Embed Size (px)
Citation preview
FRCSOrthcouk
FRCS orth course Important papers in
Orthopaedics
FRCSOrthcouk
Scaphoid fracture
FRCSOrthcouk
N=88 44 in each group early internal fixation with use of a Herbert screw without a cast avg 9days post injury vs nonop treatment for eight weeks with immobilization in a below-the-elbow plaster cast with the
thumb left free Regular fu the severity of pain tenderness swelling wrist movement grip strength and symptoms and
disability+ x-rays Patients returned to work at five to six weeks after the injury in both groups At twelve weeks grip strength was better in patients who had had surgery No significant
difference was detected between the two groups with respect to any other outcome measure at any other time
1044 nonop had not healed radiographically at twelve weeks and as a consequence the treatment was altered
944 operative gp ndashminor complications ldquono clear benefit of early fixation of acute scaphoid fractures over non op Rxrdquo aggressive conservative treatment carefully assess fracture-healing with plain radiographs and
computed tomography scans after six to eight weeks of cast immobilization and recommend surgical fixation with or without bone-grafting at that time if a gap is identified at the fracture site Such an approach should result in fracture union in over 95 of such patients
bull JBJS Am 2005 oct Should acute scaphoid fractures be fixed A randomized controlled trialDias JJ Wildin CJ Bhowal B Thompson JR Leicester UK Level 1 evidence
FRCSOrthcouk
Clinical and radiological outcome of cast immobilisation versus surgical treatment of acute scaphoid fractures at a mean follow-up of 93 monthsProf JJ Dias 2008 JBJS
N=71 Non op=36 Op=35 fu 7 frac12 years no statistical difference in symptoms and disability FOR ROM grip strength pinch strength
or patient rated scores X-rays n= 59 patients OA changes scaphotrapezial (ST)and radioscaphoid (RS)joints no
statistical difference 335 patients had asymptomatic lucency surrounding the screw 136 non-operatively treated patient developed nonunion with avascular necrosis 536 scapholunate angle ( gt 60deg) 45 asymptomatic
No medium-term difference in function or radiological outcome was identified between the two treatment groups
FRCSOrthcouk
Scaphoid fracture Ix
J Bone Joint Surg Br 2008 Sep Early magnetic resonance imaging compared with bone scintigraphy in suspected scaphoid
fractures Beeres FJ Rhemrev SJ Netherlands N=100 with a suspected scaphoid fracture but without evidence of a fracture on plain radiographs using MRI
within 24 hours of injury and bone scintigraphy three to five days after injury The reference standard for a true radiologically-occult scaphoid fracture was either a diagnosis of fracture
on both MRI and bone scan or in the case of discrepancy clinical andor radiological evidence of a fracture
MRI false negative in four patients and bone scan in eight MRI sensitivity 80 and a specificity of 100 Bone scintigraphy had a sensitivity of 100 and a specificity of 90
FRCSOrthcouk
CORR 2009 SepDiagnosing Suspected Scaphoid Fractures A Systematic Review and Meta-analysis Level IIIYin ZG China
Imaging protocols for suspected scaphoid fractures are inconsistent bone scan MRI and CT for diagnosing suspected scaphoid fractures
26 studies The pooled sensitivity specificity natural logarithm of the diagnostic odds ratio and PPV amp NPV were respectively 97 89 478 882 and 003 for bone scan 96 99 660 96 and 004 for MRI and 93 99 611 93 and 007 for CT
MRI is more specific and better for confirming scaphoid fracture
FRCSOrthcouk
Treatment
CORR2007 JulTreatment of acute scaphoid fractures systematic review and meta-analysisYin ZG China
2007 Jul Treatment of acute scaphoid fractures systematic review
and meta-analysis Yin ZG China Operative treatment of acute nondisplaced or minimally
displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization
Operative treatment of acute nondisplaced or minimally displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization however it causes more complications and perhaps a higher risk of scaphotrapezial osteoarthritis There is no evidence from randomized trials to determine whether operative treatment is superior to nonoperative treatment for an acute proximal pole fracture of scaphoid bones
There is insufficient evidence to determine which type of cast should be used in nonoperative treatment of nondisplaced scaphoid fractures
Injury 2009 MarOperative versus nonoperative treatment of acute undisplaced and minimally displaced scaphoid waist fractures--a systematic reviewModi CS Nancoo T Powers D Ho K Boer R Turner SM United Kingdom
Included studies were critically appraised using levels of evidence and RCTs were further appraised using a scoring tool
112 studies 12 included Three level 1 RCTs three level 2 RCTs two meta-analyses one economic analysis and three retrospective studies
Percutaneous fixation may result in faster union rates by approximately 5 weeks and an earlier return to sport and work by approximately 7 weeks over cast treatment
This difference is not seen when comparing ORIF with cast treatment cast treatment results in a higher non-union rate than ORIF this needs to be balanced with the 30 minor complication rate
Manual workers require significantly longer time off work than non-manual workers regardless of the method of treatment ( return to work sooner after ORIF than after cast treatment)
ldquoOperative treatment should be reserved for patients unable to work in a cast and considered for most manual workers and high-level athletesrdquo
FRCSOrthcouk
Conservative treatment of scaphoid nonunion in children and adolescents
Prolonged treatment with cast immobilisation resulted in union of the fracture and an excellent Modified Wrist Score in all patients
D M Weber JBJS Br 2009 Sep
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Scaphoid fracture
FRCSOrthcouk
N=88 44 in each group early internal fixation with use of a Herbert screw without a cast avg 9days post injury vs nonop treatment for eight weeks with immobilization in a below-the-elbow plaster cast with the
thumb left free Regular fu the severity of pain tenderness swelling wrist movement grip strength and symptoms and
disability+ x-rays Patients returned to work at five to six weeks after the injury in both groups At twelve weeks grip strength was better in patients who had had surgery No significant
difference was detected between the two groups with respect to any other outcome measure at any other time
1044 nonop had not healed radiographically at twelve weeks and as a consequence the treatment was altered
944 operative gp ndashminor complications ldquono clear benefit of early fixation of acute scaphoid fractures over non op Rxrdquo aggressive conservative treatment carefully assess fracture-healing with plain radiographs and
computed tomography scans after six to eight weeks of cast immobilization and recommend surgical fixation with or without bone-grafting at that time if a gap is identified at the fracture site Such an approach should result in fracture union in over 95 of such patients
