Embed Size (px)
Citation preview

Arch Orthop Trauma Surg (2009) 129:1511–1519
DOI 10.1007/s00402-009-0855-3TRAUMA SURGERY
Fractures of the scapula: long-term results after conservative treatment
Markus D. Schofer · Axel C. Sehrt · Nina Timmesfeld · Sabine Störmer · Horst R. Kortmann
Received: 21 August 2008 / Published online: 21 March 2009© Springer-Verlag 2009
AbstractIntroduction The aim of this study was to determine thelong-term prognoses for conservatively treated fractures ofthe scapula.Materials and methods Ascertainment of functional long-term results in 50 patients treated for a total of 51 scapularfractures in a retrospective cohort study with an averagefollow-up period of 65 months.Results The breakdown of these scapular fractures was asfollows: simple (22%) and fragmented (51%) fractures ofthe scapular body, fractures through the scapular neck(41%), fractures of the coracoid process, spine and acro-mion of the scapula (10%) and glenoid fractures (8%). In17 of these cases of scapular fracture two or more typeswere present. At the follow-up examination a restrictedrange of movement was found in all directions. In abduc-tion, Xexion and external rotation the range of motion onthe aVected as against the unaVected side was signiWcantlyrestricted, but the observed restriction did not substantiallyaVect the functional results. The Constant score on theaVected side was 79 points, with 23% very good, 51%
good, 20% satisfactory and 6% poor results. Isokinetic test-ing carried out on both sides for comparison revealed lowerpeak torque values and lower mean power output in allplanes of movement, and lower speeds on the aVected side.There was a correlation between extent of restriction onmovement and diminution of isokinetic muscular strength.Determination of the external rotation is recommended as aclinical test value, as it highlights signiWcant deWcits both inrestriction of range of motion and in isokinetic test mea-surements. The outcome of treatment was not inXuenced byfracture type, associated injuries or handedness.Conclusion After conservative treatment, scapular frac-tures heal with a good functional result despite measurablerestrictions.
Keywords Scapula fracture · Conservative treatment · Isokinetic · Shoulder · Long-term result
Introduction
The Wrst description of a scapular fracture was published in1805 by Desault [10]. As shown by Newell und Wilson inlarge patient populations, scapular fractures are basicallyrare, accounting for only 0.4–1% of all bone injuries [24,32]. Fractures of the scapula account for 3–5% of injuriesof the shoulder girdle [16, 26, 30]. As a rule they are sus-tained as the result of marked force applied in the course ofhigh-velocity trauma and lead to multiple injuries [1, 15,16, 19, 26, 30]. The incidence in this multiply injured popu-lation is 5–10% [13, 31]. Scapular fracture is suggestive ofsevere thoracic trauma in a multiply traumatised patient [2,8]. Treatment of the main, life-threatening, injury can be sourgent in such cases that the associated scapular fracture isoverlooked or neglected [24]. The serious nature of the
M. D. Schofer (&) · S. StörmerDepartment of Orthopaedics, University Hospital Marburg, Baldingerstraße, 35043 Marburg, Germanye-mail: [email protected]
A. C. Sehrt · H. R. KortmannDepartment of Trauma and Orthopaedic Surgery, Berufsgenossenschaftliche Unfallklinik Duisburg (BGU-Duisburg), Großenbaumer Allee 250, 47249 Duisburg, Germany
N. TimmesfeldInstitute of Medical Biometry and Epidemiology, Philipps-University Marburg, Bunsenstraße 3, 35037 Marburg, Germany
123

1512 Arch Orthop Trauma Surg (2009) 129:1511–1519
associated injuries means that the lethality is high inpatients with fractures of the scapula [2].
The objective of the present study was a follow-upexamination of patients who had undergone conservativetreatment for scapular fractures, with special reference tothe functional long-term results. This was intended toinclude objective measurement of the range of motion andthe development of strength. The inXuence of variousdiVerent factors, especially the type of scapular fracture, onfunctional results was also to be examined.
Materials and methods
Study design
This was a retrospective cohort study with evidence level 4.
Patients
The central patient register of the trauma unit was searchedfor all patients entered in it from 1990 to 1999 with a diag-nosis of scapular fracture. This search yielded 144 patients,including 7 whose scapular fractures were treated surgi-cally. The 137 patients who had undergone conservativetreatment were invited to attend for a follow-up investiga-tion.
Follow-up investigation
The follow-up investigation was conducted by doctors whohad not been involved in the patients’ treatment.
At the beginning of the follow-up investigation a historywas elicited and a clinical examination including determi-nation of the range of motion in both shoulders with a goni-ometer (neutral-null method) was carried out.
