. hilal ma, mcPhail mJ, Zeidan Ba, et al. aggressive multi-visceral pancreatic resections for locally advanced neuroen-docrine tumors: is it worth it? JoP 2009;10:276–9.
19. Norton Ja, Kivlen m, Li m, et al. morbidity and mortality of aggressive resection in patients with advanced neuroen-docrine tumors. arch surg 2003;138:859–66.
20. Nguyen sQ, angel LP, divino cm, et al. surgery in malig-nant pancreatic neuroendocrine tumors. J surg oncol 2007; 96:397–403.
21. Krampitz GW, Norton Ja, Poultsides Ga, et al. Lymph nodes and survival in pancreatic neuroendocrine tumors. arch surg 2012;147:820–7.
22. Yao Jc, eisner mP, Leary c, et al. Population-based study of islet cell carcinoma. ann surg oncol 2007;14:3492–500.
23. Jensen rT, cadiot G, Brandi mL, et al. eNeTs consensus guidelines for the management of patients with digestive neuroendocrine neoplasms: functional pancreatic endocrine tumor syndromes. Neuroendocrinology 2012;95:98–119.
24. Kulke mh, anthony LB, Bushnell dL, et al. NaNeTs treat-ment guidelines: well-differentiated neuroendocrine tumors of the stomach and pancreas. Pancreas 2010;39:735–52.
25. falconi m, Bartsch dK, eriksson B, et al. eNeTs consensus guidelines for the management of patients with digestive neuroendocrine neoplasms of the digestive system: well-differentiated pancreatic non-functioning tumors. Neuroen-docrinology 2012;95:120–34.
26. sarmiento Jm, heywood G, rubin J, et al. surgical treat-ment of neuroendocrine metastases to the liver: a plea for resection to increase survival. J am coll surg 2003;197: 29–37.
27. sarmiento Jm, Que fG. hepatic surgery for metastases from neuroendocrine tumors. surg oncol clin N am 2003; 12:231–42.
28. cusati d, Zhang L, harmsen We, et al. metastatic nonfunc-tioning pancreatic neuroendocrine carcinoma to the liver: surgical treatment and outcomes. J am coll surg 2012;215: 117–24.
29. o’Toole d, ruszniewski P. chemoembolization and other ablative therapies for liver metastases of gastrointestinal endocrine tumors. Best Pract res clin Gastroenterol 2005;10: 585–94.
30. reddy sK, clary Bm. Neuroendocrine liver metastases. surg clin North am 2012;90:853–61.
31. Karabulut K, akyildiz hY, Lance c, et al. multimodality treatment of neuroendocrine liver metastases. surgery 2011; 150:316–25.
32. akyildiz hY, mitchell J, milas m, et al. Laparoscopic radio-frequency thermal ablation of neuroendocrine hepatic metastases: longterm follow-up. surgery 2010;148:1288–93.
33. amazzaglia PJ, Berber e, milas m, siperstein ae. Laparo-scopic radiofrequency ablation of neuroendocrine liver metastases: a 10-year experience evaluating predictors of survival. surgery 2007;142:10–9.
34. memon K, Lewandowski rJ, mulcahy mr, et al. radioem-bolization for neuroendocrine liver metastases: safety, imaging and longterm outcomes. int J radiat oncol Biol Phys 2012;83:887–94.
35. harring Tr, Nguyen NT, Goss Ja, o’mahoney ca. Treat-ment of liver metastases in patients with neuroendocrine tumors: a comprehensive review. int J hepatol 2011;2011: 154541. doi: 10.4061/2011/154541. [epub 2011 oct 13]
36. Le Treut YP, Gregoire e, Belghiti J, et al. Predictors of long-term survival after liver transplantation for metastatic endocrine tumors: an 85-case french multicenter report. am J Transplant 2008;8:1205–13.
37. Pavel m, Baudin e, couvelard a, et al. eNeTs consensus guidelines for the management of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut, and unknown primary. Neuroen-docrinology 2012;95:157–76.
38. sideris L, dube P, rinke a. antitumor effects of somatosta-tin analogs in neuroendocrine tumors. oncologist 2012;17: 747–55.
39. strosberg J, Kvols L. antiproliferative effect of somatostatin analogs in gastroenteropancreatic neuroendocrine tumors. World J Gastroenterol 2010;16:2963–70.
40. oberg K, eriksson B. The role of interferons in the manage-ment of carcinoid tumors. Br J haematol 1991;79 suppl 1: 74–7.
41. strosberg Jr, coppola d, Klimstra ds, et al. The NaNeTs consensus guidelines for the diagnosis and management of poorly differentiated extrapulmonary neuroendocrine carcinomas. Pancreas 2010;39:799–800.
42. Kouvaraki ma, ajani Ja, hoff P, et al. fluorouracil, doxo-rubicin, and streptozocin in the treatment of patients with locally advanced and metastatic pancreatic endocrine carcinomas. J clin oncol 2004;22:4762–71.
43. strosberg Jr, fine rL, choi J, et al. first line chemotherapy with capecitabine and temozolomide in patients with metastatic pancreatic endocrine carcinomas. cancer 2011; 117:268–75.
44. Yao Jc, shah mh, ito T, et al. everolimus for advanced pancreatic neuroendocrine tumors. N engl J med 2011;364: 514–23.
45. raymond e, dahan L, raoul JL, et al. sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N engl J med 2011;364:501–13.
