Embed Size (px)
Citation preview
Respiratory Medicine (2013) 107, 1740e1747
Available online at www.sciencedirect.com
journal homepage: www.elsevier .com/locate /rmed
Functional and psychological variables bothaffect daily physical activity in COPD: Astructural equations model
Wytske A. Altenburg a,b,d,*, Linda Bossenbroek a,d,Mathieu H.G. de Greef c, Huib A.M. Kerstjens a,d,Nick H.T. ten Hacken a,d, Johan B. Wempe a,b,d
aUniversity of Groningen, University Medical Center Groningen, Department of Pulmonary Diseases,P.O. Box 30001, Internal Mail Address AA11, 9700 RB Groningen, The NetherlandsbUniversity of Groningen, University Medical Center Groningen, Center for Rehabilitation, Groningen,P.O. Box 30002, Internal Mail Address CD24, 9750 RA Haren, The NetherlandscUniversity of Groningen, University Medical Center Groningen, Institute of Human MovementSciences, P.O. Box 196, 9700AD Groningen, The NetherlandsdUniversity of Groningen, University Medical Center Groningen, Groningen Research Institute forAsthma and COPD, P.O. Box 30001, Internal Mail Address FA40, 9700RB Groningen, The Netherlands
Received 15 February 2013; accepted 2 June 2013Available online 28 June 2013
KEYWORDSCOPD;Physical activity;Functional capacity;Psychologicalcapacity;Structural equationsmodel
Abbreviations: 6MWD, six-minute walkDutch Exertion and Fatigue Scale; DPARestriction Scale; GOLD, global initiaquartile range; PPAS, Perceived PhysicRV%TLC, residual volume as percentagRespiratory Questionnaire; SPSS, Scieoxygen uptake.* Corresponding author. University o
30002, Internal Mail Address CD24, 97E-mail address: w.a.altenburg@cv
0954-6111/$ - see front matter ª 201http://dx.doi.org/10.1016/j.rmed.20
Summary
Background: Daily physical activity (DPA) level is reduced in patients with COPD. The aim ofthis study was to investigate the association of DPA with functional and psychological variablesin these patients.Methods: 155 COPD patients (102 males, median (IQR) age 62 years (54e69 years), predictedFEV1 60% (40e75%) were included. We assessed DPA (DigiWalker SW-200), functional capacityand psychological factors.Results: DPA level was significantly associated with all functional capacity variables and twopsychological variables (Perceived Physical Ability Subscale, depression subscale of the
ing distance; CCQ, Clinical COPD Questionnaire; COPD, chronic obstructive pulmonary disease; DEFS,, daily physical activity; FEV1, Forced Expiration Volume in one second; GARS, Groningen Activity andtive for chronic obstructive lung disease; HADS, Hospital Anxiety and Depression Scale; IQR, inter-al Ability Subscale; PR, pulmonary rehabilitation; RMSEA, root mean square error of approximation;e of total lung capacity; SEM, structural equations modeling; SF-36, Short Form 36; SGRQ, St. Georgentific Package of Social Sciences; SRQ-E, Self-Regulation Questionnaire for Exercise; VO2peak, peak
f Groningen, University Medical Center Groningen, Center for Rehabilitation, Groningen, P.O. Box50 RA Haren, The Netherlands. Tel.: þ31 (0)50 3614853; fax: þ31 (0)50 3619320.r.umcg.nl (W.A. Altenburg).
3 Elsevier Ltd. All rights reserved.13.06.002

Variables affecting physical activity in COPD 1741
Hospital Anxiety and Depression Scale). The six-minute walking distance and St. George Respi-ratory Questionnaire activity score explained 37% of the variance of DPA in a regression anal-ysis. A structural equations model revealed that psychological variables indirectly explainedDPA through functional capacity variables. DPA was stronger associated with functional capac-ity variables and weaker with psychological variables in patients with lower functional statusthan in patients with higher functional status.Conclusions: Higher levels of DPA are associated with better functional capacity, but interest-ingly, DPA is also affected by psychological factors, though only indirectly, via functional ca-pacity. The effect of specific treatment addressing psychological factors on DPA level andexercise tolerance needs further investigation. Clinical Trial Registration: ClinicalTrials.gov,NCT00614796.ª 2013 Elsevier Ltd. All rights reserved.
Introduction
Patients with COPD may enter a vicious circle of reducedlung function, activity-induced dyspnea, immobilization,muscle deconditioning and muscle fatigue. In addition,psychosocial consequences like depression and socialisolation may appear (www.goldcopd.com). This viciouscircle may affect daily physical activity level (DPA) in COPDpatients, assessed using accelerometers [1e6] and [7,8]pedometers. Lower DPA level is related to lower FEV1
[1e3,7,8], VO2peak [1,4,5] and 6MWD [1e6]. In addition, avery low DPA level was associated with a higher risk for all-cause and respiratory mortality [9e12]. The association ofDPA with psychological variables such as anxiety, depres-sion, self-efficacy and motivation has not been investigatedextensively; depression was not associated with DPA levelin two studies [6,13], whereas self-efficacy has been shownto correlate positively with DPA [3,14]. In addition, DPAcounseling has been shown to improve intrinsic motivationfor physical activity [15]. We hypothesized that variablesreflecting functional capacity as well as psychological var-iables influence DPA. In addition, we hypothesize thatvariables reflecting functional capacity affect DPA more inpatients with a low functional status and psychologicalaffect DPA more in patients with high functional status. Toinvestigate this a broad group of COPD patients is includedfrom the primary (general practitioner), secondary (hospi-tal outpatient clinic) and tertiary (pulmonary rehabilitationcentre) healthcare setting.