bull JBJS Am 2005 oct Should acute scaphoid fractures be fixed A randomized controlled trialDias JJ Wildin CJ Bhowal B Thompson JR Leicester UK Level 1 evidence
FRCSOrthcouk
Clinical and radiological outcome of cast immobilisation versus surgical treatment of acute scaphoid fractures at a mean follow-up of 93 monthsProf JJ Dias 2008 JBJS
N=71 Non op=36 Op=35 fu 7 frac12 years no statistical difference in symptoms and disability FOR ROM grip strength pinch strength
or patient rated scores X-rays n= 59 patients OA changes scaphotrapezial (ST)and radioscaphoid (RS)joints no
statistical difference 335 patients had asymptomatic lucency surrounding the screw 136 non-operatively treated patient developed nonunion with avascular necrosis 536 scapholunate angle ( gt 60deg) 45 asymptomatic
No medium-term difference in function or radiological outcome was identified between the two treatment groups
FRCSOrthcouk
Scaphoid fracture Ix
J Bone Joint Surg Br 2008 Sep Early magnetic resonance imaging compared with bone scintigraphy in suspected scaphoid
fractures Beeres FJ Rhemrev SJ Netherlands N=100 with a suspected scaphoid fracture but without evidence of a fracture on plain radiographs using MRI
within 24 hours of injury and bone scintigraphy three to five days after injury The reference standard for a true radiologically-occult scaphoid fracture was either a diagnosis of fracture
on both MRI and bone scan or in the case of discrepancy clinical andor radiological evidence of a fracture
MRI false negative in four patients and bone scan in eight MRI sensitivity 80 and a specificity of 100 Bone scintigraphy had a sensitivity of 100 and a specificity of 90
FRCSOrthcouk
CORR 2009 SepDiagnosing Suspected Scaphoid Fractures A Systematic Review and Meta-analysis Level IIIYin ZG China
Imaging protocols for suspected scaphoid fractures are inconsistent bone scan MRI and CT for diagnosing suspected scaphoid fractures
26 studies The pooled sensitivity specificity natural logarithm of the diagnostic odds ratio and PPV amp NPV were respectively 97 89 478 882 and 003 for bone scan 96 99 660 96 and 004 for MRI and 93 99 611 93 and 007 for CT
MRI is more specific and better for confirming scaphoid fracture
FRCSOrthcouk
Treatment
CORR2007 JulTreatment of acute scaphoid fractures systematic review and meta-analysisYin ZG China
2007 Jul Treatment of acute scaphoid fractures systematic review
and meta-analysis Yin ZG China Operative treatment of acute nondisplaced or minimally
displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization
Operative treatment of acute nondisplaced or minimally displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization however it causes more complications and perhaps a higher risk of scaphotrapezial osteoarthritis There is no evidence from randomized trials to determine whether operative treatment is superior to nonoperative treatment for an acute proximal pole fracture of scaphoid bones
There is insufficient evidence to determine which type of cast should be used in nonoperative treatment of nondisplaced scaphoid fractures
Injury 2009 MarOperative versus nonoperative treatment of acute undisplaced and minimally displaced scaphoid waist fractures--a systematic reviewModi CS Nancoo T Powers D Ho K Boer R Turner SM United Kingdom
Included studies were critically appraised using levels of evidence and RCTs were further appraised using a scoring tool
112 studies 12 included Three level 1 RCTs three level 2 RCTs two meta-analyses one economic analysis and three retrospective studies
Percutaneous fixation may result in faster union rates by approximately 5 weeks and an earlier return to sport and work by approximately 7 weeks over cast treatment
This difference is not seen when comparing ORIF with cast treatment cast treatment results in a higher non-union rate than ORIF this needs to be balanced with the 30 minor complication rate
Manual workers require significantly longer time off work than non-manual workers regardless of the method of treatment ( return to work sooner after ORIF than after cast treatment)
ldquoOperative treatment should be reserved for patients unable to work in a cast and considered for most manual workers and high-level athletesrdquo
FRCSOrthcouk
Conservative treatment of scaphoid nonunion in children and adolescents
Prolonged treatment with cast immobilisation resulted in union of the fracture and an excellent Modified Wrist Score in all patients
D M Weber JBJS Br 2009 Sep
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
N=88 44 in each group early internal fixation with use of a Herbert screw without a cast avg 9days post injury vs nonop treatment for eight weeks with immobilization in a below-the-elbow plaster cast with the
thumb left free Regular fu the severity of pain tenderness swelling wrist movement grip strength and symptoms and
disability+ x-rays Patients returned to work at five to six weeks after the injury in both groups At twelve weeks grip strength was better in patients who had had surgery No significant
difference was detected between the two groups with respect to any other outcome measure at any other time
1044 nonop had not healed radiographically at twelve weeks and as a consequence the treatment was altered
944 operative gp ndashminor complications ldquono clear benefit of early fixation of acute scaphoid fractures over non op Rxrdquo aggressive conservative treatment carefully assess fracture-healing with plain radiographs and
computed tomography scans after six to eight weeks of cast immobilization and recommend surgical fixation with or without bone-grafting at that time if a gap is identified at the fracture site Such an approach should result in fracture union in over 95 of such patients
bull JBJS Am 2005 oct Should acute scaphoid fractures be fixed A randomized controlled trialDias JJ Wildin CJ Bhowal B Thompson JR Leicester UK Level 1 evidence
FRCSOrthcouk
Clinical and radiological outcome of cast immobilisation versus surgical treatment of acute scaphoid fractures at a mean follow-up of 93 monthsProf JJ Dias 2008 JBJS
N=71 Non op=36 Op=35 fu 7 frac12 years no statistical difference in symptoms and disability FOR ROM grip strength pinch strength
or patient rated scores X-rays n= 59 patients OA changes scaphotrapezial (ST)and radioscaphoid (RS)joints no
statistical difference 335 patients had asymptomatic lucency surrounding the screw 136 non-operatively treated patient developed nonunion with avascular necrosis 536 scapholunate angle ( gt 60deg) 45 asymptomatic
No medium-term difference in function or radiological outcome was identified between the two treatment groups
FRCSOrthcouk
Scaphoid fracture Ix
J Bone Joint Surg Br 2008 Sep Early magnetic resonance imaging compared with bone scintigraphy in suspected scaphoid
fractures Beeres FJ Rhemrev SJ Netherlands N=100 with a suspected scaphoid fracture but without evidence of a fracture on plain radiographs using MRI
within 24 hours of injury and bone scintigraphy three to five days after injury The reference standard for a true radiologically-occult scaphoid fracture was either a diagnosis of fracture
