Embed Size (px)
Citation preview

FSC402HForensic Toxicology of Common Pharmaceuticals
November 11, 2003
Common Pharmaceuticals
Compendium of Pharmaceuticals and Specialties: The Canadian Drug Reference for Health Professionals
Published by: The Canadian Pharmacists Association
146 pharmaceutical companies
63 pages listing brand and generic names

Forensic Issues
Delayed Toxicity Toxicity at Low and High Concentrations Degradation of Sample in vitro High Toxicity vs Low Toxicity Age dependant toxicity Drug Interactions Role of Metabolites Impairment Postmortem Redistribution
Delayed Toxicity
Acetaminophen
Tylenol + + + also found combined with great # of combined products 350-650 mg, oral, normal-release, sustained-release Analgesic and Anti-pyretic Therapeutic Concentrations
0.2 – 5.2 mg/dL

Delayed Toxicity
Glucuronide Acetaminophen Sulfate
Reactive Intermediate
Glutathione Conjugate
Delayed Toxicity
Acetaminophen Toxicity – Overdose
Glutathione becomes depleted
Reactive Intermediate builds up
Reversible damage to hepatocytes

Delayed Toxicity
Rumack-Matthew Nomogram
Adapted from Rumack BH, Matthew H: "Acetaminophen poisoning and toxicity." Pediatrics 55(6):871-876, 1975

Delayed Toxicity
RUMACK – MATTHEWNOMOGRAM CAUTIONS
time refers to time from ingestion
serum (blood) levels drawn before 4 hours may not represent peak
used only for a single acute ingestion
if T1/2 > 4 hours - likelihood of hepatic injury

Delayed Toxicity
Phase 1: 0-24 hours asymptomatic anorexia nausea, vomiting diaphoresis malaise
Phase 2: 18-72 hours phase 1 symptoms pain in upper right quadrant liver enzymes
Acetaminophen Toxicity – Overdose
Phase 3: 72-96 hours hepatic necrosis with abdominal pain hepatic encephalopathy jaundice nausea & vomiting renal failure DEATH
Phase 4: 4d – 3wks complete resolution

Delayed Toxicity
Acetaminophen Toxicity – Overdose
hepatotoxicity – 24-48 hours
peak hepatotoxicity – 72-96 hours
death – 4-18 days
Minimal Fatal Conc.: ??9 – 32 mg/dL

Delayed Toxicity
AcetylSalicylic Acid
Aspirin + + +
also found combined with great # of combined products

Delayed Toxicity
AcetylSalicylic Acid
Analegesia, Antipryresis 325-975 mg, oral 3.1 – 11.4 mg/dL
Antiinflammatory 3000-5000 mg, oral 4.4 – 33 mg/dL (50 mg/kg)
Delayed Toxicity
AcetylSalicylic Acid – Toxicity
hyperventilation mild confusion tinnitus nausea, vomiting agitation or lethargy seizures respiratory alkalosis, metabolic acidosis pulmonary edema, hemorrhage, acute renal failure,
DEATH
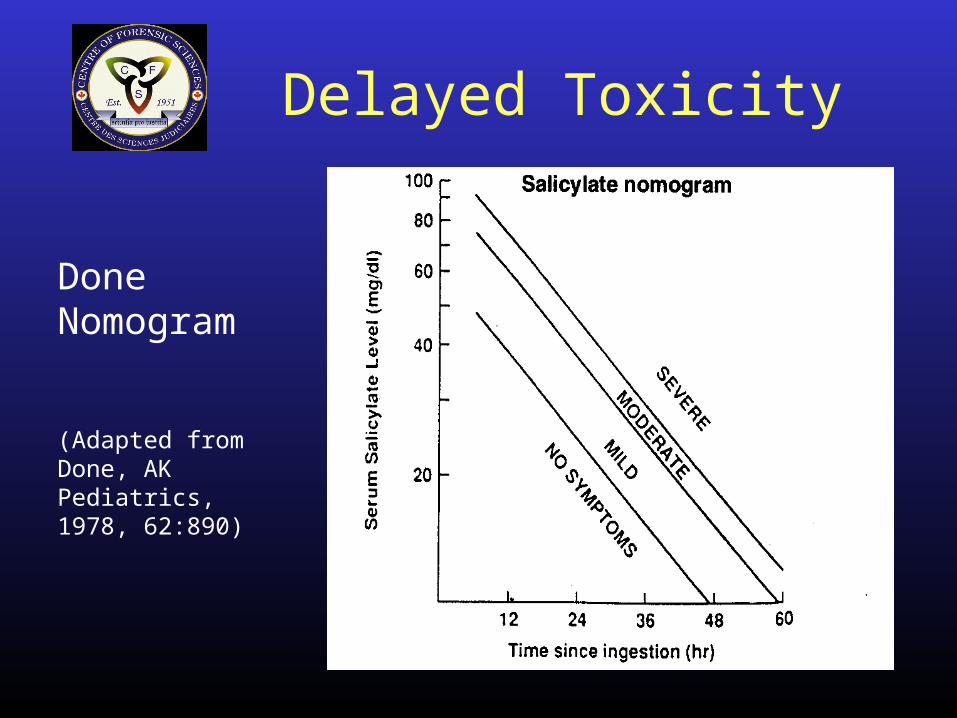
Delayed Toxicity
Done Nomogram
(Adapted from Done, AK Pediatrics, 1978, 62:890)

