Embed Size (px)
Citation preview

Acupuncture and dry-needling for low back pain (Review)
Furlan AD, van Tulder MW, Cherkin DC, Tsukayama H, Lao L, Koes BW, Berman BM
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2008, Issue 3
http://www.thecochranelibrary.com
1Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

T A B L E O F C O N T E N T S
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW . . . . . . . . . . . . . . . . . .
3SEARCH METHODS FOR IDENTIFICATION OF STUDIES . . . . . . . . . . . . . . . . . . .
4METHODS OF THE REVIEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5DESCRIPTION OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5METHODOLOGICAL QUALITY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10FEEDBACK . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11POTENTIAL CONFLICT OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . .
11ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
16TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
16Characteristics of included studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
58Characteristics of excluded studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
59Characteristics of ongoing studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62Table 01. Methodological quality assessment . . . . . . . . . . . . . . . . . . . . . . . . .
69Table 02. Clinical relevance assessment . . . . . . . . . . . . . . . . . . . . . . . . . . .
72Table 03. Adequacy of acupuncture . . . . . . . . . . . . . . . . . . . . . . . . . . . .
75Table 04. Improvement in pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
76Table 05. Search Strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
77Table 06. Internal Validity Criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
78ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
78Comparison 01. acupuncture versus no treatment ((Sub)acute LBP: < 3 months) . . . . . . . . . . . . .
78Comparison 02. acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months) . . . . . . .
79Comparison 03. acupuncture versus other intervention ((Sub)acute LBP: < 3 months) . . . . . . . . . . .
79Comparison 04. acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months) . . . . . . . . . . . . .
79Comparison 05. acupuncture versus no treatment. (Chronic LBP: > 3 months) . . . . . . . . . . . . .
79Comparison 06. acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months) . . . . . . . .
80Comparison 07. acupuncture versus other intervention. (Chronic LBP: > 3 months) . . . . . . . . . . .
81Comparison 08. acupuncture versus acupuncture. (Chronic LBP: > 3 months) . . . . . . . . . . . . . .
81Comparison 09. dry-needling versus other intervention ((Sub)acute LBP < 3 months) . . . . . . . . . . .
81Comparison 10. acupuncture versus placebo or sham intervention (unknown / mixed duration of low back pain) . .
81Comparison 11. acupuncture versus other intervention (unknown / mixed duration of low back pain) . . . . .
82Comparison 12. acupuncture versus acupuncture. (unknown / mixed duration of low back pain) . . . . . . .
82Comparison 13. acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months) . . .
82INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
82COVER SHEET . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
84GRAPHS AND OTHER TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
84Figure 01. Acupuncture compared to no treatment, placebo or sham therapy . . . . . . . . . . . . . .
85Figure 02. Acupuncture compared to another intervention or added to other interventions . . . . . . . . .
86Figure 03. Effects of dry-needling at trigger points . . . . . . . . . . . . . . . . . . . . . . .
86Figure 04. Comparison between two techniques of acupuncture . . . . . . . . . . . . . . . . . . .
87Analysis 01.01. Comparison 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months), Outcome 01 pain .
iAcupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

88Analysis 01.03. Comparison 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months), Outcome 03 functional
status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
89Analysis 01.04. Comparison 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months), Outcome 04 physical
examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
90Analysis 02.01. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months),
Outcome 01 pain (VAS) (lower values are better) . . . . . . . . . . . . . . . . . . . . .
91Analysis 02.03. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months),
Outcome 03 functional status (higher scores are better). Generic instrument . . . . . . . . . . . .
92Analysis 02.04. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months),
Outcome 04 physical examination: finger-floor distance (lower values are better) . . . . . . . . . . .
93Analysis 02.06. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months),
Outcome 06 mean difference in pain (final - initial) . . . . . . . . . . . . . . . . . . . . .
94Analysis 02.07. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months),
Outcome 07 mean difference in functional status (final - initial) Generic instrument . . . . . . . . .
95Analysis 02.08. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months),
Outcome 08 mean difference in physical examination (final - initial): finger-floor distance . . . . . . .
96Analysis 03.01. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months), Outcome 01 pain
(VAS): lower values are better . . . . . . . . . . . . . . . . . . . . . . . . . . . .
97Analysis 03.02. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months), Outcome 02
global measure (higher values are better) . . . . . . . . . . . . . . . . . . . . . . . . .
98Analysis 03.03. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months), Outcome 03
functional status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
99Analysis 03.04. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months), Outcome 04
physical examination (finger floor distance) . . . . . . . . . . . . . . . . . . . . . . .
100Analysis 03.06. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months), Outcome 06
Side effects / Complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
101Analysis 04.01. Comparison 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months), Outcome 01 pain .
102Analysis 04.02. Comparison 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months), Outcome 02 global
measure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
103Analysis 04.03. Comparison 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months), Outcome 03
functional status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
104Analysis 04.04. Comparison 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months), Outcome 04 physical
examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
105Analysis 05.01. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 01 pain
(instruments: VAS and number of words) . . . . . . . . . . . . . . . . . . . . . . . .
106Analysis 05.02. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 02 global
measure (improvement) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
107Analysis 05.03. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 03 functional
status (higher values are better) . . . . . . . . . . . . . . . . . . . . . . . . . . . .
108Analysis 05.04. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 04 limitation
of activity (higher values are worse) . . . . . . . . . . . . . . . . . . . . . . . . . .
109Analysis 05.05. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 05 physical
examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
110Analysis 05.07. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 07 functional
status (standardized measures) . . . . . . . . . . . . . . . . . . . . . . . . . . . .
111Analysis 06.01. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 01 pain (lower values mean better) . . . . . . . . . . . . . . . . . . . . . . .
112Analysis 06.02. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 02 global improvement (higher values are better) . . . . . . . . . . . . . . . . . .
113Analysis 06.03. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 03 pain disability index (lower values are better) . . . . . . . . . . . . . . . . . .
114Analysis 06.04. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 04 physical examination (fingertips-to-floor distance).( Lower values are better) . . . . . . . .
iiAcupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

115Analysis 06.05. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 05 improvement in physical examination . . . . . . . . . . . . . . . . . . . . .
116Analysis 06.06. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 06 Sick leave (higher values mean worse) . . . . . . . . . . . . . . . . . . . . .
117Analysis 06.07. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 07 Well being (SF-36). (Higher values are better) . . . . . . . . . . . . . . . . . .
118Analysis 06.08. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 08 Side effects / Complications . . . . . . . . . . . . . . . . . . . . . . . .
118Analysis 06.09. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 09 pain (percent of baseline values) . . . . . . . . . . . . . . . . . . . . . . .
119Analysis 06.10. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 10 sick leave . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
119Analysis 06.11. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 11 general level of pain (0-15 points)(more points mean less pain) . . . . . . . . . . . .
120Analysis 06.12. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 12 pain: difference between within group changes . . . . . . . . . . . . . . . . . .
120Analysis 06.13. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 13 function: difference between within group changes . . . . . . . . . . . . . . . .
121Analysis 06.14. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 14 Pain: percentage of patients with >50% pain reduction . . . . . . . . . . . . . . .
121Analysis 06.15. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 15 spine range of motion: difference between within group changes . . . . . . . . . . . .
122Analysis 07.01. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 01 pain
(lower values are better) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
123Analysis 07.03. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 03 back
specific functional status (lower scores mean better). Ex: RDQ, Oswestry and Aberdeen . . . . . . . .
123Analysis 07.04. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 04 back
specific functional status (higher scores are better). Ex: Japan Orthopedic Association Score. . . . . . . .
124Analysis 07.05. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 05 pain
disability index (lower values are better) . . . . . . . . . . . . . . . . . . . . . . . . .
124Analysis 07.06. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 06
physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
125Analysis 07.07. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 07
return to work (higher values mean better) . . . . . . . . . . . . . . . . . . . . . . . .
125Analysis 07.08. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 08 Side
effects / Complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
126Analysis 07.09. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 09 pain
and function (adjusted for baseline values) . . . . . . . . . . . . . . . . . . . . . . . .
126Analysis 07.10. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 10
general level of pain (0-15 points)(more points mean less pain) . . . . . . . . . . . . . . . . .
127Analysis 07.11. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome 11 pain:
difference between within group changes . . . . . . . . . . . . . . . . . . . . . . . .
128Analysis 08.01. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 01 pain (lower
values mean better) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
128Analysis 08.02. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 02
Improvement (higher values are better) . . . . . . . . . . . . . . . . . . . . . . . . .
129Analysis 08.03. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 03 functional
status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
129Analysis 08.04. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 04 physical
examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
129Analysis 08.06. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 06
improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiiAcupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

130Analysis 09.01. Comparison 09 dry-needling versus other intervention ((Sub)acute LBP < 3 months), Outcome 01
global measure (higher values are better) . . . . . . . . . . . . . . . . . . . . . . . . .
131Analysis 09.02. Comparison 09 dry-needling versus other intervention ((Sub)acute LBP < 3 months), Outcome 02 Side
effects / Complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
131Analysis 10.01. Comparison 10 acupuncture versus placebo or sham intervention (unknown / mixed duration of low
back pain), Outcome 01 pain (VAS): lower values are better . . . . . . . . . . . . . . . . . .
132Analysis 10.02. Comparison 10 acupuncture versus placebo or sham intervention (unknown / mixed duration of low
back pain), Outcome 02 global measure . . . . . . . . . . . . . . . . . . . . . . . . .
132Analysis 10.03. Comparison 10 acupuncture versus placebo or sham intervention (unknown / mixed duration of low
back pain), Outcome 03 functional status (higher scores are better). Generic instrument . . . . . . . .
133Analysis 10.04. Comparison 10 acupuncture versus placebo or sham intervention (unknown / mixed duration of low
back pain), Outcome 04 physical examination (higher values are better) . . . . . . . . . . . . . .
133Analysis 11.01. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back pain),
Outcome 01 pain score (lower values mean better) . . . . . . . . . . . . . . . . . . . . .
134Analysis 11.02. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back pain),
Outcome 02 pain recovery: higher values are better . . . . . . . . . . . . . . . . . . . . .
134Analysis 11.03. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back pain),
Outcome 03 global measure (higher values are better) . . . . . . . . . . . . . . . . . . . .
135Analysis 11.04. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back pain),
Outcome 04 back specific functional status (higher scores are better). Ex: Japan Orthopedic Association Score.
135Analysis 11.05. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back pain),
Outcome 05 physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . .
136Analysis 11.07. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back pain),
Outcome 07 Side effects / Complications . . . . . . . . . . . . . . . . . . . . . . . .
136Analysis 12.01. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain),
Outcome 01 pain (lower values are better) . . . . . . . . . . . . . . . . . . . . . . . .
137Analysis 12.02. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain),
Outcome 02 pain recovery (higher values are better) . . . . . . . . . . . . . . . . . . . .
137Analysis 12.03. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain),
Outcome 03 global measure (higher values are better) . . . . . . . . . . . . . . . . . . . .
138Analysis 12.04. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain),
Outcome 04 functional status (higher values are better) . . . . . . . . . . . . . . . . . . .
138Analysis 12.05. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain),
Outcome 05 physical examination (finger-floor distance) Higher values are better. . . . . . . . . . .
138Analysis 12.07. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain),
Outcome 07 improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
139Analysis 13.01. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3
months), Outcome 01 pain (lower values are better) . . . . . . . . . . . . . . . . . . . .
140Analysis 13.02. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3
months), Outcome 02 pain: difference between within group changes . . . . . . . . . . . . . .
141Analysis 13.03. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3
months), Outcome 03 pain disability index (lower values are better) . . . . . . . . . . . . . . .
142Analysis 13.04. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3
months), Outcome 04 Pain: percentage of patients with >50% pain reduction . . . . . . . . . . .
142Analysis 13.05. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3
months), Outcome 05 function: difference between within group changes . . . . . . . . . . . . .
143Analysis 13.06. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3
months), Outcome 06 global measure . . . . . . . . . . . . . . . . . . . . . . . . .
144Analysis 13.07. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: >
3 months), Outcome 07 back specific functional status (lower scores mean better). Ex: RDQ, Oswestry and
Aberdeen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
145Analysis 13.08. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3
months), Outcome 08 spine range of motion: difference between within group changes . . . . . . . .
ivAcupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

145Analysis 13.09. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3
months), Outcome 09 Side effects / Complications . . . . . . . . . . . . . . . . . . . . .
vAcupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Acupuncture and dry-needling for low back pain (Review)
Furlan AD, van Tulder MW, Cherkin DC, Tsukayama H, Lao L, Koes BW, Berman BM
This record should be cited as:
Furlan AD, van Tulder MW, Cherkin DC, Tsukayama H, Lao L, Koes BW, Berman BM. Acupuncture and dry-needling for low back
pain. Cochrane Database of Systematic Reviews 2005, Issue 1. Art. No.: CD001351. DOI: 10.1002/14651858.CD001351.pub2.
This version first published online: 24 January 2005 in Issue 1, 2005.
Date of most recent substantive amendment: 30 October 2004
A B S T R A C T
Background
Although low-back pain is usually a self-limiting and benign disease that tends to improve spontaneously over time, a large variety of
therapeutic interventions are available for its treatment.
Objectives
To assess the effects of acupuncture for the treatment of non-specific low-back pain and dry-needling for myofascial pain syndrome in
the low-back region.
Search strategy
We updated the searches from 1996 to February 2003 in CENTRAL, MEDLINE, and EMBASE. We also searched the Chinese
Cochrane Centre database of clinical trials and Japanese databases to February 2003.
Selection criteria
Randomized trials of acupuncture (that involves needling) for adults with non-specific (sub)acute or chronic low-back pain, or dry-
needling for myofascial pain syndrome in the low-back region.
Data collection and analysis
Two authors independently assessed methodological quality (using the criteria recommended by the Cochrane Back Review Group)
and extracted data. The trials were combined using meta-analyses methods or levels of evidence when the data reported did not allow
statistical pooling.
Main results
Thirty-five RCTs were included; 20 were published in English, seven in Japanese, five in Chinese and one each in Norwegian, Polish
and German. There were only three trials of acupuncture for acute low-back pain. They did not justify firm conclusions, because
of small sample sizes and low methodological quality of the studies. For chronic low-back pain there is evidence of pain relief and
functional improvement for acupuncture, compared to no treatment or sham therapy. These effects were only observed immediately
after the end of the sessions and at short-term follow-up. There is evidence that acupuncture, added to other conventional therapies,
relieves pain and improves function better than the conventional therapies alone. However, effects are only small. Dry-needling appears
to be a useful adjunct to other therapies for chronic low-back pain. No clear recommendations could be made about the most effective
acupuncture technique.
Authors’ conclusions
The data do not allow firm conclusions about the effectiveness of acupuncture for acute low-back pain. For chronic low-back pain,
acupuncture is more effective for pain relief and functional improvement than no treatment or sham treatment immediately after
treatment and in the short-term only. Acupuncture is not more effective than other conventional and “alternative” treatments. The
data suggest that acupuncture and dry-needling may be useful adjuncts to other therapies for chronic low-back pain. Because most of
the studies were of lower methodological quality, there certainly is a further need for higher quality trials in this area.
1Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

P L A I N L A N G U A G E S U M M A R Y
Thirty-five RCTs covering 2861 patients were included in this systematic review. There is insufficient evidence to make any recommen-
dations about acupuncture or dry-needling for acute low-back pain. For chronic low-back pain, results show that acupuncture is more
effective for pain relief than no treatment or sham treatment, in measurements taken up to three months. The results also show that for
chronic low-back pain, acupuncture is more effective for improving function than no treatment, in the short-term. Acupuncture is not
more effective than other conventional and “alternative” treatments. When acupuncture is added to other conventional therapies, it
relieves pain and improves function better than the conventional therapies alone. However, effects are only small. Dry-needling appears
to be a useful adjunct to other therapies for chronic low-back pain.
B A C K G R O U N D
Low-back pain is a major health problem among western indus-
trialized countries, and a major cause of medical expenses, absen-
teeism and disablement (van Tulder 1995). People with acute low-
back pain usually experience improvements in pain, disability, and
return to work within one month, further but smaller improve-
ments occur up to three months, after which, pain and disability
levels remain almost constant and most people will have at least
one recurrence within 12 months (Pengel 2003). Although low-
back pain is usually a self-limiting and benign disease (Waddell
1987), a large variety of therapeutic interventions are available to
treat it (van Tulder 1997). However, the effectiveness of most of
these interventions has not been convincingly demonstrated and
consequently, the therapeutic management of low-back pain varies
widely.
Acupuncture is one of the oldest forms of therapy and has its roots
in ancient Chinese philosophy. Traditional acupuncture is based
on a number of philosophical concepts, one of which postulates
that any manifestation of disease is considered a sign of imbal-
ance between the Yin and Yang forces within the body. In classical
acupuncture theory, it is believed that all disorders are reflected at
specific points, either on the skin surface or just below it. Vital
energy circulates throughout the body along the so-called meridi-
ans, which have either Yin or Yang characteristics. An appropriate
choice of the 361 classical acupuncture points located on these
meridians for needling is believed to restore the balance in the
body. When the needles have been placed successfully, the patient
is supposed to experience a sensation known as Teh Chi (in some
schools of traditional acupuncture). Teh Chi has been defined as
a subjective feeling of fullness, numbness, tingling, and warmth,
with some local soreness and a feeling of distension around the
acupuncture point. There is no consensus among acupuncturists
about the necessity of reaching Teh Chi for acupuncture to be
effective.
Since acupuncture disseminated to the west several hundred years
ago, many different styles of acupuncture have developed, in-
cluding Japanese Meridian Therapy, French Energetic Acupunc-
ture, Korean Constitutional Acupuncture and Lemington 5 Ele-
ment Acupuncture. While these are similar to traditional acupunc-
ture, they each have distinct characteristics. In recent decades,
new forms of acupuncture have developed, such as ear (auricular)
acupuncture, head (scalp) acupuncture, hand acupuncture and
foot acupuncture (Lao 1996). Modern acupuncturists use not only
traditional meridian acupuncture points, but also non-meridian
or extra-meridian acupuncture points, which are fixed points not
necessarily associated with meridians. Acupuncture commonly in-
cludes manual stimulation of the needles, but various adjuncts are
often used, including electrical acupuncture (in which an electri-
cal stimulator is connected to the acupuncture needle), injection
acupuncture (herbal extracts injected into acupuncture points),
heat lamps, and acupuncture with moxibustion (the moxa herb,
Artemisia vulgaris, is burned at the end of the needle) (Lao 1996).
Dry-needling is a technique that uses needles to treat myofascial
pain in any body part, including the low-back region. Myofas-
cial pain syndrome is a disease of muscle that produces local and
referred pain. It is characterized by a motor abnormality (a hard
band within the muscle) and by sensory abnormalities (tenderness
and referred pain). It is classified as a musculoskeletal pain syn-
drome that can be acute or chronic, regional or generalized. It can
be a primary disorder causing local or regional pain syndromes, or
a secondary disorder that occurs as a consequence of some other
condition (Gerwin 2001). In 1983, Travel and Simons published
the book Myofascial Pain and Dysfunction - the Trigger Point Man-ual (Travel and Simons 83), which shows the pain pattern of trig-
ger points in every muscle of the body. Myofascial trigger points,
once carefully identified, can be inactivated by various methods
including systemic muscle relaxants, botulinum toxin, antidepres-
sants, deep muscle massage (for example: Shiatsu), local injection
of substances such as steroids or lidocaine, and dry-needling. Dry-
needling involves the insertion of a needle (it can be an acupunc-
ture needle or any other injection needle without injecting any
liquid) at these trigger points. The needles are not left in situ, they
are removed once the trigger point is inactivated. The inactiva-
tion of the trigger point should be followed by exercises (usually
stretching) or ergonomic adjustments with the purpose to re-es-
tablish a painless, full range of motion, and avoid recurrences.
It is still unclear what exact mechanisms underlying the action of
acupuncture or dry-needling. Western scientific research has pro-
posed mechanisms for the effect of acupuncture on pain relief. It
2Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

has been suggested that acupuncture might act by principles of
the gate control theory of pain. One type of sensory input (low-
back pain) could be inhibited in the central nervous system by an-
other type of input (needling). Another theory, the diffuse noxious
inhibitory control (DNIC), implies that noxious stimulation of
heterotopic body areas modulates the pain sensation originating
in areas where a subject feels pain. There is also some evidence
that acupuncture may stimulate the production of endorphins,
serotonin and acetylcholine within the central nervous system, en-
hancing analgesia (Chu 1979; Stux 2003).
The effectiveness of acupuncture in the treatment of low-back
pain has been systematically reviewed before (van Tulder 1999
(a); van Tulder 1999 (b)) with inconclusive results due to the low
methodological quality of the included studies. This is an updated
review of all available scientific evidence, including evidence from
Chinese and Japanese trials, on the effectiveness of acupuncture
for both acute and chronic low-back pain, and dry-needling for
myofascial pain syndrome in the low-back region.
O B J E C T I V E S
The objectives of this systematic review were to determine the
effects of acupuncture for (sub)acute and chronic non-specific low-
back pain, and dry-needling for myofascial pain syndrome in the
low-back region, compared to no treatment, sham therapies, other
therapies, and the addition of acupuncture to other therapies.
C R I T E R I A F O R C O N S I D E R I N G
S T U D I E S F O R T H I S R E V I E W
Types of studies
Only randomized controlled trials (RCTs), with no language re-
striction, were included in this systematic review.
Types of participants
Adults (>18 years) with non-specific low-back pain and myofascial
pain syndrome in the low-back region were included. RCTs that
included subjects with low-back pain caused by specific patholog-
ical entities such as infection, metastatic diseases, neoplasm, os-
teoarthritis, rheumatoid arthritis or fractures were excluded. Low-
back pain associated with sciatica as the major symptom, preg-
nancy and post-partum were also excluded. Although some studies
did not exclusively limit the study population to patients with non-
specific symptoms, studies were included if the majority of the pa-
tients had non-specific low-back pain according to the predefined
criteria. Patients with (sub)acute (12 weeks or less) or chronic low-
back pain (more than 12 weeks), were included.
Types of intervention
Articles evaluating acupuncture or dry-needling treatments that
involve needling were included in this review. Acupuncture was
defined as “the diagnosis was made using traditional acupuncture
theory and the needles were inserted in classical meridian points,
extra points or ah-shi points (painful points)’. Dry-needling was
defined as ”the cause of pain was diagnosed as “Myofascial Pain
Syndrome”, the points were chosen by palpation in the muscle,
and the needles were inserted into these myofascial trigger points’.
Studies were included regardless of the source of stimulation (e.g.,
hand or electrical stimulation). Studies in which the acupuncture
treatment did not involve needling, such as acupressure or laser
acupuncture were excluded. The control interventions were no
treatment, placebo/sham acupuncture or other sham procedure,
and other therapeutic interventions. Trials comparing two tech-
niques of acupuncture or dry-needling were included, but anal-
ysed separately.
Types of outcome measures
RCTs were included that used at least one of the four outcome
measures considered to be important in the field of low-back pain:
pain intensity (eg, visual analog scale (VAS)), a global measure (eg,
overall improvement, proportion of patients recovered, subjective
improvement of symptoms), back specific functional status (eg,
Roland Disability Scale, Oswestry Scale) and return to work (eg,
return to work status, number of days off work). The primary
outcomes for this review were pain and functional status. Physi-
ological outcomes of physical examination (eg, range of motion,
spinal flexibility, degrees of straight leg raising or muscle strength),
generic health status (eg, SF-36, Nottingham Health Profile, Sick-
ness Impact Profile) and other symptoms, such as medication use
and side effects were considered secondary outcomes.
S E A R C H M E T H O D S F O R
I D E N T I F I C A T I O N O F S T U D I E S
See: Cochrane Back Group methods used in reviews.
The previous review had searched the literature from 1966 until
1996. The following search strategies were used for this updated
review:
1. CENTRAL, The Cochrane Library 2003, Issue 1;
2. MEDLINE (OVID) from 1996 to February 2003 (see Table
05 for strategy);
3. EMBASE (OVID) from 1996 to February 2003 (see Table 05
for strategy);
4. The Cochrane Back Review Group Trials Registry;
5. The Chinese Cochrane Centre Trials Registry;
6. A database search of controlled clinical trials published
in Japan, using “Igaku Chuo Zasshi” (Japana Centra Revuo
Medicina) web version (between 1987 - 2003);
7. Reference lists in review articles and trials retrieved;
8. Personal communication with experts in the field.
3Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

M E T H O D S O F T H E R E V I E W
Study selection
For this updated review, one author (ADF) generated the electronic
search strategies in CENTRAL, MEDLINE, and EMBASE and
downloaded the citations into Reference Manager 9.0 Two authors
(MvT and BK) then independently reviewed the information to
identify trials that could potentially meet the inclusion criteria.
Full articles describing these trials were obtained and the same
two authors independently applied the selection criteria to the
studies. Consensus was used to solve disagreements concerning
the final inclusion of RCTs and a third author was consulted if
disagreements persisted. One author (HT) searched and selected
the studies from the Japanese databases. The Chinese Cochrane
Centre generated the searches in their Trials Register and one
author (LXL) selected the studies. The authors of recent original
studies were contacted to obtain more information when needed.
Methodological quality assessment
The methodological quality of each RCT was independently
assessed by two authors (not always the same pair of authors).
Review authors were not blinded with respect to authors,
institution and journal because they were familiar with the
literature. Consensus was used to resolve disagreements and a third
author was consulted if disagreements persisted.
The methodological quality of the RCTs was assessed by using
the criteria list recommended in the Updated Method Guidelines
for systematic reviews in the Cochrane Back Review Group (van
Tulder 2003) (Table 06). Each item was scored as “yes”, “no” or
“don’t know” according to the definitions of the criteria (Table
06).
The methodological quality assessment of the studies was used
for two purposes: First, to exclude studies with fatal flaws (such
as drop-out rate higher than 50%, statistically significant and
clinically important baseline differences that were not accounted
in the analyses). Studies that passed the first screening for fatal
flaws were classified into lower or higher quality: Higher quality
was defined as a trial fulfilling six or more of the 11 methodological
quality criteria and not having a fatal flaw. Lower quality trials
were defined as fulfilling fewer than six criteria and not having a
fatal flaw. The classification into higher/lower quality was used to
grade the strength of the evidence.
Data extraction
Two authors independently extracted the data on the study
characteristics, funding, ethics, study population, interventions,
analyses and outcomes. The authors of recent studies (published
in the past five years) were contacted to obtain more information
when needed.
Adequacy of treatment
Three authors, who are experienced acupuncturists (AF, LXL and
HT), judged the adequacy of treatment. The data extraction
included four questions about the adequacy of treatment,
which were derived from the STRICTA recommendations
(MacPherson 2002): 1) Choice of acupoints, 2) Number of
sessions, 3) Needling technique and 4) Acupuncturist experience.
The control groups were also judged as 1) appropriateness
of sham/placebo intervention and 2) adequate number of
sessions/dose. In addition, a panel of experts in acupuncture
treatment for low-back pain was consulted in a three-hour session
in which each study was presented for discussion (only the
population and interventions were presented, so the panel was
blinded to authors, journal, year, country, outcomes and results).
The panel consisted of six physicians trained in a variety of
acupuncture methods (Traditional Chinese medicine, Ryodoraku,
dry-needling, trigger point injections and scalp needling) who
work at a multidisciplinary pain clinic in Sao Paulo, Brazil. The
panel also classified each study as acupuncture or dry-needling.
Clinical Relevance
The two authors who extracted the data also judged the clinical
relevance of each trial using the five questions recommended
by Shekelle et al (Shekelle 1994) and the Updated Method
Guidelines(van Tulder 2003):
1. Are the patients described in detail so that you can decide
whether they are comparable to those that you see in your practice?
2. Are the interventions and treatment settings described well
enough so that you can provide the same for your patients?
3. Were all clinically relevant outcomes measured and reported?
4. Is the size of the effect clinically important?
5. Are the likely treatment benefits worth the potential harms?
Analysis
The primary analyses, decided a priori, were:
• acupuncture compared to no treatment, placebo or sham
therapy
• acupuncture compared to another intervention
• acupuncture added to an intervention compared to the
intervention without acupuncture.
Any other comparisons were considered secondary analysis.
The results of each RCT were plotted as point estimates, ie, relative
risks (RR) with corresponding 95% confidence interval (95% CI)
for dichotomous outcomes, mean and standard deviation (SD)
for continuous outcomes, or other data types as reported by the
authors of the studies. When the results could not be plotted,
they were described in the table of included studies or the data
were entered into “other data tables”. For continuous measures,
preference was given to analyse the results with weighted mean
differences (WMD) because these results are easier to interpret
for clinicians and other readers. If this was not possible, then
standardized mean differences (SMD) or effect sizes were used.
The studies were first assessed for clinical homogeneity with respect
to the duration of the disorder, types of acupuncture, control
group and the outcomes. Clinically heterogeneous studies were
4Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

not combined in the analysis, but separately described. For studies
judged as clinically homogeneous, statistical heterogeneity was
tested by Q test (chi-square) and I2. Clinically and statistically
homogeneous studies were pooled using the fixed effect model.
Clinically homogeneous and statistically heterogeneous studies
were pooled using the random effects model. Funnel plots were
constructed when at least 10 studies were available for the meta-
analysis (Sutton 2000).
When the data could not be entered in the meta-analysis because
of the way the authors of the trials reported the results (for
example: no information about standard deviation of the means)
we performed a qualitative analysis by attributing various levels of
evidence to the effectiveness of acupuncture, taking into account
the methodological quality and the outcome of the original studies
(van Tulder 2003):
• Strong evidence*-consistent** findings among multiple higher
quality RCTs
• Moderate evidence-consistent findings among multiple lower
quality RCTs and/or one higher quality RCT
• Limited evidence-one lower quality RCT
• Conflicting evidence-inconsistent findings among multiple trials
(RCTs)
• No evidence-no RCTs
* There is consensus among the Editorial Board of the Back Review
Group that strong evidence can only be provided by multiple
higher quality trials that replicate findings of other researchers in
other settings.
** When >75% of the trials report the same findings.
The results were grouped according to the following study
characteristics:
1) Type of acupuncture: two subgroups were analysed separately:
a. acupuncture in which the points were chosen by the meridian
theory
b. dry-needling in which needles were inserted in trigger points
2) Duration of pain: three subgroups were analysed separately:
a. acute and subacute pain (duration 12 weeks or less)
b. chronic (duration more than 12 weeks)
c. unknown or mixed duration
3) Control group:
a. no treatment
b. placebo or sham acupuncture
c. other interventions or acupuncture in addition to other
interventions
d. two different techniques of acupuncture
4) Outcome measures:a. Pain
b. Global measure
c. Functional status
d. Physical examination
e. Return to work
f. Complications
5) Timing of follow-up:
a. immediately after the end of the sessions - up to one week after
the end of the sessions
b. short-term follow-up - between one week and three months
after the end of the sessions
c. intermediate-term follow-up - between three months and one
year after the end of the sessions
d. long-term follow-up - one year or longer after the end of the
sessions
D E S C R I P T I O N O F S T U D I E S
The review published in 1999 included 11 studies (van Tulder
1999 (a)). This updated review includes 35 studies and 2861 pa-
tients. Twenty were published in English, seven in Japanese (Araki
2001; Inoue 2000; Inoue 2001; Kurosu 1979(a); Sakai 1998; Sakai
2001; Takeda & Nabeta 2001), five in Chinese,(Ding 1998; He
1997; Li & Shang 1997; Wang 1996; Wu (a) 1991), one in Nor-
wegian (Kittang 2001), one in Polish (Lopacz & Gralewski), and
one in German (Von Mencke 1988). The majority of the pop-
ulation included in these trials had chronic low-back pain (24
studies, 1718 patients). The control groups were the following:
no treatment, sham acupuncture, sham transcutaneous electrical
nerve stimulation (TENS), Chinese herbal medicine, education,
exercise, massage, moxibustion, non-steroidal anti-inflammatory
drugs, physiotherapy, spinal manipulation, TENS, trigger point
injections, and usual treatment by a general practitioner. Six stud-
ies compared the effectiveness of two different acupuncture tech-
niques.
M E T H O D O L O G I C A L Q U A L I T Y
The results of the methodological quality assessment are shown
in Additional Table 01. There were two studies with fatal flaws:
Giles & Muller 1999 had a 52% dropout during treatment pe-
riod in the acupuncture group and Grant 1999 had clinically im-
portant differences in the main outcome measures at baseline.
Therefore, these two trials are not included in the analyses or used
to draw conclusions. Of the remaining 33 trials, 14 were judged
to be of higher (Araki 2001; Carlsson 2001; Ceccherelli 2002;
Cherkin 2001; Garvey 1989; Inoue 2000; Inoue 2001; Kittang
2001; Leibing 2002; Meng 2003; Sakai 2001; Molsberger 2002;
Tsukayama 2002; Yeung 2003) and 19 to be of lower methodolog-
ical quality (Coan 1980; Ding 1998; Edelist 1976; Giles & Muller
2003; Gunn 1980; He 1997; Kerr 2003; Kurosu 1979(a); Kurosu
1979(b); Li & Shang 1997; Lehmann 1986; Lopacz & Gralewski;
MacDonald 1983; Mendelson 1983; Sakai 1998; Takeda & Na-
beta 2001; Thomas & Lundberg 94; Von Mencke 1988; Wang
1996; Wu (a) 1991). In none of the 35 trials was the care provider
5Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

