Embed Size (px)
Citation preview

Gut, 1969, 10, 779-786
Gastric secretion after massive small bowelresection
COLIN W. 0. WINDSOR, J. FEJFAR, AND D. A. K. WOODWARD
From the Department of Surgery, Queen Elizabeth Hospital, Birmingham
SUMMARY This paper confirms that gastric hypersecretion can occur in man and dogs after massiveintestinal resection. The assumption, made by others, that hypersecretion in the clinical situationis similar to that observed in dogs is challenged.An acute hypersecretory state occurred in eight of 19 patients after massive intestinal resection.
This was apparent as an increased rate of basal secretion. It was usually transient and unrelated tothe length of intestine resected. A correlation was noticed between hypersecretion and jaundicein the immediate postoperative period. Histamine release after acute hepatic injury was postulatedas the cause of the hypersecretion.By contrast a chronic gastric hypersecretory state was demonstrated in dogs after massive
intestinal resection. The rate of basal secretion was not significantly altered. The increased dailyacid output was shown to be due to prolonged and enhanced response to food. The cause wasthought to be loss of inhibitory agents, such as enterogastrone, normally released by the smallintestine when in contact with food. The rationale of performing vagotomy and pyloroplasty at thesame time as the intestinal resection is questioned.
A possibly important complication of massive smallbowel resection, gastric hypersecretion, has recentlybeen described in man (Frederick, Sizer, andOsborne, 1965; Osborne, Frederick, Sizer, Blair,Cole, and Thum, 1966; Aber, Ashton, Carmalt, andWhitehead, 1967; Grundberg, Lopez, and Dragstedt,1967). Other workers have demonstrated hyper-secretion of acid from Heidenhain pouches in dogsafter massive intestinal resection (Landor and Baker,1964; Westerheide, Elliott, and Hardacre, 1965;Reul and Ellison, 1966; Kerr, Elliott, and Endahl,1968).In patients neither the incidence nor the character-
istics of the hypersecretion have been described,although it has been evident as massive aspirationsstarting in the immediate postoperative period. Thedog studies reported in the literature have constantlyshown an increase in the daily acid output fromgastric pouches; however, estimations of the basalrate of secretion and histamine responses have failedto show significant changes after resection leavingthe cause of the increased acid output speculative.
In this paper 19 patients have been studied aftermassive intestinal resection, that is, by definition,resection of more than a third or 300 cm of smallintestine (Haymond, 1935; Pullan, 1959). In addition
eight dogs, five with Heidenhain pouches and threewith Pavlov pouches, have had gastric investigationsbefore and after 75% intestinal resection. The resultsshow that the hypersecretion seen in patients afterresection has different characteristics to thatobserved in dogs. The possible explanation of thesedifferences is discussed.
MATERIALS AND METHODS
Nineteen patients aged between 12 and 68 years admittedto hospitals in the Birmingham region between 1963 and1968 have been studied. All had massive intestinal re-sections, for the reasons shown in Table I. Seven havehad gastric function studies performed since resection.The data from the immediate postoperative period havebeen retrospective in all but four instances. In fourpatients no record existed of the aspirate; however,questioning of the surgeons concerned confirmed thathypersecretion was not a problem in these particularpatients.The normal basal rate of gastric secretion in man is up
to 1,500 ml per day containing up to 120 m-equiv ofhydrochloric acid (Wright, 1952; Dragstedt, Woodward,Storer, Oberhelman, and Smith, 1950; Allen, 1959).Surgery normally produces a slight increase in basalsecretion (Dragstedt, Ragins, Dragstedt, and Evans,1956). In order to define normal aspirations, data were
779
on April 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.10.10.779 on 1 O
ctober 1969. Dow
nloaded from

Colin W. 0. Windsor, J. Fejfar, and D. A. K. Woodward
collected from 50 patients undergoing uncomplicatedabdominal surgery. The peak daily volume of aspiratesranged between 100 and 1,500 ml per day with a mean of750 ml/day. For these reasons aspirates in excess of1-5 litres/day, especially if containing more than 120m-equiv of HCI, have been judged to be abnormal. Thesecriteria maybe open to criticism but have provided a base-line necessary to define a hypersecretory state.
Gastric function studies were performed using sub-cutaneous pentagastrin (6 ,ug/kg body weight). Studieswere made six weeks to two years after resection.
