Embed Size (px)
Citation preview
3/5/2014
1
Community Based Rehabilitation (CBR) Models in the Philippines:
Lessons Learned and Applications to Decrease Health Disparities
in Oakland, California
Rolando T. Lazaro, PhD, PT, DPT, MS, GCSFulbright Senior Scholar to the Philippines, June‐November 2013
Visiting Professor, UP‐College of Allied Medical ProfessionsAssociate Professor and Co‐Chair, Samuel Merritt University,
Oakland, CA, USA
1986‐1989
• Graduated from the UP College of Allied Medical Professions (UP‐CAMP)
• Taught at the same institution right after graduation
1989‐2010
• Moved to the United States
• Became a US citizen
• Worked; pursued MS, DPT and PhD degrees
2011
• Applied for a sabbatical at SMU, was not selected
• Went back to UP‐CAMP; volunteered to teach for 6 weeks (part of my sabbatical application)
2013
• Received a Fulbright grant, back to UP‐CAMP to teach/research
• Areas of emphasis: community‐based rehabilitation, health promotion
• and disability prevention
3/5/2014
2
Significant gap in access to quality health care affects health outcomes
Area is surrounded by the best healthcare facilities but significant proportion of population have poor health/ cannot access these facilities
African Americans in Oakland have the worst outcomes in 16 of 19 key health indicators in Alameda county
May be related to socioeconomic status, but also largely associated with lack of cultural competent care
Experts recommend a multimodal approach to decrease these disparities; community involvement is critical in building capacity to improve access to quality health care at all levels.

3/5/2014
3

3/5/2014
4

3/5/2014
5
3/5/2014
6
Study the Community‐Based Rehabilitation models in the Philippines
University of the Philippines model(s)
Other models
Apply what I have learned as I prepare to expand our CBR clinic in my home community in Oakland, CA
Strategy within the general community development for the prevention of impairments, rehabilitation, equalization of opportunities, poverty reduction and inclusion of children and adults with disabilities into the mainstream society
Disability can be physical and mental

3/5/2014
7

3/5/2014
8
Bay, Laguna (Comprehensive Community Health Program‐ CCHP)
UP ran a comprehensive hospital with allied health services (PT, OT, ST)
Interns went to the Barangay Health Clinics (BHC) and did whatever needs to be done (assumption of any role within the healthcare system)
No inter/transdisciplinary approach to healthcare
Program was terminated in 1988

3/5/2014
9
Awards
1. HAMIS Bronze Award, Health and Management Information System (HAMIS) of the Department of Health and German Technical Cooperation
2. GAWAD PAGASA Award, Civil Service Commission ‐Community Based Rehabilitation (CBR) Program, CAMP, September 2004
3/5/2014
10
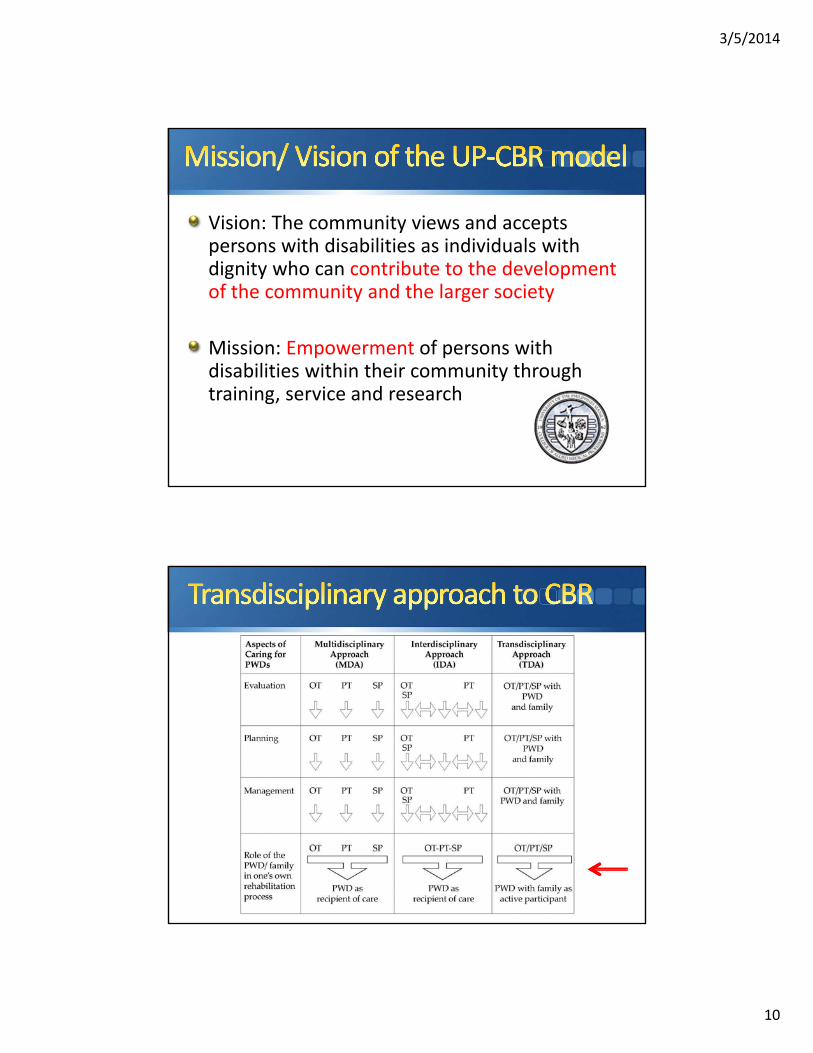
Vision: The community views and accepts persons with disabilities as individuals with dignity who can contribute to the development of the community and the larger society
Mission: Empowerment of persons with disabilities within their community through training, service and research