blinded; in 28 trials, the timing of the outcome assessment was
similar in all groups. The biggest problem was the quality of report-
ing, which did not allow us to judge the following items: method
of randomization (15 trials), concealment of allocation (16 tri-
als), baseline differences (18 trials), co-interventions (18 trials) and
compliance (17 trials). Of the seven trials published in Japanese,
four were of higher (Araki 2001; Inoue 2000; Inoue 2001; Sakai
2001) and three were of lower methodological quality. All five tri-
als published in Chinese were of lower methodological quality.
R E S U L T S
STUDY SELECTION
Our searches resulted in the identification of 68 in CENTRAL,
49 reports in MEDLINE, and 85 in EMBASE. We obtained hard
copies of 40 articles, but excluded 17 because they did not meet
our inclusion criteria. In addition, we retrieved 16 hard copies
of studies published in Japanese and 11 published in Chinese,
but excluded nine and six respectively, because they did not meet
our inclusion criteria. Reasons for the exclusion of these studies
are explained in the Table of Excluded Studies. We contacted the
primary authors of eight trials to obtain additional information
that was not reported in the published study. Six responded to our
requests - all from the Japanese language trials.
CLINICAL RELEVANCE
The results of the clinical relevance assessment of each included
study are shown in Table 02. It should be noted that there was an
enormous variance in the way the authors judged the five items of
clinical relevance. This occurred because different pairs of authors
assessed the 35 trials and each author has a different background
and training. In addition, there were no clear instructions of what
should constitute a “yes” or “no” response for each question. As a
consequence, the assessment of clinical relevance of each individual
trial is subjective and difficult to analyse in the context of this
systematic review. Additional Table 04 shows the improvement
in pain for each treatment group and for each duration of low-
back pain. The average improvement in pain with acupuncture
for acute low-back pain was 52% (based on two studies), 32% for
chronic (16 studies) and 51% for unknown or mixed durations of
pains (eight studies). The average improvement of pain with no
treatment was 6% (six studies). The average improvement of pain
with sham or placebo therapies was 22% for acute (one study),
23% for chronic (six studies) and 25% for unknown or mixed
durations of pain (three studies).
ADEQUACY OF ACUPUNCTURE
The results are shown in Table 03. In all trials, acupuncture was
judged to be adequate for the population they included.
PRIMARY ANALYSES
1. Acupuncture compared to no treatment, placebo or sham
therapy (See Figure 01)
1a. Acupuncture versus no treatment for acute low-back pain:
There is no evidence because we did not find any RCT for this
comparison.
1b. Acupuncture versus sham therapy for acute low-back pain:
We found only one RCT and it used only one session of bilateral
acupuncture on the SI3 acupoint. Therefore, there is moderate
evidence (one higher quality trial, 40 people) (Araki 2001) that
there is no difference in pain and function, between one session
of acupuncture on the SI3 acupoint bilaterally and sham needling
of the same point immediately after the session.
1c. Acupuncture versus no treatment for chronic low-back pain:
The pooled analysis of two lower quality trials (90 people) (Coan
1980; Thomas & Lundberg 94) shows that acupuncture is more
effective than no treatment for patients with chronic low-back
pain for short term pain relief, with a SMD of -0.73 (95% CI -
1.19 to -0.28) (See comparison 05.01). There is limited evidence
(one lower quality trial, 40 people) (Thomas & Lundberg 94)
that acupuncture is also more effective at intermediate follow-up
for outcomes of pain. The pooled analysis of two lower quality
trials (90 people) (Coan 1980; Thomas & Lundberg 94) shows
that acupuncture is more effective than no treatment for patients
with chronic low-back pain in short-term functional improve-
ment, with an effect size of 0.63 (95% CI 0.19 to 1.08) (compar-
ison 05.07). There is limited evidence (one lower quality trial, 40
people) (Thomas & Lundberg 94) that there is no difference at
the intermediate-term follow-up in functional outcome, between
acupuncture and no treatment.
1d. Acupuncture versus sham therapy for chronic low-back
pain: Six trials (three higher and three lower quality) measured
pain outcomes (Carlsson 2001; Kerr 2003; Lehmann 1986; Leib-
ing 2002; Mendelson 1983; Molsberger 2002), and one higher and
two lower quality trials measured functional outcomes (Lehmann
1986; Leibing 2002; Mendelson 1983). Of five trials that mea-
sured pain immediately after the end of the sessions, four tri-
als could be pooled (Mendelson 1983; Leibing 2002; Molsberger
2002; Kerr 2003). The pooled analysis (two higher and two lower
quality RCTs, 314 people) shows that acupuncture is more effec-
tive than sham therapy with a WMD of -10.21 (95% CI -14.99
to -5.44) (comparison 06.01). The trial not included in the meta-
analysis (Lehmann 1986) included 36 people and found a trend
that acupuncture was better than sham therapy, but failed to reach
statistical significance. This trial could not be pooled with the
other studies because of the scale they used to measure pain and
the way they analysed the results. For short-term measures of pain,
there is strong evidence (two higher quality trials, 138 people)
(Carlsson 2001; Molsberger 2002) that acupuncture is more ef-
fective than sham therapy for patients with chronic low-back pain,
with a WMD of -17.79 (95% CI -25.5 to -10.07) (See compari-
son 06.01 and other data table 06.09). There are three trials (two
higher and one lower quality, 255 people) that assessed intermedi-
ate-term pain (Carlsson 2001; Lehmann 1986; Leibing 2002). All
6Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

three trials found a trend that acupuncture was better than sham
therapy, but without statistical significance. It was possible to pool
two of these studies, showing a WMD of -5.74 (95% CI -14.72 to
3.25) (See comparison 06.01). The only exception was the analysis
adjusted for baseline values conducted by Carlsson and Sjolund
(See other data table 06.09.03) that showed a statistically signif-
icant effect (p=0.007) in favour of acupuncture over sham ther-
apy. For long-term measures of pain, there is moderate evidence
(one higher quality trial, 51 people) (Carlsson 2001) that there is
no difference between acupuncture and sham therapy for chronic
low-back pain. For measures of function taken immediately after
the end of the sessions, there is moderate evidence (one higher
and two lower quality trials, 316 people) (Lehmann 1986; Leib-
ing 2002; Mendelson 1983) that there is no difference between
acupuncture and sham therapy. For measures of function taken
at intermediate-term follow-up, there is moderate evidence (one
higher and one lower quality trials, 204 people) (Lehmann 1986;
Leibing 2002) that there is no difference between acupuncture
and sham therapy for patients with chronic low-back pain. There
is no evidence from RCTs on the effectiveness of acupuncture for
patients with chronic low-back pain for functional measures at
short or long-term follow-ups.
2. Acupuncture compared to another intervention (See Figure
02)
2a. Acupuncture versus other interventions for acute low-back
pain: There is moderate evidence (one higher quality trial, 57
people) (Kittang 2001) that there is no difference immediately
after, at the short-term, or at the intermediate-term follow-ups
between acupuncture and Naproxen 500 mg, taken twice daily for
10 days, in measures of pain (VAS).
2b. Acupuncture versus other interventions for chronic low-
back pain: Compared to spinal manipulation, there is limited ev-
idence (one lower quality trial, 68 people) (Giles & Muller 2003)
that acupuncture is less effective for measures of pain and function
immediately after the end of the sessions. Compared to massage,
there is moderate evidence (one higher quality trial, 172 people)
(Cherkin 2001) that there is no difference immediately after the
sessions in pain between acupuncture and massage, but there is a
statistically significant difference in favour of massage at the long-
term follow-up. For measures of function, massage was statisti-
cally significantly more effective than acupuncture immediately
after the end of the sessions, but there was only a marginally sta-
tistically significant difference in favour of massage at the long-
term follow-up. However, differences in effect were only small
(moderate evidence). Compared to celecoxib, rofecoxib or parac-
etamol, there is limited evidence (one lower quality trial, 72 peo-
ple) (Giles & Muller 2003) that there is no difference immediately
after the end of the sessions in measures of pain and function.
There is conflicting evidence (two trials, 56 people) (Tsukayama
2002; Lehmann 1986) on the effectiveness of acupuncture com-
pared to TENS for patients with chronic low-back pain for pain
measured immediately after the end of the sessions: one higher
quality trial with a small sample size (Tsukayama 2002) found
a statistically significant difference in favour of acupuncture over
TENS, while one lower quality trial (Lehmann 1986) found no
difference. There is limited evidence (one lower quality trial, 36
people) (Lehmann 1986) that there is no difference at the interme-
diate-term follow-up in pain between acupuncture and TENS for
patients with chronic low-back pain. There is moderate evidence
(one higher and one lower quality trial, 56 people) (Tsukayama
2002; Lehmann 1986) that there is no difference immediately after
the end of the sessions in functional ability, between acupuncture
and TENS, and there is limited evidence that there is no differ-
ence at the intermediate-term follow-up (Lehmann 1986). Finally,
compared to self-care education, there is moderate evidence (one
higher quality trial, 184 people) (Cherkin 2001) that there is no
difference immediately after the end of the treatments and at the
long-term follow-up in pain and function, between acupuncture
and self-care education.
3. Acupuncture added to an intervention compared to the in-
tervention without acupuncture (See Figure 02)
3a. Addition of acupuncture to other interventions for acute
low-back pain: Only one lower quality trial (100 people) (He
1997) showed that there is limited evidence that the addition of
acupuncture and moxibustion to Chinese herbal medicine is more
effective than Chinese herbal medicine alone for a global measure
of pain and function at the long-term follow-up.
3b. Addition of acupuncture to other interventions for chronic
low-back pain: There are four higher-quality trials that assessed
the effects of acupuncture added to other therapies and com-
pared it to the other therapy alone (289 people) (Leibing 2002;
Meng 2003; Molsberger 2002; Yeung 2003). The other thera-
pies included: exercises, NSAIDs, aspirin, non-narcotic analgesic,
mud packs, infrared heat therapy, back care education, ergonomics
or behavioural modification. The pooled analysis (comparison
13.01) shows that the addition of acupuncture to other interven-
tions is more effective than the other intervention alone for pain,
measured immediately after the end of the sessions (four higher
quality trials, 289 people) with a SMD of -0.76 (95% CI -1.02 to-
0.5), at the short-term follow-up (three higher quality trials, 182
people) with a SMD of -1.1 (95% CI -1.62 to-0.58), and at the
intermediate-term follow-up (two higher quality trials, 115 peo-
ple) with a SMD of -0.76 (95% CI-1.14 to-0.38). These effects
were also observed for functional outcomes (comparison 13.07)
immediately after the end of the sessions (three higher quality tri-
als, 173 people) with a SMD of -0.95 (95% CI -1.27 to-0.63), at
the short-term follow-up with a SMD of -0.95 (95% CI -1.37 to-
0.54), and at the intermediate-term follow-up with a SMD of -
0.55 (95% CI-0.92 to-0.18).
SECONDARY ANALYSES
1. Other outcome measures
7Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Other outcome measures were extracted for the purpose of com-
plementing the conclusions based on the primary outcome mea-
sures.
1a. Global measures of improvement: Measures of global im-
provement included multiple-choice categorical scales (eg, im-
proved - same - worse) or dichotomous options (eg, improved -
not improved). In the case of multiple-choice categorical scales,
we dichotomized the categories according to the principle of “im-
proved” and “not improved”. The number of patients improved
was divided by the total number of patients in that group (com-
parison 03.02, 05.02, 06.02 and 07.02). These results were in
agreement with the result of the primary analysis, therefore they
do not change the conclusions and will not be discussed in this
review.
1b. Measures of work status: Measures of work status were basi-
cally the number of people who returned or had not returned to
work at follow-up. The pooled analysis of the two trials (one higher
and one lower quality, 58 people) (Carlsson 2001; Lehmann 1986)
that compared acupuncture to sham for chronic low-back pain
patients failed to show a difference at the intermediate-term fol-
low-up (comparison 06.06). Compared to TENS, there was one
lower quality trial (Lehmann 1986) that showed no difference in
return-to-work at the intermediate-term follow-up.
1c. Measures of physical examination: Measures of physical ex-
amination basically included range of motion of the lumbar region
measured, for example, by the finger-floor distance or Schober
tests (Araki 2001; Kerr 2003; Kittang 2001; Lehmann 1986; Leib-
ing 2002; Molsberger 2002; Takeda & Nabeta 2001; Thomas &
Lundberg 94; Von Mencke 1988) and a composite outcome mea-
sure based on physical exam (Edelist 1976; Wu (a) 1991; Wang
1996). We compared the agreement between the results of physical
examination with the results of pain and function in the trials that
reported these data. There were 16 situations in which pain and
physical examination were measured (eg, same trial, same com-
parison group, same follow-up, etc). There was agreement in 13
situations and disagreement in three. There were nine situations in
which functional outcomes and physical examination were mea-
sured (eg, same trial, same comparison group, same follow-up,
etc). There were five agreements and four disagreements.
1d. Measures of complications: Only 14 trials reported any mea-
sure of complications or side-effects (Carlsson 2001; Cherkin
2001; Garvey 1989; Giles & Muller 1999; Grant 1999; Kerr 2003;
Kittang 2001; Lehmann 1986; Leibing 2002; Meng 2003; Mols-
berger 2002; Sakai 2001; Tsukayama 2002; Yeung 2003). The re-
sults for complications that happened during the treatment period
showed that for a total of 245 patients who received acupuncture,
there were only 13 minor complications (5%), while for 156 pa-
tients who received sham therapy, there were no complications
(0%). In the group of 205 patients that received other interven-
tions (eg, TENS, NSAIDs, etc), there were 21 reports of compli-
cations (10%). None of the complications were fatal or so serious
that hospitalization was required.
2. Other comparisons
2a. Efficacy and effectiveness of dry-needling at trigger and mo-
tor points: (See Figure 03) There is limited evidence (one lower
quality trial, 17 patients) that superficial needling (4 mm) inserted
at trigger points is better than placebo TENS (MacDonald 1983).
Two randomized trials compared dry-needling with other inter-
ventions. There is limited evidence (one lower quality trial, 56
people) (Gunn 1980) that a few sessions of dry-needling, added to
a regimen of physiotherapy, occupational therapy and industrial
assessments is better than the regimen alone immediately after, at
the short and the intermediate-term follow-ups. There is moder-
ate evidence (one higher quality trial, 34 people) (Garvey 1989)
that there is no difference in short term global improvement be-
tween one session of dry-needling and one session of trigger point
injection with lidocaine and steroid, one session of trigger point
injection with lidocaine only, or one session of cooling spray over
the trigger point area followed by acupressure.
2b. Comparison between different techniques of acupuncture:
(See Figure 04)
i. For acute low-back pain, one single session of bilateral needling
of SI3 is better than one single session of needling of Yaotongxue
(Extra 29, EX-UE 7) (one lower quality trial, 150 patients) (Wu
(a) 1991)
ii. For chronic low-back pain, deep stimulation (1.5 cm in the
muscle or in the trigger point) is better than superficial stimulation
(2 mm in the subcutaneous tissue) immediately after the sessions
and at the short-term follow-up (one higher quality trial, 42 pa-
tients) (Ceccherelli 2002)
iii. For chronic low-back pain, the ancient needling technique
is better than the regular needling technique at the short-term
follow-up (one lower quality trial, 54 patients) (Ding 1998)
iv. For chronic low-back pain, manual acupuncture has the same
effects as electroacupuncture, both at the short and long-term
follow-ups (one higher quality trial, 34 patients) (Carlsson 2001)
v. For low-back pain of any duration, distal point needling is no
different from local lumbar area needling for measures of pain,
function and range of motion (one lower quality trial, 20 patients)
(Takeda & Nabeta 2001)
vi. For low-back pain of any duration, needle retention for about
10 minutes is better than removal immediately after insertion (one
lower quality trial, 20 patients) (Kurosu 1979(b)
vii. For low-back pain of any duration, local needling plus cupping
is more effective than distal treatment plus electrical stimulation
(one lower quality trial, 492 patients) (Wang 1996)
viii. For low-back pain of any duration, manual acupuncture plus
cupping is better than manual acupuncture alone (one lower qual-
ity trial, 156 patients) (Li & Shang 1997)
In summary, the best technique of acupuncture is still to be de-
termined, but the available high quality randomized trials suggest
8Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

that the best technique of acupuncture for low-back pain includes
deep stimulation (1.5 cm) instead of superficial stimulation (2
mm) and it seems that electrostimulation does not add any benefit
to manual stimulation of the needles.
2c. Efficacy and effectiveness of acupuncture for mixed popu-
lations of acute/chronic low-back pain: There were a few trials
that did not specify the duration of the low-back pain or that
mixed acute with chronic patients (Inoue 2000; Inoue 2001; Von
Mencke 1988; Sakai 1998; Kurosu 1979(a)). These trials will not
be discussed because they do not change the conclusions of this
review.
D I S C U S S I O N
Thirty-five RCTs covering 2861 patients were included in this
systematic review. There were only three trials of acupuncture for
acute low-back pain that do not justify firm conclusions, because
of small sample sizes and low methodological quality of the studies.
There is some evidence that acupuncture may be better than no
treatment or sham treatment for chronic low-back pain. However,
most studies have not found acupuncture to be more effective than
other conventional treatments (eg, analgesics, NSAIDs, TENS
and self-care education) or “alternative” treatments (eg, massage
or spinal manipulation). The data suggest that both acupuncture
and dry-needling may be useful adjuncts to other therapies for
chronic low-back pain.
Although the conclusions showed some positive results of
acupuncture, the magnitude of the effects were generally small.
The average pain reduction (measured by continuous scales such
as the VAS) in the group that received acupuncture for chronic
low-back pain was 32% compared to 23% in those who received
sham therapies and 6% in those who received no treatment. Fur-
thermore, the terms used to express the strength of the evidence
(strong, moderate and limited), as is standard in many systematic
reviews, might be misinterpreted. These are relative terms and are
often used to apply to a small number of “higher” quality studies.
This may give the false impression that “strong” evidence means
“definite” evidence, but this may not be the case.
Although efforts were made to find all published RCTs, some rel-
evant trials might have been missed. Twenty of the 35 included
RCTs were published in English, seven in Japanese, five in Chinese
and one each in Norwegian, Polish and German. Although no
languages were excluded, the number of non-English journals in-
dexed in electronic databases such as MEDLINE and EMBASE is
limited. If additional trials are found, this review will be updated.
The methodologic quality of the included RCTs, although im-
proving over the past several years, was poor. There were two stud-
ies with fatal flaws, and 14 studies with higher and 19 studies with
lower methodological quality. The methodologic quality in the
current review was defined by the internal validity criteria, which
referred to characteristics of the study that might be related to
selection, performance, attrition, and detection bias. It seems rea-
sonable that in the authors’ qualitative synthesis, the best evidence
would be provided by the higher quality studies, which are less
likely to have biased results. Although the levels of evidence in this
review may be considered arbitrary, it seems unlikely that a differ-
ent rating system would have resulted in different conclusions.
The included studies were very heterogeneous in terms of popula-
tion included, type of acupuncture administered, control groups,
outcome measures, timing of follow-up, and presentation of data.
Therefore, very few meaningful meta-analyses could be performed
and it was difficult to reach conclusions for most types of treat-
ments.
The experience and training of the acupuncturists who gave the
treatments were mentioned in a few studies. Some studies used
a protocol of a fixed set of points for all patients while others
used a flexible protocol where the points were selected for each
individual. Both methods are considered to be valid and were
analyzed together in this systematic review.
No serious adverse events were reported in the trials included in
this review. The incidence of minor adverse events was 5% in the
patients submitted to acupuncture. In the literature, most of the
reports of serious adverse events related to acupuncture are de-
scribed as case reports. In the past years, various prospective stud-
ies were conducted, enabling the estimation of the true incidence
of minor and major adverse events.
Melchart and colleagues reported the biggest prospective study,
covering over 760,000 treatments delivered by 7,050 German
physicians over a 10-month period. They observed 6,936 minor
(incidence of 91 per 10,000 treatments) and five major adverse
reactions (6 per 1,000,000 treatments), which included: exacerba-
tion of depression (one case), acute hypertensive crisis (one case),
vasovagal reaction (one case), asthma attack with hypertension
and angina (one case) and two cases of pneumothorax (Melchart
2004).
The other prospective studies did not observe any major adverse
reactions. Yamashita and colleagues observed 65,482 treatments
delivered by 84 therapists over a six-year period in Japan. There
were 94 cases of minor adverse events, with an incidence of 14
per 10,000 treatments, but this incidence was estimated using
data from spontaneous reports of adverse event by the practi-
tioner (Yamashita 1999). In another similar study by Yamashita
and colleagues, they forced practitioners to detect and report every
acupuncture session, whether there were adverse reactions or not.
Then, different incident rates of adverse reaction were obtained. A
total of 391 patients were treated in 1,441 sessions, involving a to-
tal of 30,338 needle insertions. The incidence of recorded systemic
reactions in individual patients was: tiredness (8.2%); drowsiness
(2.8%); aggravation of pre-existing symptoms (2.8%); itching in
the punctured regions (1.0%); dizziness or vertigo (0.8%); feeling
9Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

of faintness or nausea during treatment (0.8%); headache (0.5%);
and chest pain (0.3%) (Yamashita 2000).
MacPherson and colleagues observed 34,407 treatments delivered
by 574 Traditional Chinese Acupuncturists in the UK, over a four-
week period. There were 43 minor adverse events (incidence of
12.5 per 10,000 treatments) (MacPherson 2001). White and col-
leagues observed 31,822 treatments delivered by 78 acupunctur-
ists (physicians and physiotherapists) in the UK, over a 21-month
period. There were 43 minor adverse reactions (incidence of 13.5
per 10,000 treatments) (White 2001). Odsberg and colleagues
observed 9,277 treatments delivered by 187 physiotherapists in
Sweden over a four-week period, and recorded 2,108 minor ad-
verse reactions (incidence of 2,272 per 10,000 treatments) (Ods-
berg 2001). Ernst and colleagues observed 3,535 treatments de-
livered by 29 acupuncturists in Germany over a 13-month period,
and recorded 402 minor adverse reactions (incidence of 1,100 per
10,000 treatments) (Ernst 2003).
The great variation in incidence of minor adverse events is prob-
ably due to different definitions of adverse reaction, research de-
signs, or styles of acupuncture in the various studies.
Because serious adverse events are rare, they continue to be re-
ported in the form of case reports. Recently published systematic
reviews of case reports showed that these serious complications
may include infections (human immunodeficiency virus, hepati-
tis, bacterial endocarditis) caused by non sterile needles, and fa-
tal tissue trauma (pneumothorax, cardiac tamponade, spinal cord
injury) (Cherkin 2003; Chung 2003; Yamashita 2001). Further-
more, we have little information about the safety of acupuncture
specifically for low-back pain. We need more information about
the safety of acupuncture that focuses on specific conditions.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
There were only three heterogeneous trials of acupuncture for
acute low-back pain. Therefore we could not reach convincing
conclusion and there is a need for future studies to make recom-
mendation in this area.
There is some evidence of the effects of acupuncture for chronic
low-back pain. Compared to no treatment, there is evidence for
pain relief and functional improvement for acupuncture at shorter-
term follow-ups. Compared to sham therapies, there is evidence
for pain relief at shorter-term follow-up, but these effects were
not maintained at the longer-term follow-ups, nor were they ob-
served for functional outcomes. Compared to other conventional
or “alternative” treatments, acupuncture is no better for measures
of pain and function. There is evidence that acupuncture, added
to other conventional therapies, relieves pain and improves func-
tion better than conventional therapies alone. According to these
results, acupuncture may be useful as either a unique therapy for
chronic low-back pain or as an adjunct therapy to other conven-
tional therapies. Although the conclusions show some positive re-
sults of acupuncture, the magnitude of the effects were generally
small.
Although dry-needling appears to be a useful adjunct to other
therapies for chronic low-back pain, no clear recommendations
can be made because of small sample sizes and low methodological
quality of the studies.
With respect to the different techniques of acupuncture, most
studies were either small, of lower methodological quality, or both,
therefore, no clear recommendation could be made.
Implications for research
Because most of the studies were of poor methodological qual-
ity, there certainly is a need for future higher-quality RCTs. Also,
because many trials were poorly reported, we recommend that
authors use the CONSORT statement as a model for reporting
RCTs (www.consort-statement.org) and use the STRICTA crite-
ria (MacPherson 2002) to report the interventions. Many trials
could not be included in the meta-analyses because of the way
the authors reported the results, therefore we suggest that publi-
cations of future trials report means with standard deviations for
continuous measures, or number of events and total patients ana-
lyzed for dichotomous measures. Future research should focus on
areas where there are few or no trials, for example, acupuncture
compared to no treatment, placebo or sham for acute low-back
pain. Future studies should also have larger sample sizes, use a
valid acupuncture treatment, and have both a short-term and a
long-term follow-up (for chronic pain). From the available high
quality trials included in this review, deep stimulation seems to
be the most promising acupuncture treatment. Future studies are
needed that evaluate superior features of acupuncture. We suggest
that publications of future trials report the proportion of subjects
who obtain a clinically important improvement in the groups be-
ing compared to facilitate a judgment about clinically important
differences between the groups. Although an evaluation of costs
was not the objective of this review, we suggest that future research
assesses cost-effectiveness of acupuncture compared to other treat-
ments.
F E E D B A C K
March 2005
Summary
Feedback 1: When assessing the outcome of acupuncture therapy
for the low back, what points were used? What I have observed
is there is an immediate proprioceptive effect with the patients
following the therapy. Where there is a mild paresis on clinical ex-
amination, what I think acupuncture does is to establish a recruit-
ment of those muscle fibres that are paretic due to whatever cause.
10Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Possible TypeII fibres are activated. Therefore, any post assessment
should not necessarily just assess pain but should include propri-
oceptive assessments, motor function and coordinatice activties.
Feedback 2: Which acupoints were used? What were the classi-
cal symptoms of pain being modified? My understanding is that
whilst acupuncture modifies pain, in doing so the manifestations
of pain are being treated. In the outcome of the study you men-
tion function as one of those outcomes. What were the functional
factors and how were they measured?
I am interested in the inclusion and exclusion criteria for partic-
ipants in the study, were there any controls, that is, particpants
without low back pain?
Author’s reply
Response 1: The outcomes were assessed immediately after the
end of treatment, and at short, intermediate and long-term fol-
low-ups. Definitions of these time-lines are given in the review.
The outcomes of interest were patient-reported pain and function.
The authors of the systematic review did not include neurological
outcomes and neither did the trials. We don’t know if data were
collected on these items in the original studies and not included
in the published reports.
Response 2: I think some of the details you are looking for can
be found in the ’Table of Included Studies’. If they are not listed,
its because they were not included in the published report of the
primary study, but to be sure, you may wish to refer to some of
the primary studies if you had particular questions. The full text
outlines which studies were included in these comparisons: [i]
Acupuncture compared to no treatment, placebo or sham therapy
[ii] Acupuncture compared to another intervention [iii] Acupunc-
ture added to an intervention compared to the intervention with-
out acupuncture. The authors also outline other outcomes and
comparisons in the results section. The inclusion criteria only in-
cluded Individuals with back pain.
Different aspects of pain and the tool used to measure them would
have been addressed in different studies ... this will be in the Table
of Included Studies; ditto for functional outcomes and measure-
ment tools and participants of each study.
Contributors
Dr Henare R Broughton, Occupation Family Physician
Dr Andrea Furlan, review author
P O T E N T I A L C O N F L I C T O F
I N T E R E S T
Three coauthors of this review (DC, HT and LXL) are also authors
of some included trials. In order to avoid any conflict of interest,
they were not involved in the methodological quality assessment
or data extraction of their own study.
A C K N O W L E D G E M E N T S
We would like to thank Maoling Wei from the Chinese Cochrane
Centre for searching the Chinese databases. We are grateful to
Mrs Gunn Elisabeth Vist who extracted the data from the Nor-
wegian paper and Marcos Hsu and Hitoshi Yamashita who were
the second authors for the Chinese and Japanese papers respec-
tively. We would like to thank the panel of experts for their im-
portant contribution to this review: Satiko Imamura, Marta Ima-
mura, Wu Tu Hsing, Helena Kazyama, Chien Hsin Fen and Lil-
iana George. We are also grateful to all authors who replied to our
requests to obtain more information. We also would like to thank
Sheilah Hogg-Johnson and Joseph Beyene for their assistance with
the statistical analyses. Finally we would like to thank the editors
of the Cochrane Back Review group who provided constructive
comments and Vicki Pennick, co-ordinator of the Cochrane Back
Review Group for her assistance and amendments.
Brian Berman’s work on this review was partially funded by Grant
Number R24 AT001293 from the National Center for Comple-
mentary and Alternative Medicine (NCCAM). The contents of
this article are solely the responsibility of the authors and do not
necessarily represent the official views of the NCCAM, or the Na-
tional Institutes of Health.
S O U R C E S O F S U P P O R T
External sources of support
• National Center for Complementary and Alternative Medicine
USA
Internal sources of support
• Institute for Work & Health CANADA
• Erasmus MC, Department of General Practice NETHER-
LANDS
• Vrije Universiteit, EMGO Institute NETHERLANDS
11Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

