Embed Size (px)
Citation preview

1
Gastrointestinal Pharmacology
Instructor: DR. AARON JACOBS
UHH DNP PROGRAM

Antrum
Body (Corpus)
Stomach
Cells found in Base of Gastric Pits: • Base mucousal cell • Parietal cell • G cell • ECL cell • D cell • Chief cells
Pit Cells: • Surface mucosal cells
Cells found in Isthmus: • Stem cells (pit cell precursors)
Overview of Stomach Cell Types
2
Gastric Pit

Gastric Acidity
Parietal Cells
Cl-
HCO3-
ATP
K+
Na+
K+
ATP
H+
CO2
H2CO3
+ H2O
H+
HCO3-
Cl-
HCl (100 - 150 mM) -log [H+] -log [0.100] = 1 -log [0.150] = 0.8 pH ∼ 0.8-1.0
pH ∼ 7.3
3
Acidity in pH
basolateral
apical

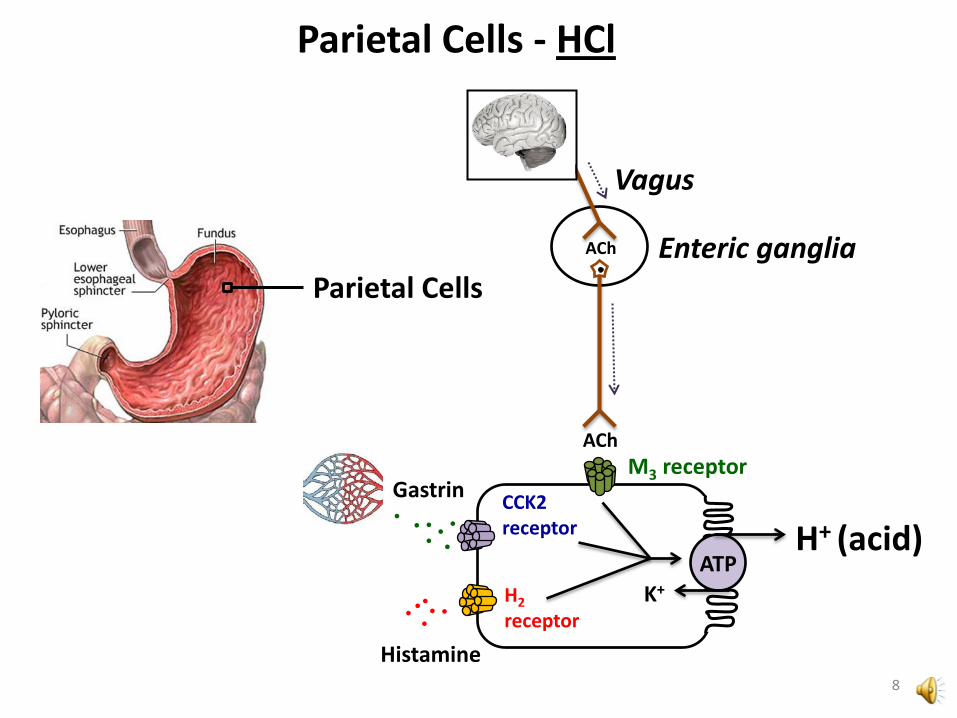
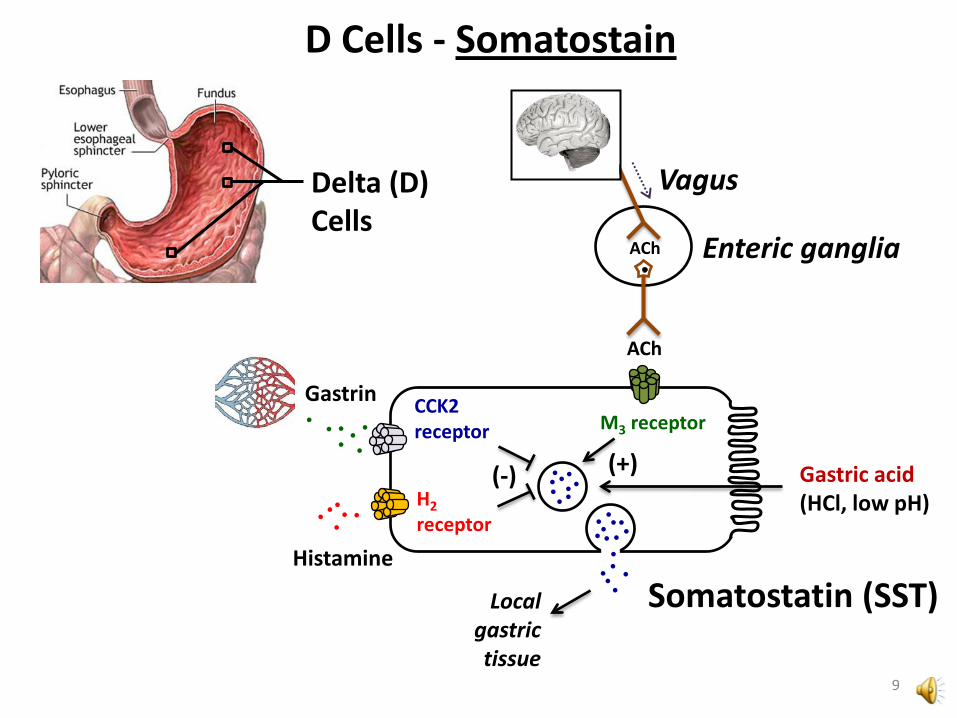
Gastric Acidity FACTORS that REGULATE GASTRIC ACID (HCl) secretion: (+) Stimulate: Endocrine: Gastrin – CCK2 receptor Paracrine: Histamine – H2 receptor Neuronal: Acetylcholine – M3 receptor Nutritional: Amino acids (digested proteins) (-) Inhibit: Endocrine: Somatostatin – SST receptor Chemical: H+
4

Gastric Acidity
Gαs
H2
AC
ATP cAMP
M3
PLC
PIP2 IP3
Gαq Gαq
CCK2
Endoplasmic Reticulum Ca2+
ATP
K+
H+
Histamine (Paracrine)
ACh (Neuronal)
Gastrin (Endocrine)
AC = adenylate cyclase PLC = phospholipase C 5
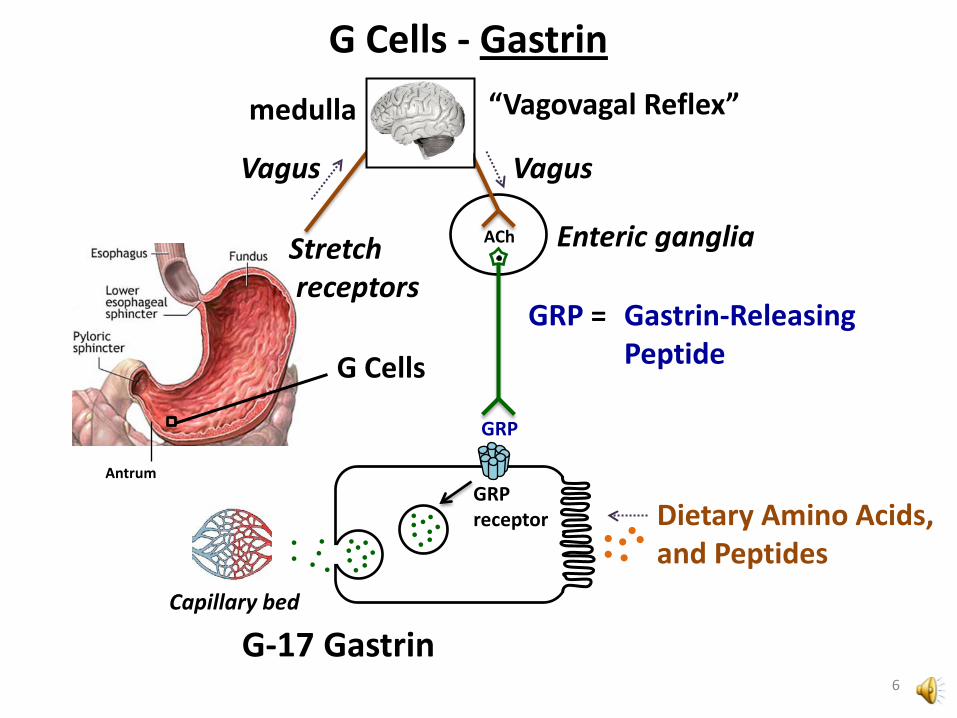
G Cells - Gastrin
G Cells
Antrum
Vagus
ACh
GRP
GRP receptor
G-17 Gastrin
Enteric ganglia
GRP = Gastrin-Releasing Peptide
Vagus
Capillary bed
Dietary Amino Acids, and Peptides
Stretch receptors
6
“Vagovagal Reflex” medulla

CCK2 receptor
Enterochromaffin- like (ECL) Cells
Body
Gastrin
Vagus
ACh
ACh
Enteric ganglia
M3 receptor
Histamine Local
tissues
ECL Cells - Histamine
7
CCK2 receptor
Gastrin
Vagus
ACh
ACh
Enteric ganglia
M3 receptor
Parietal Cells - HCl
Parietal Cells
H2 receptor
Histamine
ATP H+ (acid)
K+
8
CCK2 receptor
D Cells - Somatostain
Delta (D) Cells
H2 receptor
Gastrin
Histamine
Vagus
ACh
ACh
Enteric ganglia
M3 receptor
(-) (+)
Somatostatin (SST)
Gastric acid (HCl, low pH)
Local gastric tissue
9
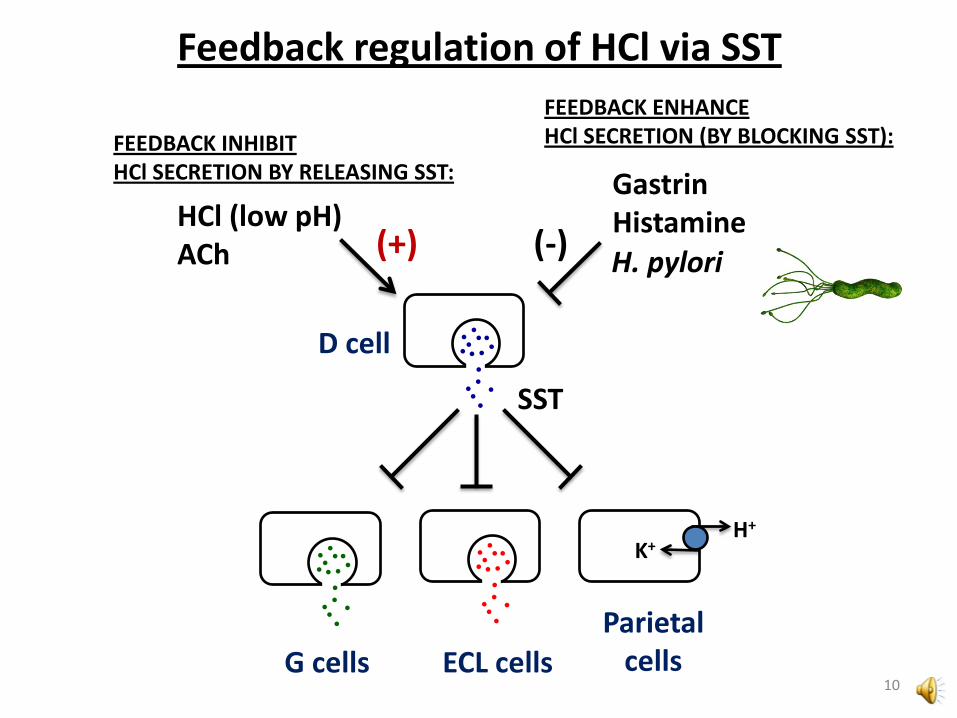
Feedback regulation of HCl via SST
D cell
SST
G cells ECL cells
H+
K+
Parietal cells
10
(-) H. pylori
FEEDBACK ENHANCE HCl SECRETION (BY BLOCKING SST):
Gastrin Histamine HCl (low pH)
ACh (+)
FEEDBACK INHIBIT HCl SECRETION BY RELEASING SST:

