Embed Size (px)
Citation preview

www.thelancet.com/infection Vol 13 June 2013 519
Articles
Galactomannan and PCR versus culture and histology for directing use of antifungal treatment for invasive aspergillosis in high-risk haematology patients: a randomised controlled trialC Orla Morrissey, Sharon C-A Chen, Tania C Sorrell, Samuel Milliken, Peter G Bardy, Kenneth F Bradstock, Jeff rey Szer, Catriona L Halliday, Nicole M Gilroy, John Moore, Anthony P Schwarer, Stephen Guy, Ashish Bajel, Adrian R Tramontana, Timothy Spelman, Monica A Slavin, for the Australasian Leukaemia Lymphoma Group and the Australia and New Zealand Mycology Interest Group
SummaryBackground Empirical treatment with antifungal drugs is often used in haematology patients at high risk of invasive aspergillosis. We compared a standard diagnostic strategy (culture and histology) with a rapid biomarker-based diagnostic strategy (aspergillus galactomannan and PCR) for directing the use of antifungal treatment in this group of patients.
Methods In this open-label, parallel-group, randomised controlled trial, eligible patients were adults undergoing allogeneic stem-cell transplantation or chemotherapy for acute leukaemia, with no history of invasive fungal disease. Enrolled patients were randomly assigned (1:1) by a computer-generated schedule to follow either a standard diagnostic strategy (based on culture and histology) or a biomarker-based diagnostic strategy (aspergillus galactomannan and PCR) to direct treatment with antifungal drugs. Patients, were followed up for 26 weeks or until death. Masking of the use of diff erent diagnostic tests was not possible for patients, treating physicians, or investigators. The primary endpoint was empirical treatment with antifungal drugs in the 26 weeks after enrolment (for the biomarker-based diagnostic strategy, a single postive galactomannan or PCR result was deemed insuffi cient to confi rm invasive aspergillosis, so treatment in this context was classifi ed as empirical). This outcome was assessed by an independent data review committee from which the study allocations were masked. Analyses were by intention to treat and included all enrolled patients. This study is registered with ClinicalTrial.gov, number NCT00163722.
Findings 240 eligible patients were recruited from six Australian centres between Sept 30, 2005, and Nov 19, 2009. 122 were assigned the standard diagnostic strategy and 118 the biomarker-based diagnostic strategy. 39 patients (32%) in the standard diagnosis group and 18 (15%) in the biomarker diagnosis group received empirical antifungal treatment (diff erence 17%, 95% CI 4–26; p=0·002). The numbers of patients who had hepatotoxic and nephrotoxic eff ects did not diff er signifi cantly between the standard diagnosis and biomarker diagnosis groups (hepatotoxic eff ects: 21 [17%] vs 12 [10%], p=0·11; nephrotoxic eff ects: 52 [43%] vs 60 [51%], p=0·20).
Interpretation Use of aspergillus galactomannan and PCR to direct treatment reduced use of empirical antifungal treatment. This approach is an eff ective strategy for the management of invasive aspergillosis in high-risk haematology patients.
Funding Australian National Health and Medical Research Council, Cancer Council New South Wales, Pfi zer, Merck, Gilead Sciences.
IntroductionThe risk of death from invasive aspergillosis in patients undergoing allogeneic stem-cell transplantation or chemotherapy for acute leukaemia is high, largely because of delays in diagnosis by culture and histology.1,2 Consequently, prophylaxis is used and empirical treat-ment with antifungal drugs is given to neutropenic patients suspected of having an invasive fungal infection because of persistent fevers despite treatment with broad-spectrum antibacterial drugs.3 Although this strategy has reduced mortality from invasive asper gillosis, the drawbacks include breakthrough invasive fungal disease, drug interactions, emergence of
anti fungal resistance, and overtreatment with expensive antifungal drugs.2
Overtreatment can be reduced by use of rapid, non-culture-based diagnostic tests, including PCR and aspergillus galactomannan ELISA, to direct antifungal therapy.2 Analyses of sensitivity and specifi city suggest that galactomannan and PCR assays enable earlier, more accurate diagnosis of invasive aspergillosis than do traditional culture and histological methods.4,5 Investi-gators of studies6–12 into such biomarker-based diagnostic strategies report reductions in the use of empirical treatment (and so in the overall costs of antifungal drugs) and earlier diagnosis of invasive aspergillosis, with no
Lancet Infect Dis 2013; 13: 519–28
Published OnlineApril 30, 2013http://dx.doi.org/10.1016/S1473-3099(13)70076-8
See Comment page 470
Infectious Diseases Unit, Alfred Health, and Department of Infectious Diseases, Central Clinical School, Monash University, Melbourne, VIC, Australia (C O Morrissey MBBCh); Centre for Infectious Diseases and Microbiology (S C-A Chen MBBS, Prof T C Sorrell MBBS, C L Halliday PhD) and Department of Haematology (Prof K F Bradstock MBBS), Westmead Hospital, Westmead, NSW, Australia; Westmead Millennium Institute, Westmead, and Western Clinical School and Sydney Emerging Infections and Biosecurity Institute, University of Sydney, Sydney, NSW, Australia (S C-A Chen, T C Sorrell); Department of Haematology, Saint Vincent’s Hospital, Darlinghurst, NSW, Australia (S Milliken MBBS, J Moore MBBS); Department of Haematology, Royal Adelaide Hospital, Adelaide, and Department of Haematology, The Queen Elizabeth Hospital, Woodville South, SA, Australia (P G Bardy MBBS); Department of Clinical Haematology and Bone Marrow Transplant Service, Royal Melbourne Hospital, Parkville, VIC, Australia (Prof J Szer MBBS, A Bajel MBBS, Prof M A Slavin MBBS); New South Wales Bone Marrow Transplant Network, Agency for Clinical Innovation, Chatswood, NSW, Australia (N M Gilroy MBBS); Department of Haematology, Alfred Health, Melbourne, and

Articles
520 www.thelancet.com/infection Vol 13 June 2013
adverse eff ect on survival. However, those studies had drawbacks: some were not randomised,6,7,12 some included patients at low risk of invasive aspergillosis,7,9,10,12 and some examined a hybrid strategy with components of the traditional, empirical approach combined with galactomannan or PCR assays to direct antifungal treat-ment.8,9 Specifi cally, the combined use of galactomannan and PCR assays has not previously been examined, nor has such a strategy been compared with the standard diagnostic strategy (ie, culture and histology) with respect to the eff ect on outcomes for patients.
We aimed to measure the eff ect of a biomarker-based diag nostic strategy, in which both aspergillus galacto-mannan and PCR testing were used to direct further investigation (including timing of high-resolution CT scans) and treatment with antifungal drugs, on the use of empirical treatment, early diagnosis of invasive aspergillosis, and survival.
MethodsStudy design and participantsWe did a randomised, controlled, open-label, parallel-group trial to compare the effi cacy and safety of our biomarker-based diagnostic strategy with the standard diag nostic strategy of culture and histology in high-risk haematology patients. Eligible patients were aged 18 years or older, were undergoing allogeneic stem-cell transplantation or intensive combination induction-consolidation chemotherapy for acute myeloid or lymphoblastic leukaemia, and had given written in-formed consent. Patients were ineligible if they had any other immunocompromised state, a previous diagnosis of proven or probable invasive aspergillosis, or active invasive fungal disease, or if they had previously been enrolled in the trial or were currently enrolled in another trial of antifungal treatment. The trial was approved by institutional review boards at all participating centres, and was sponsored by the Australasian Leu kaemia Lymphoma Group as ALLG trial number SC01.