As we were interested in both direct and indirect re-lationships between DPA, functional and psychologicalvariables, we performed, in contrast to previous studies[1e8], a path analysis using the structural equationsmodeling (SEM) technique, which allows estimation ofdirect and indirect associations of groups of variables.
Methods
Subjects
Patients with stable COPD (n Z 155) from seven generalpractices, four hospital outpatient clinics and one pulmo-nary rehabilitation centre were included. These patientsparticipated in a controlled study of a physical activity
counseling program. Inclusion criteria were diagnosis ofCOPD according to the GOLD criteria [16] and age between40 and 80 years. Exclusion criteria were significant comor-bidities interfering with physical activity and exacerbationor respiratory tract infection in the past two months. Allpatients signed a written informed consent. The study wasapproved by the local medical ethics committee of theUniversity Medical Center Groningen (METc2006/143) andregistered in ClinicalTrials.gov: NCT00614796.
Measurements
Performance-based daily physical activityPerformance-based DPA (steps/day) was measured with theDigiwalker SW-200 pedometer (Yamax; Tokyo, Japan),which is an accurate measurement tool to detect stepstaken [17e20]. Patients were instructed to wear thepedometer during two weeks (from waking up until going tobed) and to record the number of steps per day in a diary.The mean of the last week of steps was used for furtheranalyses. Data from this week were only used when morethan 5 days of 7 were filled out.
Physiological characteristicsWeight, height and fat-free mass were measured, the latterby a bioelectrical impedance analysis (Bodystat 1500) [21].
Functional capacityPerformance-based functional capacity was assessed bylung function using a spirometer (Jaeger MS-IOS) and bodyplethysmograph (Masterlab version 4.52i) according tostandardized guidelines [22]. Reference values used werethose of the European Community for Coal and Steel [22].The six-minute walking distance (6MWD) was used to assessfunctional exercise capacity and was performed in accor-dance with international standards [23].
Self-reported functional capacity was assessed by mul-tiple questionnaires. Independent functioning in daily livingwas assessed by the Groningen Activity Restriction Scale(GARS) [24]. Disease specific health-related quality of lifewas assessed by the St. George Respiratory Questionnaire(SGRQ) [25]. The domains of this questionnaire containingitems about functional capacity (activity and impactsscales) were selected for further analysis. Health statuswas assessed by the Short Form 36 (SF-36) (general) and

1742 W.A. Altenburg et al.
Clinical COPD Questionnaire (CCQ) (disease specific)[26,27]. The physical functioning scale (SF-36) and func-tional status scale (CCQ) were used for further analysis.Fatigue due to daily activities in household, body care andsocial activities were measured with the Dutch Exertion andFatigue Scale (DEFS) [28].
Psychological capacityAnxiety and depression were measured with the HospitalAnxiety and Depression Scale (HADS) [29]. Self-efficacy wasmeasured by the Perceived Physical Ability Subscale (PPAS)of the physical self-efficacy scale [30].
The level of intrinsic motivation for physical activity wasmeasured using the Self-Regulation Questionnaire for Ex-ercise (SRQ-E). This questionnaire deals with the reasonwhy a person engages in physical activities and is based onthe format of Ryan and Connell [31].
Table 1 Baseline characteristics (n Z 155).
Clinical characteristics
Age, years 62 (54e69)Gender, m/f 102/53Healthcare setting,GP/outpatient cl./PR (n)
48/46/61
Medication (n)Short acting beta agonist 43Short acting muscarinicantagonist
35
Long acting beta agonist 21Long acting muscarinicantagonist
83
ICS 32Combination (ICS þ longacting beta agonist)
99
Packyears 33 (17e50)BMI, kg/m2 26.1 (22.8e29.0)FFMI, kg/m2 17.4 (16.1e18.9)FEV1, % pred 60 (40e75)FEV1%FVC, % 45 (34e59)RV%TLC, % 47 (41e54)6MWD, m 452 (360e515)DPA, steps/day 4206 (2387e6284)
Values are presented as median (IQR) unless otherwise indi-cated.GP: general practice; PR: pulmonary rehabilitation; ICS: inhaledcorticosteroids; FEV1: Forced Expiration Volume in one second;BMI: body mass index; 6MWD: six-minute walking distance; DPA:daily physical activity.
Statistical analysis
Univariate and multivariate analysisBecause of non-normal distribution of the primary outcomemeasure steps/day, Spearman’s correlations of DPA withpsychological and functional variableswere calculated in thetotal group and in 2 subgroups based on functional statusmeasured by the 6MWD (split by the median of 6MWD).
Multiple linear regression models (method stepwise)were constructed including 1) all variables (functional andpsychological) that correlated significantly with steps/day,and 2) only psychological variables (anxiety, depression,self-efficacy and motivation). These statistical analyseswere performed using Scientific Package of Social Sciences(SPSS) version 18.0. To test the null hypothesis alpha wasset at 0.05.