Eight mongrel bitches weighing between 16 and 26 kgwere used for the studies of gastric secretion. Heidenhainpouches were made by the method ofDe Vito and Harkins(1959) and the Pavlov pouches by the method describedbyPerry, Salmon, Griffen, Root, and Wangensteen (1959).The completeness of vagal innervation was checked byinsulin testing.
After recovery from the pouch operations base-linestudies were made for a period of one month. Then a 75%resection of the small intestine was performed with pre-servation of the ileocaecal valve; the resection left theduodenum and first part of the jejunum intact. Pouchcollections were started one week after this operation andcontinued for at least a month. All dogs were fed astandard diet throughout the experiment with sodium andpotassium supplements. The following tests of gastricfunction were made: (1) 24-hour collections of pouchsecretion; (2) basal secretory rate, estimated at least fourtimes in each phase of the experiment after a 31-hourfast; (3) postcibal acid output, measured hourly for sixhours after a standard meat meal; (4) maximal acid out-put, determined in response to an injection of histaminephosphate (0.1 mg/kg body weight). At least two testswere performed in each phase of the experiment.
Hydrochloric acid was measured in all specimens bytitration with NaOH to pH 7 using autotitration equip-ment.'
RESULTS
CLINICAL STUDY Table I shows the peak dailyaspirates in the 19 patients. Eight had aspirates inexcess of 1.5 litres per day, the peak volumes beingbetween 1.9 and 4.1 litres per day (mean 3.1 litres).In the remaining 11 patients the peak volumes werebelow 1.5 litres; by the criteria laid down theseaspirates were not abnormal.Hydrogen ion losses in the aspirates were measured
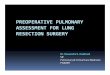
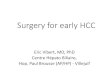
on four patients (Table II) and ranged between62.5 m-equiv/day and 480 m-equiv/day. In allinstances aspirates were bile stained, suggesting thatsome acid had been neutralized, yet in three the out-put was in excess of that expected from duodenalulcer patients. Figure 1 shows the daily aspirates of atypical patient (case 1).
In two other patients with a hypersecretory trend(cases 4 and 6) the pH of aspirates was less than
'Radiometer Copenhagen.
Case DiagnosisNo.
23
4
5
6
7
8
9
10
11
1213141S16
1718
19
TABLE 1CLINICAL DATA
Length of OutcomeSmall BowelRemaining(cm)
Superior mesenteric 40artery embolusPelvic carcinoma 200Superior mesenteric 40artery embolusSuperior mesenteric 300artery embolusSuperior mesenteric 120artery thrombosisSuperior mesenteric 400vein thrombosisSuperior mesenteric 90artery embolusSuperior mesenteric 150vein thrombosisSuperior mesenteric 15artery thrombosisSuperior mesenteric 20vein thrombosisSuperior mesenteric 40artery embolusTrauma 200Trauma 110Internal strangulation 120Internal strangulation 400Superior mesenteric 90artery embolusMesenteric tumour 120Superior mesenteric 5artery embolusSuperior mesenteric 40artery embolus
TABLE IIPEAK DAILY HYDROCHLORIC ACID
ASPIRATES
Patient No.
1237
MaximumAspiration(ml/day)
Died twelfth 4,160daySurvived 3,800Died sixth 2,319dayDied sixth 2,950daySurvived 3,590
Survived 3,800
Died fifth 3,010daySurvived 1,985
Died seventh 1,432daySurvived 394
Survived No record
SurvivedSurvivedSurvivedSurvivedSurvived
SurvivedSurvived
Survived
190No recordNo recordNo record1,190
500Smallquantities500
LOSSES IN GASTRIC
Peak Daily Loss(HCl m-equiv/day)
480238625240
2. In the remaining two patients there were no dataon the hydrogen ion losses.On this evidence it is suggested that all eight
patients with massive aspirates had a hypersecretorystate. As this was evident in the immediate post-operative period, with restriction of oral input to afew hundred millilitres of water per day, it is likelythat the hypersecretion is due to an increase of thebasal rate of acid secretion.Length of resected intestine Nine patients had
resections leaving 90 cm or less of small intestine.Three developed hypersecretion, six did not (Table1). This suggests that factors other than the resectionmay be responsible for the hypersecretion.