Randomisation and maskingPatients were stratifi ed by centre and randomly assigned (1:1) to either the standard diagnostic strategy (culture and histology) or the biomarker-based diagnostic strategy (galactomannan and PCR) within 48 h of the start of conditioning therapy or chemotherapy. The com-puter-generated, sequentially numbered, randomisation schedule was prepared by the Australasian Leukaemia Lymphoma Group trial centre to ensure that roughly equal numbers of patients were assigned to each group within each centre. For each eligible patient, the trial centre allocated a unique identifi cation number and a diagnostic strategy. Masking of the use of diff erent diagnostic tests in the two groups was not possible for patients, treating physicians, or investigators. To min-imise any related bias, the assigned diagnostic group was concealed from the independent data review com mittee
that assessed the primary and mortality endpoints (reports were formatted such that identifi cation of the assigned group of any individual patient was not possible).13
ProceduresProcedures for allogeneic stem-cell transplantation and chemotherapy were as per institutional protocols. From trial entry, all patients had blood taken for galactomannan and PCR testing twice per week (if inpatients) or once per week (if outpatients) for 26 weeks, or until death. Both assays were done as described elsewhere.4,14,15 Briefl y, the galactomannan ELISA assay (Platelia Aspergillus Ag Kit, Bio-Rad, Marnes-la-Coquette, France) was done in accordance with the manufacturer’s instructions and an optical density of 0·5 or higher was regarded as a positive result.14 A nested PCR assay that targeted an Aspergillus-genus-specifi c region of the multicopy 18S ribosomal RNA gene was used.4 Amplifi cation of a 249-base-pair band was taken as a positive PCR result.4 This assay was subsequently adapted to a qualitative real-time PCR format that incorporated an Aspergillus-genus-specifi c TaqMan probe, which had excellent reproducibility with the nested assay.15 For the qualitative real-time PCR assay, an exponential increase in fl uorescence during the fi rst 30 cycles of PCR amplifi cation was regarded as a positive result.15 All positive results were verifi ed by repeat testing.13 Samples from patients in the standard diagnosis group were batch tested with galactomannan and PCR, but results were not released to the treating physicians. In the biomarker diagnosis group, samples were tested in real time, with results notifi ed to the treating physicians within 48–72 h of sample collection.
The standard diagnostic strategy was consistent with the 2002 guidelines for antimicrobial use in neutropenic patients with cancer.3 When an invasive fungal disease was suspected (eg, because of persistent fever, defi ned as at least one temperature per day of 38·3°C or higher, or a temperature of 38·0°C or higher sustained for at least 1 h on 3–5 consecutive days),3 cultures of blood, urine, sputum (if available), and faeces (if clinically indicated), and high-resolution CT scans of the chest were done. Bronchoscopy and biopsy sampling were done in accordance with institutional protocols. Empirical treatment with antifungal drugs was recommended while patients were undergoing these investigations and was continued, de-escalated to prophylaxis, or the antifungal drug was changed to treat defi nite, probable, or possible invasive aspergillosis or other invasive fungal disease according to test results.
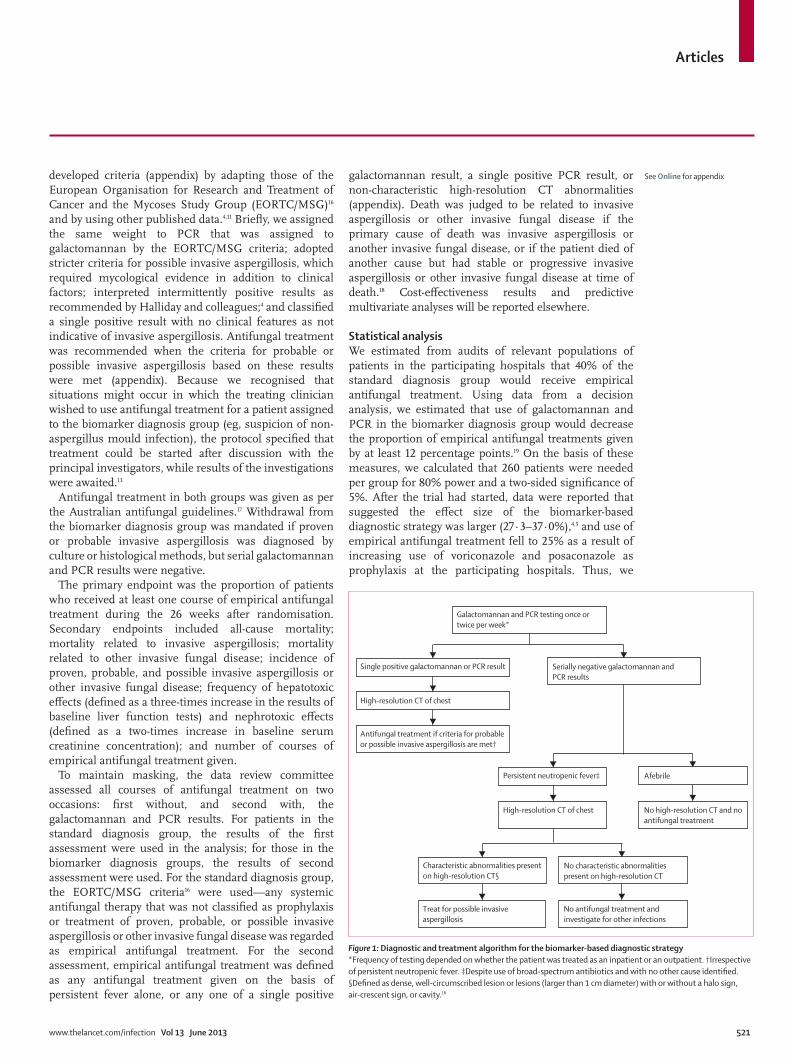
In the biomarker diagnosis group, either a single positive galactomannan or PCR result or serially negative results for both tests (in patients with persistently neutropenic fevers) prompted a high-resolution chest CT (fi gure 1). Before the start of the trial, no defi nitions existed for the classifi cation of invasive aspergillosis and guidance of antifungal treat ment based only on galactomannan, PCR, and CT results. Thus, we
Department of Haematology and Medical Oncology, Box Hill
Hospital, Box Hill, VIC, Australia (Prof A P Schwarer MD);
Department of Infectious Diseases, Western Health,
Footscray, VIC, Australia (S Guy MBBS,
A R Tramontana MBBS); Burnet Institute, Melbourne, VIC,
Australia (C O Morrissey, T Spelman MBBS, M A Slavin);
Department of Epidemiology and Preventative Medicine,
Central Clinical School, Monash University, Melbourne, VIC,
Australia (T Spelman); and Peter MacCallum Cancer
Centre, East Melbourne, and National Health and Medical
Research Council Centre for Clinical Research Excellence in
Infectious Diseases, Royal Melbourne Hospital, Parkville,
VIC, Australia (M A Slavin)
Correspondence to:Dr Orla Morrissey, Infectious Diseases Unit, Alfred Health,
85 Commercial Road, Melbourne, VIC, 3004, Australia
Articles
www.thelancet.com/infection Vol 13 June 2013 521
developed criteria (appendix) by adapting those of the European Organisation for Research and Treatment of Cancer and the Mycoses Study Group (EORTC/MSG)16 and by using other published data.4,11 Briefl y, we assigned the same weight to PCR that was assigned to galactomannan by the EORTC/MSG criteria; adopted stricter criteria for possible invasive aspergillosis, which required mycological evidence in addition to clinical factors; interpreted intermittently positive results as recommended by Halliday and colleagues;4 and classifi ed a single positive result with no clinical features as not indicative of invasive aspergillosis. Antifungal treatment was recommended when the criteria for probable or possible invasive aspergillosis based on these results were met (appendix). Because we recognised that situations might occur in which the treating clinician wished to use antifungal treatment for a patient assigned to the biomarker diagnosis group (eg, suspicion of non-aspergillus mould infection), the protocol specifi ed that treatment could be started after discussion with the principal investigators, while results of the investigations were awaited.13
Antifungal treatment in both groups was given as per the Australian antifungal guidelines.17 Withdrawal from the biomarker diagnosis group was mandated if proven or probable invasive aspergillosis was diagnosed by culture or histological methods, but serial galactomannan and PCR results were negative.
The primary endpoint was the proportion of patients who received at least one course of empirical antifungal treatment during the 26 weeks after randomisation. Secondary endpoints included all-cause mortality; mortality related to invasive aspergillosis; mortality related to other invasive fungal disease; incidence of proven, probable, and possible invasive aspergillosis or other invasive fungal disease; frequency of hepatotoxic eff ects (defi ned as a three-times increase in the results of baseline liver function tests) and nephrotoxic eff ects (defi ned as a two-times increase in baseline serum creatinine concentration); and number of courses of empirical antifungal treatment given.