Structural equations modelA path analysis (LISREL 8.7) was used to test the hypothe-sized model, in which the direct effects of functional var-iables on DPA and simultaneously the indirect effects ofpsychological variables on DPA mediated through functionalvariables were estimated.
In this model latent constructs were conceptualized by‘DPA’, ‘functional capacity’ and ‘psychological capacity’.DPA was a latent construct estimated by taking the naturallogarithm of steps/day. Indicators of the latent construct‘functional capacity’ were performance-based (FEV1,6MWD) and self-reported (GARS, SGRQ activity and impacts,SF-36 physical functioning, CCQ functional and DEFS)functional capacity. The latent construct ‘psychologicalcapacity’ was indicated by HADS anxiety, HADS depression,SRQ-E and PPAS. Variables were chosen based on theirsignificant correlation with DPA in the univariate analysis orbecause they were thought to be interesting from a theo-retical point of view. Of the lung function variables onlyFEV1 was used, and not RV%TLC because both variableswere highly associated with each other, but FEV1 had ahigher correlation with DPA. To allow for mutual compari-sons between path coefficients, the completely standard-ized solution was used. For model fit we used multiplecriteria as suggested by Bentler and Bonett [32]. The firstcriterion used for model fit is a non-significant c2 indicating
that a non-significant amount of variance in the data re-mains unexplained. However, a statistically significant c2
can often be produced as an artifact of sample size and ofsmall variations in the data [33]. The second criterion is theratio of c2 to the degree of freedom, a ratio ranging from 2to 5 has been recommended as acceptable for good modelfit [34,35]. The last criterion used is the root mean squareerror of approximation (RMSEA), which assesses how wellthe model approximates the data by determining the lackof fit of the model to the population covariance matrix,expressed as the discrepancy per degree of freedom [36].An RMSEA with values of less than 0.05 indicates a good fitto the data although values up to 0.08 are acceptable aswell [36]. However, values greater than 0.10 strongly sug-gest an unsatisfactory model fit [37].
Results
Data from 155 patients with COPD from GOLD stage I(n Z 32), II (n Z 65), III (n Z 38) and IV (n Z 20) were usedfor all analyses. The median (IQR) DPA level for the totalgroup was 4206 (2387e6284) steps/day (Table 1). Baselinescores of the questionnaires are shown in Table 2.
Correlations
Spearman’s correlations for all variables with DPA areshown in Table 3. Correlations of functional variables with

Table 2 Baseline questionnaire scores.
GARS total score 23 (18e33)SF-36 physical functioning 21 (16e26)SF-36 social functioning 8 (7e10)SF-36 physical role 6 (4e8)SF-36 emotional role 6 (5e6)SF-36 mental health 25 (21e27)SF-36 vitality 16 (13e18)SF-36 pain 50 (44e60)SF-36 general health perception 13 (10e16)SF-36 health change 4 (3e4)CCQ symptoms 2.0 (1.3e2.8)CCQ functional 1.3 (0.5e2.8)CCQ mental 0.0 (0.0e0.5)CCQ total 1.4 (0.8e2.2)SGRQ symptoms 56 (36e70)SGRQ activity 59 (30e79)SGRQ impacts 26 (11e40)SGRQ total 40 (22e54)DEFS total score 3 (1e7)PPAS total score 30 (24e35)HADS anxiety 5 (3e8)HADS depression 4 (2e6)SRQ-E 10.1 (6.8e12.8)
Values are presented as median (IQR).GARS: Groningen Activity Restriction Scale; SF-36: Short Form36; CCQ: Clinical COPD Questionnaire; SGRQ: St. George Res-piratory Questionnaire; DEFS: Dutch Exertion and Fatigue Scale;PPAS: Perceived Physical Ability Subscale of the physical self-efficacy scale (Dutch version); HADS: Hospital Anxiety andDepression Scale; SRQ-E: Self-Regulation Questionnaire for Ex-ercise.
Table 3 Spearman’s correlations of DPA with functionaland psychological variables.
DPA (steps/day)
FEV1, l 0.418b
RV%TLC, % 0.253b
6MWD, m 0.627b
GARS total �0.530b
SF-36 physical functioning 0.477b
SGRQ activity �0.565b
SGRQ impacts �0.405b
CCQ functional �0.510b
DEFS �0.509b
PPAS 0.410b
HADS anxiety �0.156HADS depression �0.191a
SRQ-E �0.005
FEV1: Forced Expiration Volume in one second; DPA: dailyphysical activity; 6MWD: six-minute walking distance; GARS:Groningen Activity Restriction Scale; SF-36: Short Form 36;SGRQ: St. George Respiratory Questionnaire; CCQ: ClinicalCOPD Questionnaire; DEFS: Dutch Exertion and Fatigue Scale;PPAS: Perceived Physical Ability Subscale of the physical self-efficacy scale (Dutch version); HADS: Hospital Anxiety andDepression Scale; SRQ-E: Self-Regulation Questionnaire forExercise.a Correlation is significant at the 0.05 level (2-tailed).b Correlation is significant at the 0.01 level (2-tailed).
