Embed Size (px)
Citation preview

Frequency and Risk of In-Stent Stenosis Following Pulmonary ArteryStenting
Anna Hallbergson, MD, PhDa,b,c, James E. Lock, MDa,b, and Audrey C. Marshall, MDa,b,*
Peripheral and central pulmonary artery (PA) stenoses can result in right ventricular hy-
aDepartment osachusetts; bDeparMassachusetts; anPhiladelphia, Philamanuscript receive
This work waMassachusetts).
See page 544*CorrespondinE-mail address
0002-9149/13/$ -http://dx.doi.org/1
pertension, dysfunction, and death. Percutaneous PA angioplasty and stent placementrelieve obstruction acutely, but patients frequently require reintervention. Within a het-erogeneous patient population with PA stents referred for catheterization because ofnoninvasive signs of PA obstruction, we have observed that in-stent stenosis (ISS) occurscommonly in some groups, challenging previous reports that this phenomenon occursinfrequently. We set out to evaluate the incidence and demographics of patients withprevious PA stent placement who develop ISS. Consecutive patients with previously placedstents presenting for catheterization and undergoing PA angiography were reviewed (104patients, 124 cases). We defined ISS angiographically, as a 25% narrowing of the contrast-filled lumen relative to the fluoroscopically apparent stent diameter at any site along thelength of the stent. For inclusion, we required that the stenotic segment be narrower orequal in size to the distal vessel. ISS was diagnosed in 24% of patients, with the highestincidence among patients with tetralogy of Fallot and multiple aortopulmonary collaterals,Williams syndrome, or Alagille syndrome. In conclusion, ISS after PA stent placement is amore frequent problem than previously reported, and patients with inherently abnormalPAs are disproportionately affected. Increased clinical surveillance after stent placementand investigation of innovative preventive strategies may be indicated. � 2014 ElsevierInc. All rights reserved. (Am J Cardiol 2014;113:541e545)
Peripheral pulmonary stenosis (PPS) occurs in the contextof diffuse arteriopathies (e.g., Williams syndrome) and car-diac developmental defects (e.g., tetralogy of Fallot [TOF]).In either case, multiple lobar and/or sublobar obstructions canlead to proximal pulmonary artery (PA) hypertension.Although right ventricular (RV) function is typically pre-served, this can result in severe RV hypertension. Unmiti-gated, this RV hypertension results in arrhythmia, ventricularfailure, and death.1,2 PPS ismanaged surgically3when lesionsare located proximally, but more peripheral disease usuallycalls for endovascular management, with transcatheterballoon angioplasty or stent placement.4,5 Stents are known tobe effective in lesions refractory to balloon angioplasty andhave greatly enhanced the therapeutic armamentarium of theinterventionalists.4e6 Rates of in-stent stenosis (ISS) havepreviously been reported to be very low.6e8 However, amongpatients with PPS referred for catheterization, we haveobserved a significant rate of angiographic ISS. Currently, nopublished information is available on rates of ISS amongpatients with PPS.We thus set out to describe the incidence ofISS in this patient cohort.
f Cardiology, Boston Children’s Hospital, Boston, Mas-tment of Pediatrics, Harvard Medical School, Boston,d cDivision of Cardiology, The Children’s Hospital ofdelphia. Manuscript received August 9, 2013; revisedd and accepted October 9, 2013.s supported by The Keane Family Foundation (Boston,
for disclosure information.g author: Tel: (617) 355-6529; fax: (617) 713-3808.: [email protected] (A.C. Marshall).