Delayed Toxicity
NOMOGRAM CAUTIONS
single, acute ingestion
serum (blood) level to be compared is at least 6 hours after time of ingestion
MINIMAL FATAL CONCENTRATION
generally > 50 mg/dL 6.1 – 732 mg/dL
Toxicity at Low and High
Anti-Convulsants
TOO LITTLE is as bad as TOO MUCH
Phenobarbital
Phenytoin
Primidone
Valproic Acid
Gabapentin
Vigabatrin
Carbamazepine
Lamotrigine

Toxicity at Low and High
Phenobarbital used as an anticonvulsant since 1912
for epilepsy 60 – 120 mg/day
often given in combination with other anticonvulsants

Toxicity at Low and High
Phenobarbital
Effective Concentration – Plasma 1 – 3 mg/dL
Effective Concentration – Blood 0.8 – 2.4 mg/dL

Toxicity at Low and High
Phenobarbital - Toxicity
Low Concentrations Ineffective control of epilepsy seizures, DEATH
High Concentrations CNS depression, coma, DEATH Begin at plasma conc. > 4 mg/dL (3.2 mg/dL blood) Coma 6.5 – 11.7 mg/dL plasma
(5.2 – 9.4 mg/dL blood) DEATH as little as 5.5 mg/dL blood

Toxicity at Low and High
Phenytoin
first use in 1938
considered by many to be drug of choice in epilepsy
300 – 400 mg/day oral
intravenous or intramuscular for acute seizure

Toxicity at Low and High
Phenytoin
Effective Concentration – Plasma 1 – 2 mg/dL general guidelines 0.23 – 2.9 mg/dL controlled study
Effective Concentration – Blood 0.63 – 1.3 mg/dL general guidelines 0.14 – 1.81 mg/dL controlled study

Toxicity at Low and High
Phenytoin - Toxicity
Low Concentrations Ineffective control of epilepsy seizures, DEATH
High Concentrations Unintentional elevations may be due to inability to
metabolize to p-hydroxyphenytoin (through drug interactions)
Few deaths 2 ½ yr boy – 11.2 mg/dL
Toxicity at Low and HighPhenytoin – Toxicity
nystagamus ataxia slurred speech confusion hyperreflexia somnelence, lethargy blurred vision nausea, vomiting coma death due to respiratory and circulatory depression
Toxicity at Low and High
Lamotrigine used as an anticonvulsant since 1992
often in conjunction with other anticonvulsants
maintenance dose 100 – 700 mg/day
Effective concentration ??