To maintain masking, the data review committee assessed all courses of antifungal treatment on two occasions: fi rst without, and second with, the galactomannan and PCR results. For patients in the standard diagnosis group, the results of the fi rst assessment were used in the analysis; for those in the biomarker diagnosis groups, the results of second assessment were used. For the standard diagnosis group, the EORTC/MSG criteria16 were used—any systemic antifungal therapy that was not classifi ed as prophylaxis or treatment of proven, probable, or possible invasive aspergillosis or other invasive fungal disease was regarded as empirical antifungal treatment. For the second assessment, empirical antifungal treatment was defi ned as any antifungal treatment given on the basis of persistent fever alone, or any one of a single positive
galactomannan result, a single positive PCR result, or non-characteristic high-resolution CT abnor malities (appendix). Death was judged to be related to invasive aspergillosis or other invasive fungal disease if the primary cause of death was invasive aspergillosis or another invasive fungal disease, or if the patient died of another cause but had stable or progressive invasive aspergillosis or other invasive fungal disease at time of death.18 Cost-eff ectiveness results and predictive multivariate analyses will be reported elsewhere.
Statistical analysisWe estimated from audits of relevant populations of patients in the participating hospitals that 40% of the standard diagnosis group would receive empirical antifungal treatment. Using data from a decision analysis, we estimated that use of galactomannan and PCR in the biomarker diagnosis group would decrease the proportion of empirical antifungal treatments given by at least 12 percentage points.19 On the basis of these measures, we calculated that 260 patients were needed per group for 80% power and a two-sided signifi cance of 5%. After the trial had started, data were reported that suggested the eff ect size of the biomarker-based diagnostic strategy was larger (27·3–37·0%),4,5 and use of empirical antifungal treatment fell to 25% as a result of increasing use of voriconazole and posaconazole as prophylaxis at the participating hospitals. Thus, we
Figure 1: Diagnostic and treatment algorithm for the biomarker-based diagnostic strategy*Frequency of testing depended on whether the patient was treated as an inpatient or an outpatient. †Irrespective of persistent neutropenic fever. ‡Despite use of broad-spectrum antibiotics and with no other cause identifi ed. §Defi ned as dense, well-circumscribed lesion or lesions (larger than 1 cm diameter) with or without a halo sign, air-crescent sign, or cavity.16
Characteristic abnormalities present on high-resolution CT§
No characteristic abnormalities present on high-resolution CT
Treat for possible invasive aspergillosis
No antifungal treatment and investigate for other infections
Persistent neutropenic fever‡ Afebrile
High-resolution CT of chest No high-resolution CT and no antifungal treatment
Single positive galactomannan or PCR result Serially negative galactomannan andPCR results
Galactomannan and PCR testing once or twice per week*
High-resolution CT of chest
Antifungal treatment if criteria for probable or possible invasive aspergillosis are met†
See Online for appendix
Articles
522 www.thelancet.com/infection Vol 13 June 2013
recalculated the sample size at 110 patients per group needed to detect a reduction in use of empirical antifungal treatment from 25% to 12·5% in the biomarker diagnosis group, to maintain 80% power and two-sided signifi cance of 5%. Our recruitment target was reset to 120 patients per group to allow for withdrawals and treatment crossover.
An interim analysis was done when 120 patients had completed 26 weeks of follow-up. The independent safety and data monitoring committee defi ned in advance that the trial was to be stopped if a signifi cant diff erence (α1<0·008) for the primary endpoint or a diff erence of 5% or more in mortality related to invasive aspergillosis between groups was detected in the interim analysis. Neither of these criteria was met and the trial was continued to completion.
The primary analysis was done with the χ² test, and the intention-to-treat principle was used such that all randomised patients were included in the analysis. A signifi cance of α2=0·042 was used to ensure that the overall proportion of type 1 errors from the two-stage testing was equal to 0·05. The number of courses of empirical antifungal treatment was sig nifi cantly skewed, so results were compared by use of the Wilcoxon rank-sum test. Incidence of proven, probable, and possible invasive aspergillosis or other invasive fungal disease, and frequencies of adverse events were compared between groups with the χ² test or, when appropriate, Fisher’s exact test. All-cause mortality, that from invasive aspergillosis, and that from other invasive fungal disease were compared with the χ² test, with the Kaplan–Meier method and log-rank test used to estimate and compare survival, respectively. Patients were censored at time of last follow-up. Competing risks regression was used to test for any signifi cant eff ect of loss to follow-up and withdrawal of consent on the study’s capacity to assess
the primary outcome of receipt of empirical antifungal treatment, in which loss to follow-up or withdrawal of consent was the competing risk. For all secondary endpoints a two-sided p value of less than 0·05 was deemed as signifi cant. Prespecifi ed subgroup analyses were done in accordance with the type of antifungal prophylaxis, underlying disease (allogeneic stem-cell transplantation vs acute leukaemia), and centre. All analyses were done with Stata 12.0 statistical package.
This study is registered with ClinicalTrials.gov, number NCT00163722.
Role of the funding sourceThe sponsors of the study had no role in trial design, data collection, data analysis, data interpretation, or writing of the report. All authors had full access to all the data in the study and had fi nal responsibility for the decision to submit for publication.
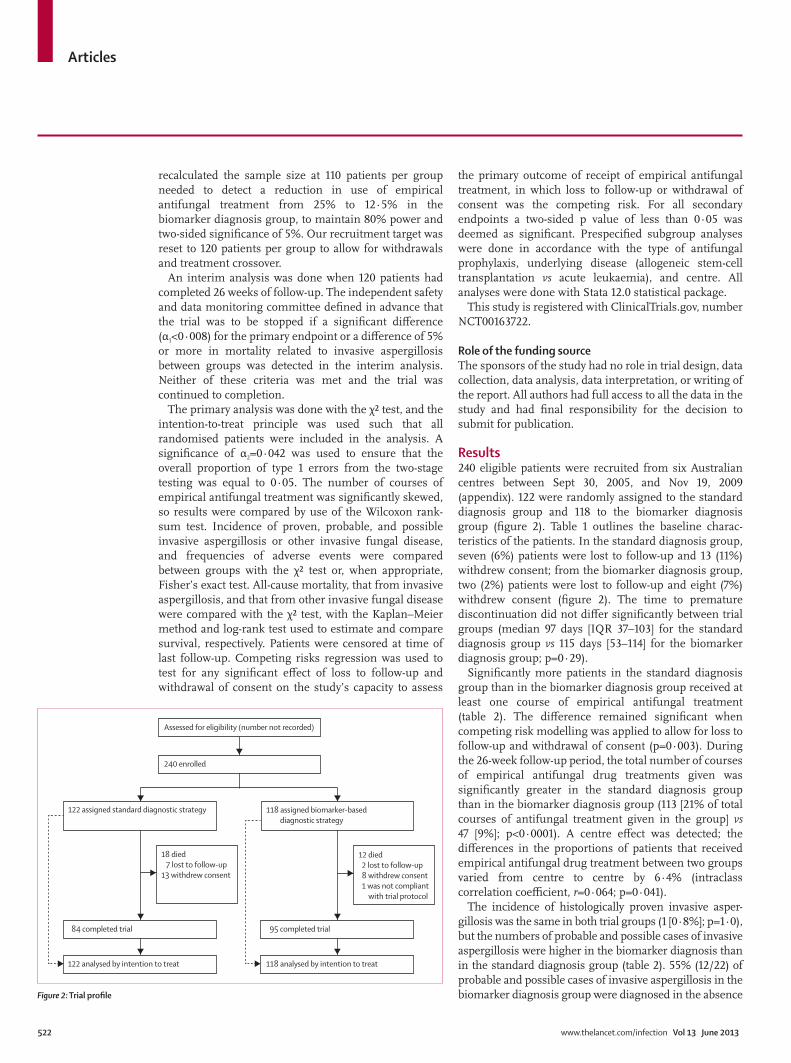
Results240 eligible patients were recruited from six Australian centres between Sept 30, 2005, and Nov 19, 2009 (appendix). 122 were randomly assigned to the standard diagnosis group and 118 to the biomarker diagnosis group (fi gure 2). Table 1 outlines the baseline charac-teristics of the patients. In the standard diagnosis group, seven (6%) patients were lost to follow-up and 13 (11%) withdrew consent; from the biomarker diagnosis group, two (2%) patients were lost to follow-up and eight (7%) withdrew consent (fi gure 2). The time to premature discontinuation did not diff er signifi cantly between trial groups (median 97 days [IQR 37–103] for the standard diagnosis group vs 115 days [53–114] for the biomarker diagnosis group; p=0·29).