see front matter � 2014 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2013.10.016
Methods
The aim of this study was to determine the incidence ofISS in (1) patients with PPS referred for catheterization and(2) patients with Williams or Alagille syndrome. To addressthe first objective, we searched an institutional database forconsecutive patients having catheterization during the year2012 who had undergone PA stent placement within theprevious 10 years. This list was supplemented with anypatient who had a PA stent redilated at our institution duringthe year 2012; this allowed us to identify some additionalpatients whose stents were not initially placed at our insti-tution or placed >10 years ago. Cases were excluded fromconsideration if there were no angiographic data availablefor review or if the stent had fractured in a manner pre-cluding meaningful measurement of stent or luminal diam-eter. A total of 124 cases (104 patients) were included in ourreview. Indication for catheterization in this patient popu-lation at our institution has remained consistent for manyyears, including preoperative examination, noninvasiveimaging suggestive of significantly elevated RV pressure(�2/3 of systemic), pulmonary blood flow maldistribution(<1/3 of flow to 1 lung), worsening RV function, cyanosisdue to PA stenosis, or worsening in symptoms.9
To address the second objective, we searched the insti-tutional database to identify all patients with either Williamsor Alagille syndrome who had been catheterized at ourcenter at any time after PA stent placement. This identified14 patients with Williams syndrome and 12 patients withAlagille syndrome who had undergone angiographic eval-uation subsequent to PA stent placement at our center from2003 to 2012. The diagnosis of either syndrome was basedon documentation of meeting genetic and/or clinical criteria.
www.ajconline.org

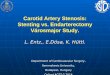
Figure 1. (A) Severe right PA ISS in a 3-year-old with Williams syndrome.(B) No significant ISS in the right PA of a 7-year-old with truncus arte-riosus. Percent ISS is calculated as follows (see arrows): (stent diameter �luminal diameter)/stent diameter � 100.
Table 1Demographics
Variable All Cases (n ¼ 124)
Male 56%Age at catheterization (yrs) 5.5 (0.10e64)Body surface area at catheterization (m2) 0.88 � 0.47Weight at catheterization (kg) 26.6 � 22Stent redilation performed (% of cases) 80Total catheterizations per patient (n) 6 (2e19)PA stents per patient 1 (1e7)Time since stent placement (yrs) 2.8 (0.04e19)Time since the most recent stent dilation (yrs) 1.5 (0.03e13)DiagnosisTOF with MAPCAs 48 (39)TOF without MAPCAs 16 (13)MAPCAs (not TOF) 6 (4.8)Alagille syndrome* 7 (5.6)Williams syndrome 4 (3.2)Nonsyndromic PPS 5 (4.0)Truncus arteriosus 5 (4.0)D-TGA 6 (4.8)Other biventricular 13 (11)HLHS 15 (12)Other univentricular 5 (4.0)
Stent type n ¼ 133 stentsGenesis premounted 76 (57)Genesis XD 21 (16)Coronary 6 (5)Other 15 (11)Unavailable 15 (11)
Data are presented as median (range) or mean � SD, as appropriate.Diagnoses and stent types are presented as % of total cases or stents,respectively.* Of 7 cases with Alagille syndrome, 6 had TOF (also accounted for in
their respective TOF group).
542 The American Journal of Cardiology (www.ajconline.org)
We defined ISS angiographically, as a 25% narrowing ofthe contrast-filled lumen relative to the fluoroscopicallyapparent stent diameter at any site along the length of thestent or stent complex (Figure 1). In addition, the segmentwas only deemed stenotic if it was equal to or narrower thanthe distal vessel to avoid inclusion of ISS due to significantstent overexpansion at the time of placement. Twenty-fivepercent ISS was empirically chosen based on our observa-tion that this degree of angiographic narrowing is oftenhemodynamically significant and responsive to redilation.Determination of ISS was expressed as percentage of cur-rent stent diameter, as opposed to absolute measurement ofluminal compartments. This allowed us to accommodate forthe large range in patient and stent sizes in the pediatricpopulation. Furthermore, defining ISS by percentage of stentlumen (rather than by a certain number of mm) removedmuch of the risk of calibration error, which otherwise couldbe significant, particularly in small vessels.