The circumference of both upper extremities was mea-sured for comparison; a measuring tape was used to takemeasurements with the arms dependent and in a standard-ised manner at Wve points: the upper arm 15 cm above theradial condyle of the humerus, the elbow at the level ofradial condyle of the humerus, the lower arm 10 cm belowthe radial condyle of the humerus, the wrist and the mid-hand (without the thumb).
Patients self-rated their shoulder pain in one of Wve cate-gories: totally pain-free, mild pain occasionally and onlywhen the shoulder was heavily stressed, pain but only whenthe shoulder was heavily stressed, pain even at normal day-to-day stress levels, and constant pain.
Shoulder function was recorded in both upper extremi-ties with the Constant score [6, 7]. An isokinetic examina-tion of the shoulders followed. This involved using theBiodex III (Biodex Medical Systems, Shirley, NY) to
examine both shoulders of each patient, while seated, inthree planes of movement (extension/Xexion, abduction/adduction, internal/external rotation in neutral position) andat two diVerent speeds (60° and 180°/s) during a predeter-mined number of movement cycles. The lower speed isclose to a static maximum strength measured in variousdiVerent joint positions. The higher speed represents thefunctional speeds of movement in the shoulder joint anddocuments the maximum output possible [9, 27]. The isoki-netic data analysed in this study were peak torque in new-ton metres (N m) and mean power output in watts (W).Following a standardised warming-up phase, the measure-ments of the unaVected shoulder were taken Wrst, initially ata speed of 60°/s and then at 180°/s. Subsequently, analo-gous measurements were taken on the aVected side. Therewas always a rest period of 30 s between any two individ-ual measurements. Standard values for isokinetic testresults are diYcult to determine in the case of the shoulder,as the output parameters depend heavily on body weight,age, sex and general physical condition. The aVected sidewas compared with the intact contralateral side for eachpatient.
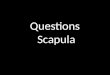
A radiologist evaluated the X-ray pictures taken at thetime of the accident in each case, and the scapular fractureswere classiWed according to the Euler and Habermeyer sys-tem [13, 14]. This classiWcation breaks down the fracturesinto fractures of the scapular body (A), fractures of the cor-acoid process, spine and acromion of the scapula (B), frac-tures of the scapular neck (C), joint fractures (D) andcombined fractures also involving fractures of the humeralhead (E). There are also further subdivisions within theseWve groups (Fig. 1). As we were interested mainly in evalu-ating the function, no new X-ray examination was carriedout for the follow-up investigation.
Fig. 1 ClassiWcation of scapular fractures according to Euler and Hab-ermeyer [13, 14]
123

Arch Orthop Trauma Surg (2009) 129:1511–1519 1513
Statistics
The descriptive statistics included calculation of means andstandard deviations and recording of the minimum andmaximum values. To test for diVerences, unless speciWedotherwise we used the t test for random and/or bound sam-ples, or in the case of nominally scaled data, the Chi-squaretest, the selected level of signiWcance being P < 0.05 ineach case. We checked for correlations with the aid of thePearson coeYcient of correlation and the appropriate testfor correlation.
Results
Patients
Of the 137 patients who had undergone conservative treat-ment for scapular fractures, Wve had died of their associatedinjuries and two from causes unrelated to their accidents. Afurther two patients had suVered high-level paraplegia as aresult of their accidents, so that it was not possible to exam-ine the upper extremities in a way that would have alloweda correct estimate of the functional results in either of thesecases. Twenty had moved away without leaving forwardingaddresses, and 58 were not prepared to take part in the fol-low-up investigation. In all, then, 50 patients with a total of51 scapular fractures were available for inclusion in the fol-low-up investigation (Table 1). This means a follow-up rateof 37% of all conservatively treated patients identiWed,which means that a bias in the selection cannot be deWnitelyexcluded.
One right-handed patient had sustained bilateral scapularfractures and was not included when questions concerningside-to-side comparison were considered.
In 38 cases (76%), the accidents had occurred while thepatients were at work, while in the remaining 12 (24%) theaccidents had happened in the patients’ free time. TraYcaccidents accounted for most of the accidents (54%).
Fifteen patients (30%) were injured while travelling in carsor trucks; 12 patients (24%) had accidents while travellingby motorcycle or pushbike. A fall from a considerableheight had caused the scapular fracture in 16 patients(32%). Six patients (12%) had been hit by falling objects,and 1 (2%) had suVered an electric shock.
None of the patients reported pre-existing shoulder dis-ease. X-rays taken directly after the accident showed nosign of shoulder osteoarthritis.
