Embed Size (px)
Citation preview

History of Neuropsychology
Dr. Durgesh K. Upadhyay Assistant Professor
Department of Psychology Mahatma Gandhi Kashi Vidyapith, Varanasi - 221002
4/2/2020 DKU - MGKVP
1

What is Neuropsychology?
Neuropsychology
Study of normal, brain-behaviour relationships
Some reasonable questions
How does the brain normally give rise to behaviour?
Which structures are involved in perceiving, interpreting and responding to the world?
Which structures are essential vs. peripheral?
How are signals received, transmitted and compiled to generate perceptions, thoughts and actions?
How are these signals transmitted and interpreted between structures?
Has relied heavily on lesion method
4/2/2020 DKU - MGKVP
2

Neuropsychology is the study of the relation between brain function and behaviour. (Kolb & Whishaw, 1996)
Neuropsychology is a bridging discipline that draws on material from neurology, experimental psychology and even psychiatry.
The term ‘neuropsychology’ was used as a subtitle in Hebb’s influential book, The Organisation of Behaviour: A Neuropsychological Theory, published in 1949
Kolb and Whishaw’s Fundamentals of Human Neuropsychology and Lezak’s Neuropsychological Assessment in 1980 and 1983 respectively.
4/2/2020 DKU - MGKVP
3

Subdisciplines
Experimental neuropsychology
Concerned with the purely academic aim of analysing the intricate relationships between normal brain structure and action, and is, perhaps, interested in the clinical effects of brain damage
Cognitive neuropsychology
Seeks to understand the neuroanatomical and neuro-functional correlates of discrete cognitive processes and to analyse the micro-processes involved in everyday cognitive functions
Clinical neuropsychology
Concerned with the assessment and rehabilitation of people with disturbed function consequent upon brain injury, illness and trauma
4/2/2020 DKU - MGKVP
4

5000 years ago in the Middle East - Heart was the organ of thinking and other mental processes - Brain as a ‘behaviour control centre’ (the brain hypothesis)
Heart is the seat of mental processes, and the brain’s principal role is to cool blood – Aristotle
Hippocrates and Plato both had some understanding of brain structure, and attributed various aspects of behaviour to it.
1st c. AD Rome – Physician Galen undermined the ‘heart hypothesis.’
For reasons that are never entirely clear, the knowledge and understanding of these early writers was lost or forgotten for the next 1500 years or so of European history.
4/2/2020 DKU - MGKVP
5

The renewed interest in rationalism and science that accompanied the Renaissance in Europe in the 15th and 16th centuries prompted scientists of the day to revisit the brain and to try to establish the functions of particular brain structures.
Descartes (1664), argued that the pineal gland is the point of interaction of the mind and body.
Gall (1758–1828) readily accepted that the brain rather than the heart was the control centre for mental function, and, with Spurzheim, the two made many important discoveries about the anatomy of the brain, its connections with the spinal cord, and its ability to control muscles.
4/2/2020 DKU - MGKVP
6

Micro models, are based on specific aspects of neuropsychological function, e.g. how we recognise faces.
In contrast, macro models take a broader perspective and attempt to provide an overview of how the brain works to process a wide variety of functions.
4/2/2020 DKU - MGKVP
7

Localisationist view was put forward by Franz Josef Gall towards the end of the eighteenth century (Boring, 1929).
The first person to identify the commissures, e.g. corpus callosum-the dense wedges of axons that allow communication between the two brain hemispheres.
Gall is credited with providing the first full account of loss of language (aphasia) linked to brain damage.
4/2/2020 DKU - MGKVP
8

Localization & Lateralization of Brain Function
The Brain is the only body organ to exhibit both localisation and lateralisation of function.
Localization = Different areas of the brain do different things.
Lateralization = Each brain hemisphere is adapted to certain functions better than the other.
4/2/2020 DKU - MGKVP
9

Franz Josef Gall (1758-1828) Cranioscopy, or phrenology
Size + shape cranium = Size + shape brain
Mental abilities innate and fixed
Level of development of ability reflection of size of cerebral organ
4/2/2020 DKU - MGKVP
10

Interest in phrenology gradually spread widely, receiving royal support when Queen Victoria had her children’s heads measured and analysed.
4/2/2020 DKU - MGKVP
11

The French scientist Pierre Flourens (1794-1867) provided the first scientific evidence that led people to question the value of phrenology.
The degree of behavioural impairment is more closely linked to the amount of damage than to its location
Critiques
Worked with pigeons and chickens, which are now known to have almost no cortex.
His behavioural measures assessed activities unrelated to Gall and Spurzheim’s faculties.
His surgical procedure was imprecise.
4/2/2020 DKU - MGKVP
12