Data collection was performed by evaluation of 2012angiographic records for assessment of ISS and review ofmedical records and a cardiology department clinical data-base for demographic information. In general, images wereacquired in 2 planes, and the best longitudinal image of eachstent was evaluated. Among patients with multiple PAstents, the identification of ISS in any of the stents resultedin the patient being considered as affected. In these cases,measurements were performed on only one of the stents,
typically the one that was most severely narrowed for pur-poses of data analysis. Computerized 2-dimensional mea-surements were performed using Vericis 8.30 (MergeHealthcare, Chicago, Illinois) by measuring the narrowestcontrast-filled lumen diameter inside the stent and thefluoroscopically apparent stent diameter at that site. Valuesare expressed as median with a range or means with SDwhere applicable. ISS rates in different diagnostic groupswere compared using Fisher’s exact test. Two-tailed pairedt tests were used to compare means of continuous variables.Statistical significance was set at p < 0.05.
Results
Age at the time of catheterization in 2012 was 5.5 years(range, 0.1 to 64). As expected based on our practice,approximately 40% of cases were performed on patientswith TOF, pulmonary atresia, and multiple aortopulmonarycollaterals (TOF/pulmonary atresia/MAPCAs). Other formsof biventricular conditions, including D-loop transpositionof the great arteries (D-TGA) and truncus arteriosus, madeup 19% of cases. Single ventricle conditions, primarilyhypoplastic left heart syndrome (HLHS) (at any stage ofpalliation), made up 15% of cases. Patients with PPS froman identified arteriopathy made up 8% of total cases. Totallifetime catheterizations through 2012 ranged from 2 to 19

Figure 2. Distribution of patients with PPS with previously placed stentscatheterized in 2012 by underlying diagnosis and portion of patients bydiagnosis with ISS. The percentage of patients in each group affected byISS is listed above each column. Bi-V ¼ biventricular.
Figure 3. Comparison of the incidence of PA ISS in patients with arterio-pathy (Williams or Alagille syndrome), TOF and/or MAPCAs, and othercongenital heart disease (including the remaining diagnoses listed in Ta-ble 1). The former 2 groups have a significantly higher rate of ISS than thelatter (p <0.01).
Congenital Heart Disease/Pulmonary Artery In-Stent Stenosis 543
(median 6). Time since stent placement was 2.8 years (range0.04 to 19) and time since most recent stent dilation was1.5 years (range 0.03 to 13). Approximately 3/4 of stents wereGenesis (Cordis, Miami Lakes, Florida) stents (premounted orXD). Demographics of patients evaluated to address the firstobjective are listed in Table 1. There were 26 patients (Wil-liams syndrome n ¼ 14, Alagille syndrome n ¼ 12) in thegroup addressing the second objective. Age at the time ofcatheterization in this group was 4.4 years (range 0.5 to 20).
In this patient cohort, the incidence of angiographic PAISS was 24% (25 of 104 patients), representing 124 totalcases. In affected patients (i.e., by our definition �25% ISSand at most equal luminal size to distal vessel), the averagedegree of ISS was 43% (SD 12%, range 27% to 72%) ste-nosis, that is, on average, the in-stent lumen was narrowedby nearly half. Subgroup analysis of ISS severity was notperformed because of limited sample size of affectedpatients. Mean time since stent placement was similar forpatients with and without ISS (4.1 � 4.1 and 4.2 �4.1 years, respectively). Time since last intervention wasless in patients with ISS (1.5 � 1.6 years) compared withthose without significant ISS (2.7 � 2.9 years, p <0.05).The distribution of stent types was also similar between the2 groups (p >0.05). Stent redilation was performed in 80%of total cases (100% of cases with ISS). Presumably, redi-lations without underlying ISS were performed to accom-modate somatic growth.