on both MRI and bone scan or in the case of discrepancy clinical andor radiological evidence of a fracture
MRI false negative in four patients and bone scan in eight MRI sensitivity 80 and a specificity of 100 Bone scintigraphy had a sensitivity of 100 and a specificity of 90
FRCSOrthcouk
CORR 2009 SepDiagnosing Suspected Scaphoid Fractures A Systematic Review and Meta-analysis Level IIIYin ZG China
Imaging protocols for suspected scaphoid fractures are inconsistent bone scan MRI and CT for diagnosing suspected scaphoid fractures
26 studies The pooled sensitivity specificity natural logarithm of the diagnostic odds ratio and PPV amp NPV were respectively 97 89 478 882 and 003 for bone scan 96 99 660 96 and 004 for MRI and 93 99 611 93 and 007 for CT
MRI is more specific and better for confirming scaphoid fracture
FRCSOrthcouk
Treatment
CORR2007 JulTreatment of acute scaphoid fractures systematic review and meta-analysisYin ZG China
2007 Jul Treatment of acute scaphoid fractures systematic review
and meta-analysis Yin ZG China Operative treatment of acute nondisplaced or minimally
displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization
Operative treatment of acute nondisplaced or minimally displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization however it causes more complications and perhaps a higher risk of scaphotrapezial osteoarthritis There is no evidence from randomized trials to determine whether operative treatment is superior to nonoperative treatment for an acute proximal pole fracture of scaphoid bones
There is insufficient evidence to determine which type of cast should be used in nonoperative treatment of nondisplaced scaphoid fractures
Injury 2009 MarOperative versus nonoperative treatment of acute undisplaced and minimally displaced scaphoid waist fractures--a systematic reviewModi CS Nancoo T Powers D Ho K Boer R Turner SM United Kingdom
Included studies were critically appraised using levels of evidence and RCTs were further appraised using a scoring tool
112 studies 12 included Three level 1 RCTs three level 2 RCTs two meta-analyses one economic analysis and three retrospective studies
Percutaneous fixation may result in faster union rates by approximately 5 weeks and an earlier return to sport and work by approximately 7 weeks over cast treatment
This difference is not seen when comparing ORIF with cast treatment cast treatment results in a higher non-union rate than ORIF this needs to be balanced with the 30 minor complication rate
Manual workers require significantly longer time off work than non-manual workers regardless of the method of treatment ( return to work sooner after ORIF than after cast treatment)
ldquoOperative treatment should be reserved for patients unable to work in a cast and considered for most manual workers and high-level athletesrdquo
FRCSOrthcouk
Conservative treatment of scaphoid nonunion in children and adolescents
Prolonged treatment with cast immobilisation resulted in union of the fracture and an excellent Modified Wrist Score in all patients
D M Weber JBJS Br 2009 Sep
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Clinical and radiological outcome of cast immobilisation versus surgical treatment of acute scaphoid fractures at a mean follow-up of 93 monthsProf JJ Dias 2008 JBJS
N=71 Non op=36 Op=35 fu 7 frac12 years no statistical difference in symptoms and disability FOR ROM grip strength pinch strength
or patient rated scores X-rays n= 59 patients OA changes scaphotrapezial (ST)and radioscaphoid (RS)joints no
statistical difference 335 patients had asymptomatic lucency surrounding the screw 136 non-operatively treated patient developed nonunion with avascular necrosis 536 scapholunate angle ( gt 60deg) 45 asymptomatic
No medium-term difference in function or radiological outcome was identified between the two treatment groups
FRCSOrthcouk
Scaphoid fracture Ix
J Bone Joint Surg Br 2008 Sep Early magnetic resonance imaging compared with bone scintigraphy in suspected scaphoid
fractures Beeres FJ Rhemrev SJ Netherlands N=100 with a suspected scaphoid fracture but without evidence of a fracture on plain radiographs using MRI
within 24 hours of injury and bone scintigraphy three to five days after injury The reference standard for a true radiologically-occult scaphoid fracture was either a diagnosis of fracture
on both MRI and bone scan or in the case of discrepancy clinical andor radiological evidence of a fracture
MRI false negative in four patients and bone scan in eight MRI sensitivity 80 and a specificity of 100 Bone scintigraphy had a sensitivity of 100 and a specificity of 90
FRCSOrthcouk
CORR 2009 SepDiagnosing Suspected Scaphoid Fractures A Systematic Review and Meta-analysis Level IIIYin ZG China
Imaging protocols for suspected scaphoid fractures are inconsistent bone scan MRI and CT for diagnosing suspected scaphoid fractures
26 studies The pooled sensitivity specificity natural logarithm of the diagnostic odds ratio and PPV amp NPV were respectively 97 89 478 882 and 003 for bone scan 96 99 660 96 and 004 for MRI and 93 99 611 93 and 007 for CT
MRI is more specific and better for confirming scaphoid fracture
FRCSOrthcouk
Treatment
CORR2007 JulTreatment of acute scaphoid fractures systematic review and meta-analysisYin ZG China
2007 Jul Treatment of acute scaphoid fractures systematic review
and meta-analysis Yin ZG China Operative treatment of acute nondisplaced or minimally
displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization
Operative treatment of acute nondisplaced or minimally displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization however it causes more complications and perhaps a higher risk of scaphotrapezial osteoarthritis There is no evidence from randomized trials to determine whether operative treatment is superior to nonoperative treatment for an acute proximal pole fracture of scaphoid bones
There is insufficient evidence to determine which type of cast should be used in nonoperative treatment of nondisplaced scaphoid fractures
Injury 2009 MarOperative versus nonoperative treatment of acute undisplaced and minimally displaced scaphoid waist fractures--a systematic reviewModi CS Nancoo T Powers D Ho K Boer R Turner SM United Kingdom
Included studies were critically appraised using levels of evidence and RCTs were further appraised using a scoring tool
112 studies 12 included Three level 1 RCTs three level 2 RCTs two meta-analyses one economic analysis and three retrospective studies
Percutaneous fixation may result in faster union rates by approximately 5 weeks and an earlier return to sport and work by approximately 7 weeks over cast treatment
This difference is not seen when comparing ORIF with cast treatment cast treatment results in a higher non-union rate than ORIF this needs to be balanced with the 30 minor complication rate
Manual workers require significantly longer time off work than non-manual workers regardless of the method of treatment ( return to work sooner after ORIF than after cast treatment)
ldquoOperative treatment should be reserved for patients unable to work in a cast and considered for most manual workers and high-level athletesrdquo
