Embed Size (px)
Citation preview
Gastroenterol Clin N Am 36 (2007) 665–685
GASTROENTEROLOGY CLINICSOF NORTH AMERICA
Irritable Bowel Syndrome: CurrentApproach to Symptoms, Evaluation,and Treatment
Elizabeth J. Videlock, BS, Lin Chang, MD*Center for Neurovisceral Sciences and Women’s Health, Division of Digestive Diseases,David Geffen School of Medicine at UCLA and VA Greater Los Angeles Healthcare System,CURE Building 115, Room 223, 11301 Wilshire Boulevard, Los Angeles, CA 90073, USA
Irritable bowel syndrome (IBS) is a common functional gastrointestinal (GI)disorder. It has a very high prevalence, estimated to be 10% to 20% in thegeneral population [1]. IBS accounts for significant health care costs with
annual direct and indirect costs estimated at $1.35 billion and at least $200 mil-lion, respectively [2]. IBS patients use more health care services than the generalpopulation, even for non–GI-related concerns [3,4].
This article provides clinicians with a current, concise, and evidence-basedreview of the symptoms, diagnostic evaluation, and treatment of IBS. A clearunderstanding of recommended diagnostic and therapeutic approaches leadsto greater patient satisfaction and reduced health care costs.
CLINICAL FEATURES OF IRRITABLE BOWEL SYNDROMEGastrointestinal SymptomsThe main symptom of IBS is chronic or recurrent abdominal pain or discom-fort associated with altered bowel habits. The new Rome III criteria for the di-agnosis of IBS were published in 2006 and are listed in Box 1 [1]. The followingare not part of the diagnostic criteria but are considered supportive symptoms:abnormal stool frequency (<3 bowel movements per week or >3 bowel move-ments per day); abnormal stool form (lumpy-hard stool or loose-watery stool);defecation; straining; urgency; a feeling of incomplete evacuation; and passingmucus and bloating.
The previous Rome II classification of IBS subtype was based on a combina-tion of symptoms including stool frequency and form, and defecation-relatedsymptoms. This classification was suboptimal because it was not evidence-based and because there was inconsistency with regard to the correct sub-classification of patients with frequent hard stools or infrequent watery stools.Furthermore, cluster analysis and symptom studies have shown that stool
*Corresponding author. E-mail address: [email protected] (L. Chang).
0889-8553/07/$ – see front matter Published by Elsevier Inc.doi:10.1016/j.gtc.2007.07.002 gastro.theclinics.com
666 VIDELOCK & CHANG
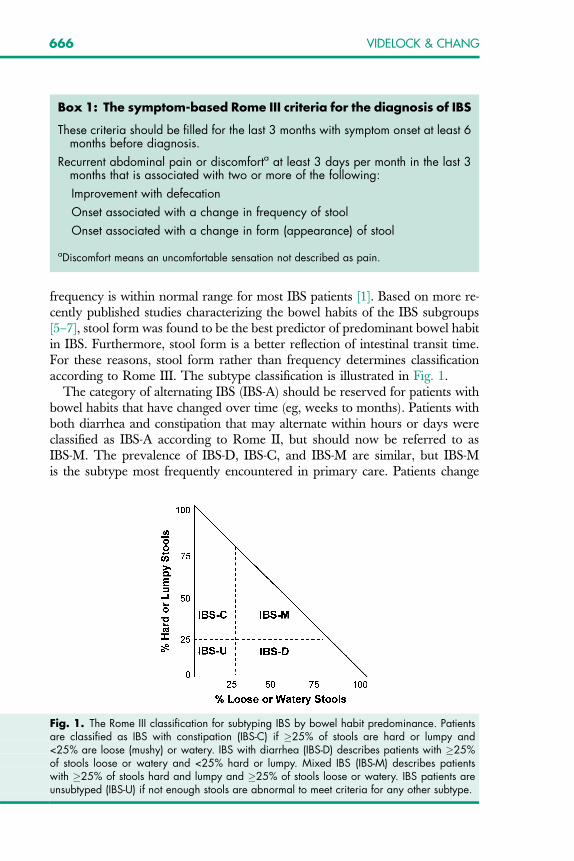
frequency is within normal range for most IBS patients [1]. Based on more re-cently published studies characterizing the bowel habits of the IBS subgroups[5–7], stool form was found to be the best predictor of predominant bowel habitin IBS. Furthermore, stool form is a better reflection of intestinal transit time.For these reasons, stool form rather than frequency determines classificationaccording to Rome III. The subtype classification is illustrated in Fig. 1.
The category of alternating IBS (IBS-A) should be reserved for patients withbowel habits that have changed over time (eg, weeks to months). Patients withboth diarrhea and constipation that may alternate within hours or days wereclassified as IBS-A according to Rome II, but should now be referred to asIBS-M. The prevalence of IBS-D, IBS-C, and IBS-M are similar, but IBS-Mis the subtype most frequently encountered in primary care. Patients change
Fig. 1. The Rome III classification for subtyping IBS by bowel habit predominance. Patientsare classified as IBS with constipation (IBS-C) if �25% of stools are hard or lumpy and<25% are loose (mushy) or watery. IBS with diarrhea (IBS-D) describes patients with �25%of stools loose or watery and <25% hard or lumpy. Mixed IBS (IBS-M) describes patientswith �25% of stools hard and lumpy and �25% of stools loose or watery. IBS patients areunsubtyped (IBS-U) if not enough stools are abnormal to meet criteria for any other subtype.
Box 1: The symptom-based Rome III criteria for the diagnosis of IBS
These criteria should be filled for the last 3 months with symptom onset at least 6months before diagnosis.
Recurrent abdominal pain or discomforta at least 3 days per month in the last 3months that is associated with two or more of the following:
Improvement with defecation
Onset associated with a change in frequency of stool
Onset associated with a change in form (appearance) of stool
aDiscomfort means an uncomfortable sensation not described as pain.
667IRRITABLE BOWEL SYNDROME
subtypes frequently, with 29% moving from IBS-C to IBS-D within 1 year [8].Because of this symptom instability, the terms ‘‘IBS with diarrhea’’ and ‘‘IBSwith constipation’’ are preferred over the previously used terms of ‘‘diarrhea-and constipation-predominant IBS’’ [8].
IBS-C and IBS-D patients have different symptom profiles, with IBS-Cpatients reporting more overall symptoms (both lower and upper abdominalpain) and particularly bloating [9]. Symptoms of IBS and functional dyspepsiaoverlap significantly and respond similarly to treatment. It has been argued thatthey are different manifestations of one condition [10].
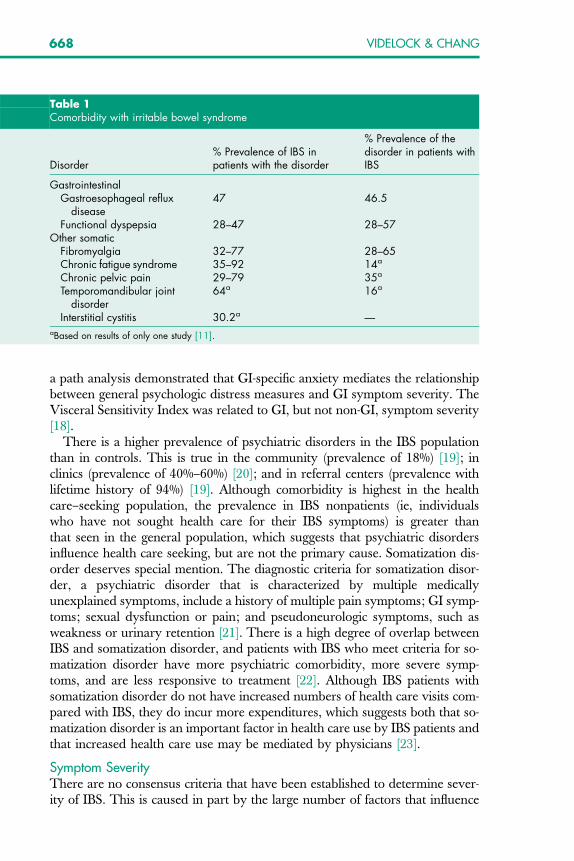
Extraintestinal Symptoms and Comorbid DisordersIBS patients make more health care visits and incur more health care coststhan non-IBS patients. More than half of additional visits and additional costsare for non-GI concerns [11]. Non-GI symptoms that are more common inIBS than controls include the following (prevalence): headache (23%–45%);back pain (27%–81%); fatigue (36%–63%); myalgia (29%–36%); dyspareunia(9%–42%); urinary frequency (21%–61%) and other urinary symptoms; anddizziness (11%–27%) [11]. IBS patients with comorbid somatic disorders (eg,fibromyalgia) report more severe IBS symptoms and lower health-related qual-ity of life (HRQOL) [11]. Common comorbid GI and other somatic disordersare listed in Table 1.