Toxicity at Low and High
LamotrigineTherapeutic Concentrations dependant on whether alone or with other anticonvulsants
Lamotrigine dose Other drug Conc.(mg/70 Kg) (mg/dL) 428 None 0.56 573 Phenytoin 0.23 491 Phenobarbital 0.34 364 Carbamazepine 0.27 197 Valproic Acid 0.90

Toxicity at Low and High
Lamotrigine – Toxicity
Low Concentrations
Ineffective control of epilepsy seizures, DEATH Difficult to determine
lack of information often used with other anticonvulsants
Toxicity at Low and High
Lamotrigine – Toxicity
High Concentrations skin rash dizziness headache somnolence ataxia blurred vision nausea, vomiting coma death

Toxicity at Low and High
Lamotrigine – Toxicity
Minimal fatal concentration difficult to determine lack of information often used with other anticonvulsants
One reported fatality 5.2 mg/dL

Degradation of Sample In Vitro
Bupropion
Olanzapine
Diltiazem
Others ???

Degradation of Sample In Vitro
Bupropion (Zyban, Wellbutrin) used in U.S. since 1990
for treatment of depression, cessation of cigarette smoking
200 – 450 mg/day
Therapeutic Concentration 0.005 – 0.01 mg/dL
can achieve 0.04 mg/dL – no toxicity
Degradation of Sample In Vitro
Bupropion – Toxicity seizures
tachycardia
lethargy
confusion
tremors
vomiting
DEATH

Degradation of Sample In Vitro
Bupropion – Toxicity DEATH
minimal fatal concentration to date
0.4 mg/dL
N = 5 (0.4 – 1.3 mg/dL)
Degradation of Sample In Vitro
Bupropion – Interpretative Problem
Bupropion breaks down in vitro – temp. & pH dependant
High Concentration (> 0.4 mg/dL)- potentially fatal
Low Concentration (0.03 – 0.4 mg/dL)- toxic- fatal with degradation

Degradation of Sample In Vitro
Bupropion – Interpretative Problem
Low Concentration (< 0.03 mg/dL)- therapeutic- toxic with degradation- fatal with degradation
Not Detected- not present- therapeutic with degradation- toxic with degradation- fatal with degradation

Degradation of Sample In Vitro
Olanzapine (Zyprexa) used since 1996
anti-psychotic
10 – 20 mg/day
Therapeutic Concentration (chronic, trough)
0.0009 – 0.0026 mg/dL
Degradation of Sample In Vitro
Olanzapine – Toxicity drowsiness
slurred speech
ataxia
disorientation
hypotension
coma

Degradation of Sample In Vitro
Olanzapine – Toxicity DEATH
Minimal information available N = 7 Overdose, survived
serum conc. = 0.005 – 0.1 mg/dL minimum fatal conc. to date 0.1 mg/dL
Degradation of Sample In Vitro
Olanzapine – Interpretative Problem
Olanzapine breaks down in vitro
- undergoes oxidation
16% loss during extraction40% loss during 1 week at 4oC45% loss during 1 day at RT- inhibited by addition of ascorbic acid
Olesen & Linnet, 1998, J. Chrom. B714:309
Degradation of Sample In Vitro
Olanzapine – Interpretative Problem
degradation is not consistent
by the time a sample is screened, significant degradation may have occurred

Degradation of Sample In Vitro
Olanzapine – Interpretative Problem High Concentration (> 0.1)
- potentially fatal
Low Concentration (< 0.005 mg/dL)- therapeutic- toxic, degradation- fatal, degradation
Not Detected- not present- therapeutic, degradation- toxic, degradation- fatal, degradation
High vs. Low Toxicity
Barbiturates vs. Benzodiazepines
Amobarbital (Amytal) vs. Diazepam (Valium)
Tricyclic vs. SSRI Antidepressants
Amitriptyline vs. Sertraline
High vs. Low Toxicity
Amobarbital- 15 –200 mg oral
- 65 – 500 mg i.v., i.m.
- therapeutic conc.0.18 – 1.2 mg/dL
Amobarbital (Amytal) vs. Diazepam (Valium)
- sedative, hypnotic
Diazepam- 2 –40 mg oral
- 2 – 40 mg i.v., i.m.
- therapeutic conc.0.01 – 0.15 mg/dL

High vs. Low Toxicity
Amobarbital
- tolerance
- drowsiness- confusion- stupor- ataxia- coma
Amobarbital vs. Diazepam - Toxicity
Diazepam
-tolerance
- drowsiness- confusion- ataxia- muscle weakness- light coma (> 2.0 mg/dL)
High vs. Low ToxCicity
Amobarbital
- DEATH
N = 55 amobarbital deaths1.3 – 9.6 mg/dL(therapeutic < 1.2 mg/dL)
Amobarbital vs. Diazepam - Toxicity
Diazepam
- few reported Deaths
N = 67 diazepam casesN= 3, diazepam aloneMean conc. 4.8 mg/dL(therapeutic < 0.15 mg/dL)