Some patient groups had a high tendency to be affectedby ISS, whereas others were rarely affected (Figure 2).Patients with MAPCAs had a 38% incidence of ISS, spe-cifically 13 (36%) of 36 patients with TOF/pulmonaryatresia/MAPCAs and 2 of 3 patients with other conditionsassociated with MAPCAs. Underlying diagnoses of thelatter 2 patients were complex biventricular heterotaxy withpulmonary atresia and single RV with pulmonary atresia,respectively. The average severity of ISS among affectedpatients in the TOF/pulmonary atresia/MAPCA group was44%, that is, similar to the average for the entire cohortaffected by ISS. In patients with TOF without MAPCAs, the
incidence was 27% (4 of 15 patients). There were 7 patientswith 22q11 deletion in the cohort, all of whom had TOF/pulmonary atresia/MAPCAs but interestingly had a lowincidence (14%) of ISS (1 of 7 patients), which was notsignificantly different from the rate seen in TOF/pulmonaryatresia/MAPCA patients without the 22q11 deletion basedon the present small sample size. ISS was nearly absent inother structural congenital heart disease, including HLHS atany stage of repair (0 of 13 patients), D-TGA (0 of 6 pa-tients), truncus arteriosus (1 of 5 patients), and otherbiventricular conditions (0 of 12). This latter group ofpatients with other structural congenital heart disease wassignificantly less affected by ISS compared with the patientswith TOF and/or MAPCAs or arteriopathy (p <0.01;Figure 3). The more extensive review of patients with ge-netic arteriopathic conditions supported their high incidenceof ISS, including 36% of patients (5 of 14) with Williamssyndrome and 50% of patients (6 of 12) with Alagillesyndrome (9 of whom also had TOF).
Discussion
ISS is a source of recurrent obstruction in previouslystented PAs and is more common among patients with PPSreferred for catheterization than previously recognized.6e8
Our results suggest that patients with arteriopathies and TOFshould receive vigilant surveillance for ISS. The incidenceof ISS after PA stent placement in our cohort of patients was24% (31% of cases). In the sole previous report that sys-tematically assessed for degree of stenosis (including adefinition and grading system), the severity of ISS wasdefined by the thickness (in mm) of tissue between lumenand stent. In designing our study, we found a static defini-tion of ISS problematic, given the range in PA sizes inchildren with congenital heart disease (e.g., a 1-mm celllayer in a 5-mm stent will contribute to more stenosis than a1-mm cell layer in a 10-mm stent). Although the previousstudy had a broader cohort of patients, most had repairedTOF and pulmonary atresia, suggesting significant overlap ofour patient populations. Median time from stent placement toreassessment was comparable with our study (2 vs 2.8 years),

544 The American Journal of Cardiology (www.ajconline.org)
although approximately 1/2 of our patients had undergonestent redilation since placement. The time interval from lastredilation was approximately 1.5 years (range, 0.03 to 13) inour cohort. Not surprisingly, the group affected by ISS hadundergone more recent stent redilation. In the previous study,significant neointimal proliferation (>1 mm) was reported inonly 4 (1.8%) of 220 patients, and restenosis based on bothangiographic and hemodynamic criteria had an incidence of5%. In contrast, using percentage of luminal loss as a markerfor ISS, we found a 24% incidence.
Underlying PA pathology clearly plays a role in thedevelopment of ISS. To our knowledge, this is the first reportsuggesting that patients with certain underlying diagnoses(TOF, MAPCAs, or primary arteriopathy) are at unique riskfor ISS after PA stent placement. Patients with othercongenital heart disease in this cohort, most of whom havestents placed because of postoperative PA obstructions, weretypically spared from ISS (39 of 41 patients unaffected).From these findings, one can infer that stents placed innormal vasculature subject to surgical anastomoses, kinking,compression, or stretching are at lower risk of ISS. Similarly,there is little risk of ISS after redilation of an unaffected stentbecause of the somatic growth of a patient in these seeminglylow-risk groups. In contrast, in patients in whom primaryinherent abnormalities of the vascular wall are central to thedisease (i.e., TOF, MAPCAs, congenital arteriopathy), thereis a significant risk of ISS. Close monitoring for increasingRV hypertension or pulmonary blood flow maldistributionwith low threshold for invasive reassessment is warrantedafter stent placement in high-risk patients.