Although it seems that these comorbid disorders and IBS may have distinctcontributing factors to their pathophysiology, there are common themes thatare mostly related to psychologic symptoms and stress reactivity [11]. Stressis defined as acute threats to the homeostasis of an organism, be they real(physical) or perceived (psychologic). Sustained, threatening life events (psy-chosocial stressors) predict symptom exacerbation in established IBS patients[12–14], and the development of IBS symptoms in asymptomatic individualsfollowing a gastroenteric infection (postinfectious IBS) [13,15]. Stress-inducedchanges in pain modulation (hyperalgesia) and cognitive processes (hypervigi-lance toward viscerosomatic stimuli) may play a key role in the pain anddiscomfort characteristic of these disorders. Although these mechanisms maybe shared, they may be more specifically related to one particular stimulusdepending on the condition. For example, IBS patients may have developedpersistent symptom-specific anxiety from previously threatening visceral stim-uli (eg, food or GI infection), whereas fibromyalgia patients have symptom-specific anxiety to somatic stimuli (eg, muscle injury). These threateningevents, which are attached to their symptoms, may be involved in the develop-ment of anticipatory or anxiety-related responses [16] related to symptomrecurrence. Symptom-specific anxiety can amplify the perception of visceraland somatic afferent input to the brain, thereby contributing to pain-relatedsymptoms. A recently developed reliable, validated scale called the VisceralSensitivity Index measures GI-specific anxiety (ie, fear of visceral sensations)and may be useful for clinical assessment, treatment outcome studies, andmechanistic studies of the role of anxiety in IBS presentation [17]. In addition,
668 VIDELOCK & CHANG
a path analysis demonstrated that GI-specific anxiety mediates the relationshipbetween general psychologic distress measures and GI symptom severity. TheVisceral Sensitivity Index was related to GI, but not non-GI, symptom severity[18].
There is a higher prevalence of psychiatric disorders in the IBS populationthan in controls. This is true in the community (prevalence of 18%) [19]; inclinics (prevalence of 40%–60%) [20]; and in referral centers (prevalence withlifetime history of 94%) [19]. Although comorbidity is highest in the healthcare–seeking population, the prevalence in IBS nonpatients (ie, individualswho have not sought health care for their IBS symptoms) is greater thanthat seen in the general population, which suggests that psychiatric disordersinfluence health care seeking, but are not the primary cause. Somatization dis-order deserves special mention. The diagnostic criteria for somatization disor-der, a psychiatric disorder that is characterized by multiple medicallyunexplained symptoms, include a history of multiple pain symptoms; GI symp-toms; sexual dysfunction or pain; and pseudoneurologic symptoms, such asweakness or urinary retention [21]. There is a high degree of overlap betweenIBS and somatization disorder, and patients with IBS who meet criteria for so-matization disorder have more psychiatric comorbidity, more severe symp-toms, and are less responsive to treatment [22]. Although IBS patients withsomatization disorder do not have increased numbers of health care visits com-pared with IBS, they do incur more expenditures, which suggests both that so-matization disorder is an important factor in health care use by IBS patients andthat increased health care use may be mediated by physicians [23].
Symptom SeverityThere are no consensus criteria that have been established to determine sever-ity of IBS. This is caused in part by the large number of factors that influence
Table 1Comorbidity with irritable bowel syndrome
Disorder% Prevalence of IBS inpatients with the disorder
% Prevalence of thedisorder in patients withIBS
GastrointestinalGastroesophageal reflux
disease47 46.5
Functional dyspepsia 28–47 28–57Other somatic
Fibromyalgia 32–77 28–65Chronic fatigue syndrome 35–92 14a
Chronic pelvic pain 29–79 35a
Temporomandibular jointdisorder
64a 16a
Interstitial cystitis 30.2a —aBased on results of only one study [11].
669IRRITABLE BOWEL SYNDROME
severity and the wide gap between patient and physician perceptions of sever-ity. Current research suggests that a multidimensional view of illness severity ismore useful than one that is based on GI symptom intensity. Factors that areimportant to consider when assessing severity are HRQOL, psychosocial fac-tors, health care use behaviors, disability, and the overall degree to whichthe illness affects the patient’s life [24,25]. A preliminary report identified sev-eral predictors for patient-assessed ‘‘overall severity of GI symptoms’’ [26]. Thepredictors included multiple symptoms, such as ratings of abdominal pain anddiscomfort (pain, bloating); defecation-related symptoms (straining, urgency);and illness-related anxiety (‘‘something serious is wrong with my body’’).More recent epidemiologic data suggest a prevalence of severe or very severeIBS ranging from 3% to 69%, which is higher than previously thought [24].
Gender DifferencesGender differences in IBS are difficult to measure because most research partic-ipants are female; however, differences have been shown both in prominentsymptoms and in the response to treatment. Although in the community theratio of women to men with IBS is estimated to be 2:1, this difference iseven greater in the health care–seeking population, with women leading menby an estimated ratio of 2 to 4:1 [27]. A recently published study, however,found equal prevalence of men and women with IBS in newly developingAsian countries [28]. Compared with men with IBS, women with IBS reportgreater overall IBS symptom severity, intensity of abdominal pain and bloating,impact of symptoms on daily life, and lower HRQOL [29,30]. It is not known,however, if this is caused by differences in the sensation of pain, cognitive re-sponse to pain, or reporting bias [27]. Women also report more extraintestinalsymptoms, such as nausea, urinary urgency, and dyspareunia, and are morelikely to report symptoms of constipation and bloating [31–35].
Symptoms in women vary according to the menstrual cycle, with increasedreporting of GI symptoms in the late luteal and menses phases when comparedwith the midfollicular phase [36]. In particular, women report looser stools andmore GI symptoms just before and during menses and rectal sensitivity hasbeen shown to be greater in women with IBS in menses compared with womenwith IBS in other phases of the menstrual cycle [37].
With regard to gender differences in IBS treatment, serotonergic agents, suchas the 5-hydroxytryptamine (HT)3 antagonist alosetron, seem to have a morerobust effect in women with IBS-D than in men [38,39]. This difference couldbe related to small sample sizes, differences in drug metabolism, or the interac-tion between serotonin and estrogen [27] but is likely related to a combinationof gender-based differences in peripheral and central mechanisms.
DIAGNOSTIC EVALUATION OF IRRITABLE BOWEL SYNDROMEThe diagnosis of IBS is symptom-based because there are not yet diagnosticbiomarkers for IBS. The symptom-based Rome III criteria had a sensitivityof 0.707 and a specificity of 0.878 in the validation sample of 328 patients
670 VIDELOCK & CHANG
who had received a clinical diagnosis of IBS [40]. Although the presence of ‘‘redflag’’ or alarm signs and symptoms may indicate a need for further diagnosticwork-up, it is not recommended that patients with red flag symptoms be ex-cluded from the diagnosis of IBS. On average, IBS patients report the presenceof at least 1.65 red flag symptoms [41]. Nocturnal symptoms (40%) and onsetover the age of 50 (32%) were most common alarm signs. Alarm signs andsymptoms include the following:
Age �50Unintentional weight lossFamily history of GI malignancySevere unrelenting large-volume diarrheaFevers, chills, recent travel to endemic regionNocturnal symptomsHematocheziaRelevant findings on physical examination (arthritis, skin lesions, lymphadenop-
athy, abdominal mass)
Historically, IBS has been a diagnosis of exclusion, but current best evidencesuggests that a battery of diagnostic tests is not necessary because the prevalenceof organic disease is not increased in the population with symptoms of IBS with-out alarm features, and the positive predictive value of such tests remains small[42,43]. Diagnostic tests are likely unnecessary, including blood tests, stool tests,lactulose breath tests, abdominal imaging, and colonic imaging; however, fur-ther research on the use of diagnostic testing is warranted. Diagnostic testsmay reveal incidental findings or findings that are not related to the symptomsof IBS. Additionally, a negative finding on colonoscopy is not associated with anincreased sense of reassurance in patients with IBS [44]. There are several sce-narios in which diagnostic testing is recommended: (1) stool ova and parasitetesting for patients who have recently traveled to endemic regions or for immu-nocompromised individuals, (2) colonoscopy in patients over 50 years of age forcolon cancer screening, and (3) testing in patients who have not improved de-spite symptom-based treatment. There is good evidence that serologic testingfor celiac disease followed by endoscopic biopsy confirmation of positive resultsis a cost-effective strategy in North American IBS-D patients [45].