Interest in Aphasia
French physicians Bouillaud’s work was reported in 1825, and Dax’s in 1836, yet little interest was shown until Auburtin (who happened to be Bouillaud’s son-in-law) described the same work at a conference in 1861 also attended by Paul Broca (1824-1880).
Patients who had lost the use of language after brain damage to the left side, often became paralysed in the right side of their bodies too, despite no apparent loss in intelligence.
4/2/2020 DKU - MGKVP
13

A few days later, Broca met Monsieur LeBorgne, a patient who became known as Tan because this was almost the only sound he could utter. However, Tan could understand speech well and could, for example, follow quite complicated instructions, although he was also paralysed on his right side.
Tan had suffered damage to the same area of cortex (the left frontal region)
Post-mortem data
The region of brain (part of the left frontal cortex) he described is now known as Broca’s area.
4/2/2020 DKU - MGKVP
14

In 1874 Carl Wernicke described two additional forms of aphasia that were distinct from Broca’s type.
Fluent or Sensory or Posterior or Wernicke’s Aphasia – Problems in understanding spoken and written language
Conduction or Associative Aphasia – intact auditory comprehension, fluent (yet paraphasic) speech production, but poor speech repetition
Paraphasia refers to unintended syllables, words, or phrases during the effort to speak
4/2/2020 DKU - MGKVP
15

Hughlings Jackson (Taylor, 1933) had an alternative theory, which was hierarchical in its structure. Father of English neurology Brain is organised into three levels within a hierarchy according to the assumed phylogenetic
evolution of the structures. The most basic level was ‘the spinal cord and cerebellum’ The next level was basal ganglia being referred to as a motor region Finally the highest level was the prefrontal cortex and sensory cortical areas such as the
occipital lobe. A lesion might result in negative or positive symptoms.
4/2/2020 DKU - MGKVP
16

Alexandra Luria and the Functional Systems Model
Russian neuropsychologist Functional systems model is outlined by Luria (1973) in his translated book,
The working brain. Different areas of the brain are specialised to carry out particular roles, but
these specialised roles or units are not sufficient on their own to produce a function - Integration
Functional systems?? For example, memorising requires not just the hippocampus for storing new
memories but also other brain areas for selecting to-be-remembered information, and others that act as a store for the new information.
4/2/2020 DKU - MGKVP
17

Luria's model describes a number of units that interact to provide functional systems.
They are described as follows:
the unit for regulating tone and waking and mental states, which is necessary for the arousal of the brain and which originates in the reticular formation of the brain stem;
the unit for receiving, analysing, and storing information, which relates to areas within the occipital lobe (vision), the temporal lobe (auditory), and the parietal lobe (somatosensory, i.e. haptic or tactile sensation);
finally, the unit for programming, regulation, and verification of activity, which Luria associates with the frontal lobe and which allows direction and control of motor movement.
4/2/2020 DKU - MGKVP
18

The influence of the cognitive neuropsychology movement
Software and Hardware
the rise of connectionist models that were loosely inspired by brain function had the side effect of increasing interest in what was known in detail about brain function
in the 1970s and 1980s there were breakthroughs in systems-level neuroscience that had implications for mainstream cognitive psychology
the development of neuroimaging techniques that produce maps of neural activity while the brain is performing some cognitive task
The functional neuroimaging revolution
4/2/2020 DKU - MGKVP
19

How does brain structure constrain mental events? Some Early Answers
Non-scientific (no data)
‚It doesn’t‛ (Aristotle)
‚It does‛ (Plato, Hippocrates, Vesalius)
‚As a conduit for humors in the ventricles‛ (Galen)
‚By transmitting information from the soul (in the pineal gland) to nerves and muscles‛ (Descartes)
4/2/2020 DKU - MGKVP
20

How does brain structure constrain mental events? Some Early Answers
Pre-scientific (anecdotal observation, uncontrolled experiments)
Lateralization/Localization
Different regions generate different behaviors (Broca,Wernicke, Gall)
Equipotentiality
Many different regions are capable of generating many different behaviors (Flourens, Lashley, Kennard, Basser)
Hierarchy
More complex behaviors arise from coordination & integration of more elemental processes (Jackson, Luria)
4/2/2020 DKU - MGKVP
21

How does brain structure constrain mental events? Modern Answers
Scientific (systematic observation, controlled experiments and ‘experiments of nature’)
Double dissociation of lesions/structures and deficits/activation provides strong support for localization and hierarchical organization of function
Double dissociation requires that ‚symptom A occurs with lesions in one structure but not with those in another, and that symptom B occurs with lesions of the other but not the one‛ – Teuber, 1959
4/2/2020 DKU - MGKVP
22

The Rationale for Neuropsychological Evaluation
Dr. Durgesh K. Upadhyay
Assistant Professor AIBAS
Amity University Uttar Pradesh, Lucknow
4/2/2020 DKU - MGKVP
23