Obviously, “underlying PA pathology” is an indistinctterm. On a microscopic level, the inherent PA abnormalitiesin patient populations vulnerable to PPS manifest as specificcellular changes, some of which have been described indetail. In the elastin-deficiency Williams syndrome, theobstructive lesions are due to increased smooth muscle cellproliferation and abnormal elastic lamellae, which result inmedial hypertrophy. Lumen loss is then exacerbated by pri-mary underdevelopment of vessels.10,11 In Alagille syndrome(aka arteriohepatic dysplasia), mutations in JAG-1 anddisruption in notch signaling result in abnormal vasculo-genesis, affecting multiple vascular beds, including the PAs.12
In these pathologic vessels, the endothelial response to injuryimposed by stent placement may be unique. However, if thereare similarities to the mechanism of ISS studied in coronaryartery disease, then effective therapies (such as mammaliantarget of rapamycin inhibitors) may offer benefit to our pa-tients with PA stenosis.
Many stress factors may modulate the degree to whichvessels exhibit and/or develop ISS. These include stent im-plantation techniques, preexisting endothelial vessel wallinjury, and stent location and type. At our center, predilationwith either low- or high-pressure balloons is typical beforestent placement, which conceivably could be an instigatingfactor to neointimal proliferation. At the time of stent place-ment and redilation, balloon angioplasty can be performedusing high or low inflation pressure, which could potentiallyalso confer different risk of ISS. Although these factors mayplay a role in PA ISS, we use relatively similar implantationtechniques such as predilation, inflation pressure, stent typedespite underlying diagnosis. Of note, among our patients
with arteriopathy, we have observed a higher rate of vascularinjury in response to angioplasty, which could potentiallycontribute to their higher rates of ISS at the time of subse-quent stent placement. Previous reports of ISS in PA havesuggested that stent placement at an unfavorable angle orleaving a gap between 2 tandem stents increases risk of ISS.7,8
In the present study cohort, stent types were evenly distri-buted among patients with and without ISS, suggestinglittle contribution of stent type to subsequent development ofISS.
Our findings suggest that purely anatomic managementin the catheterization laboratory may be insufficient tocombat PA ISS and that reducing ISS may be a focus offuture outpatient management. In fact, necessary redilationsin the catheterization laboratory may in some patients act asa stimulus for further ISS. Our observations of patientsaffected by ISS suggest that it occurs early and rapidly afterthe procedure indicating that the proliferative response afterinjury sets in motion the process of luminal loss in a fashionsimilar to that observed in coronary arteries. Drug-elutingstents are now well established for coronary artery stentingand have been associated with lower rates of cardiac death,myocardial infarction, and stent thrombosis than bare-metalstents.13 Use of drug-eluting stents in PAs would be pref-erable for our patient population as well but appropriatestent sizes are currently unavailable making investigation ofother proliferative inhibition for patients with PPS war-ranted. Future innovative therapies to address ISS mayinclude antiproliferative therapy such as rapamycin (siroli-mus) as suggested from animal models.14 The data pre-sented herein indicate that the patients most likely to benefitfrom such therapy are those with TOF, MAPCAs, and/orarteriopathies. Our center is currently investigating the po-tential for future clinical use of rapamycin in this patientpopulation.
Our study was a retrospective review of patients referredfor catheterization, which imposes several study limitations.A selection bias may be introduced as patients are typicallyreferred because of clinical and/or noninvasive imaging in-dications, which may bias toward higher rates of ISS(as opposed to scheduled prospective reassessment of po-tential ISS at a set time after stent placement). Furthermore,there is a lack of a standardized definition of ISS in the PAliterature making comparisons to previous studies difficultand necessitated an arbitrary definition based on our clinicalexperience of what constitutes significant ISS. We limitedthis definition to angiographic appearance, whereas it maybe preferably to also include hemodynamic data, forexample, stent pressure gradients, which are not universallyrecorded or available for review at our institution.