FRCSOrthcouk
Conservative treatment of scaphoid nonunion in children and adolescents
Prolonged treatment with cast immobilisation resulted in union of the fracture and an excellent Modified Wrist Score in all patients
D M Weber JBJS Br 2009 Sep
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Scaphoid fracture Ix
J Bone Joint Surg Br 2008 Sep Early magnetic resonance imaging compared with bone scintigraphy in suspected scaphoid
fractures Beeres FJ Rhemrev SJ Netherlands N=100 with a suspected scaphoid fracture but without evidence of a fracture on plain radiographs using MRI
within 24 hours of injury and bone scintigraphy three to five days after injury The reference standard for a true radiologically-occult scaphoid fracture was either a diagnosis of fracture
on both MRI and bone scan or in the case of discrepancy clinical andor radiological evidence of a fracture
MRI false negative in four patients and bone scan in eight MRI sensitivity 80 and a specificity of 100 Bone scintigraphy had a sensitivity of 100 and a specificity of 90
FRCSOrthcouk
CORR 2009 SepDiagnosing Suspected Scaphoid Fractures A Systematic Review and Meta-analysis Level IIIYin ZG China
Imaging protocols for suspected scaphoid fractures are inconsistent bone scan MRI and CT for diagnosing suspected scaphoid fractures
26 studies The pooled sensitivity specificity natural logarithm of the diagnostic odds ratio and PPV amp NPV were respectively 97 89 478 882 and 003 for bone scan 96 99 660 96 and 004 for MRI and 93 99 611 93 and 007 for CT
MRI is more specific and better for confirming scaphoid fracture
FRCSOrthcouk
Treatment
CORR2007 JulTreatment of acute scaphoid fractures systematic review and meta-analysisYin ZG China
2007 Jul Treatment of acute scaphoid fractures systematic review
and meta-analysis Yin ZG China Operative treatment of acute nondisplaced or minimally
displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization
Operative treatment of acute nondisplaced or minimally displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization however it causes more complications and perhaps a higher risk of scaphotrapezial osteoarthritis There is no evidence from randomized trials to determine whether operative treatment is superior to nonoperative treatment for an acute proximal pole fracture of scaphoid bones
There is insufficient evidence to determine which type of cast should be used in nonoperative treatment of nondisplaced scaphoid fractures
Injury 2009 MarOperative versus nonoperative treatment of acute undisplaced and minimally displaced scaphoid waist fractures--a systematic reviewModi CS Nancoo T Powers D Ho K Boer R Turner SM United Kingdom
Included studies were critically appraised using levels of evidence and RCTs were further appraised using a scoring tool
112 studies 12 included Three level 1 RCTs three level 2 RCTs two meta-analyses one economic analysis and three retrospective studies
Percutaneous fixation may result in faster union rates by approximately 5 weeks and an earlier return to sport and work by approximately 7 weeks over cast treatment
This difference is not seen when comparing ORIF with cast treatment cast treatment results in a higher non-union rate than ORIF this needs to be balanced with the 30 minor complication rate
Manual workers require significantly longer time off work than non-manual workers regardless of the method of treatment ( return to work sooner after ORIF than after cast treatment)
ldquoOperative treatment should be reserved for patients unable to work in a cast and considered for most manual workers and high-level athletesrdquo
FRCSOrthcouk
Conservative treatment of scaphoid nonunion in children and adolescents
Prolonged treatment with cast immobilisation resulted in union of the fracture and an excellent Modified Wrist Score in all patients
D M Weber JBJS Br 2009 Sep
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
CORR 2009 SepDiagnosing Suspected Scaphoid Fractures A Systematic Review and Meta-analysis Level IIIYin ZG China
Imaging protocols for suspected scaphoid fractures are inconsistent bone scan MRI and CT for diagnosing suspected scaphoid fractures
26 studies The pooled sensitivity specificity natural logarithm of the diagnostic odds ratio and PPV amp NPV were respectively 97 89 478 882 and 003 for bone scan 96 99 660 96 and 004 for MRI and 93 99 611 93 and 007 for CT
MRI is more specific and better for confirming scaphoid fracture
FRCSOrthcouk
Treatment
CORR2007 JulTreatment of acute scaphoid fractures systematic review and meta-analysisYin ZG China
2007 Jul Treatment of acute scaphoid fractures systematic review
and meta-analysis Yin ZG China Operative treatment of acute nondisplaced or minimally
displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization
Operative treatment of acute nondisplaced or minimally displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization however it causes more complications and perhaps a higher risk of scaphotrapezial osteoarthritis There is no evidence from randomized trials to determine whether operative treatment is superior to nonoperative treatment for an acute proximal pole fracture of scaphoid bones
There is insufficient evidence to determine which type of cast should be used in nonoperative treatment of nondisplaced scaphoid fractures
Injury 2009 MarOperative versus nonoperative treatment of acute undisplaced and minimally displaced scaphoid waist fractures--a systematic reviewModi CS Nancoo T Powers D Ho K Boer R Turner SM United Kingdom
Included studies were critically appraised using levels of evidence and RCTs were further appraised using a scoring tool
112 studies 12 included Three level 1 RCTs three level 2 RCTs two meta-analyses one economic analysis and three retrospective studies
Percutaneous fixation may result in faster union rates by approximately 5 weeks and an earlier return to sport and work by approximately 7 weeks over cast treatment
This difference is not seen when comparing ORIF with cast treatment cast treatment results in a higher non-union rate than ORIF this needs to be balanced with the 30 minor complication rate
Manual workers require significantly longer time off work than non-manual workers regardless of the method of treatment ( return to work sooner after ORIF than after cast treatment)
ldquoOperative treatment should be reserved for patients unable to work in a cast and considered for most manual workers and high-level athletesrdquo
FRCSOrthcouk
Conservative treatment of scaphoid nonunion in children and adolescents
Prolonged treatment with cast immobilisation resulted in union of the fracture and an excellent Modified Wrist Score in all patients
D M Weber JBJS Br 2009 Sep
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Treatment
CORR2007 JulTreatment of acute scaphoid fractures systematic review and meta-analysisYin ZG China
2007 Jul Treatment of acute scaphoid fractures systematic review
and meta-analysis Yin ZG China Operative treatment of acute nondisplaced or minimally
displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization
Operative treatment of acute nondisplaced or minimally displaced fractures of the scaphoid waist does not provide greater benefits regarding nonunion rate return to work grip strength range of wrist motion or patient satisfaction than cast immobilization however it causes more complications and perhaps a higher risk of scaphotrapezial osteoarthritis There is no evidence from randomized trials to determine whether operative treatment is superior to nonoperative treatment for an acute proximal pole fracture of scaphoid bones
There is insufficient evidence to determine which type of cast should be used in nonoperative treatment of nondisplaced scaphoid fractures
Injury 2009 MarOperative versus nonoperative treatment of acute undisplaced and minimally displaced scaphoid waist fractures--a systematic reviewModi CS Nancoo T Powers D Ho K Boer R Turner SM United Kingdom
Included studies were critically appraised using levels of evidence and RCTs were further appraised using a scoring tool
112 studies 12 included Three level 1 RCTs three level 2 RCTs two meta-analyses one economic analysis and three retrospective studies
Percutaneous fixation may result in faster union rates by approximately 5 weeks and an earlier return to sport and work by approximately 7 weeks over cast treatment
This difference is not seen when comparing ORIF with cast treatment cast treatment results in a higher non-union rate than ORIF this needs to be balanced with the 30 minor complication rate
Manual workers require significantly longer time off work than non-manual workers regardless of the method of treatment ( return to work sooner after ORIF than after cast treatment)
ldquoOperative treatment should be reserved for patients unable to work in a cast and considered for most manual workers and high-level athletesrdquo
FRCSOrthcouk
Conservative treatment of scaphoid nonunion in children and adolescents
Prolonged treatment with cast immobilisation resulted in union of the fracture and an excellent Modified Wrist Score in all patients
D M Weber JBJS Br 2009 Sep
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Conservative treatment of scaphoid nonunion in children and adolescents
Prolonged treatment with cast immobilisation resulted in union of the fracture and an excellent Modified Wrist Score in all patients
D M Weber JBJS Br 2009 Sep
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists a systematic review of outcomesMulford JS Ceulemans LJ Nam D Axelrod TSJ Hand Surg Eur Vol 2009 Apr
motion-preserving salvage procedures for scaphoid nonunion (SNAC) or scapholunate advanced collapse (SLAC)
52 articles SNAC or SLAC for PRC or 4CF both procedures give improvements in pain and subjective outcome measures for
patients with symptomatic and appropriately staged SLAC or SNAC wrists PRC better postoperative range of movement and 4CF nonunion hardware issues and dorsal impingement PRCrisk of subsequent OA significantly higher Grip strength pain relief and subjective outcomes similar in both treatment
groups
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
SNAC scaphoid and triquetral excision combined with capitolunate arthrodesis versus 4-corner (capitate hamate lunate triquetrum) fusion
Hand Surg Am 2009 sept
Clinical Outcomes of Scaphoid and Triquetral Excision With Capitolunate Arthrodesis Versus Scaphoid Excision and Four-Corner Arthrodesis
Gaston RG USA retrospective n=50 patients
radiographs wrist range of motion grip strength VAS and DASH questionnaire Out come same at 3 years fuCLAa lessened need for bone graft harvesting low nonunion rateeasier reduction of the lunate following triquetral excisionavoiding subsequent symptomatic pisotriquetral arthritis
Screw migration however remains a concern with this technique
Level of evidenceIII
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Degenerative arthritis of the wrist proximal row carpectomy versus scaphoid excision and four-corner arthrodesisCohen MS USA J Hand Surg Am 2001
Both PRC and scaphoid excision and 4-corner arthrodesis are motion-preserving options for the treatment of scapholunate advanced collapse arthritis with minimal subjective or objective differences in short-term follow-up evaluations
FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Scapholunate advanced collapse wrist proximal row carpectomy or limited wrist arthrodesis with scaphoid excisionTomaino MM USA J Hand Surg Am 1994
for wrists without capitolunate arthritis PRC avoids the technical demands lengthy postoperative immobilization and risk of nonunion associated with LWF (limited intercarpal arthrodesis with scaphoid excision) but for stage III disease (capitolunate arthritis) pain relief may be unsatisfactory and LWF is recommended
N=24 Retrospective
FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Distal Radial Fracture
FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
REDISPLACED UNSTABLE FRACTURES OF THEDISTAL RADIUSA PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OFTREATMENTM M MCQUEEN C HAJDUCKA C M COURT-BROWN Edinburgh Scotland JBJS Br May 1996 Level 1
A PROSPECTIVE RANDOMISED COMPARISON OF FOUR METHODS OF TREATMENT N=120 ( 30 in each group) 1) remanipulation + forearm cast 652 2) open reduction and bone grafting (McBirnie et al 1995) 3) closed re-reduction and application of a Pennig external fixator removed at 652 4) closed re-reduction and application of a Pennig external fixator as in group 3 but early mobilisation at
352 Radiological results better improvement in angulation of the distal radius Functional results652 3-6 and 12 months no difference Carpal malalignment statistically ndashve effect on functional results
FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Do young patients with malunited fractures of the distal radius inevitably develop symptomatic post-traumatic osteoarthritisD P Forward T R C Davis Nottingham JBJS May 200838 years fu
N=106 adults fracture of the distal radius between 1960-1968 and who were below the age of 40 years at the time of injury
Clinical and radiological assessment at a mean follow-up of 38 years (33 to 42) No patient required a salvage procedure there was radiological evidence of post-traumatic osteoarthritis after an intra-articular fracture
in 68 of patients (27 of 40) (DASH) scores were not different from population norms and function significant relationship between narrowing of the joint space and extra-articular malunion
(dorsal angulation and radial shortening) as well as intra-articular injury grip strength had fallen to 89 of that of the uninjured side in the presence of dorsal
malunion imperfect reduction of these fractures may not result in symptomatic arthritis in the long term
FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Functional Outcomes for Unstable Distal Radial Fractures Treated with Open Reduction and Internal Fixation or Closed Reduction and Percutaneous FixationA Prospective Randomized Trial JBJS Am 2009
Tamara D Rozental USA level 1 N=45 22 CR+ k wire 23 volar plate Both closed reduction with percutaneous pin fixation and open reduction with internal fixation