R E F E R E N C E S
References to studies included in this review
Araki 2001 {published and unpublished data}
Araki S, Kawamura O, Mataka T, Fujioka H, et al.Randomized con-
trolled trial comparing the effect of manual acupuncture with sham
acupuncture for acute low back pain [RCT ni yoru kyusei yotsu-sho
ni taisuru shishin-gun to gishin-gun no tiryou koka]. Journal of the
Japan Society of Acupuncture and Moxibustion 2001;51(3):382.
Carlsson (even) {published data only}
Carlsson (morn) {published data only}
Carlsson 2001 {published data only}
Carlsson CP, Sjolund BH. Acupuncture for chronic low back pain:
a randomized placebo-controlled study with long-term follow-up.
Clin J Pain 2001;17(4):296–305. [MEDLINE: 915].
Ceccherelli 2002 {published data only}
Ceccherelli F, Rigoni MT, Gagliardi G, Ruzzante L. Comparison of
superficial and deep acupuncture in the treatment of lumbar myofas-
cial pain: a double-blind randomized controlled study. Clin J Pain
2002;18(3):149–153. [MEDLINE: 1045].
Cherkin 2001 {published data only}
Cherkin DC, Eisenberg D, Sherman KJ, Barlow W, Kaptchuk TJ,
Street J, et al.Randomized trial comparing traditional Chinese med-
ical acupuncture, therapeutic massage, and self-care education for
chronic low back pain. Archives of Internal Medicine 2001;161(8):
1081–1088. [MEDLINE: 886].
Kalauokalani D, Cherkin DC, Sherman KJ, Koepsell TD, Deyo RA.
Lessons from a trial of acupuncture and massage for low back pain:
patient expectations and treatment effects. Spine 2001;26(13):1418–
1424.
Cherkin 2001 (mass) {published data only}
Cherkin 2001 (sc) {published data only}
Coan 1980 {published data only}
Coan RM, Wong G, Ku SL, Chan YC, Wang L, Ozer FT, et al.The
acupuncture treatment of low back pain: a randomized controlled
study. Am J Chinese Med 1980;8:181–189.
Ding 1998 {published data only}
Ding YD. Fly-probing-acupoint manipulation as a main treatment
for lumbago. Shanghai Journal of Acupuncture and Moxibustion 1998;
17(5):25–26. [MEDLINE: 4].
Edelist 1976 {published data only}
Edelist G, Gross AE, Langer F. Treatment of low back pain with
acupuncture. Canad Anaesth Soc J 1976;23:303–306.
Garvey 1989 {published data only}
Garvey TA, Marks MR, Wiesel SW. A prospective, randomized, dou-
ble-blind evaluation of trigger-point injection therapy for low-back
pain. Spine 1989;14:962–964.
Garvey 1989 (lidoc) {published data only}
Garvey 1989 (spray) {published data only}
Garvey 1989(steroid) {published data only}
Giles & Muller 1999 {published data only}
Giles LG, Muller R. Chronic spinal pain syndromes: a clinical pilot
trial comparing acupuncture, a nonsteroidal anti-inflammatory drug,
and spinal manipulation. 1999;22(6):376–381. [MEDLINE: 807].
Giles & Muller 2003 {published data only}
Giles LGF, Muller R. Chronic spinal pain. A randomized clinical trial
comparing medication, acupuncture and spinal manipulation. Spine
2003;28(14):1490–1503.
Giles 1999 (manip) {published data only}
Giles 1999 (NSAID) {published data only}
Giles 2003 (manip) {published data only}
Giles 2003 (NSAID) {published data only}
Grant 1999 {published data only}
Grant DJ, Bishop-Miller J, Winchester DM, Anderson M, Faulkner
S. A randomized comparative trial of acupuncture versus transcuta-
neous electrical nerve stimulation for chronic back pain in the elderly.
Pain 1999;82(1):9–13. [MEDLINE: 1081].
Gunn 1980 {published data only}
Gunn CC, Milbrandt WE, Little AS, Mason KE. Dry needling of
muscle motor points for chronic low-back pain: a randomized clinical
trial with long-term follow-up. Spine 1980;5:279–291.
He 1997 {published data only}
He RY. Clinical Observation on Treatment of Lumbago due to Cold-
Dampness By Warm-Acupuncture Plus Chinese Medicine. Chi-
nese Acupuncture & Moxibustion 1997;17(5):279–80. [MEDLINE:
1753].
Inoue 2000 {published and unpublished data}
Inoue M, Kitakouji H, Ikeuchi R, Katayama K, Ochi H, et
al.Randomized controlled pilot study comparing acupuncture with
sham acupuncture for lumbago [Yotsu ni taisuru gishin wo mochiita
randamuka hikaku-shiken no kokoromi]. Journal of the Japan Soci-
ety of Acupuncture and Moxibustion 2000;50(2):356. [MEDLINE:
1771].
Inoue 2001 {published and unpublished data}
Inoue M, Kitakouji H, Ikeuchi R, Katayama K, Ochi H, et
al.Randomized controlled pilot study comparing manual acupunc-
ture with sham acupuncture for lumbago (2nd report) [Yotsu ni
taisuru gishin wo mochiita randamuka hikaku-shiken no kokoromi].
Journal of The Japan Society of Acupuncture and Moxibustion 2001;51
(3):412.
Kerr 2003 {published data only}
Kerr DP, Walsh DM, Baxter D. Acupuncture in the management of
chronic low back pain: a blinded randomized controlled trial. The
Clinical Journal of Pain 2003;19:364–370.
Kittang 2001 {published data only}
Kittang G, Melvaer T, Baerheim A. [Acupuncture contra antiphlogis-
tics in acute lumbago]. Tidsskr Nor Laegeforen 2001;121(10):1207–
1210. [MEDLINE: 1101].
Kurosu 1979(a) {published data only}
Kurosu Y. Acupuncture and Moxibustion for Lumbago (II) - Com-
parative Experiment of the Therapeutic Effectiveness of Acupunc-
ture and Garlic Moxibustion. The Journal of the Japan Acupuncture
& Moxibustion Association 1979;28(2):31–34. [MEDLINE: 1765].
12Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Kurosu 1979(b) {published data only}
Lehmann 1986 {published data only}
Lehmann TR, Russell DW, Spratt KF. The impact of patients with
nonorganic physical findings on a controlled trial of transcutaneous
electrical nerve stimulation and electroacupuncture. Spine 1983;8:
625–634.
∗Lehmann TR, Russell DW, Spratt KF, Colby H, Liu YK, Fairchild
ML, Christensen S. Efficacy of electroacupuncture and TENS in the
rehabilitation of chronic low back pain patients. Pain 1986;26:277–
290.
Leibing 2002 {published data only}
Leibing E, Leonhardt U, Koster G, Goerlitz A, Rosenfeldt JA, Hilgers
R, et al.Acupuncture treatment of chronic low-back pain - a random-
ized, blinded, placebo-controlled trial with 9-month follow-up. Pain
2002;96(1-2):189–196. [MEDLINE: 1113].
Li & Shang 1997 {published data only}
Li Q, Shang WM. The effect of acupuncture plus cupping on 78
cases with lumbago. Hebei Chinese Traditional Medicine 1997;19(5):
28. [MEDLINE: 1754].
Lopacz & Gralewski {published data only}
Lopacz S, Gralewski Z. A trial of assessment of the results of acupunc-
ture or suggestion in the treatment of low back pain. Neur Neurochir
Pol 1979;8:405–409.
MacDonald 1983 {published data only}
MacDonald AJ, Macrae KD, Master BR, Rubin AP. Superficial
acupuncture in the relief of chronic low back pain. Ann Royal Coll
Surg Engl 1983;65:44–46.
Mendelson 1983 {published data only}
Mendelson G, Kidson MA, Loh ST, Scott DF, Selwood TS, Kranz
H. Acupuncture analgesia for chronic low back pain. Clin Exp Neurol
1978;15:182–185.
∗Mendelson G, Selwood TS, Kranz H, Loh TS, Kidson MA, Scott
DS. Acupuncture treatment of chronic back pain.: a double-blind
placebo-controlled trial. Am J Med 1983;74:49–55.
Meng 2003 {published data only}
Meng CF, Wang D, Ngeow J, Lao L, Peterson M, Paget S. Acupunc-
ture for chronic low back pain in older patients: a randomized, con-
trolled trial. Rheumatology 2003;42:1–10.
Molsberger 2002 {published data only}
Molsberger A, Winkler J, Schneider S, Mau J. Acupuncture and con-
ventional orthopedic pain treatment in the management of chronic
low back pain - a prospective randomised and controlled clinical trial.
ISSLS. 1998:87.
Molsberger AF, Mau J, Pawelec DB, Winkler J. Does acupuncture
improve the orthopedic management of chronic low back pain--a
randomized, blinded, controlled trial with 3 months follow up. Pain
2002;99(3):579–587. [MEDLINE: 1760].
Sakai 1998 {published and unpublished data}
Sakai T, Tsukayama H, Amagai H, Kawamoto M, Masuda K, et
al.Controlled trial on acupuncture for lumbago [Yotsu ni taisuru hari
no hikaku-taisyo-shiken]. Journal of the Japan Society of Acupuncture
and Moxibustion 1998;48(1):110. [MEDLINE: 1773].
Sakai 2001 {published data only}
Sakai T, Tsutani K, Tsukayama H, Nakamura T, Ikeuchi T,
Kawamoto M, et al.Multi-center randomized controlled trial of
acupuncture with electric stimulation and acupuncture-like transcu-
taneous electrical nerve stimulation for lumbago. Journal of the Japan
Society of Acupuncture and Moxibustion 2001;51:175–84.
Yamashita H. Are the Effects of Electro-Acupuncture on Low Back
Pain Equal to those of TENS?. Focus on Alternative and Complemen-
tary Therapies 2001;6(4):254–255. [MEDLINE: 1752].
Takeda & Nabeta 2001 {published and unpublished data}
Takeda H, Nabeta T. Randomized controlled trial comparing the
effect of distal point needling with local point needling for low back
pain [RCT ni yoru yotsu-sho ni taisuru enkakubu-sisin to kyokusho-
sisin no koka hikaku]. Journal of the Japan Society of Acupuncture and
Moxibustion 2001;51(3):411.
Thomas & Lundberg 94 {published data only}∗Thomas M, Lundberg T. Importance of modes of acupuncture in
the treatment of chronic nociceptive low back pain. Acta Anaesthesiol
Scand 1994;38:63–69.
Tsukayama 2002 {published data only}
Tsukayama H, Yamashita H, Amagai H, Tanno Y. Randomised con-
trolled trial comparing the effectiveness of electroacupuncture and
TENS for low back pain: a preliminary study for a pragmatic trial.
Acupuncture in Medicine 2002;20(4):175–180. [MEDLINE: 1758].
Von Mencke 1988 {published data only}∗Von Mencke M, Wieden TE, Hoppe M, Porschke W, Hoffmann
O, Herget HF. Akupunktur des Schulter-Arm-Syndroms und der
Lumbagie/Ischialgie - zwei prosepktive Doppelblind-Studien* (Teil
I). Akupunktur 1988;4:204–215.
Von Mencke M, Wieden TE, Hoppe M, Porschke W, Hoffmann
O, Herget HF. Akupunktur des Schulter-Arm-Syndroms und der
Lumbagie/Ischialgie - zwei prosepktive Doppelblind-Studien* (Teil
II). Akupunktur 1989;5:5–13.
Wang 1996 {published data only}
Wang JX. The effect of acupuncture on 492 cases with lumbago.
Shanghai Acupuncture Journal 1996;15(5):28. [MEDLINE: 1755].
Wu (a) 1991 {published data only}
Wu YC ea. Acupuncture for 150 cases of acute lumbago. Shanghai
Journal of Acupuncture and Moxibustion 1991;10(2):18–19. [MED-
LINE: 3].
Wu (b) 1991 {published data only}
Yeung 2003 {published data only}
Yeung CKN, Leung MCP, Chow DHK. The use of electro-acupunc-
ture in conjunction with exercise for the treatment of chronic low-
back pain. The journal of alternative and complementary medicine
2003;9(4):479–490.
References to studies excluded from this review
Cai 1996
Cai Gw ZDLL. Clinic research in treatment of acute sciatica by
needling YaoYangKuan (DU3) deep. Shangai J of Acupuncture 1996;
15(2):8–9.
13Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Duplan 1983
Duplan B, Cabanel G, Piton JL, Grauer Jl, Phelip X. Acupuncture
et lombosciatique a la phase aiguë: etude en double aveugle de trente
cas. Sem Hop Paris 1983;59:3109–3114.
Fox and Melzack 1976
Fox EJ, Melzack R. Transcutaneous electrical stimulation and
acupuncture: comparison of treatment for low-back pain. Pain 1976;
2(141-148).
Franke 2000
Franke A, Gebauer S, Franke K, Brockow T. [Acupuncture massage
vs Swedish massage and individual exercise vs group exercise in low
back pain sufferers--a randomized controlled clinical trial in a 2 x 2
factorial design]. Forsch Komplementarmed Klass Naturheilkd 2000;7
(6):286–293. [MEDLINE: 958].
Fujinuki 1989
Fujinuki R. Yobu sekityukan kyosakusyo no shinkyu tiryo ni kansuru
kenkyu (2). The study of acupuncture & moxibustion for lumbar
spinal canal stenosis (2). Journal of the Japan Acupuncture and Moxi-
bustion 1989;48(11):6–13. [MEDLINE: 1769].
Galacchi 1981
Gallacchi G, Muller W, Plattner GR, Schnorrenberger CC.
[Akupunktur - und Laserstrahlbehandlung beim Zervikal - and Lum-
balsyndrom]. Schweiz Med Wschr 1981;111:1360–66.
Gallacchi 1983
Gallacchi G, Muller W. [Akupunktur - bringt sie etwas?]. Schweiz
Rundschau Med 1983;72(22):778–82.
Ghia 1976
Guia JN, Mao W, Toomey T, Gregg JM. Acupuncture and chronic
pain mechanisms. Pain 1976;2(285-99).
Hackett 1988
Hackett GI, Seddon D, Kaminski D. Electroacupuncture compared
with paracetamol for acute low back pain. Practitioner 1988;232:
163–164.
Ishimaru 1993
Ishimaru K, Shinohara S, Kitade T, Yhodo M. Clinical efficacy of
electrical heat acupuncture (First report): effect on low-back pain.
American Journal of Acupuncture 1993;21(1):13–18.
Junnila 1982
Junnila SYT. Acupuncture therapy for chronic pain. American Journal
of Acupuncture 1982;10(3):259–62.
Kinoshita 1965
Kinoshita H. Comparative observation in Goshin-ho and Hinaishin-
po. The Journal of the Japan Acupuncture & Moxibustion Association
1965;18(2):5–9. [MEDLINE: 1763].
Kinoshita 1971
Kinoshita H. Consideration of tonification and dispertion based
upon clinical experiment. The Journal of the Japan Acupuncture &
Moxibustion Association 1971;20(3):6–13. [MEDLINE: 1762].
Kinoshita 1981
Kinoshita H, Kinoshita N. Clinical Research in the Use of Paraneural
Acupuncture for Sciatica. The Journal of the Japan Acupuncture &
Moxibustion Association 1981;30(1):4–13. [MEDLINE: 1767].
Koike 1975
Koike Y. Quantity of stimulation in the treatment of lumbago.
Acupuncture treatment for lumbago. The Journal of the Japan
Acupuncture & Moxibustion Association 1975;24(3):8–13. [MED-
LINE: 1761].
Kuramoto 1977
Kuramoto S. A clinical study of the effects of electrical acupuncture
on protrusions of the intervertebral discs. The Journal of the Japan
Acupuncture & Moxibustion Association 1977;26(2):45–48. [MED-
LINE: 1764].
Laitinen 1976
Laitinen J. Acupuncture and transcutaneous electric stimulation in
the treatment of chronic sacrolumbalgia and ischialgia. American
Journal of Chinese Medicine 1976;4(2):169–175.
Li 1994
Li J, Chenard JR, Marchand S, Charest J, Lavignolle B. Points
d’acupuncture et zones-gachettes: réponse a la presson et résistance
cutanée chez des lombalgies chroniques. Rhumatologie 1994;46:11–
19. [MEDLINE: 437].
Megumi 1979
Megumi N. Acupuncture-moxibustion Therapy for the Lumbago
known as Colic. The Journal of the Japan Acupuncture & Moxibustion
Association 1979;28(2):35–44. [MEDLINE: 1766].
Ren 1996
Ren, Tian-Ming. Needling Taichong (Liv 3) and Mingmen (Du 4 or
GV 4) to treat lower back pain. Journal of Clinical Acupuncture 1996;
12(5-6):90.
Shinohara 2000
Shinohara S, Kitade K, Tanzawa S. Effect of acupuncture based on
Jingjin (channel sinews) theory for musculoskeletal conditions [Un-
doki-kei shojo ni keikin no gainen wo katsuyo-shita rinsyo-hoho to
sono koka]. Journal of the Japan Society of Acupuncture and Moxibus-
tion 2000;50(2):340. [MEDLINE: 1770].
Sodipo 1981
Sodipo JOA. Transcutaneous electrical nerve stimulation (TENS)
and acupuncture: comparison of therapy for low-back pain. Pain.
1981:S277.
Sugiyama 1984
Sugiyama N, Ito F, Takagi T. The effect of acupuncture and mobi-
lization on lumbago. Journal of the Japan Society of Acupuncture and
Moxibustion 1984;33(4):402–9. [MEDLINE: 1768].
Wang 1997
Wang RY. The effect of acupuncture with moxibustion or acupunc-
true with cupping on 167 cases with lumbago. Anhui Chinese Tradi-
tional Medicine Clinical Journal 1997;9:272–3. [MEDLINE: 1756].
Wang 2000
Wang RR, Tronnier V. Effect of acupuncture on pain management
in patients before and after lumbar disc protrusion surgery - a ran-
domized control study. American Journal of Chinese Medicine 2000;
28(1):25–33.
Wedenberg 2000
Wedenberg K. A prospective randomized study comparing acupunc-
ture with physiotherapy for low-back and pelvic pain in pregnancy.
Acta Obstet Gynecol Scand 2000;79:331–335.
Xingsheng 1998
Xingsheng C. Comparative study on acupuncture needling methods
for sciatica: routine needling vs point-to-point penetration and deep
puncture. American Journal of Acupuncture 1998;26(1):37–41.
14Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Xu 1996
Xu L, Zhi-xiang Z, Xian-ming L, Guang-zhan L, Cheng-xuan Q.
Acupuncture plus massage versus massage alone in treating acute
lumbar sprain. International Journal of Clinical Acupuncture 1996;7
(3):365–67.
Yue 1978
Yue SJ. Acupuncture for chronic back and neck pain. Acupuncture &
Electro-Therapeut Res Int J 1978;3:323–24.
Zhang 1995
Zhang ZT, Zhang QZ. The effect of acupuncture plus chiropractic
on 57 cases with waist protrusion of the intervertebral disk. Neck pain
and Lumbago Journal 1995;16(2):97–8. [MEDLINE: 1757].
Zhang 1996
Zhang HP, Du SP, u LJ. [Observation on therapeutic effects of
110 cases with sciatica treated by electro-acupuncture deeply at
Yaoyangguan]. Chinese Acupuncture & Moxibustion 1996;16(8):19–
20. [MEDLINE: 2].
Zhi 1995
Zhi L, Jing S. Clinical comparison between scalp acupuncture com-
bined with a single body acupoint and body acupuncture alone for
the treatment of sciatica. American Journal of Acupuncture 1995;23
(4):305–7.
References to ongoing studies
Cherkin
Efficacy of Acupuncture for Chronic Low Back Pain. Ongoing
study Funding: National Center for Complementary and Alternative
Medicine (NCCAM).
GerAc
German Acupuncture Trials. Ongoing study Starting date of trial not
provided. Contact author for more information.
Harvard Med School
Physical CAM Therapies for Chronic Low Back Pain. Ongoing study
Funding: NIH.
Kong
Ongoing study Starting date of trial not provided. Contact author
for more information.
Munglani
Randomised controlled single-blinded trial of deep intra-muscular
stimulation in the treatment of chronic mechanical low back pain..
Ongoing study Starting date of trial not provided. Contact author
for more information.
Thomas
Longer term clinical and economic benefits of offering acupuncture
to patients with chronic low back pain.. Ongoing study Funding:
NHS.
Additional referencesCherkin 2003
Cherkin DC, Sherman KJ, Deyo RA, Shekelle PG. A review of the
evidence for the effectiveness, safety and costs of acupuncture, mas-
sage therapy and spinal manipulation for back pain. Ann Int Med
2003;138:898–906.
Chu 1979
Chu LSW, Yeh SDJ, Wood DD. Acupuncture manual: a western ap-
proach. New York: Marcel Dekker Inc.
Chung 2003
Chung A, Bui L, Mills E. Adverse effects of acupuncture. Which are
clinically significant?. Canadian Family Physician 2003;49:985–89.
Ernst & White 1997
Ernst E, White A. Life-threatening adverse reactions after acupunc-
ture? A systematic review. Pain 1997;71:123–126.
Ernst 2003
Ernst G, Strzyz H, Hagmeister H. Incidence of adverse effects during
acupuncture therapy- a mutlicentre survey. Complementary Therapies
in Medicine 2003;11:93–97.
Gerwin 2001
Gerwin RD. Classification, epidemiology, and natural history of my-
ofascial pain syndrome. Current Pain and Headache Reports 2001;5
(5):412–20.
Lao 1996
Lao L. Acupuncture techniques and devices. J Alternative Comple-
mentary Med 1996;2:23–5.
MacPherson 2001
MacPherson H, Thomas K, Walters S, Fitter M. The York acupunc-
ture safety study: prospective survey of 34 000 treatments by tradi-
tional acupuncturists. BMJ 2001;323(486-7).
MacPherson 2002
MacPherson H, White A, Cummings M, Jobst KA, Rose K, Niemt-
zow RC, STRICTA Group. Standards for Reporting Interventions in
Controlled Trials of Acupuncture: the STRICTA recommendations.
J Altern Complement Med 2002;8(1):85–9.
Melchart 2004
Melchart D, Weidenhammer W, Streng A, Reitmayr S, Hoppe A,
Ernst E, et al.Prospective investigation of adverse effects of acupunc-
ture in 97,733 patients. Arch Intern Med 2004;164:104–5.
Odsberg 2001
Odsberg A, Schill U, Haker E. Acupuncture treatment: side effects
and complications reported by Swedish physiotherapists. Comp Ther
Med 2001;9:17–20.
Pengel 2003
Pengel LHM, Herbert RD, Maher CG, Refshauge KM. Acute low-
back pain: systematic review of its prognosis. BMJ 2003;327(323-
327).
Shekelle 1994
Shekelle PG, Andersson G, Bombardier C, et al.A brief introduction
to the critical reading of the clinical literature. Spine 1994;19:2028S–
31S.
Stux 2003
Stux G, Berman B, Pomeranz B. Basics of acupuncture. 5th Edition.
Berlin Heidelberg: Springer-Verlag, 2003.
Sutton 2000
Sutton AJ, Duval SJ, Tweedie RL, Abrams KR, Jones DR. Empirical
assessment of effect of publication bias on meta-analyses. BMJ 2000
June 10;320(7249):1574–7.
Travel and Simons 83
Travell JG, Simons DG. Myofascial Pain and Dysfunction: The Trigger
Point Manual. Williams & Wilkins, 1983.
van Tulder 1995
van Tulder MW, Koes BW, Bouter LM. A cost-of-illness study of
back pain in the Netherlands. Pain 1995;62:233–40.
15Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

