Embed Size (px)
Citation preview

Infection Prevention & Control
Annual Report 2011 - 2012

1.0 Executive Summary Cwm Taf Local Health Board continues to make significant progress in reducing Health Care associated infections. The implementation of a systematic process of surveillance and swift action to prevent and control infections acquired in hospital has had a notable impact in reducing the number of infections. Feedback is given regularly to Directorates on their alert organism trends, line associated bacteraemia and performance on Infection Prevention and Control Team (IPCT) verification audits.
1.1 The rate of Clostridium difficile infections is the lowest in Wales at
2.77/1000 admissions compared to a rate of 12.88/1000 admissions in 2008. Further measures were introduced last year and national targets for the reduction of Clostridium difficile infection were again surpassed with the HB achieving a reduction of about 40% over the significant reduction achieved the previous year. MRSA bacteraemia was reduced by a further 20%. A reduction of 48.7% was achieved in 2010-2011.
1.2 The 1000 Lives Plus initiative used to introduce two care bundles in
2010-2011: the Catheter Associated Urinary Tract Infection (CAUTI) bundle to decrease catheter associated urinary tract infections and the Peripheral Vascular Catheter (PVC) bundle to improve peripheral intravenous line management, have progressed and spread through several wards at both ends of the Health Board (HB). This work has achieved recognition in Wales and a short film of the team was presented at the 1000 lives conference in March 2012.
1.3 The Antimicrobial stewardship programme remains underdeveloped
without an antimicrobial pharmacist in post. In the past two years a reduction in the use of cephalosporins and fluoroquinolones has resulted in the increased prescribing of other antibiotics. Co-amoxiclav usage appears to have increased both in primary and secondary care within Cwm Taf and overall in Wales. An Antibiotic Resistance Alert was released in December 2011 on an ‘Increase in co-amoxiclav resistance in E. coli from blood cultures and in urinary coliforms’ with an action plan to minimise risk.
1.4 The large number of bed days lost this year was mainly due to the increased number of Norovirus outbreaks in 2011-12. Insufficient isolation facilities at some hospitals and the high bed occupancy rate contributed to prolonged closures and the increased number of bed days lost. It is recommended that side room availability and usage is reviewed along with bed occupancy rates.
Page 2 of 17

2.0 Infection Prevention & Control Arrangements Cwm Taf Health Board endorses the Welsh Government (WG) principle that infection prevention and control is the responsibility of all staff within the organisation. They are supported by the infection prevention and control team. Infection Prevention Control Committee The function of the Infection Prevention Control Committee is split into two groups:
i) Operational Group Infection Prevention & Control Operational Group (IPCOG)
Meetings are held bi monthly and deal with the operational detail of Infection prevention and control. The Water Group and Decontamination Group are sub committees of the Operational Group and provide reports to the Group.
ii) Strategic Group
Infection Prevention & Control Strategic Group (IPCSG)
Meetings are held quarterly, this is at Director level and has partnership involvement from Public Health Wales and both Local Authorities and provides strategic direction.
The meetings are chaired by the Executive Nurse Director or her deputy. The terms of reference and membership of the groups are clearly defined Infection Prevention and Control Team (IPCT) The Infection Prevention and Control Team (IPCT) sits within the Pathology Directorate and reports to the Executive Nurse Director or her deputy on infection prevention and control (IP&C) matters. The Executive Nurse Director reports directly to the Chief Executive and the Board. The Lead Infection Prevention and Control Doctor (LIPCD) and the lead Infection Prevention And Control Nurse (LIPCN) liaise closely with the Assistant Director of Nursing delegated with the responsibility for IP&C. The IPCT hold weekly meetings at both acute hospital sites to act on surveillance and trend data. Trend data analysis of alert organisms/conditions highlights areas for improvement and this data is shared weekly with clinical areas. IPCT staff: The current staff within the IPCT are as follows:
• The Lead IPCD 0.4 WTE (fixed) • Deputy IPCD 0.2 WTE (variable) • Lead IPCN 1.0 WTE • Senior IPCN 1.0 WTE • Nursing staff 4.0 WTE • IPC co-ordinators 1.8 WTE
Page 3 of 17