Variables affecting physical activity in COPD 1743
psychological variables are shown in the Supplementarymaterial. In general, patients with low functional statusshow weaker associations of DPA with psychological factors(anxiety, depression, self-efficacy; all rho’s �0.20 and non-significant) and stronger associations of DPA with variablesreflecting functional capacity (except SGRQ impacts allrho’s >0.20, all p < 0.05) (Table 4). For patients with higherfunctional status associations of DPA with psychologicalvariables are significant for self-efficacy and depression. Inaddition, in patients with higher functional status, less ofthe variables reflecting functional capacity are significantlyassociated with DPA than in patients with low functionalstatus (only 6MWD, SGRQ activity, CCQ function and DEFS).
Regression analyses
In the stepwise multiple linear regression model 6MWD andSGRQ activity were predictors of DPA (Table 5). The modelexplains 37% of the variance, in which psychological vari-ables did not contribute significantly. To further assess thecontribution of psychological factors on DPA we performeda stepwise multiple linear regression containing only thepsychological variables (Table 6). This model explains 16%of the variance with only PPAS (self-efficacy) as a significantindependent predicting variable.
Structural equations model
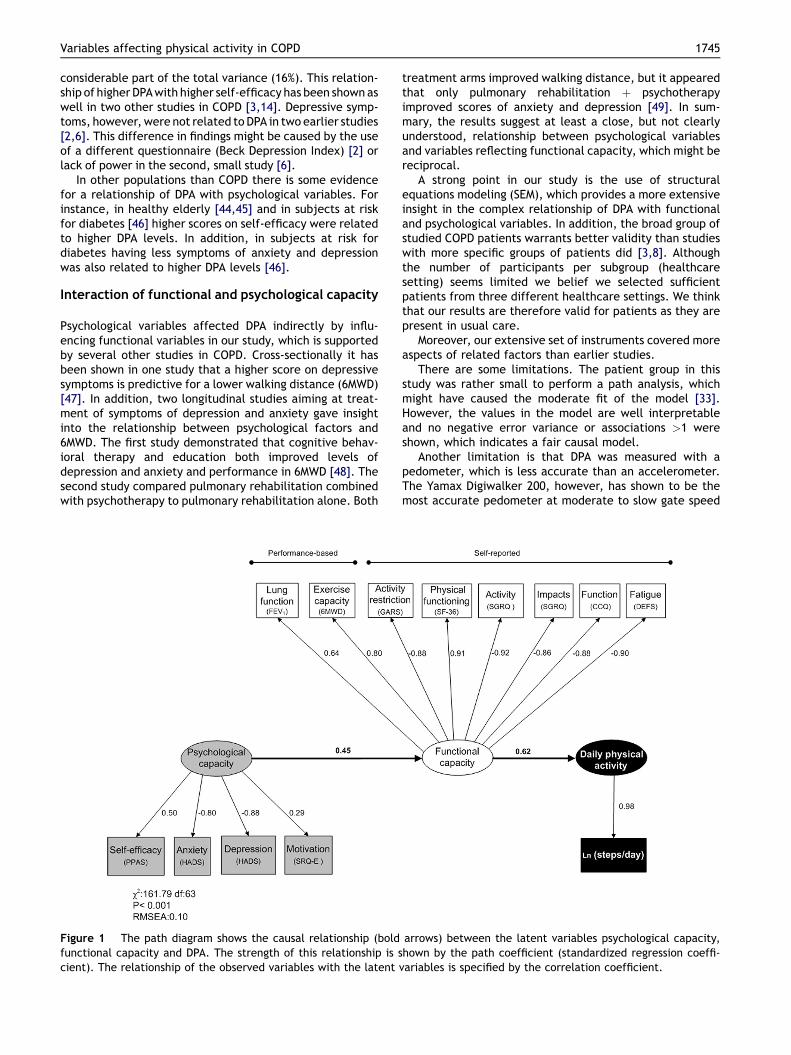
Based on the results of the regression analyses we hy-pothesized that psychological variables might indirectlyaffect DPA by affecting variables reflecting functional ca-pacity. Path coefficients (standardized regression co-efficients) are shown in Fig. 1 indicating a possible causallinkage between the latent variables psychological capacityand functional capacity (0.45) and between the latentvariable functional capacity and steps/day (0.62). Analysisof the model fit shows a c2 Z 161.8, (df Z 63); p < 0.001and RMSEA Z 0.10. The model shows a clear, but indirect,association between psychological variables and DPA. Amodel with a direct association of psychological capacitywith DPA was tested as well, but this association was verylow and not significant. The fit of the model meets thecriteria of the relative normed c2 (c2/df) of Wheaton et al.and the criteria of the RSMEA [34,35].
Discussion
DPA level in our COPD population was low, with a median(IQR) of 4206 (2387e6284) steps per day, which is consideredto be sedentary [38]. In the univariate analysis, DPA wassignificantly associated with variables reflecting functionalcapacity (performance-based and self-reported), and withpsychological variables (depression and self-efficacy). Whensubjects were divided in having lower or higher functionalstatus, DPA in patients with a lower functional status showedsignificant associations with seven of the variables reflectingfunctional capacity (i.e. FEV1, 6MWD, GARS total, SF-36physical function, SGRQ activity, CCQ function and DEFS),

Table 4 Correlations of DPA for low and high functionalstatus separately.