van Tulder 1997
van Tulder MW, Koes BW, Bouter LM. Conservative treatment of
acute and chronic nonspecific low back pain. A systematic review
of randomized controlled trials of the most common interventions.
Spine 1997;22(18):2128–56.
van Tulder 1999 (a)
van Tulder MW, Cherkin D, Berman B, Lao L, Koes BW. Acupunc-
ture for low back pain. Cochrane Database Systematic Reviews 1999,
Issue 2.Art. No.: CD001351. DOI:10.1002/14651858.CD001351.
van Tulder 1999 (b)
van Tulder MW, Cherkin DC, Berman B, Lao L, Koes BW. The
effectiveness of acupuncture in the management of acute and chronic
low back pain. A systematic review within the framework of the
Cochrane Collaboration Back Review Group. Spine 1999;24(11):
1113–23.
van Tulder 2003
van Tulder M, Furlan A, Bombardier C, Bouter L, The Editorial
Board of the Cochrane Collaboration Back Review Group. Updated
method guidelines for systematic reviews in the Cochrane Collabo-
ration Back Review Group. Spine 2003;28(12):1290–9.
Verhagen 1998
Verhagen AP, De Vet HCW, De Bie RA, Kessels AGH, Boers M,
Knipschild PG. Balneotherapy and quality assessment: interobserver
reliability of the Maastricht criteria list and the need for blinded
quality assessment. Clin Epidemiol 1998;51:335–341.
Waddell 1987
Waddell G. A new clinical model for the treatment of low back pain.
Spine 1987;12:632–644.
White 2001
White A, Hayhoe S, Hart A, Ernst E. Adverse events following
acupuncture: prospective survey of 32 000 consultations with doc-
tors and physiotherapists. BMJ 2001;323:485–6.
Yamashita 1999
Yamashita H, Tsukayama H, Tanno Y, Nishijo K. Adverse events in
acupunture and moxibustion treatment: a six-year survey at a national
clinic in Japan. J Altern Complement Med 1999;5(3):229–36.
Yamashita 2000
Yamashita H, Tsukayama H, Hori N, Kimura T, Tanno Y. Incidence
of adverse reactions associated with acupuncture. J Altern Complement
Med 2000;6(4):345–50.
Yamashita 2001
Yamashita H, Tsukayama H, White AR, Tanno Y, Sugishita C, Ernst
E. Systematic review of adverse events following acupuncture: the
Japanese literature. Comp Ther Med 2001;9:98–104.
∗Indicates the major publication for the study
T A B L E S
Characteristics of included studies
Study Araki 2001
Methods -Randomized (draw lots). Used sealed opaque envelopes by the acupuncturist.
-Patients and outcome assessors were blinded.
-Funding: not reported
-Setting: private clinic in Osaka, Japan.
-Informed consent obtained orally from patients.
-Ethics approval: not described
-All patients were followed.
-Analysis: Mean difference between before and after. Repeated measure ANOVA for responses.
Participants 40 patients with acute low-back pain (less than three days) and no sciatica.
Diagnoses: lumbar disc herniation, discopathy and lumbago.
Mean age: 44 years old
28 males and 7 females.
Working status:?
Previous treatments:?
Co-morbidity:?
Interventions 1) The needles were inserted into SI3 (bilaterally) with Teh Chi sensation, in supine position, and then
patients were made to perform back exercise. Needles were left in situ during the back exercise. Insertion
16Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
depth was 2.5 cm with stainless steel needles (50 mm length, 0.20 mm diameter). Acupuncture treatment
was performed once only.
Randomized to this group: 20
Acupuncturists’ experience: three and six years.
2) Sham needling was performed to SI3 (bilaterally) point in supine position. Acupuncturist mimicked
needle insertion: tapped head of needle guide tube and then patients were made to perform back exercise.
Gesture of needling was performed during the back exercise. Sham treatment was performed once only.
Randomized to this group: 20
Outcomes 1) Pain: Visual Analog Scale (VAS) from 0 to 100 mm;
2) Function: Japan Orthopedic Association (JOA) score, ranges from 0 to 14 (higher is better). Used only
the category of restriction of daily activities.
3) Flexion: Finger-to-floor distance
All three outcomes were taken before and immediately after the single session.
Costs: not reported
Complications: not reported
Notes The original study was published in abstract only. We obtained additional information from the authors.
Language: Japanese
For results, see the comparisons:
02.01
02.03
02.04
02.06
02.07
02.08
Conclusion: “There is no difference between the effect of acupuncture and that of sham acupuncture”
Allocation concealment A – Adequate
Study Carlsson (even)
Methods see Carlsson 2001
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Carlsson (morn)
Methods see Carlsson 2001
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
17Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Carlsson 2001
Methods - Randomized by computer generated list. A secretarial assistant who was not involved in the study performed
the assignments.
- Patients and outcome assessors were blinded.
- Funding: One author is supported by Swedish Medical Research Council.
- Setting: Pain clinic (outpatients) in Malmo General Hospital affiliated with University in Sweden.
- Informed consent: yes
- Ethics approval: yes
- Follow-up: 100% at one month, 62% at three months, and 53% at six months.
- Analysis: used “last observation carried forward” for missing values.
Baseline differences in pain (VAS) were resolved by analysing percent changes at follow-ups. However, for
this analysis they used the non-parametric Mann-Whitney test.
There is no information about which test they used to analyse the global assessments. But, when we replicate
the analysis using RevMan, we get different results from the authors if we use relative risks, but not if we use
odds ratios.
For sick leave they used Wilcoxon signed ranks test.
Participants 51 patients with low back pain for six months or longer (mean 9.5 years) without radiation below the knee
and normal neurological examination.
Diagnoses: 39 muscular origin, 11 severe structural changes on X-rays.
Excluded: trauma, systemic disease, pregnancy and history of acupuncture treatment.
Mean age: 50 years
17 males and 33 females.
Working status: 20 on sick leave, 17 retired, 12 full time, one unemployed.
Previous treatments: corsets, nerve blocks, analgesics, TENS, physiotherapy. Two had undergone surgery.
Interventions 1) Manual acupuncture: local points (BL24, BL25, BL26, Ex Jiaji) and distal points (LI11, LI4, BL40, BL57
and BL60). “Teh-Chi” feeling was sought in all instances, mostly at a needle-tip depth of 2 to 3 cm. The
needles were stimulated three times during the 20-minute treatment sessions to restore Teh Chi feelings. The
needles were disposable, stainless steel, with a diameter between 0.3 and 0.32 mm and a length between 30
and 70 mm.
Frequency: once per week for eight weeks; two further treatments were given during the follow-up assessments
period of six months or longer.
Randomized to this group:16
Acupuncturist’ experience: board certified anesthesiologist with more than 10,000 acupuncture treatments.
2) In addition to the needles as in the manual acupuncture group, they performed electrical stimulation of
four needles (one pair per side in the low back). Frequency: 2 Hz every 2.5 seconds, interrupted by a 15 Hz
train for 2.5 seconds.
Randomized to this group: 18
3) Mock transcutaneous electrical nerve stimulation (TENS) given by an impressive, stationary, but dis-
connected GRASS (gradient-recalled acquisition in a steady state) stimulator attached to two large TENS
electrodes. The electrodes were placed on the skin over the most intensely painful area in the low back.
During stimulation, flashing lamps were displayed and visible to the patient. This group was seen once per
week for 8 weeks.
Randomized to this group: 16
Outcomes 1) Pain: Visual Analog Scale (VAS) from 0 to 100 mm; measured in the morning and in the evening. Not
clear how many patients filled all pain diaries everyday.
2) Global assessment by physician. Subjective. Improvement is not defined
3) Present work status: number of people on sick leave.
4) Intake of analgesics recorded daily
18Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
5) Sleep quality recorded daily
Outcomes were taken at 1 month, 3 months and 6 months or longer after the end of the 8 sessions.
The results of these outcomes at baseline are not reported, except for pain which is slightly different between
acupuncture and placebo.
Costs: not reported
Complications: no complications occurred during treatment or follow-up period
Notes Language: English
Publication: full paper
Additional information from authors: no
The authors pooled groups 1 and 2 and compared with group 3.
The results for pain are similar in the morning and evening measurements.
For results, see the comparisons:
06.01
06.02
06.06
06.08
06.09 (other data table)
06.10 (other data table)
08.02
Conclusion: “The authors demonstrated a long-term pain-relieving effect of needle acupuncture compared
with true placebo in some patients with low-back pain”
Allocation concealment A – Adequate
Study Ceccherelli 2002
Methods -Randomized (table of random numbers). No description of allocation concealment.
-Outcome assessors were blinded.
-Funding: AIRAS (Associazone Italiana per la Ricerca e l’Aggiornamento Scientifico)
-Setting: Pain clinic, University of Padova, Italy.
-Informed consent and ethics approval not reported
-All patients were followed
-Analysis: Between groups were initially compared by repeated measurements two-way ANOVA. Post hoc
comparison was done by the Bonferroni correction of the unpaired t-test.
Participants 42 patients with continuous pain for more than 3 months. Normal neurologic exam. No signs of radicular
compression.
Diagnoses: chronic lumbosacral myofascial pain.
Excluded: spinal cord injury, osteoporosis, rheumatic diseases, disk herniation, fibromyalgia, organic diseases,
hypertension or obesity.
Age: between 30-50 years old. Mean 42 years old.
30 males and 12 females
Working status: ?
Previous treatments: none had been treated with acupuncture
Co-morbidity: ?
19Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Interventions 1) Deep acupuncture: 1.5 cm in the muscle or in the trigger point. Needles: disposable Sedatelec 300um
diameter of 3 different lengths: 10 mm, 29 mm and 49 mm. Points: Extra 19, VG6. The following were
inserted bilaterally: GB34, UB54, UB62. Plus four trigger points or as second choice in the four most painful
muscular tender points found in the lumbar area. Total of eight sessions (total 6 weeks), each session lasted
for 20 minutes.
All needles were stimulated for 1 minute immediately after the insertion and for 20 s. every 5 min at 5, 10
and 15 minutes. The frequency of alternate right and left rotation of the needles was 2 Hz.
Randomized to this group: not described
Acupuncturist’s experience: not described
2) Same as described for acupuncture, but the depth of insertion was only 2 mm in the skin.
Randomized to this group: not described
Outcomes 1) Pain: verbally using the McGill Pain Questionnaire. They used the number of words chosen and the pain
rating index. The pain rating index is the sum of numerical values that has been assigned to each word used
to describe the pain.
Measured immediately after the end of the sessions and after 3 months.
Costs: not reported
Complications: not reported
Notes Language: English
Publication: full paper
Additional information from authors: we contacted authors, but no response was received.
For results, see the comparisons:
08.01
Conclusions: “Clinical results show that deep stimulation has a better analgesic effect when compared with
superficial stimulation”
Allocation concealment B – Unclear
Study Cherkin 2001
Methods -Randomized (computer-generated random sequence). A research assistant confirmed eligibility, collected
baseline data and randomized the eligible ones.
-Outcome assessors were blinded.
-Funding: Group Health Cooperative, The Group Health Foundation (Seattle), Wash and the John E. Fetzer
Institute (Kalamazoo) and Agency for Health Care Research and Quality, Rockville.
-Setting. Health Maintenance Organization in Washington State, USA
-Informed consent: yes
-Ethics approval: yes
-Follow-up: 95% at 4 weeks, 95% at 10 weeks and 95% at 52 weeks.
-Analysis: Intention-to-treat. ANCOVA for continous variables and Logistic regression for dichotomous
variables. Adjustments for baseline values: Roland score, baseline symptom bothersomeness scale score, pain
below the knee, more than 90 days of back pain, satisfaction with previous back care, sex and age.
Participants 262 patients who visited a primary care physician for low-back pain who had persistent pain for at least 6
weeks.
Diagnoses: Non-specific low-back pain.
Excluded: sciatica, acupuncture or massage for back pain, back care from a specialist or CAM provider, clotting
disorders or anticoagulant therapy, cardiac pacemakers, systemic or visceral disease, pregnancy, litigation or
compensation, inability to speak English, severe or progressive neurologic deficits, previous lumbar surgery,
20Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
recent vertebral fracture, serious comorbid conditions and bothersomeness of back pain less than 4 (on a 0
to10 scale).
Mean age: 44.9 years old
42% males and 58% females
Working status: 84% employed or self-employed
Treatments being received at the time of entry in the study: medications (68%), massage (16%), acupuncture
(3%), narcotics (10%)
Co-morbidity: see exclusion criteria
Interventions 1) Acupuncture: Traditional Chinese Medical acupuncture by licensed acupuncturists with at least 3 years of
experience; Basic TCM needling techniques, electrical stimulation and manual manipulation of the needles,
indirect moxibustion, infrared heat, cupping, and exercise recommendation.
Proscribed: massage including acupressure, herbs and treatments not considered common TCM (Japanese
meridian therapy). Number and location of needles were left to the provider. They were allowed up to 10
visits over 10 weeks for each patient. All patients were needled and “teh chi” was reported for 89%. Mean of
12 needles (range 5-16) were inserted in each visit. Acupuncturists recommended exercise for about half of
their patients, usually stretching, walking or swimming.
Randomized to this group: 94 (88 received acupuncture as randomized).
2) Massage by a licensed therapist with at least 3 years of experience. Manipulation of soft tissue: Swedish
(71%), movement reeducation (70%), deep-tissue (65%), neuromuscular (45%), and trigger and pressure
point (48%), moist heat or cold (51%). Prohibited: energy techniques (Reiki, therapeutic touch), meridian
therapies (acupressure and shiatsu) and approaches deemed too specialized (craniosacral and Rolfing). Massage
therapists recommended exercise. They were allowed up to 10 visits over 10 weeks per patient.
Randomized to this group: 78 (74 received massage as randomized).
3) Self-care education: high-quality and inexpensive educational material designed for persons with chronic
back pain: a book and 2 professionally produced videotapes.
Randomized to this group: 90
Outcomes 1) Pain: bothersomeness of back pain (0 to10), leg pain (0 to10) or numbness or tingling (0 to10). The
higher score was used.
2) Function: Roland Disability Scale
3) Disability: National Health Interview Survey
4) Utilization: provider visits, X-rays, operations, hospitalizations, medication use, visits to other massage
therapists or acupuncturists
5) Costs
6) Satisfaction
7) SF-12 Mental and Physical Health summary scales
8) Number of days of exercise
Outcomes were measured at baseline, 4, 10 and 52 weeks after randomization
Complications: no serious adverse effects were reported by any study participant
Notes Language: English
Publication: full paper
For results, see the comparisons:
07.01
07.03
07.08
However, the results shown in the table of comparisons are the unadjusted analysis. We based our conclusions
on the authors analyses.
21Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Therefore, the results are presented in the other data table:
07.09
Conclusions: “Massage is an effective short-term treatment for chronic low-back pain, with benefits that
persist for at least one year. Self-care educational materials had little early effect, but by one year were almost
as effective as massage. If acupuncture has a positive effect, it seems to be concentrated during the first four
weeks because there was little improvement thereafter”.
Allocation concealment B – Unclear
Study Cherkin 2001 (mass)
Methods See Cherkin 2001
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Cherkin 2001 (sc)
Methods See Cherkin 2001
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Coan 1980
Methods -Randomization was carried out by having prepared in advance a small box with 50 identically-sized pieces
of paper, folded so that they could not be read. 25 had A and 25 had B written on them. The box was shaken
and one of the pieces of paper was removed from the box blindly.
-Nobody was blinded
-Funding: National Health and Medical Research Council of Australia
-Setting: Acupuncture Center in Maryland, USA
-Informed consent: ?
-Ethics approval:?
-All patients were followed
-Analysis: Adherers (or “per protocol analysis”).
Participants 50 patients recruited via newspapers with low-back pain for at least 6 months.
Diagnoses: Abnormal X-ray (38/43), Sciatica (27/49), Muscle spasm (36/46)
Inclusion criteria: no previous acupuncture treatments, no history of diabetes, infection or cancer, and not
more than 2 back surgeries.
Mean age: 47 years old (range 18 to 67)
23 males and 27 females
Working status:?
Previous treatments: back surgery (4)
Interventions 1) Acupuncture: Classical Oriental meridian theory. Electrical acupuncture in some patients. Selection of
acupuncture loci varied. ’Acknowledged acupuncturists’. 10 or more sessions, approximately 10 weeks. Teh
chi unclear.
22Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Randomized to this group: 25
2) Waiting list, no treatment for 15 weeks. Then they received the same acupuncture treatment as above.
Randomized to this group: 25
Outcomes 1) Pain: Mean pain scores (0=no pain and 10=worst pain)
2) Function: Mean limitation of activity (0=none and 3=severe)
3) Mean pain pills per week
4) Global improvement (improved, same, worse)
Results after 10 weeks in acupuncture and after 15 weeks in waiting list group
Costs: not reported
Complications: not reported
Notes The authors reported a per protocol analysis. However, because there is individual patient data reported in
the article, we were able to recalculate using the intention-to-treat principle.
Language: English
Publication: full paper
Additional information from authors: no
For results, see the comparisons:
05.01
05.02
05.04
05.07
Conclusions: “This study demonstrated that acupuncture was a superior form of treatment for these people
with low-back pain, even though they had the condition for an average of 9 years”.
Allocation concealment A – Adequate
Study Ding 1998
Methods - Randomized (method not described). No mention of concealment of allocation.
-Patients blinded
-Funding: not reported
-Setting: University in GuangZhou, China
-Informed consent: Not reported
-Ethics approval: Not reported
-All patients were followed
-Analysis: chi-squares between groups
Participants 54 patients with chronic low-back pain, frequent recurrence, worse during work and relief with rest.
Diagnosis: chronic low-back pain.
Excluded: specific pathological entities using lab tests and x-rays.
Mean age: 45 years old in the ancient needling technique and 42 in regular needling technique group (range
19-68)
40 males and 14 females
Working status: ?
Previous treatments: ?
Interventions 1) Ancient needling technique “The turtle exploring the holes”. Major points: GV3, Ashi point(s). Supple-
ment points: BL40. Needles 0.38 mm X 75 mm were used for deeper insertion and to different direction
23Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
in 45 degree angle. Strong Teh chi sensation was obtained. The needles were retained for 40 to 50 minutes.
Treatments were given daily up to 10 treatments.
Randomized to this group: 35
2) Regular needling technique. Needles 0.38 mm X 75 mm were used for deeper perpendicular insertion
with twirling or rotating technique was used until strong Teh Chi sensation was acquired. Needle retaining
was 20 minutes with 3 to 4 times twirling or rotating stimulation in between. Treatments were given daily
for up to 10 days.
Randomized to this group: 19
Outcomes 1. Pain on a 4-point scale: “cure”: no pain for 2 months;
“marked effective”: pain markedly improved;
“improved”: pain is somewhat relieved; and “no change”.
Measured immediately after and 2 months after the end of the sessions.
Costs: Not reported
Complications: Not reported
Notes Language: Chinese
Publication: full paper
No additional information from authors
For results, see the other data table:
08.06
Conclusions: “An ancient needling technique is better than the regular needling technique in treating chronic
low back pain”.
Allocation concealment B – Unclear
Study Edelist 1976
Methods - Randomized (method not described). No mention of concealment of allocation.
-Outcome assessors blinded
-Funding: not reported
-Setting: University Hospital in Toronto. Canada
-Informed consent: yes
-Ethics approval: yes
-Not sure if follow-up is complete
-Analysis: not reported
Participants 30 patients with low-back pain with no improvement after conventional therapy, including bed rest, anal-
gesics, heat and physiotherapy. Patients were felt to have disc disease, which could not be surgically improved.
Interventions 1) Acupuncture: Manual insertion of 4 sterile needles into traditional acupuncture points (BL 60 and BL
25 bilaterally) until reaching Teh Chi, then electroacupuncture at 3-10 Hz. 30 minutes, 3 treatments in
maximum 2 weeks. Training & experience of acupuncturists unknown.
Randomized to this group: not reported
2) Sham acupuncture, 4 needles placed in areas devoid of classic acupuncture points, no Teh Chi.
Randomized to this group: not reported
Outcomes 1) Global assessment: subjective improvement of back/leg pain
2) Global assessment: objective improvement as measured by increased range of spinal movement, improve-
ment in tests for nerve root tension and objective improvement in neurological signs.
Costs: not reported
Complications: not reported
24Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Notes Number of patients randomized unknown. We only know that 30 were analysed.
We classified the patients into “chronic low-back pain”.
Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
06.02
06.05
Conclusions: “There seemed to be no difference in either the subjective or objective changes between the
two effects and suggest that much of the improvement in pain syndromes associated with acupuncture may
be on the basis of placebo effect”.
Allocation concealment C – Inadequate
Study Garvey 1989
Methods -Randomized (computer generated four-tier list). No mention of concealment of allocation.
-Patients and outcome assessors blinded. Therapists were blinded for content of injections (groups 2 and 3)
-Funding: not reported
-Setting: Outpatient clinic in a hospital. USA
-Informed consent: not reported
-Ethics approval: not reported
-Follow-up: 51 of 63 randomized (81%)
-Analysis: Adherers and intention-to-treat (with worst case scenario). Continuity chi squared, adjusted test.
Participants 63 patients with acute non radiating low-back pain, normal neurological examination, absence of tension
signs, normal x-ray, persistent pain despite initial treatment of 4 weeks, being able to localize a point of
maximum tenderness (trigger point).
Age: mean 38 years old
Gender: 41 men and 22 women
Working status: not reported
Previous treatment: non-steroidal anti-inflammatory drugs, hot showers, avoidance of activities that aggravate
the pain. No exercise program had been started.
Interventions 1) Dry-needling stick with a 21-gauge needle after an isopropyl alcohol wipe. 1 session. Training & experience
of therapists unknown
Randomized to this group: 20
2) injection with 1.5 ml of 1% lidocaine using a 1.5 inch, 21-gauge needle after an isopropyl alcohol wipe.
Randomized to this group: 13
3) injection with 0.75 ml of 1% lidocaine and 0.75 ml of Aristospan (Triamcinolone Hexacetonide) using a
1.5 inch, 21-gauge needle after an isopropyl alcohol wipe.
Randomized to this group: 14
4) 10-second ethyl chloride spray from 6 inches away, followed by 20 second acupressure using the plastic
needle guard after an isopropyl alcohol wipe.
Randomized to this group: 16
Outcomes 1) global improvement: percentage of not improved or improved.
This outcome was measured at 2 weeks after the interventions.
25Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Costs: Not reported
Complications:
Group 1) 1 case of “fever, chills and systemic upset”; 2 cases of increased pain due to intramuscular hematoma.
Group 3) “increased pain”
Notes Intervention is “dry-needling”
Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
09.01
09.02
Conclusions: “The injected substance apparently is not the critical factor, since direct mechanical stimulus
to the trigger-point seems to give symptomatic relief equal to that of treatment with various types of injected
medication”.
Allocation concealment B – Unclear
Study Garvey 1989 (lidoc)
Methods
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Garvey 1989 (spray)
Methods
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Garvey 1989(steroid)
Methods
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
26Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Giles & Muller 1999
Methods -Randomized (method not described). Person drew an envelope out of a box with 150 well-shuffled envelopes,
each containing one of three colour codes (50 envelopes per intervention)
-Outcome assessor and data analyst blinded
-Funding: Green Projects Donation fund Limited via the Royal Melbourne Institute of Technology and
partly supported by Townsville General Hospital and James Cook University
-Setting: Outpatient pain clinic in a hospital setting. Townsville Australia.
-Informed written consent was obtained.
-Ethical approval by the Northern Regional Health Authority’s Townsville General Hospital
-Follow up: 77 of 130 randomized (59%)
-Analysis: Based on “adherers only principle”, i.e.. discarded those who did not comply with the treatment
assigned. Checked for possible confounders and interactions by multiple regression and logistic regression.
Participants 77 patients with spinal pain for at least 13 weeks (median 6 years).
Diagnoses: 82% lower back pain; 42% neck pain and 34% upper back pain.
Excluded: nerve root involvement, spinal anomalities, pathology other than mild to moderate osteoarthrosis,
previous spinal surgery and leg inequality > 9mm.
Median age: 42 years old
30 males and 47 females
Working status: 56% blue collar, 26% white collar, 13% academic, 5% retired
Previous treatments: 77% drugs, 42% manipulation, 40% physiotherapy and 6% acupuncture
Co-morbidity: not described
Interventions 1) The treating clinician decided which form of acupuncture to use.
One of four experienced medical acupuncturists using sterile HWATO Chinese disposable acupuncture
guide tube needles 50 mm long with a gauge of 0.25 mm for 20 minutes. An average number of 8 to 10
needles were placed in local tender points and in distant acupuncture points according to the “near and far”
technique, depending on the condition being treated. Once patients could satisfactorily tolerate the needles
for 20 minutes, low-volt electrical stimulation was applied to the needles. Six treatments were applied in a 3
to to 4-week.
Randomized to this group: 46
Drop-outs: 26 (52%). Reasons: unrelated to the outcome
2) Spinal manipulation was performed as judged to be safe and appropriate by the treating chiropractor for
the spinal level of involvement only. A high-velocity, low-amplitude spinal manipulation was performed. Six
treatments applied in a 3 to to 4-week period.
Randomized to this group: 49
Drop-outs: 13 (26%). Reasons: same as in the acupuncture group
3) Medication: tenoxican (20 mg/d) and ranitidine (50 mg x 2/ day). Medication was given to the patients
for the defined 3 to 4-week treatment period. Treatment times were standardized by arranging 15 to 20-
minute appointments for all visits to eliminate a potential placebo effect originating from different lengths
of exposure to the clinician
Randomized to this group: 31
Drop-outs: 10 (33%). Reasons: same as in the acupuncture group.
Outcomes 1) Pain: Visual Analog Scale (VAS) from 0 to 10 cm
2) Pain frequency on 5-ordered categories: 1/month, 1/week, 1/day, frequent and constant.
3) Function: Oswestry Disability Index
4) Cross over to another intervention after the study period
All outcomes were measured immediately after the end of the treatment period
27Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Costs: Not reported
Complications: No side effects occurred for acupuncture or manipulation. Three medically treated subjects
had gastric symptoms
Notes The results of this study are not used in this review because of the high drop-out rate in the acupuncture
group (52%) that might invalidate the results of this trial.
Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
07.01
07.03
07.08
Study conclusions: “the manipulation group displayed the most substantial improvements that were uni-
formly found to be significant. In the other intervention groups, not a single significant improvement could
be found in any of the outcome measures”.
Allocation concealment B – Unclear
Study Giles & Muller 2003
Methods -Randomized (method not described). Person drew an envelope out of a box with 150 well-shuffled envelopes,
each containing one of three colour codes (50 envelopes per intervention)
-Data analyst blinded
-Funding: Queensland State Government. Partly supported by Townsville General Hospital.
-Setting: Outpatient pain clinic in a hospital setting. Townsville Australia.
-Informed written consent was obtained.
-Ethical approval by the Northern Regional Health Authority’s Townsville General Hospital
-Follow up: 115 were randomized. Six dropped out before treatment for reasons not related to outcomes.
69/109 (63.3%) were followed.
-Analysis: Based on “intention-to-treat analysis”. Checked for possible confounders and interactions by
multiple regression and logistic regression.
Participants 109 patients with uncomplicated spinal pain for a minimum of 13 weeks (average duration was 6.4 years)
Diagnosis: mechanical spinal pain
Excluded: nerve root involvement, spinal anomalies, pathology other than mild to moderate osteoarthrosis,
spondylolisthesis exceeding grade 1, previous spinal surgery and leg length inequality >9 mm.
Median age: 39 years old
60 males and 49 females
Working status: 29% skilled trade, 20% pensioner or unemployed, 20% manager, clerk or sales, 12%
professional, 18% other.
Previous treatments: not described
Co-morbidity: not described
Interventions 1) The clinician determined the form of acupuncture technique. The Near and Far technique consists of:
needling the trigger point and distal analgesia producing sympatholytic acupuncture points below the elbow
or knee.
Acupuncture was performed by one of two experienced acupuncturists using sterile disposable acupuncture
guide tube needles (length 50 mm, gauge 0.25 mm) during 20-minute appointments.
28Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
For each patient, 8 to 10 needles were placed in local paraspinal intramuscular maximum pain areas and
approximately 5 needles were placed in distal acupuncture point meridians depending on the spinal pain
syndrome being treated. Once patients could tolerate the needles, needle agitation was performed by turning
or “flicking” the needles at approximately 5-minute intervals for 20 minutes. The needles were inserted to a
length of 20 to 50 mm, in the maximum pain area, and up to approximately 5 mm in the distal points.
Two treatments per week up to the defined maximum of 9 weeks of treatment.
Randomized to this group: 36. Two were lost before treatment, 2 during treatment and 10 changed treatment
because of no effect.
2) Spinal manipulation. 20-minute appointment. High-velocity, low-amplitude thrust spinal manipulation
to a joint was performed as judged to be safe and usual treatment by the treating chiropractor for the spinal
level of involvement to mobilize the spinal joints. Two treatments per week up to a maximum of 9 weeks.
Randomized to this group: 36. One was lost before treatment, 1 during treatment and 8 changed treatments
because of “no effect”.
3) A medication could be selected that had not already been tried by a patient randomized into the mediation
arm of the study. The patients normally were given Celecoxib (200 to 400 mg/day) unless it had previously
been tried. The next drug of choice was Rofecoxib (12.5 to 25 mg/day) followed by paracetamol (up to 4
g/day). Doses, left to the sports physician’s discretion, were related particularly to the patient’s weight, with
the severity of symptoms playing a minor role. The treating sports physician also was allocated 20 minutes
for follow-up visits.
Randomized to this group: 43. Three were lost before treatment and 18 changed treatment (11 for “no effect”
and 8 for “side effects”)
Outcomes 1) Pain: Visual Analog Scale (VAS) from 0 to 10 cm
2) Pain frequency on 5-ordered categories: 1/month, 1/week, 1/day, frequent and constant.
3) Function: Oswestry Disability Index
4) Cross over to another intervention after the study period
5) SF-36 Health Survey Questionnaire
All outcomes were measured immediately after the end of the treatment period
Costs: Not reported
Complications: Not reported
Notes Not sure about proportion of patients with lower back pain.
The results might be biased by the high and differential drop out rates.
Results are presented as medians and 25th and 75th percentiles and were transformed to means and standard
deviations.
Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
07.01
07.03
Study results: “Manipulation yielded the best results over all the main outcome measures except the Neck
Disability Index, for which acupuncture achieved a better result than manipulation”. “All three therapies
showed positive response according to the SF-36 general health status questionnaire”
Conclusions: “In patients with chronic spinal pain, manipulation, if not contraindicated, results in greater
short-term improvement than acupuncture or medication”.
Allocation concealment B – Unclear
29Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Giles 1999 (NSAID)
Methods See Giles and Muller 1999
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Giles 1999 (manip)
Methods See Giles and Muller 1999
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Giles 2003 (NSAID)
Methods See Giles and Muller 2003
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Giles 2003 (manip)
Methods See Giles and Muller 2003
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Grant 1999
Methods - Random numbers were used (method not described) to generate a sequence of sealed envelopes containing
the treatment code, the next available envelope being opened on the patient’s entry into the trial.
-Outcome assessors were blinded.
-Funding: Grant from the Trustees of the Liberton Hospital Endowment Funds
-Setting: Outpatients clinic in the United Kingdom
-Informed consent: not reported
-The study was approved by the Lothian Research Ethics Committee
-Follow-up: 57 out of 60 randomized
-Analysis: No intention-to-treat. Mann-Whitney U-tests for between group differences.
Participants 60 patients aged 60 years or over, with a complaint of pain of at least 6 months duration.
Diagnoses: chronic low-back pain.
Excluded: treatment with anticoagulants, systemic corticosteroids, dementia, previous treatments with
acupuncture or TENS, cardiac pacemaker, other severe concomitant disease, inability of patient or therapist
to apply TENS machine.
30Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Mean age: 73.6 years old
6 males and 54 females
Previous treatments: not reported
Interventions 1) Two sessions of manual acupuncture weekly for 4 weeks, i.e. eight sessions in total. The needles were of a
standard size (32 gauge, 1.5 inch length with guide tube). Points were chosen for the individual patient as in
routine clinical practice, only using points in the back. Six needles were used on average at each treatment
with a minimum of two and a maximum of eight. Treatment sessions lasted for 20 minutes.
Randomized to this group: 32. Two dropped out during the study. Reasons: influenza and dental problem.
2) TENS: Standard machine (TPN 200, Physio-Med-Services) using 50 Hz stimulation with the intensity
adjusted to suit the patient, again as a routine clinical practice. The patient was given her/his own machine
to use at home, and instructed to use it during the day as required for up to 30 minutes per session to a
maximum of 6 hours per day. She/he was also seen for 20 minutes, twice weekly, by the physiotherapist,
ensuring the same contact with him. At each visit, symptoms were reviewed, treatment discussed and the
optimum use of the TENS machine ensured.
Randomized to this group: 28. One dropped out due to acute depression.
Co-interventions: The patients were advised to continue existing medication but not to commence any new
analgesics or any additional physical treatments for the duration of the trial.
Outcomes 1) Pain: visual Analog scale (0 to 200 mm).
2) Pain subscale of the 38-item Nottingham Health Profile part 1.
3) Analgesics consumption
4) Spinal flexion
These outcomes were taken at baseline, 4 days and 3 months after last treatment session.
Costs: not reported
Complications: 3 acupuncture patients reported dizziness and 3 TENS patients developed skin reactions.
(Comparison 07.08)
Notes The two groups appear different at baseline with respect to the four outcome measures. Patients in the
acupuncture group have higher VAS and NHP pain scores, reduced spinal flexion and lower tablet consump-
tion compared to the TENS group.
Because the authors had not adjusted for baseline values, no conclusions can be made based on this study.
We could try to obtain raw data from authors and run ANCOVA, but the data is also skewed and transfor-
mation is not appropriate.
Results:
07.01
07.08
Language: English
Publication: full paper
No additional information from authors
Conclusions: “A 4-week course of either acupuncture or TENS had demonstrable benefits on subjective
measures of pain (VAS and NHP score) and allowed them to reduce their consumption of analgesic tablets.
The benefits of both treatments remained significant 3 months after completion, with a trend towards further
improvement in the acupuncture patients.”
Allocation concealment A – Adequate
31Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Gunn 1980
Methods -Randomized (randomized blocks, blocks defined by age and operation status; the first subject from each
block was assigned to the acupuncture treatment.)
-No information about concealment of allocation
-Nobody was blinded
-Funding: Workers’ Compensation board of British Columbia
-Setting: Pain Clinic in Richmond, British Columbia, Canada
-Informed consent: Yes
-Ethics approval: not reported
-Follow-up: 56 (100%) at discharge, 53 (95%) at 12 weeks and 44 (78%) at time of writing.
-Analysis: Analysis of covariance. No intention-to-treat.
Participants 56 males with chronic low-back pain of at least 12 weeks duration, who had 8 weeks of a standard clinic
regimen.
Diagnoses: disc diseases, low-back strain, spondylitis, spondylolisthesis, radiculopathy, low-back contusion,
pseudoarthrosis, disc protrusion, prolapsed disc, lumbar disc syndrome, post-laminectomy syndrome, neu-
ropathy, sciatica, nerve root compression, facet sprain, musculo-ligamentous strain, compression fracture,
interspinous ligament strain,
Excluded: Psychosomatic backache. Females.
Mean age: 40.6 years old (range 20 to 62 years)
Working status: all off work.
Previous treatments: some had surgery.
Interventions 1) Dry-needling: Standard therapy (physiotherapy, remedial exercises, occupational therapy, industrial as-
sessment) plus dry-needling on muscle motor points (non-meridian), 3 to 5 cm needles, direction of the
needle perpendicular to the skin, mechanical stimulation by pecking and twirling, low voltage (9V) electrical
stimulation interrupted direct current or phasic current.
Maximum of 15 treatments (average 8), once or twice a week. Training & experience unknown.
Randomized to this group: 29
2) Standard therapy only (physiotherapy, remedial exercises, occupational therapy, industrial assessment).
Randomized to this group: 27
Outcomes 1) Global improvement:
0: no improvement. Still disabled. Unable to return to any form of employment
+: Some improvement. Some subjective discomfort. Able to return to lighter employment.
++: Good improvement. Slight subjective discomfort but able to return to work and function at pre-accident
employment (or equivalent).
+++: Total improvement. No subjective discomfort. Returned to previous (or equivalent) employment.
The above was measured after discharge, 12 weeks after discharge and at the time of writing of the paper.
(all these varied)
Costs: not reported
Complications: not reported
Notes Intervention is dry-needling.
We dichotomized at 0 versus +/++/+++.
Language: English
Publication: full paper
No additional information from authors
32Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
For results, see the comparisons:
09.01
Conclusion: “The group that had been treated with needling was found to be clearly and significantly better
than the control group with regard to status at discharge, at 12 weeks, and at final follow-up”.
Allocation concealment B – Unclear
Study He 1997
Methods -Randomized (method not reported). No information about concealment of allocation
-Patients were blinded
-Funding: Not reported
-Setting: outpatient clinic in a hospital. University Centre in Sichuan Province, China
-Informed consent: Not reported
-Ethics approval: Not reported
-Follow-up: All 100 patients were followed.
-Analysis: Not reported
Participants 100 patients with low-back pain (5 days to 6 months duration), with limited range of motion, and symptoms
worse in cold and rainy weather.
Excluded: kidney or bone disease confirmed by urine test and X-ray.
Age range: 22 to 79 years old
44 males and 56 females
Working status: not reported
Previous treatments: not reported
Interventions 1) Manual acupuncture with moxibustion plus Chinese herbal medicine. Two groups of points: 1) GV 4,
BL 22 , Ashi-points. 2) BL23, GV 3 and Extra 9 (L3-L4). Moxibustion was used 2 to 3 times on the handle
of the needles and needles were retained for 30 minutes. Treatments were given daily up to 10 treatments.
Teh Chi sensation was obtained. Herbal formula was given daily.
Randomized to this group: 50
Experience: unknown
2) Chinese herbal treatment alone.
Randomized to this group: 50
Outcomes 1) Overall assessment that includes pain, physical function, sensitivity to weather change and return to work.
According to this measure, patients are classified into:
a) cured: no pain, return to normal life and work, remains normal at one-year follow-up;
b) marked effective: pain is generally gone, but still feels uncomfortable in cold and damp weather;
c) improved: pain is markedly relieved, still feels uncomfortable in cold and damp weather, but better than
pre-treatment
d) no changes: no significant change.
The overall assessment was measured one year after the end of the sessions.
Costs: not reported
Complications: not reported
Notes We classified the duration as acute/subacute.
We dichotomized at a/b/c versus d.
Language: Chinese
Publication: full paper
33Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
No additional information from authors
For results, see the comparisons:
03.02
Conclusion: “Manual acupuncture with moxibustion plus Chinese herbal medicine is better (p<0.01) than
Chinese herbal medicine alone for treating low-back pain with cold and dampness, based on TCM diagnosis”.
Allocation concealment B – Unclear
Study Inoue 2000
Methods -Randomized (computer generated numbers). Allocation was done by a centralized office using the Internet.
-Patients and outcome assessors were blinded.
-Funding: Not reported
-Setting: University hospital in Kyoto, Japan.
-Written informed consent was taken from patients
-The Ethics Committee approved this study.
-Follow-up: All 27 patients were followed (100%)
-Analysis: Mann-Whitney’s U test was used for between group analysis.
Participants 27 patients with low back pain of unknown duration who attended the outpatient acupuncture clinic.
Excluded: (1) neurological findings, pain or numbness in lower extremity; (2) malignancy, (3) infection or
inflammatory disease; (4) fracture; (5) lumbago due to urological problem, gynaecological problem, digestive
problem or cardio-vascular problem; (6) patients who cannot stop other conflicting or ongoing treatments;
(7) problem of general condition; (8) dementia; (9) pregnancy.
Mean age: 59.6 years old
Gender: no information
Working status: no information
Previous treatments: no information.
Interventions 1) Real acupuncture: Two needling points were chosen bilaterally from lumbar area (i.e. 4 points in total):
BL52 and extra point (yao-yan: EX-B7). Needles were inserted to a depth of 20 mm, manipulated by sparrow
pecking method for 20 seconds, and then removed. One treatment session was performed.
Randomized to this group: 15
Acupuncturist had more than 10 years of experience.
2) Sham acupuncture: The same two points were chosen. Acupuncturist mimicked needle insertions: tapped
head of needle guide tube, then gesture of needling was performed for 20 seconds. One session.
Randomized to this group: 12
Outcomes 1) Pain: visual analog scale (VAS) at the most restricted action immediately after the single session.
Costs: not reported
Complications: not reported
Notes Language: Japanese
Publication: abstract
We obtained additional information from authors.
For results, see the comparisons:
10.01
Conclusion: “There was no difference between real needling and sham needling”.
Allocation concealment A – Adequate
34Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Inoue 2001
Methods -Randomized (computer generated numbers). Allocation was done by a centralized office using the Internet.
-Patients and outcome assessors were blinded.
-Funding: Not reported
-Setting: University hospital in Kyoto, Japan.
-Written informed consent was obtained.
-The Ethics Committee approved this study.
-Follow-up: All 21 patients were followed (100%)
-Analysis: Mann-Whitney’s U test was used for between group analysis.
Participants 21 patients with low-back pain of unknown duration who attended the outpatient acupuncture clinic were
included.
Excluded: (1) neurological findings, pain or numbness in lower extremity; (2) malignancy, (3) infection or
inflammatory disease; (4) fracture; (5) lumbago due to urological problem, gynaecological problem, digestive
problem or cardio-vascular problem; (6) patients who can not stop other conflicting or ongoing treatments;
(7) problem of general condition; (8) dementia; (9) pregnancy.
Mean age: 55.1 years old
Gender: no information
Working status: no information
Previous treatments: no information.
Interventions 1) Real acupuncture: One needling point was chosen from lumbar area: most painful locus was detected.
Needles were inserted and sparrow-picking technique was performed for 20 seconds. One session.
Randomized to this group: 10
Experience: not reported
2) Sham acupuncture: One needling point was chosen from lumbar area: most painful locus was detected,
same as real acupuncture group. Acupuncturist mimicked needle insertion: tapped head of needle guide tube,
then gesture of needling was performed for 20 seconds. One session.
Randomized to this group: 11
Outcomes 1) Pain: visual analog scale (VAS) at the most restricted action immediately after the single session.
Costs: not reported
Complications: not reported
Notes Language: Japanese
Publication: abstract
We obtained additional information from authors.
For results, see the comparisons:
10.01
Conclusion: “Real needling is superior to sham needling”.
Allocation concealment A – Adequate
35Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Kerr 2003
Methods -Randomized (computer generated numbers). No information about who performed allocation of patients.
-Patients and outcome assessors were blinded
-Funding: Department of Health and Social Services for Northern Ireland
-Setting: outpatient clinic in a hospital
-Signed a consent form and were verbally advised as to the nature of the intervention. Patients were informed
that they would receive one of 2 different forms of treatment being investigated
-Ethics permission was obtained from the University of Ulster’s Research Ethical Committee
-46 of 60 randomized patients (76%) finished the trial period and 40/60 (66.7%) were followed at 6 months.
-Analysis: Only those who completed the study (46/60). T-tests for paired and independent samples.
Participants 60 patients with chronic low-back pain (> 6 months) with or without leg pain and with no neurologic deficits.
Mean duration of pain was 75.8 months.
Excluded: age < 18 years old, pregnancy, underlying systemic disorder, rheumatoid arthritis, osteoarthritis of
the spine or cancer.
Mean age: 41 years old
28 males and 32 females
Working status: not reported
Previous treatments: not reported
Interventions 1) Same set of acupoints for everyone, regardless of the distribution of their symptoms: Bl23, Bl25, GB
30, Bl40, Ki3 (all bilateral) and GV4. Eleven needles were used in each session (Seirin acupuncture needles
N8, 0.30 x 50 mm, c-type needle). The needles were inserted until Teh Chi was produced. Position: prone.
Duration: 30 minutes. Needles were manually rotated to produce Teh Chi initially and at 10 to 20 minute
intervals. Sessions: 6 sessions, over a 6-week period.
Patients were also given a leaflet regarding their low-back pain that included standardized advice and exercises.
A Chartered Physiotherapist trained in acupuncture carried out all treatments.
Randomized to this group: 30
2) Placebo-TENS: Patients were advised that the treatment was relatively novel and that they should not
feel any discomfort with the procedure and, in fact, should not be aware of any sensation at all. They were
advised that the treatment had an effect on the nerve-endings and that it should relieve their symptoms.
Patient lying in the prone position for 30 minutes. A non-functioning TENS machine was attached to 4
electrodes placed over the lumbar spine and the unit was placed in a position to make it difficult to interfere
with the apparatus. The investigator monitored the patient’s condition after 10 and 20 minutes. Sessions: 6
over a 6-week period.
Patients were also given the advice and exercise leaflet and the same principal investigator carried out all
treatments.
Randomized to this group: 30
Outcomes 1) Pain (VAS)
2) SF-36
3) Physical examination: finger-floor distance.
All these outcomes were measured immediately after the end of the 6th session.
4) Global improvement measured at 6 months: ”Did you experience pain relief? “Yes” or “No”. But only 40
(66.7%) patients were followed up to 6 months
Costs: not reported
Complications: In the acupuncture group there were 2/23 patients who reported side effects and 2/17 in the
placebo group.
Notes Language: English
36Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Publication: full paper
No additional information from authors
For results, see the comparisons:
06.01
06.02
06.04
06.07
Conclusions: “Although acupuncture showed highly significant differences in all the outcome measures
between pre and post-treatment, the differences between the two groups were not statistically significant”.
Allocation concealment B – Unclear
Study Kittang 2001
Methods - Randomization in blocks of four patients (method not described). No description of who performed the
allocation of patients
-Outcome assessor was blinded
-Funding: Three governmental, medical association and science council funding sources as well as funding