All Consultant Microbiologists advise the IPCT on acute infection control issues. Activities of the IPCT include:
• Surveillance of alert organisms • Provision of surveillance data and verification audit data to Directorates. • Analysis of C.difficile infections • Outbreak management • Policy development • Clinical advice. • Support to directorate IP&C groups. • Education and Training • Audit • Advice and support to Occupational Health, Estates and Facilities. • Leadership in saving lives initiative. • Communication and advice to the public • Complaints and legal services • Involvement in Infection Prevention and Control Committee (IPCC): 3.0 Report on the 2011 Point Prevalence Survey (PPS) of Antimicrobial Usage, Healthcare Associated Infections and Medical Device Usage During November 2011, Cwm Taf Health Board participated in the first standardised Europe wide point prevalence survey of HAI (healthcare associated infections), AMU (Antimicrobial usage) and MDU (Medical device usage). Though this provides a snapshot, the data can be useful to focus interventions to reduce the burden of disease providing there is an understanding of the limitations of the survey. Cwm Taf HB had an HAI prevalence of 1.6% which was lower than the average in Wales.
Page 4 of 17

Page 5 of 17
2011 Prevalence Survey of Healthcare Associated Infection (HAI) and Antimicrobial usage
Invasive Device Utilisation for Cwm Taf Health Board
4.0 Healthcare associated infections: statistics and performance
4.1 C. difficile Infection (CDI): The C. difficile rate for Cwm Taf in hospital in-patients over 65 years of age is 2.77/1000 admissions. The average rate for Wales is 7.18/1000 admissions. Cwm Taf HB has the lowest rate in Wales and surpassed a 40% reduction on the baseline year. Improvements continue from the 38.5% reduction achieved in 2010-2011. A root, cause analysis report is sent to all Directorates on a regular basis for appropriate actions to be taken.

Total Number of Clostridium difficile in inpatients aged 66+
for the period 01/04/11 to 31/03/12 Progress against baseline year (April 2010 to March 2011)
4.2 Staphylococcus aureus (S. aureus) bacteraemia A significant reduction was achieved for S. aureus bacteraemia. Methicillin Resistant Staphylococcus Aureus (MRSA) bacteraemia was reduced by a further 20%. A reduction of 48.7% was achieved in 2010-2011.
Numbers of MRSA Bacteraemias
for the period 01/04/11 to 31/03/12 Progress against baseline year (April 2010 to March 2011)
Page 6 of 17

Numbers of MSSA Bacteraemias for the period 01/04/11 to 31/03/12
Progress against baseline year (April 2010 to March 2011)
5.0 Surgical Site Infection(SSI) Surveillance Surveillance of surgical site infections (SSI) using standardised methods allows Health Boards to analyse their SSI data to improve the quality of care and benchmark allowing comparison between different hospitals.
5.1 Orthopaedics As displayed in the table below, the SSI rate for both mandatory procedures in Cwm Taf is below the All Wales SSI rate. The SSI rate in Royal Glamorgan Hospital has reduced significantly compared with the same time period in 2010-2011. A task and finish group was set up in November 2011 to address the increase in SSI’s and ward based surveillance was set up to monitor all SSI’s identified post operatively. Training was also provided by the Welsh Healthcare Associated Infection Programme (WHAIP) team to correctly identify infections and a standardised reporting mechanism was introduced.
Page 7 of 17

Page 8 of 17
5.2 Caesarean Section A significant reduction in SSI was achieved in March 2011 following an increased incidence of SSI in late 2010. The SSI’s are monitored within the Directorate Infection Prevention & Control Group meeting. The overall SSI rate has increased again in 2011-2012 which the Directorate is investigating with support from the IPCT.