Signifi cantly more patients in the standard diagnosis group than in the biomarker diagnosis group received at least one course of empirical antifungal treatment (table 2). The diff erence remained signifi cant when competing risk modelling was applied to allow for loss to follow-up and withdrawal of consent (p=0·003). During the 26-week follow-up period, the total number of courses of empirical antifungal drug treatments given was signifi cantly greater in the standard diagnosis group than in the biomarker diagnosis group (113 [21% of total courses of antifungal treatment given in the group] vs 47 [9%]; p<0·0001). A centre eff ect was detected; the diff erences in the proportions of patients that received empirical antifungal drug treatment between two groups varied from centre to centre by 6·4% (intraclass correlation coeffi cient, r=0·064; p=0·041).
The incidence of histologically proven invasive asper-gillosis was the same in both trial groups (1 [0·8%]; p=1·0), but the numbers of probable and possible cases of invasive aspergillosis were higher in the biomarker diagnosis than in the standard diagnosis group (table 2). 55% (12/22) of probable and possible cases of invasive aspergillosis in the biomarker diagnosis group were diagnosed in the absence Figure 2: Trial profi le
122 assigned standard diagnostic strategy 118 assigned biomarker-based diagnostic strategy
18 died 7 lost to follow-up13 withdrew consent
12 died 2 lost to follow-up 8 withdrew consent 1 was not compliant with trial protocol
84 completed trial 95 completed trial
122 analysed by intention to treat 118 analysed by intention to treat
Assessed for eligibility (number not recorded)
240 enrolled
Articles
www.thelancet.com/infection Vol 13 June 2013 523
of persistent fevers. The methods of diagnosis of invasive aspergillosis and other invasive fungal disease and the sites of infection are reported in the appendix. More probable cases of invasive aspergillosis in the biomarker diagnosis group were diagnosed by PCR than by galactomannan (11 vs 5; appendix).
All-cause mortality and that related to invasive aspergillosis did not diff er signifi cantly between the two groups (table 2). All causes of death other than invasive fungal disease are reported in the appendix.
The numbers of patients who had hepatotoxic and nephrotoxic eff ects did not diff er signifi cantly between the trial groups (hepatotoxic eff ects: 21 [17%] in the standard diagnosis group vs 12 [10%] in the biomarker diagnosis group, p=0·11; nephro toxic eff ects: 52 [43%] vs 60 [51%], p=0·20). No patients in the biomarker diagnosis group with serially negative galactomannan and PCR results had invasive aspergillosis diagnosed by standard culture and histological methods.
Subgroup analysis of patients who received prophylactic fl ucon azole or itraconazole and allogeneic stem-cell trans plantation revealed that the signifi cant diff erences between the trial groups in the proportion treated empirically with antifungal drugs and numbers of cases of invasive aspergillosis remained (tables 3, 4). Only one case of probable invasive asper gillosis was detected in a patient who was receiving voriconazole or posaconazole prophylaxis in the biomarker diagnosis group (table 4). None of fi ve patients diagnosed with possible invasive fungal disease on the basis of characteristic CT changes alone (negative results for PCR and galactomannan) was receiving voriconazole or posaconazole prophylaxis. Overall, signifi cantly more patients received voriconazole or posaconazole prophy laxis as the trial progressed (χ² for trends 14·08, p=0·003).
Had galactomannan and PCR testing been applied to patients in the standard diagnosis group, 26% (10/39) of those who received empirical antifungal treatment would have been diagnosed with probable or possible invasive aspergillosis a median of 4 days (IQR 2–9) earlier and 83% (5/6) of those whose death was related to invasive aspergillosis would have been diagnosed with probable or
Standard diagnosis group (n=122)
Biomarker diagnosis group (n=118)
(Continued from previous column)
Patients with acute leukaemia
Acute myeloid leukaemia 20 (16%) 18 (15%)
Neutropenia 13 (11%) 11 (9%)
Initial prophylaxis
Fluconazole 8 (7%) 5 (4%)
Itraconazole 4 (3%) 9 (8%)
Voriconazole 2 (2%) 3 (3%)
Posaconazole 6 (5%) 0
Liposomal amphotericin B 0 1 (1%)
Acute lymphoblastic leukaemia** 10 (8%) 1 (1%)
Neutropenia 5 (4%) 1 (1%)
Initial prophylaxis
Fluconazole 4 (3%) 1 (1%)
Itraconazole 4 (3%) 0
Posaconazole 1 (1%) 0
Liposomal amphotericin B 1 (1%) 0
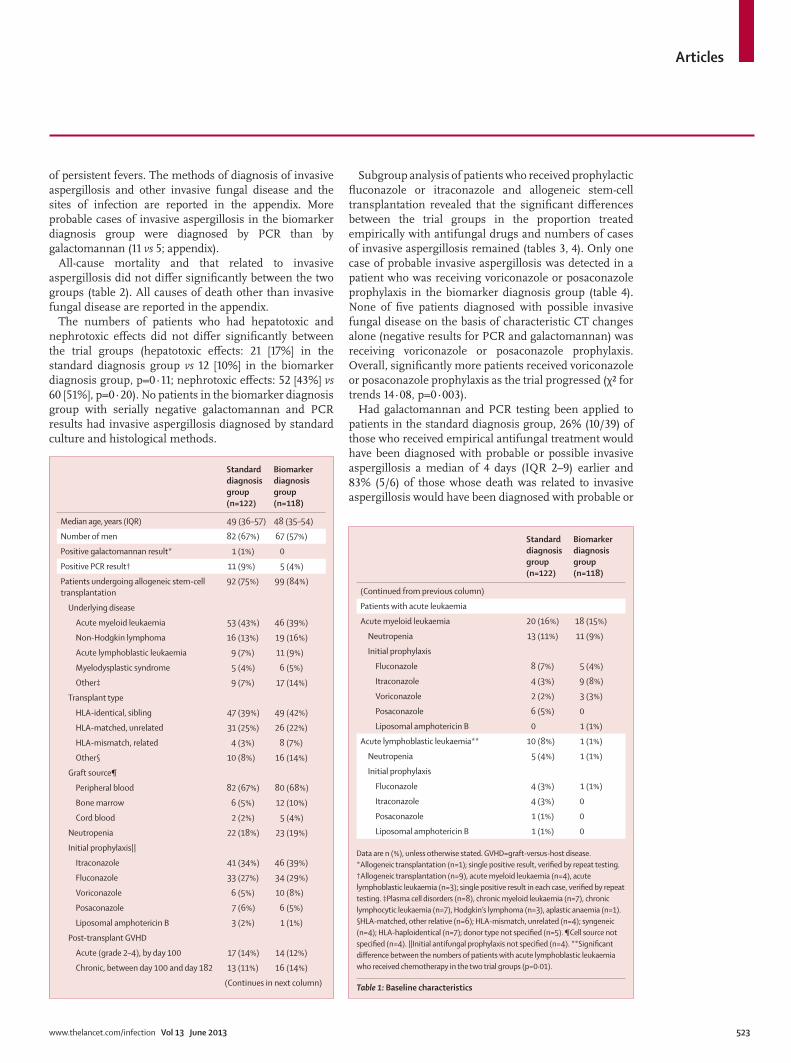
Data are n (%), unless otherwise stated. GVHD=graft-versus-host disease. *Allogeneic transplantation (n=1); single positive result, verifi ed by repeat testing. †Allogeneic transplantation (n=9), acute myeloid leukaemia (n=4), acute lymphoblastic leukaemia (n=3); single positive result in each case, verifi ed by repeat testing. ‡Plasma cell disorders (n=8), chronic myeloid leukaemia (n=7), chronic lymphocytic leukaemia (n=7), Hodgkin’s lymphoma (n=3), aplastic anaemia (n=1). §HLA-matched, other relative (n=6); HLA-mismatch, unrelated (n=4); syngeneic (n=4); HLA-haploidentical (n=7); donor type not specifi ed (n=5). ¶Cell source not specifi ed (n=4). ||Initial antifungal prophylaxis not specifi ed (n=4). **Signifi cant diff erence between the numbers of patients with acute lymphoblastic leukaemia who received chemotherapy in the two trial groups (p=0·01).