3/5/2014
11

3/5/2014
12
Two failed mayoral bids, successful third try
Father used to be Mayor of Bustos; mother was a physician and owns the town’s private hospital
Has a Doctor of Public Administration degree
Has siblings in the medical field
Fully supports the CBR program; allocates specific funds to sustain the program
Housing subsidy
Some expenses

3/5/2014
13
Disability surveys: PWD*s identified
Refer the PWD to the Barangay Health Workers
(BHW); paperwork started
BHWs follow up with family, LGUs regarding registration process; necessary disciplines contacted (MD, PT,
etc.)
PT/OT/ST services provided in close coordination with BHW (often co‐treatments);
MD/nurse/ etc. for primary care as
needed
Family and BHW Trained on techniques; when competency is attained, client is taken off the clinic
caseload
(add livelihood projects)
*PWD: persons with disabilities

3/5/2014
14
Planning process
Determine the two barangays to be served (delimit due to limited resources)
Coordination with the LGU to set up the program
Meetings with PWD in each barangay
Asked two questions to the group, then discussed their answers
Discussions with Local Government Units
Mayor
Barangay Captain and Kagawads (Council persons)
PWD groups in barangays
Prevalence of PWD (from records)
Location (accessibility, flooding, etc.) and infrastructure to support clinical training of students in CBR

3/5/2014
15
Encoded responsesLooked at responses where goal was self sufficiency, NOT dole outs
Progress in terms of working together toward a shared goal
Discussed support from personalities, issues, challenges
Discussed locations of the barangays

3/5/2014
16
Mariano Marcos State University, Physical Therapy Department
PT Program only
Commission of Higher Education (CHED) Mandates that all PT Programs provide didactic and clinical exposure to CBR
CBR Curriculum with specific competencies
Governor Imee Marcos
• Current Governor of Ilocos Norte
• Provided funds for the construction of the MMSU Physical Therapy department
• Patient of the department as well

3/5/2014
17
CBR Team: 2 faculty members and Physiatrist (Dr. Wendell Lozano)

3/5/2014
18
Referrals from everyone (students, families, BHWs) go to MD for evaluation
MD evaluates the patient; provides recommendations; identifies necessary connections and referrals; starts paperwork
BHWs follow up with family, LGUs regarding registration process
PT services provided until MD terminates
the service
Disability surveys: PWDs identified
Refers the PWD to the Barangay Health
Workers; paperwork started
BHWs follow up with family, LGUs regarding registration process
PT/OT/ST services provided in close
coordination with BHW
Family and BHW Trained on techniques; when competency is
attained, client is taken off the clinic caseload
Referrals from everyone (students, families, BHWs)
MD evaluates the patient; provides recommendations;
identifies necessary connections and referrals; starts paperwork
BHWs follow up with family, LGUs regarding registration
process
PT services provided until MD terminates the service
Traditional CBR Model (Medical Model)
Transdisciplinary Care Model