Small bowel bacterial overgrowth has been theorized to play a role in thesymptoms of IBS. Although some studies have shown an increased prevalenceof small bowel bacterial overgrowth in IBS as diagnosed by a lactulose breathtest [46,47], the use of this diagnostic tool is limited by the lack of evidence thattreatment of small bowel bacterial overgrowth with antibiotics leads to long-term abatement of IBS symptoms.
Testing for lactase deficiency is not generally recommended because true lac-tose malabsorption is not well-correlated with reported lactose intolerance [48]and because lactose restriction has not been shown to improve IBS symptoms[49,50]. This is likely because lactose intolerance coexists with IBS but is notthe predominant cause of symptoms.
671IRRITABLE BOWEL SYNDROME
TREATMENTPatient-Centered CareA good health care provider–patient relationship is the cornerstone of effectivecare of IBS. The quality of this relationship has been shown to improve patientoutcomes [51]. Elements of a good provider-patient relationship include a non-judgmental patient-centered interview, a careful and cost-effective evaluation,inquiry into the patient’s understanding of the illness, patient education, andinvolvement of the patient in treatment decisions [6]. Because IBS is a chronicdisease, it is important to assess specific reasons for the current visit, which maydiffer among patients (eg, concern about cancer, worsening pain, lack of re-sponse to treatment, and so forth) [52]. An intrinsic part of the clinical assess-ment is the psychosocial interview, which is usually quite relevant in IBSpatients. Because IBS patients may have stress-related symptoms or comorbidpsychologic symptoms, the psychosocial interview may uncover previouslyunexpressed associated symptoms and concerns that could be contributing tothe patient’s illness severity, daily functioning, and health-related outcome.Addressing psychosocial factors may improve health status and treatmentresponse [53].
DietMany patients report an inconsistent symptom response to certain foods, anda 1- to 2-week food and symptom diary can aid in careful analysis of potentialfood triggers. Although most patients cannot completely control symptomsthrough diet alterations alone, diet-related exacerbations may be minimized.Common food triggers include high-fat foods, raw fruits and vegetables, andcaffeinated beverages.
There is some evidence that the symptoms of IBS are related to a visceral hy-persensitivity to low-grade immune reactivity that does not cause symptoms inthe general population. A group in the United Kingdom conducted a random-ized controlled trial of food elimination based on IgG levels. IBS patients weregiven either a list of foods to which they had increased levels of IgG ora sham diet of similar foods to eliminate. Twenty-eight percent of patients adher-ing to the true diet had global improvement of symptoms versus 16.7% on shamdiets. This difference was statistically significant and corresponds to a number-needed-to-treat of 9. A larger percentage of patients who fully adhered to the diethad improved symptoms (54% versus 15% of strict adherers to the sham diet),corresponding to a number-needed-to-treat of 2.5. Additionally, resumption ofthe regular diet caused a worsening of symptoms in a greater percentage of thosefollowing the true diet than the control diet. There was not a significant effect onHRQOL. It has been suggested, however, that the effect seen in this study wasa result of diet alone regardless of IgG levels. IgG levels have not been shown tobe predictive of food intolerance and a large percentage of patients in the truediet treatment group eliminated milk and wheat, which are known to affectsymptoms in IBS [54,55]. Modification of diet may affect symptoms regardlessof whether or not there is true food intolerance.
672 VIDELOCK & CHANG
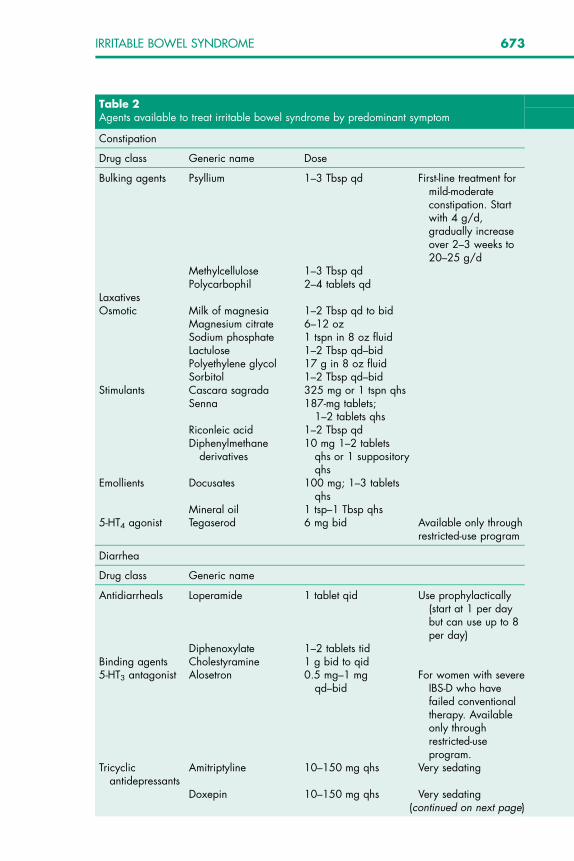
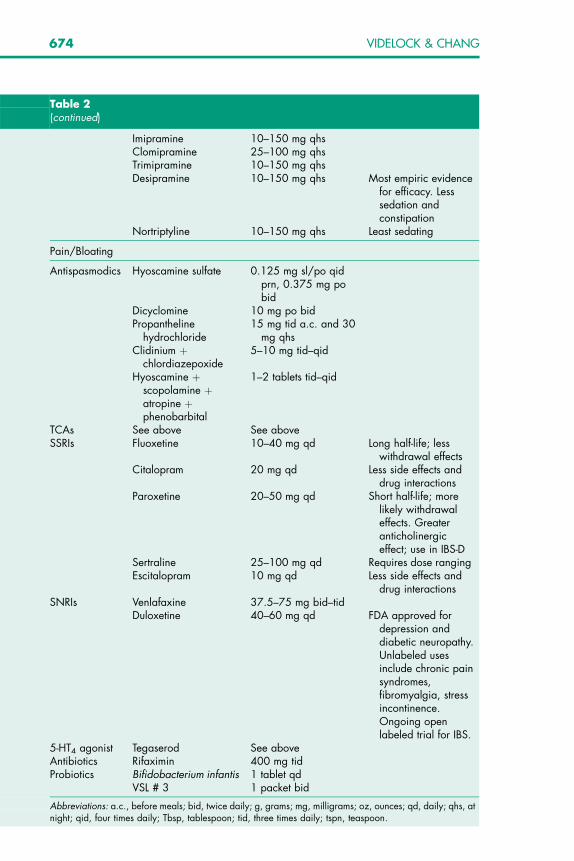
Pharmacologic AgentsIn 2002, the American College of Gastroenterology (ACG) Functional Gastro-intestinal Disorders Task Force published a comprehensive systematic reviewon the treatment of IBS [56]. In a subsequent publication in 2005, Schoenfeld[57] updated and expanded on the ACG’s review. The section of this articlefocusing on pharmacologic treatment summarizes these findings, taking into ac-count high-quality trials that have since been published (Table 2).
Bulking AgentsBulking agents include psyllium, methylcellulose, corn fiber, calcium polycar-bophil, and ispaghula husk. Fiber supplementation has often been used as ini-tial management of IBS; however, the ACG Functional GastrointestinalDisorders Task Force evaluated randomized, placebo-controlled treatment tri-als for IBS and found that none of the trials of bulking agents were of high qual-ity [56]. A meta-analysis showed a small, but significant improvement withsoluble fiber (psyllium, ispahula, calcium polycarbophil), but not with insolublefiber (corn, wheat bran) [58]. This meta-analysis is limited by the inclusion ofresults from divergent studies and the extrapolation of end points [57]. Fibermay increase stool frequency in IBS-C, but it is not clear whether this iswell-correlated with relief of pain or other symptoms. Additionally, bulkingagents in quantities that are therapeutic can cause adverse effects includingbloating and abdominal pain and discomfort, and it may be helpful to recom-mend a gradual initiation of the dose to minimize side effects, particularly inthose who have relatively little fiber in their diets or those with predominantbloating [57].