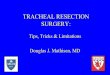
Onset and duration Figure 2 shows the time of
780
on April 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.10.10.779 on 1 O
ctober 1969. Dow
nloaded from

Gastric secretion after massive small bowel resection
Metabolic alkalosis(pH up to 7.59)
>, Resection
4 . as 3 ~~~~~~~~~DiedQ~ 2 . | 1~ 480 mEq.HCI Normal
O- w - maximum0_
0 2 4 6 8 10 12 14
Embolectomy Days
FIG. 1. Daily gastric aspirates from case 1, showing a
persistent hypersecretory state associated with a metabolicalkalosis. This patient also had a low serum potassiumlevel (< 3 m-equiv/l).
12345678
0Resection
1 1
1 11 1ME
1 -1
2 4 6 8 10 12 14 40Days
FIG. 2. Onset and duration of the hypersecretory phase.Patients 1 to 8 are represented as horizontal bars indicatingthe postoperative period during which massive aspiratesoccurred. Dark bars denote patients who died.
onset and the duration of the hypersecretory trend.Each patient is represented by a horizontal line. Ineach instance the onset was within four days ofresection and persisted in one case for up to 40 days.Usually, however, it was a transient phenomenonlasting less than 14 days.
Liver function Perhaps the most striking findingsas a result of the liver function studies (Table III)were that six of the 19 patients had elevated bilirubinlevels and each of these developed a hypersecretorystate. There was no evidence that the remainingpatients had abnormal liver function, or jaundice.It is here that the weakness of a retrospective studybecomes apparent since Tablem summarizes all theliver function tests carried out on these patients.However, it is suggested that gastric hypersecretionafter massive intestinal resection is fairly well cor-related with evidence of hepatic parenchymal celldamage and elevated bilirubin levels.
Gastric function Table IV shows the results of-seven gastric function studies in the survivors; noneof these patients showed evidence of hypersecretionin the immediate postoperative period. The range of-the basal output (0.6 to 5.6 m-equiv hydrochloric
TABLE IVRESULTS OF GASTRIC FUNCTION STUDIES IN SURVIVORS
AFTER MASSIVE INTESTINAL RESECTION
Case No. Basal Rate Peak Acid(m-equiv/hour) Output
10111213141617
3-64.70-63-8561*11-1
32-519-711-215-428-15.0
24-0
acid per hour) is within the normal range for ourlaboratory as is the peak acid output (5 to32.5 m-equiv hydrochloric acid per hour). There isno evidence that survivors after massive resection,in whom there was no evidence of postoperativehypersecretion, have hypochlorhydria or a raisedbasal secretory rate.
DOG STUDIES The tests of gastric functions gave thefollowing results.
Daily acid output Table V shows the daily acidoutput before and after 75% intestinal resection inthe Heidenhain and Pavlov pouch dogs. One dog,
TABLE IIIRESULTS OF LIVER FUNCTION STUDIES
Case MaximumNo. Aspirate
(mil/day)
4,1603,8002,9503,8003,0101,985
Bilirubin SGPT(mg/100 ml) Units
2-6-4-71*2-9-13.412
16-16-6
850
85022
120+
SGOT AlkalineUnits Phosphatase
(King-ArmstrongUnits)
66042
200 +
16-9
157.5
Thymol ZincFlocculation Turbidity
(Normal1-6)
- - 2-1- - 2-4
++ - 3.4- 3-- 3-1
2.467.8
Lowest LowestAlbumin Level Globulin Level(glCOO ml) (gl100 ml)
1*63-0
2-22-9
781
r---i
on April 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.10.10.779 on 1 O
ctober 1969. Dow
nloaded from

Colin W. 0. Windsor, J. Fejfar, and D. A. K. Woodward
TABLE VDAILY ACID OUTPUT FROM HEIDENHAIN AND PAVLOV POUCHES BEFORE AND AFTER MASSIVE RESECTION
Dog Collection before and No. oJ Mean ChangeNo. qfter Resection Observations (m-equiv/day) (m-equiv/day)
102 BeforeAfter
103 BeforeAfter
105 BeforeAfter
106 BeforeAfter
114 BeforeAfter
121 BeforeAfter
122 BeforeAfter
123 BeforeAfter
3129229342724302331
261726133313
4-8812-718-33
21-069.9513-007-8714-957-236-43
10-334.926-740.37-113-8
+ 7-38
+ 12-73
+ 305
+ 706
- 0-8
+ 24-6
+ 13-6
+ 6-7
< 0o001
< 0-001
< 0.25
< 0001
< 0.25
< 0-001
< 0-001
< 0-01
no. 114, did not show an increased acid output; thereason for this is not apparent from this study. Theremainder of the animals markedly increased theirdaily output.