Evaluation of the physical stress at work at the time ofthe follow-up investigation as deWned by the Association ofGerman Pension Insurance Funds [Verband deutscherRentenversicherungsträger] gave the following breakdown[18]:
– 18 Patients (36%) did physically light work– 8 Patients (16%) did moderately heavy physical work– 24 Patients (48%) did heavy physical work
Fitness for work
The duration of the patients’ unWtness for work was28.53 § 15.62 weeks for those who normally did lightphysical work, 34.81 § 23.43 weeks for those normallyengaged in moderately heavy work, and 37.54 §14.63 weeks for those who normally did heavy work. ThediVerences were not signiWcant.
Types of fracture
When the fractures were classiWed according to the Eulerand Habermeyer system it was not always possible toassign patients to a single fracture category. Allocation to asingle fracture type was possible in 34 of our cases of scap-ular fracture. In each of the other 17 patients with scapularfractures a combination of fracture types was present, sothat for each of these more than one fracture type wasrecorded (Table 2). In a total of 11 shoulders (22%) therewere simple fractures of the scapular body (type A1); 26fractures (51%) were multiple-fragment fractures of thescapular body (type A2); in 21 shoulders (41%) the frac-tures were through the scapular neck (type C2); in 5 shoul-ders, fractures of the coracoid process, spine and acromionof the scapula (type B); and 4 of the scapular fractures (8%)were glenoid fractures (type D). One patient was found tohave a fracture of the scapular neck associated with tears ofthe coracoclavicular and coracoacromial ligaments (typeC3b).
In the further course of the evaluation only the four fre-quent fracture types A1, A2, A2 + C2 and C2 were consid-ered in group comparisons. For the remaining fracture typesthe case numbers were too low for statistical evaluation(Table 2).
Table 1 Description of patients followed up in study population
No. of patients 50
Handedness 48 right- and 2 left-handed
No. of scapular fractures 51
Male/female patients 44/6
Average age at time of accident 44 (20–82) years
Average age at time of follow-up investigation
50 (29–85) years
Follow-up period 65 (13–120) months
Scapular fracture on dominant side 22
Scapular fracture on non-dominant side 29
123

1514 Arch Orthop Trauma Surg (2009) 129:1511–1519
Associated injuries
In 8 patients (16%), the scapular fracture was the soleinjury. The remaining 42 patients (84%) had a total of 176substantial associated injuries. The average number of asso-ciated injuries for the entire study group of 50 patients was3.5 per patient, while that exclusively for the 42 patientswho had such injuries was 4.2 per patient. For example,ipsilateral fractures of the ribs were detected in 22 patients,contralateral fractures of the ribs, in 8 patients, pneumo- orhaemothorax, in 14 and ipsilateral fractures of the clavicle,in 14 patients. Associated injuries to the ipsilateral shouldergirdle and hemithorax were found in 34 patients (68%).
Conservative treatment
The scapular fracture was treated conservatively in each ofthe patients in our study group. The type of conservativetreatment was selected by the doctor in attendance in eachcase, depending on the type of scapular fracture and on thepatient’s associated injuries. In 25 cases a Gilchrist bandwas applied to immobilise the shoulder. The period ofimmobilisation in these patients was 10 § 6.36 (2–28) days. In 25 patients no treatment speciWcally intendedto immobilise the shoulder was performed.
Five patients had not had any physiotherapy prescribed.In a further 7 it is not clear when their physiotherapy wasstarted. The remaining 38 patients started physiotherapyafter 15 § 4.79 (1–36) days and had an average of38.78 § 8.32 (10–90) therapy sessions.
None of the patients had undergone a surgical operationon the injured shoulder during the follow-up period.
Pain
At the time of the follow-up examination 14 patients (28%)were completely free of pain; 9 patients (18%) reportedoccasional mild pain only, and only when the shoulder washeavily stressed; 16 (32%) complained of pain only whenthe shoulder was heavily stressed; 9 patients (18%) com-plained of pain at normal day-to-day levels of stress to theshoulder and 2, of constant pain in the shoulder. We foundno diVerences in frequency of pain that could be linkedwith the fracture type or with associated injuries to shouldergirdle and thorax.
Circumference
Determination of the circumference of the patients’ upperextremities at diVerent points revealed no signiWcant diVer-ences in circumference between the dominant and non-dominant sides or between the aVected and unaVectedsides.
Range of motion
According to the neutral-null method, the range of motionof the aVected shoulder was signiWcantly smaller than thatof the contralateral shoulder in all directions except internalrotation in the neutral position. The side-to-side diVerencewas particularly marked in abduction, Xexion and externalrotation: abduction P < 0.001; adduction P = 0.009; XexionP < 0.001; extension P = 0.003; external rotation in neutralposition P < 0.001; internal rotation in neutral positionP = 0.302; external rotation in 90° abduction P < 0.001;internal rotation in 90° abduction P = 0.011 (Fig. 2).