Antidiarrheal AgentsThe use of antidiarrheal agents has shown no benefit for global IBS symptomsor abdominal pain [56,57]. Loperamide seems to be effective at prolonging in-testinal transit time and improving stool consistency in IBS-D. These agentsmay be very useful in some IBS-D patients to manage stool urgency, frequency,and fecal incontinence. They can be used on a more regular basis in patientswith more frequent symptoms or on an as-needed basis. It is often useful forpatients to use antidiarrheals prophylactically before leaving the house,a long car trip, a meal, or a stressful event. This can decrease both the diarrheaand the anticipatory stress often felt by patients before a known symptomtrigger.
LaxativesOsmotic laxatives are available over the counter and are widely used in thetreatment of IBS-C and chronic constipation. Although no randomized, con-trolled studies have shown efficacy of laxatives in IBS, they may be useful intreating the constipation symptoms in those with IBS-C. Osmotic laxatives,such as polyethylene glycol or magnesium-containing products, are generallysafe and well tolerated. Polyethylene glycol can be easily titrated by the patient,allowing adjustment in stool frequency and consistency as symptoms vary.
673IRRITABLE BOWEL SYNDROME
Table 2Agents available to treat irritable bowel syndrome by predominant symptom
Constipation
Drug class Generic name Dose
Bulking agents Psyllium 1–3 Tbsp qd First-line treatment formild-moderateconstipation. Startwith 4 g/d,gradually increaseover 2–3 weeks to20–25 g/d
Methylcellulose 1–3 Tbsp qdPolycarbophil 2–4 tablets qd
LaxativesOsmotic Milk of magnesia 1–2 Tbsp qd to bid
Magnesium citrate 6–12 ozSodium phosphate 1 tspn in 8 oz fluidLactulose 1–2 Tbsp qd–bidPolyethylene glycol 17 g in 8 oz fluidSorbitol 1–2 Tbsp qd–bid
Stimulants Cascara sagrada 325 mg or 1 tspn qhsSenna 187-mg tablets;
1–2 tablets qhsRiconleic acid 1–2 Tbsp qdDiphenylmethane
derivatives10 mg 1–2 tablets
qhs or 1 suppositoryqhs
Emollients Docusates 100 mg; 1–3 tabletsqhs
Mineral oil 1 tsp–1 Tbsp qhs5-HT4 agonist Tegaserod 6 mg bid Available only through
restricted-use program
Diarrhea
Drug class Generic name
Antidiarrheals Loperamide 1 tablet qid Use prophylactically(start at 1 per daybut can use up to 8per day)
Diphenoxylate 1–2 tablets tidBinding agents Cholestyramine 1 g bid to qid5-HT3 antagonist Alosetron 0.5 mg–1 mg
qd–bidFor women with severe
IBS-D who havefailed conventionaltherapy. Availableonly throughrestricted-useprogram.
Tricyclicantidepressants
Amitriptyline 10–150 mg qhs Very sedating
Doxepin 10–150 mg qhs Very sedating(continued on next page)
674 VIDELOCK & CHANG
Table 2(continued)
Imipramine 10–150 mg qhsClomipramine 25–100 mg qhsTrimipramine 10–150 mg qhsDesipramine 10–150 mg qhs Most empiric evidence
for efficacy. Lesssedation andconstipation
Nortriptyline 10–150 mg qhs Least sedating
Pain/Bloating
Antispasmodics Hyoscamine sulfate 0.125 mg sl/po qidprn, 0.375 mg pobid
Dicyclomine 10 mg po bidPropantheline
hydrochloride15 mg tid a.c. and 30
mg qhsClidinium þ
chlordiazepoxide5–10 mg tid–qid
Hyoscamine þscopolamine þatropine þphenobarbital
1–2 tablets tid–qid
TCAs See above See aboveSSRIs Fluoxetine 10–40 mg qd Long half-life; less
withdrawal effectsCitalopram 20 mg qd Less side effects and
drug interactionsParoxetine 20–50 mg qd Short half-life; more
likely withdrawaleffects. Greateranticholinergiceffect; use in IBS-D
Sertraline 25–100 mg qd Requires dose rangingEscitalopram 10 mg qd Less side effects and
drug interactionsSNRIs Venlafaxine 37.5–75 mg bid–tid
Duloxetine 40–60 mg qd FDA approved fordepression anddiabetic neuropathy.Unlabeled usesinclude chronic painsyndromes,fibromyalgia, stressincontinence.Ongoing openlabeled trial for IBS.
5-HT4 agonist Tegaserod See aboveAntibiotics Rifaximin 400 mg tidProbiotics Bifidobacterium infantis 1 tablet qd
VSL # 3 1 packet bid
Abbreviations: a.c., before meals; bid, twice daily; g, grams; mg, milligrams; oz, ounces; qd, daily; qhs, atnight; qid, four times daily; Tbsp, tablespoon; tid, three times daily; tspn, teaspoon.
675IRRITABLE BOWEL SYNDROME
Lactulose and sorbitol may also increase stool frequency, but are often associ-ated with the side effects of bloating or cramping in IBS patients. Stimulant lax-atives, such as senna, cascara, or bisacodyl, are useful on an intermittent basisfor refractory constipation, although frequently cause cramping, loose stools,and urgency.
AntispasmodicsAntispasmodics work either by a direct effect on intestinal smooth muscle (eg,mebeverine, pinaverine) or by their anticholinergic or antimuscarinic proper-ties (eg, dicyclomine, hyoscyamine). A meta-analysis evaluated 23 randomizedclinical trials (RCTs) and reported a significantly higher global improvementwith drug versus placebo (56% versus 38%) and a greater pain improvement(53% versus 41%) [59]. The ACG systematic review, however, evaluated 18English-language RCTs assessing the efficacy of antispasmodic agents [56].This review concluded that there is little evidence for the efficacy of antispas-modics for global relief of IBS symptoms [57]. Most of these studies have shortduration, small sample sizes, and suboptimal quality. Of three higher-qualityRCTs [60–62], only one showed a significant difference between placebo andtreatment (dicyclomine), but this was using a dose high enough to cause 15%of the treatment group to withdraw from the study because of adverse effects com-pared with no withdrawals in the placebo group [62]. Side effects of these agentsinclude dry mouth, constipation, urinary retention, and visual disturbances.
Serotonergic Agonist or AntagonistsTegaserodTegaserod is a selective 5-HT4 partial agonist that stimulates gut transit andmay also have an effect on visceral sensation [63,64]. Tegaserod was approvedby the Food and Drug Administration (FDA) for the treatment of IBS-C inwomen and more recently has been approved for the treatment of chronicconstipation in men and women under the age of 65. On March 30, 2007, how-ever, Novartis Pharmaceuticals suspended marketing of Zelnorm (tegaserod)because of important safety information. This suspension occurred at therequest of the FDA because of the incidence of cardiovascular ischemic events be-ing significantly higher with Zelnorm treatment than with placebo treatment (13per 11,614 [0.11%] with Zelnorm and 1 per 7031 [0.01%] with placebo [P ¼ .024]).
Several large and well-designed trials have shown tegaserod to be more effec-tive than placebo in improving symptoms of IBS-C [65–68]. More recent stud-ies have shown that tegaserod remains as effective with repeated use (aftera treatment-free interval) as it is in initial therapy, and there is no rebound effect(worsening of symptoms after treatment withdrawal) [69,70]. In addition toimproving IBS-C symptoms, tegaserod has been proved to improve outcomesrelated to productivity and work impairment [71].
AlosetronAlosetron is a 5-HT3 receptor antagonist that is currently available under a re-stricted use program and is approved only for women with severe IBS-D who
676 VIDELOCK & CHANG
have failed conventional therapy. This restriction is because of the occurrenceof GI-related adverse events including ischemic colitis and serious complica-tions of severe constipation. These events occurred at a rate of 1.1 per 1000patient years for ischemic colitis and 0.66 per 1000 patient years for seriouscomplications of constipation [72]. A recent systematic review concluded thatthere is a significantly increased rate of ischemic colitis among alosetron-usingpatients compared with placebo-using patients (0.15% versus 0.0%), but no sig-nificant difference in the rate of serious complications of constipation. All of thealosetron-using patients with ischemic colitis had a reversible colopathy withoutlong-term sequelae and most cases occurred within the first month of treatment[73]. The restriction notwithstanding, alosetron has been proved efficacious inseven placebo-controlled trials with over 3000 patients with nonconstipationIBS. Five of the seven studies showed relief of abdominal pain or discomfortand two showed relief of urgency [72]. There is a recently publishedplacebo-controlled long-term study that demonstrated significant efficacy ofalosetron compared with placebo over a treatment period of 48 weeks [74].Alosetron is not FDA-approved for the treatment of IBS-D in men, but one trialdid show an increased rate of relief from symptoms during 8 weeks of treat-ment with 1 mg alosetron twice a day (53%) compared with placebo (40%)[39]. Alosetron significantly reduced stool consistency scores indicating moreformed stools; however, no significant effects of alosetron were seen withregard to the other secondary symptom end points.