Page 9 of 17
5.3 Critical Care Surveillance 5.3.1 Central Venous Catheter (CVC) Surveillance Mandatory central venous catheter care (CVC) surveillance is performed throughout critical care units in Wales. Until compliance with the surveillance is known, it is difficult to compare rates across units in Wales. Cwm Taf had an overall HELICS defined CVC infection rate of 0.57/1000 critical care catheter days compared to 0.7/1000 critical care catheter days in 2010-2011.
Page 10 of 17
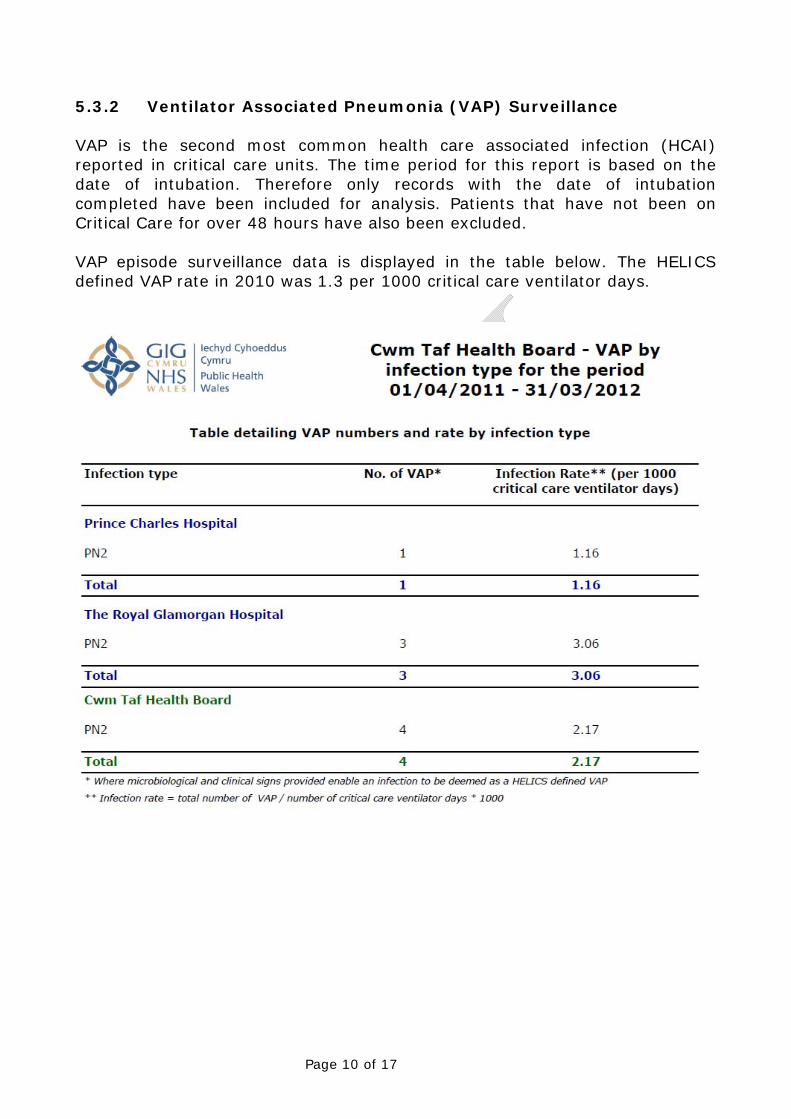
5.3.2 Ventilator Associated Pneumonia (VAP) Surveillance VAP is the second most common health care associated infection (HCAI) reported in critical care units. The time period for this report is based on the date of intubation. Therefore only records with the date of intubation completed have been included for analysis. Patients that have not been on Critical Care for over 48 hours have also been excluded.
VAP episode surveillance data is displayed in the table below. The HELICS defined VAP rate in 2010 was 1.3 per 1000 critical care ventilator days.

6.0 IP&C Policies Approved in 2011 – 2012 The following Infection Prevention and Control policies/procedures and guidelines were approved at the Infection Prevention & Control Groups and were endorsed at the Quality Patient Safety and Public Health Committee/Clinical Governance Committee. All staff have access to these documents via the Intranet.
No. Title IPCS Approval
QPS Approval
IPC04 Hand Hygiene Procedure April 2011 July 2011 IPC06 Linen Policy April 2011 July 2011 IPC08 Notification Infectious Diseases &
Notification Process October 2011 N/A
IPC10 Management of Blood & Body Fluid Spillages
April 2011 July 2011
IPC11 Water Cooler & Ice Machine Guidelines
October 2011 N/A
IPC15 Creutzfield Jakob Disease January 2012 N/A IPC17 Laboratory Support to IPC January 2012 N/A IPC23 Tuberculosis October 2011 January 2012 IPC25 Measles Policy April 2011 July 2011
The following documents are related to IPC and have been endorsed by the Infection Prevention and Control Groups.
No. Title IPCS Approval
RM19 Needlestick (sharps) injuries management from occupational exposure procedure
April 2012
RM21 Waste Policy April 2012 RM25 Think Clean and Tidy Guidelines April 2012 RM26 Cleaning Procedure Office & Department Areas April 2012 FAC21 Cleanliness Standards Roles, Responsibility and
Audit Tool Procedure April 2012
FAC40 Wheelchair Cleaning and Maintenance Procedure April 2012 7.0 Internal Audit Programme and performance All clinical areas are required to perform weekly hand hygiene and environmental audits. Directorates must monitor and act on their audit findings and report to the IPCOG. The IPCT have a rolling programme of verification audits and also audit clinical areas if there is an increase in alert organisms or conditions. Verification audit reports are cascaded to Directorate leads. Audits are repeated in areas of poor performance supported by training if required.
Page 11 of 17