from two pharmaceutical companies
-Setting: Private clinic in Flora and Kinn, Norway
-Consent not described, ethics approval obtained
-57/60 patients were followed
-Analysis: t-test & Fishers exact test
Participants 60 patients with acute low-back pain (lasting less than 10 days).
Excluded: Neurologic outcomes, rheumatic illness, malign disease, systemic use of anti-inflammatory drugs
or steroids before inclusion and use of medicine that may interact with anti-inflammatory drugs.
Between 18 and 67 years of age
Gender: both sexes
Working status: 2/3 on sick leave at time of inclusion
Interventions 1) First treatment was needling in “lumbago 1 and 3” with medial lumbago, and in “upper lip” with more
lateral pain. Later treatments were 5 needles across at level L2, at “Ashi points” (local pain points) and in both
ankles. Analgesia was allowed and sick leave provided when necessary. Four treatments within two weeks.
Patients in both groups were given general advise and encouraged to daily physical activity.
Randomized to this group: 30
2) Naproxen 500 mg twice daily for ten days
Randomized to this group: 30
Outcomes 1) Pain (VAS) measured at baseline, 1 and 2 weeks and 3 and 6 months
2) Use of other analgesics measured at 1 and 2 weeks
3) Number of back pain episodes at 6 and 18 months
4) Side effects at 1 and 2 weeks
5) Stiffness measured at baseline, 1 and 2 weeks and 3 and 6 months
6) Lateral flexion measured at baseline, 1 and 2 weeks and 3 and 6 months
Costs: not reported
Notes Language: Norwegian
Publication: full paper
Asked authors for additional information: no response.
For results, see the comparisons:
37Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
03.01
03.04
03.06
Conclusions: “No difference in reduction of pain or stiffness over a six-month evaluation”
Allocation concealment B – Unclear
Study Kurosu 1979(a)
Methods -Randomized (method not described). No information about concealment of allocation
-No information about blinding
-Funding: Not reported
-Setting: Private clinic in Tokyo, Japan
-There is no description about informed consent or ethics approval.
-Follow-up: 20 of 20 (100%)
-Analysis: Intention-to-treat, used t-test for between group analyses
Participants 20 patients with lumbar or sacral region pain.
Most of patients were between 40 and 50 years old.
10 males and 10 females
Working status: Not reported
Previous treatments: Not reported
Interventions 1) Acupuncture: the needles were inserted, and left in situ for 10 minutes, and then removed. Insertion depth
was 2 to 4 cm, depending on one’s figure. Acupuncture needles used were stainless steel needles (50 mm
length, 0.25 mm diameter). Six to eight points in lumbar part were chosen from BL23, 24, 25, 26, 27, 31,
52 and 3 extra channel points by palpation. Abdominal needling was added: needles were inserted to a depth
of 1 to 1.5 cm at CV4,13 and ST25 (bilaterally). Acupuncture treatment was performed more than 4 times.
Randomized to this group: 10
Experience: well-known and well-experienced acupuncturist.
2) Garlic moxibustion in lumbar region: Moxa is placed on top of a slice of garlic. Six to eight points in
lumbar area were chosen from BL23, 25, 27, 52 and the other points by palpation.
Randomized to this group: 10
Outcomes 1) Pain: 10-item questionnaire about the specific actions that caused pain. Possible range of this questionnaire
is -10 to 20 (if patient feels pain at all actions) and higher scores are better. It was measured immediately
before second and fourth session
Costs: not reported
Complications: not reported
Notes Language: Japanese
Publication: full paper
No additional information from authors.
For results, see the comparisons:
11.02
Conclusions: “There is no difference between needle retention technique and garlic moxibustion for low-
back pain”.
Allocation concealment B – Unclear
38Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Kurosu 1979(b)
Methods -Randomized (method not described). No information about concealment of allocation
-No information about blinding
-Funding: Not reported
-Setting: Private clinic in Tokyo, Japan
-There is no description about informed consent or ethics approval.
-Follow-up: 20 out of 20 (100%)
-Analysis: Intention-to-treat, used t-test for between group analyses
Participants 20 patients with lumbar or sacral region pain.
Most of patients were between 40 and 50 years old.
11 males and 9 females
Working status: Not reported
Previous treatments: Not reported
Interventions 1) Acupuncture: the needles were left in situ for 10 minutes, and then removed. Depth was 2 to 4 cm,
depending on one’s figure. Stainless steel needles (50 mm length, 0.25 mm diameter). Six to eight points
in lumbar part were chosen from BL23, 24, 25, 26, 27, 31, 52 and 3 extra channel points by palpation;
abdominal needling was added: needles were inserted to a depth of 1 to 1.5 cm at CV4,12 and ST25
(bilaterally). Acupuncture treatment was performed more than 4 times.
Experience: well-known and well-experienced acupuncturist.
Randomized to this group: 10
2) Other acupuncture technique: needles were removed immediately after insertion. Insertion depth was
2 to 4 cm, depending on one’s figure. Stainless steel needles (50 mm length, 0.25 mm diameter). Six to
eight points in lumbar part were chosen from BL23, 24, 25, 26, 27, 31, 52 and 3 extra channel points by
palpation. Abdominal needling was added: needles were inserted to a depth of 1 to 1.5 cm at CV4,12 and
ST25 (bilaterally); needles were left in situ for 10 minutes, and then removed. Acupuncture treatment was
performed 3 times.
Randomized to this group: 10
Outcomes 1) Pain: 10-item questionnaire about the specific actions that caused pain. Possible range of this questionnaire
is -10 to 20 (if patient feels pain at all actions) and higher scores are better. It was measured immediately
after the fourth session
Costs: not reported
Complications: not reported
Notes Language: Japanese
Publication: full paper
No additional information from authors.
For results, see the comparisons:
12.02
Conclusions: “Results of needle retention technique is superior to that of simple insertion technique for low-
back pain”.
Allocation concealment B – Unclear
39Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Lehmann 1986
Methods -Block randomization, blocks defined by prior lumbar surgery (method not reported). No information about
concealment of allocation.
-Therapists were blinded between real TENS and sham TENS, but not between acupuncture and TENS
-Funding: NIHR Grant
-Setting: Multidisciplinary inpatient clinic in a University of Iowa Hospital, USA.
-Informed consent and ethics approval were not reported
-Follow-up: 39 of 54 randomized patients (72%)
-Analysis: Multivariate analysis of covariance (adjustments for baseline scores and for non-organic signs). No
intention-to-treat analysis.
Participants 54 patients screened at orthopaedic clinic with chronic (>3 months) disabling low-back pain.
Excluded: candidates for lumbar surgery, pain less than 3 months, pregnancy, osteomyelitis of the spine,
discitis, tumour, ankylosing spondylitis, vertebral fractures and structural scoliosis.
Diagnoses: chronic disabling (not working) low-back pain. Duration of low-back pain: 48% more than 18
months.
Mean age: 39 years old (ranged from 20 to 59)
Gender: 33% females.
93% married.
Working status: 1/54 was working. 51 were receiving compensation. 33% were involved with litigation.
Previous treatments: some had surgery.
Interventions 1) Electroacupuncture with needles, biphasic wave at 2 to 4 Hz, inner and outer bladder meridian for
paravertebral pain. Gall bladder meridian for lateral (sciatic) pain. LI4 points and additional points were
stimulated according to the patient’s pattern of pain; certified and experienced acupuncturist; twice weekly
for 3 weeks. Teh Chi not reported.
Randomized to this group: 18
2) Real TENS, pulse width of 250/second at 60 Hz, 15 treatments in 3 weeks, sub-threshold intensity, points
of stimulation over the center of pain, experienced physiotherapist.
Randomized to this group: 18
3) Sham TENS, same as TENS but dead battery.
Randomized to this group: 18
Outcomes 1) Peak pain and average pain (VAS)
2) Activities of daily living: 15 items (yes/no)
3) Physician’s perception of improvement
4) Range of motion
All these outcomes were measured at baseline, at discharge and between 3 to 6 months after discharge
5) Return to Work after 6 months (from no disability=10 points, to not able to work at all=0 points);
Costs: not reported
Complications: there were no complications.
Notes Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
06.06
06.08
40Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
06.11 (other data table)
07.07
07.08
07.10 (other data table)
Conclusions: “There were no significant differences between treatment groups with respect to their overall
rehabilitation”. “The electroacupuncture group demonstrated slightly better results than the other groups.”
Allocation concealment B – Unclear
Study Leibing 2002
Methods -Computer-based randomization method.
-Patients and outcome assessors were blinded. (Patients were blinded only between two types of acupuncture)
-Funding: Ministry of Education, Science, Research and Technology, Federal Republic of Germany.
-Setting: Outpatient clinic. Department of Orthopaedics, University Goettingen, Germany
-Informed consent and ethics approval were obtained.
-Follow-up: 150 patients were randomized. 131 initiated treatment. 114 (76%) were followed at the end of
the treatment and 94 (63%) at 9 months.
-Analysis: ANOVA with post-hoc comparisons using Tukey studentized range tests when significant overall
effects observed. No intention-to-treat analysis, but used last observation carried forward from the 131
patients that initiated treatment.
Participants 150 patients with chronic (> 6 months) non-radiating low-back pain.
Excluded: Abnormal neurological status, concomitant severe disease, psychiatric illness, current psychother-
apy, pathological lumbosacral anterior-posterior and lateral X-rays (except for minor degenerative changes),
rheumatic inflammatory disease, planned hospitalization and refusal of participation.
Mean age: 48.1 years old
Gender: 58% female
76% married
Mean BMI: 26.3
Working status: 82% employed
Current treatments: 8.4% surgery. 50% analgesics
Interventions 1) All patients received standardized active physiotherapy of 26 sessions (each 30 minutes) over 12 weeks. It
was performed by trained physiotherapists according to the Bruegger-concept. In addition, 20 sessions (each
30 minutes) by an experienced Taiwanese physician over 12 weeks. In the first 2 weeks, acupuncture was
done 5/week, and in the next 10 weeks, 1/week.
Combined traditional body and ear acupuncture. Twenty fixed body acupoints (9 bilateral, two single points)
and six on the ear (alternately on one ear) were selected according to their function in TCM and were needled
in every patient. No diagnostic procedure was done to determine individual acupoints.
Body points were manually stimulated until Teh Chi and left in place for 30 minutes: GV3, GV4, BL23,
BL25, BL31, BL32, BL40, BL60, GB34, SP6, Yautungdien (extra meridian, at the back of the hand).
Ear points (left in for one week): 38, 51, 52, 54, 55, 95
Randomized to this group: 50, but only 40 initiated treatment. Ten were lost before first session. Reasons:
withdrew consent=3; exclusion criteria appeared prior to treatment=5; relocated=2.
2) No additional treatment. Only active physiotherapy (as described above)
Randomized to this group: 50, but only 46 started treatment. Four were lost before first treatment. Reasons:
withdrew consent=2; exclusion criteria=2.
3) Sham acupuncture plus physiotherapy. Sham acupuncture received 20 sessions (each 30 minutes) of
minimal acupuncture by the same physician over 12 weeks. Sham acupuncture was done following the
41Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
standards of minimal acupuncture. Needles were inserted superficially, 10 to 20 mm distant to the verum-
acupoints, outside the meridians, and were not stimulated (no Teh Chi).
Randomized to this group: 50, but only 45 started treatment. Reasons: withdrew consent=1; exclusion
criteria=4.
Outcomes 1) Pain intensity: 10 cm VAS
2) Pain disability: total score consists of 7 areas of activity (min 0, max 70) O=no disability, and 70=total
disability.
3) Psychological distress: Hospital Anxiety and Depression Scale, 14-item instrument for use in non-psychi-
atric medical patients. Total score (0 to 42) is a measure of psychological distress.
4) Spine flexion, fingertip-to-floor distance (min = 0 cm)
Costs: not reported
Complications: minor, not serious adverse events occurred in three patients in the acupuncture group.
Notes The use of last observation carried forward usually attenuates the differences between groups.
Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
06.01 06.03
06.08 06.12
06.13 06.15
13.01 13.02
13.03 13.05
13.08 13.09
Conclusions: “Acupuncture plus physiotherapy was superior to physiotherapy alone regarding pain inten-
sity, disability and psychological distress at the end of the treatment. Compared to sham acupuncture plus
physiotherapy, acupuncture (plus physiotherapy) reduced psychological distress only. At 9 months, the su-
periority of acupuncture plus physiotherapy compared to physiotherapy alone became less and acupuncture
plus physiotherapy was not different from sham plus physiotherapy”.
Allocation concealment A – Adequate
Study Li & Shang 1997
Methods -Randomized (method not reported).
No mention of concealment of allocation.
-Patients were blinded. Comment: since both groups were given active treatments, all the patients should know
that they were treated by “real” acupuncture. However, they probably couldn’t tell which active treatment
group they were in.
-Funding: not reported
-Setting: Outpatient clinic in a hospital. Hebei Province, China.
-Informed consent and ethics approval were not mentioned
-Follow-up: all 156 patients were followed.
-Analysis: U-test: between groups
Participants 156 patients with low-back pain of varying duration (between 2 days and 8 years)
Diagnoses: not reported
Excluded: not reported
Age between 20 and 71 years old
80 males and 76 females
42Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Working status: not reported
Previous treatments: not reported
Interventions 1) Manual acupuncture plus cupping. Teh Chi sensation was obtained and needles were retained for 20
minutes. Major points: BL23, 40. GV 2, 26, LU5. Supplement points: for coldness and dampness: GV3,
BL31, 34. For blood stasis: BL17, 18. For kidney deficiency: GV4 and KI 3. Treatment was given every other
day (except for acute back pain, which was treated daily) up to 10 treatments.
Randomized to this group: 78
Experience: adequate
2) Manual acupuncture alone. Major points: BL23, 40 and GV2. Supplement points: same as treatment
group.
Randomized to this group: 78
Outcomes 1) Overall assessment (see description in He 1997). Measured immediately after the end of the sessions.
Costs: not reported
Complications: not reported
Notes Language: Chinese
Publication: full paper
No additional information from authors
For results, see the comparisons:
12.07 (other data table)
Conclusions: “Manual acupuncture plus cupping technique is better than manual acupuncture alone for
treating low-back pain”
Allocation concealment B – Unclear
Study Lopacz & Gralewski
Methods - Randomization procedure not described.
- Nobody was blinded.
Participants 34 male patients from a neurology department.
Inclusion criteria: low-back pain for 1 month or more.
Age: mean 42 years old (ranged from 25 to 52).
Interventions 1) Acupuncture: 4 needles close to spine, 10 minutes, 4 treatments, 8 days, plus pharmacotherapy. Teh Chi
unclear. Training & experience of acupuncturists unknown.
Randomized to this group: 18
2) Placebo, suggestion, new Swedish method for pain relief, same 4 points echo-encephalography, 10 minutes,
4 treatments, 8 days, plus pharmacotherapy.
Randomized to this group: 16
Outcomes 1) Global improvement (5-point scale): very good, good, doubtful, unchanged and worsening.
Measured after first treatment and after 4 treatments
Costs: not reported
Complications: not reported
Notes Very short term follow-up only. Small sample size.
Authors dichotomized at very good + good versus others.
We classified the patients as chronic low-back pain.
43Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Language: Polish
Publication: full paper
No additional information from authors
For results, see the comparisons:
06.02
Conclusions: “The therapeutic results were better, both immediately and after a series of acupuncture. The
difference in the results of treatment was statistically significant in the patients with longest duration of pains
(>3 months)”.
Allocation concealment B – Unclear
Study MacDonald 1983
Methods -A stratified random process to divide the sexes as equally as possible between the two groups.
-Patients and observers were blinded.
-Funding: North West Thames Regional Health Authority
-Setting: London
-Informed consent and ethics approval not reported
-Follow-up: not reported
-Analysis: Wilcoxon rank sum test.
Participants 17 patients referred from orthopaedic or rheumatological departments.
Inclusion criteria: chronic LBP for at least one year, no relief from conventional treatments.
Diagnoses: spondylitis, ankylosing spondylitis, degenerative disc lesion, idiopathic, non-articular rheuma-
tism, osteoarthritis, prolapsed intervertebral disc, arachnoiditis, ligamentous strain and Scheuermann’s os-
teochondritis.
Exclusion criteria: not reported
Demographics: not reported. But it says ”the two groups were comparable in terms of age, duration of pain,
mood scores, number of physical signs and severity of pain.
Interventions 1) Superficial needling: subcutaneous (4 mm) 30-gauge needle insertion at trigger points. (Number of trigger
points unknown). 5 to 20 minutes, maximum of 10 treatments in 10 weeks. Electrical impulses 700µs at 2
Hz if manual stimulation failed. Randomized to this group: 8
Experience: unknown
2) Placebo transcutaneous electrical stimulation: electrodes connected to dummy apparatus, maximum 10
treatments in 10 weeks.
Randomized to this group: 9
Outcomes 1) Pain relief:
- worse (-1)
- no change (0)
- minimal improvement (1% to 24%) (1)
- moderate improvement (25% to 49%) (2)
- good (50% to 74%) (3)
- excellent (75% to 99%) (4)
- complete resolution (100%) (5)
2) Pain score reduction
3) Activity pain score reduction
4) Physical signs reduction
5) Severity and pain area reduction
Costs: not reported
44Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Complications: not reported
Notes Intervention is dry-needling.
Very small sample size, number of treatments unknown, and follow-up time unknown.
Language: English
Publication: full paper
No additional information from authors
Results:
1) Pain relief: dry-needling: 77.36, placebo: 30.14 (p<0.01);
2) Pain score: dry-needling: 57.15, placebo 22.71 (p:NS);
3) Activity: dry-needling 52.04, placebo 5.83 (p<0.05);
4) Physical signs: dry-needling: 96.78, placebo: 29.17 (p<0.01);
5) Severity and pain area: dry-needling: 73.75, placebo: 18.89 (p<0.01);
Conclusions: “Needling achieved better responses than the placebo in all five measures. Four of the five inter-
group differences were statistically significant.”
Allocation concealment B – Unclear
Study Mendelson 1983
Methods -Randomized (method not described). Unclear about concealment of allocation. Cross-over study.
-Patients and outcome assessors were blinded.
-Funding: National Health and Medical research Council of Australia.
-Setting: Prince Henry’s and Alfred Hospitals, Melbourne, Australia.
-Informed written consent was obtained. Ethics approval by the Ethics Review Committee.
-Follow-up: 77 of the 95 patients randomized (81%).
-Analysis: T-tests. No intention to treat analysis.
Participants 95 volunteers with chronic low-back pain, no compensation or litigation pending, no overt psychiatric
disease.
Diagnoses: Osteoarthritis, traumatic spondylopathy, disc lesion, sacroiliac joint disorder and backache not
specified.
Mean age: 54 years old
Gender: 37 males and 40 females.
Pain duration: 12 years.
Interventions 1) Traditional Chinese acupuncture by a surgeon trained in Peking; points: B23, 25, 36, 40 and 60. If
sciatica: GB 30, 34 and 39. Average 8 needles, manual stimulation until reaching Teh Chi, 30 minutes with
no further stimulation, twice weekly, 4 weeks.
Randomized to this group: don’t know. 36 completed the study.
2) Sham acupuncture, intradermal injection of 2% lidocaine at non-acupuncture, non-tender sites, then
acupuncture needles superficially into the infiltrated areas for 30 minutes without stimulation, twice weekly,
4 weeks.
Randomized to this group: don’t know. 41 completed the study.
Outcomes 1) Pain (VAS) 100-mm scale.
2) Pain relief
3) McGill Pain Questionnaire
4) Disability (method not described)
Costs: not reported
45Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Complications: not reported
Notes Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
06.01
06.02
Conclusions: “Patients receiving acupuncture had a greater but not significantly different reduction in pain
rating scores compared with those receiving placebo. Similarly, no significant difference was found between
the two groups based on self-assessment of disability”.
Allocation concealment B – Unclear
Study Meng 2003
Methods -Randomized (computer generated random allocation sequence). Serially numbered, sealed, opaque envelopes
-No blinding
-Funding: New York Chapter of the Arthritis Foundation
-Setting: Private surgeries clinics of the Hospital for Special Surgery at the New York Presbyterian Hospital.
USA
-Written informed consent; approval by Institutional Review Board
-Follow-up: 47 of 55 randomized patients (85%)
-Analysis: ANOVA for between group differences. Both intention-to-treat and completers only analysis
Participants 55 patients with chronic nonspecific low back pain (>12 weeks) and older than 60 years.
Excluded: specific cause for low-back pain, prior use of acupuncture, use of corticosteroids, muscle relaxants,
narcotics, anticoagulants.
Mean age: 71 years old
Gender: 22 male and 33 female
Previous treatments: 27 NSAID, 10 analgesics, 1 muscle relaxant and 2 aspirin.
Ethnicity: 47 Caucasian, 5 African-American and 3 Hispanic.
Charlson Comorbidity Index: 1.7 (+/- 2.0)
Interventions 1) Acupuncture plus standard therapy: Acupuncture twice a week for 5 weeks. Total 10 sessions. 30-gauge
needles with electrical stimulation (4 to 6 Hz) with a pulse duration of 0.5 ms. Teh Chi response at all
points were verified. Between 10 and 14 needles were used per session. Needle retention was 20 minutes.
Fixed acupoints: UB23, 24, 25, 28 (bilateral). Du3 and 4. Supplementary acupoints: maximum 4 additional
needles: UB36, 54, 37, 40, GB 30, 31.
Two anaesthetists certified in acupuncture.
Randomized to this group: 31. Received acupuncture: 28. Completed follow-up: 24.
2) Standard therapy: Primary physician for 5-week intervention period: NSAID, aspirin, non-narcotic anal-
gesic. Continue back exercise (physical therapy) or home exercise regimen. Prohibited: narcotics, muscle
relaxants, TENS, epidural steroid injections and trigger point injections.
Randomized to this group: 24. Received standard therapy: 23. Completed follow-up: 23.
Outcomes 1) Back specific functional status (modified Roland Disability Questionnaire)
2) Pain (VAS)
These outcomes were measured at 0, 2, 6 and 9 weeks during the trial period, but we only used the measures
at 6 weeks (at the end of all sessions) and 9 weeks (3 to 4 weeks after the end of the sessions) .
46Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Costs: not reported
Complications: no difference in adverse effects.
Notes Language: English
Publication: full paper
For results, see the comparisons:
13.01
13.02
13.05
13.07
Conclusions: “Our data indicate that acupuncture plus standard therapy does decrease back pain and disability
in older patients compared with standard therapy alone in a clinically and statistically significant manner”
Allocation concealment A – Adequate
Study Molsberger 2002
Methods -Randomized (computer generated) stratified according to pain duration. Central telephone randomization.
-Patients and outcome assessors were blinded.
-Funding: Grant from the German Ministry of Education, Science and Research
-Setting: Inpatients in the Hospital. Dusseldorf, Germany.
-All patients were informed about the trial and written consent was obtained.
-Follow-up: 124 of 186 patients randomized (66%)
-Analysis: Approximate chi-square or exact Fisher test, non-parametric Mann-Whitney-Wilcoxon rank test.
Per protocol analysis (n=174) and intention-to-treat analysis (n=186). Main analysis is adjusted for multiple
testing.
Participants 186 patients with low-back pain lasting longer than 6 weeks, with average pain scores greater than 50 mm
(max 100 mm) during the last week. Aged between 20 and 60 years old, and speak German.
Excluded: sciatica, neurological disorder, disc or spine surgery, bone or joint disorder, previous treatment
with acupuncture, psychiatric illness, pregnancy, regular intake of analgesics, off work longer than 6 months,
no litigation.
Mean age: 50 years old
Gender: 97 males and 89 females.
Mean duration of pain: 9.9 years.
Working status: not reported
Previous treatments: not reported
Interventions 1) Verum acupuncture plus conventional orthopedic therapy. Acupuncture: standard points: BL23, 25, 40
and 60 and GB30 and 34. In addition, up to four points of maximum pain “Ah shi points”, which were often
close but not necessarily identical to BL 54, 31, 32 were needled. Needle insertion ranged from 1 to 10 cm
and needle manipulation was mild to strong. A Teh Chi feeling was always achieved. During the acupuncture
treatment, no additional treatment was administered. All patients received 12 verum acupuncture treatments,
3/week, each lasting for 30 minutes.
Acupuncture was carried out by an experienced medical doctor, who had studied in China (Beijing).
Randomized to this group: 65. Drop-outs during treatment: 7. Lost to follow-up: 11.
2) Sham acupuncture plus conventional orthopedic therapy. Sham acupuncture received 12 sham acupuncture
treatments, 3/week, each lasting 30 minutes. Sham acupuncture was standardized to ten needles applied
superficially (depth of needle insertion was less than 1 cm) at defined non-acupuncture points of the lumbar
region, and five needles on either side of the back.
47Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Randomized to this group: 61. Drop-outs during treatment: 3. Lost to follow-up: 17
3) The conventional orthopedic therapy consisted of: daily physiotherapy, physical exercises, back school,
mud packs, infrared heat therapy. On demand they received 50 mg diclofenac up to three times a day.
Injections or cortisone application of any kind were not allowed.
Randomized to this group: 60. Drop-outs during treatment: 2. Lost to follow-up: 22
Outcomes 1) Pain intensity (VAS) during the last 7 days.
2) At least 50% reduction in pain intensity
3) Effectiveness of treatment: excellent, good, satisfactory and failed. Dichotomized at exc+good versus
satisfactory+failed.
4) Schober and finger-to-floor distance.
All outcomes were taken at the end of the treatment period and 3 months later.
Costs: not reported
Complications: no side effects or complications occurred in any treatment group
Notes Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
06.01
06.02
06.14
13.01
13.04
13.06
Conclusions: “Together with conservative orthopedic standard therapy, acupuncture helps to decrease pain
intensity directly after treatment, and patients’ rating of the acupuncture treatment is significantly better
than that of the standard therapy alone. The therapeutic effect lasts for at least 3 months after the end of
treatment”
Allocation concealment A – Adequate
Study Sakai 1998
Methods -Randomized (method not described). Sealed envelopes.
-Not blinded.
-Funding: Grant from the Foundation for Training and Licensure Examination in Anma-Massage-Acupres-
sure, Acupuncture and Moxibustion.
-Setting: Outpatients in a University Hospital. Tokyo, Japan.
-Informed consent was taken orally. No description of ethics approval.
-Follow-up: no information
-Analysis: No statistical test.
Participants 26 patients with non-specific low-back pain of variable duration
Excluded: (1) osteoarthritis of lumbar spine, osteoporosis, scoliosis, spondylolysis, spondylolisthesis, herni-
ation of lumbar disc, spinal stenosis or fracture; (2) radiculopathy or neuropathy in the lower extremity;
(3) urological problem, gynaecological problem, neurological problem, collagen, diabetes or malignancy; (4)
increase of CRP or ESR; (5) medication of corticosteroid, immunosuppressant agent, NSAID or muscle
relaxant; (6) problem of general condition; (7) dementia; (8) pregnancy; (9) elderly patient; (10) those who
were judged to be inappropriate for the trial by the authors.
Mean age: 51 years old
48Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Gender: 7 males and 19 females
Working status: not reported
Previous treatments: not reported
Interventions 1) Needling points in lumbar area were chosen from BL23, 25, 32, 52 and 2 extra channel points near the
spinous process of L4 and L5, and that in lower extremity were chosen from BL37, 40, 57, ST36, GB34
by palpation. Manual acupuncture technique such as needle retention and sparrow pecking technique were
performed. Electro-acupuncture was applied in some cases. Other details in technique not reported. Patients
were treated twice a week for two weeks, i.e. four sessions in total.
Randomized to this group: 14
Experience: unknown
2) Oral medication, which includes NSAID and/or kampo medicine (Chinese herbs).
Randomized to this group: 12
Outcomes 1) Pain relief (VAS) on average on the pervious day, rated by the patient. Higher values are better.
2) JOA (Japan Orthopaedic Association) Score rated by the physician. Subjective symptoms of back pain
and restriction of daily activities. Maximum 17 points. Higher values are better.
Outcomes were measured Immediately at the end of all sessions.
Costs: not reported
Complications: not reported
Notes This study reports on two distinct trials, but we used only the data from one trial, which was randomized.
The other trial allocated patients using alternation, therefore it was not randomized.
Language: Japanese
Publication: abstract (and unpublished report).
We obtained additional information from authors
For results, see the comparisons:
11.01
11.04
Conclusions: “Results of acupuncture are the same as those of medication for low-back pain”
Allocation concealment B – Unclear
Study Sakai 2001
Methods -Multicentric study.
-An independent controller in central office prepared an allocation table and sealed envelopes. A computer-
generated randomized allocation table was used to make a sequence of sealed opaque envelopes containing
the code of intervention. The assigned envelope was opened by acupuncturist at the patient’s entry into the
trial
-Outcome assessor was blinded.
-Funding: Grant from the Foundation for Training and Licensure Examination in Anma-Massage-Acupres-
sure, Acupuncture and Moxibustion.
-Setting: Outpatients in a University Hospital. Tokyo, Osaka, Kyoto and Tsukuba, Japan.
-Written informed consent was taken from patients. At two of the four centers, judgement of ethics committee
was asked and the committees approved the protocol. The other two centers did not have ethics committees.
-Follow-up: 64 of 68 randomized (94%)
-Analysis: 95%CI and repeated measures ANOVA.
Participants 68 patients with low-back pain (at least 2 weeks) and age 20 years or older.
49Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Diagnoses: lumbago (22), lumbar spondylosis (15), discopathy (9), acute low-back pain (3), spondylolysis
(3) , spondylolisthesis (1), sacroiliitis (1) and unclassified (10).
Excluded: (1) neurological findings, pain or numbness in lower extremity; (2) malignancy, (3) infection or
inflammatory disease; (4) fracture; (5) lumbago due to urological problem, gynaecological problem, digestive
problem or cardio-vascular problem; (6) patients who can not stop other conflicting or ongoing treatments;
(7) problem of general condition; (8) dementia; (9) pregnancy; (10) other patients who were judged to be
inappropriate for participating in the trial.
Mean age: 37 years old
Gender: 35 females and 29 males.
Working status: not reported
Previous treatments: not reported
Interventions 1) Needling points were chosen by palpation from the part of quadratus lumborum (around BL52) and/or
erector spinae (around BL23 and BL26) in the lumbar area. Two points were used bilaterally - in total four
points - for each treatment. Patients were treated twice a week for two weeks.
Two types of disposable stainless steel needles were used according to patient’s stature and fat: 0.20 mm in
diameter and 50 mm in length, and 0.24 mm in diameter and 60 mm in length. Needles were inserted into
the muscles. Electro-stimulation at frequency of 1 Hz was applied for 15 minutes. The intensity was adjusted
to make muscle contraction without pain.
Randomized to this group: 32. Drop-outs during treatment: 1. Lost to follow-up: 0
Experience: unknown
2) TENS: Same points as above. Two points were used bilaterally - in total four points - for each treatment.
Patients were treated twice a week for two weeks, i.e. four sessions in total.
Gel type disposable electrodes of 20 x 30 mm in size were used. Stimulation with the frequency of 1 Hz was
applied for 15 minutes
Randomized to this group: 36. Drop-outs during treatment: 2. Lost to follow-up: 1
Outcomes 1) JOA (Japan Orthopaedic Association) Score rated by the physician. Subjective symptoms of back pain
and restriction of daily activities. Maximum 20 points. Higher values are better.
2) Pain relief (VAS) on average on the pervious day, rated by the patient. Higher values are better.
These outcomes were taken after the end of the 4 sessions.
Costs: not reported
Complications: no adverse event was reported in the electroacupuncture group. In the TENS group: 1 itching
and 1 dullness after session.
Notes Duration of low-back pain mixed.
Language: English and Japanese
Publication: full paper
We obtained additional information from the authors.
For results, see the comparisons:
11.01
11.03
11.04
11.07
Conclusions: “There was no significant difference between groups in any parameter”
Allocation concealment A – Adequate
50Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Takeda & Nabeta 2001
Methods -Randomized (using draws). Stratified by pain duration and gender. Using sealed and numbered envelopes,
but the person doing the randomization was not independent.
-Patients blinded.
-Funding: no funding was received.
-Setting: Acupuncture College in Osaka, Japan.
-Informed consent was obtained from participants and there was no description of ethics approval.
-Follow-up: 18 of 20 patients randomized (90%)
-Analysis: Mann-Whitney U test for between group differences. No intention-to-treat analysis.
Participants 20 students of acupuncture college who were suffering from lumbago.
Excluded: sciatica
Duration of pain: Mean 40.4 months in distal group and 81.0 months in local group.
Mean age: 26.4 years old in distal group and 35.8 years in local group.
Gender: 17 males and 3 females
Working status: all students.
Previous treatments: not described
Interventions 1) Distal point technique: At the acupuncture points in lumber area: BL23, 26 and Yao-yan (extra-point: EX-
B7), acupuncturist mimicked needle insertion: tapped head of needle guide tube, then gesture of needling
was performed. Acupuncture points in lower extremity: BL37, 40 and 58, were needled by real acupuncture
needle (40 mm in length and 0.2 mm in diameter). Insertion depth was 1 to 2 cm. Sparrow-picking technique
was performed 5 times, then needles were removed. Participants were treated once a week for 3 weeks.
Experience: unknown
Randomized to this group: 10. Drop-outs during study: 1.
2) Local points technique: Acupuncture points in lumber area: BL23, 26 and Yo-gan (extra-point: EX-B7),
were needled by real acupuncture needle (40 mm in length and 0.2 mm in diameter). Insertion depth was 1
to 2 cm. Sparrow-picking technique was performed 5 times, then needles were removed. At the acupoints in
lower extremity: BL37, 40 and 58, acupuncturist mimicked needle insertion: tapped head of needle guide
tube, then gesture of needling was performed. Participants were treated once a week for 3 weeks.
Experience: unknown
Randomized to this group: 10. Drop-out during treatment: 1.
Outcomes 1) Pain (VAS)
2) Function: activity of daily living score. 8 questions about difficulty of specific actions. Maximum 16 points.
Higher values are better.
3) Finger-to-floor distance.
All these outcomes were measured immediately before and after the treatment.
Costs: not reported
Complications: not reported
Notes Language: Japanese
Publication: abstract only
We obtained additional information from authors.
For results, see the comparisons:
12.01
12.04
12.05
51Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Conclusions: “There is no difference between the effects of lumbar area needling and that of distal point
needling”
Allocation concealment B – Unclear
Study Thomas & Lundberg 94
Methods - Randomized (method not described). No description of concealment of allocation.
- Outcome assessors were independent and not involved in the treatment.
- Funding: Karolinksa Institute Foundation, King Gustav Vth 80 year anniversary Fund, Tore Nilssons
Foundation for Medical Research, Torsten and Ragnar Soderbergs Foundation and The Swedish Medical
Research Council.
- Setting: Outpatient clinic at the Karolinska Hospital. Stockholm, Sweden.
- Oral informed consent was obtained. No description of ethics approval:
- Follow-up: 40 of 43 randomized patients (93%)
- Analysis: Student t-test for independent samples and multiple comparisons ANOVA. No intention-to-treat
analysis.
Participants 43 patients from 2 clinics with nociceptive LBP for 6 months or more, restriction of trunk or hip movement
due to pain, restriction of ADL, muscle spasm.
Excluded: previous surgery, claudication, depression, neurosis, clinical examination not nociceptive.
Diagnoses: Osteoarthritis, sacroiliac joint, sciatica, intervertebral disc degeneration, disc prolapse, lumbar
strain, osteoporosis
Demographics and patients characteristics: not reported, but they say there were no significant differences
between the groups.
Interventions 1) Acupuncture: three different modes of acupuncture: a) manual stimulation, b) low frequency (2 Hz) and
c) high frequency (80 Hz) electrical stimulation of needles. Six local points (3 pairs of paraspinal points: UB
23, 25, 26 or 32) and 3 to 4 distal points (SI 6, UB40 or 60, GB 30 or 34 or St36). Insertion 1 to 5 cm,
rotation producing Teh Chi, 10 sessions of 30 minutes; 2 registered physiotherapists trained in acupuncture.
Randomized to this group: 33
2) Waiting list controls, no treatment.
Randomized to this group: 10
Outcomes 1) Pain: number of words from chart of 83 words describing pain intensity
2) Global improvement: 3-point scale (improved, no change, worse)
3) Functional status: VAS on 12 ADL . Results are presented as number of activities that cause less than 50%
pain.
4) Mobility: goniometry of the lumbar spine
Outcomes were measured after 6 weeks and 6 months.
Costs: not reported
Complications: not reported
Notes Randomization only for comparison acupuncture versus WLC, not for different modes of acupuncture.
Language: English
Publication: full paper
No additional information from authors
Results see comparisons:
05.01
05.03
05.07
52Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
The results for global improvement could not be entered in the graphs.
The authors found significant differences for pain outcomes, however, when we entered this data in RevMan
(comparison 05.01) this was not significant. Because we did this based on the data extracted from the figure,
we decided to follow the author’s conclusions.
Functional outcomes had to be transformed to effect sizes (comparison 05.07 to be combined with another
trial)
Conclusions: “After 6 weeks, patients receiving acupuncture were statistically significantly better than the
control group on measures of pain, global improvement and mobility. The same results were observed at 6
months, but only for the group that received low frequency electroacupuncture”.
Allocation concealment B – Unclear
Study Tsukayama 2002
Methods -Randomized. Computer-generated random number were used to make a sequence of sealed envelopes. An
independent person prepared an allocation table and sealed envelopes.
-Outcome assessors were blinded.
-Funding: Grant from the Foundation for Training and Licensure Examination in Anma-Massage-Acupres-
sure, Acupuncture and Moxibustion” and the Tsukuba College of Technology.
-Setting: Private clinic in Tsukuba, Japan.
-The study was approved by the Ethics Committee of TCT Clinic. Informed consent was taken from patients
according to the ICH/GCP.
-Follow-up: 19 of 20 patients (95%)
-Analysis: Repeated measures ANOVA. No intention-to-treat analysis.
Participants 20 patients with low-back pain of at least 2 weeks and over 20 years old.
Excluded: radiculopathy or neuropathy, fracture, tumour, infection or internal disease, other general heath
problem and conflicting or ongoing treatments.
Duration of low back pain: acupuncture group=2900 days (+/- 1983) and TENS group=3120 days (+/-
3306).
Mean age: 45 years old
Gender: 3 males and 16 females.
Working status: not described
Previous treatments: acupuncture (4)
Interventions 1) Acupuncture: Points selected by tenderness and palpable muscle bands detected on the lower back and
the buttock. Four points bilaterally (8 in total) were used for each treatment. Points most frequently used
were BL23 and BL26. Two types of disposable stainless steel needles were used, depending on stature and
fat: 0.20 mm in diameter and 50 mm in length and 0.24 mm in diameter and 60 mm in length. Needles
were inserted into the muscles. The average insertion depth was approximately 20 mm. Electrostimulation
was applied to the inserted needles with an electronic stimulator with a frequency of 1 Hz for 15 minutes.
Press tack needles were inserted after EA at four of the 8 chosen points and left in situ for several days, they
are 1.3 mm long projecting from the sticky side of a small round adhesive dressing.
Patients were treated twice a week for 2 weeks, for 4 sessions in total.
Randomized to this group: 10. Drop-outs: 1
Experience: unknown
2) TENS: Gel type disposable electrodes of 20x30 mm were used for 8 points. Electro-stimulation was
applied in the same manner as in the acupuncture group. The intensity was adjusted to the maximum
comfortable level, and muscle contraction was observed. After each session, a poultice containing methyl
salicylic acid, menthol and antihistamine was prescribed to be applied to the low-back region, at home, in-
between treatments.
53Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Patients were treated twice a week for two weeks, in total 4 sessions.
Randomized to this group: 10. No drop-outs.
Outcomes 1) Pain (VAS): average pain level on the previous day.
2) JOA score. See description in Sakai 2001
These outcomes were measured 3 days after the last session.
Costs: not reported
Complications: no adverse events reported by the evaluator. The therapists reported transient aggravation of
symptoms in the acupuncture group (1), discomfort due to tack needles (1), pain on needle insertion (1)
and small subcutaneous bleeding (1). In the TENS group: transient aggravation (1), transient fatigue (1) and
itching (1).
Notes Language: English
Publication: full paper
For results, see the comparisons:
07.09 (other data table)
07.11
07.08
Conclusions: “The results of the present trial showed a significant between-group difference in pain relief in
favour of acupuncture”
Allocation concealment D – Not used
Study Von Mencke 1988
Methods -Randomization procedure not described.
-Patient and outcome assessors blinded.
-Setting: Secondary care.
Participants 65 patients from an orthopedic clinic with lumbago and/or ischias, no relief after conventional treatment.
Diagnoses: Lombociatalgia (30), low-back pain (20), LWS Syndrome (10) and Ischialgia (5).
Exclusion criteria: neurological problems, scoliosis, concurrent treatment, acute disc prolapse or protrusion,
chronic degenerative disorders, infection.
Age and gender: not described.
Heterogeneous population regarding type, location and duration of disorder.
Interventions 1) Manual acupuncture, traditional meridian acupuncture or trigger points, rotation, insertion 0.2 to 3 cm,
6 to 12 needles 5 to 20 minutes, 8 treatments. Training & experience of acupuncturists unknown.
Points:
- Posterior: GV20, BL26, 31,33, 35, 48, 50, 54, 57, 58, 60.
- Lateral: GV20, GB 26, 28, 30, 32, 34, 37, 38, 40. BL 26, 31, 33, 48, 60
- Anterior: GV 20, ST 36, 40. BL 31, 33, 48, 60.
Randomized to this group: 35
2) Sham acupuncture, no traditional acupuncture nor trigger points.
Randomized to this group: 30
Outcomes 1) Pain (VAS)
2) Global improvement
3) Schober’s test
4) Lasegue’s test
Notes Language: German
54Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Publication: full paper
No additional information from authors
Results:
1) Improvement in pain at short-term follow-up: acupuncture=55%; sham acupuncture=37%. Long-term:
44% versus 30%.
2) Global improvement: acupuncture=94%, sham acupuncture=50% (Table 10.02).
3) Increase in Shober test: short-term: acupuncture=6.4, sham acupuncture=2.7. Long-term: 7.8 versus -0.9
4) Lasegue: short-term: acupuncture=6.0, sham acupuncture=2.2. Long-term, acupuncture=6.7, sham
acupuncture=0.6
Conclusions: “The difference in improvement between typically and atypically treated patients was highly
significant (p<0.0001).”
Allocation concealment B – Unclear
Study Wang 1996
Methods -Randomized (method not reported). No description of concealment of allocation.
-Patients were blinded.
-Funding: not reported
-Setting: Not reported. Vanuatu, Southwest Pacific Ocean.
-Informed consent and ethics approval: Not mentioned
-Follow-up: not described but it seems 100%.
-Analysis: U-test. No intention-to-treat analysis
Participants 492 patients with low-back pain of unknown duration.
Diagnoses: back pain
Exclusion criteria not reported.
Mean age: 48% were older than 40 years old.
Gender: 231 males and 261 females.
Working status: not reported
Previous treatments: not reported
Interventions 1) Local treatment plus cupping. Teh Chi sensation was obtained and needles were retained for 20 minutes.
Points: BL23, 25 and 32. Treatments were given daily up to 10 treatments.
Randomized to this group: 246
Experience: unknown
2) Distal treatment plus electrical stimulation. Points: ST36, GB 39, BL60 and LI4.
Randomized to this group: 246
Experience: unknown
Outcomes 1) Overall assessment: a) cure: no pain and normal range of motion, no tenderness upon palpation, and
normal life and work status. b) effective: pain is markedly improved, normal lumbar movement, no obvious
tenderness upon palpation, and life and work is not affected c) no significant change.
Measured 3 months after the sessions.
Costs: not reported
Complications: not reported
Notes The authors dichotomized at : Cure+effective versus no change.
Language: Chinese
Publication: full paper
55Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
No additional information from authors
For results, see the comparisons:
12.03
Conclusions: “Local acupuncture treatment plus cupping is more effective (p<0.05) than the distal treatment
plus electrical stimulation.”
Allocation concealment B – Unclear
Study Wu (a) 1991
Methods -Randomized (based on odd or even number of the date of patient admission). No mention of concealment
of allocation
-Patients were blinded.
-Funding: Not reported
-Setting: Outpatients in a hospital. Morocco.
-Informed consent and ethics approval not mentioned.
-Follow-up: 100% (single session of acupuncture)
-Analysis: Not reported
Participants 150 patients with acute low-back pain.
Exclusion criteria not described
Age between 20 and 55 years old
Gender: 105 males and 45 females
Working status: not described
Previous treatments: not described
Interventions 1) SI3 point treatment
Randomized to this group: 75
2) Extra 29 (EX-UE7) treatment
Randomized to this group: 75
Manual acupuncture technique (no electro-stimulation) was used. Strong Teh Chi sensation was obtained
combined with lumbar spine movement until symptom relieved. No mention of the duration of the treatment.
Outcomes 1) Global assessment (pain and range of motion).
- cure: no pain and normal range of motion
- marked effective: pain is generally gone and ROM marked improved
- effective: pain is relieved and ROM is somewhat improved.
- no change
Costs: not reported
Complications: not reported
Notes The authors dichotomized at:
a) cure+marked effective+effective versus no change
and
b) cure+marked effective versus effective+no change
Language: Chinese
Publication: full paper
No additional information from authors
For results, see the comparisons:
56Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Dichotomization a) 04.02
Dichotomization b) 04.02
Conclusions: “Acupuncture point SI 3 is more effective than the point Yaotongxue.”
Allocation concealment B – Unclear
Study Wu (b) 1991
Methods See Wu (a) 1991
Participants
Interventions
Outcomes
Notes
Allocation concealment D – Not used
Study Yeung 2003
Methods -Randomized in blocks (method not described). Randomization was blinded.
-Outcome assessors blinded.
-Funding: The Hong Kong Development Fund and Tung Wah Board Fund
-Setting: Outpatient clinic in a hospital. Hong Kong.
-The aims and procedures of the study were explained before written consent was obtained.
Ethical approval from the Ethics Committee of the Hong Kong Hospital Authority and the Human Subject
Ethics Subcommittee of the Hong Kong Polytechnic University was obtained prior to the start of the study.
-Follow-up: 49 of 52 patients randomized (94%)
-Analysis: 2-factor mixed repeated measures ANOVA. Intention-to-treat analysis. Dropping patients for
reasons other than the treatment were given baseline values. Dropping patients for reasons related to the
treatments were given worst score.
Participants 52 patients with chronic low-back pain (>6 months) with or without radiation. Age between 18 and 75 years.
Diagnoses: non-specific low-back pain.
Excluded: 1. Structural deformity (ankylosing spondylitis, scoliosis) 2. Lower limb fracture 3. Tumours 4.
Spinal infection 5. Cauda equina syndrome 6. Pregnancy 7. Spinal cord compression 8. Subjects who were
unable to keep the appointments 9. Receiving acupuncture treatment within the past 6 months 10. Receiving
physiotherapy treatment within the past 3 months
Mean age: 53 years old
Gender: 9 males and 43 females
Working status: not described
Previous treatments: tui na, massage, chiropractor, bone setter or corset.
Interventions 1) Electro-acupuncture: 3/week for 4 weeks by a physiotherapist certificated in acupuncture. Points were
chosen according to the literature: BL23, BL25, BL40 and SP6. Acupuncture was applied to the side on
which patients reported pain. If the reported pain was bilateral, EA was applied to the more painful side.
Sterilised disposable needles, number 30 (0.3 mm) 40-mm long needles were inserted and manipulated until
Teh Chi was obtained. Electrical stimulation on needles at a frequency of 2 Hz for 30 minutes. The intensity
of the stimulation was set at the level that the patient could tolerate and often with evoked visible muscle
contractions. The current had biphasic waveform to the four selected acupoints in two pairs. In addition, all
patients also received exercise therapy, the same as in the control group.
Randomized to this group: 26. Lost to follow-up: 1
2) Standard group exercise program led by the same physiotherapist.
57Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