AntidepressantsTricyclic antidepressantsThe rationale of using antidepressants in IBS is that these agents may alter painperception by a central modulation of visceral afferents, treat comorbid psycho-logic symptoms, and alter GI transit. Different classes of antidepressants likelyact by different combinations of mechanisms. Tricyclic antidepressants are thebest studied, and are often used at low doses, because their major impact in IBSmay be more associated with an analgesic effect rather than treatment ofpsychologic symptoms. A systematic review found that none of the sevenrandomized placebo-controlled trials evaluating the effect of tricyclic antide-pressants in the treatment of IBS were of high quality because of relativelysmall sample sizes and poorly defined primary and secondary end points[56]. A large randomized 12-week placebo-controlled trial, which evaluatedthe efficacy of desipramine in treating moderate to severe functional boweldisorders, conducted by Drossman and colleagues [75], however, was pub-lished subsequent to the systematic review. Desipramine was shown to havestatistically significant benefit over placebo in the per protocol analysis, whichincluded only those patients who completed treatment (responder rate 73%versus 49%), but not in the intention-to-treat analysis. The lack of benefit inthe intention-to-treat analysis may have been related to a significant drop outrate primarily because of symptom side effects. This study also found thatthe patients most likely to improve with desipramine were patients with

677IRRITABLE BOWEL SYNDROME
IBS-D, no depression, and mild to moderate symptoms. The most commonside effects associated with tricyclic antidepressants include dry mouth, consti-pation, and drowsiness. Often initiating the drug at the lowest available doseand increasing it gradually can minimize adverse events while trying to achievea therapeutic effect (eg, starting dose of 10 mg at bedtime and increasing up to75 mg if needed). In patients who have coexistent sleep disturbances, amitrip-tyline may be a good choice because it has a greater sedative effect caused by itsmore potent antihistaminic effects. Desipramine and nortriptyline are lesssedating. If a tricyclic antidepressant is used in IBS-C, desipramine should beconsidered because it has less anticholinergic effects and is less constipatingthan the other tricyclic antidepressants.
Selective serotonin reuptake inhibitorsSelective serotonin reuptake inhibitors are commonly used to treat IBS eventhough there have been relatively few placebo-controlled trials. Preliminaryevidence suggests that selective serotonin reuptake inhibitors have an effecton overall HRQOL, symptom frequency, and abdominal pain, and theseeffects seem to be independent of effects on mood. A RCT of paroxetine inIBS patients who failed therapy with a high-fiber diet showed a greater increasein overall well-being with paroxetine than placebo [76]. This was true fordepressed and nondepressed participants [76]. Fluoxetine was evaluated in44 patients with IBS-C and was more effective than placebo in decreasingthe frequency of symptoms including abdominal discomfort and bloatingand increasing frequency of bowel movements and improving consistency ofstool [77]. A controlled crossover study of citalopram in 23 nondepressedIBS patients showed an improvement in abdominal pain, bloating, and overallwell-being [78]. There is more evidence for the efficacy of tricyclic antidepres-sants as analgesics, but tricyclic antidepressants are not as well tolerated asselective serotonin reuptake inhibitors. Large, high-quality trials are neededto evaluate the effectiveness of selective serotonin reuptake inhibitors in IBS;however, in patients with severe IBS, treatment with selective serotonin reup-take inhibitors may be helpful and has been shown to be cost-effective whencompared with routine care [79]. Combined serotonin-norepinephrine reuptakeinhibitors, such as venlaxifine and duloxetine, may have possible beneficialeffects in IBS but further studies are needed.
AntibioticsSmall bowel bacterial overgrowth has been theorized to play a role in IBSand is supported by an abnormal lactulose breath test in most IBS patients[46,47]. Rifaximin is an antibiotic that has very low systemic absorption andbroad-spectrum activity against gram-positive and gram-negative aerobes andanaerobes. In a randomized, double-blind placebo-controlled trial, 400 mg ofrifaximin given three times per day for 10 days was superior to placebo in improv-ing global symptoms (mean improvement of 36.4% versus 21%) and bloating (butnot abdominal pain, diarrhea, or constipation). The effects were present through-out the 10-week follow-up of the study. Although difficult to evaluate in a small

678 VIDELOCK & CHANG
sample (N ¼ 87), adverse effects were uncommon and included nausea andabdominal pain [80]. Future studies including an ongoing multicenter RCTwill likely provide more information on the efficacy of this antibiotic treatmentin IBS.
ProbioticsProbiotics are hypothesized to work by several mechanisms. These includea shift from a proinflammatory to an anti-inflammatory cytokine profile, thereduction of bile acid delivery to the colon, and alteration of motility [81]. Atrial of probiotics comparing either Bifidobacterium infantis (B infantis) or Lactoba-cillus salivarius with placebo in 75 patients with IBS over a 12-week treatmentperiod showed a significant reduction in abdominal pain and discomfort, bloat-ing, and difficulty with bowel movements with B infantis but not with L salivarius[82]. IBS patients were found to have a decreased blood interleukin-10/interleu-kin-12 ratio indicative of a proinflammatory, Th-1 state. Normalization of thisratio occurred in patients who received B infantis but not in those taking L sal-ivarius or placebo. A larger study (N ¼ 362) from the same group further eval-uated B infantis in a capsule formulation in women with IBS seen in a primarycare setting. A dose of 1 � 108 colony-forming units given once a day over4 weeks significantly reduced specific symptoms of IBS and global assessmentcompared with placebo or lower doses of B infantis. A higher dose of B infantiswas not observed to be beneficial, but this may have been caused by problemswith dissolution of the capsule [83].
Data from placebo-controlled trials also exists for VSL# 3, a probiotic that isa combination of three species of Bifidobacteria, four species of Lactobacilli, andStreptococcus salivarius ssp. thermophilus. VSL#3 decreased flatulence but did notshow clinical efficacy for overall relief of IBS symptoms [84,85]. Another pro-biotic mixture (Lactobacillus rhamnosus GG, L rhamnosis LC705, Bifidobacteriumbreve Bb99, and Propionibacterium freudenreichii ssp. shermanii JS) was effective inreducing IBS symptoms overall, but when the effect on individuals symptomswas analyzed, there was only a statistically significant reduction of borborygmi,and HRQOL was not significantly improved [86].
Novel Drugs in Development for Irritable Bowel SyndromeThere are a number of drugs in various phases of drug development that arebeing studied for the treatment of IBS. Many of these agents have novel mech-anisms of action. Drugs undergoing phase III clinical trials for IBS include thechloride channel activator lubiprostone and the 5-HT4 agonist–5-HT3 antago-nist renzapride. Lubiprostone is a FDA-approved treatment of chronic consti-pation in men and women that was demonstrated to be efficacious at a doseof 24 lg twice daily in improving stool frequency, stool form, and straining[87,88]. Renzapride improved stool consistency and frequency in IBS-C pa-tients but provided no overall relief of abdominal pain and discomfort [89]. Ca-milleri and colleagues [90] reported that renzapride was associated with animprovement in bowel function scores and a significant linear dose responsefor colon transit in 48 IBS-C patients, but there was no significant effect on
679IRRITABLE BOWEL SYNDROME
gastric emptying and small intestinal transit. Acceleration of colon transit pos-itively correlated with improvements in ease of passage and stool form but notwith stool frequency. Tack and colleagues [91] recently showed that a dose of2 mg twice daily reduced overall colonic transit time and in the cecum–ascending colon and descending colon. Other drugs in various stages of devel-opment for IBS include a CRF1 antagonist; neurokinin antagonists; guanylatecyclase-C agonist (linaclotide); 2,3-benzodiazepine (dextofisopam); kappaopioid antagonist (asimadoline); serotonin noradrenergic reuptake inhibitor(duloxetine); novel serotonergic agents; and opioid receptor agents.