46. Villard L, romer a, marincek N, et al. cohort study of somatostatin based radiopeptide therapy with 90Y-doTa-Toc versus 09Y-doTa-Toc plus 177Lu-doTa-Toc in neuroendocrine cancers. J clin oncol 2012;30:100–6.

Scientific American Surgery
05/15
gastro neuroendocrine tumors of the pancreas — 14
47. haynes aB, deshpande V, ingkakul T, et al. implications of incidentally discovered, nonfunctioning pancreatic endocrine tumors. arch surg 2011;146:534–9.
48. cheema a, Weber J, strosberg Jr. incidental detection of pancreatic neuroendocrine tumors: an analysis of incidence and outcomes. ann surg oncol 2012;19:2932–6.
49. Lee Lc, Grant cs, salomao dr, et al. small nonfunctioning, asymptomatic pancreatic neuroendocrine tumors (PNeTs): role for nonoperative management. surgery 2012;152: 965–73.
50. Kooby da, Gillespie T, Bentram d, et al. Left sided pancre-atectomy: a multicenter comparison of laparoscopic and open approaches. ann surg 2008;248:438–46.
51. Venkat r, edil Bh, schulick rd, et al. Laparoscopic distal pancreatectomy is associated with significantly less overall morbidity compared to the open technique: a systematic review and meta-analysis. ann surg 2012;255:1048–59.
52. crippa s, Bassi c, salvia r, et al. enucleation of pancreatic neoplasms. Br J surg 2007;94:1254–9.
53. crippa s, Bassi c, Warshaw aL, et al. middle pancreatec-tomy: indications, short- and long-term operative outcomes. ann surg 2007;246:69–76.
54. cauley ce, Pitt ha, Ziegler Km, et al. Pancreatic enucle-ation: improved outcomes compared to resection. J Gastro-intest surg 2012;16:1347–53.
55. hackert T, hinz u, fritz s, et al. enucleation in pancreatic surgery: indications, technique, and outcome compared to standard pancreatic resections. Langenbecks arch surg 2011;396:1197–203.
56. diNorcia J, Lee mK, reavey PL, et al. one hundred thirty resections for pancreatic neuroendocrine tumor: evaluating the impact of minimally invasive and parenchyma sparing techniques. J Gastrointest surg 2010;14:1536–46.
57. crippa s, Zerbi a, Boninsegna L, et al. surgical manage-ment of insulinomas: short and long term outcomes after enucleations and pancreatic resections. arch surg 2012;147: 261–6.
58. cryer Pe, axelrod L, Grossman aB, et al. evaluation and management of adult hypoglycemic disorders: an endo-crine society clinical Practice Guideline. J clin endocrinol metab 2009;94:709–28.
59. doherty Gm, doppman JL, shawker Th, et al. results of a prospective strategy to diagnose, localize, and resect insulinomas. surgery 1991;110:989–96.
60. Nikfarjam m, Warshaw aL, axelrod L, et al. improved con-temporary surgical management of insulinomas: a 25 year
experience at the massachusetts General hospital. ann surg 2008;247:165–72.
61. ellison ec, Johnson Ja. The Zollinger-ellison syndrome: a comprehensive review of historical, scientific, and clinical considerations. curr Prob surg 2009;46:103–6.
62. Berna mJ, hoffman Km, serrano J, et al. serum gastrin in Zollinger ellison syndrome: prospective study of fasting serum gastrin in 309 patients from the National institutes of health and comparison with 2229 cases from the literature. medicine 2006;85:295–330.
63. anlauf m, enosawa T, henopp T, et al. Primary lymph node gastrinoma or occult duodenal microgastrinoma with lymph node metastases in a meN1 patient: the need for a systematic search for the primary tumor. am J surg Pathol 2008;32:1101–5.
64. cisco rm, Norton Ja. surgery for gastrinoma. adv surg 2007;41:165–76.
65. Norton Ja, fraker dL, alexander hr, Jensen rT. Value of surgery in patients with negative imaging and sporadic Zollinger-ellison syndrome, ann surg 2012;256:509–17.
66. Norton Ja, fraker dL, alexander hr, et al. surgery increases survival in patients with gastrinoma. ann surg 2006;244:410–8.
67. Kindmark h, sundin a, Granberg d, et al. endocrine pan-creatic tumors with glucagon hypersecretion: a retrospec-tive study of 23 cases during 20 years. med oncol 2007;24: 330–7.
68. ramage JK, davies ahG, ardill J, et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumors. Gut 2005;54 suppl 4:iv1–16.
69. Garbrecht N, anlauf m, schmitt a, et al. somatostatin producing neuroendocrine tumors of the duodenum and pancreas: incidence types, biologic behavior, association with inherited syndromes, and functional activity. endocr relat cancer 2008;15:229–41.
70. clark oh, ajani J, Benson aB, et al Neuroendocrine tumors. NccN clinical practice guidelines in oncology. J Natl compr canc Netw 2009;7:712–47.
71. Tanaka s, Yamasaki s, matsushita h, et al. duodenal somatostatinoma: a case report and review of 31 cases with special reference to the relationship between tumor size and metastasis. Pathol int 2000;50:146–52.
72. soga J, Yakuwa Y. ViPoma/diarrheogenic syndrome: a sta-tistical evaluation of 241 reported cases. J exp clin cancer res 1998;17:389–400.
73. frucht h, howard Jm, slaff Ji, et al. secretin and calcium provocative tests in the Zollinger-ellison syndrome. a prospective study. ann intern med 1989;111:713–22.