3/5/2014
19
Features Traditional Medical CBR Model UP CBR Model
Focus Provide rehabilitation services (forever)
Sustainability of CBR; constant movement in and out of places
Leadership Physician CBR Head (not a physician)
Orientation Interdisciplinary Transdiciplinary
Disciplines directly involved
MD, PT PT, OT, ST, Social Work, Nursing, MD, etc.
Service provision Primary, tertiary care Tertiary care with referral to primary services PRN; livelihood, self sustainability
Positive points Physician clout Multi‐faceted; familyinvolvement mandatory
Challenges Sustainability is questionable; no projects that support self‐sufficiency or empowerment
Progress highly dependent LGU and non‐governmentalorganization (NGO) support
By law, 5% of internal revenue allotment of each LGU must be set aside for senior citizens and persons with disabilities (PWD)
4% to senior citizens; 1% to PWD
LGUs have difficulty showing where the money for PWD went; often source of conflicts between mayors and barangay chairmen
Several PWD groups funded by LGU and NGOsPersons in positions of power draw salaries and allowances
Unclear hierarchy also source of conflict among groups
3/5/2014
20
What I have learned and what can I apply?
• Systematic process of developing a CBR program (the San Mateo experience)• “If you build it they won’t necessarily come”
• Need to be part of the community; establish relationships with people
• Statistics on disability prevalence
• Readiness of the community
• Commitment from local government
• Identify first what their needs are and their level of commitment‐ sustainability is key!
Personalities
ALL of them came from a family of politicians
NOT all of them have shown commitment to CBR
The person who did (Arnel Mendoza): comes from a family with a medical background
Moral of the story: educate our city officials on the importance of rehabilitation and disability prevention
3/5/2014
21
What I have learned and what can I apply?
• More feasible to provide services in a specific location rather than at home (logistically and also due to liability issues) BUT within the community it serves• SMU’s collaboration with Allen Temple and other
clinical entities in the area
• While there are various agencies that coordinate care, they don’t necessarily talk to each other‐ we need to advocate for the client
What I have learned and what can I apply?
• Transdiciplinary model is better suited for the US healthcare environment (include the PWD/family!)
• Establish collaborative agreements with other disciplines
• Interprofessional education
• Comprehensive transdisciplinary (interprofessional) free clinics with funding from non‐profit agencies through community grants and a sliding scale fee for services
• Aim must be to provide care but to also educate the publicto take responsibility of their health and well‐being

3/5/2014
22
What I have learned and what can I apply?
• Less concern on personalities and conflicts; more transparency in the US so this will be less of an issue
• Funding agencies are usually separate from those in positions of power; lots of checks and balances
• Emphasize culturally competent care; must have the commitment to provide care to all
Introduction to the Fulbright Program

3/5/2014
23
Merit‐based grants for international exchange for students, scholars, teachers, professionals, scientists and artists
Founded by US Senator J. William Fulbright in 1946
Primary intent is to promote mutual understandingbetween the people of the US and other countries through the exchange of persons, knowledge, and skills
Several available opportunities; those most applicable to the SMU community: Fulbright Student, Core (scholar) and Specialist
For graduating seniors (BS)
Current students completing their master’s or doctoral studies‐ allow to complete their research in another country
Young professionals, artists
Study or research for up to one academic year
Variety of disciplines/areas available
Doctoral degree/enrollment in doctoral level education NOT required in many of the opportunities

3/5/2014
24
Doctorally prepared individuals in a variety of fields
However, many scholarships that DO NOTrequire a PhD/ doctoral degree
Study, research, consult (or combination) in field of specialty
(Core) Scholar program: 2‐12 months
Specialist program 2‐6 weeks
Additional programs of interest: academic administration, science and technology expertise, etc.
Almost all academic disciplines except clinical medical research involving patient contact
Some that may be applicable to SMU community include:
Nursing (MANY subspecialties open)
Public health/ global health
Disaster management, risk reduction
Education, Administration/ Public Administration
Social Justice, Peace studies
Politics, Economics
Computer science