Nonpharmacologic AgentsThere are several psychologic treatments for which there is convincing evi-dence of efficacy. Cognitive-behavioral therapy is a short-term, goal-orientedform of psychotherapy that focuses on the role that thoughts play in determin-ing behaviors and emotional responses. In IBS, the overall negative effect ofsymptoms may be increased by such thoughts as ‘‘there is something wrongwith my body’’ or ‘‘what will people think if I go to the bathroom again?’’[92] Cognitive-behavioral therapy helps patients to identify these thoughts asthey occur and to find alternative, more constructive ways to view the situa-tion. It also helps people become aware of and be more in control of theirown autonomic physiology. Cognitive-behavioral therapy was more effectivethan patient education in terms of global well-being and satisfaction with treat-ment and no different than desipramine in one randomized controlled trial [75].In another high-quality study, cognitive-behavioral therapy was shown to im-prove symptoms but was no different than standard care or relaxation therapy[93].
Gut-directed hypnotherapy is another area in which there has been substan-tial research. Gut-directed hypnotherapy is hypnosis that is directed towardrelaxation and control of intestinal motility by repeated suggestion of controlover symptoms followed by ego-strengthening [94]. It is difficult to comparestudies, because they have used different controls and end points and becausehypnosis is highly operator-sensitive. Yet, many have reported positive results,and a recent systematic review [95] concluded that the evidence suggests thathypnotherapy is effective, but warned that the studies were conducted in refer-ral centers and the subjects for the most part had refractory IBS of a longduration, and so the results may not apply to all clinic settings [95].
Complementary and Alternative MedicineBecause even the most effective treatments for IBS do not help all patients,many turn to complementary and alternative medicine in search of other treat-ment options. Furthermore, many patients prefer complementary and alterna-tive medicine treatments because they view them as natural and time-tested. Inaddition, complementary and alternative medicine treatments often providea more holistic approach and meaningful clinician-patient relationship thanwestern medicine. It is important for clinicians to have an understanding ofthese treatments and whether there is any evidence for their efficacy.
680 VIDELOCK & CHANG
Acupuncture has been a popular therapy for IBS patients. Despite the factthat theory predicts effectiveness of a treatment modulating ascending painstimuli, it has not been well-studied and conclusions across studies are difficultto make because of nonstandardized experimental and placebo treatment mo-dalities. The authors of a recent Cochrane review concluded that acupuncturewas likely no better than sham acupuncture, but may have been better thanother controls; however, more research is required to make any recommenda-tions because of the heterogeneity of the studies [96].
Herbal medicine is another area of complementary and alternative medicinein which patients express interest. Theoretically, this is more amenable torigorous randomized and controlled study designs, but few high-quality studieshave been published. The best evidence is for Chinese herbal medicine. Ben-soussan and colleagues [97] showed an improvement in symptoms and globalscores over placebo for patients treated either with standard or individualizedChinese herbal medicine. Only those who received individualized Chineseherbal medicine treatment maintained a more sustained relief of their IBSsymptoms. Peppermint oil has smooth muscle relaxant effects and there issome evidence that it may improve symptoms [98]. Other alternative or herbalmedicines that have been studied are extract of artichoke [99], carmint [100],the herbal mixture STW 5 [101], and melatonin [102,103].
SUMMARYIBS is a prevalent and heterogeneous disorder and patient care should be focusedon reducing costs and improving patient satisfaction and HRQOL. The cultiva-tion of a trusting and cooperative clinician-patient relationship reduces the order-ing of unnecessary diagnostic tests and facilitates a collaborative effort of patientand clinician to find the treatment that provides the most relief of symptoms, andthe greatest management of their illness and improvement of HRQOL.
References[1] Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenter-
ology 2006;130(5):1480–91.[2] Inadomi JM, Fennerty MB, Bjorkman D. The economic impact of irritable bowel syndrome.
Aliment Pharmacol Ther 2003;18(7):671–82.[3] Levy RL, Von Korff M, Whitehead WE, et al. Costs of care for irritable bowel syndrome
patients in a health maintenance organization. Am J Gastroenterol 2001;96(11):3122–9.[4] Longstreth GF, Wilson A, Knight K, et al. Irritable bowel syndrome, health care use, and
costs: a U.S. managed care perspective. Am J Gastroenterol 2003;98(3):600–7.[5] Tillisch K, Labus JS, Naliboff BD, et al. Characterization of the alternating bowel habit
subtype in patients with irritable bowel syndrome. Am J Gastroenterol 2005;100(4):896–904.
[6] Drossman DA. The functional gastrointestinal disorders and the Rome III process. Gastroen-terology 2006;130(5):1377–90.
[7] Mearin F, Balboa A, Badia X, et al. Irritable bowel syndrome subtypes according to bowelhabit: revisiting the alternating subtype. Eur J Gastroenterol Hepatol 2003;15(2):165–72.
[8] Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenter-ology 2006;130:1480–91.
681IRRITABLE BOWEL SYNDROME
[9] Talley NJ, Dennis EH, Schettler-Duncan VA, et al. Overlapping upper and lower gastroin-testinal symptoms in irritable bowel syndrome patients with constipation or diarrhea. AmJ Gastroenterol 2003;98(11):2454–9.
[10] Cremonini F, Talley NJ. Review article: the overlap between functional dyspepsia andirritable bowel syndrome—a tale of one or two disorders? Aliment Pharmacol Ther2004;20(Suppl 7):40–9.
[11] Whitehead WE, Palsson O, Jones KR. Systematic review of the comorbidity of irritablebowel syndrome with other disorders: what are the causes and implications? Gastroenter-ology 2002;122(4):1140–56.
[12] Whitehead WE, Crowell MD, Robinson JC, et al. Effects of stressful life events on bowelsymptoms: subjects with irritable bowel syndrome compared with subjects without boweldysfunction. Gut 1992;33(6):825–30.
[13] Gwee KA, Leong YL, Graham C, et al. The role of psychological and biological factors inpostinfective gut dysfunction. Gut 1999;44(3):400–6.
[14] Bennett EJ, Tennant CC, Piesse C, et al. Level of chronic life stress predicts clinical outcomein irritable bowel syndrome. Gut 1998;43(2):256–61.
[15] Dunlop SP, Jenkins D, Neal KR, et al. Relative importance of enterochromaffin cell hyper-plasia, anxiety, and depression in postinfectious IBS. Gastroenterology 2003;125(6):1651–9.
[16] Devinsky O, Morrell MJ, Vogt BA. Contributions of anterior cingulate cortex to behaviour.Brain 1995;118(Pt 1):279–306.
[17] Labus JS, Bolus R, Chang L, et al. The Visceral Sensitivity Index: development and valida-tion of a gastrointestinal symptom-specific anxiety scale. Aliment Pharmacol Ther2004;20(1):89–97.
[18] Labus JS, Mayer EA, Chang L, et al. The central role of gastrointestinal-specific anxiety inirritable bowel syndrome: further validation of the visceral sensitivity index. PsychosomMed 2007;69(1):89–98.
[19] Walker EA, Katon WJ, Jemelka RP, et al. Comorbidity of gastrointestinal complaints,depression, and anxiety in the Epidemiologic Catchment Area (ECA) Study. Am J Med1992;92(1A):26S–30S.
[20] Drossman DA, Camilleri M, Mayer EA, et al. AGA technical review on irritable bowelsyndrome. Gastroenterology 2002;123(6):2108–31.
[21] American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders,4th Edition, Text-Revision. 4th edition. Washington, DC: American Psychiatric Press;2000.
[22] North CS, Downs D, Clouse RE, et al. The presentation of irritable bowel syndrome in thecontext of somatization disorder. Clin Gastroenterol Hepatol 2004;2(9):787–95.
[23] Spiegel BM, Kanwal F, Naliboff B, et al. The impact of somatization on the use of gastro-intestinal health-care resources in patients with irritable bowel syndrome. Am J Gastroen-terol 2005;100(10):2262–73.
[24] Lembo A, Ameen VZ, Drossman DA. Irritable bowel syndrome: toward an understandingof severity. Clin Gastroenterol Hepatol 2005;3(8):717–25.
[25] Drossman DA, Whitehead WE, Toner BB, et al. What determines severity among patientswith painful functional bowel disorders? Am J Gastroenterol 2000;95(4):974–80.
