-
From the basement to the sixth floor : the pathway to a
clinical
France LÉGARÉMD PhD (F) CCFPfloor : the pathway to a
clinical
scientist award and a research career
MD PhD (F) CCFP
McGill Family M di i S it
Du sous-sol au 6ème étage: le chemin vers une bourse et une
Medicine Summit: Training Tomorrow’s Leaders, N b 14 2009le
chemin vers une bourse et une
carrière de chercheur clinicienNovember 14, 2009
-
PlanPlan•Career development:
• personal story• personal story • difficult choices
The way family medicine enabled me to•The way family medicine
enabled me to develop my researchH till b li i i d h•How we can
still be clinicians and researchers
•What makes our research makes a difference
“One can’t have a successful research career without having your
fair share of rejection letters for grants and publications.”
Dawes, M (2009)
-
Career development
-
1990: MD HSFA 1995: MSc Santé com1995: MSc Santé com.1995: FRSQ
subvention #11995: CR-SFA1996: FRSQ subvention #21999: FRSQ bourse
PhD
-
2000 E t PhD P h l2000: Enter PhD Psychology 2001: Transfer PhD
Pop. health2005: PhD Pop health2005: PhD Pop. health2005: FRSQ
junior 12005: Head of KT-HTA CRCHUQQ2006: Canada Research Chair
-
Productivity KT-HTA CRCHUQ
2005-6 2006-7 2007-82008-9
Productivity KT HTA CRCHUQ
2008-9# of FTR (CRCHUQ)
5.6 (3.7%) 5.6 5.6 6.6 (4%)↑18%
Grants $498 668,15 $926 677,06 $574 465,34 $1 181 360,87
Scholarships $108 792 92 $199 793 42 $327 850 83 $301 804
89Scholarships $108 792,92 $199 793,42 $327 850,83 $301 804,89
Total $607 461,07 $1 126 470,48 $902 316,17 $1 483 165,76(1.6%)
(4.5%)↑144%
-
The way family medicineThe way family medicine enabled me to
develop m researchmy research
-
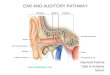
Patient Centered CarePatient Centered Care
Based on Stewart M 1996; Charles Gafni & Whelan 1997; Makoul
&
Dunn 2008
Based on Stewart M 1996; Charles, Gafni & Whelan 1997;
Makoul & Clayman 2006
-
Prise de décision partagéep g•Point de décision
•Meilleures preuves scientifiques
•Risques et bénéfices de toutes les optionsRisques et bénéfices
de toutes les options disponibles (y compris « ne rien faire »)
•Communication du caractère probabiliste•Communication du
caractère probabiliste
•Valeurs et préférences du patient
•Décision
Charles et al., 1997; Towle et al., 1999; Elwyn, 2000Moumjid,
2007
-
Shared Decision MakingShared Decision Making•Crux of
patient-centered care
• overuse of options not clearly associated with benefits for
all
reduction of unwarranted practice
• use of options clearly associated with benefits for the vast
majority
pvariations
• treatment agreement and patient outcomes in chronic
diseases
• sustainability of healthcare systemsWeston 2001; Evans 2005;
O’Connor 2007; Joosten 2008; Coulter 2006; Weston 2001; Evans 2005;
O Connor 2007; Joosten 2008; Coulter 2006; Wennberg 2002
-
How we can still beHow we can still be clinicians and
researchersresearchers
-
CRC Research Program
Intervention
CRC Research Program
A l ti l th d
Descriptive studies
Concepts and measurements
Analytical methods
Systematic reviews
InfrastructureCRC: Canadian Research ChairCRC: Canadian Research
Chair
-
What makes our researchWhat makes our research makes a
difference
-
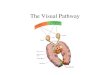
DÉCISION+Sources
d’information
A1Estimer le plus justement possible les probabilités 1
DÉCISION
Prescrire de façon
Favoriser l’utilisation Contribuer à
Intégrer l’ensemble des connaissance
Connaître les risques et les bénéfices de
A1 probabilités diagnostiques des IAVR
1
A2
façon optimale les AB dans le contexte des IAVR
optimale par le patient des AB dans le contexte des IAVR
l’amélioration de la santé de la population
7 86s et compétences acquises afin de favoriser la prise de
décision
5toutes les options thérapeutiques disponibles y compris celle
de « ne rien faire »
2
A3
Résultats
Favoriser la 4
partagée en matière d’AB pour les IAVR
Communiquer efficacement ces risques et bénéfices
3
A3 participation active du patient à la décision
4
© Légaré Labrecque 2005© Légaré, Labrecque 2005
-
Recrutement GMFDevis
RandomisationINTERVENTIONIMMÉDIATE
INTERVENTIONRETARDÉE
Recrutement GMF
Patient (5 Pt/ MF)
MF recrutés MF recrutés
Patient (5 Pt/ MF)1
DECISION+
Patient (5 Pt/ MF) Patient (5 Pt/ MF)1
Patient (5 Pt/ MF)
DECISION+
Patient (5 Pt/ MF)2
Patient (5 Pt/ MF)
DECISION+
Patient (5 Pt/ MF)3
Légaré, Labrecque et al. BMC Fam Pract. 2007
-
© Labrecque, Leblanc, Légaré. Décision Plus. 2007
-
Décision AB (patients)Décision AB (patients)
54%
56%49% 46%
56%
33% 35%
-
DÉCISION+ 2009-2012Sources
d’information
A1Estimer le plus justement possible les probabilités 1
DÉCISION 2009 2012
Prescrire de façon
Favoriser l’utilisation Contribuer à
Intégrer l’ensemble des connaissance
Connaître les risques et les bénéfices de
A1 probabilités diagnostiques des IAVR
1
A2
façon optimale les AB dans le contexte des IAVR
optimale par le patient des AB dans le contexte des IAVR
l’amélioration de la santé de la population
7 86s et compétences acquises afin de favoriser la prise de
décision
5toutes les options thérapeutiques disponibles y compris celle
de « ne rien faire »
2
A3
Résultats
Favoriser la 4
partagée en matière d’AB pour les IAVR
Communiquer efficacement ces risques et bénéfices
3
A3 participation active du patient à la décision
4
© Légaré Labrecque 2005© Légaré, Labrecque 2005
-
SDM in dietitians practicep
Applying a theory-based approach to identify the determinants of
the intention of dietitians to engage inintention of dietitians to
engage in shared decision making behaviors
• SOPHIE DESROCHES (PI) (FRSQ junior 1)F Lé é MP G A E S l (
PI)• F Légaré, MP Gagnon, A.E. Sales (co-PI)
CIHR 2009-04-01 to 2011-03-31FRSQ 2009-2012
-
http //decision chaire fmed la al
ca/http://decision.chaire.fmed.ulaval.ca/