Table 1: Baseline characteristics
Standard diagnosis group (n=122)
Biomarker diagnosis group (n=118)
Median age, years (IQR) 49 (36–57) 48 (35–54)
Number of men 82 (67%) 67 (57%)
Positive galactomannan result* 1 (1%) 0
Positive PCR result† 11 (9%) 5 (4%)
Patients undergoing allogeneic stem-cell transplantation
92 (75%) 99 (84%)
Underlying disease
Acute myeloid leukaemia 53 (43%) 46 (39%)
Non-Hodgkin lymphoma 16 (13%) 19 (16%)
Acute lymphoblastic leukaemia 9 (7%) 11 (9%)
Myelodysplastic syndrome 5 (4%) 6 (5%)
Other‡ 9 (7%) 17 (14%)
Transplant type
HLA-identical, sibling 47 (39%) 49 (42%)
HLA-matched, unrelated 31 (25%) 26 (22%)
HLA-mismatch, related 4 (3%) 8 (7%)
Other§ 10 (8%) 16 (14%)
Graft source¶
Peripheral blood 82 (67%) 80 (68%)
Bone marrow 6 (5%) 12 (10%)
Cord blood 2 (2%) 5 (4%)
Neutropenia 22 (18%) 23 (19%)
Initial prophylaxis||
Itraconazole 41 (34%) 46 (39%)
Fluconazole 33 (27%) 34 (29%)
Voriconazole 6 (5%) 10 (8%)
Posaconazole 7 (6%) 6 (5%)
Liposomal amphotericin B 3 (2%) 1 (1%)
Post-transplant GVHD
Acute (grade 2–4), by day 100 17 (14%) 14 (12%)
Chronic, between day 100 and day 182 13 (11%) 16 (14%)
(Continues in next column)
Articles
524 www.thelancet.com/infection Vol 13 June 2013
possible invasive aspergillosis a median of 7 days (6–35) earlier. The incidences of probable and possible invasive aspergillosis would not have diff ered signifi cantly from those in the biomarker diagnosis group had galactomannan and PCR been applied in the standard diagnosis group (probable: 11 [9%] in the standard
diagnosis group vs 16 [14%] in the biomarker diagnosis group; p=0·36; possible: 5 [4%] vs 6 [5%]; p=0·96). 64% (25/39) of patients in the standard diagnosis group who were treated empirically with antifungal drugs had repeatedly negative galactomannan and PCR results.
DiscussionThe practice of giving empirical antifungal therapy in haematology patients with persistent febrile neutropenia of unknown cause is under challenge. We have shown that clinical management of this high-risk group of patients can be guided by the use of galactomannan and PCR results in combination, and that such an approach was eff ective in reducing use of empirical antifungal treatment by 52% (for the biomarker-based diagnostic strategy, a single positive galactomannan or PCR result was deemed insuffi cient to confi rm invasive aspergillosis, so treatment in this context was classifi ed as empirical; appendix; table 2). Reductions of 68–78% have been reported from previous open-label and other non-randomised clinical studies.6,7,9,12 Notably, no cases of invasive aspergillosis were missed by the biomarker-based diagnostic strategy in our study, and mortality related to invasive aspergillosis was low (3%) in the biomarker diagnosis group during the extended follow-up period of 26 weeks.7 Since untreated invasive aspergillosis has a mortality of 100%, mortality would have been higher than it was if invasive aspergillosis had been missed by our biomarker-based diagnostic strategy.6 This fi nding suggests that the biomarker-based strategy could be used in routine clinical practice to improve diff erentiation be tween patients with and without invasive aspergillosis and so to improve therapeutic decision making (panel).
More cases of invasive aspergillosis were identifi ed with the biomarker-based diagnostic strategy than with the standard diagnostic strategy. Such fi ndings have previously been interpreted by other research groups as being due to an increased risk for the development of invasive aspergillosis. As a result, they have recom mended that a biomarker-based strategy should not be used.9,20 However, since the post-hoc inclusion of the results of galactomannan and PCR for patients in the standard diagnosis group in our study yielded a similar incidence of invasive aspergillosis to that in the biomarker diagnosis group, invasive aspergillosis was underdiagnosed by the standard diagnostic strategy. Moreover, testing and empirical treatment in the standard diagnostic strategy is triggered by persistent fever, whereas 55% of cases of invasive aspergillosis diagnosed by the biomarker-based approach had no persistent fever. Maertens and colleagues6 reported similar results with galactomannan testing alone. Since the risk of developing invasive aspergillosis was not diff erent between the two groups in our study, we conclude that the diff erence in the incidence of invasive aspergillosis between the two groups is related to the diff erence in the sensitivity of the tests used in each group.
Standard diagnosis group (n=122)
Biomarker diagnosis group (n=118)
% diff erence between groups (95% CI)
p value
Received empirical treatment with antifungal drugs
39 (32%) 18 (15%) 17% (4 to 26) 0·002
Mortality
All-cause 18 (15%) 12 (10%) 5% (–4 to 14) 0·31
Invasive aspergillosis-related 6 (5%) 3 (3%) 2% (–2·5 to 7·3) 0·5
Other invasive fungal disease-related* 0 2 (2%) ·· 0·24
Incidence of invasive aspergillosis
Proven 1 (1%) 1 (1%) ·· 1·0
Probable 0 16 (14%) –14% (–20 to –7) <0·0001
Possible 0 6 (5%) –5% (–9 to –1) 0·013
Incidence of other invasive fungal disease†
Proven 4 (3%) 5 (4%) ·· 0·75
Probable 0 1 (1%) ·· 0·49
Data are n (%). Results for possible other invasive fungal disease are not shown because cases were not individually identifi ed by microscopic or culture methods. *Scedosporium prolifi cans fungaemia (n=1), disseminated mucormycosis (Rhizopus sp; n=1). †Candida guilliermondii (n=1), Candida glabrata (n=3), Candida krusei (n=1), Candida parapsilosis (n=1), Rhizopus sp (n=1), Rhizopus microsporus (n=1), S prolifi cans (n=1), Exserohilum sp (n=1).
Table 2: Empirical treatment with antifungal drugs, mortality , and incidence of invasive fungal infections through 26 weeks of follow-up
Standard diagnosis group
Biomarker diagnosis group
p value
Fluconazole or itraconazole prophylaxis 32/94 (34%) 15/95 (16%) 0·004
Voriconazole or posaconazole prophylaxis 5/22 (23%) 3/19 (16%) 0·70
Fluconazole prophylaxis 17/45 (38%) 4/40 (10%) 0·005
Itraconazole, voriconazole, or posaconazole prophylaxis 20/71 (28%) 14/74 (19%) 0·19
Allogeneic stem-cell transplantation 25/92 (27%) 13/99 (13%) 0·015
Acute leukaemia 14/30 (47%) 5/19 (26%) 0·15
Data are n/N (%).
Table 3: Empirical treatment with antifungal drugs by subgroup in the intention-to-treat population
Standard diagnosis group
Biomarker diagnosis group
p value
Fluconazole or itraconazole prophylaxis 1/94 (1%) 16/95 (17%) <0·0001
Voriconazole or posaconazole prophylaxis 0/22 1/19 (5%) 0·67
Fluconazole prophylaxis 0/45 5/40 (13%) 0·02
Itraconazole, voriconazole, or posaconazole prophylaxis 1/71 (1%) 12/74 (16%) 0·002
Allogeneic stem-cell transplantation 0/92 16/99 (16%) <0·0001
Acute leukaemia 1/30 (3%) 1/19 (5%) 1·0
Data are n/N (%).
Table 4: Incidence of proven and probable invasive aspergillosis by subgroup in the intention-to-treat population
Articles
www.thelancet.com/infection Vol 13 June 2013 525
The biomarker-based diagnostic strategy increased the cer tainty of diagnosis of invasive aspergillosis. 90% (9/10) of invasive aspergillosis cases in the standard diagnosis group were identifi ed solely on the basis of characteristic lesions on high-resolution chest CT (appendix). Although characteristic CT fi ndings are an early indicator of invasive aspergillosis and the routine use of CT confers a survival advantage,21,22 CT is not thought suffi ciently specifi c for this purpose.16,22 By contrast, in the biomarker diagnosis group in our trial, only 18% (5/28) of cases of invasive aspergillosis were diagnosed solely on the basis of characteristic CT fi ndings (appendix). In the remaining 82% (23/28), the diagnosis was directed by more specifi c criteria: culture in one (4%) and biomarker tests (galactomannan, PCR, or both) in 22 (79%) cases (appendix).