Low functionalstatus(6MWD <452)
High functionalstatus(6MWD �452)
DPA(steps/day)
p DPA(steps/day)
p
FEV1, l 0.312 0.009 0.137 0.2476MWD, m 0.454 0.000 0.375 0.001
GARS total L0.344 0.004 �0.228 0.053SF-36 physicalfunction
0.287 0.017 0.151 0.199
SGRQ activity L0.288 0.016 L0.357 0.002
SGRQ impacts �0.091 0.481 �0.181 0.129CCQ function L0.247 0.038 L0.251 0.032
DEFS L0.260 0.035 L0.296 0.011
PPAS 0.201 0.101 0.393 0.001
HADS anxiety �0.154 0.209 �0.219 0.061HADSdepression
�0.033 0.791 L0.283 0.015
SRQ-E 0.091 0.459 0.075 0.530
p-values <0.05 printed bold.FEV1: Forced Expiration Volume in one second; DPA: dailyphysical activity; 6MWD: six-minute walking distance; GARS:Groningen Activity Restriction Scale; SF-36: Short Form 36;SGRQ: St. George Respiratory Questionnaire; CCQ: ClinicalCOPD Questionnaire; DEFS: Dutch Exertion and Fatigue Scale;PPAS: Perceived Physical Ability Subscale of the physical self-efficacy scale (Dutch version); HADS: Hospital Anxiety andDepression Scale; SRQ-E: Self-Regulation Questionnaire for Ex-ercise.
Table 6 Resulting multiple regression model for explain-ing DPA from psychological variables (method stepwise).
Unstandardizedcoefficients
Standardizedcoefficients
t Sig.
B Std. error Beta
Constant 557.866 855.313 0.652 0.515PPAS 143.131 24.604 0.400 5.185 0.000
R2 Z 0.16, adjusted R2 Z 0.15.PPAS: Perceived Physical Ability Subscale of the physical self-efficacy scale (Dutch version).
1744 W.A. Altenburg et al.
whereas DPA in patients with a higher functional statusshowed significant associations with only four of these vari-ables (i.e. 6MWD, SGRQ activity, CCQ function and DEFS). Inaddition, DPA in patients with a higher functional status wassignificantly associatedwith twopsychological variables (i.e.self-efficacy and depression), which was not found in pa-tients with low functional status.
Multivariate analysis showed only two significant vari-ables, both reflecting functional capacity (6MWD and SGRQactivity) explaining 37% of the variance of DPA. However,the structural equations model (SEM) suggests that
Table 5 Resulting multiple regression model for explain-ing DPA from functional and psychological variables(method stepwise).
Unstandardizedcoefficients
Standardizedcoefficients
t Sig.
B Std. error Beta
Constant 2703.165 1329.575 2.033 0.0446MWD, m 7.899 2.053 0.378 3.848 0.000SGRQactivity
�0.016 9.706 �0.275 �2.801 0.006
R2 Z 0.37, adjusted R2 Z 0.36.6MWD: six-minute walking distance; SGRQ: St. George Respira-tory Questionnaire.
psychological variables indeed do contribute to DPA, butindirectly, through an effect on variables reflecting func-tional capacity.
Functional capacity and daily physical activity
The observed associations of DPA with variables reflectingfunctional capacity in the regression analyses and struc-tural equations model are in line with other studies in COPDshowing a relationship of higher DPA with higher FEV1
[1e3,7,8,14] higher general quality of life (SF-36) [3,6], andhigher disease specific quality of life (SGRQ and CCQ)[4,8,14]. The 6MWD, which explained the largest part of thevariance in our multiple regression model, was also foundto be a determining factor in three other studies [1,3,4].We hypothesize that the relationship between functionalcapacity and DPA is reciprocal: better functional capacityindeed enables a higher DPA level, but on the other hand ahigher DPA level will lead to better functional capacity.
The relationship of DPA with variables reflecting func-tional capacity has also been demonstrated in other pop-ulations. For example, a moderate positive association ofDPA with peak exercise VO2 has been shown in healthysubjects [18], and in patients with diabetes mellitus [39]. Inpatients with heart failure a higher 6MWD was associatedwith higher DPA level [40]. In our study, DPA was negativelyassociated with disability (GARS), which has to our knowl-edge not been reported before. In addition, fatigue (DEFS)was negatively associated with DPA, which has been foundas well in one other study in COPD [41]. Fatigue is partic-ularly interesting as it is increasingly recognized as animportant outcome in COPD [42] and other populations,such as frail elderly [43]. Fatigue may negatively affect DPAlevel, which leads to deconditioning and consequentlycontributes to the vicious circle of dyspnea and fatigue.