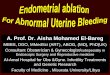
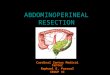
Postcibal response Figure 3 shows the results oftest meals in the Heidenhain and Pavlov pouch dogsbefore and after resection. The control curves are themean of 35 studies (Heidenhain pouch) and eightstudies (Pavlov pouch) and 22 and eight studiesrespectively in the resected animals. Each pointrepresents the mean hourly output for the group, thestandard error being shown as vertical bars.
Intestinal resection prolongs the acid responseafter food. In the Heidenhain pouch dogs the peakoutput has moved from the third hour to the fourthhour, but the peaks are not statistically different. Thepost-resection curve follows the normal pattern for
HEIDENHAIN pouches
the first three hours, continues to rise, and shows astatistically significant difference from controls in thesixth hour (fifth hour 0 1 > p > 0.05, sixth hour0.01 > p > 0001). The differences in the acid outputbetween the total six-hour period before and afterresection (1.8 m-equiv and 2.5 m-equiv) is notstatistically significant. In the Pavlov pouch dogs asimilar curve is seen, acid output in the resected dogsbeing significantly greater than control in the fourth,fifth, and sixth hours (fourth hour 0.05 > p > 002,fifth hour 001 > p > 0001, sixth hour P < 0001).
Basal secretory rate In five dogs there was a smallincrease in the basal rate of secretion, in two adecrease, and in one no change (Table VI). Statisticalanalysis of the group and of individual dogs showsno statistical significance in these changes (t test ondifference of means to zero, t 1.71; p > 0 1O.)
PAVLOV pouches
0.81
060
04[
4
3
2
02
0 1 2 3 4 5 6
Postresection FIG. 3. Postcibal acid output in
Heidenhain and Pavlov pouch dogsbefore (control) and after 75%intestinal resection. The curves arethe means for all dogs in thegroups. The standard error isshown as vertical bars.
PControl
O 1 2 3 4 5 6Hours
782
Type ofPouch
Heidenhain
Pavlov
c0
0)
KL)
Eu11
on April 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.10.10.779 on 1 O
ctober 1969. Dow
nloaded from

Gastric secretion after massive small bowel resection
TABLE VIEFFECT OF INTESTINAL RESECTION ON THE BASAL SECRETORY RATE AND RESPONSE TO HISTAMINE
Dog Collections Basal Rate Peak Histamine ResponseNo. before and after (m-equiv HClIhour) Change (m-equiv HCl/hour) Change
Resection (m-equiv HCI/hour) (m-equiv HCl/hour)
102
103
105
106
114
121
122
123
BeforeAfterBeforeAfterBeforeAfterBeforeAfterBeforeAfter
BeforeAfterBeforeAfterBeforeAfter
0-010-080.010-240-020-010-040050-010-01
1.21.72-11-30-010-02
+ 007
+ 0-23
- 0-01
+ 0-01
0
1-121-691-024031*611.212-362-673.134.9
+ 048
+ 3-01
- 04
+ 031
+ 1.77
+ 05
- 08
+ 0-02
Histamine response In four dogs there was anincrease in the peak response to histamine (0 1 mg/kghistamine phosphate) and in one a decrease (TableVI). The greatest increase (dog 103 + 3.01 m-equiv/hour) is not statistically significant (t 2.11, p > 0 10).Comparison of the group before and after resectionshows a mean increase of 1-03 m-equiv/hour whichagain is not statistically significant (p > 0.1).
DISCUSSION
CLINICAL STUDY Postoperative gastric hypersecre-tlOIi was observed in eight of 19 patients aftermassive small intestinal resection. This was evidentas an increase in the basal secretory rate beginningwithin four days of resection. The duration of thehypersecretion was usually less than two weeks butin one instance it persisted for 40 days.
These was no relationship between the length ofresected intestine and the appearance of hyper-secretion. This suggests that factors other than theremoval of bowel are responsible for the phenom-enon. In the following paragraphs consideration isgiven to possible causes of hypersecretion which maybe important if resection is not the prime cause.These are the effects on gastric secretion of surgery,infection, acid base disturbances, and deranged liverfunction.