In this trial, PCR had greater diagnostic sensitivity for invasive aspergillosis than did galactomannan, and thus proved clinically useful. Aspergillus PCR has not previously been included in the EORTC/MSG defi nitions because it is not deemed adequately standardised or clinically validated.16 Evidence that a diagnostic test is clinically useful is the ultimate criterion for its use in routine clinical practice.23 Thus, a priority should now be to complete the standardisation of aspergillus PCR for inclusion in the EORTC/MSG defi nitions.24 Notably, these defi nitions were designed only for use in clinical trials.16,25 Our fi ndings of improved diagnostic sensitivity and certainty compared with culture, histology, and high-resolution CT suggest that the biomarker-based diag-nostic strategy used in this trial, which incorporates galactomannan and PCR, is appropriate for both enrolment of patients with invasive aspergillosis into clinical trials and for directing antifungal therapy in routine clinical practice.
Broad-spectrum, mould-active prophylaxis impairs the performance of galactomannan and PCR testing,26,27 which might account for the one case of invasive asper-gillosis we saw. Another explanation is that voriconazole or posaconazole prophylaxis eff ectively treats occult and prevents breakthrough invasive fungal disease, which would imply that the consistently negative galactomannan and PCR results we noted in patients receiving voriconazole or posaconazole prophylaxis were probably truly negative results. Furthermore, if the sensitivity of galactomannan and PCR were reduced then we would expect to see cases of invasive aspergillosis diagnosed by radiological fi ndings alone in patients on voriconazole or posaconazole prophylaxis. However, we saw no such cases in this trial. Ullmann and colleagues28 have reported that, in patients with baseline positive galactomannan results, breakthrough invasive fungal disease was signifi cantly reduced in patients on posaconazole prophylaxis compared with those on fl uconazole prophylaxis (2 [10%] vs 7 [23%]), which adds further strength to the suggestion that the low number of cases of invasive aspergillosis diagnosed in those on voriconazole
or posaconazole prophylaxis results more from the prophylactic effi cacy of these drugs rather than from a reduction in the sensitivity of the biomarkers. Although itraconazole has similar in-vitro activity to voriconazole and posaconazole, results of clinical studies in high-risk patients suggest that it does not diff er signifi cantly from fl uconazole (which has no mould activity) in prophylactic effi cacy, mainly because it has lower bioavailability and higher toxicity than fl u conazole.29,30 Analysis of the eff ect of various azoles on the usefulness of our biomarker-based diagnostic strategy showed that itraconazole has greater similarity with fl uconazole than with voriconazole or posaconazole with respect to effi cacy. On the basis of our fi ndings, we recommend that intensive screening with a biomarker-based diagnostic strategy should be used only in patients receiving fl uconazole, itraconazole, or no prophylaxis. Additionally, these data allow us to refi ne our previously reported diagnostic and treatment algorithms,31 which we now recommend for use in routine clinical practice (fi gure 3, appendix). Furthermore, we have shown that our biomarker-based diagnostic strategy provides an alternative to voriconazole or posaconazole prophylaxis in specifi c high-risk groups of
Panel: Research in context
Systematic reviewWe searched PubMed for full reports of studies published before Sept 30, 2012, with the terms “galactomannan”, “PCR”, “invasive aspergillosis”, “allogeneic”, “acute leukaemia”, “haematological malignancy”, “pre-emptive”, “utility”, “empiric antifungal therapy”, “prophylaxis”, and “treatment”. We identifi ed four randomised controlled trials8–11 that assessed biomarker-diagnosis-based strategies for invasive aspergillosis in patients undergoing allogeneic stem-cell transplantation or chemotherapy for a haematological malignancy. These trials variously used either galactomannan9,10 or PCR,8,11 but not both in combination; used clinical features, imaging, and persistent fever despite use of broad-spectrum antibiotics in addition to galactomannan or PCR as components of their biomarker-based diagnostic strategy;8,9 delayed the start of the biomarker-based diagnostic strategy;9 were of shorter duration than the at-risk period for development of invasive aspergillosis;9,10 and included patients at low risk of invasive aspergillosis.9,10Additionally, three of these trials only compared their biomarker-based diagnostic strategies with an empirical strategy for antifungal therapy rather than with a strategy based on standard diagnostic techniques.8–10 Therefore, the fi ndings varied substantially and some were contradictory.
InterpretationOur fi ndings showed an increased sensitivity and discriminatory power for our biomarker-based diagnostic strategy compared with a standard diagnostic strategy for the diagnosis of invasive aspergillosis, which improved our ability to target antifungal therapy correctly and safely. A new fi nding from our trial was that a biomarker-based diagnostic strategy was most effi cacious for patients on fl uconazole, itraconazole, or no prophylaxis. Aspergillus galactomannan and PCR can replace culture and histology for diagnosis of invasive aspergillosis, both for enrolment into clinical trials and as a practical trigger of commencement of antifungal treatment in clinical practice. Although more research is needed in patients with acute leukaemia and to compare a biomarker-based diagnostic strategy for directing antifungal therapy with prophylaxis, this trial provides important evidence in favour of a biomarker-based diagnostic strategy for the management of invasive aspergillosis in high-risk haematology patients.
Articles
526 www.thelancet.com/infection Vol 13 June 2013
patients, and identifi es clinical situations in which empirical antifungal treatment can be started, but then stopped early once negative galactomannan and PCR results become available (fi gure 3).
Earlier diagnosis of invasive aspergillosis has been associated with improved outcomes.21,22 Although our trial was not powered to detect a diff erence in mortality between groups, we saw that mortality was 31% lower in the biomarker diagnosis group, despite this group having more cases of invasive aspergillosis than the standard diagnosis group. Although not signifi cant, this fi nding is probably clinically important and suggests that the improved ability of our biomarker-based diagnostic strategy to detect invasive aspergillosis is an advantage rather than a limitation. Additionally, our overall survival results (appendix) were similar to the fungal-free survival outcomes reported by Wingard and colleagues,25 who examined prophylaxis and structured galactomannan monitoring in recipients of allogeneic stem-cell trans-plants. Our fi ndings suggest that had galactomannan and PCR testing been used in our standard diagnosis group, 26% of patients who received empirical antifungal treatment would have been diagnosed with probable or possible invasive aspergillosis a median of 4 days earlier and 83% of patients whose deaths were related to invasive aspergillosis would have been diag nosed with probable or possible invasive aspergillosis a median of 7 days earlier. Others have reported5,25,32 that galactomannan or PCR can diagnose invasive asper gillosis 2–9 days earlier than culture and high-resolution CT in up to 88·8% of patients.
The capacity of our biomarker-based diagnostic strategy for earlier diagnosis of invasive aspergillosis probably contributed to the im proved survival compared with the standard diagnosis group, despite a greater number of invasive aspergillosis diagnoses. By contrast, Cordonnier and colleagues9 re ported reduced survival in patients receiving induction chemotherapy who were randomly assigned to their biomarker diagnosis group compared with those treated empirically. However, this result was probably related to the delay in implementation of galactomannan testing until 96 h of persistent fever had elapsed, which led to a delay in the start of antifungal treatment in their biomarker diagnosis group until 7 days later than in their empirical treatment group. Thus, we believe that not only is the use of rapid, highly sensitive diagnostic assays such as galactomannan and PCR crucial to optimum survival, but also that these assays must be implemented for screening at the earliest possible point in the high-risk period for invasive aspergillosis.
One limitation of our trial was the small number of patients enrolled who had acute leukaemia, which could account for the diff erence in the numbers of patients with acute lymphoblastic leukaemia between the two groups. The diffi culties in enrolling patients with acute leukaemia have been described previously.33 Although we used broad eligibility criteria in an attempt to optimise the generalisability of our fi ndings,13 the small number of patients with acute leukaemia included in the trial suggests that validation of our fi ndings in this group of patients would be worthwhile. The numbers of patients who were lost to follow-up or withdrew consent were substantial in both groups, but not to an extent that would bias the primary endpoint result. We chose 26 weeks as the follow-up period to maximise the capture of trial-related events. Having examined the median time when patients were lost to follow-up, which generally coincided with the time of discharge from the transplant centre or completion of all courses of chemotherapy, we believe that the numbers of patients lost would have been much smaller with a shorter follow-up period. A small but signifi cant centre eff ect was seen, which could bias and limit the generalisability of our results.34 This fi nding emphasises that careful assessment of the preparedness of centres to implement a biomarker-based diagnostic strategy should be undertaken before such a strategy is adopted.35 A potential drawback of the approach used in our trial is that the biomarker-based diagnostic strategy we used does not detect non-aspergillus mould infections. However, we have established a clear proof of principle in this work; in centres where non-aspergillus mould infections are common, appropriate strategies can be adapted—eg, by incorporation of pan-fungal PCR and β-D-glucan assays.