Defenses Against Acid
Protects esophagus from gastric acid reflux
Gastric mucus • Secreted primarily by surface mucous cells (pit cells) • Coats the mucosal surface of the stomach • Slows (H+) diffusion • Prevents damage by proteases (e.g. pepsin) • Consists of water + salts + mucins:
Branched sugars
Protein backbone 11
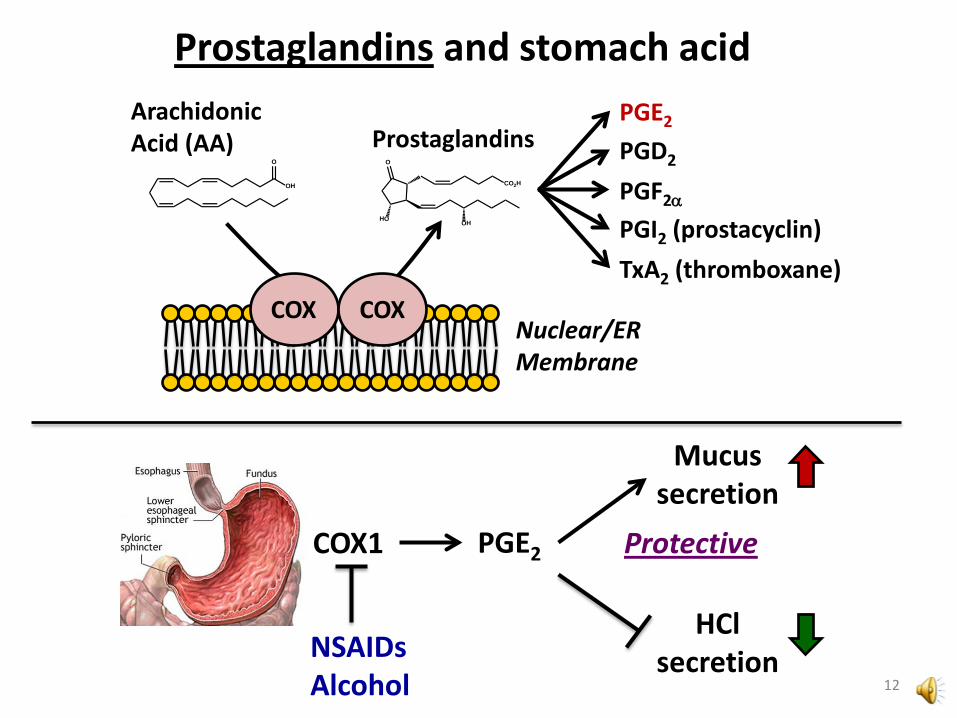
Prostaglandins and stomach acid
Prostaglandins O
HO
CO2H
OH
Nuclear/ER Membrane
COX COX
Arachidonic Acid (AA)
O
OH
PGE2
PGD2
PGF2α
PGI2 (prostacyclin)
TxA2 (thromboxane)
NSAIDs Alcohol
Mucus secretion
HCl secretion
COX1 PGE2 Protective
12
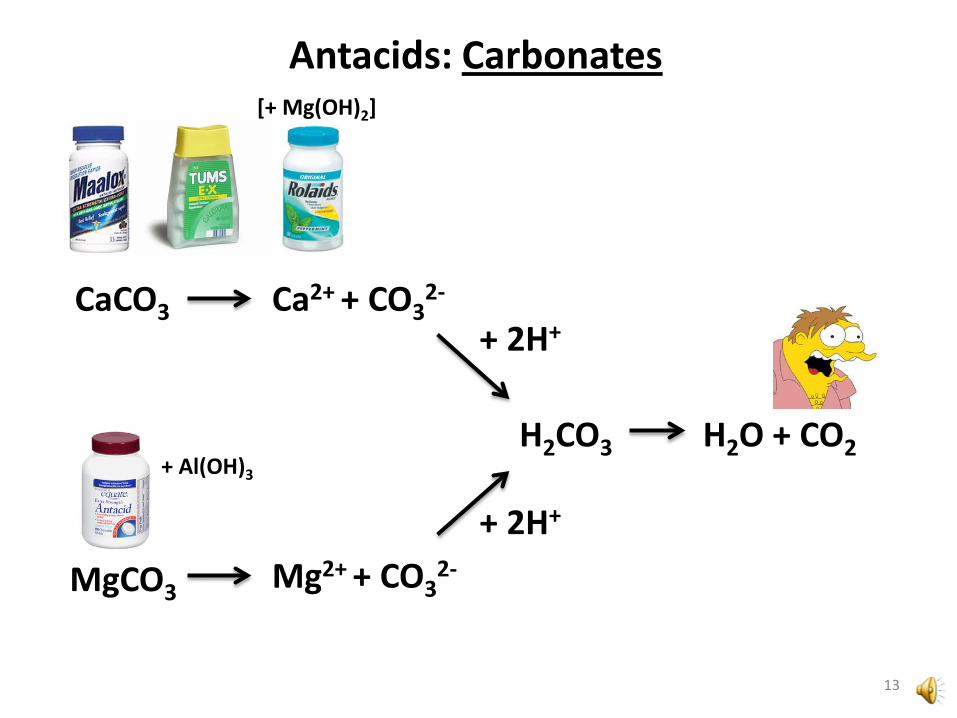
CaCO3 Ca2+ + CO32-
+ 2H+
H2CO3 H2O + CO2
Antacids: Carbonates
MgCO3 Mg2+ + CO32-
+ 2H+
[+ Mg(OH)2]
+ Al(OH)3
13

Al(OH)3 Mg(OH)2
+ 2H+ + 3H+
3 H2O 2 H2O
Mg2+ + 2 OH-
fast
Al3+ + 3 OH-
slow
Combinations Mg(OH)2 + Al(OH)3 provide quick onset and sustained action
Magaldrate = [Al3+][Mg2+]2[OH-]7[H2O] EU, Mexico, South America (Riopan®)
low pH Mg(OH)2 + Al(OH)3
14
Antacids: Hydroxides
NON-US COMBINATION:

Antacids – Acid Neutralization
Converting between H+ conc. and pH pH ∼ -log[H+] [H+] ∼ 10-pH
If pH 1.0; [H+] ∼ 10-1 = 0.1 mol/L If pH 2.0; [H+] ∼ 10-2 = 0.01 mol/L If pH 3.0; [H+] ∼ 10-3 = 0.001 mol/L
• Raising pH by 1 unit removes 90% of acid • Raising pH by 2 units removes 99% of acid
15
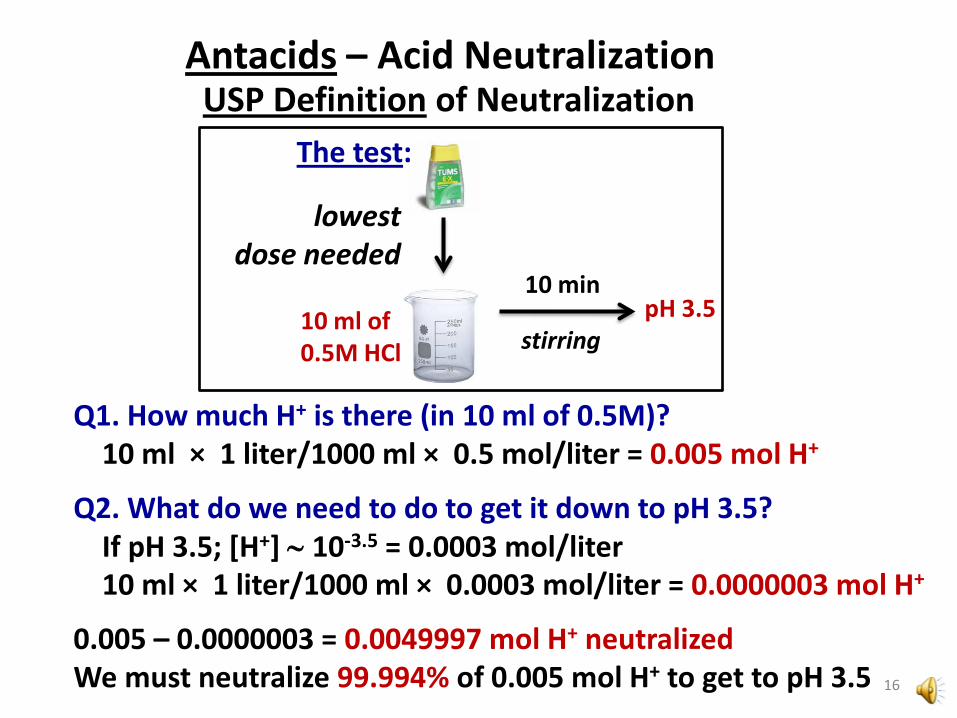
Antacids – Acid Neutralization USP Definition of Neutralization
lowest dose needed
10 ml of 0.5M HCl
Q1. How much H+ is there (in 10 ml of 0.5M)? 10 ml × 1 liter/1000 ml × 0.5 mol/liter = 0.005 mol H+
Q2. What do we need to do to get it down to pH 3.5? If pH 3.5; [H+] ∼ 10-3.5 = 0.0003 mol/liter 10 ml × 1 liter/1000 ml × 0.0003 mol/liter = 0.0000003 mol H+
0.005 – 0.0000003 = 0.0049997 mol H+ neutralized We must neutralize 99.994% of 0.005 mol H+ to get to pH 3.5
10 min
stirring pH 3.5
The test:
16

Antacids – Absorption Sodium bicarbonate (NaHCO3)
• Rapidly and completely absorbed • Sodium intake may adversely affect patients with blood pressure or cardiac conditions • Alkali intake may raise blood pH in patients with renal failure
Calcium carbonate (CaCO3) • Ca2+ absorption is about 15% of dose • Not important UNLESS renal failure or large doses taken with other Ca2+ sources (milk-alkalai syndrome – next slide)
Aluminum hydroxide (Al(OH)3) Magnesium hydroxide (Mg(OH)2)
• Poorly absorbed • Multivalent cations - can chelate some drugs • Increase in Al3+ risk to patients with renal failure
• Osteodystrophy • Encephalopathies (e.g. Alzheimer’s)
17