When the four most frequent fracture types were com-pared no correlation was discovered between fracture typeand direction or degree of restriction of the range ofmotion.
Shoulder function reXected in constant score
Shoulder function was assessed at an average of78.80 § 4.45 points on the aVected side and an average of94.88 § 1.77 points on the unaVected side (out of a possi-ble 100 points in each case). The average side-to-sidediVerence was 16.08 § 4.42 points. The total score attainedwas signiWcantly (P < 0.001) lower on the injured side.
The Constant score showed very good results on theaVected side in 23% of the patients, good in 51%, satisfac-tory in 20% and poor in 6%. On the unaVected side 76% ofthe patients had very good shoulder function, 22%, goodand 2%, satisfactory shoulder function. The patient with thebilateral multiple-fragment fractures of the scapular bodyhad the maximum score of 100 points on each side.
Table 2 Distribution of the 51 scapular fractures by fracture type
The four most common types are in bold
ClassiWcation after Euler and Habermeyer [13, 14] No. of patients
A1 (simple corpus fracture) 8
A1 + B3 1
A1 + C2 1
A1 + E 1
A2 (fragmented corpus fracture) 13
A2 + B2 + C1 + D1 + D3 1
A2 + C2 10
A2 + C2 + D1 + D3 1
A2 + D2a + D3 1
B3 3
C1 1
C2 (fracture of neck of scapula) 8
C2 + D1 + D3 1
C3b 1
123

Arch Orthop Trauma Surg (2009) 129:1511–1519 1515
No signiWcant diVerences between the four most fre-quently encountered fracture types were detected in totalscore in the aVected shoulder, scores on the individual com-ponents of the Constant score, or side-to-side diVerences inthe total number of points scored.
The 31 patients with scapular fractures and associatedinjuries to the shoulder girdle and/or thoracic injury had nosigniWcantly diVerent Constant scores from those withoutsuch associated injuries.
Patients’ handedness had no inXuence on the Constantscore. For the aVected shoulder, statistical testing did notdemonstrate any correlation between patient age and Con-stant score. On the unaVected side of the body there was anegative correlation, with a Pearson coeYcient of correla-tion (r) of r = –0.43 (P = 0.002).
The Constant score was signiWcantly (P = 0.017) betterin patients who had fewer than 30 physiotherapy sessionsthan in patients with more than 30 sessions.
Isokinetic testing
One patient broke oV the isokinetic investigation because ofsevere pain, so that 49 patients were evaluable and 48patients were considered in the side-to-side comparison.
The average test values for the peak torque and the meanpower output achieved were lower on the aVected than onthe unaVected side at both speeds and in all planes of move-ment (Table 3). Statistically signiWcant diVerences in peaktorque were found for external rotation at a speed of 60°/s(P = 0.007) and at 180°/s (P = 0.026), and also for extension
at a speed of 60°/s (P = 0.032). There were signiWcant side-to-side diVerences in mean power output in external rota-tion at both speeds (60°/s: P = 0.002; 180°/s: P < 0.001)and in both extension (P = 0.014) and adduction(P = 0.016) at a speed of 180°/s (Table 3).
The mean percentage side-related deWcit in the isokinetictest results for all planes of movement investigated andcompared to check for diVerences between the aVected andunaVected side amounted to 12.30 § 5.36% and5.80 § 4.99% for the peak torque at 60° and 180°/s, respec-tively, and to 17.48 § 9.33% at 60°/s and 26.37 § 8.93%for mean power output at 180°/s, respectively.
Thomas et al. recommend converting the torque duringabduction to Constant scores and vice versa to make thetwo methods comparable [27]. A torque of 50 N m inabduction is equivalent to the maximum Constant score of25 points for strength measured. Following conversion ofthe peak torque values measured at a speed of 60°/s thePearson coeYcient of correlation between these values andthe Constant scores for power measurement was 0.885(P < 0.002).
To highlight any possible link between restrictions inmovement and restrictions of strength in the correspondingplane of movement, correlations were sought between theside-to-side diVerences in the isokinetic peak torque valuesand those in the ranges of motion. This showed a correla-tion for abduction (P < 0.02), adduction (P < 0.01), exten-sion (P < 0.01), Xexion (P < 0.002), and internal rotation(P < 0.01) at the lower speed of 60°/s. In these planes ofmovement the limitation of muscular strength worsened
Fig. 2 Average (and 95% conW-dence intervals) ranges of mo-tion and side-to-side diVerences in range of motion in shoulders in all directions considered
123

1516 Arch Orthop Trauma Surg (2009) 129:1511–1519
with increasing limitation of the range of movement. Nosuch eVect was detected for external rotation or at thehigher speed of 180°/s.