Dragstedt et al (1956) found a slight increase inthe basal rate of gastric secretion after operation insix of 13 patients studied. They suggested that thiswas due to an increase of vagal tone as it was notapparent in patients after vagotomy. 'Surgical stress'is known to increase adrenal, medullary, and cortical
secretions (Hume, 1957). The effects of ACTH andcorticoids on human gastric secretion have beenconflicting, some showing a slight increase insecretion (Gray, Benson, Reifenstein, and Spiro,1951) and others a decrease (Hirschowitz, Streeten,Pollard, and Boldt, 1955). It is thought unlikely,therefore, that surgery or 'surgical stress' would causehypersecretion of the magnitude seen in thesepatients.
Peritonitis, and in some instances septicaemnia,complicated the postoperative course of somepatients; however, extensive studies over the yearshave repeatedly shown that bacterial infection sup-presses gastric secretion (Bandes, Hollander, andBierman, 1948; Blickenstaff and Grossman, 1950).Any coincident infection would therefore be expectedto suppress the hypersecretion.Four of the patients with hypersecretion had a
marked metabolic alkalosis and low serum potas-sium levels. Alkalosis has been shown to decreasethe basal acid output (Byers, Jordan, and Maren,1961) and a low serum potassium is known to sup-press gastric secretion (Carrone and Cooke, 1953;Muro, Rowinski, Calaresu, and Fraghi, 1961).Depletion of hydrochloric acid by continuous gastricaspiration has, however, been shown to induce ametabolic alkalosis and simultaneously increaserenal potassium losses, leading to a hypokalaemicalkalosis (Needle, Kaloyanides, and Schwartz, 1964;Kassirer and Schwartz, 1966). The electrolytechanges encountered in our patients are thereforethought to be secondary to the hydrochloric acidloss.
There was a correlation in this series of patientsbetween biochemical evidence of liver damage and
Type ofPouch
Heidenhain
Pavlov
783
on April 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.10.10.779 on 1 O
ctober 1969. Dow
nloaded from

Colin W. 0. Windsor, J. Fejfar, and D. A. K. Woodward
gastric hypersecretion. Is it possible to link intestinalresection, particularly ofgangrenous gut in a shockedpatient, with hepatic cell injury? In 1932 Cole andElman showed in dogs that strangulated loops ofsmall intestine caused centrilobular liver cell necrosiswithout evidence of bacterial invasion of the liver.Resection of normal intestine from dogs has, how-ever, been shown to have no effect on liver functionor histology (Landor and Baker, 1964; Frederick etal, 1965). Boyce (1941) found that of 715 patientswith intestinal obstruction, 23 had biochemicalevidence of liver damage. Other factors such as myo-cardial infarction and hypotension are known toresult in liver damage (Sherlock, 1951; Schalm andHoogenboom, 1952). From this evidence it seemspossible that a combination of factors such as in-farcted or strangulated intestine, and liver anoxiadue to hypotension could lead to liver damage of atype noted in our patients.
Is it possible that the liver damage is the cause ofthe hypersecretion? Again a link has been estab-lished. Pikula and Dunphy (1959) demonstratedhepatic cell damage after bile duct ligation and morerecently Silen, Hein, Albo, and Harper (1963) haveproduced gastric hypersecretion by bile duct ligationin dogs. These experiments would suggest thathepatic cellular damage causes gastric hypersecre-tion. Apparently conflicting evidence (Orloff andWindsor, 1966) has shown that liver damage in dogsresults in gastric hyposecretion. However, in thisexperiment the liver damage was produced bychronic venous congestion. It is now thoughtpossible that acute liver damage and chronic liverdamage have different effects on gastric secretionwhich could account for the difference between thisand other reports (Skillman, Silen, Harper, Neely,and Simmons, 1961; Hein, Silen, Skillman, andHarper, 1963). Recent studies have shown that portalvein infusions of small doses of carbon tetrachloride(0.1 mg/kg body weight daily), in dogs with Heiden-hain pouches, produce gastric hypersecretion withinseven to 10 days (Baddeley, 1968). The hypersecre-tion was coincident with biochemical evidence ofliver failure and was evident as an increase in thebasal secretory rate. The hypersecretion was thoughtto be due to acute damage of the hepatic parenchymawith a coincident release of secretory agents.Previous workers have also suggested that acutehepatic injury releases histamine from the liver(Anrep and Barsoum, 1953; Anrep, Barsoum, andTalaat, 1953).