with use of a volar plate are effective methods for the treatment of dorsally displaced
unstable extra-articular or simple intra-articular fractures of the distal part of the radius Better functional results can be expected in the early postoperative period in association with
open reduction and internal fixation and this form of treatment should be considered for patients requiring a faster return to function after the injury
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Locking plates
A revolution in the management of fractures of the distal radiusN D Downing JBJS 2008 A number of clinical and biomechanicalstudies have demonstrated the advantages of restoring normal anatomy but the number of studies which have used validated patient-derived outcome measures has been few and there are no long-term prospective comparative studies of alternative methods of treatment to guide our management
A comparison between subjective outcome score and moderate radial shortening following a fractured distal radius in patients of mean age 69 years J Hand Surg Eur Vol 2007
Barton found no correlation between moderate shortening (up to 8mm)
and outcome as assessed by the Patient Related Wrist Evaluation at a mean follow-up of 29 months
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Distal radius
2009 Jul Prospective randomised study of intra-
articular fractures of the distal radius comparison between external fixation and plate fixation
Xu GG Chan SP Puhaindran ME Chew WY compare the outcomes of external fixation (EF)
with open reduction internal fixation (ORIF) with plates and screw fixation in the treatment of intra-articular fractures of the distal radius
N=35 after a failure of initial conservative treatment The patients were randomised patients were followed-up at 1 week 3 6 12 and 24 months
Of the 35 patients 5 were excluded Out come not significantly different Complication rates similar
CONCLUSION There is no significant difference in the outcome of intra-articular distal radius fractures treated with either EF or ORIF
Cochrane database2007 Jul Percutaneous pinning for treating distal radial
fractures in adults Handoll HH Vaghela MV Madhok R Edinburg Adult fracture of the distal radiuscompared
percutaneous pinning with conservative treatment or different aspects of percutaneous pinning
CONCLUSIONS Though there is some evidence to support its use the precise role and methods of percutaneous pinning are not established The higher rates of complications with Kapandji pinning and biodegradable materials casts some doubt on their general use
External fixation versus conservative treatment for distal radial fractures in adults
Handoll HH Huntley JS Madhok R Edinburgh There is some evidence to support the use of external
fixation for dorsally displaced fractures of the distal radius in adults Though there is insufficient evidence to confirm a better functional outcome external fixation reduces redisplacement gives improved anatomical results and most of the excess surgically-related complications are minor
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Distal radius fracture
JBJS am 2007 Management of Distal Radial
Fractures Neal C Chen J Jupiter
Prediction of Instability in Distal Radial Fractures
MM McQueen JBJS AM 2006 4000 distal radial fractures were
prospectively recorded over a 55-year period The database was validated by re-examining a sample of it
Complex but fairly accurate in predicting instability
FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Hallux valgus
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Hallux valgus
AHN Robinson Modern concepts in the treatment of hallux valgus JBJS am 2005
Proximal metatarsal orsquomy for HV comparison of outcome for moderate and severe deformities
Okuda R Foot and ankle 2008 Jul N=54 feet fu 30 months Group M (moderate) (24 feet HVAlt= 40 degrees and IMAlt18 degrees)
and Group S (severe) (30 feet HVAgt40 degrees or IMAof 18 degrees or
greater) The prevalence of recurrent hallux valgus (hallux valgus angle of 20
degrees or greater) in Group S was significantly higher than that in Group M (p = 0013
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Hallux valgus
HV associated with age female sex amp components of generalised OA eg nodal OA knee pain big toe pain amp self reported OA
Arthritis rheum 2008 Jun Pre op HVA main radiological predictor for correction Correction rate declines after preop HVA
37 IMA and DMAA have a minor role with HVAlt 37 but may contribute to pre op HVAgt = 37 BMC musculo skeletal disoders 2008 May
Scarf versus proximal closing wedge osteotomy in hallux valgus treatment Arch orthop trauma surg 2008 apr Paczesny L
to evaluate the DMMA as a key factor in choosing between the proximal closing wedge osteotomy and scarf osteotomy 40 feet 32 females aged 13-68 in whom 24 unilateral and 8 bilateral operations had been performed from 24 to 63 months previously
RESULTS There were statistically significant differences between groups in the postoperative hallux valgus angle and in first metatarsal shortening ldquoinverse correlation betn pre op DMAA and IMA improvement after proximal closing wedge orsquomy and +ve correlation after scarf orsquomy
This study confirmed the value of distal metatarsal articular angle assessment
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Hallux valgus
Scarf orsquomy for correction of HV midterm clinical outcomeLipscombe S Molloy A Sirikonda S Hennessy MSJ Foot Ankle Surg 2008 Jul-Aug
Prospective study N=22pts (33 feet) Significant improvement in pain scores from preoperative mean of
2129 +- 110 to 3290 +- 957 at 5 years (P lt 01) was noted and 909 of patients remained satisfied
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Hallux valgus
Distal first metatarsal osteotomy for repair of mild to moderate hallux valgus deformitylt14 degrees IMA
Tonbul M
J Foot and ankle Surg 2008 May
FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Hallux Valgus
Foot Ankle Int 2009 Sep Proximal first metatarsal opening wedge osteotomy with a low profile plate Shurnas PS Watson TS Crislip TW Eighty-four patients (90 feet) underwent PMOW osteotomy with distal
bunionectomy There were 78 patients (93) and 84 (93) feet available for followup Mean followup was 24yrs
The mean preoperative VAS score was 59 (+- 22) compared with a mean postoperative score of 05 (+- 08)
The mean 1-2 IMA preoperatively was 145 (+-33) degrees postop 46 (+- 28) degrees
HVA improved from a mean of 30 degrees to 10 degrees 1 nonunion delayed union mild hallux varus severe hallux varus (2) recurrent
hallux valgus (3) patients (including the nonunion) and no instances of plate Ninety percent of patients reported good to excellent subjective results after the
index surgery a first web space release may result in hallux varus and increased distal
metatarsal articular angle (DMAA) was associated with hallux valgus recurrence
FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Hallux Valgus
Scarf and Akin osteotomies for moderate and severe hallux valgus clinical and radiographic results
Garrido IM Foot Ankle Surg 200814(4)194-203
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Hallux valgus