Psychological capacity and daily physical activity
The relationship of DPAwith psychological factors in COPD isless clear than the relationship with variables reflectingfunctional capacity. In our study, having higher self-efficacyand less depressive symptoms were associated with higherDPA. However, self-efficacy and depressive symptoms werenot independent determinants of DPA in a multiple regres-sion model which also included variables reflecting func-tional capacity. Nevertheless, in a model that included onlypsychological variables, self-efficacy explained a
Variables affecting physical activity in COPD 1745
considerable part of the total variance (16%). This relation-ship of higher DPAwith higher self-efficacy has been shownaswell in two other studies in COPD [3,14]. Depressive symp-toms, however,were not related to DPA in two earlier studies[2,6]. This difference in findings might be caused by the useof a different questionnaire (Beck Depression Index) [2] orlack of power in the second, small study [6].
In other populations than COPD there is some evidencefor a relationship of DPA with psychological variables. Forinstance, in healthy elderly [44,45] and in subjects at riskfor diabetes [46] higher scores on self-efficacy were relatedto higher DPA levels. In addition, in subjects at risk fordiabetes having less symptoms of anxiety and depressionwas also related to higher DPA levels [46].
Interaction of functional and psychological capacity
Psychological variables affected DPA indirectly by influ-encing functional variables in our study, which is supportedby several other studies in COPD. Cross-sectionally it hasbeen shown in one study that a higher score on depressivesymptoms is predictive for a lower walking distance (6MWD)[47]. In addition, two longitudinal studies aiming at treat-ment of symptoms of depression and anxiety gave insightinto the relationship between psychological factors and6MWD. The first study demonstrated that cognitive behav-ioral therapy and education both improved levels ofdepression and anxiety and performance in 6MWD [48]. Thesecond study compared pulmonary rehabilitation combinedwith psychotherapy to pulmonary rehabilitation alone. Both
Figure 1 The path diagram shows the causal relationship (boldfunctional capacity and DPA. The strength of this relationship is scient). The relationship of the observed variables with the latent v
treatment arms improved walking distance, but it appearedthat only pulmonary rehabilitation þ psychotherapyimproved scores of anxiety and depression [49]. In sum-mary, the results suggest at least a close, but not clearlyunderstood, relationship between psychological variablesand variables reflecting functional capacity, which might bereciprocal.
A strong point in our study is the use of structuralequations modeling (SEM), which provides a more extensiveinsight in the complex relationship of DPA with functionaland psychological variables. In addition, the broad group ofstudied COPD patients warrants better validity than studieswith more specific groups of patients did [3,8]. Althoughthe number of participants per subgroup (healthcaresetting) seems limited we belief we selected sufficientpatients from three different healthcare settings. We thinkthat our results are therefore valid for patients as they arepresent in usual care.
Moreover, our extensive set of instruments covered moreaspects of related factors than earlier studies.
There are some limitations. The patient group in thisstudy was rather small to perform a path analysis, whichmight have caused the moderate fit of the model [33].However, the values in the model are well interpretableand no negative error variance or associations >1 wereshown, which indicates a fair causal model.
Another limitation is that DPA was measured with apedometer, which is less accurate than an accelerometer.The Yamax Digiwalker 200, however, has shown to be themost accurate pedometer at moderate to slow gate speed
arrows) between the latent variables psychological capacity,hown by the path coefficient (standardized regression coeffi-ariables is specified by the correlation coefficient.

1746 W.A. Altenburg et al.
and only tended to underestimate the number of steps atvery low gate speed [50]. Furthermore, pedometers aremore accurate than questionnaires and diaries, lessexpensive and time consuming than double labeled wateror direct observation, and easy to use, and therefore allowinclusion of a large cohort [51].
In conclusion, DPA levels in COPD are low. A betterfunctional capacity is strongly and independently associ-ated with higher levels of DPA. Psychological factors such asanxiety, depression and self-efficacy also affect DPA, butindirectly by an effect on functional capacity. Finally, theinfluence of psychological factors seems larger in patientswith better functional capacity. There is a need for inves-tigating whether treatment of psychological factors shouldbe addressed when patients enroll in an exercise training orphysical activity counseling program and whether the ef-fects depend on functional capacity.
Conflicts of interest
All authors declare to have no conflict of interest.
Acknowledgements
W.A. Altenburg had full access to all the data in the studyand takes responsibility for the integrity of the data and theaccuracy of the data analysis, including and especially anyadverse effects. WA and JB participated in the studydesign. WA and LB performed the data collection. WA andMdG performed the statistical analysis. WA, MdG, HK, NtH,JW interpreted the data. All authors participated in writingthe manuscript and approved the final version.
This study was supported by an unrestricted grant fromBoehringer Ingelheim B.V. and by the University MedicalCenter Groningen.
Appendix A. Supplementary material
Supplementary material associated with this article can befound, in the online version, at http://dx.doi.org/10.1016/j.rmed.2013.06.002.
References
[1] Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M,Gosselink R. Characteristics of physical activities in daily lifein chronic obstructive pulmonary disease. Am J Respir CritCare Med 2005;171:972e7.
[2] Watz H, Waschki B, Meyer T, Magnussen H. Physical activity inpatients with COPD. Eur Respir J 2009;33:262e72.
[3] Belza B, Steele BG, Hunziker J, Lakshminaryan S, Holt L,Buchner DM. Correlates of physical activity in chronicobstructive pulmonary disease. Nurs Res 2001;50:195e202.