Antacids – Adverse Effects
CaCO3 • Bloating, belching • Modest elevation of urine pH (~1 unit) • Ca2+ can accumulate in patients with renal failure • Potential toxicity if high doses combined with
milk or calcium supplements (milk-alkalai syndrome) “Sippy diet” – 1920’s – 1950’s Hypercalcemia (cramps; constipation; kidney stones; renal insufficiency; confusion)
Mg(OH)2
Al(OH)3
laxative effect
slows GI motility (constipation)
18
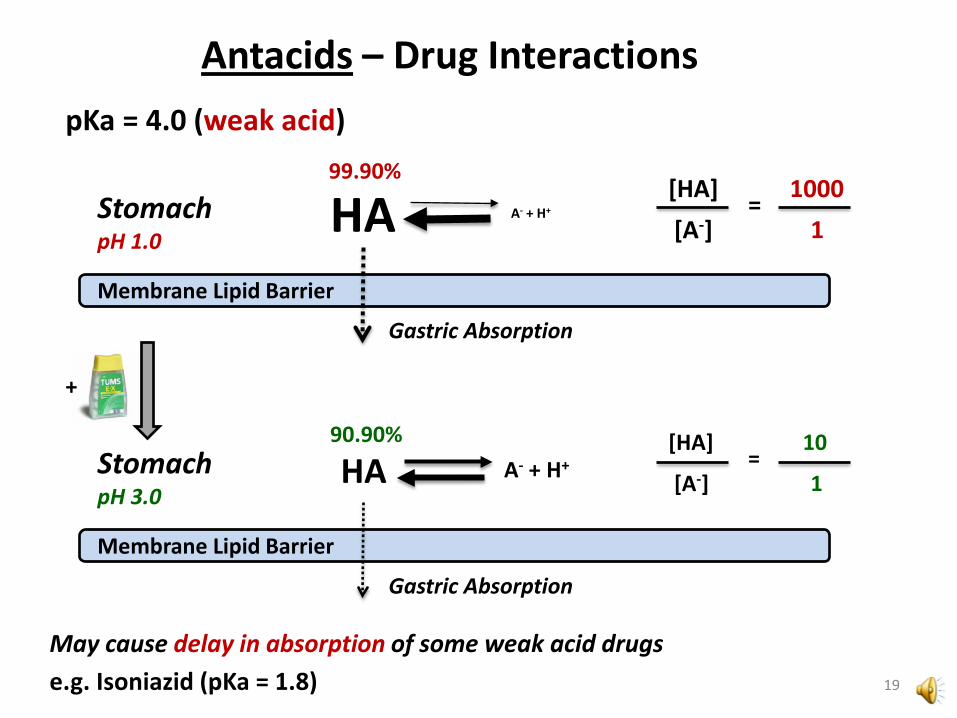
Antacids – Drug Interactions
Membrane Lipid Barrier
Stomach pH 1.0
pKa = 4.0 (weak acid)
[HA] [A-]
= 1000 1
Membrane Lipid Barrier
[HA]
[A-] =
10
1
+
Stomach pH 3.0
HA A- + H+
Gastric Absorption
99.90%
HA A- + H+
Gastric Absorption
90.90%
May cause delay in absorption of some weak acid drugs e.g. Isoniazid (pKa = 1.8) 19
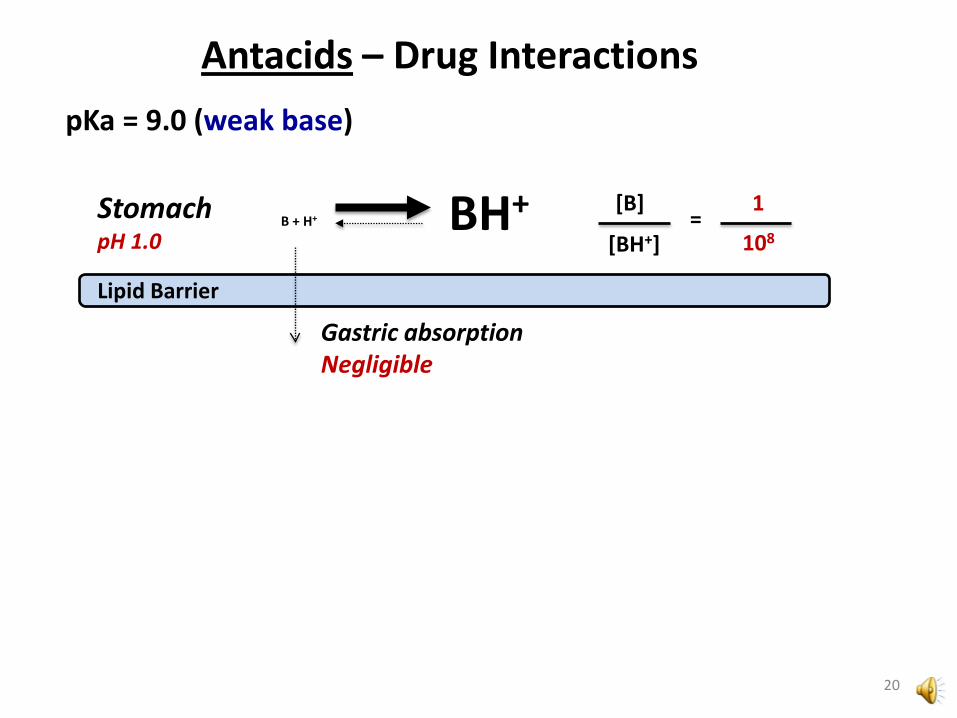
Antacids – Drug Interactions
Lipid Barrier
Stomach pH 1.0
pKa = 9.0 (weak base)
[B]
[BH+] =
108
1 BH+ B + H+
Gastric absorption Negligible
20

Antacids – Drug Interactions
Iron solubility
Fe3+ Fe2+
Gastric pH after antacids
Acidic pH Basic pH
• low ferric iron solubility • reduced iron absorption
21
most dietary iron

Mg2+ Al3+ Chelation by Multivalent Cations
• Fluoroquinolone antibiotics • Tetracycline antibiotics • Ketoconazole (antifungal) • Most Bisphosphonates (except: Pamidronate; Zoledronic Acid)
Antacids – Drug Interactions
Reduced absorption
22

Anti-flatulents
Simethicone • Silica-based (siloxane) surfactant • Anti-foaming agent • Not absorbed • Decreases surface tension of gas bubbles • Prevents formation of gas pockets • Makes gas easier to “pass” • Often in antacid combinations • Or sold alone (e.g. Gas-X®; Phazyme®)
Got gas?
23

Prostaglandin Analog: Misoprostol
EP3
Misoprostol (Cytotec®) PGE1 analog
luminal membrane
basolateral membrane
INCREASED MUCUS secretion 24
AC
ATP cAMP
ATP
K+
H+
DECREASED H+ secretion
Gαi
EP4
PARIETAL CELL
STOMACH LUMEN

Prostaglandin Analog: Misoprostol
• Absorption: Rapid, complete • Metabolism: Rapidly de-esterified to misoprotol acid
(active metabolite) • Serum half-life of misoprostol acid 20-40 min • Duration of action: up to 3 hr • Excretion: Urine (mainly as misoprostol acid)
Pharmacokinetics
Adverse Effects
• Diarrhea – 30% of patients (self-resolving) • Worsening of Inflammatory Bowel Disease (IBD) • Uterine Contractions – contraindicated in pregnancy
Misoprostol is used in combination with mifepristone (RU-486) for pregnancy termination
25

Sucralfate Sucralfate (Carafate®)
• Slimy, cross-linked polymer • Not absorbed by GI tract • Binds to and coats ulcerated tissues • Buffer against excessive H+
• Absorbs BILE SALTS • Useful for duodenal ulcers (caused by bile salts)
“SUCRose-ALuminium-sulFATE complex”
+ Gastric Acid (HCl)
Drug interactions – may limit other drug bioavailability Adverse effects - few – constipation (2%)
26
Tablet or Suspension

Proton Pump Inhibitors Omeprazole (Prilosec®; Rapinex®; Zegerid®) – racemic Esomeprazole (Nexium®) – S-enantiomer of omeprazole Lansoprazole (Prevacid®) Rabeprazole (Aciphex®) Pantoprazole (Protonix®) Dexlansoprazole (Dexilant®, formerly Kapidex®)
First Approved Drug: Omeprazole (1989) Newest Drug: Dexlansoprazole (2009)
27
Administration: ORAL:
• All IV Injection:
• Esomeprazole • Pantoprazole

Proton Pump Inhibitors
Proton pump P-type ATPase
cytoplasmic ATPase domain
ATP
ADP + Pi
transmembrane pump domain
Cys - SH
PPI (benzimidazole)
active metabolite (cyclic sulfenamide)
[H+] H+ Parietal cells
• Forms covalent bond with Cysteine (Cys813)
Mechanism
28

Ca2+ ATPase Na+/K+ ATPase
OTHER P-type ATPases
Cys - SH Cysteine is too hindered in these types of ATPases to be reactive with PPIs
Proton Pump Inhibitors
• Not affected by PPIs
29

PPI [H+]
Active metabolite “off target” reactions; drug degradation in stomach
Active metabolite (cyclic sulfenamide)
[H+] in
parietal cells
specific inhibition of proton pump
Proton Pump Inhibitors Stability
1. Enteric coating – Intestinal absorption a. enteric coated drug inside gel cap b. enteric coated powder for suspension c. enteric coated tablet
2. Co-administration with bicarbonate (raises pH of stomach, inhibits degradation)
3. Intravenous administration (if oral route unavailable – only some PPIs)
30
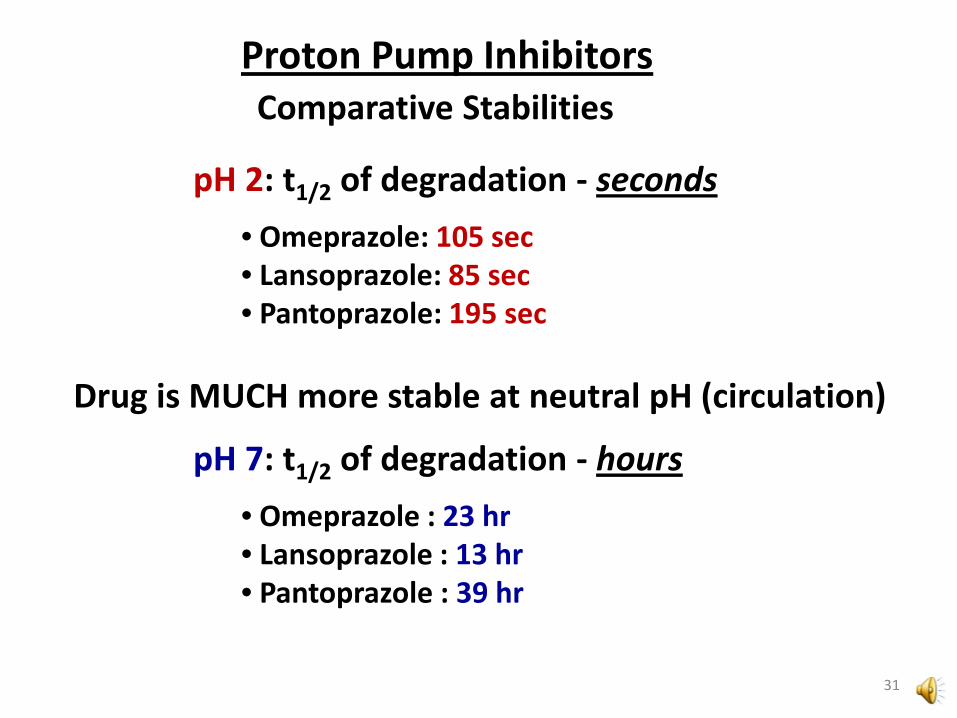
pH 2: t1/2 of degradation - seconds • Omeprazole: 105 sec • Lansoprazole: 85 sec • Pantoprazole: 195 sec
Proton Pump Inhibitors Comparative Stabilities
31
Drug is MUCH more stable at neutral pH (circulation)
pH 7: t1/2 of degradation - hours • Omeprazole : 23 hr • Lansoprazole : 13 hr • Pantoprazole : 39 hr
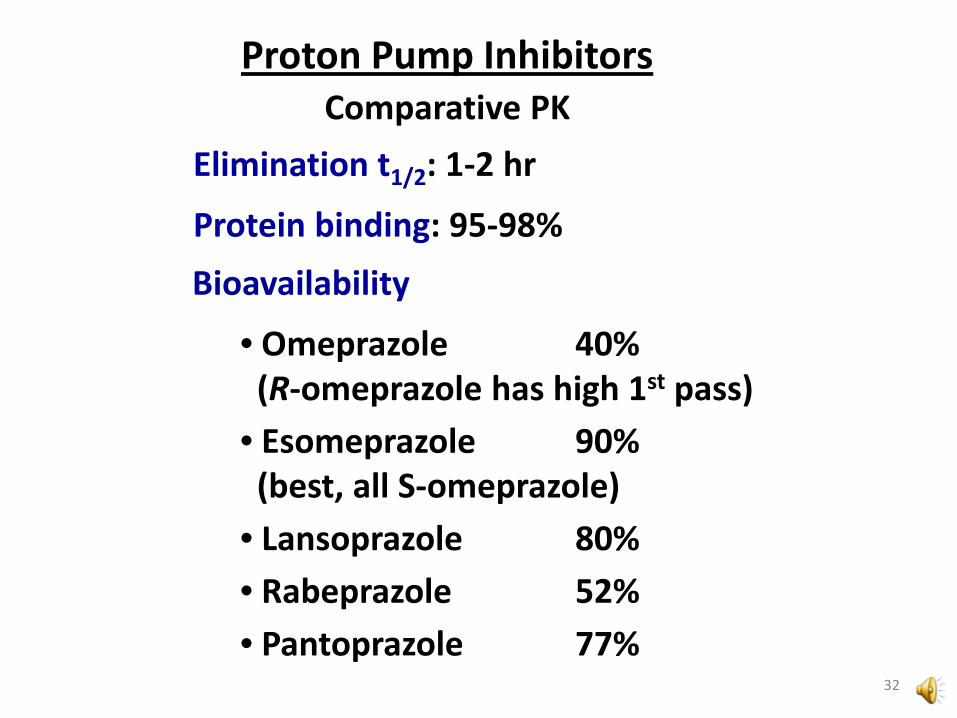
Proton Pump Inhibitors Comparative PK
Bioavailability
• Omeprazole 40% (R-omeprazole has high 1st pass) • Esomeprazole 90% (best, all S-omeprazole) • Lansoprazole 80% • Rabeprazole 52% • Pantoprazole 77%
Elimination t1/2: 1-2 hr
Protein binding: 95-98%
32