Correlations were found between the side-to-sidediVerence in the Constant score and the isokinetic testresult for the peak torque at 60°/s (r = 0.758, P < 0.002)and for the mean power output at speeds of both 60°/s(r = 0.814, P < 0.002) and 180°/s (r = 0.789, P < 0.002).No correlation was detected for peak torque at 180°/s(r = 0.251).
Fracture type, concomitant injuries and handedness wereall found not to have any inXuence on the results of theisokinetic investigation.
Discussion
As shown by a review of studies published by Zlowodzkiet al. in 2006 on the treatment of scapular fractures, up tothat point there had been no prospective investigations onthis topic [33]. All 22 of the publications identiWed by theauthors are retrospective studies or small, retrospective caseseries. We are also unaware of any prospective studies onthe conservative treatment of scapular fractures in therecent literature.
The proportion of work-related falls causing the relevantaccident is higher in our patient population than in the liter-ature [1, 3, 13, 15, 17, 25, 26, 31]. At 54%, traYc accidentsas the cause are in the middle of the range of 32–80%reported in the literature [1, 3, 31].
Our patient population’s average age of 44 years is at thehigh end of the range of average ages (25–46 years)reported in other publications [1, 3, 15, 16, 25, 31]. The sexdistribution agrees well with the reports in the literature [1,11, 15, 16, 22, 25, 31].
As in our patient population, so also in the literaturefractures of the scapular body and neck are the most fre-quently reported scapular fractures [1, 5, 25]. Severalgroups have found a sequence with fractures of the scapularbody followed by those of the scapular neck, glenoid, acro-mion and coracoid process of the scapula in declining orderof frequency, which is in keeping with our results [1, 4, 22,29, 31]. This fracture type distribution can be regarded astypical.
The associated injuries in our patient population weresimilar in type and frequency to those reported in the litera-ture [1, 5]. In our sample 84% of the patients had associatedinjuries, as against reports of 56–98% in the literature [1, 5,25]. Ipsilateral fractures of the ribs were the most commonassociated injury in our population, aVecting 44% of ourpatients, and are also the associated injury most frequentlyreported in the literature [1, 5, 25, 31].
Overall, then, the patient population we examined waslargely typical of patients with scapular fractures.
The conservative treatment recommended in the litera-ture is generally physiotherapy starting soon—perhaps aweek—after the accident [5, 23, 31]. In our patient popula-tion the time to start of physiotherapy, 15 § 4.8 days, wasin excess of this. When the inXuence of physiotherapy wasassessed, signiWcantly better shoulder function (as reXected
Table 3 Mean (and 95% conW-dence intervals) peak torque and mean power output at various speeds
Speed Peak torque (N m) Mean power output (W)
60°/s 180°/s 60°/s 180°/s
Abduction
AVected side 44.18 § 3.76 46.63 § 3.90 25.80 § 3.43 41.32 § 6.15*
UnaVected side 48.18 § 3.98 47.80 § 4.54 30.33 § 3.76 51.46 § 7.19*
Adduction
AVected side 40.70 § 4.95 50.67 § 6.94 20.25 § 4.14 20.89 § 6.50*
UnaVected side 47.21 § 5.59 55.25 § 6.70 25.98 § 4.39 35.31 § 9.36*
Flexion
AVected side 50.75 § 5.35 50.27 § 5.07 29.90 § 4.63 46.04 § 7.75
UnaVected side 55.68 § 5.56 53.26 § 4.97 33.79 § 4.54 54.25 § 7.69
Extension
AVected side 45.95 § 6.78* 55.83 § 7.56 23.91 § 5.62 22.62 § 8.78*
UnaVected side 56.41 § 7.45* 63.18 § 8.50 31.62 § 6.48 41.75 § 12.8*
External rotation
AVected side 16.88 § 2.21* 16.79 § 1.69* 8.54 § 1.56* 12.09 § 2.39*
UnaVected side 21.03 § 2.07* 19.17 § 1.47* 12.18 § 1.66* 19.15 § 2.80*
Internal rotation
AVected side 29.59 § 3.77 30.27 § 3.93 18.01 § 3.07 29.91 § 6.25*
UnaVected side 34.11 § 3.87 34.28 § 3.68 22.18 § 3.38 40.71 § 7.00**SigniWcant side-to-side diVerence
123

Arch Orthop Trauma Surg (2009) 129:1511–1519 1517
in the Constant score) was found in patients who had hadfewer than 30 sessions than in those who had had more than30 sessions of physiotherapy. Certainly this should not beinterpreted as an indication that more physiotherapy neces-sarily leads to worse shoulder function. Rather we canassume that when good shoulder function is achieved quitesoon the physiotherapy is quickly broken oV, while whenfunction remains poor the physiotherapy is continued forlonger, without however being able to compensate fully forthe poorer function.