Page 12 of 17
The graphs below show cumulative results of IPCT verification audits across staff groups in secondary care. 7.1 Hand Hygiene Audits
Total No. of Staff Groups Compliant with Appropriate Hand Hygiene Practices
01/04/11 – 31/03/12
514
468
208
117
363
323
274
203
0
100
200
300
400
500
600
TOTA
L N
O. O
BSE
RVA
TIO
NS
Nurses Opportunities
NursesCompliant
DoctorsOpportunities
DoctorsCompliant
HCA'sOpportunities
HCA'sCompliant
Others Opportunities
OthersCompliant
STAFF GROUPS
CWM TAFHBIP&C HAND HYGIENE VERIFICATION AUDITS (01/04/11 TO 31/03/12)
Percentage of Staff Groups Compliant with Appropriate Hand Hygiene Practices
Staff Group Compliance
Score Nurses
Doctors
Health Care Assistants
Others
2010 - 11 81% 50% 81% 65% 2011 -12 91% 56% 89% 74%
Breakdown of hand hygiene practices compliant by Directorate
Directorate Merthyr & Cynon Rhondda Cynon Taf 2010-11 2011-12 2010-11 2011-12
Medicine 58% 72% 69% 88% Surgery 71% 76% 88% 91% Orthopaedics 76% 69% 100% 90% Anaesthetics 64% 82% 77% 100% Women 70% 75% 100% 65% Children 65% 73% 98% 100% Rehabilitation 82% 93% 97% 92%

7.2 Environmental Cleanliness Audits
Merthyr & Cynon Rhondda Cynon Taf
DIRECTORATE 2010/11 2011/12 2010/11 2011/12 Medicine 91% 93% 88% 89% Surgery 90% 88% 91% 91% Anaesthetics 91% 96% 95% 93% Women & Child 86% 82% 86% 87% Mental Health Unit 77% 72% 97% 80% Rehab 96% 91% 91% 86%
8.0 Antimicrobial Stewardship Results of the Point Prevalence Survey in November 2011 show that the prevalence of antimicrobial prescribing in hospitals within the HB is 26.0%.
The usage data appears to indicate there is widespread and possible unnecessary use of co-amoxiclav where other agents are available. The Antimicrobial Guide for the Management of Adults in Secondary Care at the Cwm Taf Health Board approved by the Medicine Management Committee in June 2010 is in the final stages of review after extensive consultation. Antimicrobial stewardship remains underdeveloped; however with adequate resources antimicrobial stewardship could greatly improve outcomes for patients and infection rates i.e. highlighting the benefits. 9.0 Decontamination A new Decontamination Lead was appointed in 2011-12. The Balanced Score Card approach is adopted to establish the current situations and risk matrix to ensure the higher risk for the Health Board were addressed. Several areas of risk highlighted during 2010 or earlier are still to be addressed. Bench top sterilizers are still in use. The requirement for scoping all endoscopes within the Health Board remains a priority. There is an urgent need for a comprehensive Decontamination Procedure. 10.0 Education & Training Activities The Training department was tasked to coordinate and organise training which would be delivered by specialist IPCT staff. IP&C induction is run twice yearly for junior medical staff.
Page 13 of 17

The table below identifies the number of staff trained between 1st April 2011 to 31st March 2012. Training is mandated for Registered Practitioners and ancillary staff. The attendance of training has improved and has been supported by providing group specific training at a local level to encourage attendance of staff at both acute and community hospitals. The plans for extending invitation to primary care users to utilise Health Board training has been implemented.
Total monthly numbers of staff who attended IPC Training in 2011 - 2012
MONTH Total No. April 231 May 153 June 142 July 130 August 107 September 85 October 208 November 56 December 72 January 20 February 41 March 72 Total 1317
11.0 1000 Lives Plus 11.1 Catheter Associated Urinary Tract Infections (CAUTI) The CAUTI care bundle was introduced to three pilot wards in Dewi Sant Hospital in 2010 and following successful implementation has been rolled to various wards/directorates within the Health Board. The success has been well documented in these areas and plans to spread to other areas will be developed. The work undertaken by the organisation was presented in an All Wales meeting and recognition was given to the work and progress made. 11.2 Peripheral Vascular Cannula (PVC) Limited progress has been made since the PVC care bundle was introduced to three pilot wards in 2011. Education and support provided by the Infection Prevention and Control Team has improved compliance with the use of the care bundle and outcome and process measures. Clinical engagement is essential in order to improve and standardise infection prevention and control practices in relation to PVC management. Plans to spread to other areas will be developed.
Page 14 of 17