Proton Pump Inhibitors Metabolism
Proton pump inhibitors Eliminated by Phase I reactions CYP2C19 (major pathway) CYP3A4 (minor; except for esomeprazole, 30%) Pantoprazole also undergoes Phase II metabolic reactions (conjugation)
33

34
Proton Pump Inhibitors Patenting
S-omeprazole patent method = “Chiral Switching”
R-omeprazole + S-omeprazole
same active product at acid pH
(cyclic sulfenamide)
Prilosec® Patent protection 1989 – 2001
Nexium® Patent protection 2001 – 2014 (2010 sales: #2, $6.3 Bil) Teva will begin making generics in 2014 by license
If it’s the same active metabolite, what DID they patent?

65% 30% 95%
Proton Pump Inhibitors
Omeprazole 50% R-omeprazole + 50% S-omeprazole
Metabolism
CYP2C19 CYP2C19 CYP3A4
R-omeprazole is more Rapidly AND more Extensively metabolized by CYP2C19 than S-omeprazole (esomeprazole)
35
RAPID

Poor Metabolizers (CYP2C19) • Caucasian: 3-5% • Asian: 10-15% • Melanesians*: 40-80%
*Pharmacogenetics 9(5):581-590 (1999) higher risk of side effects?
high AUC for R-omeprazole
AstraZeneca – switching to pure S-enantiomer should eliminate some of this variability (since it is about 30% metabolized by CYP3A4)
36
Proton Pump Inhibitors Metabolism

European Journal of Clinincal Pharmacology 60: 779–784 (2005)
Proton Pump Inhibitors Patenting
t1/2 for duration of action ∼ 15 hr
Is vs clinically significant? Where are the error bars?
Publication by AstraZeneca
37
TWELVE SUBJECTS
Proton Pump Inhibitors
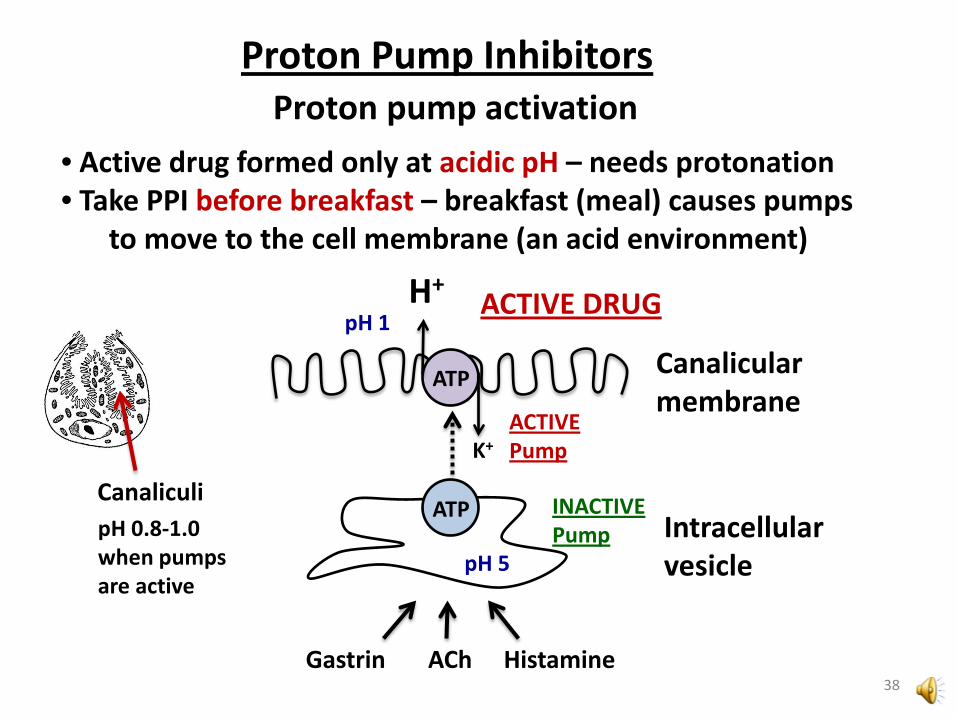
ATP
K+
H+
ATP
pH 5
pH 1
Canalicular membrane
Intracellular vesicle
ACTIVE Pump
INACTIVE Pump
Gastrin ACh Histamine
• Active drug formed only at acidic pH – needs protonation • Take PPI before breakfast – breakfast (meal) causes pumps
to move to the cell membrane (an acid environment)
Proton pump activation
Canaliculi pH 0.8-1.0 when pumps are active
38
ACTIVE DRUG

Proton Pump Inhibitors Drug duration / Recovery
Duration of action ∼ 15 hr
Elimination t1/2 for PPI’s: 1-2 hr Does PPI elimination rate influence duration of action?
• Not significantly What property mainly determines duration of action?
• “Recovery” of proton pumps
39

Proton Pump Inhibitors
Cys – S – S – Drug
ATP
INHIBITED PUMP
1. Protein turnover
Protein degradation
ATP
K+
H+
ATP
New protein synthesis and activation
t1/2 for proton pump TURNOVER ∼ 48 hr But t1/2 for recovery of HCl secretion ∼ 15 hr
40 There MUST be another way to recover...
Recovery
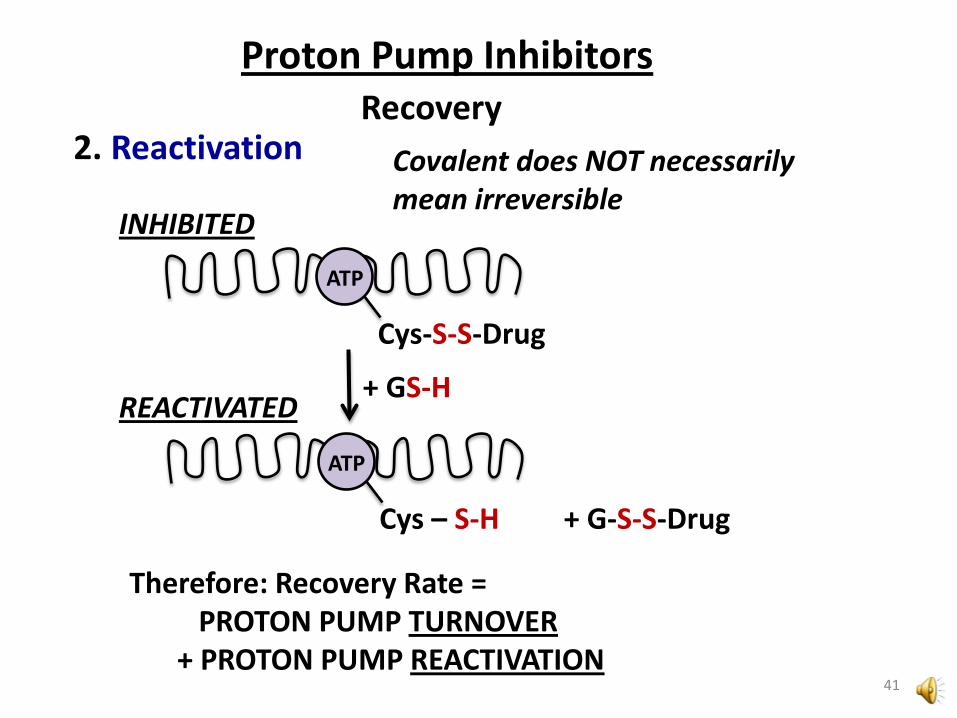
Proton Pump Inhibitors
Cys-S-S-Drug
ATP
INHIBITED
Cys – S-H + G-S-S-Drug
ATP
REACTIVATED + GS-H
2. Reactivation
41
Therefore: Recovery Rate = PROTON PUMP TURNOVER + PROTON PUMP REACTIVATION
Covalent does NOT necessarily mean irreversible
Recovery

Proton Pump Inhibitors Adverse Effects
Adverse effects – FEW: • Nausea, cramps, flatulence, constipation or diarrhea • LONG-TERM use may cause LOW Mg++ levels • LONG-TERM use may cause excessive gastrin secretion (Hypergastrinemia) – 5-10% of chronic users
• Causes REBOUND acidity upon discontinuation • Associated with ECL cell hyperplasia in lab animals • Gastric carcinomas? • Data do not suggest cancer link in human studies (30 years)
42

active drug
Platelet aggregation
(clotting)
Proton Pump Inhibitors Drug Interactions
PPIs: MINOR inhibition of CYP2C19 Clearance of diazepam, disulfiram, phenytoin, warfarin (+ other CYP2C19 substrates) is REDUCED
Lansoprazole: MINOR induction of CYP1A2 isoform Clearance of theophylline, caffeine, imipramine (+ other CYP1A2 substrates) is INCREASED
Clopidogrel (Plavix®) prodrug
CYP2C19
PPIs
43