Postoperative Incomplete Reduction of the Sesamoids as a Risk Factor for Recurrence of Hallux Valgus
Ryuzo Okuda MD Journal of Bone and Joint Surgery (American) 2009 level III
Proximal Metatarsal Osteotomy with Distal Soft-Tissue Correction and Arthrodesis of the Metatarsophalangeal Joint
V James Sammarco JBJS 2007
Juvenile hallux valgus A conservative approach to treatment JA Groiso JBJS AM 1992
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
TREATMENT OF PES PLANUS DEFORMITY Treatment Stage Nonoperative Treatment Operative Treatment I Immobilize (cast boot brace) NSAIDs medial heel and sole wedge orthosis Synovectomy IIA Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Medial displacement calcaneal osteotomy Subtalar arthrodesis IIB Ankle brace (over-the-counter or custom) UCBL orthosis short articulated AFO medial heel and sole wedge orthosis TAL or gastroc slide FDL to navicular transfer Bone options Lateral column lengthening with or without medial displacement calcaneal osteotomy Subtalar arthrodesis III Articulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide IV Nonarticulated AFO custom ankle brace Triple arthrodesis TAL or gastroc slide and deltoid ligament reconstruction AFO ankle-foot orthosis FDL flexor digitorum longus gastroc gastrocnemius NSAIDs nonsteroidal anti-inflammatory drugs TAL
Achilles tendon lengthening UCBL University of CaliforniandashBerkeley Biomechanics Laboratory
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior and Rheumatoid foot
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior Orthopedics 1996May Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon
transfer and calcaneal osteotomy Myerson MS Coriigan J USA
N=32 patients stage-II posterior tibial tendon dysfunction with calcaneal osteotomy and flexor digitorum longus tendon transfer
These 32 patients (29 F 3 Mnd had been symptomatic for an average of 25 years (range 1 to 8 years) before surgical correction
The indication for surgery was the presence of medial foot pain refractory to nonoperative treatments
All patients were examined at a mean of 20 months after surgery AOFAS score improved from a preoperative mean of 48 points (range 23 to 76) to a
postoperative mean of 84 points (range 68 to 92) Most patients (94) experienced pain relief had improvement in the arch of the foot and were
able to wear regular shoes without orthotic support In order to correct deformity and provide substantial relief of foot pain and dysfunction a medial translational calcaneal osteotomy was performed in addition to a flexor digitorum longus tendon transfer for management of stage-II posterior tibial tendon dysfunction
FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Dysfunction of the tendon oftibialis posterior
Review article HJ Trnka JBJA Br 2004 Rosenberg reported that MRI is the best method for imaging the
tendon because of its multiplanar imaging ability and soft-tissue contrast resolution
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
classification
1989 Johnson and Strom described three clinical stages of dysfunction Myerson added a fourth to describe the most severe deformity with valgus collapse of the talus within the ankle
Stage I incorporates tenosynovitis In this stage the tendon is of normal length and symptoms are usually mild to moderate Pain and swelling are present on the medial aspect of the foot Mild weakness and minimal deformity are present
Stage II there is elongation or tearing of the tendon The limb is weak and the patient is unable to stand on tiptoe on the affected side There is secondary
deformity as the midfoot pronates and the forefoot abducts at the transverse tarsal joint The subtalar joint remains mobile
Stage III is characterised by a more severe deformity and a fixed hindfoot Stage IV there is a valgus deformity of the talus with early degenerative
changes of the ankle
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
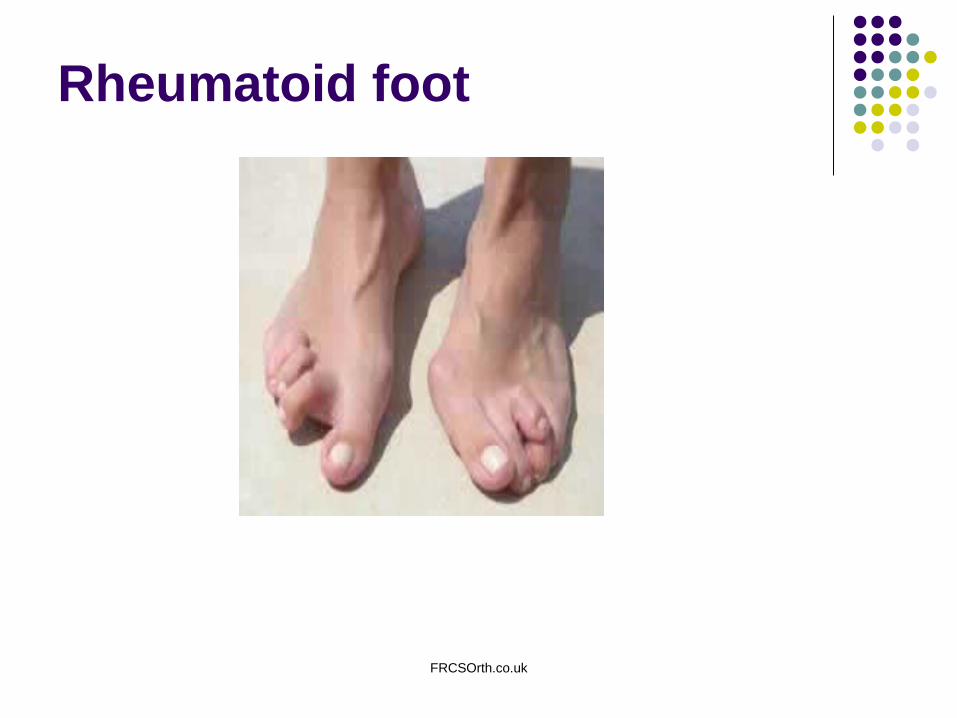
FRCSOrthcouk
Rheumatoid foot
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Rheumatoid foot
K Trieb review article JBJSBr 2005 Management of foot in Rhematoid Arthritis Autoimmune systemic inflammatory disease FgtM 31 ARA diagnostic criteria T- lymphocyte mediated auto immune response via HLA-II Locus Non ndash op pressure relieving foot wear Soft for rigid and rigid for to support and
limit joint movement for flexible deformity Op forefoot 90 MTP J HV planter displacement of metatarsal heads varus little toe dislocation of PIP J
dordally migration of planter fat pad distally large bursae intr-extr imbalance- clawing + ve Gaensslen test
Kellerrsquos 1st MTP J fusion Weilrsquos osteotomy ndashsynovectomy+ ext tendon lengthening
Modified Fowlerrsquos procedure talonavicular fusion triple fusionankle fusionreplacement
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Long-Term Results of the Modified Hoffman Procedure in the Rheumatoid Forefoot JBJS am 2005
average of five and a half years following thirtyseven consecutive forefoot arthroplasties performed in twenty patients
a technique involving resection of all five metatarsal heads satisfactory to excellent in the short term (six weeks postoperatively) and
no patient sought additional surgical treatment for the feet A superficial infection subsequently developed in two feet and two feet had delayed wound-healing
At an average of 649 months postoperatively the average AOFAS forefoot score was 645 points and the average hallux valgus angle was 223deg There were no reoperations
Conclusions Resection of all five metatarsal heads in patients with metatarsalgia and hallux valgus associated with rheumatoid arthritis can be a safe procedure that provides reasonable if rarely complete relief of symptoms
Rheumatoid foot
FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Ankle TAR Arthrodesis
FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
TARBP STAR
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
TAR
A randomised controlled trial of two mobile-bearing total ankle replacements P L R Wood C Sutton JBJS Br Jan 2009 Buechel-Pappas (BP) and the Scandinavian Total Ankle Replacement (STAR min 36 months
fu similar in design consisting of three components with a meniscal polyethylene bearing which
was highly congruent on its planar tibial surface and on its curved talar surface However the designs were markedly different with respect to the geometry of the articular surface of the talus and its overall shape
six-year survivorship of the BP = 79 STAR =95 replacement be advised with caution in the presence of varus or valgus deformity and that it
should not be performed when the deformity exceeds 15deg
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
TAR
MEDIUM-TERM RESULTS IN 200 SCANDINAVIAN TOTAL ANKLE REPLACEMENTS P L R Wood C Sutton JBJS Br Sept2008 prospective study of 200 total ankle replacements at a single-centre using the Scandinavian
Total Ankle Replacement 24 ankles (12) revised 20 by fusion and four by further replacement and 27 patients (33 ankles) died