High vs. Low Toxicity
Amitriptyline- Tricyclic
- oral, i.m., up to 150 mg
- therapeutic conc.0.004 – 0.016 mg/dL
Amitriptyline (Elavil) vs. Sertraline (Zoloft)
- antidepressant
Sertraline- Selective-serotonin reuptake inhibitor
- oral, 50 –200 mg
- therapeutic conc.0.002 – 0.03 mg/dL

High vs. Low Toxicity
Amitriptyline- confusion, agitation- stupor, drowsiness- vomiting- cardiac dysrhythmias
(0.04 mg/dL)- hypotension- convulsions- CNS depression- coma
Amitriptyline vs. Sertraline
Sertraline- sedation
- nausea, vomiting
- tachycardia
- anxiety

High vs. Low Toxicity
Amitriptyline
- DEATH
> 0.1 mg/dL (therapeutic < 0.02 mg/dL)
Amitriptyline vs. Sertraline
Sertraline
-No reported Fatalities
N = 5 sertraline unrelated0.06 – 0.14 mg/dL(therapeutic < 0.03 mg/dL)
Age Dependant Toxicity
The Very Young
Brompheniramine
Acetaminophen
The Very Old
Diphenhydramine
Age Dependant Toxicity
Brompheniramine
antihistamine
available in OTC preparations with other drugs- Dimetame; Dimetapp- Dimetapp Oral Infant Cold Drops
Therapeutic Concentrations- only adult information available- up to 0.002 mg/dL

Age Dependant Toxicity
Brompheniramine – Toxicity
CNS depression
may cause stimulation in children
No reported fatalities in adults

Age Dependant Toxicity
INFANTS
several cases, < 8 weeks old, male
Brompheniramine concentrations of 0.02 mg/dL
Is this fatal ??????
no other drugs detected
no anatomical cause of death
SIDS?

Age Dependant Toxicity
Acetaminophen
analgesic, antipyretic
available in OTC preparations alone and with other drugs
Therapeutic Concentrations- Adults 0.2 – 5.2 mg/dL- Children 1.0 – 4.0 mg/dL

Age Dependant Toxicity
Acetaminophen
Fetus and Neonate (< 2 months)
appear to metabolize acetaminophen through mixed oxidase system reactive intermediate
at risk for liver toxicity

Age Dependant Toxicity
Diphenhydramine
antihistamine
available in OTC preparations alone or with other drugs
oral 50 – 100 mg
also available for i.v. and i.m.
Therapeutic concentrations
up to 0.03 mg/dL
Age Dependant Toxicity
Diphenhydramine – Toxicity
Potential for toxicity is increased in those > 60 yrs
agitation
confusion
hallucination
coma
seizures
CNS depression

Age Dependant Toxicity
Diphenhydramine – Toxicity
DEATH
Minimal Fatal Concentrations
Diphendydramine 0.5 mg/dL
Diphenhydramine - Elderly 0.21 mg/dL

Drug Interactions
Metabolism Interactions
- Inhibition of Enzymes
- Induction of Enzymes
Serotonin Syndrome

Drug Interactions
SEROTONIN SYNDROME from excess serotonin
- irritability - dysphoria- confusion - anxiety
- delirium - hyperthermia- tachycardia - tremor- diaphoresis - hyperreflexia- shivering - muscle rigidity- tachypnea - ataxia- coma
DEATH
Drug Interactions
SEROTONIN SYNDROMEFrom Drug Interactions
***MAO Inhibitor + SSRI
- MAO + Tricyclic Antidepressant (TCA)
- MAO Inhibitor + Meperidine
- MAO Inhibitor + Dextromethorphan