Neuropsychological Evaluation (NPE)
A testing method through which a neuropsychologist can acquire data about a subject’s cognitive, motor, behavioral, linguistic, and executive functioning.
These data can provide information leading to the diagnosis of a cognitive deficit or to the confirmation of a diagnosis, as well as to the localization of organic abnormalities in the central nervous system (CNS).
The data can also guide effective treatment methods for the rehabilitation of impaired patients.
Provides insight into the psychological functioning of an individual
4/2/2020 DKU - MGKVP
24

Referrals for Neuropsychological Evaluation
Individuals with following brain injuries –
Traumatic brain injury (TBI), concussion, acceleration-deceleration injury.
Cerebro-vascular accident (CVA) which includes stroke and ruptured aneurysm (An aneurysm is a bulge in a blood vessel caused by a weakness in the blood vessel wall, usually where it branches).
Brain tumour - originated in the brain or metastasized into the brain from other parts of the body.
Anoxia (lack of oxygen), as in drowning, chocking or strangulation.
Toxic injury - caused by neurotoxins, such as CO, Pb, Hg and certain illicit drugs.
Infection – encephalitis, meningitis, abscess or chronic brain Lyme disease.
Degenerative diseases – Alzheimer's Disease, Pick's Disease, Huntington's Disease, Lewy Body Disease and sometimes Multiple Sclerosis and Guillome-Barr Disease.
4/2/2020 DKU - MGKVP
25

Referrals for Neuropsychological Evaluation
Head injury
Failure to achieve developmental milestones
Learning or attention deficits
Exposure to drugs, alcohol, or maternal illness in utero
Exposure to chemicals, toxins, or heavy metals
Neurodegenerative diseases
Cerebral palsy
Genetic disorders including, but not limited to, trisomies, monosomies, and trinucleotide repeat disorders
Parkinson disease
Seizure disorders
Substance abuse
Strokes
Dementia
Psychiatric disorders
4/2/2020 DKU - MGKVP
26

Major Domains of Neuropsychological Functioning
Intellectual functioning
Academic achievement
Language processing
Visuospatial processing
Attention/concentration
Verbal learning and memory
Visual learning and memory
Executive functions
Speed of processing
Sensory-perceptual functions
Motor speed and strength
Motivation/symptom validity
Personality assessment
4/2/2020 DKU - MGKVP
27
NPE is useful for measuring many function categories, including the following:

Commonly Used Neuropsychological Tests
Domain Neuropsychological Test Intellectual functioning Wechsler Scales
Wechsler Adult Intelligence Scale-Revised (WAIS-R) Wechsler Adult Intelligence Scale-III (WAIS-III) Wechsler Intelligence Scale for Children-IV (WISC-IV) Stanford-Binet Intelligence Scale-IV
Academic achievement Wechsler Individual Achievement Test (WIAT) Woodcock-Johnson Achievement Test
Language processing Boston Naming Test Multilingual Aphasia Examination Boston Diagnostic Aphasia Examination Token Test
4/2/2020 DKU - MGKVP
28

Commonly Used Neuropsychological Tests
Domain Neuropsychological Test Visuospatial processing Rey-Osterrieth Complex Figure – Copy condition WAIS Block Design Subtest Judgment of Line Orientation Hooper Visual Organization Test Attention/ concentration Digit Span Forward and Backward Trail Making Tests Cancellation Tasks (Letter and symbol) Paced Auditory Serial Addition Test (PASAT) Vanderbilt Assessment Scale Behavior Assessment System for Children (BASC) Serial Sevens
4/2/2020 DKU - MGKVP
29

Commonly Used Neuropsychological Tests
Domain Neuropsychological Test Verbal learning and memory Wechsler Memory Scale (WMS) Logical Memory I and II - Contextualized prose Verbal Paired-Associates WMS-III Verbal Memory Index Rey Auditory Verbal Learning Test California Verbal Learning Test Verbal Selective Reminding Test Hopkins Verbal Learning Test Visual learning and memory WMS Visual Reproduction I and II WMS-III Visual Memory Index Rey-Osterrieth Complex Figure - Immediate and delayed
recall Nonverbal Selective Reminding Test Continuous Recognition Memory Test Visuo-Motor Integration Test - Block design
4/2/2020 DKU - MGKVP
30

Commonly Used Neuropsychological Tests
Domain Neuropsychological Test
Executive functions Wisconsin Card Sorting Test Category Test Stroop Test Trail Making Test-B WAIS Subtests of Similarities and Block Design Porteus Maze Test Multiple Errands Test (MET) Serial Sevens Mini-Mental State Exam Motor speed and strength Index Finger Tapping Grooved Pegboard Task Hand Grip Strength Thurstone Uni- and Bimanual Coordination Test
4/2/2020 DKU - MGKVP
31