[26] Spiegel BM, Strickland A, Chang L. Predictors of patient-assessed illness severity in irritablebowel syndrome (IBS)—DDW abstract. Gastroenterology 2007;132:A-680.
[27] Chang L, Heitkemper MM. Gender differences in irritable bowel syndrome. Gastroenter-ology 2002;123(5):1686–701.
[28] Gwee KA. Irritable bowel syndrome in developing countries: a disorder of civilization orcolonization? Neurogastroenterol Motil 2005;17(3):317–24.
[29] Coffin B, Dapoigny M, Cloarec D, et al. Relationship between severity of symptoms andquality of life in 858 patients with irritable bowel syndrome. Gastroenterol Clin Biol2004;28(1):11–5.
682 VIDELOCK & CHANG
[30] van der Horst HE, van Dulmen AM, Schellevis FG, et al. Do patients with irritable bowelsyndrome in primary care really differ from outpatients with irritable bowel syndrome?Gut 1997;41(5):669–74.
[31] Lee OY, Mayer EA, Schmulson M, et al. Gender-related differences in IBS symptoms. AmJ Gastroenterol 2001;96(7):2184–93.
[32] Simren M, Abrahamsson H, Svedlund J, et al. Quality of life in patients with irritable bowelsyndrome seen in referral centers versus primary care: the impact of gender and predom-inant bowel pattern. Scand J Gastroenterol 2001;36(5):545–52.
[33] Corney RH, Stanton R. Physical symptom severity, psychological and social dysfunction ina series of outpatients with irritable bowel syndrome. J Psychosom Res 1990;34(5):483–91.
[34] Talley NJ, Boyce P, Jones M. Identification of distinct upper and lower gastrointestinal symp-tom groupings in an urban population. Gut 1998;42(5):690–5.
[35] Talley NJ, Zinsmeister AR, Melton LJ III. Irritable bowel syndrome in a community: symptomsubgroups, risk factors, and health care utilization. Am J Epidemiol 1995;142(1):76–83.
[36] Heitkemper M, Jarrett M, Bond EF, et al. Impact of sex and gender on irritable bowel syn-drome. Biol Res Nurs 2003;5(1):56–65.
[37] Houghton LA, Lea R, Jackson N, et al. The menstrual cycle affects rectal sensitivity inpatients with irritable bowel syndrome but not healthy volunteers. Gut 2002;50(4):471–4.
[38] Camilleri M. Therapeutic approach to the patient with irritable bowel syndrome. Am J Med1999;107(5A):27S–32S.
[39] Chang L,AmeenVZ,DukesGE,etal.Adose-ranging,phase II studyof theefficacyand safetyof alosetron in men with diarrhea-predominant IBS. Am J Gastroenterol 2005;100(1):115–23.
[40] Whitehead WE. Development and validation of the ROME III diagnostic questionaire. In:Drossman DA, Corazziar E, Delvaux M, et al, editors. Rome III: the functional gastrointes-tinal disorders. Durham (NC): Degnon; 2006. p. 835–53.
[41] Whitehead WE, Palsson OS, Feld AD, et al. Utility of red flag symptom exclusions in thediagnosis of irritable bowel syndrome. Aliment Pharmacol Ther 2006;24(1):137–46.
[42] Cash BD, Chey WD. Irritable bowel syndrome: an evidence-based approach to diagnosis.Aliment Pharmacol Ther 2004;19(12):1235–45.
[43] Cash BD, Schoenfeld P, Chey WD. The utility of diagnostic tests in irritable bowel syndromepatients: a systematic review. Am J Gastroenterol 2002;97(11):2812–9.
[44] Spiegel BM, Gralnek IM, Bolus R, et al. Is a negative colonoscopy associated with reassur-ance or improved health-related quality of life in irritable bowel syndrome? GastrointestEndosc 2005;62(6):892–9.
[45] Spiegel BM, DeRosa VP, Gralnek IM, et al. Testing for celiac sprue in irritable bowelsyndrome with predominant diarrhea: a cost-effectiveness analysis. Gastroenterology2004;126(7):1721–32.
[46] Pimentel M, Chow EJ, Lin HC. Eradication of small intestinal bacterial overgrowth reducessymptoms of irritable bowel syndrome. Am J Gastroenterol 2000;95(12):3503–6.
[47] Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breath testing correlates withsymptom improvement in irritable bowel syndrome: a double-blind, randomized,placebo-controlled study. Am J Gastroenterol 2003;98(2):412–9.
[48] Suarez FL, Savaiano DA, Levitt MD. A comparison of symptoms after the consumption ofmilk or lactose-hydrolyzed milk by people with self-reported severe lactose intolerance.N Engl J Med 1995;333(1):1–4.
[49] Parker TJ, Woolner JT, Prevost AT, et al. Irritable bowel syndrome: is the search for lactoseintolerance justified? Eur J Gastroenterol Hepatol 2001;13(3):219–25.
[50] Tolliver BA, Jackson MS, Jackson KL, et al. Does lactose maldigestion really play a role inthe irritable bowel? J Clin Gastroenterol 1996;23(1):15–7.
[51] Stewart M, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes.J Fam Pract 2000;49(9):796–804.
683IRRITABLE BOWEL SYNDROME
[52] Drossman DA. Diagnosing and treating patients with refractory functional gastrointestinaldisorders. Ann Intern Med 1995;123(9):688–97.
[53] Chang L, Drossman D. Optimizing patient care: the psychological interview in irritablebowel syndrome. Clinical Perspectives 2002;5(6):336–42.
[54] Hunter JO, Whorwell PJ, Atkinson W, et al. Food elimination in IBS: the case for IgG testingremains doubtful. Author’s reply. Gut 2005;54(8):1203.
[55] Atkinson W, Sheldon TA, Shaath N, et al. Food elimination based on IgG antibodies inirritable bowel syndrome: a randomised controlled trial. Gut 2004;53(10):1459–64.
[56] Brandt LJ, Bjorkman D, Fennerty MB, et al. Systematic review on the management of irrita-ble bowel syndrome in North America. Am J Gastroenterol 2002;97(Suppl 11):S7–26.
[57] Schoenfeld P. Efficacy of current drug therapies in irritable bowel syndrome: what worksand does not work. Gastroenterol Clin North Am 2005;34(2):319–35, viii.
[58] Bijkerk CJ, Muris JW, Knottnerus JA, et al. Systematic review: the role of different types offibre in the treatment of irritable bowel syndrome. Aliment Pharmacol Ther 2004;19(3):245–51.
[59] Poynard T, Regimbeau C, Benhamou Y. Meta-analysis of smooth muscle relaxants in thetreatment of irritable bowel syndrome. Aliment Pharmacol Ther 2001;15(3):355–61.
[60] Wheatley D. Irritable colon syndrome treated with an antispasmodic drug. Practitioner1976;217(1298):276–80.
[61] Ritchie JA, Truelove SC. Treatment of irritable bowel syndrome with lorazepam, hyoscinebutylbromide, and ispaghula husk. Br Med J 1979;1(6160):376–8.
[62] Page JG, Dirnberger GM. Treatment of the irritable bowel syndrome with Bentyl (dicyclo-mine hydrochloride). J Clin Gastroenterol 1981;3(2):153–6.
[63] Coffin B, Farmachidi JP, Rueegg P, et al. Tegaserod, a 5-HT4 receptor partial agonist,decreases sensitivity to rectal distension in healthy subjects. Aliment Pharmacol Ther2003;17(4):577–85.
[64] Prather CM, Camilleri M, Zinsmeister AR, et al. Tegaserod accelerates orocecal transit in pa-tients with constipation-predominant irritable bowel syndrome. Gastroenterology2000;118(3):463–8.
[65] Muller-Lissner SA, Fumagalli I, Bardhan KD, et al. Tegaserod, a 5-HT(4) receptor partialagonist, relieves symptoms in irritable bowel syndrome patients with abdominal pain,bloating and constipation. Aliment Pharmacol Ther 2001;15(10):1655–66.
[66] Novick J, Miner P, Krause R, et al. A randomized, double-blind, placebo-controlled trial oftegaserod in female patients suffering from irritable bowel syndrome with constipation.Aliment Pharmacol Ther 2002;16(11):1877–88.
[67] Kellow J, Lee OY, Chang FY, et al. An Asia-Pacific, double blind, placebo controlled, rand-omised study to evaluate the efficacy, safety, and tolerability of tegaserod in patients withirritable bowel syndrome. Gut 2003;52(5):671–6.