In conclusion, our biomarker-based diagnostic strategy signifi cantly reduced use of empirical antifungal treatment and increased the sensitivity of invasive aspergillosis diagnosis, which led to better-directed
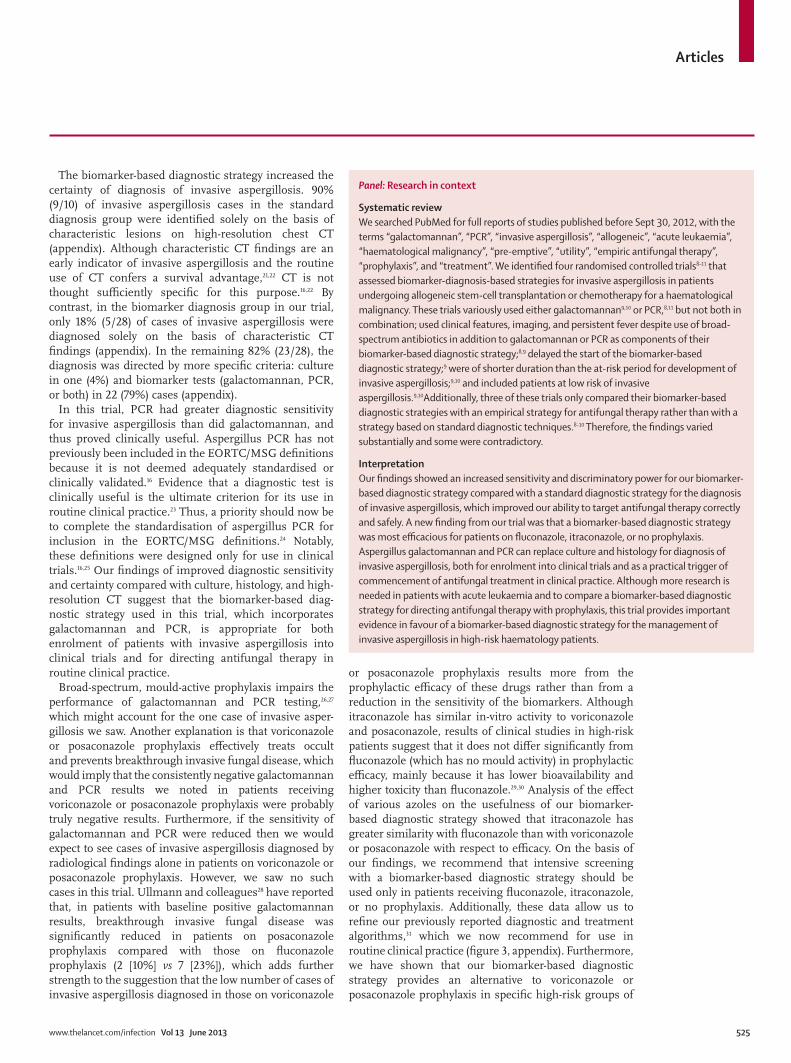
Figure 3: Integrated antifungal strategies for patients at risk of invasive fungal diseasePatients at high risk of invasive fungal infection are listed in the appendix. High-risk patients for whom a biomarker-based diagnostic strategy combined with fl uconazole, itraconazole, or no prophylaxis is a suitable alternative to voriconazole or posaconazole prophylaxis are also listed in the appendix. In the targeted diagnostic strategy, appropriate investigations are determined by clinical symptoms and signs, and by abnormalities seen on high-resolution CT of the chest—these investigations are outlined in full in the appendix.16,31 *On-site access to galactomannan or fungal PCR assays is not available, and high-resolution CT or bronchoscopy with lavage are not readily accessible or available.
Not on prophylaxis On fluconazole or itraconazole prophylaxis
Biomarker-based diagnostic strategy
Biomarker-based diagnostic strategy
Patients at high risk of invasive fungal disease
Reserve empirical treatment with antifungal drugs for patients with persistent febrile neutropenia in whom an invasive fungal disease is suspected or patient is unwell: • When diagnostic tests are unavailable*• For a short time until diagnosis of invasive fungal disease is confirmed or excluded
On voriconazole or posaconazole prophylaxis
Targeted diagnostic strategy• Bronchoscopy• High-resolution CT-guided fine needle aspirate• Biopsy

Articles
www.thelancet.com/infection Vol 13 June 2013 527
antifungal treatment with no increase in mortality. This strategy prevents the overuse of empirical treatment with antifungal drugs and represents an appropriate alternative to broad-spectrum, mould-active prophylaxis in specifi c groups of patients. Furthermore, galacto-mannan and PCR can replace culture and histology for the diagnosis of invasive aspergillosis and as a practical trigger for commencement of antifungal treatment in routine clinical practice.
ContributorsCOM, SC-AC, TCS, CLH, NMG, and MAS contributed to the search of
the scientifi c literature, trial design, data collection, data analysis and
interpretation, and writing of the report. KFB and JS contributed to the
trial design, data interpretation, and writing of the report. SM, PGB, and
JM contributed to the data collection, data interpretation, and writing of
the report. APS contributed to the trial design, data collection, and
writing of the report. SG, AB, and ART contributed to data analysis and
interpretation, and the writing of the report. TS did the statistical
analysis and assisted in writing of the report.
Confl icts of interestCOM has been a member of advisory boards for, received investigator-
initiated grants from, and given lectures for Gilead Sciences, Pfi zer,
Merck Sharp & Dohme, and Orphan Australia. SC-AC has received
investigator-initiated grants from and been a member of advisory boards
for Pfi zer, Gilead Sciences, and Merck Sharp & Dohme. TCS has been a
member of advisory boards for and has received investigator-initiated
grants from Pfi zer and Merck Sharp & Dohme. KFB has received
consultancy payments from Pfi zer, Merck Sharp & Dohme, and Gilead
Sciences. NMG has been a member of advisory boards for Schering
Plough (2006) and Pfi zer (2012) and has given talks at events sponsored
by Pfi zer, Merck Sharp & Dohme, and Gilead Sciences. AB received a
travel grant to a conference from Merck Sharp & Dohme. ART has
received a travel grant to a conference from Pfi zer. MAS has been a
member of advisory boards for and received research funding from
Pfi zer, Merck Sharp & Dohme, Schering Plough, and Gilead Sciences.
SM, PGB, JS, CLH, JM, APS, SG, and TS declare that they have no
confl icts of interest.
AcknowledgmentsThese fi ndings were presented in part at the 51st Interscience
Conference on Antimicrobial Agents and Chemotherapy (Chicago, IL,
USA, Sept 17–20, 2011). We thank the trial coordinators (N Griffi ths,
E J Furphy, S Firth, T Luff , C Kesby, P Plenge, D Barham, M Antipas,
T Lewis), laboratory research assistants (S Sleiman, G Kularatne,
A Campbell, A-L Chan, S Kidd), and data managers (A Matera,
T Morgan, J Di Iulio) for their important contributions to the trial. This
work was supported by grants from the Australian National Health and
Medical Research Council (NHMRC) Project Grant (331305) and Cancer
Council New South Wales. We are also grateful to Pfi zer for a large,
unrestricted, investigator-initiated grant and to Merck Sharp & Dohme
(Australia) and Gilead Sciences, who provided minor, unrestricted,
investigator-initiated grants for this trial. Funding was also provided by
the NHMRC Centre for Clinical Research Excellence in Infectious
Diseases (219275), Royal Melbourne Hospital, Melbourne, VIC,
Australia; the NHMRC Centre for Clinical Research Excellence in
Infections, Bioethics and Haematological Malignancies (264625),
Westmead Millennium Institute, University of Sydney, Sydney, NSW,
Australia; Bio-Rad, Marnes-la-Coquette, France; and Sigma-Aldrich
Company, St Louis, MO, USA. The Victorian Operational Infrastructure
Support Program received by the Burnet Institute provided
infrastructure support for this trial. Without all of these funding sources
the trial would not have been completed. TCS is a Sydney Medical
School Foundation Fellow.
References1 Neofytos D, Horn D, Anaissie E, et al. Epidemiology and outcome
of invasive fungal infections in adult hematopoietic stem cell transplant recipients: analysis of multicenter prospective antifungal therapy (PATH) alliance registry. Clin Infect Dis 2009; 48: 265–73.