Commonly Used Neuropsychological Tests
Domain Neuropsychological Test Motivation Rey 15 Item Test Dot Counting Forced-Choice Symptom Validity Testing Personality assessment Minnesota Multiphasic Personality Inventory (MMPI) Millon Clinical Multiaxial Inventory Beck Depression Inventory (BDI) Rorschach Test Myers-Briggs Type Indicator (MBTI) Thematic Apperception Test for Children or Adults Speed of processing Simple and Choice Reaction Time Symbol Digit Modalities Test - Written and oral Sensory-perceptual functions Halstead-Reitan Neuropsychological Battery (HRNB)
4/2/2020 DKU - MGKVP
32

Usefulness and Purpose of the Neuropsychological Evaluation
Clarification of diagnosis by assessing the cognitive profile and degree of cognitive impairment in suspected cases of brain injury.
Establishing a baseline from which comparisons of the effectiveness of therapeutic interventions or changes in cognitive status can be made.
Using the evaluation results to design a specific and targeted cognitive treatment plan.
Assisting social workers and discharge planners by providing a realistic picture of cognitive strengths and goals for community placement and development of rehabilitation and training programs.
Predicting prognostic outcomes
Documentation of cognitive status for vocational & educational, forensic or litigation proceedings.
4/2/2020 DKU - MGKVP
33

Types of Brain Injuries
Concussion Contusion Coup-Contrecoup Injury Diffuse Axonal Injury Traumatic Brain Injury
Closed Brain Injury Open (Penetrating) Brain Injury
Acquired Brain Injury (ABI) Anoxic Event Acquired Brain Disorder (ABD) Second Impact Syndrome ‚Recurrent Traumatic Brain Injury‛ Shaken Baby Syndrome Locked in Syndrome
4/2/2020 DKU - MGKVP
34

Plasticity of Brain “We never use the same brain twice.”
Dr. Durgesh K. Upadhyay
Assistant Professor
AIBAS
Amity University Uttar Pradesh, Lucknow
4/2/2020 DKU - MGKVP
35

In which manner the nervous system (NS) can modify its organization and ultimately its functioning throughout an individual’s lifetime.
A tiny worm C. Elegans, whose NS has only 302 cells.
4/2/2020 DKU - MGKVP
36

The Nature of Brain Plasticity
If behaviour changes, there must be some change in organization or properties of the neural circuitry that produces the behaviour and vice versa.
How can researchers measure change in neural circuitry?
Which synapses should be studied?
4/2/2020 DKU - MGKVP
37

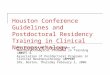
In the view on the left, the dendritic field with the extensive dendritic network is visible. On the right are higher-power views of dendritic branches showing the spines, where most synapses are located. If there is an increase in dendritic length, spine density, or both, there are presumed to be more synapses in the neuron.
Camillo Golgi (Late 1800s) – technique for staining a random subset of neurons (1-5%) so that the cell bodies and the dendritic trees of individual cells can be visualised.
4/2/2020 DKU - MGKVP
38

Factors Affecting Brain Plasticity
Sensory and Motor Experience (both leading pre and post-natal)
Psychoactive drugs (e.g., amphetamine, morphine)
Gonadal hormones (e.g., estrogen, testosterone)
Anti-inflammatory agents (e.g., COX-2 inhibitors)
Growth factors (e.g., nerve growth factor)
Dietry factors (e.g., vitamine and mineral supplements)
Genetic factors (e.g., strain differences, genetically modified mice)
Disease (e.g., Parkinson’s disease, schizophrenia, epilepsy, stroke)
Stress
Brain injury and leading disease
Peer relationships
Intestinal flora
4/2/2020 DKU - MGKVP
39

Stages of Brain Development
1. Cell birth (neurogenesis, gliogenesis)
2. Cell migration
3. Cell differentiation
4. Cell maturation (dendrite and axon growth)
5. Synaptogenesis (formation of synapses)
6. Cell death and synaptic pruning
7. Myelogenesis (formation of myelin)
4/2/2020 DKU - MGKVP
40

General Principles of Plasticity in Normal Brain
Changes in the brain can be shown at many levels of analysis
Different measures of neuronal morphology change independently of each other and sometimes in opposite directions
Experience-dependent changes tend to be focal
Plastic changes are time-dependent
Experience-dependent changes interact
Plastic changes are age-dependent
Not all plasticity is good
4/2/2020 DKU - MGKVP
41