[68] Whorwell PJ, Krumholz S, Mueller-Lissner S. Tegaserod has a favorable safety and tolera-bility profile in patients with constipation predominant and alternating forms of irritablebowel syndrome. Gastroenterology 2000;118(4):A1204.
[69] Bardhan KD, Forbes A, Marsden CL, et al. The effects of withdrawing tegaserod treatmentin comparison with continuous treatment in irritable bowel syndrome patients with abdom-inal pain/discomfort, bloating and constipation: a clinical study. Aliment Pharmacol Ther2004;20(2):213–22.
[70] Tack J, Muller-Lissner S, Bytzer P, et al. A randomised controlled trial assessing the efficacyand safety of repeated tegaserod therapy in women with irritable bowel syndrome withconstipation. Gut 2005;54(12):1707–13.
[71] Reilly MC, Barghout V, McBurney CR, et al. Effect of tegaserod on work and daily activityin irritable bowel syndrome with constipation. Aliment Pharmacol Ther 2005;22(5):373–80.
[72] Harris L, Chang L. Alosetron: an effective treatment for diarrhea-predominant irritablebowel syndrome. Womens Health 2007;3(1):15–27.
684 VIDELOCK & CHANG
[73] Chang L, Chey WD, Harris L, et al. Incidence of ischemic colitis and serious complicationsof constipation among patients using alosetron: systematic review of clinical trials andpost-marketing surveillance data. Am J Gastroenterol 2006;101(5):1069–79.
[74] Chey WD, Chey WY, Heath AT, et al. Long-term safety and efficacy of alosetron in womenwith severe diarrhea-predominant irritable bowel syndrome. Am J Gastroenterol2004;99(11):2195–203.
[75] Drossman DA, Toner BB, Whitehead WE, et al. Cognitive-behavioral therapy versuseducation and desipramine versus placebo for moderate to severe functional boweldisorders. Gastroenterology 2003;125(1):19–31.
[76] Tabas G, Beaves M, Wang J. Paroxetine to treat irritable bowel syndrome not respondingto high-fiber diet: a double-blind, placebo-controlled trial. Am J Gastroenterol 2004;99:914–20.
[77] Vahedi H, Merat S, Rashidioon A, et al. The effect of fluoxetine in patients with pain andconstipation-predominant irritable bowel syndrome: a double-blind randomized-controlled study. Aliment Pharmacol Ther 2005;22(5):381–5.
[78] Tack J, Broekaert D, Fischler B, et al. A controlled crossover study of the selective serotoninreuptake inhibitor citalopram in irritable bowel syndrome. Gut 2006;55(8):1095–103.
[79] Creed F, Fernandes L, Guthrie E, et al. The cost-effectiveness of psychotherapy and parox-etine for severe irritable bowel syndrome. Gastroenterology 2003;124(2):303–17.
[80] Pimentel M, Park S, Mirocha J, et al. The effect of a nonabsorbed oral antibiotic (rifaximin)on the symptoms of the irritable bowel syndrome. Ann Intern Med 2006;145:557–63.
[81] Camilleri M. Probiotics and irritable bowel syndrome: rationale, putative mechanisms, andevidence of clinical efficacy. J Clin Gastroenterol 2006;40(3):264–9.
[82] O’Mahony L, McCarthy J, Kelly P, et al. Lactobacillus and bifidobacterium in irritablebowel syndrome: symptom responses and relationship to cytokine profiles. Gastroenterol-ogy 2005;128(3):541–51.
[83] Whorwell PJ, Altringer L, Morel J, et al. Efficacy of an encapsulated probiotic Bifidobacte-rium infantis 35624 in women with irritable bowel syndrome. Am J Gastroenterol2006;101(7):1581–90.
[84] Kim HJ, Camilleri M, McKinzie S, et al. A randomized controlled trial of a probiotic,VSL#3, on gut transit and symptoms in diarrhoea-predominant irritable bowel syndrome.Aliment Pharmacol Ther 2003;17(7):895–904.
[85] Kim HJ, Vazquez Roque MI, Camilleri M, et al. A randomized controlled trial of a probioticcombination VSL# 3 and placebo in irritable bowel syndrome with bloating. Neurogas-troenterol Motil 2005;17(5):687–96.
[86] Kajander K, Hatakka K, Poussa T, et al. A probiotic mixture alleviates symptoms in irritablebowel syndrome patients: a controlled 6-month intervention. Aliment Pharmacol Ther2005;22(5):387–94.
[87] Johanson JF, Gargano M, Holland P. Phase III efficacy and safety of RU-0211, a novelchloride channel activator, for the treatment of constipation. Gastroenterology 2003;124(Suppl 1):A48.
[88] Johanson JF, Gargano M, Holland P. Phase III patient assessments of the effects of lubipro-stone, chloride channel-s (ClC-2) activator, for the treatment of constipation [abstract 899].Am J Gastroenterol 2005;100(S-329).
[89] Meyers NL, Palmer RMJ, George A. Efficacy and safety of renzapride in patients withconstipation-predominant IBS: a phase IIb study in the UK primary healthcare setting. Gas-troenterology 2004;126:A-640.
[90] Camilleri M, McKinzie S, Fox J, et al. Effect of renzapride on transit in constipation-predom-inant irritable bowel syndrome. Clin Gastroenterol Hepatol 2004;2(10):895–904.
[91] Tack J, Middleton SJ, Horne MC, et al. Pilot study of the efficacy of renzapride on gastro-intestinal motility and symptoms in patients with constipation-predominant irritable bowelsyndrome. Aliment Pharmacol Ther 2006;23(11):1655–65.
685IRRITABLE BOWEL SYNDROME
[92] Hutton J. Cognitive behaviour therapy for irritable bowel syndrome. Eur J GastroenterolHepatol 2005;17(1):11–4.
[93] Boyce PM, Talley NJ, Balaam B, et al. A randomized controlled trial of cognitive behaviortherapy, relaxation training, and routine clinical care for the irritable bowel syndrome. AmJ Gastroenterol 2003;98(10):2209–18.
[94] Whorwell PJ. Review article: the history of hypnotherapy and its role in the irritable bowelsyndrome. Aliment Pharmacol Ther 2005;22(11–12):1061–7.
[95] Wilson S, Maddison T, Roberts L, et al. Systematic review: the effectiveness of hypnother-apy in the management of irritable bowel syndrome. Aliment Pharmacol Ther 2006;24(5):769–80.
[96] Lim B, Manheimer E, Lao L, et al. Acupuncture for treatment of irritable bowel syndrome.Cochrane Database Syst Rev 2006;4:CD0051111.
[97] Bensoussan A, Talley NJ, Hing M, et al. Treatment of irritable bowel syndrome withChinese herbal medicine: a randomized controlled trial. JAMA 1998;280(18):1585–9.
[98] Spanier JA, Howden CW, Jones MP. A systematic review of alternative therapies in the ir-ritable bowel syndrome. Arch Intern Med 2003;163(3):265–74.
[99] Bundy R, Walker AF, Middleton RW, et al. Artichoke leaf extract reduces symptoms of irri-table bowel syndrome and improves quality of life in otherwise healthy volunteers sufferingfrom concomitant dyspepsia: a subset analysis. J Altern Complement Med 2004;10(4):667–9.
[100] Vejdani R, Shalmani HR, Mir-Fattahi M, et al. The efficacy of an herbal medicine, Carmint,on the relief of abdominal pain and bloating in patients with irritable bowel syndrome: a pi-lot study. Dig Dis Sci 2006;51(8):1501–7.
[101] Madisch A, Holtmann G, Plein K, et al. Treatment of irritable bowel syndrome with herbalpreparations: results of a double-blind, randomized, placebo-controlled, multi-centre trial.Aliment Pharmacol Ther 2004;19(3):271–9.
[102] Lu WZ, Gwee KA, Moochhalla S, et al. Melatonin improves bowel symptoms in femalepatients with irritable bowel syndrome: a double-blind placebo-controlled study. AlimentPharmacol Ther 2005;22(10):927–34.
[103] Song GH, Leng PH, Gwee KA, et al. Melatonin improves abdominal pain in irritable bowelsyndrome patients who have sleep disturbances: a randomised, double blind, placebocontrolled study. Gut 2005;54(10):1402–7.





