It seems likely that release of a secretagogue,possibly histamine, from the acutely damaged liveris the cause of the elevated basal secretory ratedescribed in these patients with hypersecretion.The gastric function studies carried out on the
survivors in Table IV show that both the basal rateand the peak acid output are within the normal rangeafter massive resection. This suggests that nopermanent changes occur in the parietal cell popula-tion after resection. These findings do not lend sup-port to the view that patients who survive massiveresection of the small intestine without evidence ofhypersecretion have hypochlorhydria or achlor-hydria (Oxborne et al, 1966). In addition therewould seem to be no rationale in performing vago-tomy and pyloroplasty at the same time as resectionas suggested by Osborne, Sizer, Frederick, andZamcheck (1967).
EXPERIMENTAL STUDY The dog studies show thatmassive resection increases the 24-hour acid outputbut there is no significant change in the basal secre-tory rate. These results agree with those of Osborneet al (1966). Others (Reul and Ellison, 1966) haddifficulty in attaining basal rates after a 24-hour fastin Heidenhain pouch dogs. The results of our studywere obtained after a 31-hour fast when basal con-ditions had been reached. The Pavlov pouch resultswould seem to exclude the possibility that intestinalresection causes increased vagal activity. Such amechanism could have accounted for the raisedbasal rate seen in the patients. By beginning basalrate measurements within one week of the resectionin the dogs it is felt unlikely that an acute hyper-secretory state as seen in the human subjectshas been missed.The postcibal acid secretion is the only significant
difference between the pouch dogs before and afterresection (Fig. 3). This confirms tentative suggestionsmade by Reul and Ellison (1966). In both theHeidenhain and Pavlov pouch dogs there is a pro-longed and enhanced response to feeding. Duringthe fourth and fifth hours after the meal, whennormally acid secretion is diminishing, there is con-tinued secretory activity. At this time food hasusually reached the small intestine and inhibitorypathways of gastric secretion have been activated. Inthe animals studied the antrum and duodenum wereintact suggesting that primarily small intestinal in-hibitory activity is compromised by resection. Delayin gastric emptying has been suggested as a cause ofthe phenomenon but the results of other studies(Landor and Baker, 1964; Osborne et al, 1966)have failed to show a decreased rate of emptyingafter massive small intestinal resection. The resultsof antrectomy, vagotomy, and metabolic studies onour dogs (Windsor, 1968a) has led to the belief thatthe main factor is the loss of a fat-stimulated in-testinal inhibitory agent, probably enterogastrone,which normally modifies the antral phase ofsecretion.
784
on April 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.10.10.779 on 1 O
ctober 1969. Dow
nloaded from

Gastric secretion after massive small bowel resection 785
GENERAL It remains probable that a hypersecretorystate with similar characteristics to that seen in dogsexists in patients after resection. Studies on infants inwhich the secretory rate of the stomach after massiveresection was measured three hours after feedinglend support to this view (Avery, Randolph, andWeaver, 1966). These workers showed a highlysignificant increase in acid output at this time whenthese patients were compared with normal infants.This correlates well with the findings of this investiga-tion, that the maximum rate of secretion after re-section is delayed after feeding (Fig. 3). The tests ofgastric function with pentagastrin and histamine per-formed on patients and dogs showed no abnormali-ties after resection; this would be as expected sincethey give no information on defects of intestinalinhibition.The clinical and experimental models studied were
somewhat different; in man diseased or ischaemicbowel was resected, while in dogs the intestine re-moved was healthy. Further studies in dogs in whichischaemic intestine is resected would be valuable inconfirming the conclusions reached from the clinicalinvestigations. Despite these differences the resultsdo not support the view that vagotomy and pyloro-plasty should be performed at the same time asmassive resection in patients (Craig and Stewart,1960; Duval, 1964; Osborne et al, 1967; Leonard,Levine, Wittner, Buchwald, and Varco, 1967). Thehypersecretory phase was usually transient, lastingless than two weeks in most instances, and there wasno evidence of an increased parietal cell count orelevated basal rate of secretion after resection. Inaddition we found no evidence that the massivefluid, electrolyte, and hydrogen ion losses, ifaggressively treated, contributed to the cause ofdeath in our patients. Studies in dogs with Heiden-hain pouches and Pavlov pouches have shown thatthe postcibal hypersecretion is enhanced by vago-tomy and pyloroplasty to the main stomach(Windsor, 1968a, 1968b). In addition, faecal fatmeasurements gave no support to the view thatmalabsorption may be prevented by vagotomy andpyloroplasty (Windsor, 1968a).I should like to thank the Medical Research Council forfinancial support for the experimental part of this study,and the consultant surgeons in the West Midlands Regionwho supplied the details of the cases presented.