4/2/2020 DKU - MGKVP
42

4/2/2020 DKU - MGKVP
43

4/2/2020 DKU - MGKVP
44

4/2/2020 DKU - MGKVP
45

4/2/2020 DKU - MGKVP
46

4/2/2020 DKU - MGKVP
47

4/2/2020 DKU - MGKVP
48

4/2/2020 DKU - MGKVP
49

4/2/2020 DKU - MGKVP
50

4/2/2020 DKU - MGKVP
51

4/2/2020 DKU - MGKVP
52

4/2/2020 DKU - MGKVP
53

4/2/2020 DKU - MGKVP
54

4/2/2020 DKU - MGKVP
55

4/2/2020 DKU - MGKVP
56

4/2/2020 DKU - MGKVP
57

4/2/2020 DKU - MGKVP
58

4/2/2020 DKU - MGKVP
59

4/2/2020 DKU - MGKVP
60

4/2/2020 DKU - MGKVP
61

4/2/2020 DKU - MGKVP
62

4/2/2020 DKU - MGKVP
63

4/2/2020 DKU - MGKVP
64

Frontal Lobe
Largest lobe
Traditional classification systems divide the frontal lobes into
precentral cortex (the strip immediately anterior to the central or Sylvian fissure),
prefrontal cortex (extending from the frontal poles to the precentral cortex and including the frontal operculum, dorsolateral, and superior mesial regions),
orbitofrontal cortex (including the orbitobasal or ventromedial and the inferior mesial regions), and
superior mesial regions (containing, primarily, the anterior cingulate gyrus)
Each of these areas has widespread connectivity
4/2/2020 DKU - MGKVP
65

4/2/2020 DKU - MGKVP
66

Dorsolateral frontal cortex - planning, strategy formation, and executive function.
Dorsolateral frontal lesions - apathy, personality changes, abulia, and lack of ability to plan or to sequence actions or tasks; poor working memory for verbal information (if the left hemisphere is predominantly affected) or spatial information (if the right hemisphere bears the lesion brunt)
Frontal operculum - center for expression of language
Left frontal operculum lesions - Broca aphasia and defective verb retrieval
Right opercular lesions - expressive aprosodia
Orbitofrontal cortex - response inhibition
Orbitofrontal lesions - difficulty with dis-inhibition, emotional lability, and memory disorders
4/2/2020 DKU - MGKVP
67

Orbital personality - impulsiveness, puerility, a jocular attitude, sexual disinhibition, and complete lack of concern for others
Superior mesial lesions affecting the cingulate cortex - akinetic mutism
Inferior mesial (basal forebrain) lesions - anterograde and retrograde amnesia and confabulation
Broca aphasia (lesion in areas 44 and 45 on the left hemisphere) – non-fluent speech, agrammatism, paraphasias, anomia, and poor repetition
Lesions anterior, superior, and deep to (but sparing) the Broca area - abnormal syntax and grammar but repetition and automatic language are preserved (transcortical motor aphasia) and uninhibited echolalia is common
Memory disturbances only develop with lesion extension into the septal nucleus of the basal forebrain
4/2/2020 DKU - MGKVP
68

Neuropsychological Functions of the Frontal Lobe
A. Executive Functioning – capacities that enable a person to engage in purposive, independent and sub-serving behaviour; include the ability to plan, to disengage from the immediate environment, to show flexibility of thinking, to fluently generate concepts, and to inhibit responses to overlearned patterns of behaviour.
Damage to the dorsolateral prefrontol cortex
B. Mental flexibility – requires the capacity to shift a course of thought or action according to rapidly changing situational demands Wisconsin Card Sorting Test (WCST) – concept formation, abstract reasoning, and
mental flexibility California Card Sorting Test (CCST)
4/2/2020 DKU - MGKVP
69

Neuropsychological Functions of the Frontal Lobe
C. Response inhibition – ability to inhibit responses to established patterns of behaviour
Stroop Test
D. Verbal fluency – person’s ability to rapidly generate words The Controlled Oral Word Association Test (COWAT) – also known as FAS Circumscribed left or bilateral frontal lobe lesions (Janowsky, Shimamura, & Squire, 1989)
E. Planning The Porteus Maze Test (Levin, 1991) Tower of London Test (Shallice & Burgess, 1991); Tower of Hanoi (Glosser & Goodglass, 1991) –
patients with anterior lesions performed worse than the patients with posterior lesions; Visual Planning Test (Miotto & Morris, 1998)
4/2/2020 DKU - MGKVP
70

Neuropsychological Functions of the Frontal Lobe
F. Memory – frontal lobe damage does not significantly impair the ability to memorize material but does interface with the ability to organize, attend to, and spontaneously retrieve information
G. Retrieval – frontal lobe impairment leads to poor recollection or retrieval of information in the context of relatively preserved recognition memory
‘Working Memory’ – Allan Baddeley
H. Temporal sequencing – prefrontal cortex-damaged patients demonstrate deficiencies in their ability to integrate temporally separated events (Kesner, Hopkins, & Fineman, 1994)
I. Source memory – patients with frontal lobe lesions exhibit impaired source memory (identifying the source of their knowledge) – Janowsky et al. (1989)
J. Autobiographical memory – prefrontal damage
4/2/2020 DKU - MGKVP
71