[4] Garcia-Rio F, Lores V, Mediano O, Rojo B, Hernanz A, Lopez-Collazo E, et al. Daily physical activity in patients withchronic obstructive pulmonary disease is mainly associatedwith dynamic hyperinflation. Am J Respir Crit Care Med 2009;180:506e12.
[5] Hernandes NA, Teixeira Dde C, Probst VS, Brunetto AF,Ramos EM, Pitta F. Profile of the level of physical activity in
the daily lives of patients with COPD in Brazil. J Bras Pneumol2009;35:949e56.
[6] Moy ML, Matthess K, Stolzmann K, Reilly J, Garshick E. Free-living physical activity in COPD: assessment with acceler-ometer and activity checklist. J Rehabil Res Dev 2009;46:277e86.
[7] Schonhofer B, Ardes P, Geibel M, Kohler D, Jones PW. Eval-uation of a movement detector to measure daily activity inpatients with chronic lung disease. Eur Respir J 1997;10:2814e9.
[8] McGlone S, Venn A, Walters EH, Wood-Baker R. Physical ac-tivity, spirometry and quality-of-life in chronic obstructivepulmonary disease. COPD 2006;3:83e8.
[9] Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Anto JM.Regular physical activity reduces hospital admission andmortality in chronic obstructive pulmonary disease: a popu-lation based cohort study. Thorax 2006;61:772e8.
[10] Esteban C, Quintana JM, Aburto M, Moraza J, Arostegui I,Espana PP, et al. The health, activity, dyspnea, obstruction,age, and hospitalization: prognostic score for stable COPDpatients. Respir Med 2011;105:1662e70.
[11] Garcia-Rio F, Rojo B, Casitas R, Lores V, Madero R, Romero D,et al. Prognostic value of the objective measurement of dailyphysical activity in COPD patients. Chest 2012.
[12] Waschki B, Kirsten A, Holz O, Muller KC, Meyer T, Watz H,et al. Physical activity is the strongest predictor of all-causemortality in patients with COPD: a prospective cohort study.Chest 2011;140:331e42.
[13] Watz H, Waschki B, Boehme C, Claussen M, Meyer T,Magnussen H. Extrapulmonary effects of chronic obstructivepulmonary disease on physical activity: a cross-sectionalstudy. Am J Respir Crit Care Med 2008;177:743e51.
[14] Lemmens KM, Nieboer AP, Huijsman R. Designing patient-related interventions in COPD care: empirical test of atheoretical model. Patient Educ Couns 2008;72:223e31.
[15] Hospes G, Bossenbroek L, Ten Hacken NH, van Hengel P, deGreef MH. Enhancement of daily physical activity increasesphysical fitness of outclinic COPD patients: results of an ex-ercise counseling program. Patient Educ Couns 2009;75:274e8.
[16] Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P,et al. Global strategy for the diagnosis, management, and pre-vention of chronic obstructive pulmonary disease: GOLD exec-utive summary. Am J Respir Crit Care Med 2007;176:532e55.
[17] Crouter SE, Schneider PL, Karabulut M, Bassett Jr DR. Validityof 10 electronic pedometers for measuring steps, distance,and energy cost. Med Sci Sports Exerc 2003;35:1455e60.
[18] Tudor-Locke C, Williams JE, Reis JP, Pluto D. Utility of pe-dometers for assessing physical activity: construct validity.Sports Med 2004;34:281e91.
[19] Schneider PL, Crouter SE, Bassett DR. Pedometer measuresof free-living physical activity: comparison of 13 models. MedSci Sports Exerc 2004;36:331e5.
[20] Schneider PL, Crouter SE, Lukajic O, Bassett Jr DR. Accuracyand reliability of 10 pedometers for measuring steps over a400-m walk. Med Sci Sports Exerc 2003;35:1779e84.
[21] Kyle UG, Genton L, Mentha G, Nicod L, Slosman DO,Pichard C. Reliable bioelectrical impedance analysis esti-mate of fat-free mass in liver, lung, and heart transplantpatients. JPEN J Parenter Enteral Nutr 2001;25:45e51.
[22] Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R,Yernault JC. Lung volumes and forced ventilatory flows.Report Working Party Standardization of Lung Function Tests,European Community for Steel and Coal. Official Statementof the European Respiratory Society. Eur Respir J Suppl 1993;16:5e40.
[23] ATS Committee on Proficiency Standards for Clinical Pulmo-nary Function Laboratories. ATS statement: guidelines for

Variables affecting physical activity in COPD 1747
the six-minute walk test. Am J Respir Crit Care Med 2002;166:111e7.
[24] Kempen GI, Miedema I, Ormel J, Molenaar W. The assessmentof disability with the Groningen Activity Restriction Scale.Conceptual framework and psychometric properties. Soc SciMed 1996;43:1601e10.
[25] Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limi-tation. The St. George’s Respiratory Questionnaire. Am RevRespir Dis 1992;145:1321e7.
[26] Ware Jr JE, Sherbourne CD. The MOS 36-item short-formhealth survey (SF-36). I. Conceptual framework and itemselection. Med Care 1992;30:473e83.
[27] van der Molen T, Willemse BW, Schokker S, ten Hacken NH,Postma DS, Juniper EF. Development, validity and respon-siveness of the Clinical COPD Questionnaire. Health Qual LifeOutcomes 2003;1:13.