Role of Metabolites
Drugs are metabolized to help increase elimination, not necessarily decrease action or toxicity.
Active Metabolites
Toxic Metabolites
Added Information Acute vs. Chronic
Role of Metabolites
Active Metabolites
1) Metabolite Activity = Parent Activity
Acebutolol Diacetolol (anti-hypertensive)
Buspirone 1-pyrimidinylpiperazine (anxiolytic)
Clobazam Desmethylclobazam (anticonvulsant; anxiolytic)
Diazepam Nordiazepam* (anxiolytic; anticonvulsant)

Role of Metabolites
Active Metabolites
1) Metabolite Activity = Parent Activity
Doxepin Nordoxepin (antidepressant)
Fluoxetine Norfluoxetine* (antidepressant)
Ketamine Norketamine (induction agent)
Thioridazine mesoridazine & sulforidazine (antipsychotics)
Role of Metabolites
Active Metabolites
2) Metabolite is a drug itself
Amitriptyline Nortriptyline* (anti-depressant)
Chlordiazepoxide Demoxepam*; Oxazepam*; Nordiazepam *(sedative/hypnotic)
Oxazepam is a drug itself; demoxepam and nordiazepam are active metabolites
Imipramine Desipramine *(antidepressant)

Role of Metabolites
Active Metabolites
2) Metabolite is a drug itself
Oxycodone Oxymorphone (potent drug itself) (narcotic analgesic)
Primidone Phenobarbital* (minimal) (anticonvulsant)
Selegiline Methamphetamine* (anti-Parkinson)
Temazepam Oxazepam* (drug) (hypnotic)

Role of Metabolites
Active Metabolites
3) Metabolite has same activity and longer half-life
Chloral Hydrate Trichloroethanol*; major active component (sedative) - chloral hydrate transforms rapidly, not measured
Venlafaxine O-desmethylvenlafaxine (same; longer halflife) (anitdepressant)

Role of Metabolites
Active Metabolites
4) Metabolite has less activity but has longer half-life
Bupropion 3 metabolites; longer half-life; less activity than parent (anti-depressant)
Propoxyphene norpropoxyphene (1/2-1/4) (narcotic analgesic)

Role of Metabolites
Active Metabolites
5) Metabolite has less activity than parent
Amobarbital 3-Hydroxyamobarbital (1/3)(sedative, hypnotic; anticonvulsant)
Clonazepam 7-aminoclonazepam; conc. similar to parent but minimal activity (anticonvulsant; sedative)
Chlorpromazine 168 possible metabolites; 20 isolated; 2 confirmed less active (antipsychotic)
Role of Metabolites
Active Metabolites
5) Metabolite has less activity than parent
Diltiazem deaetyldiltiazem* (20%); nordiltiazem (45%) (anti-hypertensive)
Triazolam Hydroxymethyltriazolam (50-100%) (hynotic)
Verapamil Norverapamil (20%) (Anti-anginal)

Role of Metabolites
OTHER
Codeine Morphine* (significance of activity controversial; 10% conversion)

Role of Metabolites
TOXIC Metabolites
Meperidine (narcotic analgesic)
the metabolite Normeperidine is more toxic
has different toxicity than meperidine
– seizure vs CNS depression
Role of Metabolites
Added Information
Chronic vs. Acute Ingestion
Parent Concentration > Metabolite Concentration
= Acute
Parent Concentration = or < Metabolite Concentration
= Chronic
Impairment
Pharmaceutical Drugs Shown to Have Impairing Effects with respect to Driving
Information is obtained through
Laboratory studies
Driving studies
Epidemiology

Impairment
Challenges
Tolerance needs to be considered
Often information on dose, not plasma (blood) concentration is available
No means through law to obtain a blood sample from an individual
– seized hospital samples from motor vehicle collisions

Impairment
Drugs shown to impair motor and/or cognitive performance
BenzodiazepinesBarbituratesTricyclic AntidepressantsAnti-HistaminesSome Anticonvulsants (Carbamazepine, Gabapentin, Phenytoin)Anti-psychotics (Chloripromazine, Haloperidol, Lithium, Thioridazine)Narcotic Analgesics

Post Mortem Redistribution
A phenomenon whereby increased concentrations of some drugs are observed in postmortem samples and/or site dependent differences in drug concentrations may be observed
Typically central blood samples are more prone to postmortem changes (will have greater drug concentrations than peripheral blood samples)