H2 Receptor Antagonists
Cimetidine (Tagamet®) Ranitidine (Zantac®) Famotidine (Pepcid®) Nizatidine (Axid®)
First Approved Drug: Cimetidine (1979) Newest Drug: Nizatidine (1988)
44
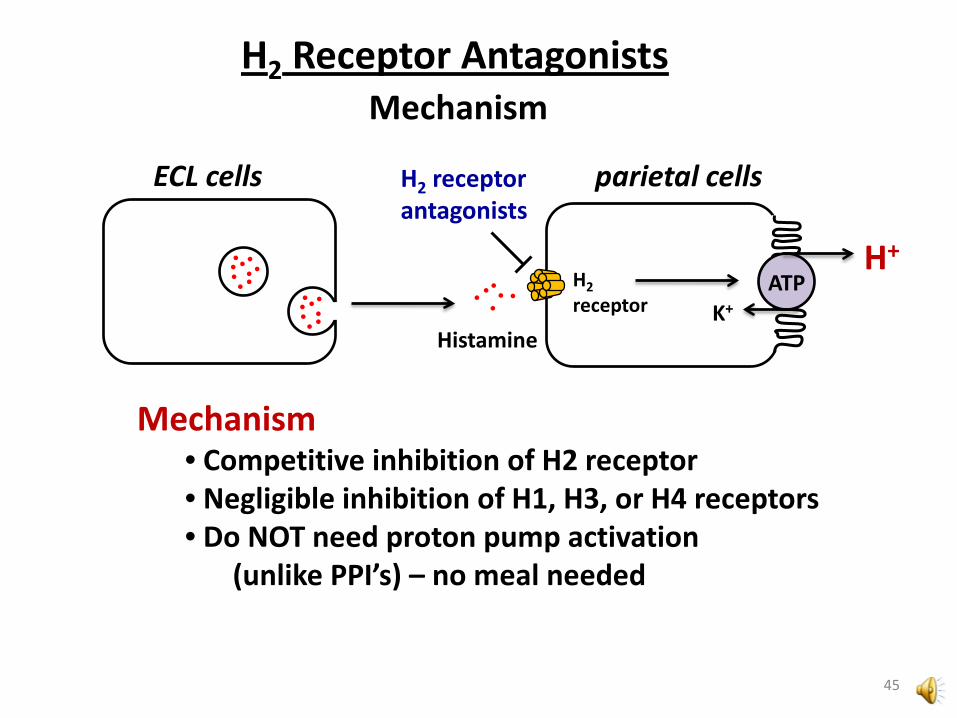
H2 Receptor Antagonists Mechanism
H2 receptor
ATP H+
K+
H2 receptor antagonists
parietal cells
Histamine
ECL cells
Mechanism • Competitive inhibition of H2 receptor • Negligible inhibition of H1, H3, or H4 receptors • Do NOT need proton pump activation
(unlike PPI’s) – no meal needed
45
Efficacies - Similar, suppress 24 hr gastric acid secretion by only ∼70% (compared to >99% by PPIs!) Duration of Action - up to 12 hr (depending on agent, dose, route) Relative Potencies Famotidine >> Nizatidine, Ranitidine > Cimetidine most potent least potent
H2 Receptor Antagonists Comparisons
46

H2 Receptor Antagonists
Cimetidine: MULTIPLE P450 inhibitor (CYP isoforms: 1A2; 3A4; 2D6; 2C19)
INCREASES levels of the following drugs: • Warfarin • Cisapride (Propulsid®) – prokinetic agent • Phenytoin • Certain beta blockers (e.g. Propranolol) • Certain calcium channel blockers (e.g. Nifedipine) • Diazepam (+ other benzodiazepines) • Clozapine • Theophylline
May DECREASE the activation of tamoxifen
Drug Interactions
47

H2 Receptor Antagonists Mechanism
H2 receptor antagonists useful for nighttime heartburn – why?
• BASAL gastric HCl production Histamine-mediated • BREAKTHROUGH (nighttime) heartburn sometimes occurs with PPIs • Do NOT need “activation” of proton pumps to work • Tolerated in combination with PPIs
48

H2 Receptor Antagonists Adverse Effects
H1
• Awakeness, diurnal cycle • Intestinal motility (diarrhea) • Rash (pruritus) • Bronchoconstriction • Nausea
H3
• Inhibitory CNS autoreceptors
H4
• Mast cell chemotaxis (asthma, allergy)
Because they are H2 specific these agents do NOT cause the side effects of other H-receptor antagonists (nonspecific antihistamines cause sedation, constipation, inhibit nausea)
49
Other Roles for H2-Receptors • Increased gastric motility • Relaxation of smooth muscle (airway and vascular) • Increased contraction (rate and force) cardiac muscle • Inhibition of immune responses
Am J Physiol Gastrointest Liver Physiol 273:987-996 (1997)
H2-Related side-effects?
• Not significant
H2 Receptor Antagonists Adverse Effects
50

Adverse Effects Adverse effects (usually well tolerated)
• Headache, drowsiness, fatigue, muscular pain, constipation or diarrhea are most common
• Cimetidine: • Mental effects in elderly (confusion) • Competes with creatinine for clearance,
giving an “ILLUSION” of renal insufficiency • Long term use at HIGH DOSES:
• Antagonism of androgen receptor • Increased estradiol levels • Causes galactorrhea in women,
gynecomastia and infertility in men
H2 Receptor Antagonists
51
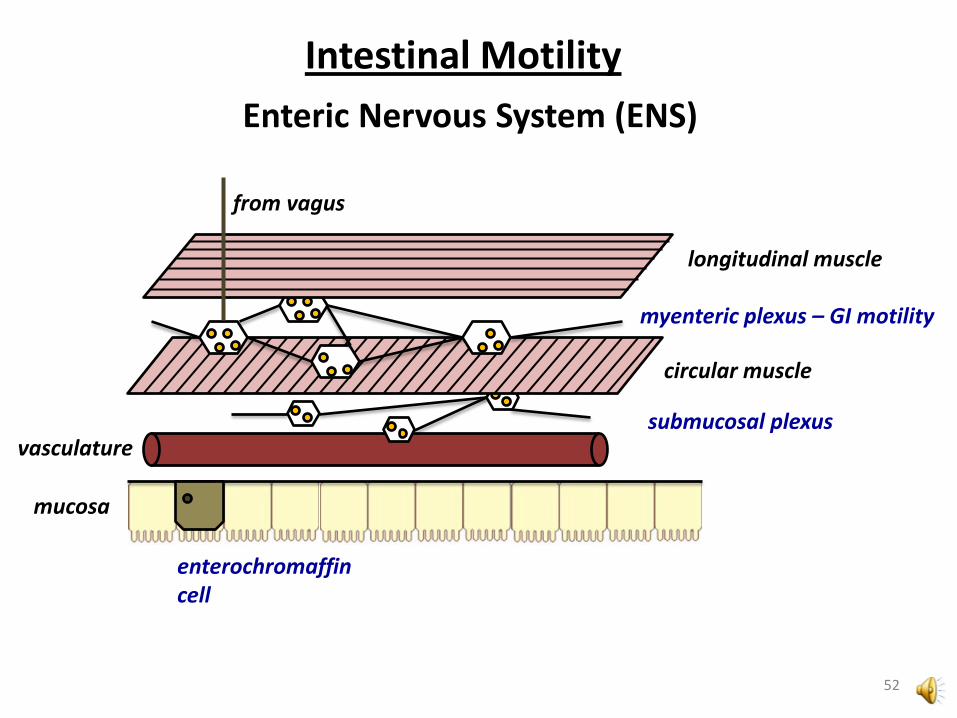
mucosa
circular muscle
longitudinal muscle
vasculature submucosal plexus
myenteric plexus – GI motility
Enteric Nervous System (ENS)
enterochromaffin cell
Intestinal Motility
from vagus
52

5-HT (serotonin)
NO = nitric oxide VIP = vasoactive intestinal peptide
Enterochromaffin Cell
Myenteric plexus
contraction
relaxation
MOVEMENT
Intestinal Motility
circular muscle
(-) NO, ATP, VIP
INHIBITORY (+) ACh
EXCITATORY
53
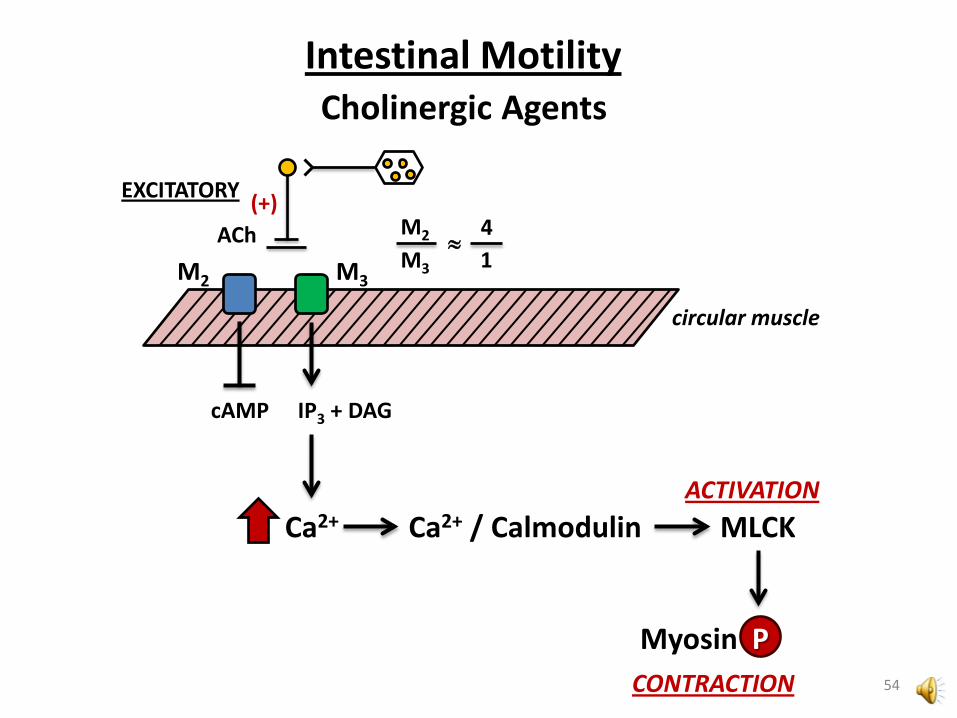
Intestinal Motility Cholinergic Agents
circular muscle
(+) ACh
EXCITATORY M2
M3
4 1
≈ M2
cAMP
M3
IP3 + DAG
Ca2+ Ca2+ / Calmodulin
Myosin P CONTRACTION
MLCK ACTIVATION
54
Why isn’t ACh used to promote intestinal motility? • Cholinesterases • Multiple receptor subtypes (side effects)
Example: Bethanechol (Urecholine®) (unlabeled use for GERD) NOT an AChE substrate But DOES cause CHOLNIERGIC adverse effects:
• Bradycardia • Hypotension / reflex tachycardia • Diarrhea • Salivation • Bronchoconstriction • Blurred vision
55
Intestinal Motility Cholinergic Agents

ACh
Choline + Acetate
Acetylcholinesterase (AChE) Butyrylcholinesterase (BuChE)
Neostigmine (Prostigmin®)
Also causes CHOLINERGIC adverse effects
56
Intestinal Motility Cholinergic Agents
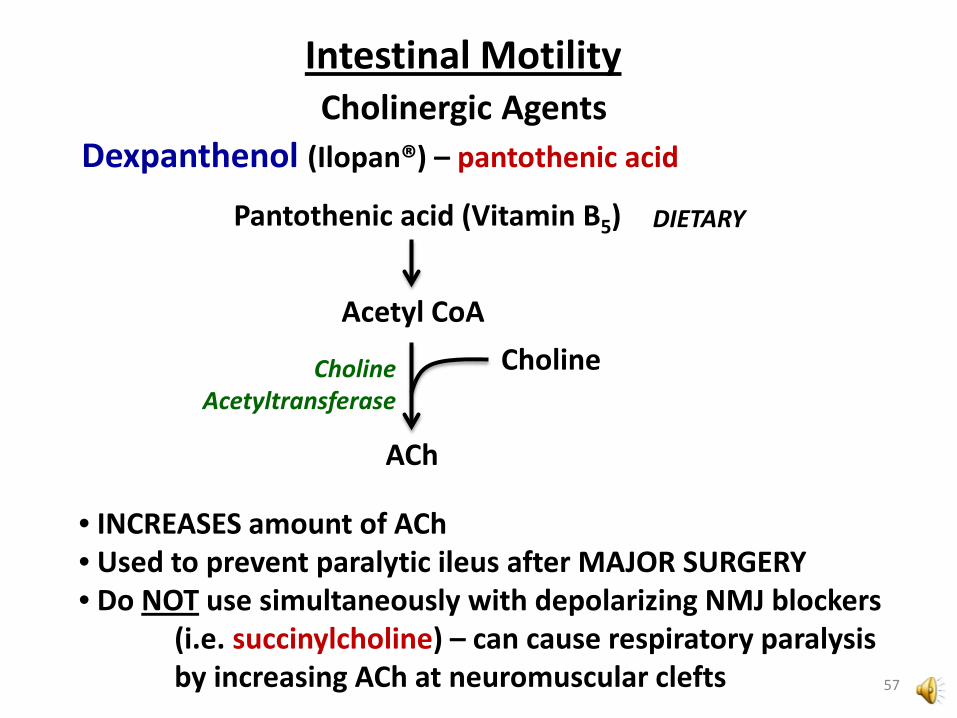
Dexpanthenol (Ilopan®) – pantothenic acid
Choline Choline Acetyltransferase
ACh
Pantothenic acid (Vitamin B5)
Acetyl CoA
DIETARY
• INCREASES amount of ACh • Used to prevent paralytic ileus after MAJOR SURGERY • Do NOT use simultaneously with depolarizing NMJ blockers (i.e. succinylcholine) – can cause respiratory paralysis by increasing ACh at neuromuscular clefts 57
Intestinal Motility Cholinergic Agents
Intestinal Motility Prokinetic Agents
Metoclopramide (Reglan®)
MECHANISM of ACTION: complex Dopaminergic: ANTAGONIST of D2 receptors* ,♦ Serotonergic: Antagonist of 5-HT3 receptors ♦ Agonist of 5-HT4 receptors ♦ Cholinergic: Sensitization of M3 receptors* * GI motility effect ♦ Antiemetic effect
58