3/5/2014
25
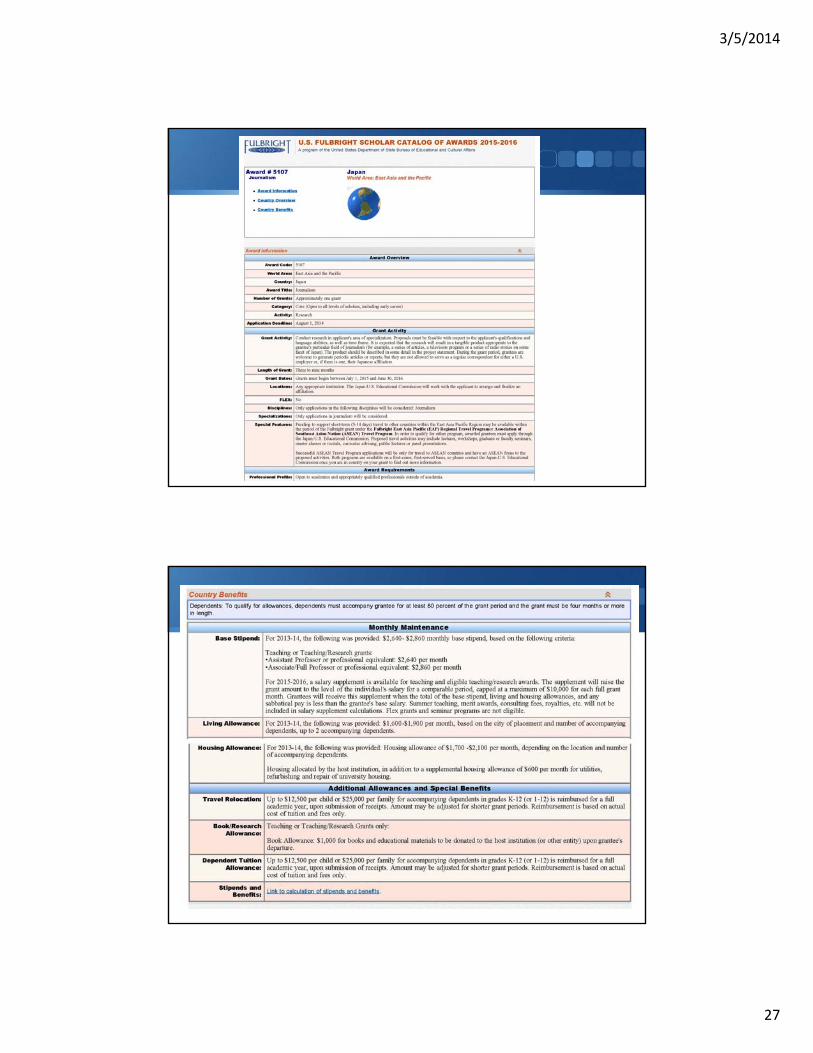
Round‐trip airfare via US‐based airline (Fly America Initiative); excess baggage upon return
Housing stipend and living expenses (some grants provide a more generous $$$ amount)
Basic medical coverage for emergency treatment while overseas; life insurance
“Start‐up” costs (up to $1,000)‐ books/ supplies/equipment that you will leave the in the host institution upon program completion
Short travel grants to neighboring countries available (East Asia travel)
First STEP: SEARCH!!!
http://catalog.cies.org/
3/5/2014
26
http://us.fulbrightonline.org/about/fulbright‐us‐student‐program
3/5/2014
27

3/5/2014
28
Very well‐written, specific and clear Project Description (2 pages)
Make sure you use words that are closely linked to the intent to the Fulbright program (mutual understanding between US and other countries)
Do your homework‐ read the award details closely and match the needs as perfectly as you can
Some require letter or support, some do not
Measurable goals and timelines

3/5/2014
29





