Neuropsychological Functions of the Frontal Lobe
K. Language – loss of grammar (aggramatism) and the production of unintended syllables, words, or phrases during speech (paraphasic errors)
L. Broca’s aphasia – nonfluent, effortful speech production, semantic and phonetic patraphasias, articulatory errors, aggramatism, and relatively preserved comprehension Poor repetition, reading, and writing ability Lesion in left posterior, inferior frontal gyrus Lesions in inferior central Rolandic area, the insula, subcortical regions, and the antrior parietal
regions
M. Pure motor aphasia (or Verbal Apraxia) – refers to the articulatory and prosodic disturbance of language output in the absence of the aggramatic component Left lower motor cortex and posterior operculum Precentral gyrus of the insula – articulatory deficites
4/2/2020 DKU - MGKVP
72

Neuropsychological Functions of the Frontal Lobe
N. Transcortical motor aphasia (TCMA)
lesion in left frontal lobe–supplementary motor area (SMA), just antrior and superior to Broca’s area, results in a lack of plan or program to carry out voluntary speech
O. Frontal-subcortical aphasias – lesion in frontal-subcortical brain regions
Patients with subcortical aphasia with capsular/putaminal (C/P) lesion sites with anterior-superior white matter extension had good comprehension, grammatical but slow dysarthric speech, and lasting right hemiplegia – (Naeser, 1982)
4/2/2020 DKU - MGKVP
73

Diseases of Frontal Lobe
A. Frontal Lobe Dementia (FLD)
a. Behavioural features
b. Neuropsychological features
Frontotemporal dementia (FTD) or frontotemporal degenerations refers to a group of disorders caused by progressive nerve cell loss in the brain's frontal lobes (the areas behind your forehead) or its temporal lobes (the regions behind your ears).
The nerve cell damage caused by FTD leads to loss of function in these brain regions, which variably cause deterioration in behavior and personality, language disturbances, or alterations in muscle or motor functions. There are a number of different diseases that cause frontotemporal degenerations. The two most prominent are 1) a group of brain disorders involving the protein tau and 2) a group of brain disorders involving the protein called TDP43. For reasons that are not yet known, these two groups have a preference for the frontal and temporal lobes that cause dementia
B. Traumatic Brain Injury (TBI)
4/2/2020 DKU - MGKVP
74

4/2/2020 DKU - MGKVP
75

Spasticity (from Greek spasmos-, meaning "drawing, pulling") is a feature of altered skeletal muscle performance with a combination of paralysis, increased tendon reflex activity and hypertonia. It is also colloquially referred to as an unusual "tightness", stiffness, or "pull" of muscles.
Lhermitte's sign – Sudden, transient, electric like shocks spreading down the body when the head is flexed forward, occurring chiefly in multiple sclerosis but also in compression disorders of the cervical spinal cord.
Abulia - An absence of willpower or an inability to act decisively, a symptom of schizophrenia or other mental illness.
Akinetic mutism: A state in which a person is unable to speak (mute) or move (akinetic). Akinetic mutism is often due to damage to the frontal lobes of the brain.
Incontinence or Incontinent may refer to: Fecal incontinence, the involuntary excretion of bowel contents Urinary incontinence, the involuntary excretion of urine Lack of moderation or self-control, especially related to sexual desire
4/2/2020 DKU - MGKVP
76

4/2/2020 DKU - MGKVP
77

4/2/2020 DKU - MGKVP
78

4/2/2020 DKU - MGKVP
79

4/2/2020 DKU - MGKVP
80

4/2/2020 DKU - MGKVP
81

Neuropsychological Assessment and Rehabilitation
Dr. Durgesh K. Upadhyay
Assistant Professor
Amity Institute of Behavioural and Allied Sciences
Amity University Uttar Pradesh, Lucknow
4/2/2020 DKU - MGKVP
82

4/2/2020 DKU - MGKVP
83 Concepts
‘Localizationist’ view of brain function
Halstead-Reitan Battery (HRNB)
Wechsler Scales of Intelligence and Memory
Raven’s Matrices etc.
Integrational approach to brain-behaviour relationships
Pre-eminent Soviet neuropsychologist, A. R. Luria (1966)
Complex mental processes arise from the concerted and integrated action of separate and autonomous cortical and subcortical processing sites
Highly standardised or psychometric procedures
Idiosyncratic and flexible administration of procedures
Example – The Statndardised Luria-Nebraska Battery
Inferential Process

The Process of Neuropsychological Assessment
Neuropsychological assessment may be used clinically:
1. To determine the presence or absence of organic pathology
2. To determine, within the individual, the interaction between organic and non-organic processes which lead to pathology
3. To determine change of function over time, for example, as a consequence of treatment or spontaneous recovery, or alternatively to monitor deterioration
4. To plan cognitive rehabilitation
4/2/2020 DKU - MGKVP
84