CONTRACTION
D2
M3
Dopaminergic neuron
Cholinergic neuron
ACh ACh ACh (+) EXCITATORY
DA DA
DA
INHIBITORY (-)
Metoclopramide
Metoclopramide
59
Intestinal Motility Prokinetic Agents

Metoclopramide
Fourth ventricle
Chemoreceptor trigger zone (CTZ) (area postrema)
Vomiting center (medulla)
5-HT3 (+) H1 (+) M1 (+) NK1 (+)
Duodenal distension, irritation
VOMITING NAUSEA
Receptor effect on vomiting: (+) stimulates (-) inhibits
5-HT3 (+) 5-HT4 (-) NK1 (+)
D2 (+) 5-HT3 (+) MOR (+)
MOR = Mu opioid receptor NK1 = Neurokinin 1 receptor
H1 (+) M1 (+) Inner ear
60
Intestinal Motility Prokinetic Agents
Metoclopramide EFFECTS:
• INCREASES: • lower esophageal sphincter tone • gastric contractions (faster emptying) • intestinal motility (peristalsis)
• NO EFFECT on GI secretions • INHIBITS vomiting and nausea
61
Intestinal Motility Prokinetic Agents

Metoclopramide • Onset of action: Oral: 30-60 min IM: 10-15 min IV: 1-3 min • Duration of action: 1-2 hr (regardless of route) • Absorption: Rapid, 60-95% • DOES CROSS BBB • Excretion: Urine
Adverse Effects (CNS)
Pharmacokinetics
• Drowsiness • Akathesia • Extrapyramidal effects (dystonias) – movement disorder (after months – years of therapy) Tardive dyskinesia – potentially irreversible 62
Intestinal Motility Prokinetic Agents

Hypothalamus
Pituitary
DA
Prolactin
DOPAMINE a.k.a. Prolactin Inhibitory Factor (PIF)
Metoclopramide
Adverse Effects
• Galactorrhea, Gynecomastia
Lactation
63
Intestinal Motility Prokinetic Agents

Domperidone (Motilium®) – Clinical trials (Jannsen)
• SELECTIVE D2 Antagonist
• Administration: Oral, Rectal, IV • Does NOT cross BBB:
• Does NOT cause extrapyramidal side effects of D2 • Still inhibits nausea/vomiting (CTZ lacks BBB) • Still enhances prolactin release (Anterior pituitary lacks BBB)
Adverse effects (most common): • Gynecomastia, lactation
Adverse effects (rare but dangerous) • Hypernatremia – anecdotal, idiopathic • QTc prolongation (don’t combine w/QTc enhancing drugs)
64
Intestinal Motility Prokinetic Agents
Tegaserod (Zelnorm®) – Emergency approval
Use: IBS-related constipation in females
Mechanism of action: partial 5-HT4 AGONIST Effects:
• Stimulates GI motility (esophagus to ascending colon) • Stimulates Cl- secretion (draws Na+ and H2O into lumen)
Pharmacokinetics • Administration: ORAL • Absorption: VERY POOR • Bioavailability: 10% • Excretion: FECES, mainly UNCHANGED
65
Intestinal Motility Prokinetic Agents
Cisapride (Propulsid®) – limited access protocol in US
5-HT4 agonist Withdrawn from US market (2000) Adverse effect: QTc prolongation Effect on hERG channel (KIR)
66
Intestinal Motility Prokinetic Agents

Prucalopride – phase III trials
• Advertized as “differs structurally from other serotonergic prokinetic agents” ..But actually shares very similar structural motifs • Data suggest it does NOT cause QTc prolongation
67
Intestinal Motility Prokinetic Agents

Intestinal Water Flux
from Goodman and Gilman (2006)
stool = 70-85% water
Constipation • Delayed motility • Enhanced water uptake • Dehydration
Water Flux • 2 liters: dietary • 7 liters: secretions
68
Diarrhea • Enhanced motility • Osmotic (pulling water into bowel) • Secretory (secreting water into bowel) • Inflammatory / Infection
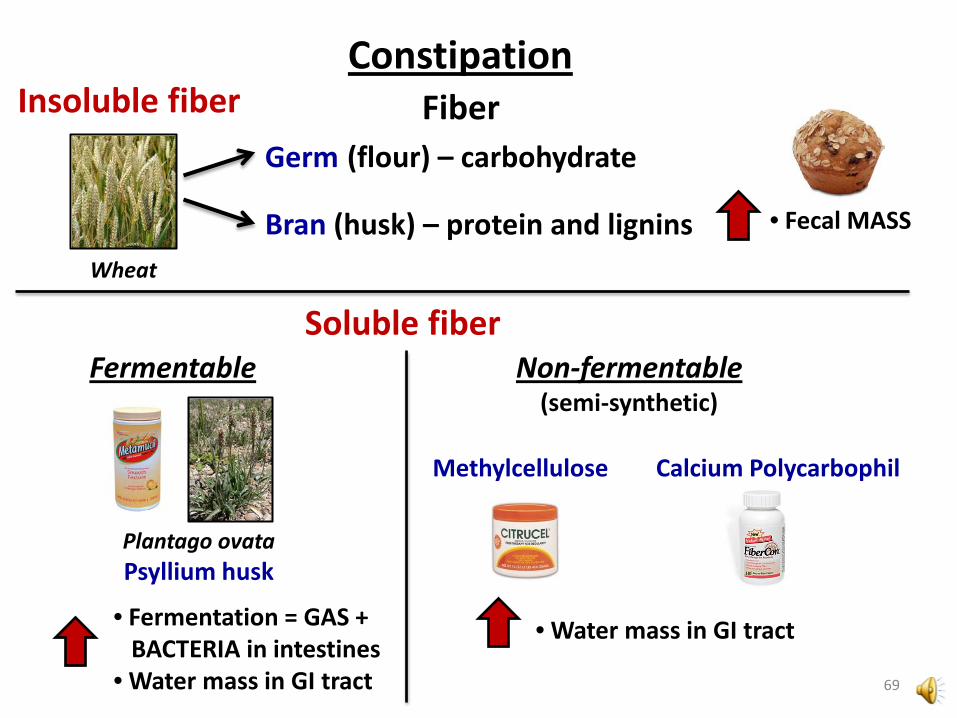
Wheat
Germ (flour) – carbohydrate
Bran (husk) – protein and lignins
• Fermentation = GAS + BACTERIA in intestines • Water mass in GI tract
Constipation Fiber
Plantago ovata Psyllium husk
• Fecal MASS
Insoluble fiber
Soluble fiber Non-fermentable
(semi-synthetic) Fermentable
• Water mass in GI tract
Methylcellulose Calcium Polycarbophil
69
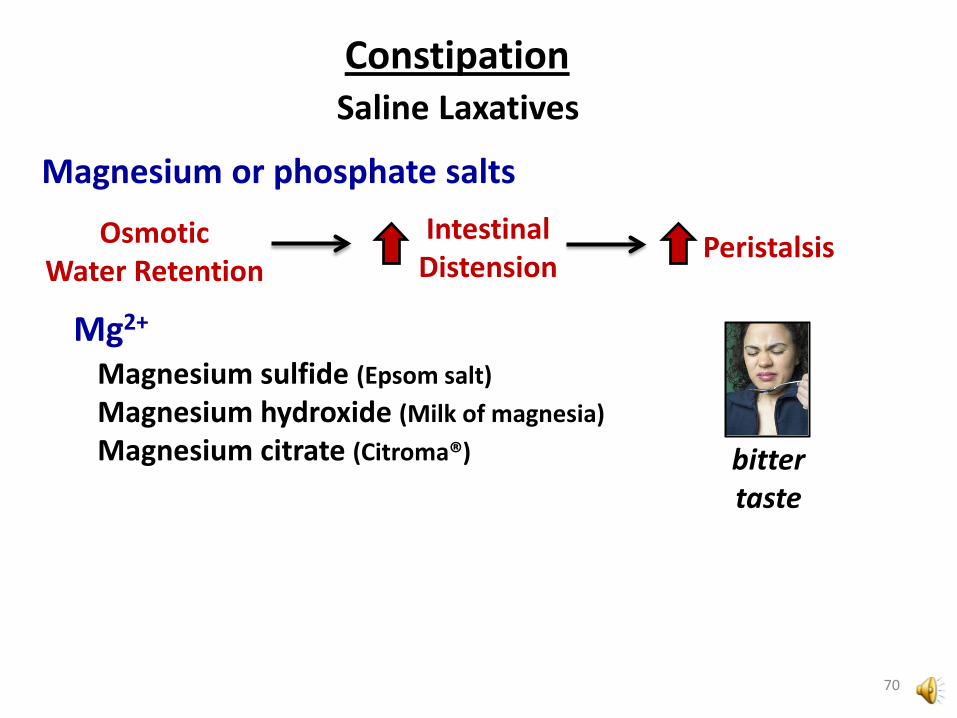
Saline Laxatives Constipation
Osmotic Water Retention
Intestinal Distension Peristalsis
Mg2+
Magnesium sulfide (Epsom salt) Magnesium hydroxide (Milk of magnesia) Magnesium citrate (Citroma®) bitter
taste
Magnesium or phosphate salts
70

Constipation
HPO4-; PO4
2-
Sodium Phosphate (OsmoPrep®; Visicol®; Fleet Phospho-soda®) Oral or Enema
PO42- is better absorbed than Mg2+
Adverse Effects: • Electrolyte disturbances
• Dehydration • Renal failure • Metabolic acidosis • Tetany from hypocalcemia
• Acute Phosphate Nephropathy (phosphate crystals in kidney)
71
Saline Laxatives
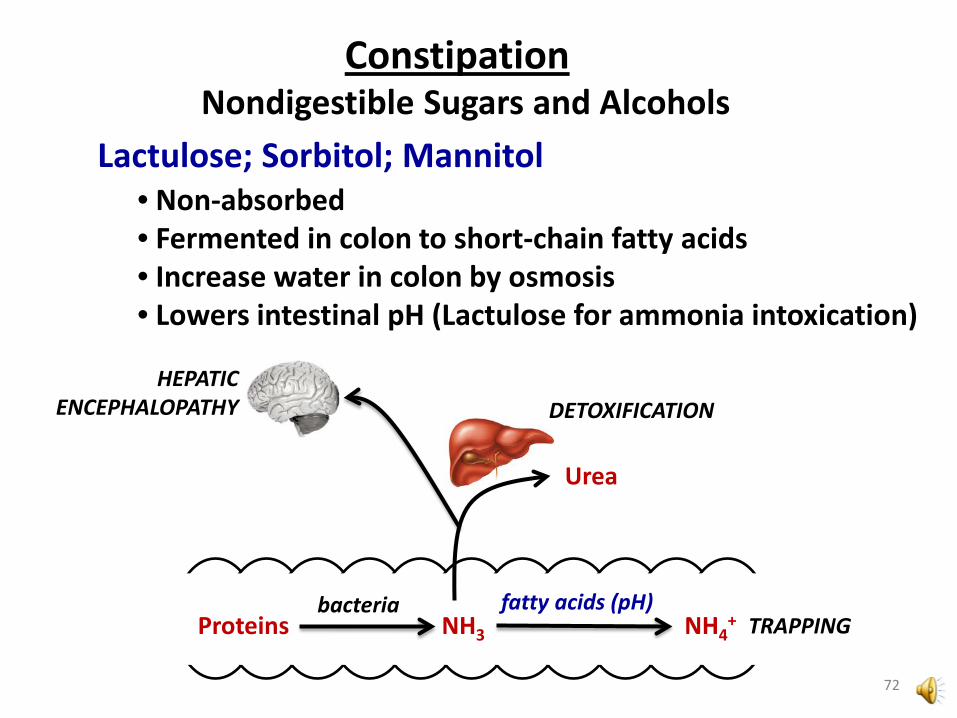
Nondigestible Sugars and Alcohols Constipation
Lactulose; Sorbitol; Mannitol • Non-absorbed • Fermented in colon to short-chain fatty acids • Increase water in colon by osmosis • Lowers intestinal pH (Lactulose for ammonia intoxication)
Proteins bacteria
NH3
Urea
DETOXIFICATION HEPATIC
ENCEPHALOPATHY
NH4+
fatty acids (pH) TRAPPING
72