The program consisted of an hourly session each week for 4 consecutive weeks, and comprised back strength-
ening and stretching exercises
In addition, patients were advised on spinal anatomy and body mechanics, back care and postural correction,
lifting and ergonomic advice, and behavioural modification, as well as a series of home exercises (15 min/day).
Randomized to this group: 26. Lost to follow-up: 2
Outcomes 1) Pain: Numerical rating scale for “average” and for “worst” pain intensity during the last week, by asking
the patient to rate perceived level of pain on a scale from 0 to 10, where 0 represents no pain and 10 represents
pain as bad as it could be.
2) Disability: The Aberdeen LBP scale (19-item) was used to measure low-back pain disability, because it is
the only LBP-specific functional disability scale validated for Chinese subjects. Responses to the questions
were summed and converted to a score percentage between 0 and 100, with 0 representing the least disabled
and 100 the most severely disabled.
These outcomes were measured immediately after, 1 month and 3 months after.
Costs: not reported
Complications: no adverse reaction or complication.
Notes Language: English
Publication: full paper
No additional information from authors
For results, see the comparisons:
13.01
13.07
13.09
Conclusions: “Significantly better scores in the NRS and Aberdeen LBP scale were found in the exercise plus
EA group immediately after treatment, at 1-month follow-up and at 3-month follow-up”
Allocation concealment B – Unclear
Key:
CAM = complementary and alternative medicine
ADL = activities of daily living
WLC = waiting list control
Characteristics of excluded studies
Study Reason for exclusion
Cai 1996 Sciatica
Duplan 1983 Acute sciatica of disc origin.
Fox and Melzack 1976 Not randomized
Franke 2000 Acupuncture treatment did not involve needling.
Fujinuki 1989 Lumbar spinal canal stenosis
Galacchi 1981 Percentage of low-back pain unknown
Gallacchi 1983 Percentage of low-back pain unknown
Ghia 1976 Specific causes of low-back pain
Hackett 1988 Acupuncture treatment did not involve needling.
Ishimaru 1993 Not randomized
Junnila 1982 No back pain
58Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
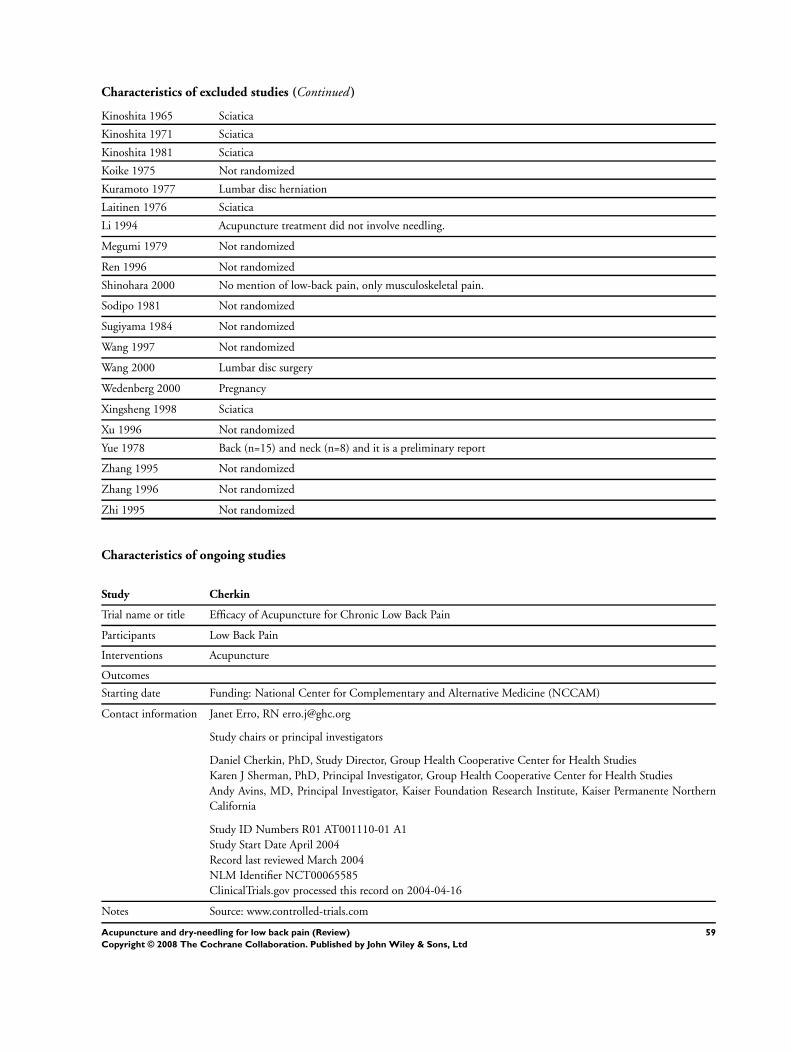
Characteristics of excluded studies (Continued )
Kinoshita 1965 Sciatica
Kinoshita 1971 Sciatica
Kinoshita 1981 Sciatica
Koike 1975 Not randomized
Kuramoto 1977 Lumbar disc herniation
Laitinen 1976 Sciatica
Li 1994 Acupuncture treatment did not involve needling.
Megumi 1979 Not randomized
Ren 1996 Not randomized
Shinohara 2000 No mention of low-back pain, only musculoskeletal pain.
Sodipo 1981 Not randomized
Sugiyama 1984 Not randomized
Wang 1997 Not randomized
Wang 2000 Lumbar disc surgery
Wedenberg 2000 Pregnancy
Xingsheng 1998 Sciatica
Xu 1996 Not randomized
Yue 1978 Back (n=15) and neck (n=8) and it is a preliminary report
Zhang 1995 Not randomized
Zhang 1996 Not randomized
Zhi 1995 Not randomized
Characteristics of ongoing studies
Study Cherkin
Trial name or title Efficacy of Acupuncture for Chronic Low Back Pain
Participants Low Back Pain
Interventions Acupuncture
Outcomes
Starting date Funding: National Center for Complementary and Alternative Medicine (NCCAM)
Contact information Janet Erro, RN [email protected]
Study chairs or principal investigators
Daniel Cherkin, PhD, Study Director, Group Health Cooperative Center for Health Studies
Karen J Sherman, PhD, Principal Investigator, Group Health Cooperative Center for Health Studies
Andy Avins, MD, Principal Investigator, Kaiser Foundation Research Institute, Kaiser Permanente Northern
California
Study ID Numbers R01 AT001110-01 A1
Study Start Date April 2004
Record last reviewed March 2004
NLM Identifier NCT00065585
ClinicalTrials.gov processed this record on 2004-04-16
Notes Source: www.controlled-trials.com
59Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of ongoing studies (Continued )
This is a 4-arm multi-site randomized controlled trial to clarify the extent to which various types of acupuncture
needling can diminish the effect of chronic low back pain on patient functioning and symptoms. Reviews have
noted the poor quality of research in this area and urged that scientifically rigorous studies be conducted. Recent
higher quality trials suggest acupuncture is a promising treatment for back pain. This study directly addresses
methodological shortcomings that have plagued previous studies. A total of 640 subjects (160 per arm) with
low back pain lasting at least 3 months will be recruited from group model HMOs in Seattle, WA and Oakland,
CA. They will be randomized to one of three different methods of stimulation of acupuncture or to continue
usual medical care. Ten treatments will be provided over 7 weeks. The primary outcomes, dysfunction and
bothersomeness of low back pain, will be measured at baseline, and after 8, 26, and 52 weeks by telephone
interviewers masked to treatment. Analysis of covariance within an intention-to-treat context will be used to
analyze the data. Because chronic back pain is a major public health problem and the top reason patients seek
acupuncture treatment, a clear, unambiguous assessment is critical for making informed decisions about whether
acupuncture should be included as part of conventional care for back pain or covered by insurance. Results of
this study will provide the clearest evidence to date about the value of acupuncture needling as a treatment for
chronic low back pain.
Study GerAc
Trial name or title German Acupuncture Trials
Participants
Interventions
Outcomes
Starting date
Contact information http://www.gerac.de/index1.html
Notes
Study Harvard Med School
Trial name or title Physical CAM Therapies for Chronic Low Back Pain
Participants Chronic Low Back Pain
Interventions Procedure: massage therapy
Procedure: chiropractic
Procedure: acupuncture
Outcomes Study Design: Treatment, Randomized, Open Label, Active Control, Parallel Assignment
Starting date Funding: NIH
Contact information Expected Total Enrollment: 120
Location Information
Massachusetts
Harvard Vanguard Medical Associates, Boston, Massachusetts, 00000, United States
Harvard medical school, Boston, Massachusetts, 00000, United States
More Information
Study ID Numbers 1 R01 AT00622-01; EisenbergD
Study Start Date April 2002; Estimated Completion Date December 2002
Record last reviewed August 2003
NLM Identifier NCT00065975
ClinicalTrials.gov processed this record on 2004-04-16
Notes Source: www.controlled-trials.com
This study compares two approaches to the management of acute low back pain: usual care (standard benefit)
vs. the choice of: usual care, chiropractic, acupuncture or massage therapy (expanded benefit). 480 subjects with
uncomplicated, acute low back pain will be recruited from a health maintenance organization, and randomized
60Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of ongoing studies (Continued )
to either usual care (n=160) or choice of expanded benefits (n=320). Patients’ preferences for individual therapies
and expectations of improvement will be measured at baseline and throughout the study. Subjects randomized
to the expanded benefits arm who choose chiropractic, acupuncture or massage will receive up to 10 treatments
over a five-week period. Additional treatments will be available after the fifth week but will require a copayment.
Treatments will be provided by licensed providers who have met strict credentialing criteria. Chiropractic,
acupuncture or massage treatments will begin within 48 hours. Chiropractic, acupuncture and massage therapy
scope of practice guidelines for the treatment of acute low back pain have been developed as have detailed
data tracking procedures to be used at each patient visit. Symptom relief, functional status, restricted activity
days, use of health care, and patient and provider satisfaction will be assessed at 2, 5,12, 26 and 52 weeks
after initiation of treatment. Primary outcomes will include: 1) change in symptoms; 2) change in functional
status; 3) patient satisfaction; and 4) total utilization of services associated with care for low back pain. Medical
records and the HMO’s cost management information system will identify use of services. It is hypothesized
that patients offered their choice of expanded benefits will experience a more rapid improvement in symptoms,
a faster return to baseline functional status, a decrease in utilization of conventional medical services, and will
be more satisfied with their care. The study is a direct examination of the effectiveness of an insurance eligibility
intervention, not a test of the efficacy of specific, non-allopathic treatment regimens. The results of this study
will provide valuable information to clinicians, patients and third party payers on the relative benefits and costs
of an “expanded benefits” treatment option which incorporates chiropractic, acupuncture and massage services
for low back
Study Kong
Trial name or title
Participants
Interventions
Outcomes
Starting date
Contact information
Notes
Study Munglani
Trial name or title Randomised controlled single-blinded trial of deep intra-muscular stimulation in the treatment of chronic
mechanical low back pain.
Participants Out-patients between 18 and 65 years old
Interventions
Outcomes
Starting date
Contact information Dr Rajesh Munglani
Contact details Box No 215
Pain Clinic
Addenbrooke’s NHS Trust
CB2 2QQ
Tel: 2346
Notes Source: www.controlled-trials.com
Deep Intra-Muscular Stimulation is a technique that consists of needling the body of contracted or shortened
muscles, and it is claimed to relieve muscle spasm more effectively than other treatments, but no randomised
controlled trials have been performed, especially to compare its effects with the effects of other needling tech-
niques such as acupuncture or trigger point needling. As the Pain Clinic is at present able to make use of the
services of a highly experienced practitioner of this technique, we are planning to conduct a randomised, con-
trolled, single-blinded trial comparing the benefits of deep Intra-Muscular stimulation with superficial needling
61Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of ongoing studies (Continued )
of subcutaneous tissues in patients with chronic mechanical low back pain. We wish to asses if the needling
of deep muscles specifically produces pain relief over and above that produced by needling of more superficial
structures. We plan to treat two groups of 25 patients each, or a total of 50 patients, administering four treatment
episodes to each patient. Patients will be asked to turn up for four treatment episodes, and to fill in two self-
reporting questionnaires (SCL-90 and Pain VAS) before and at 2, 6 and 26 weeks after treatment.
Study Thomas
Trial name or title Longer term clinical and economic benefits of offering acupuncture to patients with chronic low back pain.
Participants patients with low back pain. Age 20-65 years with low back pain or sciatica, greater than 4 weeks and less than
12-months pain this episode
Interventions i) traditional Chinese acupuncture, up to 10 treatments ii) standard care offered by GP only
Outcomes
Starting date Funding: NHS
Contact information Ms Kate Thomas
Address Medical Care Research Unit
University of Sheffield
ScHARR
Regent Court
30 Regent Street
City/town Sheffield
Zip/Postcode S1 4DA
Country United Kingdom
Tel +44 0114 222 0753
Fax +44 0114 272 4095
Email [email protected]
Sponsor NHS Research and Development Health Technology Assessment Programme (HTA)
Notes Source: www.controlled-trials.com
A D D I T I O N A L T A B L E S
Table 01. Methodological quality assessment
Study A and B C D, E and F G H I J K
Comments,
flaws, etc
Araki 2001 Y and Y Y Y, N, Y Y Y Y Y Y Score=10 and
no serious flaws
(High)
Carlsson 2001 Y and Y DK Y, N, Y DK DK Y (1 month);
N (3 and 6
months)
Y Y Score=7 at 1
month (follow-
up=100%),
Score=6 at 3
and 6 months
(follow-
up=64%
and 54%
respectively)
(High)
62Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 01. Methodological quality assessment (Continued )
Study A and B C D, E and F G H I J K
Comments,
flaws, etc
Ceccherelli
2002
Y and DK Y DK, N, Y DK DK Y Y Y Score=6. No
serious flaws.
(High)
Cherkin 2001 Y and DK Y N, N, Y Y Y Y Y Y Score=8. No
serious flaws
(High)
Coan 1980 Y and Y DK N, N, N DK N N N N Score=2 (Low)
Ding 1998 DK and N DK Y, N, N DK DK Y Y N Score=3
(Low). Main
outcome is very
subjective.
Edelist 1976 DK and DK DK Y, N, Y DK Y DK DK DK Score=3 (Low).
Main outcome
is a subjective
measure.
Methods
poorly
described.
Garvey 1989 Y and DK DK Y, N, Y Y Y Y Y Y Score=8.
No serious
flaws (High).
Baseline
characteristics
are not shown.
Groups are very
different in
size.
Giles 1999 DK and Y DK N, N, Y DK N N Y N Fatal flaw=
52% drop
out during
treatment
period in the
acupuncture
group.
Giles 2003 Y and Y Y N, N, DK Y DK N Y Y Score=6. 39%
drop out at 9-
weeks (Low).
No adjustment
for multiple
comparisons
Grant 1999 Y and Y N N, N, Y Y DK Y Y N Fatal flaw=
baseline
differences in
main outcome
63Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 01. Methodological quality assessment (Continued )
Study A and B C D, E and F G H I J K
Comments,
flaws, etc
measures. VAS
(range 0-200)
at baseline in
acup group was
140 and in the
TENS group
was 101.
Gunn 1980 N and DK DK N, N, DK DK DK Y N N Score=1 (Low).
Allocation by
alternation and
not concealed.
No mention
of blinded
assessments.
We don’t have
baseline values
for pain. Co-
interventions
were allowed
and not
standardized or
monitored. No
ITT: this is not
a big problem
for the 12-week
follow-up, but
maybe for the
longer term
follow-up
He 1997 DK and N Y Y, N, N DK DK N Y DK Score=3
(Low). No
information
about
allocation of
patients. No
description of
lost patients.
Inoue 2000 Y and Y DK Y,N, Y Y Y Y Y Y Score=9
(High). We
believe there
were no losses
because the
follow-up was
shortly after the
single session.
Inoue 2001 Y and Y DK Y,N,Y Y Y Y Y Y Score=9
64Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 01. Methodological quality assessment (Continued )
Study A and B C D, E and F G H I J K
Comments,
flaws, etc
(High). We
believe there
were no losses
because the
follow-up was
shortly after the
single session.
Kerr 2003 Y and DK DK Y,N,Y DK DK N Y N Score=4
(Low). Co-
interventions
might have
influenced the
results. Patients
followed: 76%
in the short and
66.7% in the
intermediate
follow-ups.
Kittang 2001 N and DK N DK,DK,Y Y Y Y Y Y Score=6.
No serious
flaws (High).
Baseline
differences in
three factors
(days of sick
leave previous
year, previous
attendance at
back schools
and use of pain
killers)
Kurosu 1979
(a) and (b)
DK and DK DK N, N, DK DK Y DK Y DK Score=2 (Low)
Lehmann 1983 DK and DK DK N, N, N Y DK N Y N Score=2
(Low). Follow-
up: 77%
immediately
after and 61%
after 6 months.
Leibing 2002 Y and Y Y Y,N, Y Y DK N Y DK Score=7 (High)
However, drop-
out rate: 24%
in the short
and 37% in the
long-term
65Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 01. Methodological quality assessment (Continued )
Study A and B C D, E and F G H I J K
Comments,
flaws, etc
Li 1997 DK and N DK Y, N, N DK DK N Y DK Score=2 (Low)
No information
about
allocation of
patients. No
description of
lost patients.
Lopacz and
Gralewski 1979
DK and DK DK N, N, N Y DK Y Y Y Score=4
(Low). No
information
about
randomization
and not
blinded.
Macdonald
1983
DK and DK Y Y, N, DK DK DK Y DK Y Score=4
(Low). No
information
about
randomization
and timing
of follow-up
measures
Mendelson
1983
DK and DK Y Y, N, Y DK DK Y Y N Score=5 (Low).
Cross over
study.
Meng 2003 Y and Y Y (pain); N
(Roland)
N, N, N Y DK Y Y Y Score=7 (small
difference in
baseline in pain
outcomes).
Score= 6
(important
baseline
difference
in RDQ
(acupuncture
group: 9.8 and
control group:
11.8). (High)
Molsberger
2002
Y and Y Y Y, N, Y DK Y Y (immed), N
(short)
Y Y Score=9
(immediately
after) and
Score=8 (short-
term: drop-
out rate at 3
months was
34%) (High).
66Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 01. Methodological quality assessment (Continued )
Study A and B C D, E and F G H I J K
Comments,
flaws, etc
Blinding was
between verum
and sham
acupuncture,
but not
between verum
and nothing.
Sakai 1998 DK and DK N N,N,DK DK DK N N DK Score=0 (Low).
Methods
poorly
described. A
statistically
significant
difference was
observed in
disability score
at baseline.
ADL was 7.6
in acupuncture
group and 10.3
in medication
group. Other
parameters
such as
subjective
symptom of
pain, JOA
score, duration
of pain, gender
were not
statistically
different at
baseline.
Sakai 2001 Y and Y Y N,N, Y Y Y Y Y N Score=8. No
serious flaws
(High)
Takeda &
Nabeta 2001
Y and DK DK Y,N,N DK Y Y Y DK Score=5 (Low)
Thomas and
Lundberg 1994
DK and DK Y N,N, DK N Y DK Y Y Score=4
(Low). We get
different results
when we re-
analysed using
the data from
the figures.
67Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 01. Methodological quality assessment (Continued )
Study A and B C D, E and F G H I J K
Comments,
flaws, etc
Tsukayama
2002
Y and Y Y N, N, Y Y Y Y Y Y Score=9.
No serious
flaws (High).
Outcome
assessor was
blinded, but
patient was
not. So it is
possible that
the blindness
was broken,
especially
because the
outcomes are
subjective.
Von Mencke
1988
DK and DK DK Y, N, Y N N N N N Score=2 (Low)
Wang 1996 DK and N DK Y, N, N DK N N DK DK Score=1 (Low).
Not adequately
randomized.
Doubts about
reliability
of outcome
measures
Wu 1991 N and N DK Y,N,N DK Y N Y DK Score=3 (Low).
Not adequately
randomized.
Doubts about
reliability
of outcome
measures
Yeung 2003 DK and Y Y N, N, Y Y Y Y Y Y Score=8.
No serious
flaws (High).
Outcome
assessor was
blinded, but
patient was
not. So it is
possible that
the blindness
was broken,
especially
because the
outcomes are
subjective. One
68Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 01. Methodological quality assessment (Continued )
Study A and B C D, E and F G H I J K
Comments,
flaws, etc
of the few
studies that
adjusted for
confounders in
the analysis,
but small
sample size and
did not account
for attention
effects.
Total “Yes” 17 14 14 18, 0, 19 15 15 20 28 16
Total “No” 3 5 3 15, 34, 10 2 3 12 4 10
Total “DK” 15 16 18 2, 1, 6 18 17 3 3 9
Table 02. Clinical relevance assessment
Study Patients Interventions
Relevant
outcomes Size of the effect
Benefits and
harms
Serious
deficiences?
Araki 2001 N Y Y DK DK Population is
poorly described.
Power to detect a
difference (alpha
0.05, 2-tailed) in
pain is 12% and in
function is 5.1%.
Carlsson 2001 Y Y Y Y Y
Ceccherelli 2002 Y Y N DK DK
Cherkin 2001 Y N Y DK Y Intervention is
individualized
to each patient.
Pragmatic trial.
Coan 1980 Y N Y Y DK Intervention is
poorly described
Ding 1998 Y N Y Y Y The strong and
deep needling
technique may not
be practical for
all acupuncture
settings.
Edelist 1976 N Y N N DK Irrelevant
outcomes.
Garvey 1989 N Y N Y N Benefists do not
69Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 02. Clinical relevance assessment (Continued )
Study Patients Interventions
Relevant
outcomes Size of the effect
Benefits and
harms
Serious
deficiences?
seem to be worth
the harms
Giles 1999 N N Y Y DK Patients and
interventions are
poorly described
Giles 2003 N Y Y DK DK Difficult to
interpret results
due to nature of
data presentation.
No follow-up
beyond 9 weeks.
Grant 1999 N N Y N N Population and
interventions are
poorly described
Gunn 1980 Y N N Y DK We don’t
know how co-
interventions were
applied. We don’t
have a separate
measure for pain.
He 1997 Y N Y Y DK No description
of acupuncture
points used.
Not sure about
validity/reliability
of outcome
measure.
Inoue 2000 N Y DK N DK
Inoue 2001 N Y DK Y Y
Kerr 2003 N Y Y N DK No clinically
important effects
detected in this
study
Kittang 2001 Y N Y N DK
Kurosu 1979 (a)
and (b)
N Y N DK DK
Li 1997 Y N Y Y DK No description
of acupuncture
points used.
Not sure about
validity/reliability
of outcome
70Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 02. Clinical relevance assessment (Continued )
Study Patients Interventions
Relevant
outcomes Size of the effect
Benefits and
harms
Serious
deficiences?
measure.
Lehmann 1983 N N N DK Y No description
of acupuncture
points used. Teh
Chi unclear.
Leibing 2002 Y Y Y DK N
Lopacz and
Gralewski 1979
N N N DK DK Poor description
of patients and
interventions.
Macdonald 1983 Y Y Y Y DK It is not meridian
acupuncture and
the depth is too
superficial. Very
small sample size
Mendelson 1983 Y Y Y N DK
Meng 2003 Y Y Y DK DK Size of effect might
be biased by small
sample size. Harms
were assessed,
but should be
evaluated in larger
sample.
Molsberger 2002 Y Y Y Y DK
Sakai 1998 Y N Y DK DK Not sure about
validity of JOA
score. Number of
points and sessions
too small.
Sakai 2001 Y Y Y N DK Not sure about
validity of JOA
score. Number of
points and sessions
too small.
Takeda 2001 N Y Y N DK
Thomas and
Lundberg 1994
N Y Y N DK
Tsukayama 2002 Y Y Y DK N
Von Mencke 1988 Y Y Y Y DK Teh Chi unclear.
Wang 1996 Y Y Y Y Y
Wu 1991 Y Y Y Y Y
71Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 02. Clinical relevance assessment (Continued )
Study Patients Interventions
Relevant
outcomes Size of the effect
Benefits and
harms
Serious
deficiences?
Yeung 2003 Y Y Y Y Y
Table 03. Adequacy of acupuncture
Study
Choice of
acupoints
Number of
sessions
Needling
technique Experience Control group Comments
Araki 2001 Adequate
because this is
acute low-back
pain
Adequate
because it is acute
low-back pain
Adequate Adequate Appropriate
sham
acupuncture
But there is
no description
about credibility
of sham
acupuncture.
Carlsson 2001 Adequate Adequate Adequate Adequate Adequate sham
TENS
The authors also
compared needle
acupuncture
with elec-
troacupuncture.
Ceccherelli 2002 Adequate Adequate Adequate for the
purpose of the
study, which was
to compare two
techniques of
acupuncture.
Not reported Other
acupuncture
technique
Cherkin 2001 Individualized
points.
Adequate TCM typically
with Teh Chi
Adequate Other common
therapies.
Coan 1980 Not reported Adequate Not reported Not reported Waiting list. No
treatment
Poorly reported,
but seems OK
(published in
1980).
Ding 1998 Adequate Adequate Adequate Adequate Other
acupuncture
technique
Edelist 1976 Adequate Few sessions Adequate Not reported Sham
acupuncture (but
may have some
analgesic effect)
The control
group used
needles placed
in areas devoid
of classic
acupuncture
points.
Garvey 1989
(dry needling)
Adequate (dry-
needling)
Adequate Not reported Not reported Three common
treatments
Giles 1999 Not reported Adequate Not reported. Adequate Two common
treatments:
manipulation
72Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 03. Adequacy of acupuncture (Continued )
Study
Choice of
acupoints
Number of
sessions
Needling
technique Experience Control group Comments
and drugs
Giles 2003 Not reported Adequate Not reported. Adequate Two common
treatments:
manipulation
and drugs
Grant 1999 Individualized
points.
Adequate Not reported. Not reported Another
common
treatment:
TENS
Gunn 1980 (dry
needling)
Muscle motor
points. Not
adequate for dry
needling.
Adequate Adequate Not reported Standar therapy:
physiotherapy,
remedial
exercises,
occupational
therapy,
industrial
assessment.
He 1997 Adequate Adequate Adequate Not reported Chinese herbs. No information
about which
herbs were used.
Inoue 2000 Adequate Adequate for the
purpose of the
study.
Not reported Adequate Sham
acupuncture
But there is
no description
about credibility
of sham
acupuncture.
Inoue 2001 Adequate (non
meridian)
Adequate for the
purpose of the
study
Not reported Not reported Sham
acupuncture
But there is
no description
about credibility
of sham
acupuncture.
Kerr 2003 Adequate Adequate Adequate Not reported Sham TENS
Kittang 2001 Seems adequate Not reported Not reported Not reported Naproxen:
adequate dose
and duration of
treatment
Kurosu 1979 (a) Adequate Adequate for the
purpose of the
study.
Adequate Not reported Garlic
moxibustion
may be adequate
treatment for
LBP in some
cases
Kurosu 1979 (b) Adequate Adequate for the
purpose of the
Adequate Not reported Other
acupuncture
73Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 03. Adequacy of acupuncture (Continued )
Study
Choice of
acupoints
Number of
sessions
Needling
technique Experience Control group Comments
study. technique
(needle insertion
and no retention)
Lehmann 1983 Choice of
meridians is OK
Adequate Adequate Adequate Sham TENS
Leibing 2002 Adequate Adequate Adequate Adequate Sham
acupuncture
Li 1997 Adequate Adequate Adequate Not reported Manual
acupuncture
without cupping.
Lopacz and
Gralewski 1979
Not reported Adequate Not reported Not reported Placebo: to
control for
attention effect.
Macdonald 1983 Adequate (not
meridian)
Adequate Adequate for the
purpose of the
study
Not reported Sham TENS. It is easy for
patients to
perceive that they
were receiving
different
treatments.
Mendelson 1983 Adequate Adequate Adequate Adequate Maybe not
adequate
placebo. May
have some
analgesic effect.
Meng 2003 Adequate Adequate Adequate Adequate Standard therapy
Molsberger 2002 Adequate Adequate Adequate Adequate Sham
acupuncture:
good placebo.
Sakai 1998 Adequate Adequate for the
purpose of the
study
Not reported Not reported Medication
Sakai 2001 Adequate (not
meridian)
Adequate for the
purpose of the
study
Not reported Not reported TENS: seems
adequate.
But number
of sessions too
small.
Takeda 2001 Adequate for the
purpose of the
study
Adequate Not reported Not reported Other
acupuncture
technique: local
versus distal
points.
But there is
no description
about credibility
of sham
acupuncture.
Thomas and
Lundberg 1994
Adequate Adequate Adequate Adequate No treatment
Tsukayama 2002 Adequate Adequate for the Adequate Not reported TENS but number
74Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 03. Adequacy of acupuncture (Continued )
Study
Choice of
acupoints
Number of
sessions
Needling
technique Experience Control group Comments
purpose of the
study
of sessions too
small.
Von Mencke
1988
Adequate Adequate Adequate Not reported Sham
acupuncture
Wang 1996 Adequate Adequate Adequate Adequate Active
acupuncture:
distal points
Wu 1991 Adequate (for
acute LBP)
Adequate (single
session for acute
LBP)
Adequate Adequate Another active
acupuncture
treatment
Yeung 2003 Adequate Adequate for the
purpose of the
study
Adequate Adequate Physiotherapy
(standard
exercises)
Patients in
the exercise
group did not
receive the same
attention as in
the acupuncture
group.
Table 04. Improvement in pain
Comparison group Acute Chronic Unknown / Mixed
Acupuncture Number of studies 2 16 8
Average improvement 52% 32% 51%
Standard deviation 39% 24% 19%
Minimum 25% -17% 22%
Maximum 80% 62% 77%
No treatment Number of studies 6
Average improvement 6%
Standard deviation 25%
Minimum -33%
Maximum 42%
Sham / placebo Number of studies 1 6 3
Average improvement 22% 23% 25%
Standard deviation 22% 17%
Minimum -19% 6%
Maximum 44% 37%
Other treatments Number of studies 1 6 3
Average improvement 79% 25% 99%
75Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Standard deviation 19% 73%
Minimum 0% 41%
Maximum 50% 181%
Table 05. Search Strategies
MEDLINE EMBASE
1 randomized controlled trial.pt. (72769)
2 controlled clinical trial.pt. (16977)
3 Randomized Controlled Trials/ (17706)
4 Random Allocation/ (11879)
5 Double-Blind Method/ (26902)
6 Single-Blind Method/ (4389)
7 or/1-6 (120640)
8 Animal/ not Human/ (583159)
9 7 not 8 (112795)
10 clinical trial.pt. (144571)
11 exp Clinical Trials/ (45063)
12 ((singl$ or doubl$ or trebl$ or tripl$) adj (mask$ or
blind$)).tw. (24652)
13 Placebos/ (4548)
14 placebo$.tw. (30921)
15 random$.tw. (123481)
16 Research Design/ (12824)
17 (latin adj square).tw. (663)
18 (clinic$ adj25 trial$).tw. (43883)
19 or/10-18 (275600)
20 19 not 8 (256926)
21 20 not 9 (147773)
22 Comparative Study/ (298320)
23 exp Evaluation Studies/ (155611)
24 Follow-Up Studies/ (95462)
25 Prospective Studies/ (77754)
26 (control$ or prospective$ or volunteer$).tw. (521438)
27 Cross-Over Studies/ (9791)
28 or/22-27 (917800)
29 28 not 8 (737443)
30 29 not (9 or 21) (559548)
31 9 or 21 or 30 (820116)
32 Intervertebral disk/ (1230)
33 Lumbar vertebrae/ (6673)
34 Low-back pain/ (3418)
35 Sciatica/ (544)
36 low back pain.tw. (2796)
37 backache.tw. (276)
38 lumbago.tw. (174)
39 or/32-38 (11150)
40 ACUPUNCTURE/ (114)
41 exp ACUPUNCTURE ANALGESIA/ (185)
1 clinical article/ (299265)
2 clinical study/ (2230)
3 clinical trial/ (184343)
4 controlled study/ (953915)
5 randomized controlled trial/ (58211)
6 major clinical study/ (352156)
7 double blind procedure/ (27710)
8 multicenter study/ (19950)
9 single blind procedure/ (3090)
10 crossover procedure/ (9288)
11 placebo/ (23129)
12 or/1-11 (1350338)
13 allocat$.ti,ab. (10381)
14 assign$.ti,ab. (34017)
15 blind$.ti,ab. (39706)
16 (clinic$ adj25 (study or trial)).ti,ab. (103723)
17 compar$.ti,ab. (592128)
18 control$.ti,ab. (435060)
19 cross?over.ti,ab. (7854)
20 factorial$.ti,ab. (2463)
21 follow?up.ti,ab. (3710)
22 placebo$.ti,ab. (32609)
23 prospectiv$.ti,ab. (81230)
24 random$.ti,ab. (119291)
25 ((singl$ or doubl$ or trebl$ or tripl$) adj25 (blind$ or
mask$)).ti,ab. (27455)
26 trial.ti,ab. (57298)
27 (versus or vs).ti,ab. (144304)
28 or/13-27 (1052880)
29 12 or 28 (1707121)
30 human/ (1767116)
31 nonhuman/ (855690)
32 animal/ (592)
33 animal experiment/ (266367)
34 31 or 32 or 33 (857723)
35 30 and 34 (145063)
36 29 not 34 (1118616)
37 29 and 35 (85582)
38 36 or 37 (1204198)
39 Lumbar Spine/ (4963)
40 Lumbosacral Spine/ (629)
41 Intervertebral Disk/ (710)
76Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 05. Search Strategies (Continued )
MEDLINE EMBASE
42 exp ACUPUNCTURE, EAR/ (31)
43 exp ACUPUNCTURE POINTS/ (403)
44 exp ACUPUNCTURE THERAPY/ (1918)
45 acupuncture.tw. (1655)
46 electro-acupuncture.tw. (62)
47 acupressure.tw. (84)
48 or/40-47 (2324)
49 31 and 39 and 48 (49)
42 Intervertebral Disk Disease/ (295)
43 Lumbar Disk Hernia/ (835)
44 Low back pain/ (5403)
45 Ischialgia/ (743)
46 low back pain.tw. (3184)
47 backache.tw. (270)
48 lumbago.tw. (162)
49 or/39-48 (12240)
50 exp ACUPUNCTURE/ (2907)
51 exp ACUPUNCTURE ANALGESIA/ (143)
52 acupuncture.tw. (1775)
53 electro-acupuncture.tw. (56)
54 acupressure.tw. (71)
55 or/50-54 (3014)
56 38 and 49 and 55 (85)
Table 06. Internal Validity Criteria
Criteria Operationalization
A. Was the method of randomization adequate? A. A random (unpredictable) assignment sequence. Examples of
adequate methods are computer generated random number table
and use of sealed opaque envelopes. Methods of allocation using
date of birth, date of admission, hospital numbers, or alternation
should not be regarded as appropriate.
B. Was the treatment allocation concealed? B. Assignment generated by an independent person not
responsible for determining the eligibility of the patients. This
person has no information about the persons included in the
trial and has no influence on the assignment sequence or on the
decision about eligibility of the patient.
C. Were the groups similar at baseline regarding the most
important prognostic indicators?
C. In order to receive a “yes,” groups have to be similar at
baseline regarding demographic factors, duration and severity of
complaints, percentage of patients with neurologic symptoms,
and value of main outcome measure(s).
D. Was the patient blinded to the intervention? D. The reviewer determines if enough information about the
blinding is given in order to score a “yes.”
E. Was the care provider blinded to the intervention? E. The reviewer determines if enough information about the
blinding is given in order to score a “yes.”
F. Was the outcome assessor blinded to the intervention? F. The reviewer determines if enough information about the
blinding is given in order to score a “yes.”
G. Were cointerventions avoided or similar? G. Cointerventions should either be avoided in the trial design or
similar between the index and control groups.
H. Was the compliance acceptable in all groups? H. The reviewer determines if the compliance to the interventions
is acceptable, based on the reported intensity, duration, number
and frequency of sessions for both the index intervention and
control intervention(s).
77Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 06. Internal Validity Criteria (Continued )
Criteria Operationalization
I. Was the drop-out rate described and acceptable? I. The number of participants who were included in the study but
did not complete the observation period or were not included in
the analysis must be described and reasons given. If the percentage
of withdrawals and drop-outs does not exceed 20% for immediate
and short-term follow-ups, 30% for intermediate and long-term
follow-ups and does not lead to substantial bias a “yes” is scored.
J. Was the timing of the outcome assessment in all groups similar? J. Timing of outcome assessment should be identical for all
intervention groups and for all important outcome assessments.
K. Did the analysis include an intention-to-treat analysis? K. All randomized patients are reported/analyzed in the group
they were allocated to by randomization for the most important
moments of effect measurement (minus missing values)
irrespective of noncompliance and cointerventions.
A N A L Y S E S
Comparison 01. acupuncture versus no treatment ((Sub)acute LBP: < 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain Weighted Mean Difference (Fixed) 95% CI Totals not selected
02 global improvement Peto Odds Ratio 95% CI Totals not selected
03 functional status Weighted Mean Difference (Fixed) 95% CI Totals not selected
04 physical examination Weighted Mean Difference (Fixed) 95% CI Totals not selected
05 return to work Peto Odds Ratio 95% CI Totals not selected
Comparison 02. acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (VAS) (lower values are
better)
Weighted Mean Difference (Random) 95% CI Totals not selected
02 global measure Peto Odds Ratio 95% CI Totals not selected
03 functional status (higher scores
are better). Generic instrument
Weighted Mean Difference (Random) 95% CI Totals not selected
04 physical examination: finger-
floor distance (lower values are
better)
Weighted Mean Difference (Random) 95% CI Totals not selected
05 return to work Peto Odds Ratio 95% CI Totals not selected
06 mean difference in pain (final -
initial)
Weighted Mean Difference (Random) 95% CI Totals not selected
07 mean difference in functional
status (final - initial) Generic
instrument
Weighted Mean Difference (Random) 95% CI Totals not selected
08 mean difference in physical
examination (final - initial):
finger-floor distance
Weighted Mean Difference (Random) 95% CI Totals not selected
78Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 03. acupuncture versus other intervention ((Sub)acute LBP: < 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (VAS): lower values are
better
Weighted Mean Difference (Fixed) 95% CI Totals not selected
02 global measure (higher values
are better)
Relative Risk (Random) 95% CI Totals not selected
03 functional status Weighted Mean Difference (Fixed) 95% CI Totals not selected
04 physical examination (finger
floor distance)
Weighted Mean Difference (Fixed) 95% CI Totals not selected
05 return to work Peto Odds Ratio 95% CI Totals not selected
06 Side effects / Complications Relative Risk (Random) 95% CI Totals not selected
Comparison 04. acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain Weighted Mean Difference (Fixed) 95% CI Totals not selected
02 global measure Relative Risk (Random) 95% CI Totals not selected
03 functional status Weighted Mean Difference (Fixed) 95% CI Totals not selected
04 physical examination Weighted Mean Difference (Fixed) 95% CI Totals not selected
05 return to work Peto Odds Ratio 95% CI Totals not selected
Comparison 05. acupuncture versus no treatment. (Chronic LBP: > 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (instruments: VAS and
number of words)
Standardised Mean Difference (Random) 95%
CI
Subtotals only
02 global measure (improvement) Odds Ratio (Random) 95% CI Totals not selected
03 functional status (higher values
are better)
Weighted Mean Difference (Random) 95% CI Totals not selected
04 limitation of activity (higher
values are worse)
Weighted Mean Difference (Fixed) 95% CI Totals not selected
05 physical examination Weighted Mean Difference (Fixed) 95% CI Totals not selected
06 return to work Peto Odds Ratio 95% CI Totals not selected
07 functional status (standardized
measures)
Effect size (Random) 95% CI Subtotals only
Comparison 06. acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (lower values mean better) Weighted Mean Difference (Random) 95% CI Subtotals only
02 global improvement (higher
values are better)
Relative Risk (Random) 95% CI Subtotals only
03 pain disability index (lower
values are better)
Weighted Mean Difference (Random) 95% CI Totals not selected
04 physical examination
(fingertips-to-floor distance).(
Lower values are better)
Weighted Mean Difference (Fixed) 95% CI Totals not selected
79Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