Disclosures
The authors have no conflicts of interest to disclose.
1. Bird LM, Billman GF, Lacro RV, Spicer RL, Jariwala LK, Hoyme HE,Zamora-Salinas R, Morris C, Viskochil D, Frikke MJ, Jones MC.Sudden death in Williams syndrome: report of ten cases. J Pediatr1996;129:926e931.
2. Geggel RL, Gauvreau K, Lock JE. Balloon dilation angioplasty ofperipheral pulmonary stenosis associated with Williams syndrome.Circulation 2001;103:2165e2170.

Congenital Heart Disease/Pulmonary Artery In-Stent Stenosis 545
3. MongeMC,MainwaringRD,SheikhAY,PunnR,ReddyVM,HanleyFL.Surgical reconstruction of peripheral pulmonary artery stenosis inWilliams and Alagille syndromes. J Thorac Cardiovasc Surg 2013;145:476e481.
4. Maglione J, Bergersen L, Lock JE, McElhinney DB. Ultra-high-pressure balloon angioplasty for treatment of resistant stenoses withinor adjacent to previously implanted pulmonary arterial stents. CircCardiovasc Interv 2009;2:52e58.
5. Law MA, Shamszad P, Nugent AW, Justino H, Breinholt JP, Mullins CE,Ing FF. Pulmonary artery stents: long-term follow-up. Catheter Car-diovasc Interv 2010;75:757e764.
6. Fogelman R, Nykanen D, Smallhorn JF, McCrindle BW, Freedom RM,Benson LN. Endovascular stents in the pulmonary circulation. Clinicalimpact on management and medium-term follow-up. Circulation1995;92:881e885.
7. Ing FF, Grifka RG, Nihill MR, Mullins CE. Repeat dilation of intra-vascular stents in congenital heart defects. Circulation 1995;92:893e897.
8. McMahon CJ, El-Said HG, Grifka RG, Fraley JK, Nihill MR, MullinsCE. Redilation of endovascular stents in congenital heart disease:factors implicated in the development of restenosis and neointimalproliferation. J Am Coll Cardiol 2001;38:521e526.
9. Baker CM, McGowan FX, Keane JF, Lock JE. Pulmonary arterytrauma due to balloon dilation: recognition, avoidance and manage-ment. J Am Coll Cardiol 2000;36:1684e1690.
10. Urbán Z, Riazi S, Seidl TL, Katahira J, Smoot LB, Chitayat D, BoydCD, Hinek A. Connection between elastin haploinsufficiency andincreased cell proliferation in patients with supravalvular aortic stenosisand Williams-Beuren syndrome. Am J Hum Genet 2002;71:30e44.
11. Williams JCP, Barratt-Boyes BG, Lowe JB. Supravalvular aortic ste-nosis. Circulation 1961;24:1311e1318.
12. Kamath BM, Spinner NB, Emerick KM, Chudley AE, Booth C, Piccoli D,Krantz ID. Vascular anomalies in Alagille syndrome: a significant cause ofmorbidity and mortality. Circulation 2004;109:1354e1358.
13. Palmerini T, Biondi-Zoccai G, Della Riva D, Mariani A, Sabaté M,Valgimigli M, Frati G, Kedhi E, Smits PC, Kaiser C, Genereux P,Galatius S, Kirtane AJ, Stone GW. Clinical outcomes with drug-elutingand bare metal stents in patients with ST-segment elevation myocardialinfarction: evidence from a comprehensive network meta-analysis.J Am Coll Cardiol 2013;62:496e504.
14. Li W, Li Q, Qin L, Ali R, Qyang Y, Tassabehji M, Pober BR, SessaWC, Giordano FJ, Tellides G. Rapamycin inhibits smooth muscle cellproliferation and obstructive arteriopathy attributable to elastin defi-ciency. Arterioscler Thromb Vasc Biol 2013;33:1e8.