Polyethylene glycol (PEG) Constipation
PEG 3350 (MiraLax®) • Non-absorbed, hydrophilic polymers • Average 3350 daltons (PEG 3350) • Short-term for occasional constipation • Powder, suspended and taken orally
PEG – Electrolyte solutions (CoLyte®, GoLYTELY®, etc.) • Used to evacuate GI tract for exams • PEG 3350 + Electrolytes
sodium sulfate sodium bicarbonate sodium chloride potassium chloride
LOW dose
HIGH dose
73

Constipation Stool Softeners
Docusate (Colace®, etc.) • Anionic surfactant (detergent) • Allows mixing of fats and water – makes stool softer • Generally safe for routine use
Mineral oil (heavy) • Hydrocarbons from petroleum distillation, not absorbed • Allows mixing of fats and water – makes stool softer • Do NOT use “light” (baby) mineral oil – topical use only • Harmful to lungs if aspirated • NOT safe for routine use:
• Can interfere with vitamin absorption • Can promote inflammation, elicit immune responses
• Contraindication – Docusate sodium • Can permit mineral oil absorption
74
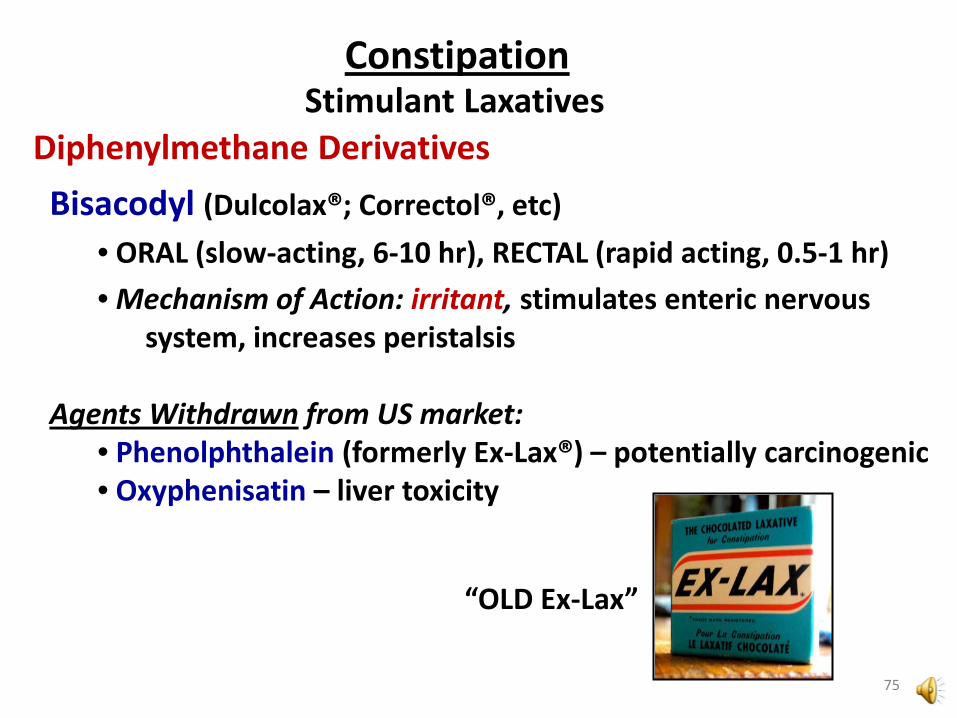
Stimulant Laxatives Constipation
Diphenylmethane Derivatives Bisacodyl (Dulcolax®; Correctol®, etc)
• ORAL (slow-acting, 6-10 hr), RECTAL (rapid acting, 0.5-1 hr) • Mechanism of Action: irritant, stimulates enteric nervous system, increases peristalsis
Agents Withdrawn from US market:
• Phenolphthalein (formerly Ex-Lax®) – potentially carcinogenic • Oxyphenisatin – liver toxicity
75
“OLD Ex-Lax”
Anthraquinones
Sennosides (Sennakote®; Ex-Lax®, etc)
• Natural products (senna; cascara; aloe; rhubarb) • Plant products are dimers or glycosides (not active) • Converted in colon to active anthraquinones – irritants • Produces large colon contractions 6-12 hr after ingestion
Senna hebecarpa
Rhamnus purshiana (cascara)
Cascara
76
“NEW Ex-Lax”
Stimulant Laxatives Constipation

77
Chloride Channels Constipation
Na+
Na+ K+
K+
2Cl-
Cl-
Cl- Na+ (+ H2O) Intestinal Lumen
K+
Cl-
Channel
Na+/K+
ATPase Na+/K+/2Cl-
Symporter
K+
Channel K+
apical
basolateral
78
Chloride Channels Constipation
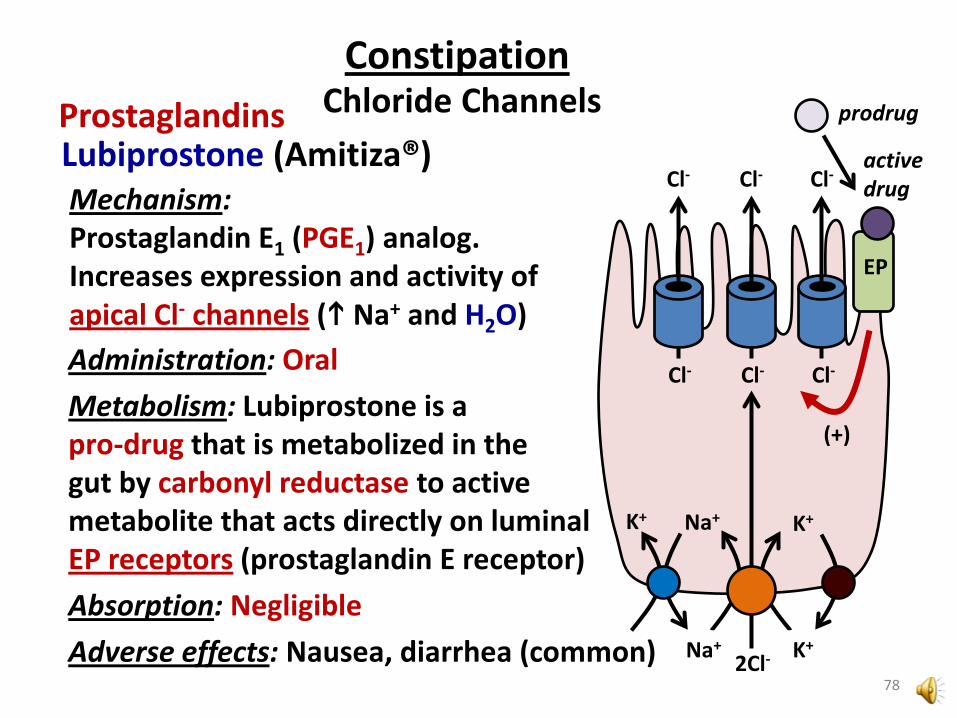
Mechanism: Prostaglandin E1 (PGE1) analog. Increases expression and activity of apical Cl- channels ( Na+ and H2O)
Lubiprostone (Amitiza®) Prostaglandins
Na+
Na+ K+
K+
2Cl-
Cl-
Cl-
K+
Cl-
Cl-
Cl-
Cl-
Administration: Oral Metabolism: Lubiprostone is a pro-drug that is metabolized in the gut by carbonyl reductase to active metabolite that acts directly on luminal EP receptors (prostaglandin E receptor) Absorption: Negligible Adverse effects: Nausea, diarrhea (common)
EP
(+)
active drug
prodrug
Diarrhea
1980’s – 2004 Attapulgite (Mg2+ Al3+ silicate; clay) + Pectin (fiber)
2004 – present Bismuth subsalicylate
Kaopectate
Kaolin (Al3+ silicate; clay) + Pectin (fiber) Until 1980’s
Clays
79

Diarrhea Bismuth Subsalicylate
Bismuth subsalicylate (Kaopectate®; Pepto-Bismol®)
Bismuth subsalicylate
Salicylic acid (absorbed) – Antisecretory Antiinflammatory
Bismuth (not absorbed) - Antimicrobial
H+
+ sulfur
BLACK tongue
BLACK stool
Bismuth sulfide (BLACK color)
80
Diarrhea Opioids
Loperamide (Immodium A-D®, etc) • Increases anal sphincter tone • Anti-diarrheal potency 50X morphine • Slowly absorbed (peak 5-6 hr)
Diphenoxylate + Atropine (Lomotil®; Motofen®) • Diphenoxylate is similar to meperidine, but unlike meperidine, is anti-diarrheal • Atropine is ANTICHOLINERGIC, has side effects:
constipation, dry mouth, blurred vision, urinary retention
• Mu Receptor AGONISTS • POOR CNS penetration • INHIBIT GI tract motility
81

Antiemetics
Fourth ventricle
Vomiting center (medulla)
5-HT3 (+) VOMITING NAUSEA
Duodenal distension, irritation
5-HT3 (+)
Chemoreceptor trigger zone (CTZ) (area postrema)
5-HT3 (+)
Nonspecific: • Metoclopramide
5-HT3 Specific: • Ondansetron (Zofran®) • Dolasetron (Anzemet®) • Granisetron (Kytril®) • Palonosetron (Aloxi®)
First approved: Ondansetron (1992) Newest: Palonosetron (2003)
82
5-HT3 Antagonists

Mechanism: INHIBIT stimulation of: Vomiting center CTZ Duodenum They do NOT inhibit vomiting due to motion sickness (inner ear) Adverse effects (minor, usually well tolerated): Headache, fatigue, constipation
Drug Interactions: QTc prolongation – ondansetron and dolasteron worst offenders
83
Antiemetics 5-HT3 Antagonists