12.0 Outbreaks and Incidents The tables below identify a significant increase in the number of bed days lost due to ward closures/bay restrictions in 2011/12 compared to 2010/11. Ward Closures & Bay restrictions 2010 – 2011
2011 – 2012
No. of Outbreaks (Due to Suspected/Confirmed Viral Diarrhoea and Vomiting)
23
79
No. of Patients 204 435
No. of Staff 30 140
No. of Bed Days lost 508 1532
Cwm Taf Health Board No. of Norovirus Outbreaks 2010 - 2011 2011- 2012 Confirmed 6 18 Suspected 17 42 Breakdown of all hospital Norovirus outbreaks (confirmed or suspected) by site Rhondda Cynon Taff Merthyr & Cynon 2010 - 2011 9 14 2011 - 2012 57 22 The large number of bed days lost this year was mainly due to the increased number of Norovirus outbreaks in 2011-12. Insufficient isolation cubicles contributed to prolonged bay closures at the RGH site. A high bed occupancy rate made it very difficult to manage outbreaks as there was little leeway to move or isolate patients. It is recommended that side room availability and usage particularly at the RGH site is reviewed along with bed occupancy rates. 12.1 Other incidents
• Pseudomonas An increase in the isolation of Pseudomonas on ward 20 RGH between August and November 2011 occurred. 11 patients were affected with 90 bed days lost. Meetings were held to determine the cause and actions were taken to address the issues identified.
Page 15 of 17

• Methicillin Sensitive Staph. Aureus (MSSA)
MSSA increased in SCBU in RGH during December 2011 where 8 babies were colonised or infected. Appropriate investigations and actions were swiftly taken.
13.0 Influenza There has been no significant activity affecting secondary care for influenza during this financial year. 14.0 Review of isolation facilities A point prevalence study was performed in 2010 to determine the isolation facilities available within Cwm Taf Health Board. At that time, single room accommodation formed 22% of the total bed capacity available within Cwm Taf HB. The audit highlighted that patient placement was often inappropriate due to the shortage of isolation rooms. A review of the isolation facilities available was not undertaken in 2011-2012 but following ward refurbishments at Prince Charles Hospital and commissioning of the new Ysbyty Cwm Cynon hospital, the isolation facilities available within Cwm Taf have increased. The refurbished wards at Prince Charles Hospital have 8 single rooms per ward and each ward at Ysbyty Cwm Cynon has 13 single rooms. Due to ward closures there has been a reduction in single rooms on the Royal Glamorgan site. 15.0 Legionella/Water Subgroup Legionella risk assessment for the HB was undertaken two years ago by an external company- Hydrops with a report produced on the risks. The highlighted risks are being worked through using the balance score card system. It currently indicates seven high risks out of twenty seven identifiers. These will be actively progressed by Estates. A Policy for the Management of Legionellosis was in the final stages of preparation. The Senior Estates Manager confirmed that he is currently developing a procedural document which will provide information on all aspects of the planned preventative maintenance requirements for Legionella control and emergency situations such as loss of water supplies, reduced hot water temperatures, high total viable counts and Legionella counts. The Policy for the Management of Water Coolers & Machines was approved.
Page 16 of 17

Page 17 of 17
16.0 Theatres The main theatre ventilation plants in PCH are being revamped to allow supply fan drive motors to be taken out of the main airstream. An Annual verification report on theatres at RGH produced by the NHS Wales Shared Services – Facility services in February 2012 identified several areas of concern. The maintenance condition of all of the plant room equipment was rated as ‘POOR’ for general condition and maintenance quality and ‘AVERAGE’ for compliance with minimum standards. The recommendation to produce and implement an action plan to bring up the theatre suites and ventilation plant to the current standard is to be addressed by Estates (Facilities) Department. Dr Bonny Banerji, Lead Infection Prevention and Control Doctor Mrs Bethan Cradle, Senior Infection Prevention and Control Nurse Acknowledgement to Mrs Julie Donovan, Infection Prevention and Control Co-ordinator for providing the local data and help with drawing up the document Acknowledgement to the WHAIP team for providing the surveillance data.





