Ada und Miller showed that 70% of patients complainedof pain at rest following scapular fractures. In view of thesmall number of cases there is no justiWcation for conclud-ing that there is a link between frequency of pain and frac-ture type [1]. Following conservative treatment of scapularand ipsilateral clavicular fractures, Edwards et al. and vanNoort et al. showed that about half of their patients werefree of pain by the time of their follow-up examinations[12, 28]. Wilber und Evans showed that conservative treat-ment of fractures of the body, neck and spine of the scapulawas followed by fracture healing and freedom from shoul-der pain. In a small series of scapular fractures aVecting theacromion, coracoid and glenoid, shoulder pain persisted in5 of 6 cases [31]. In our patient population the proportion ofpatients who were free of pain during day-to-day activitieswas higher, at 78%, than reported in the literature. As inMcGahan et al.’s study, it was not possible to detect anycorrelation between pain and fracture type [21]. Nor couldany correlation be detected between shoulder pain and thepresence of associated injuries to the shoulder girdle or tho-rax on the same side, so that it is possible that the associ-ated injuries examined in this study do not have anyinXuence on the development of shoulder pain in the caseof scapular fractures treated conservatively.
In all planes of movement examined the average rangeof movement achieved in the aVected shoulder was signiW-cantly smaller than that on the unaVected side, abduction,Xexion and external rotation being more markedly aVectedthan the other directions. The average limitations of move-ment on the aVected side were clinically at a level that doesnot indicate any functional restrictions in day-to-day activi-ties. In other studies better results were recorded for shoul-der mobility. Lindholm and Levén found free shouldermovement in 54 patients after conservative treatment forscapular fractures mostly aVecting the scapular body andneck [20].
Reports in the literature linking limitations on movementwith diVerent fracture types vary. As in the present study,McGahan et al. found no correlation between fracture typeand persisting restricted movement [21]. Other authors, incontrast, do indicate a correlation between fracture type andrestriction of movement. Ada and Miller, on the basis of astudy in 113 patients, report no persisting restricted move-
ment in any of them, even after badly dislocated fracturesof the scapular body, whilst in the case of fractures of thescapular spine and dislocated fractures of the scapular necka restricted abduction capacity was frequently found [1].Wilber und Evans studied 40 patients with a total of 41scapular fractures [31]. The 30 patients with fractures ofbody, neck and spine of the scapula recovered freemovement. Of 6 patients followed up after fractures of theacromion, coracoid or glenoid, only 1, who had had a non-dislocated fracture of the acromion, recovered free move-ment [31].
Shoulder function as reXected in the Constant score wassigniWcantly poorer on the aVected side, with 79 points,than on the uninjured side (95 points). Neither fracture typenor concomitant injuries were found to inXuence the Con-stant score. There are few studies in the literature in whichshoulder function after conservative treatment of scapularfractures has been noted with a Constant score. Goodresults after conservative treatment of scapular neck frac-tures are described by two working groups, with Constantscores of 79 and 90 points, respectively [4, 29]. Edwardset al. report remarkably good results with an average Con-stant score of 96 in 20 patients who had conservative treat-ment after scapular and clavicular fractures on the sameside (“Xoating shoulder”) [12]. These results are better thanthose recorded even for the uninjured shoulder in ourpatient population. In a multi-centre study with 28 patients,after conservative treatment of Xoating shoulder a Constantscore of 76 was achieved [28].
The further literature on conservatively treated scapularfractures reports on function as assessed according to indi-vidually set up criteria or limits itself to a descriptiveassessment of the clinical condition, so that no comparisonof results is possible. Edeland et al. found no restrictedfunction in 61% of their 18 cases of scapular fracturetreated conservatively [11]. McGinnis and Denton reportedgenerally very good and good results in 73% of their casesof scapular fracture after conservative treatment [22].Nordqvist and Petersson examined 68 patients who hadundergone conservative treatment for fractures of the scap-ular body, neck and spine, 75% of whom achieved a goodtreatment outcome and 22%, a satisfactory outcome, whilein 3% the result was poor [25].
The observation that the Constant score declines asexpected with advancing age of the patient only for theunaVected side should therefore be interpreted as an indica-tion that the injury has had a greater inXuence than that ofadvancing age.
Isokinetic testing is a precise and objective method ofevaluating limitations of the motor function of a joint. Incontrast to isometric measurements of strength, as in thecase of the Constant score, for example, isokinetic testinghas the advantage of determining the strength in a dynamic
123

1518 Arch Orthop Trauma Surg (2009) 129:1511–1519
manner over almost the entire range of movement. Thehigh-level investment in terms of equipment, acquisitioncost and staV limits general application of these methods inroutine practice. The literature does not include any compa-rable results of isokinetic measurements following conser-vative treatment of scapular fractures.