REFERENCES
Aber, G. M., Ashton, F., Carmalt, M. H. B., and Whitehead, T. P.(1967). Gastric hypersecretion following massive small-bowelresection in man. Amer. J. dig. Dis., 12, 785-794.
Allen, J. G. (1959). The Physiology and Treatment of Peptic Ulcer,p. 5. University of Chicago Press, U.S.A.
Anrep, G. V., and Barsoum, G. S. (1953). Blood histamine in experi-mental obstruction of the common bile duct. J. Physiol.(Lond.), 120, 427-430.
- , and Talaat, M. (1953). Release of histamine by the liver.Ibid, 120, 419-426.
Avery, G. B., Randolph, J. G., and Weaver, T. (1966). Gastricresponse to specific disease in infants. Pediatrics, 38, 874-878.
Bandes, J., Hollander, F., and Bierman, W. (1948). The effect ofphysically induced pyrexia on gastric acidity. Gastroenterology,10, 697-707.
Baddeley, R. M. (1968). Gastric secretion in human and experimentalliver disease. Ch.M. Thesis, Birmingham University.
Blickenstaff, D., and Grossman, M. I. (1950). A quantitative studyof the reduction of gastric acid secretion associated withpyrexia. Amer. J. Physiol., 160, 567-571.
Boyce, F. F. (1941). The Role of the Liver in Surgery, pp. 17-20.Thomas, Springfield, Ill.
Byers, F. M., Jordan, P. H., Jr, and Maren, T. H. (1961). Effects ofacetazolamide (diamox) and of metabolic acidosis and alka-losis upon gastric acid secretion in dogs. Surg. Forum, 12,289-291.
Carone, F. A., and Cooke, R. E. (1953). Effect of potassium deficiencyon gastric secretion in the rat. Amer. J. Physiol., 172, 684-688.
Cole, W. H., and Elman, R. (1932). Pathological changes in liveraccompanying intestinal obstruction and strangulation. Proc.Soc. exp. Biol. (N. Y.), 29, 1274-1275.
Craig, T. V., and Stewart, W. R. C. (1960). Massive bowel resectionin a patient with 75 per cent gastrectomy. Surgery, 48, 678-681.
De Vito, R. V., and Harkins, H. N. (1959). Techniques in Heidenhainpouch experiments. J. appl. Physiol., 14, 138-139.
Dragstedt, L. R., Ragins, H., Dragstedt, L. R., II, and Evans, S. 0.,Jr (1956). Stress and duodenal ulcer. Ann. Surg., 144, 450-463.Woodward, E. R., Storer, E. H., Oberhelman, H. A., Jr, andSmith, C. A. (1950). Quantitative studies on the mechanismof gastric secretion in health and disease. Ibid, 132, 626-640.
Duval, M. K., Jr (1964). Discussion to Frederick, P. L., and Craig,T. V. The effect of vagotomy and pyloroplasty on weight lossand survival of dogs after massive intestinal resection. Surgery,56, 141-142.
Frederick, P. L., Sizer, J. S., and Osborne, M. P. (1965). Relation ofmassive bowel resection to gastric secretion. New Engl. J.Med., 272, 509-514.
Gray, S. J., Benson, J. A., Jr, Reifenstein, R. W., and Spiro, H. M.(1951). Chronic stress and peptic ulcer. I. Effect of cortico-trophin (ACTH) and cortisone on gastric secretion. J. Amer.med. Ass., 147, 1529-1537.
Grundberg, A. B., Lopez, A. S., and Dragstedt, L. R., II (1967).Effect of intestinal reversal and massive resection on gastricsecretion. Arch. Surg., 94, 326-329.
Haymond, H. E. (1935). Massive resection of the small intestine; ananalysis of 257 collected cases. Surg. Gynec. Obstet., 61,693-705.
Hein, M. F., Silen, W., Skillman, J. J., and Harper, H. A. (1963).Effect of portacaval shunting on gastric secretion in cirrhoticdogs. Gastroenterology, 44,637-641.