2 Maertens JA, Nucci M, Donnelly JP. The role of antifungal treatment in hematology. Haematologica 2012; 97: 325–27.
3 Hughes WT, Armstrong D, Bodey GP, et al. 2002 guidelines for the use of antimicrobial agents in neutropenic patients with cancer. Clin Infect Dis 2002; 34: 730–51.
4 Halliday C, Hoile R, Sorrell T, et al. Role of prospective screening of blood for invasive aspergillosis by polymerase chain reaction in febrile neutropenic recipients of haematopoietic stem cell transplant and patients with acute leukaemia. Br J Haematol 2006; 132: 478–86.
5 Maertens J, Van Eldere J, Verhaegen J, Verbeken E, Verschakelen J, Boogaerts M. Use of circulating galactomannan screening for early diagnosis of invasive aspergillosis in allogeneic stem cell transplant recipients. J Infect Dis 2002; 186: 1297–306.
6 Maertens J, Theunissen K, Verhoef G, et al. Galactomannan and computed tomography-based preemptive antifungal therapy in neutropenic patients at high-risk for invasive fungal infection: a prospective feasibility study. Clin Infect Dis 2005; 41: 1242–50.
7 Barnes RA, White PL, Bygrave C, Evans N, Healy B, Kell J. Clinical impact of enhanced diagnosis of invasive fungal disease in high-risk haematology and stem cell transplant patients. J Clin Pathol 2009; 62: 64–69.
8 Hebart H, Klingspor L, Klingebiel T, et al. A prospective randomized controlled trial comparing PCR-based and empirical treatment with liposomal amphotericin B in patients after allo-SCT. Bone Marrow Transplant 2009; 43: 553–61.
9 Cordonnier C, Pautas C, Maury S, et al. Empirical versus preemptive antifungal therapy for high-risk, febrile neutropenic patients: a randomized, controlled trial. Clin Infect Dis 2009; 48: 1042–51.
10 Tan BH, Low JG, Chlebicka NL, et al. Galactomannan-guided preemptive vs. empirical antifungals in the persistently febrile neutropenic patient: a prospective randomized study. Int J Infect Dis 2011; 15: 350–56.
11 Blennow O, Remberger M, Klingspor L, et al. Randomized PCR-based therapy and risk factors for invasive fungal infection following reduced-intensity conditioning and hematopoietic SCT. Bone Marrow Transplant 2010; 45: 1710–18.
12 Dignan FL, Evans SO, Ethell ME, et al. An early CT-diagnosis-based treatment strategy for invasive fungal infection in allogeneic transplant recipients using caspofungin fi rst line: an eff ective strategy with low mortality. Bone Marrow Transplant 2009; 44: 51–56.
13 Morrissey CO, Chen SC, Sorrell TC, et al. Design issues in a randomized controlled trial of a pre-emptive versus empiric antifungal strategy for invasive aspergillosis in patients with high-risk hematologic malignancies. Leuk Lymphoma 2011; 52: 179–93.
14 Maertens J, Verhaegen J, Demuynck H, et al. Autopsy-controlled prospective evaluation of serial screening for circulating galactomannan by a sandwich enzyme-linked immunosorbent assay for haematological patients at-risk for invasive aspergillosis. J Clin Microbiol 1999; 37: 3223–28.
15 Halliday CH, Wu QX, James G, Sorrell T. Development of a nested qualitative real-time PCR assay to detect Aspergillus species DNA in clinical specimens. J Clin Microbiol 2005; 43: 5366–68.
16 de Pauw B, Walsh TJ, Donnelly JP, et al. Revised defi nitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infection Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 2008; 46: 1813–21.
17 Slavin MA, Szer J, Grigg AP, et al. Guidelines for the use of antifungal agents in the treatment of invasive Candida and mould infections. Intern Med J 2004; 34: 192–200.
18 Nivoix Y, Velten M, Letscher–Bru V, et al. Factors associated with overall and attributable mortality in invasive aspergillosis. Clin Infect Dis 2008; 47: 1176–84.
19 Severens JL, Donnelly JP, Meis JF, et al. Two strategies for managing invasive aspergillosis: a decision analysis. Clin Infect Dis 1997; 25: 1148–54.
20 Maertens J, Marchetti O, Herbrecht R, et al. European guidelines for antifungal management in leukemia and hematopoietic stem cell transplant recipients: summary of the ECIL–3 2009 Update. Bone Marrow Transplant 2011; 46: 709–18.

Articles
528 www.thelancet.com/infection Vol 13 June 2013
21 Caillot D, Casasnovas O, Bernard A, et al. Improved management of invasive pulmonary aspergillosis in neutropenic patients using early thoracic computed tomographic scan and surgery. J Clin Oncol 1997; 15: 139–47.
22 Greene RE, Schlamm HT, Oestmann JW, et al. Imaging fi ndings in acute invasive pulmonary aspergillosis: clinical signifi cance of the halo sign. Clin Infect Dis 2007; 44: 373–79.
23 Guyatt GH, Tugwell PX, Feeny DH, Haynes RB, Drummond M. A framework for clinical evaluation of diagnostic technologies. CMAJ 1986; 134: 587–94.
24 White PL, Bretagne S, Klingspor L, et al. Aspergillus PCR: one step closer to standardization. J Clin Microbiol 2010; 48: 1231–40.
25 Wingard JR, Carter SL, Walsh TJ, et al. Randomized, double-blind trial of fl uconazole versus voriconazole for prevention of invasive fungal infection after allogeneic hematopoietic stem cell transplantation. Blood 2010; 116: 5111–18.
26 Marr KA, Laverdiere M, Gugel A, Leisenring W. Antifungal therapy decreases sensitivity of the Aspergillus galactomannan enzyme immunoassay. Clin Infect Dis 2005; 40: 1762–69.
27 Buchheidt D, Hummel M, Schleiermacher D, et al. Prospective clinical evaluation of a LightCycler-mediated polymerase chain reaction assay, a nested-PCR assay and a galactomannan enzyme-linked immunosorbent assay for detection of invasive aspergillosis in neutropenic cancer patients and haematological stem cell transplant recipients. Br J Haematol 2004; 125: 196–202.
28 Ullmann AJ, Lipton JH, Vesole DH, et al. Posaconazole or fl uconazole for prophylaxis in sever graft-versus-host disease. N Engl J Med 2007; 356: 335–47.
29 Marr KA, Crippa F, Leisenring W, et al. Itraconazole versus fl uconazole for prevention of fungal infections in patients receiving allogeneic stem cell transplants. Blood 2004; 103: 1527–33.
30 Vardakas KZ, Michalopoulos A, Falagas ME. Fluconazole versus itraconazole for antifungal prophylaxis in neutropenic patients with haematological malignancies: a meta-analysis of randomised-controlled trials. Br J Haematol 2005; 131: 22–28.
31 Morrissey CO, Bardy PG, Slavin MA, et al. Diagnostic and therapeutic approach to persistent or recurrent fevers of unknown origin in adult stem cell transplantation and haematological malignancy. Intern Med J 2008; 38: 477–95.
32 Hebart H, Loffl er J, Meisner C, et al. Early detection of Aspergillus infection after allogeneic stem cell transplantation by polymerase chain reaction screening. J Infect Dis 2000; 181: 1713–19.
33 Murray P, Kerridge I, Tiley C, et al. Enrolment of patients to clinical trials in haematological cancer in New South Wales: current status, perceived barriers and opportunities for improvement. Intern Med J 2010; 40: 133–138.
34 Biau DJ, Halm JA, Ahmadieh H, et al. Provider and center eff ect in multi-center randomized controlled trials of surgical specialities: an analysis on patient-level data. Ann Surg 2008; 247: 892–98.
35 Agrawal S, Hope W, Sinko J, Kibbler C. Optimizing management of invasive mould diseases. J Antimicrob Chemother 2011; 66 (suppl 1): 145–53.





























![Aspergillosis - Youngstown State Universitypeople.ysu.edu/~crcooper01/Aspergillosis[1]- Katie Jacquie Qazi.pdf•People with Aspergillosis are in three distinct groups •Healthy immune](https://img.dokumen.tips/doc/110x75/5e3883b0e2f2970b7b1c24ad/aspergillosis-youngstown-state-crcooper01aspergillosis1-katie-jacquie-qazipdf.jpg)