The isokinetic measurements indicate lower peak torquevalues and mean power outputs on the injured than on theuninjured side in all planes of movement examined at boththe lower and the higher angular velocity. Not all of thesediVerences were statistically signiWcant, but they do suggestrestricted function of the injured shoulder. As in the case ofthe restrictions of movement observed, on isokinetic testingshows that the range of movement on the external rotationwas markedly restricted in the aVected shoulder, which wasnot uniformly so for the other planes of motion. Externalrotation can therefore be recommended as a clinical testvalue, as it seems to be the most susceptible plane of move-ment.
As shown by analysis of the percentage side-related deW-cit in the isokinetic test results, the sequelae of scapularfractures become obvious in the form of restrictions ofmean power output in movements at functional speed(180°/s).
The results recorded in our study and those published inthe literature indicate that fracture type, concomitant inju-ries and handedness have no inXuence on treatment out-come [1, 2, 21, 22, 25, 29].
The correlation between the Constant score and theisokinetic test results for the aVected side and the non-aVected side indicates a proportional link between the testvalues. The correlation between the Constant score forstrength and the peak torque in abduction at a speed of 60°/s conWrms this. It seems therefore that it is not necessary toperform complicated isokinetic testing routinely for thepurpose of recording the clinical assessment of strength.
The retrospective design of the study, the inhomoge-neous clinical pictures, the low follow-up rate, the widescatter of time to follow-up and the lack of a control groupare weaknesses of this study and of those available in theliterature.
The level of fracture dislocation was not determined inour study or in other available studies. To determine this, astandardised CT examination would be necessary for exam-ple. Such images were not available for our retrospectivegroup. The extent to which the level of fracture dislocation,particularly of type C and D fractures, inXuenced the out-come can not be answered in this study.
In our retrospective group we documented the scapulafractures and associated injuries. As we were mainlyinterested in evaluating the function, no new X-ray examin-ations were carried out for the follow-up investigation.None of the patients reported pre-existing shoulder disease.
X-rays taken directly after the accident showed no sign ofshoulder osteoarthritis. We compared the aVected shoulderand the unaVected shoulder. Therefore, we attributed thelimited range of motion and shoulder function mainly to thescapula fracture.
Conclusion
After conservative treatment of scapular fractures the func-tional result is good despite quantiWable restrictions. Deter-mination of the external rotation can be recommended as aclinical test, as this shows up signiWcant deWcits both inrange of movement and in isokinetic test results. We foundno indication that type of associated injuries or handednesshad any inXuence on treatment outcome; nor was there anystatistically conWrmed inXuence of fracture type on treat-ment outcome in this patient population. Studies in largerpatient populations are needed for comprehensive investi-gation of the divergent results in the literature.
ConXict of interest statement There is no conXict of interests.
References
1. Ada JR, Miller ME (1991) Scapular fractures. Analysis of 113 cas-es. Clin Orthop Relat Res 269:174–180
2. Armstrong CP, Van Der Spuy J (1984) The fractured scapula:importance and management based on a series of 62 patients. Inju-ry 15:324–329. doi:10.1016/0020-1383(84)90056-1
3. Bauer G, Fleischmann W, Dussler E (1995) Displaced scapularfractures: indication and long-term results of open reduction andinternal Wxation. Arch Orthop Trauma Surg 114:215–219.doi:10.1007/BF00444266
4. Bozkurt M, Can F, Kirdemir V et al (2005) Conservative treatmentof scapular neck fracture: the eVect of stability and glenopolar an-gle on clinical outcome. Injury 36:1176–1181. doi:10.1016/j.inju-ry.2004.09.013
5. Butters KP (1998) The scapula. In: Rockwood CA Jr, Matsen FA-III (eds) The shoulder. Saunders, Philadelphia, pp 391–427
6. Constant CR (1991) Assessment of shoulder function. Orthopade20:289–294
7. Constant CR, Murley AH (1987) A clinical method of func-tional assessment of the shoulder. Clin Orthop Relat Res214:160–164