Antiemetics
Fourth ventricle
VOMITING NAUSEA
Chemoreceptor trigger zone (CTZ) (area postrema)
D2 (+)
Prochlorperazine (Compazine®) Chlorpromazine (Thorazine®)
Dopamine Antagonists
“Typical” antipsychotics
• Antagonists of D2 receptor in CTZ • Also inhibit H1 and M1 receptors
...so are useful for treating vertigo
H1 (+) M1 (+)
Inner ear
84
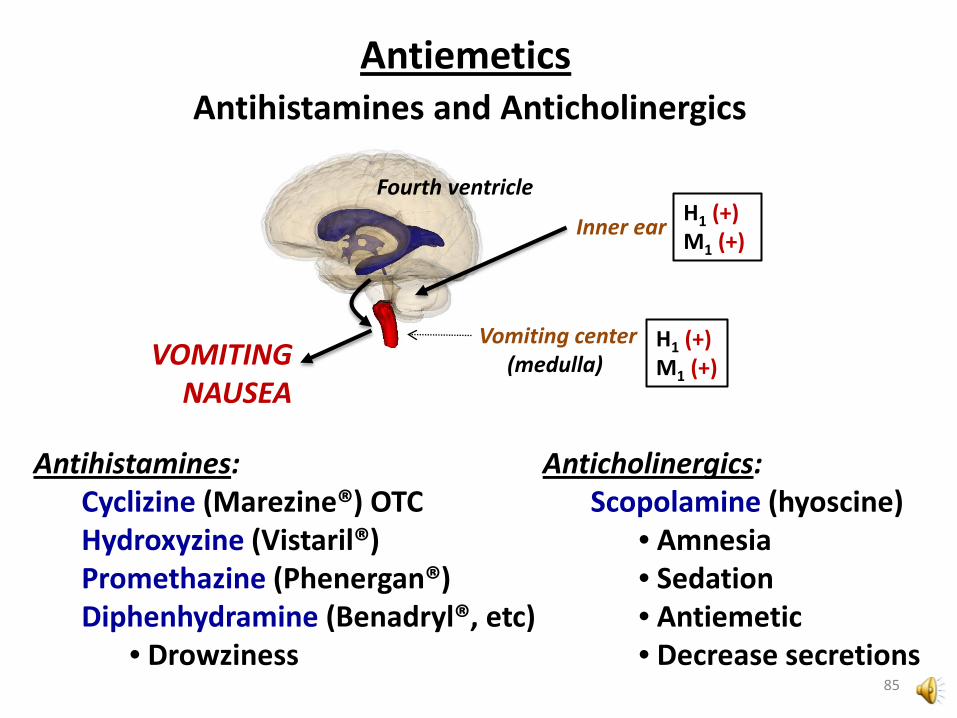
Antiemetics Antihistamines and Anticholinergics
Fourth ventricle
Vomiting center (medulla)
H1 (+) M1 (+) VOMITING
NAUSEA
H1 (+) M1 (+) Inner ear
Antihistamines: Cyclizine (Marezine®) OTC Hydroxyzine (Vistaril®) Promethazine (Phenergan®) Diphenhydramine (Benadryl®, etc)
• Drowziness
Anticholinergics: Scopolamine (hyoscine)
• Amnesia • Sedation • Antiemetic • Decrease secretions
85

Antiemetics Substance P Antagonists
Fourth ventricle
VOMITING NAUSEA
Vomiting center (medulla)
NK1 (+)
Duodenal distension, irritation
NK1 (+)
Aprepitant (Emend®) - capsule Fosaprepitant (Emend injection®)
Oral Bioavailability: 60% Metabolism: CYP3A4 Adverse Effects:
Fatigue, weakness Drug Interactions:
Strong CYP3A4 inhibitors may INCREASE levels of aprepitant
86
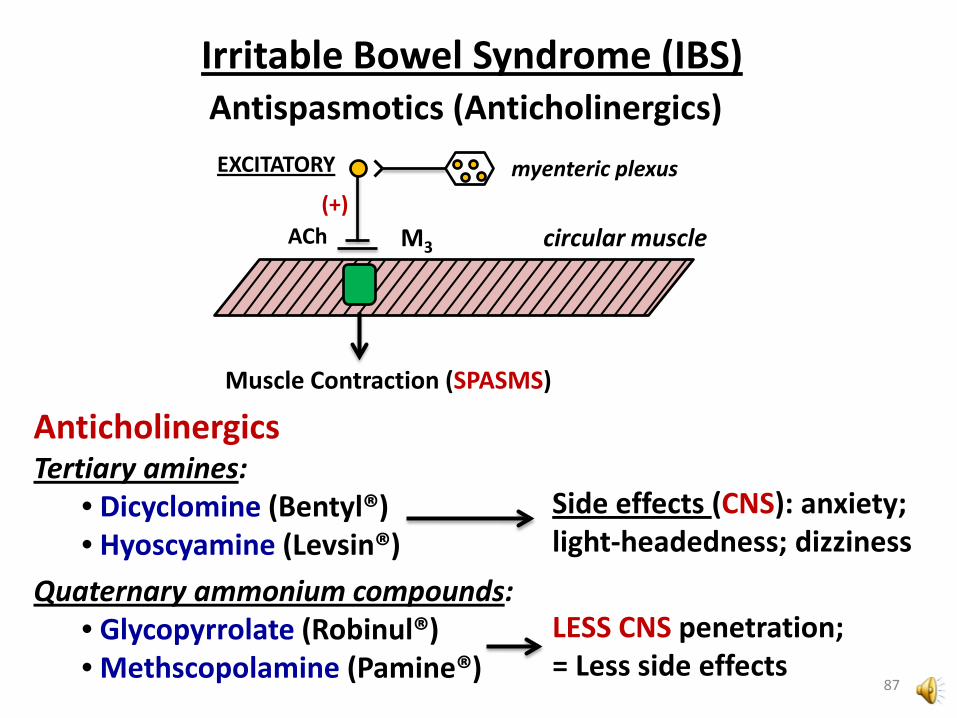
Irritable Bowel Syndrome (IBS) Antispasmotics (Anticholinergics)
circular muscle (+)
ACh
EXCITATORY myenteric plexus
M3
Muscle Contraction (SPASMS)
Anticholinergics Tertiary amines:
• Dicyclomine (Bentyl®) • Hyoscyamine (Levsin®)
Quaternary ammonium compounds: • Glycopyrrolate (Robinul®) • Methscopolamine (Pamine®)
Side effects (CNS): anxiety; light-headedness; dizziness
LESS CNS penetration; = Less side effects
87

Inflammatory Bowel Disease (IBD) Crohn’s Disease (CD) or Ulcerative Colitis (UC)
bacteria
intestinal/colon lumen
ulceration
antigen
macrophage Th0
APC
Th1
Th2 B IL-1 IL-12 TNF-α
INFLAMMATORY CYTOKINES
IFN-γ
INFLAMMATORY CYTOKINES
ANTIBODIES 88

Inflammatory Bowel Disease 5-ASA
Mesalamine (5-aminosalicylic acid; 5-ASA) Sulfasalazine (Azulfidine®) Olsalazine (Dipentum®) Balsalazide (Colazide®)
macrophage
IL-1 IL-12 TNF-α
IFN-γ
Th1 5-ASA
ABSORBED in stomach
NOT absorbed in stomach; MUST BE ACTIVATED by colon bacteria
• Antioxidant • NF-κB inhibitor
89
Mechanism:
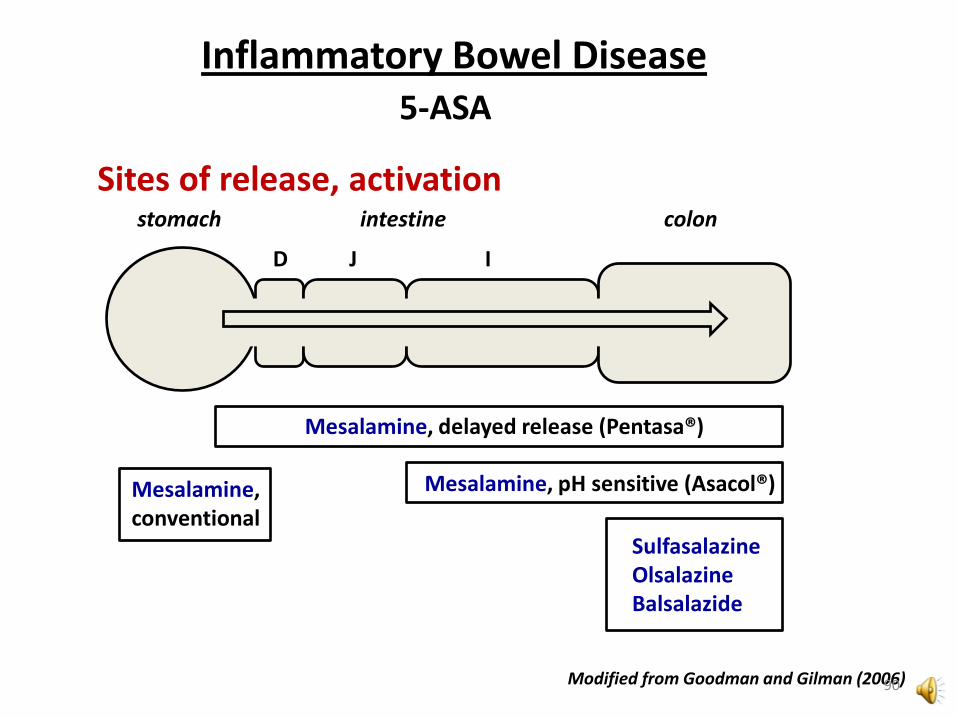
stomach intestine colon
D J I
Mesalamine, delayed release (Pentasa®)
Mesalamine, pH sensitive (Asacol®)
Sulfasalazine Olsalazine Balsalazide
Sites of release, activation
Modified from Goodman and Gilman (2006) 90
Inflammatory Bowel Disease 5-ASA
Mesalamine, conventional

Sulfasalazine Olsalazine Basalazide
Mesalamine (active drug)
N-acetyl-ASA (inactive metabolite)
Sulfapyridine (metabolite)
“Sulfa” drug SIDE EFFECTS
4-ABA (inactive metabolite)
• Headache • Nausea • Fatigue
91
Inflammatory Bowel Disease 5-ASA

Inflammatory Bowel Disease Thiopurine Immunosuppressants
6-Mercaptopurine (6-MP; Purinethol®) Azathioprine (AZA; Azasan®) • Both are inactive PRO-DRUGS (Metabolic activation needed)
PURINE biosynthesis
Incorporation into DNA
6-MP
Azathioprine
92
6-TGTP (AKA thioguanine
triphosphate)
Methyl TIMP
Immunosuppression

Hepatic Detoxification
6-MP 6-Methyl-MP TPMT (inactive)
Xanthine Oxidase (XO)
6-Thiouric acid (inactive)
• 10% of population have TPMT deficiency (poor metabolizers of 6-MP) • Requires 6-MP dose-reduction
Allopurinol • Used for hyperuricemia (often for leukemia – tumor lysis) • Requires 6-MP dose-reduction
93
Inflammatory Bowel Disease Thiopurine Immunosuppressants
6-MP, AZA Typical Indication: Acute lymphoblastic leukemia (ALL) - childhood Administration: ORAL Absorption: 6-MP: POOR and erratic AZA: GOOD Serum half-life: 6-MP: 1-3 hr AZA: 12 min (quickly forms 6-MP, which = 1-3 hr) Precautions: Dose-reduction NEEDED with allopurinol Dose-reduction NEEDED in TMPT poor metabolizers (genetic testing is available) Potential adverse effect: CANCER
94
Inflammatory Bowel Disease Thiopurine Immunosuppressants

Glucocorticoids Inflammatory Bowel Disease
IκB P
IκB
(+) NF-κB
Inflammatory Gene Expression
IKK complex (kinase)
(+)
Anti-inflammatory
(-)
Glucocorticoids
CD3(+)
Antibody
TNF-α
TNFR
95

Inflammatory Bowel Disease
Prednisone Adverse Effects of Prednisone
• Immunosuppression – (risk of infection, sepsis) • Hyperglycemia • Osteoporosis • Appetite; Weight gain • Muscle loss
Budesonide (Entocort®) • Enteric coating • EXTENSIVE FIRST PASS metabolism • Less severe adverse effects than prednisone
96
Glucocorticoids





