Assessment comprises initially a comprehensive interview covering medical, psychological, social, educational and vocational history in relation to the emergence and course of disturbed cognition, emotion and behaviour
In addition, obtain a detailed account of the manifestation of cognitive disturbance within the person’s natural environment
On the basis of such interviews, an assessment is instigated, the precise nature of which undoubtedly varies across practitioners.
Application of a comprehensive, standardized battery such as Halstead-Reitan or Luria-Nebraska battery.
4/2/2020 DKU - MGKVP
85

4/2/2020 DKU - MGKVP
86 An alternative (but not mutually exclusive) approach would be a stepwise process such as follows:
1. Assessment of fundamental problem areas (using specific procedures such as an aphasia battery, memory test or tests of perceptual disturbance); the aim here is to obtain a precise understanding of the degree of disturbance of a specific function
2. Use of general organic screening procedures (e.g., tests such as the Stroop, Category Test and Trail Making Test are highly sensitive to the presence of brain damage but tell us little, when used in isolation, in respect of possible localisation); the use of organic screens helps to determine whether the primary problems reflect organic impairment (brain damage) or functional (psychogenic) disturbance
3. Flexible assessment to determine precise cognitive strengths and weaknesses, thereby gaining a more complete understanding of the specificity of disturbance as well as documenting intact functions or retained abilities
4. Further testing, determined by hypothesis testing (namely a hypothesis of localisation); such an approach may be termed ‘hypothesis driven’.

In addition to specific cognitive testing, use may be made of self-reporting questionnaires of emotional state such as anxiety, depression, hypomania, anger or hostility, and so on.
The interpretation of a neuropsychological profile, particularly for differential diagnosis, must be made on the basis of a convergent analysis of the test results and symptoms
4/2/2020 DKU - MGKVP
87

Global cognitive disturbance as a function of site of damage, and tests of use in its localization
Site of damage; cognitive disturbance Test
Frontal Lobe • Expressive language disorders • Disorders of planning, programming, execution, monitoring and regulation of
behaviour • Disturbance of reasoning, abstraction and logical analysis • Rigidity of cognitive processing • Disorganization of complex motor actions • Disturbance of focused attention • Memory disturbance • Dysregulation of mood • Personality disturbance
• Benton Verbal Fluency Test • Trail Making Test • Wisconsin Card Sorting Test and Halstead Category Test
Temporal Lobe • Auditory-perceptual defects • Visual field disturbances • Disorders of visual organization • Short-term memory deficits • Amnesic syndrome • Receptive language disorders
• Speech Sound Perception Test & Seashore Rhythms Test • Benton Visual Retention Test, Complex Figure of Rey, and Revised
Wechsler Memory Scale
4/2/2020 DKU - MGKVP
88

Site of damage; cognitive disturbance Test
Parietal Lobe • Sensory and perceptual disturbance • Disorders of inter-sensory association • Spatial disorientation • Impaired location and topographical memory • Constructional apraxia • Spatial dyslexia and dyscalculia • Unilateral spatial neglect • Spatial agnosias • Receptive language disorders
• Left-Right Disorientation Test • Complex Figure of Rey, Block Design and Object Assembly of the WAIS-R
and Tactual Performance Test • Arithmetic Subset of the WAIS-R and Arithmetic Scale of the Luria-
Nebraska Battery
Occipital Lobe • Cortical blindness • Visual agnosias • Pure word blindness (agnosic alexia)
4/2/2020 DKU - MGKVP
89
Global cognitive disturbance as a function of site of damage, and tests of use in its localization

Issues
Accuracy
‘Stand Alone’ system???
Reliability
Cost
4/2/2020 DKU - MGKVP
90

Summary
NPA may be seen as an approach which combines both quantitative and qualitative interpretation
Neuropsychological interpretation in the determination of brain damage is an inferential process and is, therefore, not strictly equivalent to or an alternative to neurological diagnostic procedures
There is a need to view NPA as an investigative adjunct to other clinical examinations
NPA may be only viewed in the realm of cognitive rehabilitation as operating largely independently from neurological examination
4/2/2020 DKU - MGKVP
91

Neuropsychological Rehabilitation
Often seen as being synonymous with cognitive rehabilitation.
NPR may be seen to comprise the following:
1. Informational Care
2. Psychotherapeutic support
3. Cognitive rehabilitation – memory retraining
4. Social and vocational skills training
Cognitive rehabilitation may play a vital role in the restoration or remediation of cognitive disturbance following brain damage
4/2/2020 DKU - MGKVP
92

4/2/2020 DKU - MGKVP
93 Neuropsychological Rehabilitation
Cognitive rehabilitation comprises three approaches:
The use of compensation to enable the client to minimise or work round deficits
Substitution, whereby alternative methods are used to solve cognitively mediated problems
Retraining methods to stimulate specific impaired functions