05 improvement in physical
examination
Odds Ratio (Random) 95% CI Totals not selected
06 Sick leave (higher values mean
worse)
Relative Risk (Random) 95% CI Subtotals only
07 Well being (SF-36). (Higher
values are better)
Weighted Mean Difference (Fixed) 95% CI Totals not selected
08 Side effects / Complications Risk Difference (Random) 95% CI Totals not selected
09 pain (percent of baseline values) Other data No numeric data
10 sick leave Other data No numeric data
11 general level of pain (0-15
points)(more points mean less
pain)
Other data No numeric data
12 pain: difference between within
group changes
differences between (Random) 95% CI Totals not selected
13 function: difference between
within group changes
differences between (Random) 95% CI Totals not selected
14 Pain: percentage of patients
with >50% pain reduction
Relative Risk (Random) 95% CI Totals not selected
15 spine range of motion:
difference between within
group changes
difference between (Random) 95% CI Totals not selected
Comparison 07. acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (lower values are better) Standardised Mean Difference (Random) 95%
CI
Totals not selected
02 global measure Relative Risk (Random) 95% CI Totals not selected
03 back specific functional status
(lower scores mean better). Ex:
RDQ, Oswestry and Aberdeen
Standardised Mean Difference (Random) 95%
CI
Totals not selected
04 back specific functional status
(higher scores are better). Ex:
Japan Orthopedic Association
Score.
Weighted Mean Difference (Random) 95% CI Totals not selected
05 pain disability index (lower
values are better)
Weighted Mean Difference (Random) 95% CI Totals not selected
06 physical examination Weighted Mean Difference (Fixed) 95% CI Totals not selected
07 return to work (higher values
mean better)
Relative Risk (Random) 95% CI Totals not selected
08 Side effects / Complications Risk Difference (Random) 95% CI Totals not selected
09 pain and function (adjusted for
baseline values)
Other data No numeric data
10 general level of pain (0-15
points)(more points mean less
pain)
Other data No numeric data
11 pain: difference between within
group changes
differences between (Random) 95% CI Totals not selected
80Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 08. acupuncture versus acupuncture. (Chronic LBP: > 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (lower values mean better) Weighted Mean Difference (Fixed) 95% CI Totals not selected
02 Improvement (higher values are
better)
Relative Risk (Random) 95% CI Totals not selected
03 functional status Weighted Mean Difference (Fixed) 95% CI Totals not selected
04 physical examination Weighted Mean Difference (Fixed) 95% CI Totals not selected
05 return to work Peto Odds Ratio 95% CI Totals not selected
06 improvement Other data No numeric data
Comparison 09. dry-needling versus other intervention ((Sub)acute LBP < 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 global measure (higher values
are better)
Relative Risk (Random) 95% CI Totals not selected
02 Side effects / Complications Relative Risk (Random) 95% CI Totals not selected
Comparison 10. acupuncture versus placebo or sham intervention (unknown / mixed duration of low back pain)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (VAS): lower values are
better
Weighted Mean Difference (Random) 95% CI Totals not selected
02 global measure Relative Risk (Random) 95% CI Totals not selected
03 functional status (higher scores
are better). Generic instrument
Weighted Mean Difference (Fixed) 95% CI Totals not selected
04 physical examination (higher
values are better)
Weighted Mean Difference (Fixed) 95% CI Totals not selected
05 return to work Peto Odds Ratio 95% CI Totals not selected
Comparison 11. acupuncture versus other intervention (unknown / mixed duration of low back pain)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain score (lower values mean
better)
Weighted Mean Difference (Random) 95% CI Totals not selected
02 pain recovery: higher values are
better
Standardised Mean Difference (Random) 95%
CI
Totals not selected
03 global measure (higher values
are better)
Relative Risk (Random) 95% CI Totals not selected
04 back specific functional status
(higher scores are better). Ex:
Japan Orthopedic Association
Score.
Weighted Mean Difference (Random) 95% CI Totals not selected
05 physical examination Weighted Mean Difference (Fixed) 95% CI Totals not selected
06 return to work Peto Odds Ratio 95% CI Totals not selected
07 Side effects / Complications Risk Difference (Random) 95% CI Totals not selected
81Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 12. acupuncture versus acupuncture. (unknown / mixed duration of low back pain)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (lower values are better) Weighted Mean Difference (Random) 95% CI Totals not selected
02 pain recovery (higher values are
better)
Weighted Mean Difference (Random) 95% CI Totals not selected
03 global measure (higher values
are better)
Relative Risk (Random) 95% CI Totals not selected
04 functional status (higher values
are better)
Weighted Mean Difference (Random) 95% CI Totals not selected
05 physical examination (finger-
floor distance) Higher values
are better.
Weighted Mean Difference (Random) 95% CI Totals not selected
06 return to work Peto Odds Ratio 95% CI Totals not selected
07 improvement Other data No numeric data
Comparison 13. acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 pain (lower values are better) Standardised Mean Difference (Random) 95%
CI
Subtotals only
02 pain: difference between within
group changes
differences between (Random) 95% CI Subtotals only
03 pain disability index (lower
values are better)
Weighted Mean Difference (Random) 95% CI Totals not selected
04 Pain: percentage of patients
with >50% pain reduction
Relative Risk (Random) 95% CI Totals not selected
05 function: difference between
within group changes
differences between (Random) 95% CI Subtotals only
06 global measure Relative Risk (Random) 95% CI Totals not selected
07 back specific functional status
(lower scores mean better). Ex:
RDQ, Oswestry and Aberdeen
Standardised Mean Difference (Random) 95%
CI
Subtotals only
08 spine range of motion:
difference between within
group changes
difference between (Random) 95% CI Totals not selected
09 Side effects / Complications Risk Difference (Random) 95% CI Totals not selected
I N D E X T E R M S
Medical Subject Headings (MeSH)∗Acupuncture Therapy; Low Back Pain [∗therapy]; Randomized Controlled Trials as Topic
MeSH check words
Humans
C O V E R S H E E T
Title Acupuncture and dry-needling for low back pain
82Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Authors Furlan AD, van Tulder MW, Cherkin DC, Tsukayama H, Lao L, Koes BW, Berman BM
Contribution of author(s) - Furlan, van Tulder, Cherkin, Lao, Koes and Berman wrote the protocol for this review;
- Furlan, van Tulder, Koes conducted the literature search and study selection of the English
language trials;
- Tsukayama conducted the literature search and study selection of the Japanese language
trials;
- The Chinese Cochrane Centre conducted the literature search of the Chinese language
trials and Lao selected the studies;
- Furlan, van Tulder, Cherkin, and Koes performed the quality assessment and date extrac-
tion of the English language trials;
- Lao and Tsukayama performed the quality assessment and data extraction of the Japanese
and Chinese language trials;
- All authors were involved in writing the final draft of the manuscript.
Issue protocol first published 1998/2
Review first published 1999/1
Date of most recent amendment 22 August 2006
Date of most recent
SUBSTANTIVE amendment
30 October 2004
What’s New The first version of this review included 11 randomized trials. This update added 24 more
randomized trials, for a total of 35. Meta-analyses were performed for some comparison
groups.
In contrast to the previous review that concluded that the poor methodological quality of
the trials did not allow any conclusions on the effectiveness of acupuncture, the current
update demonstrated the effectiveness of meridian acupuncture for chronic low-back pain
in some special cases:
1) compared to no treatment, acupuncture improved pain and function at short-term follow-
up
2) compared to sham therapies, acupuncture improved pain at short-term follow-up, but
these effects were not maintained at longer-term follow-up and they were not observed for
functional outcomes
3) when acupuncture was added to other conventional therapies, there was better pain relief
and improved function when compared to the conventional therapies alone.
Also, this updated review examined acupuncture separately from dry-needling. The authors
concluded that no clear recommendations could be made about dry-needling because of
the small sample sizes and low methodological quality of the studies, although it appeared
that dry-needling was a useful adjunct to other therapies for chronic low-back pain. Effects
in all cases were only small.
Date new studies sought but
none found
Information not supplied by author
Date new studies found but not
yet included/excluded
Information not supplied by author
Date new studies found and
included/excluded
02 June 2003
Date authors’ conclusions
section amended
23 June 2004
Contact address Dr Andrea Furlan
Evidence-based practice co-ordinator
83Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Institute for Work & Health
481 University Avenue, Suite 800
Toronto
ON
M5G 2E9
CANADA
E-mail: [email protected]
Tel: 416 927 2027
Fax: 416 927 4167
DOI 10.1002/14651858.CD001351.pub2
Cochrane Library number CD001351
Editorial group Cochrane Back Group
Editorial group code HM-BACK
G R A P H S A N D O T H E R T A B L E S
Figure 01. Acupuncture compared to no treatment, placebo or sham therapy
84Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Figure 02. Acupuncture compared to another intervention or added to other interventions
85Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Figure 03. Effects of dry-needling at trigger points
Figure 04. Comparison between two techniques of acupuncture
86Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 01.01. Comparison 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months), Outcome 01
pain
Review: Acupuncture and dry-needling for low back pain
Comparison: 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months)
Outcome: 01 pain
Study Acupuncture No treatment Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupuncture favours control
87Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 01.03. Comparison 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months), Outcome 03
functional status
Review: Acupuncture and dry-needling for low back pain
Comparison: 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months)
Outcome: 03 functional status
Study Acupuncture No treatment Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupuncture favours control
88Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 01.04. Comparison 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months), Outcome 04
physical examination
Review: Acupuncture and dry-needling for low back pain
Comparison: 01 acupuncture versus no treatment ((Sub)acute LBP: < 3 months)
Outcome: 04 physical examination
Study Acupuncture No treatment Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupuncture favours control
89Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 02.01. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3
months), Outcome 01 pain (VAS) (lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months)
Outcome: 01 pain (VAS) (lower values are better)
Study Acupuncture placebo / sham Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after end of sessions
Araki 2001 20 49.55 (22.63) 20 55.65 (27.41) -6.10 [ -21.68, 9.48 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
favours acupuncture favours control
90Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 02.03. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3
months), Outcome 03 functional status (higher scores are better). Generic instrument
Review: Acupuncture and dry-needling for low back pain
Comparison: 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months)
Outcome: 03 functional status (higher scores are better). Generic instrument
Study Acupuncture placebo / sham Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Araki 2001 20 6.60 (3.22) 20 6.50 (3.09) 0.10 [ -1.86, 2.06 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours control favours acupuncture
91Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 02.04. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3
months), Outcome 04 physical examination: finger-floor distance (lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months)
Outcome: 04 physical examination: finger-floor distance (lower values are better)
Study Acupuncture placebo / sham Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Araki 2001 20 25.25 (18.69) 20 28.78 (19.41) -3.53 [ -15.34, 8.28 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
favours acupuncture favours control
92Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 02.06. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3
months), Outcome 06 mean difference in pain (final - initial)
Review: Acupuncture and dry-needling for low back pain
Comparison: 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months)
Outcome: 06 mean difference in pain (final - initial)
Study Treatment Control Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after end of sessions
Araki 2001 20 17.05 (15.74) 20 15.85 (25.50) 1.20 [ -11.93, 14.33 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
Favours control Favours acupuncture
93Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 02.07. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3
months), Outcome 07 mean difference in functional status (final - initial) Generic instrument
Review: Acupuncture and dry-needling for low back pain
Comparison: 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months)
Outcome: 07 mean difference in functional status (final - initial) Generic instrument
Study Acupuncture placebo / sham Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Araki 2001 20 -2.15 (4.32) 20 -1.15 (2.68) -1.00 [ -3.23, 1.23 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours control favours acupuncture
94Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 02.08. Comparison 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3
months), Outcome 08 mean difference in physical examination (final - initial): finger-floor distance
Review: Acupuncture and dry-needling for low back pain
Comparison: 02 acupuncture versus placebo or sham intervention ((Sub)acute LBP: < 3 months)
Outcome: 08 mean difference in physical examination (final - initial): finger-floor distance
Study Acupuncture placebo / sham Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Araki 2001 20 -3.65 (7.62) 20 -0.13 (9.66) -3.52 [ -8.91, 1.87 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupuncture favours control
95Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 03.01. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months),
Outcome 01 pain (VAS): lower values are better
Review: Acupuncture and dry-needling for low back pain
Comparison: 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months)
Outcome: 01 pain (VAS): lower values are better
Study Acupuncture Other intervention Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Kittang 2001 28 13.00 (0.0) 29 12.90 (0.0) Not estimable
02 Short-term follow-up (up to 3 months after the end of the sessions)
Kittang 2001 28 6.40 (0.0) 29 8.70 (0.0) Not estimable
03 Intermediate-term follow-up (3 months to 1 year)
Kittang 2001 28 9.60 (0.0) 29 14.40 (0.0) Not estimable
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
96Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 03.02. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months),
Outcome 02 global measure (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months)
Outcome: 02 global measure (higher values are better)
Study Acupuncture Other intervention Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
He 1997 49/50 42/50 1.17 [ 1.03, 1.33 ]
0.5 0.7 1 1.5 2
favours other interv favours acupuncture
97Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 03.03. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months),
Outcome 03 functional status
Review: Acupuncture and dry-needling for low back pain
Comparison: 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months)
Outcome: 03 functional status
Study Acupuncture Other intervention Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
98Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 03.04. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months),
Outcome 04 physical examination (finger floor distance)
Review: Acupuncture and dry-needling for low back pain
Comparison: 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months)
Outcome: 04 physical examination (finger floor distance)
Study Acupuncture Other intervention Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Kittang 2001 28 46.00 (0.0) 29 46.00 (0.0) Not estimable
02 Short-term follow-up (up to 3 months after the end of the sessions)
Kittang 2001 28 46.00 (0.0) 29 49.00 (0.0) Not estimable
03 Intermediate-term follow-up (3 months to 1 year)
Kittang 2001 28 46.00 (0.0) 29 47.00 (0.0) Not estimable
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
99Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 03.06. Comparison 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months),
Outcome 06 Side effects / Complications
Review: Acupuncture and dry-needling for low back pain
Comparison: 03 acupuncture versus other intervention ((Sub)acute LBP: < 3 months)
Outcome: 06 Side effects / Complications
Study Treatment Control Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Kittang 2001 3/28 12/29 0.26 [ 0.08, 0.82 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.01 0.1 1 10 100
Favours acupuncture Favours other interv
100Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 04.01. Comparison 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months), Outcome 01
pain
Review: Acupuncture and dry-needling for low back pain
Comparison: 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months)
Outcome: 01 pain
Study Technique 1 Technique 2 Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
101Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 04.02. Comparison 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months), Outcome 02
global measure
Review: Acupuncture and dry-needling for low back pain
Comparison: 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months)
Outcome: 02 global measure
Study Technique 1 Technique 2 Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Wu (a) 1991 70/75 60/75 1.17 [ 1.03, 1.33 ]
Wu (b) 1991 60/75 45/75 1.33 [ 1.07, 1.66 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.5 0.7 1 1.5 2
favours technique 2 favours technique 1
102Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 04.03. Comparison 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months), Outcome 03
functional status
Review: Acupuncture and dry-needling for low back pain
Comparison: 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months)
Outcome: 03 functional status
Study Technique 1 Technique 1 Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
103Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 04.04. Comparison 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months), Outcome 04
physical examination
Review: Acupuncture and dry-needling for low back pain
Comparison: 04 acupuncture versus acupuncture. ((Sub)acute LBP: < 3 months)
Outcome: 04 physical examination
Study Technique 1 Technique 2 Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
104Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 05.01. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 01
pain (instruments: VAS and number of words)
Review: Acupuncture and dry-needling for low back pain
Comparison: 05 acupuncture versus no treatment. (Chronic LBP: > 3 months)
Outcome: 01 pain (instruments: VAS and number of words)
Study Acupuncture No treatment Standardised Mean Difference (Random) Weight Standardised Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Immediately after the end of the sessions
Subtotal (95% CI) 0 0 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
02 Short-term follow-up (up to 3 months after the end of the sessions)
Coan 1980 25 2.84 (2.00) 25 4.69 (2.00) 60.5 -0.91 [ -1.50, -0.33 ]
Thomas % Lundberg 94 30 4.00 (5.00) 10 6.10 (1.75) 39.5 -0.46 [ -1.19, 0.26 ]
Subtotal (95% CI) 55 35 100.0 -0.73 [ -1.19, -0.28 ]
Test for heterogeneity chi-square=0.89 df=1 p=0.35 I² =0.0%
Test for overall effect z=3.16 p=0.002
03 Intermediate-term follow-up (3 months to 1 year)
Thomas % Lundberg 94 30 4.00 (3.00) 10 6.20 (1.80) 100.0 -0.78 [ -1.52, -0.04 ]
Subtotal (95% CI) 30 10 100.0 -0.78 [ -1.52, -0.04 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.07 p=0.04
04 Long-term follow-up (more than 1 year)
Subtotal (95% CI) 0 0 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
-4 -2 0 2 4
favours acupuncture favours no treatment
105Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 05.02. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 02
global measure (improvement)
Review: Acupuncture and dry-needling for low back pain
Comparison: 05 acupuncture versus no treatment. (Chronic LBP: > 3 months)
Outcome: 02 global measure (improvement)
Study Acupuncture No treatment Odds Ratio (Random) Odds Ratio (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
Coan 1980 19/25 5/25 12.67 [ 3.31, 48.50 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.01 0.1 1 10 100
favours no treatment favours acupuncture
106Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 05.03. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 03
functional status (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 05 acupuncture versus no treatment. (Chronic LBP: > 3 months)
Outcome: 03 functional status (higher values are better)
Study Acupuncture No treatment Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
Thomas % Lundberg 94 30 8.50 (2.30) 10 7.00 (2.50) 1.50 [ -0.25, 3.25 ]
03 Intermediate-term follow-up (3 months to 1 year)
Thomas % Lundberg 94 30 8.90 (3.10) 10 9.00 (2.40) -0.10 [ -1.96, 1.76 ]
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours no treatment favours acupuncture
107Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 05.04. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 04
limitation of activity (higher values are worse)
Review: Acupuncture and dry-needling for low back pain
Comparison: 05 acupuncture versus no treatment. (Chronic LBP: > 3 months)
Outcome: 04 limitation of activity (higher values are worse)
Study Acupuncture No treatment Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
Coan 1980 25 1.33 (0.70) 25 1.77 (0.70) -0.44 [ -0.83, -0.05 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-1 -0.5 0 0.5 1
favours acupuncture favours control
108Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 05.05. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 05
physical examination
Review: Acupuncture and dry-needling for low back pain
Comparison: 05 acupuncture versus no treatment. (Chronic LBP: > 3 months)
Outcome: 05 physical examination
Study Acupuncture No treatment Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupuncture favours control
109Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 05.07. Comparison 05 acupuncture versus no treatment. (Chronic LBP: > 3 months), Outcome 07
functional status (standardized measures)
Review: Acupuncture and dry-needling for low back pain
Comparison: 05 acupuncture versus no treatment. (Chronic LBP: > 3 months)
Outcome: 07 functional status (standardized measures)
Study Acupuncture No treatment Effect size (SE) Effect size (Random) Weight Effect size (Random)
N N 95% CI (%) 95% CI
01 Immediately after the end of the sessions
Subtotal (95% CI) 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
02 Short-term follow-up (up to 3 months after the end of the sessions)
Coan 1980 25 25 0.63 (0.29) 61.9 0.63 [ 0.06, 1.20 ]
Thomas % Lundberg 94 30 10 0.64 (0.37) 38.1 0.64 [ -0.09, 1.37 ]
Subtotal (95% CI) 100.0 0.63 [ 0.19, 1.08 ]
Test for heterogeneity chi-square=0.00 df=1 p=0.98 I² =0.0%
Test for overall effect z=2.78 p=0.005
03 Intermediate-term follow-up (3 months to 1 year)
Thomas % Lundberg 94 30 10 0.03 (0.37) 100.0 0.03 [ -0.70, 0.76 ]
Subtotal (95% CI) 100.0 0.03 [ -0.70, 0.76 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.08 p=0.9
04 Long-term follow-up (more than 1 year)
Subtotal (95% CI) 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
-4 -2 0 2 4
Favours no treatment Favours acupuncture
110Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.01. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 01 pain (lower values mean better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 01 pain (lower values mean better)
Study Acupuncture placebo / sham Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Immediately after the end of the sessions
Kerr 2003 26 51.30 (22.40) 20 61.70 (30.60) 9.0 -10.40 [ -26.34, 5.54 ]
Leibing 2002 35 21.00 (22.00) 40 32.00 (22.00) 22.9 -11.00 [ -20.98, -1.02 ]
Mendelson 1983 36 30.20 (18.00) 41 40.00 (24.30) 25.3 -9.80 [ -19.28, -0.32 ]
Molsberger 2002 58 26.00 (21.00) 58 36.00 (19.00) 42.9 -10.00 [ -17.29, -2.71 ]
Subtotal (95% CI) 155 159 100.0 -10.21 [ -14.99, -5.44 ]
Test for heterogeneity chi-square=0.03 df=3 p=1.00 I² =0.0%
Test for overall effect z=4.20 p=0.00003
02 Short-term follow-up (up to 3 months after the end of the sessions)
Carlsson (even) 34 52.00 (24.00) 16 64.00 (25.00) 27.7 -12.00 [ -26.67, 2.67 ]
Molsberger 2002 47 23.00 (20.00) 41 43.00 (23.00) 72.3 -20.00 [ -29.07, -10.93 ]
Subtotal (95% CI) 81 57 100.0 -17.79 [ -25.50, -10.07 ]
Test for heterogeneity chi-square=0.83 df=1 p=0.36 I² =0.0%
Test for overall effect z=4.52 p<0.00001
03 Intermediate-term follow-up (3 months to 1 year)
Carlsson (even) 23 48.00 (22.00) 9 62.00 (30.00) 17.4 -14.00 [ -35.56, 7.56 ]
Leibing 2002 33 31.00 (18.00) 31 35.00 (22.00) 82.6 -4.00 [ -13.88, 5.88 ]
Subtotal (95% CI) 56 40 100.0 -5.74 [ -14.72, 3.25 ]
Test for heterogeneity chi-square=0.68 df=1 p=0.41 I² =0.0%
Test for overall effect z=1.25 p=0.2
04 Long-term follow-up (more than 1 year)
Carlsson (even) 21 42.00 (24.00) 6 54.00 (35.00) 100.0 -12.00 [ -41.83, 17.83 ]
Subtotal (95% CI) 21 6 100.0 -12.00 [ -41.83, 17.83 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.79 p=0.4
-100 -50 0 50 100
favours acupuncture favours control
111Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.02. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 02 global improvement (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 02 global improvement (higher values are better)
Study Acupuncture placebo / sham Relative Risk (Random) Weight Relative Risk (Random)
n/N n/N 95% CI (%) 95% CI
01 Immediately after the end of the sessions
Lopacz % Gralewski 13/18 9/16 11.2 1.28 [ 0.76, 2.16 ]
Mendelson 1983 21/36 21/41 18.2 1.14 [ 0.76, 1.71 ]
Molsberger 2002 52/62 41/61 70.6 1.25 [ 1.02, 1.53 ]
Subtotal (95% CI) 116 118 100.0 1.23 [ 1.04, 1.46 ]
Total events: 86 (Acupuncture), 71 (placebo / sham)
Test for heterogeneity chi-square=0.19 df=2 p=0.91 I² =0.0%
Test for overall effect z=2.35 p=0.02
02 Short-term follow-up (up to 3 months after the end of the sessions)
Carlsson 2001 16/34 2/16 9.8 3.76 [ 0.98, 14.44 ]
Edelist 1976 7/15 6/15 22.7 1.17 [ 0.51, 2.66 ]
Molsberger 2002 36/49 23/42 67.5 1.34 [ 0.97, 1.85 ]
Subtotal (95% CI) 98 73 100.0 1.44 [ 0.92, 2.24 ]
Total events: 59 (Acupuncture), 31 (placebo / sham)
Test for heterogeneity chi-square=2.65 df=2 p=0.27 I² =24.6%
Test for overall effect z=1.61 p=0.1
03 Intermediate-term follow-up (3 months to 1 year)
Kerr 2003 21/23 13/17 100.0 1.19 [ 0.89, 1.60 ]
Subtotal (95% CI) 23 17 100.0 1.19 [ 0.89, 1.60 ]
Total events: 21 (Acupuncture), 13 (placebo / sham)
Test for heterogeneity: not applicable
Test for overall effect z=1.19 p=0.2
04 Long-term follow-up (more than 1 year)
Carlsson 2001 14/34 2/16 100.0 3.29 [ 0.85, 12.80 ]
Subtotal (95% CI) 34 16 100.0 3.29 [ 0.85, 12.80 ]
Total events: 14 (Acupuncture), 2 (placebo / sham)
Test for heterogeneity: not applicable
Test for overall effect z=1.72 p=0.09
0.1 0.2 0.5 1 2 5 10
favours control favours acupuncture
112Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.03. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 03 pain disability index (lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 03 pain disability index (lower values are better)
Study Acupuncture placebo / sham Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Leibing 2002 35 11.30 (15.00) 40 15.80 (10.50) -4.50 [ -10.44, 1.44 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 33 16.20 (12.50) 31 17.00 (11.30) -0.80 [ -6.63, 5.03 ]
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupuncture favours control
113Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.04. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 04 physical examination (fingertips-to-floor distance).( Lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 04 physical examination (fingertips-to-floor distance).( Lower values are better)
Study Acupuncture placebo / sham Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Kerr 2003 26 23.60 (20.00) 20 28.40 (24.20) -4.80 [ -17.90, 8.30 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
favours acupuncture favours control
114Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.05. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 05 improvement in physical examination
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 05 improvement in physical examination
Study Treatment Control Odds Ratio (Random) Odds Ratio (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
Edelist 1976 6/15 5/15 1.33 [ 0.30, 5.91 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.1 0.2 0.5 1 2 5 10
Favours control Favours acupuncture
115Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.06. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 06 Sick leave (higher values mean worse)
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 06 Sick leave (higher values mean worse)
Study Acupuncture placebo / sham Relative Risk (Random) Weight Relative Risk (Random)
n/N n/N 95% CI (%) 95% CI
01 Immediately after the end of the sessions
Subtotal (95% CI) 0 0 0.0 Not estimable
Total events: 0 (Acupuncture), 0 (placebo / sham)
Test for heterogeneity: not applicable
Test for overall effect: not applicable
02 Short-term follow-up (up to 3 months after the end of the sessions)
Subtotal (95% CI) 0 0 0.0 Not estimable
Total events: 0 (Acupuncture), 0 (placebo / sham)
Test for heterogeneity: not applicable
Test for overall effect: not applicable
03 Intermediate-term follow-up (3 months to 1 year)
Carlsson 2001 3/21 5/11 38.5 0.31 [ 0.09, 1.08 ]
Lehmann 1986 6/13 7/13 61.5 0.86 [ 0.40, 1.86 ]
Subtotal (95% CI) 34 24 100.0 0.58 [ 0.22, 1.54 ]
Total events: 9 (Acupuncture), 12 (placebo / sham)
Test for heterogeneity chi-square=1.89 df=1 p=0.17 I² =47.1%
Test for overall effect z=1.09 p=0.3
04 Long-term follow-up (more than 1 year)
Subtotal (95% CI) 0 0 0.0 Not estimable
Total events: 0 (Acupuncture), 0 (placebo / sham)
Test for heterogeneity: not applicable
Test for overall effect: not applicable
0.1 0.2 0.5 1 2 5 10
favours acupuncture favours control
116Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.07. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 07 Well being (SF-36). (Higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 07 Well being (SF-36). (Higher values are better)
Study Treatment Control Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Kerr 2003 26 63.90 (20.30) 20 57.50 (23.20) 6.40 [ -6.42, 19.22 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
Favours control Favours acupuncture
117Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.08. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 08 Side effects / Complications
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 08 Side effects / Complications
Study Treatment Control Risk Difference (Random) Risk Difference (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Carlsson 2001 0/34 0/16 0.0 [ -0.09, 0.09 ]
Leibing 2002 3/35 0/40 0.09 [ -0.02, 0.19 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
Carlsson 2001 0/21 0/6 0.0 [ -0.20, 0.20 ]
Lehmann 1986 0/13 0/13 0.0 [ -0.14, 0.14 ]
04 Long-term follow-up (more than 1 year)
-0.5 -0.25 0 0.25 0.5
Favours acupuncture Favours other interv
Analysis 06.09. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 09 pain (percent of baseline values)
Immediately after the end of the sessionsStudy
Short-term follow-up (up to 3 months after the end of the sessions)Study Group Follow-up Number of patients Percent of baseline Standard Deviation p value
Carlsson (even) Acupuncture 1 month 34 87% 32 0.003
Carlsson (even) Placebo 1 month 16 123% 46
Carlsson (morn) Acupuncture 1 month 34 88% 32 0.000
Carlsson (morn) Placebo 1 month 16 138% 40
Intermediate-term follow-up (3 months to 1 year)Study Group Follow-up Number of patients Percent of baseline Standard Deviation p value
Carlsson (even) Acupuncture 3 months 23 75% 34 0.007
Carlsson (even) Placebo 3 months 9 120% 50
Carlsson (morn) Acupuncture 3 months 23 76% 37 0.001
Carlsson (morn) Placebo 3 months 9 130% 39
118Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Long-term follow-up (more than 1 year)
Study Group Follow-up
Number of
patients Percent of baseline
Standard
Deviation p value
Carlsson (even) Acupuncture 6 months or longer 21 69% 31 0.056
Carlsson (even) Placebo 6 months or longer 6 100% 48
Carlsson (morn) Acupuncture 6 months or longer 21 76% 33 0.128
Carlsson (morn) Placebo 6 months or longer 6 133% 76
Analysis 06.10. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 10 sick leave
Long-term follow-upStudy Group Time Full time work Sick leave part-time Sick leave full time p value
Carlsson 2001 Acupuncture Baseline 7 6 8
Carlsson 2001 After 6 months 11 7 3 0.024
Carlsson 2001 Placebo Baseline 4 2 5
Carlsson 2001 After 6 months 5 1 5 0.655
Analysis 06.11. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 11 general level of pain (0-15 points)(more points mean less pain)
Immediately after the end of the sessionsStudy Group Value p value
Lehmann 1986 Acupuncture 10.59 F 2,50 = 1.66 (p<0.2)
Lehmann 1986 TENS 9.16
Lehmann 1986 Sham TENS 9.00
Short-term follow-up (up to 3 months after the end of the sessions)Study
Intermediate-term follow-up (3 months to 1 year)Study Group Value p value