5 year survival was 933 and 10 year survival 803 Subtalar arthritis may continue to progress after total ankle replacement
Brodsky gait analysis superior compared to Ankle arthrodesis Schneiderbauer31 infection rate (n=386TAR)
How Successful are Current Ankle Replacements A Systematic Review of the Literature
Gougoulias N Khanna A Maffulli N CORR July 2009 deep infection up to 46 Level IV
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Ankle arthrodesis
Arthroscopic ankle arthrodesis Gougoulias NE Agathangelidis FG Parsons SW Foot Ankle Int 2007 Jun N=78 48 ankles had minor deformity (group A) 30 ankles had a varus or valgus deformity of more than 15 degrees (maximum 45 degrees)
(group B) 21months Fusion 47 48 (979) group A and in 29 of 30 (967) ankles group B The outcome was graded as very good in 792 (38 feet) in group A and 80 (24 feet) in
group B fair in 188 (9 feet) in group A and 167 (5 feet) in group B and poor in one ankle in each group (p = 068)
The arthroscopic technique offered high fusion rates and low morbidity Deformity correction was achieved with good results
Patients with poor bone quality or post traumatic deformity may require more rigid fixation
FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Anterior plate supplementation increases ankle arthrodesis construct rigidity Tarkin Foot Ankle Int 2007 Feb
Cadeveric study Compared to screws alone anterior plate supplementation increases construct rigidity and
decreases micromotion at the ankle fusion interface Arthrodesis of the ankle in the presence of a large deformity in the coronal plane PLR Wood R Smith N=23(25 ankles) Open arthrodesis with cannulated 65 mm screws 2425 primary union Rx of choice for severe deformities with arthritis fu 20 mths AOFAS pain score 10 pre op ndash 352 post op
Ankle arthrodesis
FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Diabetic foot
Surgical aspects of the diabetic foot
AHN Robinson
JBJS Br 2009 1)DM with complications ulcer infection charcoat neuroarthopathy 2) Routine problem with coincedental DM
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Diabetic foot
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Diabetic foot
Neuropathy The cause is thought to be an ischaemic insult secondary to damage to the vasa nervorum
the sensory neuropathy and not vascular disease is the primary cause of most foot conditions in diabetic patients
Sensory motor autonomic Assessment by 128Hz tuning fork 10g Semmes Weinstein monofilament Vasculopathy large small vessels and microcirculation affected arteriosclerosis
45after 20yrs DM -nt pulse further Ix should be requested
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
ulceration Wegner Brodsky classification Treatment protocol for the diabetic foot as based on the depth-ischaemia classification Classification Definition Treatment Depth 0 At-risk foot no ulceration Patient education accommodative footwear regular clinical
examination 1 Superficial ulceration not infected Off-loading with total contact cast walking brace or
special footwear 2 Deep ulceration exposing tendons or joints Surgical debridement wound care off-loading
culture-specific antibiotics 3 Extensive ulceration or abscess Debridement or partial amputation off-loading culture-
specific antibiotics
Ischaemia A Not ischaemic B Ischaemia without gangrene Non-invasive vascular testing and vascular reconstruction with
angioplastybypass C Partial (forefoot) gangrene Vascular reconstruction and partial foot amputation
FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
neuroarthropathy
FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Diabetic foot
Total contact cast Exostectomy Arthrodesis Avulsion of TA non op Rx
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Diabetic foot
Lengthening of the Achilles Tendon in Diabetic Patients Who Are at High Risk for Ulceration of the Foot DAVID G ARMSTRONG JBJS am 1999
peak pressures on the plantar aspect of the forefoot are significantly reduced following percutaneous lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
Effect of Initial Weight-Bearing in a Total Contact Cast on Healing of Diabetic Foot Ulcers J Bone Joint Surg Am Dec 2004 Charles L Saltzman
Moderate early weight-bearing retards healing of plantar ulcers only minimally in patients with diabetes mellitus treated with total contact casts Allowing patients to walk immediately after placement of a total contact cast may improve their acceptance of this form of therapy Only excessive walking during the first twenty-four or forty-eight hours after cast application is likely to prolong the duration of cast treatment
Arthrodesis as an Early Alternative to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot
Sheldon R Simon J Bone Joint Surg Am Jul 2000
FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Ankle fractures in DM
Mc Cormack RG Leith JM J B JS Br Jul 1998 N=26 Ankle fractures in
diabetics COMPLICATIONS OF SURGICAL MANAGEMENT
Level III Complications gt40 Six major complications
Johnson NWB 312 PWB with cast 312 then brace upto 1 year for ankle
K B Jones K A Maiers-Yelden USA Ankle fractures in patients with diabetes mellitusJ B J S Br Apr 2005
N=42 21 DM 21 DM comorbidities DM comorbidities 47
complication rate DM without comobrbidities no
diff with control Longer immobilization reqd the comorbidity of a history of
Charcot neuroarthropathy was independently associated with every complication measured
FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Kienbockrsquos
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
ASPECTS OF CURRENT MANAGEMENTKienboumlckrsquos disease F SchuindSEslamiP Ledoux JBJS Br 2008
There is no strong evidence to support any particular form of treatment Many patients are improved by temporary immobilisation of the wrist which does not stop the progression of carpal collapse
Radial shortening may be the treatment of choice in young symptomatic patients presenting with stages I to III-A of Kienboumlckrsquos disease and negative ulnar variance
Anatomical difference (TFCC and joint with capitate hamate)and blood supply YIXpattern single volardorsal several volar dorsal no central anastomosis with anastomosis(Lee) Hulten noted increased incidence (74 wrists with ulnar ndashve variance )
13 rd load thru Radiolunate jt Adult male manual worker 20-40yr-ve ulnar variance Lichtman classification aetio exact cause not known the consequence of impaired venous outflow
FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you

FRCSOrthcouk
Kienbockrsquos
Rx non op op Radial shortening ulnar lengthening Vascularised graftulnar plus hand (dorsal metacarpal arteriovenous Pedicle)or by dorsal aspect of the radius via pedicles from the fourth and fifth
extensor compartments(ICSRA) PRCFusion Assessment of the different published studies indicates that radial shortening
offers durable pain relief and may improve grip strength but does not offer a cure Radial shortening less satisfactory results in patients over the age of 30 J Hand Surg Am 2009 Jan Vascularized bone grafting for treatment of
Kienboumlcks disease Elhassan BT Shin AY
FRCSOrthcouk
Thank you
FRCSOrthcouk
Thank you





