[28] Tiesinga LJ, Dassen TW, Halfens RJ. DUFS and DEFS: devel-opment, reliability and validity of the Dutch Fatigue Scaleand the Dutch Exertion Fatigue Scale. Int J Nurs Stud 1998;35:115e23.
[29] Zigmond AS, Snaith RP. The hospital anxiety and depressionscale. Acta Psychiatr Scand 1983;67:361e70.
[30] Bosscher RJ, Laurijssen L, de Boer E. Measuring physical self-efficacy in old age. Percept Mot Skills 1993;77:470.
[31] Ryan RM, Connell JP. Perceived locus of causality andinternalization: examining reasons for acting in two domains.J Pers Soc Psychol 1989;57:749e61.
[32] Bentler PM, Bonett DG. Significance tests and goodness of fitin the analysis of covariance-structures. Psychol Bull 1980;88:588e606.
[33] Hu LT, Bentler P. Structural equation modelling: concepts,issues and applications. In: Hoyle RH, editor. Evaluatingmodel fit. Thousand Oaks, CA: Sage; 1995. p. 77e99.
[34] Tabachnick BG, Fidell LS. Using multivariate statistics. 5thed. New York: Allyn and Bacon; 2007.
[35] Wheaton B, Muthen B, Alwin DF, Summers G. Assessing reli-ability and stability in panel models. Sociol Methodol 1977;8(84):84e136.
[36] Browne M. Alternative ways of assessing model fit. In:Bollen K, editor. Testing structural equation models. New-bury Park, CA: Sage; 1993. p. 136e62.
[37] Hu LT, Bentler P. Cutoff criteria for fit indexes in covariancestructure analysis: conventional criteria versus new alter-natives. Struct Equ Model 1999;6(1):1e55.
[38] Tudor-Locke C, Hatano Y, Pangrazi RP, Kang M. Revisiting“how many steps are enough?”. Med Sci Sports Exerc 2008;40:S537e43.
[39] Bjorgaas M, Vik JT, Saeterhaug A, Langlo L, Sakshaug T,Mohus RM, et al. Relationship between pedometer-registeredactivity, aerobic capacity and self-reported activity and
fitness in patients with type 2 diabetes. Diabetes Obes Metab2005;7:737e44.
[40] Witham MD, Argo IS, Johnston DW, Struthers AD,McMurdo ME. Predictors of exercise capacity and everydayactivity in older heart failure patients. Eur J Heart Fail 2006;8:203e7.
[41] Waschki B, Spruit MA, Watz H, Albert PS, Shrikrishna D,Groenen M, et al. Physical activity monitoring in COPD:compliance and associations with clinical characteristics in amulticenter study. Respir Med 2012;106:522e30.
[42] Baltzan MA, Scott AS, Wolkove N, Bailes S, Bernard S,Bourbeau J, et al. Fatigue in COPD: prevalence and effect onoutcomes in pulmonary rehabilitation. Chron Respir Dis 2011;8:119e28.
[43] Theou O, Jones GR, Overend TJ, Kloseck M, Vandervoort AA.An exploration of the association between frailty and musclefatigue. Appl Physiol Nutr Metab 2008;33:651e65.
[44] Van Dyck D, Cardon G, Deforche B, Giles-Corti B, Sallis JF,Owen N, et al. Environmental and psychosocial correlates ofaccelerometer-assessed and self-reported physical activityin Belgian adults. Int J Behav Med 2011;18:235e45.
[45] Pan SY, Cameron C, Desmeules M, Morrison H, Craig CL,Jiang X. Individual, social, environmental, and physicalenvironmental correlates with physical activity amongCanadians: a cross-sectional study. BMC Public Health2009;9:21.
[46] Delahanty LM, Conroy MB, Nathan DM., Diabetes PreventionProgram Research Group. Psychological predictors of phys-ical activity in the diabetes prevention program. J Am DietAssoc 2006;106:698e705.
[47] Spruit MA, Watkins ML, Edwards LD, Vestbo J, Calverley PM,Pinto-Plata V, et al. Determinants of poor 6-min walkingdistance in patients with COPD: the ECLIPSE cohort. RespirMed 2010;104:849e57.
[48] Kunik ME, Veazey C, Cully JA, Souchek J, Graham DP,Hopko D, et al. COPD education and cognitive behavioraltherapy group treatment for clinically significant symptomsof depression and anxiety in COPD patients: a randomizedcontrolled trial. Psychol Med 2008;38:385e96.
[49] de Godoy DV, de Godoy RF. A randomized controlled trial ofthe effect of psychotherapy on anxiety and depression inchronic obstructive pulmonary disease. Arch Phys MedRehabil 2003;84:1154e7.
[50] Bassett Jr DR, Ainsworth BE, Leggett SR, Mathien CA,Main JA, Hunter DC, et al. Accuracy of five electronic pe-dometers for measuring distance walked. Med Sci SportsExerc 1996;28:1071e7.
[51] Hartman JE, Boezen HM, de Greef MH, Bossenbroek L, tenHacken NH. Consequences of physical inactivity in chronicobstructive pulmonary disease. Expert Rev Respir Med 2010;4:735e45.





