Lehmann 1986 Acupuncture 11.08 F 2,41=3.57
p=0.04 (not adjusted for multiple comparisons).
p=0.1 (adjusted for multiple comparisons)
Lehmann 1986 TENS 8.28
Lehmann 1986 Sham TENS 7.94
119Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Long-term follow-up (more than 1 year)Study
Analysis 06.12. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 12 pain: difference between within group changes
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 12 pain: difference between within group changes
Study differences between (SE) differences between (Random) differences between (Random)
95% CI 95% CI
01 Immediately after the end of the sessions
Leibing 2002 -0.60 (0.54) -0.60 [ -1.66, 0.46 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 -0.10 (0.53) -0.10 [ -1.14, 0.94 ]
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
Favours acupuncture Favours control
Analysis 06.13. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 13 function: difference between within group changes
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 13 function: difference between within group changes
Study differences between (SE) differences between (Random) differences between (Random)
95% CI 95% CI
01 Immediately after the end of the sessions
Leibing 2002 -4.20 (2.96) -4.20 [ -10.00, 1.60 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 -0.50 (2.98) -0.50 [ -6.34, 5.34 ]
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
Favours acupuncture Favours control
120Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 06.14. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 14 Pain: percentage of patients with >50% pain reduction
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 14 Pain: percentage of patients with >50% pain reduction
Study Treatment Control Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Molsberger 2002 39/60 20/58 1.89 [ 1.26, 2.81 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
Molsberger 2002 36/47 12/41 2.62 [ 1.59, 4.32 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.1 0.2 0.5 1 2 5 10
Favours sham Favours acupuncture
Analysis 06.15. Comparison 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months),
Outcome 15 spine range of motion: difference between within group changes
Review: Acupuncture and dry-needling for low back pain
Comparison: 06 acupuncture versus placebo or sham intervention (Chronic LBP: > 3 months)
Outcome: 15 spine range of motion: difference between within group changes
Study difference between (SE) difference between (Random) difference between (Random)
95% CI 95% CI
01 Immediately after the end of the sessions
Leibing 2002 -3.50 (3.26) -3.50 [ -9.89, 2.89 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 -0.90 (3.19) -0.90 [ -7.15, 5.35 ]
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
Favours acupuncture Favours sham
121Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 07.01. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
01 pain (lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 07 acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome: 01 pain (lower values are better)
Study Acupuncture Other intervention Standardised Mean Difference (Random) Standardised Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Giles 1999 (manip) 16 5.10 (7.80) 32 2.50 (6.96) 0.35 [ -0.25, 0.96 ]
Giles 1999 (NSAID) 16 5.10 (7.80) 20 3.80 (4.81) 0.20 [ -0.46, 0.86 ]
Giles 2003 (manip) 33 7.00 (5.18) 35 3.00 (5.18) 0.76 [ 0.27, 1.26 ]
Giles 2003 (NSAID) 33 7.00 (5.18) 39 5.00 (3.70) 0.45 [ -0.02, 0.92 ]
Grant 1999 32 0.0 (0.0) 28 0.0 (0.0) Not estimable
02 Short-term follow-up (up to 3 months after the end of the sessions)
Cherkin 2001 (mass) 94 4.00 (0.40) 78 3.60 (0.30) 1.11 [ 0.79, 1.43 ]
Cherkin 2001 (sc) 94 4.00 (0.40) 90 4.60 (0.40) -1.49 [ -1.82, -1.17 ]
03 Intermediate-term follow-up (3 months to 1 year)
Cherkin 2001 (mass) 94 4.50 (0.40) 78 3.20 (0.40) 3.24 [ 2.78, 3.69 ]
Cherkin 2001 (sc) 94 4.50 (0.40) 90 3.80 (0.40) 1.74 [ 1.40, 2.08 ]
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours acupunctur favours other interv
122Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 07.03. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
03 back specific functional status (lower scores mean better). Ex: RDQ, Oswestry and Aberdeen
Review: Acupuncture and dry-needling for low back pain
Comparison: 07 acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome: 03 back specific functional status (lower scores mean better). Ex: RDQ, Oswestry and Aberdeen
Study Acupuncture Other intervention Standardised Mean Difference (Random) Standardised Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Giles 1999 (manip) 16 24.50 (26.60) 32 19.50 (30.74) 0.17 [ -0.43, 0.77 ]
Giles 1999 (NSAID) 16 24.50 (26.60) 20 20.00 (21.47) 0.18 [ -0.47, 0.84 ]
Giles 2003 (manip) 34 26.00 (20.70) 35 14.00 (24.40) 0.52 [ 0.04, 1.00 ]
Giles 2003 (NSAID) 34 26.00 (20.70) 40 32.00 (23.70) -0.27 [ -0.72, 0.19 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
Cherkin 2001 (mass) 94 7.90 (0.70) 78 6.30 (0.60) 2.43 [ 2.03, 2.82 ]
Cherkin 2001 (sc) 94 7.90 (0.70) 90 8.80 (0.70) -1.28 [ -1.60, -0.96 ]
03 Intermediate-term follow-up (3 months to 1 year)
Cherkin 2001 (mass) 94 8.00 (0.70) 78 6.80 (0.70) 1.71 [ 1.36, 2.06 ]
Cherkin 2001 (sc) 94 8.00 (0.70) 90 6.40 (0.70) 2.28 [ 1.90, 2.65 ]
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours acupunctur favours other interv
Analysis 07.04. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
04 back specific functional status (higher scores are better). Ex: Japan Orthopedic Association Score.
Review: Acupuncture and dry-needling for low back pain
Comparison: 07 acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome: 04 back specific functional status (higher scores are better). Ex: Japan Orthopedic Association Score.
Study Acupuncture Other intervention Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours acupuncture favours other interv
123Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 07.05. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
05 pain disability index (lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 07 acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome: 05 pain disability index (lower values are better)
Study Treatment Control Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
Favours acupuncture Favours other interv
Analysis 07.06. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
06 physical examination
Review: Acupuncture and dry-needling for low back pain
Comparison: 07 acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome: 06 physical examination
Study Acupuncture Other intervention Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
124Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 07.07. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
07 return to work (higher values mean better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 07 acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome: 07 return to work (higher values mean better)
Study Acupuncture Other intervention Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
Lehmann 1986 7/13 8/13 0.88 [ 0.45, 1.70 ]
04 Long-term follow-up (more than 1 year)
0.1 0.2 0.5 1 2 5 10
favours other interv favours acupuncture
Analysis 07.08. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
08 Side effects / Complications
Review: Acupuncture and dry-needling for low back pain
Comparison: 07 acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome: 08 Side effects / Complications
Study Treatment Control Risk Difference (Random) Risk Difference (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Giles 1999 (manip) 0/16 0/32 0.0 [ -0.09, 0.09 ]
Giles 1999 (NSAID) 0/16 3/20 -0.15 [ -0.33, 0.03 ]
Grant 1999 3/32 3/28 -0.01 [ -0.17, 0.14 ]
Tsukayama 2002 4/9 3/10 0.14 [ -0.29, 0.58 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
Cherkin 2001 (mass) 0/94 0/78 0.0 [ -0.02, 0.02 ]
Cherkin 2001 (sc) 0/94 0/90 0.0 [ -0.02, 0.02 ]
03 Intermediate-term follow-up (3 months to 1 year)
Cherkin 2001 (mass) 0/94 0/78 0.0 [ -0.02, 0.02 ]
Cherkin 2001 (sc) 0/94 0/90 0.0 [ -0.02, 0.02 ]
Lehmann 1986 0/13 0/13 0.0 [ -0.14, 0.14 ]
04 Long-term follow-up (more than 1 year)
-1 -0.5 0 0.5 1
Favours acupuncture Favours other interv
125Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 07.09. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
09 pain and function (adjusted for baseline values)
Immediately after the end of teh sessionsStudy Comparison Outcome measure Timing p value
Tsukayama 2002 Acupuncture versus TENS Functional status (JOA): higher scores are better Immediately after 0.24
Tsukayama 2002
Short-term follow-up (up to 3 months after the end of the sessions)Study Comparison Outcome measure Timing p value
Cherkin 2001 (mass) Acupuncture versus massage Pain 9 weeks 0.23
Cherkin 2001 (mass) Function 9 weeks 0.01 (massage is better)
Cherkin 2001 (sc) Acupuncture versus self-care education Pain 9 weeks 0.55
Cherkin 2001 (sc) Function 9 weeks 0.75
Intermediate-term follow-up (3 months to 1 year)Study Comparison Outcome measure Timing p value
Cherkin 2001 (mass) Acupuncture versus massage Pain 52 weeks 0.002 (massage is better)
Cherkin 2001 (mass) Function 52 weeks 0.05 (massage is better)
Cherkin 2001 (sc) Acupuncture versus self-care education Pain 52 weeks 0.10
Cherkin 2001 (sc) Function 52 weeks 0.10
Long-term follow-up (more than 1 year)Study
Analysis 07.10. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
10 general level of pain (0-15 points)(more points mean less pain)
Immediately after the end of the sessionsStudy Group Value p value
Lehmann 1986 Acupuncture 10.59 F 2,50 = 1.66 (p<0.2)
Lehmann 1986 TENS 9.16
Lehmann 1986 Sham TENS 9.00
Short-term follow-up (up to 3 months after the end of the sessions)Study
126Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Intermediate-term follow-up (3 months to 1 year)Study Group Value p value
Lehmann 1986 Acupuncture 11.08 F 2,41=3.57
p=0.04 (not adjusted for multiple comparisons).
p=0.1 (adjusted for multiple comparisons)
Lehmann 1986 TENS 8.28
Lehmann 1986 Sham TENS 7.94
Long-term follow-up (more than 1 year)Study
Analysis 07.11. Comparison 07 acupuncture versus other intervention. (Chronic LBP: > 3 months), Outcome
11 pain: difference between within group changes
Review: Acupuncture and dry-needling for low back pain
Comparison: 07 acupuncture versus other intervention. (Chronic LBP: > 3 months)
Outcome: 11 pain: difference between within group changes
Study differences between (SE) differences between (Random) differences between (Random)
95% CI 95% CI
01 Immediately after the end of the sessions
Tsukayama 2002 -2.10 (0.86) -2.10 [ -3.79, -0.41 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
Favours acupuncture Favours control
127Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 08.01. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 01
pain (lower values mean better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months)
Outcome: 01 pain (lower values mean better)
Study Technique 1 Technique 2 Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Ceccherelli 2002 21 14.54 (10.88) 21 22.25 (16.08) -7.71 [ -16.01, 0.59 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
Ceccherelli 2002 21 7.50 (12.94) 21 18.00 (17.16) -10.50 [ -19.69, -1.31 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
favours technique 1 favours technique 2
Analysis 08.02. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 02
Improvement (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months)
Outcome: 02 Improvement (higher values are better)
Study Technique 1 Technique 2 Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
Carlsson 2001 8/18 7/16 1.02 [ 0.48, 2.17 ]
03 Intermediate-term follow-up (3 months to 1 year)
Carlsson 2001 8/19 6/16 1.12 [ 0.49, 2.56 ]
04 Long-term follow-up (more than 1 year)
0.2 0.5 1 2 5
favours Technique 2 favours Technique 1
128Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 08.03. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 03
functional status
Review: Acupuncture and dry-needling for low back pain
Comparison: 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months)
Outcome: 03 functional status
Study Acupuncture Conventional tx Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
Analysis 08.04. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 04
physical examination
Review: Acupuncture and dry-needling for low back pain
Comparison: 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months)
Outcome: 04 physical examination
Study Acupuncture Conventional tx Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
Analysis 08.06. Comparison 08 acupuncture versus acupuncture. (Chronic LBP: > 3 months), Outcome 06
improvement
Immediately after the end of the sessionsStudy Improvement Technique 1: Regular Technique 2: Ancient p value
Ding 1998 Marked effective 4 8
Ding 1998 Improved 6 3
Ding 1998 No change 5 2
129Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Immediately after the end of the sessions (Continued )
Study Improvement Technique 1: Regular Technique 2: Ancient p value
Short-term follow-up (up to 3 months after the end of the sessions)Study Improvement Technique 1: Regular Technique 2: Ancient p value
Ding 1998 Cure 4 22 Chi-square=12.44
p<0.01
Ding 1998 Marked effective 4 8
Ding 1998 Improved 6 3
Ding 1998 No change 5 2
Intermediate-term follow-up (3 months to 1 year)Study
Long-term follow-up (more than 1 year)Study
Analysis 09.01. Comparison 09 dry-needling versus other intervention ((Sub)acute LBP < 3 months),
Outcome 01 global measure (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 09 dry-needling versus other intervention ((Sub)acute LBP < 3 months)
Outcome: 01 global measure (higher values are better)
Study Dry-needling Other intervention Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Gunn 1980 28/29 16/27 1.63 [ 1.18, 2.24 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
Garvey 1989 (lidoc) 11/20 4/13 1.79 [ 0.72, 4.43 ]
Garvey 1989 (spray) 11/20 8/16 1.10 [ 0.59, 2.07 ]
Garvey 1989(steroid) 11/20 5/14 1.54 [ 0.69, 3.45 ]
Gunn 1980 27/29 14/27 1.80 [ 1.23, 2.62 ]
03 Intermediate-term follow-up (3 months to 1 year)
Gunn 1980 21/21 14/23 1.64 [ 1.18, 2.28 ]
04 Long-term follow-up (more than 1 year)
0.1 0.2 0.5 1 2 5 10
Favours control Favours dry-needling
130Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 09.02. Comparison 09 dry-needling versus other intervention ((Sub)acute LBP < 3 months),
Outcome 02 Side effects / Complications
Review: Acupuncture and dry-needling for low back pain
Comparison: 09 dry-needling versus other intervention ((Sub)acute LBP < 3 months)
Outcome: 02 Side effects / Complications
Study Dry-needling Control Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
Garvey 1989 3/20 1/14 2.10 [ 0.24, 18.17 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.01 0.1 1 10 100
Favours dry-needling Favours other interv
Analysis 10.01. Comparison 10 acupuncture versus placebo or sham intervention (unknown / mixed duration
of low back pain), Outcome 01 pain (VAS): lower values are better
Review: Acupuncture and dry-needling for low back pain
Comparison: 10 acupuncture versus placebo or sham intervention (unknown / mixed duration of low back pain)
Outcome: 01 pain (VAS): lower values are better
Study Acupuncture placebo / sham Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Short term (immediately after end of sessions)
Inoue 2000 15 3.90 (2.60) 12 3.60 (2.10) 0.30 [ -1.47, 2.07 ]
Inoue 2001 10 3.73 (2.44) 11 6.41 (1.35) -2.68 [ -4.39, -0.97 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupuncture favours control
131Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 10.02. Comparison 10 acupuncture versus placebo or sham intervention (unknown / mixed duration
of low back pain), Outcome 02 global measure
Review: Acupuncture and dry-needling for low back pain
Comparison: 10 acupuncture versus placebo or sham intervention (unknown / mixed duration of low back pain)
Outcome: 02 global measure
Study Acupuncture placebo / sham Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
Von Mencke 1988 33/35 15/30 1.89 [ 1.31, 2.72 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.1 0.2 0.5 1 2 5 10
favours placebo/sham favours acupuncture
Analysis 10.03. Comparison 10 acupuncture versus placebo or sham intervention (unknown / mixed duration
of low back pain), Outcome 03 functional status (higher scores are better). Generic instrument
Review: Acupuncture and dry-needling for low back pain
Comparison: 10 acupuncture versus placebo or sham intervention (unknown / mixed duration of low back pain)
Outcome: 03 functional status (higher scores are better). Generic instrument
Study Acupuncture placebo / sham Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours control favours acupuncture
132Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 10.04. Comparison 10 acupuncture versus placebo or sham intervention (unknown / mixed duration
of low back pain), Outcome 04 physical examination (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 10 acupuncture versus placebo or sham intervention (unknown / mixed duration of low back pain)
Outcome: 04 physical examination (higher values are better)
Study Acupuncture placebo / sham Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours control favours acupuncture
Analysis 11.01. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back
pain), Outcome 01 pain score (lower values mean better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 11 acupuncture versus other intervention (unknown / mixed duration of low back pain)
Outcome: 01 pain score (lower values mean better)
Study Acupuncture Other intervention Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Sakai 1998 14 2.30 (1.50) 12 2.40 (1.50) -0.10 [ -1.26, 1.06 ]
Sakai 2001 31 5.30 (3.00) 33 5.90 (3.40) -0.60 [ -2.17, 0.97 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours acupuncture favours other interv
133Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 11.02. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back
pain), Outcome 02 pain recovery: higher values are better
Review: Acupuncture and dry-needling for low back pain
Comparison: 11 acupuncture versus other intervention (unknown / mixed duration of low back pain)
Outcome: 02 pain recovery: higher values are better
Study Acupuncture Other intervention Standardised Mean Difference (Random) Standardised Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Kurosu 1979(a) 10 0.86 (0.80) 10 1.18 (0.75) -0.40 [ -1.28, 0.49 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours other interv favours acupuncture
Analysis 11.03. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back
pain), Outcome 03 global measure (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 11 acupuncture versus other intervention (unknown / mixed duration of low back pain)
Outcome: 03 global measure (higher values are better)
Study Acupuncture Other intervention Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Sakai 2001 13/31 10/33 1.38 [ 0.71, 2.69 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.2 0.5 1 2 5
favours control favours acupuncture
134Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 11.04. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back
pain), Outcome 04 back specific functional status (higher scores are better). Ex: Japan Orthopedic Association
Score.
Review: Acupuncture and dry-needling for low back pain
Comparison: 11 acupuncture versus other intervention (unknown / mixed duration of low back pain)
Outcome: 04 back specific functional status (higher scores are better). Ex: Japan Orthopedic Association Score.
Study Acupuncture Other intervention Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Sakai 1998 14 12.10 (2.00) 12 13.30 (0.80) -1.20 [ -2.34, -0.06 ]
Sakai 2001 31 15.90 (2.00) 33 15.80 (2.60) 0.10 [ -1.03, 1.23 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours other interv favours acupuncture
Analysis 11.05. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back
pain), Outcome 05 physical examination
Review: Acupuncture and dry-needling for low back pain
Comparison: 11 acupuncture versus other intervention (unknown / mixed duration of low back pain)
Outcome: 05 physical examination
Study Acupuncture Other intervention Weighted Mean Difference (Fixed) Weighted Mean Difference (Fixed)
N
Mean(SD) N
Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours acupunctur favours control
135Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 11.07. Comparison 11 acupuncture versus other intervention (unknown / mixed duration of low back
pain), Outcome 07 Side effects / Complications
Review: Acupuncture and dry-needling for low back pain
Comparison: 11 acupuncture versus other intervention (unknown / mixed duration of low back pain)
Outcome: 07 Side effects / Complications
Study Treatment Control Risk Difference (Random) Risk Difference (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Sakai 2001 0/31 2/33 -0.06 [ -0.16, 0.04 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-0.5 -0.25 0 0.25 0.5
Favours acupuncture Favours control
Analysis 12.01. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back
pain), Outcome 01 pain (lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain)
Outcome: 01 pain (lower values are better)
Study Technique 1 Technique 2 Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Short term (immediately after end of sessions)
Takeda % Nabeta 2001 9 28.00 (24.30) 9 17.00 (20.90) 11.00 [ -9.94, 31.94 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
favours technique 1 favours technique 2
136Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 12.02. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back
pain), Outcome 02 pain recovery (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain)
Outcome: 02 pain recovery (higher values are better)
Study Techique 1 Technique 2 Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Kurosu 1979(b) 10 1.10 (0.83) 10 0.43 (0.39) 0.67 [ 0.10, 1.24 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-4 -2 0 2 4
favours technique 2 favours technique 1
Analysis 12.03. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back
pain), Outcome 03 global measure (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain)
Outcome: 03 global measure (higher values are better)
Study Technique 1 Technique 2 Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
02 Short-term follow-up (up to 3 months after the end of the sessions)
Wang 1996 239/246 175/246 1.37 [ 1.26, 1.48 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.5 0.7 1 1.5 2
favours technique 2 favours technique 1
137Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 12.04. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back
pain), Outcome 04 functional status (higher values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain)
Outcome: 04 functional status (higher values are better)
Study Technique 1 Technique 2 Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Takeda % Nabeta 2001 9 14.40 (1.60) 9 15.00 (1.40) -0.60 [ -1.99, 0.79 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours technique 2 favours technique 1
Analysis 12.05. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back
pain), Outcome 05 physical examination (finger-floor distance) Higher values are better.
Review: Acupuncture and dry-needling for low back pain
Comparison: 12 acupuncture versus acupuncture. (unknown / mixed duration of low back pain)
Outcome: 05 physical examination (finger-floor distance) Higher values are better.
Study Technique 1 Technique 2 Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Takeda % Nabeta 2001 9 14.30 (9.90) 9 18.00 (10.00) -3.70 [ -12.89, 5.49 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
favours technique 2 favours technique 1
Analysis 12.07. Comparison 12 acupuncture versus acupuncture. (unknown / mixed duration of low back
pain), Outcome 07 improvement
Immediately after the end of the sessionsStudy
138Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Short-term follow-up (up to 3 months after the end of the sessions)Study
Intermediate-term follow-up (3 months to 1 year)Study
Long-term follow-up (more than 1 year)Study Improvement Technique 1: Ac+cupp Technique 2: Acup p value
Li & Shang 1997 Cure 33 22 <0.01
Li & Shang 1997 Marked effective 32 28
Li & Shang 1997 Improved 13 26
Li & Shang 1997 No change 0 2
Analysis 13.01. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 01 pain (lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 01 pain (lower values are better)
Study Acup + intervention Intervention alone Standardised Mean Difference (Random) Weight Standardised Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Immediately after the end of the sessions
Leibing 2002 35 2.10 (2.20) 39 4.40 (1.70) 24.1 -1.17 [ -1.66, -0.67 ]
Meng 2003 24 1.50 (1.20) 23 2.40 (1.30) 17.7 -0.71 [ -1.30, -0.12 ]
Molsberger 2002 58 2.60 (2.10) 58 3.90 (2.10) 38.5 -0.61 [ -0.99, -0.24 ]
Yeung 2003 26 3.81 (2.10) 26 5.12 (2.18) 19.7 -0.60 [ -1.16, -0.05 ]
Subtotal (95% CI) 143 146 100.0 -0.76 [ -1.02, -0.50 ]
Test for heterogeneity chi-square=3.49 df=3 p=0.32 I² =14.2%
Test for overall effect z=5.69 p<0.00001
02 Short-term follow-up (up to 3 months after the end of the sessions)
Meng 2003 24 1.30 (0.80) 23 2.40 (1.00) 30.3 -1.20 [ -1.82, -0.57 ]
Molsberger 2002 47 2.30 (2.00) 36 5.20 (1.90) 36.4 -1.47 [ -1.96, -0.98 ]
Yeung 2003 26 3.77 (2.12) 26 5.19 (2.47) 33.3 -0.61 [ -1.16, -0.05 ]
Subtotal (95% CI) 97 85 100.0 -1.10 [ -1.62, -0.58 ]
Test for heterogeneity chi-square=5.24 df=2 p=0.07 I² =61.8%
-4 -2 0 2 4
favours acup + inter favours inter alone (Continued . . . )
139Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study Acup + intervention Intervention alone Standardised Mean Difference (Random) Weight Standardised Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Test for overall effect z=4.15 p=0.00003
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 33 3.10 (1.80) 30 4.50 (2.00) 55.1 -0.73 [ -1.24, -0.22 ]
Yeung 2003 26 3.46 (2.18) 26 5.27 (2.31) 44.9 -0.79 [ -1.36, -0.23 ]
Subtotal (95% CI) 59 56 100.0 -0.76 [ -1.14, -0.38 ]
Test for heterogeneity chi-square=0.03 df=1 p=0.87 I² =0.0%
Test for overall effect z=3.91 p=0.00009
04 Long-term follow-up (more than 1 year)
Subtotal (95% CI) 0 0 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
-4 -2 0 2 4
favours acup + inter favours inter alone
Analysis 13.02. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 02 pain: difference between within group changes
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 02 pain: difference between within group changes
Study differences between (SE) differences between (Random) Weight differences between (Random)
95% CI (%) 95% CI
01 Immediately after the end of the sessions
Leibing 2002 -1.70 (0.53) 42.9 -1.70 [ -2.74, -0.66 ]
Meng 2003 -0.60 (0.33) 57.1 -0.60 [ -1.25, 0.05 ]
Subtotal (95% CI) 100.0 -0.91 [ -1.46, -0.36 ]
Test for heterogeneity chi-square=3.10 df=1 p=0.08 I² =67.8%
Test for overall effect z=3.24 p=0.001
02 Short-term follow-up (up to 3 months after the end of the sessions)
Meng 2003 -0.70 (0.32) 100.0 -0.70 [ -1.33, -0.07 ]
Subtotal (95% CI) 100.0 -0.70 [ -1.33, -0.07 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.19 p=0.03
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 -0.80 (0.51) 100.0 -0.80 [ -1.80, 0.20 ]
-4 -2 0 2 4
Favours acup + inter Favours interv alone (Continued . . . )
140Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study differences between (SE) differences between (Random) Weight differences between (Random)
95% CI (%) 95% CI
Subtotal (95% CI) 100.0 -0.80 [ -1.80, 0.20 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.57 p=0.1
04 Long-term follow-up (more than 1 year)
Subtotal (95% CI) 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
-4 -2 0 2 4
Favours acup + inter Favours interv alone
Analysis 13.03. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 03 pain disability index (lower values are better)
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 03 pain disability index (lower values are better)
Study Acup + interv Interv alone Weighted Mean Difference (Random) Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI 95% CI
01 Immediately after the end of the sessions
Leibing 2002 40 11.30 (15.00) 46 22.30 (7.80) -11.00 [ -16.17, -5.83 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 40 16.20 (12.50) 46 22.60 (10.00) -6.40 [ -11.23, -1.57 ]
04 Long-term follow-up (more than 1 year)
-100 -50 0 50 100
Favours acup + inter Favours interv alone
141Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 13.04. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 04 Pain: percentage of patients with >50% pain reduction
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 04 Pain: percentage of patients with >50% pain reduction
Study Acup + intervention Intervention alone Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Molsberger 2002 39/60 23/53 1.50 [ 1.05, 2.15 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
Molsberger 2002 36/47 5/36 5.51 [ 2.41, 12.63 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.1 0.2 0.5 1 2 5 10
Favours interv alone Favours acup + inter
Analysis 13.05. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 05 function: difference between within group changes
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 05 function: difference between within group changes
Study differences between (SE) differences between (Random) Weight differences between (Random)
95% CI (%) 95% CI
01 Immediately after the end of the sessions
Leibing 2002 -11.30 (2.95) 44.9 -11.30 [ -17.08, -5.52 ]
Meng 2003 -2.60 (0.98) 55.1 -2.60 [ -4.52, -0.68 ]
Subtotal (95% CI) 100.0 -3.46 [ -5.29, -1.64 ]
Test for heterogeneity chi-square=7.83 df=1 p=0.005 I² =87.2%
Test for overall effect z=3.73 p=0.0002
02 Short-term follow-up (up to 3 months after the end of the sessions)
Meng 2003 -3.10 (1.10) 100.0 -3.10 [ -5.26, -0.94 ]
Subtotal (95% CI) 100.0 -3.10 [ -5.26, -0.94 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.82 p=0.005
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 -6.80 (2.96) 100.0 -6.80 [ -12.60, -1.00 ]
Subtotal (95% CI) 100.0 -6.80 [ -12.60, -1.00 ]
-100 -50 0 50 100
Favours acup + inter Favours interv alone (Continued . . . )
142Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study differences between (SE) differences between (Random) Weight differences between (Random)
95% CI (%) 95% CI
Test for heterogeneity: not applicable
Test for overall effect z=2.30 p=0.02
04 Long-term follow-up (more than 1 year)
Subtotal (95% CI) 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
-100 -50 0 50 100
Favours acup + inter Favours interv alone
Analysis 13.06. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 06 global measure
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 06 global measure
Study Acup + interv Intervention alone Relative Risk (Random) Relative Risk (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Molsberger 2002 52/62 31/55 1.49 [ 1.15, 1.92 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
Molsberger 2002 36/49 11/37 2.47 [ 1.46, 4.17 ]
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
0.1 0.2 0.5 1 2 5 10
favours interv alone favours acup + inter
143Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 13.07. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 07 back specific functional status (lower scores mean better). Ex: RDQ, Oswestry and
Aberdeen
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 07 back specific functional status (lower scores mean better). Ex: RDQ, Oswestry and Aberdeen
Study Acup + intervention Intervention alone Standardised Mean Difference (Random) Weight Standardised Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Immediately after the end of the sessions
Leibing 2002 35 11.30 (15.00) 39 22.30 (7.80) 43.0 -0.93 [ -1.41, -0.44 ]
Meng 2003 24 6.50 (4.00) 23 11.20 (4.80) 26.5 -1.05 [ -1.66, -0.43 ]
Yeung 2003 26 20.02 (10.47) 26 30.82 (13.03) 30.4 -0.90 [ -1.47, -0.33 ]
Subtotal (95% CI) 85 88 100.0 -0.95 [ -1.27, -0.63 ]
Test for heterogeneity chi-square=0.14 df=2 p=0.93 I² =0.0%
Test for overall effect z=5.90 p<0.00001
02 Short-term follow-up (up to 3 months after the end of the sessions)
Meng 2003 24 6.30 (4.40) 23 11.40 (4.80) 46.0 -1.09 [ -1.71, -0.47 ]
Yeung 2003 26 20.36 (13.06) 26 32.48 (15.31) 54.0 -0.84 [ -1.41, -0.27 ]
Subtotal (95% CI) 50 49 100.0 -0.95 [ -1.37, -0.54 ]
Test for heterogeneity chi-square=0.34 df=1 p=0.56 I² =0.0%
Test for overall effect z=4.47 p<0.00001
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 33 16.20 (12.50) 30 22.60 (10.00) 54.7 -0.56 [ -1.06, -0.05 ]
Yeung 2003 26 19.36 (10.12) 26 25.82 (13.11) 45.3 -0.54 [ -1.10, 0.01 ]
Subtotal (95% CI) 59 56 100.0 -0.55 [ -0.92, -0.18 ]
Test for heterogeneity chi-square=0.00 df=1 p=0.97 I² =0.0%
Test for overall effect z=2.89 p=0.004
04 Long-term follow-up (more than 1 year)
Subtotal (95% CI) 0 0 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
-4 -2 0 2 4
favours acup + inter favours interv alone
144Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 13.08. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 08 spine range of motion: difference between within group changes
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 08 spine range of motion: difference between within group changes
Study difference between (SE) difference between (Random) difference between (Random)
95% CI 95% CI
01 Immediately after the end of the sessions
Leibing 2002 -4.50 (3.26) -4.50 [ -10.89, 1.89 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
Leibing 2002 -4.70 (3.19) -4.70 [ -10.95, 1.55 ]
04 Long-term follow-up (more than 1 year)
-10 -5 0 5 10
Favours acup + inter Favours interv alone
Analysis 13.09. Comparison 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP:
> 3 months), Outcome 09 Side effects / Complications
Review: Acupuncture and dry-needling for low back pain
Comparison: 13 acupuncture plus intervention versus other intervention alone. (Chronic LBP: > 3 months)
Outcome: 09 Side effects / Complications
Study Acupuncture + interv Intervention alone Risk Difference (Random) Risk Difference (Random)
n/N n/N 95% CI 95% CI
01 Immediately after the end of the sessions
Leibing 2002 3/35 0/39 0.09 [ -0.02, 0.19 ]
Yeung 2003 0/26 0/26 0.0 [ -0.07, 0.07 ]
02 Short-term follow-up (up to 3 months after the end of the sessions)
03 Intermediate-term follow-up (3 months to 1 year)
04 Long-term follow-up (more than 1 year)
-1 -0.5 0 0.5 1
Favours acup + inter Favours interv alone
145Acupuncture and dry-needling for low back pain (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd





