Emergence of Clinical Neuropsychology
Clinical Neuropsychology
application of human neuropsychological knowledge to
assist in the diagnosis and management of cognitive
deficits in people
Response to a Clinical Need
identify cognitive abilities and disabilities for reintegration
and rehabilitation of WW II wounded
accurate diagnosis of brain disorders (e.g., strokes,
tumors) in pre-imaging era
4/2/2020 DKU - MGKVP
94

Emergence of Clinical Neuropsychology
New Questions
Is the behavior a sign of brain damage/disease?
What areas of the brain/disease mechanisms are
involved?
How severe is the dysfunction?
What cognitive processes account for the deficit?
How can the patient adapt to deficits to minimize
functional impact?
Will the patient return to work or independent living?
4/2/2020 DKU - MGKVP
95

Added Value of Clinical Psychology
Background & Training in
Theories of cognitive and behavioral function
Standardized assessment of individual differences
Quantitative analysis
Experimental design
Actuarial prediction
Behavioral treatment methods
4/2/2020 DKU - MGKVP
96

Early Contributions to Clinical Neuropsychology
Ward Halstead & Ralph Reitan
developed battery of tests with standard administration &
scoring given to all patients
empirically-derived cutoffs discriminated brain-damaged
from non-brain damaged patients
lateralized and localized lesions based on sensory-motor
asymmetries
limited assessment of higher cognitive functions or
underlying processing impairments
4/2/2020 DKU - MGKVP
97

Early Contributions to Clinical Neuropsychology
David Wechsler
refined existing IQ tests, using multiple subtests assessing
different aspects of verbal and visual-spatial skills
developed clinical tests of attention and verbal and
visual memory
rigorous psychometric design and large normative
samples improved precision
neuropsychologists identified subtest profiles associated
with focal brain lesions
4/2/2020 DKU - MGKVP
98

4/2/2020 DKU - MGKVP
99

Early Contributions to Clinical Neuropsychology
Edith Kaplan
early colleague of Geschwind, influenced by Luria
developed flexible, non-standard assessment approaches
focus on analysis of error types to describe deficits in
underlying, hierarchical cognitive processes (i.e., “process
approach”)
tasks tailored to patient or question, well-suited to
rehabilitative goals of identifying compensatory strategies
limited normative database for discriminating subtle
impairment from normal
4/2/2020 DKU - MGKVP
100

Foundations of
Neuropsychology Dr. Durgesh K. Upadhyay

Consciousness as a Problem of
the Psychology of Behavior
Consciousness as a Problem of the Psychology of Behavior
Vygotsky in 1925 (Collected Works, vol. 1, 1982b; English edition—hereinafter E.—1997)
the first very general understanding of the correlation between the social and biological genesis of the human psyche or mind.
“reflex”
“doubling experience” - a human can consciously represent (in mind) the goal of his/her action.
4/2/2020 DKU - MGKVP
102

Luria as a creator of neuropsychology
4/2/2020 DKU - MGKVP
103

4/2/2020 DKU - MGKVP
104

4/2/2020 DKU - MGKVP
105

4/2/2020 DKU - MGKVP
106

Neuropsychological
rehabilitation
amelioration of cognitive social and emotional deficits
caused by an insult to the brain
Main purpose is to enable people with disabilities to
achieve their optimum level of well being, to reduce
the impact of their problems on everyday life and to
help them return to their most appropriate
environments
4/2/2020 DKU - MGKVP
107

Theories of Neuropsychological Rehabilitation
Six treatment paradigms - Powell (1981)
1. The non-intervention strategy (letting nature take its course).
2. The prosthetic paradigm whereby patients are helped to make the most effective use of prostheses.
3. Practice or stimulation
4. The maximizing paradigm in which therapists tend to maximize the extent, speed, and level of learning by such procedures as positive reinforcement and feedback.
5. Brain function therapy, or directed stimulation which aims to focus or direct tasks at certain regions of the brain to increase its activity or re-establish functions in new areas.
6. Medical, biochemical, and surgical treatments which, can sometimes be combined with other therapeutic treatments
4/2/2020 DKU - MGKVP
108

Models of neuropsychological
interventions
Gross and Schutz (1986)
1. The environmental control model
2. The stimulus-response (S-R) conditioning model
3. The skill training model
4. The strategy substitution model
5. The cognitive cycle model
4/2/2020 DKU - MGKVP
109

Sinfonia Hemispherica
Buffery and Burton (1982)
Three factors affecting the overall performance of the orchestra.
1. The size of the lesion – the more violinists who have died the worse will be the performance.
2. The position of the lesion – some violinists, such as the leader, are more important than others.
3. Shock – although the remaining members of the orchestra are not ill themselves, initially they will be affected by the sudden demise of their colleagues.
Buffery and Burton suggest several ways the orchestra might cope with its predicament. First, the orchestra could recruit new members to replace those who have died. Second, the orchestra could change its repertoire so that missing members are not required to perform. Third, the leader of the orchestra could ask some other members to learn the violin.
4/2/2020 DKU - MGKVP
110