8. Da Thompson, Flynn TC, Miller PW et al (1985) The signiWcanceof scapular fractures. J Trauma 25:974–977
9. Davies GJ (1985) A compendium of isokinetics in clinical usageand rehabilitation techniques. S & S Publishers, La Crosse
10. Desault PJ (ed) (1805) A treatise on fractures, luxations and otheraVections of the Bones. Fry and Kammerer, Philadelphia
11. Edeland HG, Zachrisson BE (1975) Fracture of the scapular notchassociated with lesion of the suprascapular nerve. Acta OrthopScand 46:758–763
12. Edwards SG, Whittle AP, Wood GW 2nd (2000) Nonoperativetreatment of ipsilateral fractures of the scapula and clavicle. J BoneJoint Surg Am 82:774–780. doi:10.1302/0301-620X.82B5.11311
13. Euler E, Habermeyer P, Kohler W et al (1992) Scapula fractures–classiWcation and diVerential therapy. Orthopade 21:158–162
123

Arch Orthop Trauma Surg (2009) 129:1511–1519 1519
14. Euler E, Rüedi T (1996) Skapulafraktur. In: Habermeyer P,Schweiberer L (eds) Schulterchirurgie. Urban & Schwarzenberg,Munich, pp 261–272
15. Hardegger F (1984) Treatment of fractures of the scapula. Unfallh-eilkunde 87:58–66
16. Hardegger FH, Simpson LA, Weber BG (1984) The operativetreatment of scapular fractures. J Bone Joint Surg Br 66:725–731
17. Ideberg R, Grevsten S, Larsson S (1995) Epidemiology of scapularfractures. Incidence and classiWcation of 338 fractures. Acta Ort-hop Scand 66:395–397
18. Kolenda KD (1998) Social medicine evaluation and advice for pa-tients with coronary heart disease. Dtsch Med Wochenschr123:741–747. doi:10.1055/s-2007-1024048
19. Leutenegger A, Ruedi T (1993) Fractures of the scapula and inju-ries of the acromioclavicular joint. The traumatized shoulder andits sequelae. Z Unfallchir Versicherungsmed 86:22–26
20. Lindholm A, Leven H (1974) Prognosis in fractures of the bodyand neck of the scapula. A follow-up study. Acta Chir Scand140:33–36
21. McGahan JP, Rab GT, Dublin A (1980) Fractures of the scapula.J Trauma 20:880–883. doi:10.1097/00005373-198010000-00011
22. McGinnis M, Denton JR (1989) Fractures of the scapula: a retro-spective study of 40 fractured scapulae. J Trauma 29:1488–1493.doi:10.1097/00005373-198911000-00006
23. Mckoy BE, Bensen CV, Hartsock LA (2000) Fractures about theshoulder: conservative management. Orthop Clin North Am31:205–216. doi:10.1016/S0030-5898(05)70141-3
24. Newell ED (1927) Review of over 2000 fractures in seven years.South Med J 20:644–648
25. Nordqvist A, Petersson C (1992) Fracture of the body, neck, orspine of the scapula. A long-term follow-up study. Clin OrthopRelat Res 283:139–144
26. Schmidt M, Armbrecht A, Havemann D (1992) Results of surgicalmanagement of scapula fractures. 78th Annual Meeting of theSwiss society of accident surgery, occupational diseases, 4–5 Sep-tember in Olten. Z Unfallchir Versicherungsmed 85:186–188
27. Thomas M, Dieball O, Busse M (2003) Normal values of theshoulder strength in dependency on age and gender–comparisonwith the constant, UCLA, ASES scores and SF36 health survey. ZOrthop Ihre Grenzgeb 141:160–170. doi:10.1055/s-2003-38662
28. Van Noort A, Te Slaa RL, Marti RK et al (2001) The Xoatingshoulder. A multicentre study. J Bone Joint Surg Br 83:795–798.doi:10.1302/0301-620X.83B6.10806
29. Van Noort A, Van Kampen A (2005) Fractures of the scapula sur-gical neck: outcome after conservative treatment in 13 cases. ArchOrthop Trauma Surg 125:696–700. doi:10.1007/s00402-005-0044-y
30. Wiedemann E (2004) Fractures of the scapula. Unfallchirurg107:1124–1133. doi:10.1007/s00113-004-0892-x
31. Wilber MC, Evans EB (1977) Fractures of the scapula. An analy-sis of forty cases and a review of the literature. J Bone Joint SurgAm 59:358–362
32. Wilson PD (1938) Experience of the management of fractures anddislocations (based on an analysis of 4390 cases) by staV of thefracture service MGH JB Lippincott, Boston
33. Zlowodzki M, Bhandari M, Zelle BA et al (2006) Treatment ofscapula fractures: systematic review of 520 fractures in 22 case se-ries. J Orthop Trauma 20:230–233. doi:10.1097/00005131-200603000-00013
123









![Conservative Approach to Unilateral Condylar Fracture in a … · 2016-10-09 · of condylar fractures [7]. It appears that pediatric condylar fractures could be managed by closed](https://img.dokumen.tips/doc/110x75/5f48360e47a39a42e102f2f1/conservative-approach-to-unilateral-condylar-fracture-in-a-2016-10-09-of-condylar.jpg)