Hirschowitz, B. I., Streeten, D. H. P., Pollard, H. M., and Boldt,H. A., Jr (1955). Role of gastric secretions in activation ofpeptic ulcers by corticotrophin. J. Amer. med. Ass., 158,27-32.
Hume, D. M. (1957). The secretion of epinephrine, nor-epinephrineand corticosteroids in the adrenal venous blood of the dogfollowing single and repeated trauma. Surg. Forum, 8, 111-115.
Kassirer, J. P., and Schwartz, W. B. (1966). The response of normalman to selective depletion of hydrochloric acid. Amer. J. Med.,40, 10-18.
Kerr, G., Elliott, D. W., and Endahl, G. L. (1968). Effect of antrec-tomy on gastric acid hypersecretion induced by isolation ofthe proximal small bowel. Amer. J. Surg., 115, 157-164.
Landor, J. H., and Baker, W. K. (1964). Gastric hypersecretionproduced by massive small bowel resection in dogs. J. surg.Res., 4, 518-522.
Leonard, A. S., Levine, A. S., Wittner, R., Buchwald, H., and Varco,R. L. (1967). Massive small-bowel resections. Operative anddietary management. Arch. Surg., 95, 429-435.
Muro, P. de, Rowinski, P., Calaresu, L., and Fraghi, A. (1961). Theimportance of potassium in the mechanism of gastric hydro-chloric acid secretion. Acta med. scand., 170, 403-410.
Needle, M. A., Kaloyanides, G. J., and Schwartz, W. B. (1964). Theeffects of selective depletion of hydrochloric acid on acid-baseand electrolyte equilibrium. J. clin. Invest., 43, 1836-1846.
Orloff, M. J., and Windsor, C. W. 0. (1966). Effect of portacavalshunt on gastric acid secretion in dogs with liver disease,portal hypertension and massive ascites. Ann. Surg., 164, 69-80.
on April 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.10.10.779 on 1 O
ctober 1969. Dow
nloaded from

786 Colin W. 0. Windsor, J. Fejfar, and D. A. K. Woodward
Osborne, M. P., Frederick, P. L., Sizer, J. S., Blair, D., Cole, P., andThum, W. (1966). Mechanism of gastric hypersecretionfollowing massive intestinal resection. Clinical and experi-mental observations. Ibid, 164, 622-634.
, Sizer, J., Frederick, P. L., and Zamcheck, N. (1967). Massivebowel resection and gastric hypersecretion. Amer. J. Surg.,114, 393-397.
Perry, J. F., Jr, Salmon, P., Griffen, W. 0., Jr, Root, H. D., andWangensteen, 0. H. (1959). A simple technique for preparingvagally innervated gastric pouches in dogs. Surgery, 45,937-940.
Pikula, J. V., and Dunphy, J. E. (1959). Some effects of stenosis ofthe terminal common bile duct on the biliary tract and liver.New Engl. J. Med., 260, 315-318.
Pullan, J. M. (1959). Massive intestinal resection. Proc. roy. Soc. Med.,52, 31-37.
Reul, G. J., and Ellison, E. H. (1966). Effect of 75 per cent distal smallbowel resection on gastric secretion. Amer. J. Surg., 111,772-776.
Schalm, L., and Hoogenboom, W. A. H. (1952). Blood bilirubin incongestive heart failure. Amer. Heart J., 44, 571-580.
Sherlock, S. (1951). The liver in heart failure. Brit. Heart J., 13, 273-293.Silen, W., Hein, M. F., Albo, R. 3., and Harper, H. A. (1963). In-
fluence of liver upon canine gastric secretion. Surgery, 54,29-36.
Skillman, J. J., Silen, W., Harper, H. A., Neely, S. C., and Simmons,E. L. (1961). Effect of hepatocellular injury on gastric secretionin dogs. Surg. Forum, 12, 276-277.
Westerheide, R. L., Elliott, D. W., and Hardacre, J. M. (1965). Thepotential of the upper small bowel in regulating acid secretion.Surgery, 58, 73-83.
Windsor, C. W. 0. (1968a). Gastric secretion after massive intestinalresection. A clinical and experimental study. Ch.M. Thesis,Birmingham University.
(1968b). Gastric secretion following massive small intestinalresection. (Abstr.) Brit. J. Surg., 55, 392.
Wright, S. (1952). Applied Physiology, 9th ed., p. 781. Oxford Uni-versity Press, London.
on April 10, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.10.10.779 on 1 O
ctober 1969. Dow
nloaded from