Embed Size (px)
Citation preview

Force and complexity of tongue tasktraining influences behavioralmeasures of motor learning
Mohit Kothari1, Peter Svensson1,2,Xueliang Huo3, MaysamGhovanloo3, Lene Baad-Hansen1
1Department of Clinical Oral Physiology,School of Dentistry, Aarhus University, AarhusC, Denmark; 2MINDLab, Center forFunctionally Integrative Neuroscience, AarhusUniversity Hospital, Aarhus C; 3GT-BionicsLab, School of Electrical and ComputerEngineering, Georgia Institute of Technology,Atlanta, GA, USA
Rapid and effective control of the tongue musculature isrequired in many daily oral functions, for example,chewing, swallowing, and speech (1–3). The swallowingprocess consists of a highly complex and semi-automaticsequence of events involving extrinsic and intrinsic ton-gue muscles, leading to protection of the airways duringfood ingestion (4, 5). Tongue dysfunction may be con-genital or caused by neurological diseases or brain injury,such as stroke (6–8), and may have a serious negativeimpact on health and quality of life. Approximately 50%of stroke patients suffer from dysphagia with a high riskof aspiration of food, which may lead to potentially life-threatening pneumonia (9–11). Infantile swallowing andcerebral palsy are other types of tongue dysfunction withimplications for dental occlusion and jaw growth pattern(12, 13).Previous studies have examined corticomotor control
of tongue movements (4, 14). A series of tongue-trainingstudies performed by our group have revealed training-induced neuroplasticity in human corticomotor controlof the tongue by demonstrating an increase in motor-evoked potentials produced by transcranial magneticstimulation, as well as an increase in the motor cortex(MI) tongue representation (14–17). These studies haveall used a highly standardized tongue-protrusion taskwith a constant target force and timing of the task (risetime (protrude tongue), top delay (hold tongue protru-
sion force), fall time (retract tongue), and bottom delay(rest)) (14–16, 18, 19). The tongue-protrusion task isnevertheless one-dimensional tongue training. The maingoal of many neurorehabilitation regimes is to promoteneuroplasticity at the subcortical and cortical levels, suchthat long-lasting and beneficial alterations in motorcontrol strategies can be achieved (20). As a one-dimensional standard task may prove less beneficial forpatients with compromised tongue function because ofits simplicity, there is a need to study modulation oftraining parameters to enhance performance. The pres-ent clinical oral rehabilitation techniques involve variousstimulation paradigms such as Facio-oral Tract Therapy(FOTT), but these are mostly based on experience andlack scientific evidence (21). In order to be able to pri-oritize the use of available resources for neurorehabili-tation, more knowledge is required on examination andtraining methods in patients with compromised tonguefunction.In this study we introduce a complex tongue-training
paradigm that uses the Tongue Drive System (TDS) as anovel tongue-training approach (22–24). The TDS is awireless, non-invasive, unobtrusive, and accurate ton-gue–computer interface. The TDS can wirelessly detectthe tongue position inside the oral cavity and translate itsfree voluntary motion into a set of specific user-definedcomputer commands (22, 25). The tongue thereby can
Kothari M, Svensson P, Huo X, Ghovanloo M, Baad-Hansen L. Force and complexity oftongue task training influences behavioral measures of motor learning.Eur J Oral Sci 2012; 120: 46–53. � 2011 Eur J Oral Sci
Relearning of motor skills is important in neurorehabilitation. We investigated theimprovement of training success during simple tongue protrusion (two force levels)and a more complex tongue-training paradigm using the Tongue Drive System (TDS).We also compared subject-based reports of fun, pain, fatigue, and motivation betweenparadigms. Three randomized sessions and one control experiment were performed.Sixteen healthy subjects completed two different 1-h sessions of simple tongue trainingwith 1 N and 3 N, respectively, and one TDS session. After 1 wk, six out of 16 subjectsparticipated as experienced subjects with six naive subjects in a control experimentwith 2 · 5-min TDS training separated by a 30-min rest. Performance improvedduring training in all sessions. The mean ± SEM relative increase in success was80 ± 12% (1 N), 52 ± 11% (3 N), and 285 ± 45% (TDS). In the control experimentthe experienced group performed equal to the last 5 min of their first TDS session andneither group improved during rest. Training with the TDS was rated as more fun, lesspainful, less fatiguing, and more motivating compared with simple tongue training. Inconclusion, force level and complexity of tongue training influences behavioral aspectsof tongue motor learning.
Mohit Kothari, Department of Clinical OralPhysiology, School of Dentistry, AarhusUniversity, Denmark
Telefax: +45–89–424297E-mail: [email protected]
Key words: motor control; neuroplasticity;Tongue Drive System; tongue training; trigem-inal physiology
Accepted for publication September 2011
Eur J Oral Sci 2012; 120: 46–53DOI: 10.1111/j.1600-0722.2011.00894.xPrinted in Singapore. All rights reserved
� 2011 Eur J Oral Sci
European Journal ofOral Sciences

act as a computer mouse, and three-dimensional tonguetraining can consist of playing tongue-controlled com-puter games (23, 25, 26). Training by playing a computergame may increase subjects� motivation and perfor-mance. In healthy individuals, novel motor skill training,in contrast to passive assistance or repetitions of generalexercise (strength training), has been associated withimprovements in task performance and increased repre-sentation of the trained muscle in the motor cortex(14, 17, 27).Therefore, we hypothesize that force and complexity of
tongue training influences behavioral measures of tonguemotor learning (i.e. performance). The present studyaimed to investigate the degree (percentage) of improve-ment of training success during simple tongue protrusion(two different force levels) and a more complex tongue-training paradigm using the TDS. In addition, we aimedto compare subject-based reports of fun, pain, fatigue,and motivation between training paradigms.
Material and methods
Subjects
Twenty-two healthy subjects (nine men and 13 women, 19–66 yr of age with a mean ± SEM age of 27.6 ± 5.8 yr)were recruited at the School of Dentistry, Aarhus Univer-sity, where the study was performed. The subjects had nomedical, physical, or psychological disorders. Inclusioncriteria were the ability to read and to understand the pro-ject information. Exclusion criteria were the inability tofinish the entire tongue-training session and prior experiencewith either of the two types of tongue training applied in thepresent study. All subjects gave informed consent andreceived compensation for their participation. The studywas approved by the local Ethics Committee and wasperformed in accordance with the Declaration of Helsinki.Every session lasted for approximately 1 h and 30 min,including preparation and calibration.
Procedure
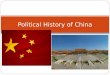
The present cross-over study consisted of three sessions(sessions 1–3) in randomized order and one control experi-ment, 1 wk after the third session. Sixteen healthy subjectswere included in sessions 1–3. Two of these sessions in-cluded a 1-h simple tongue-protrusion task with a differentforce level in each session (1 N in one session and 3 N in theother session) (14–16, 28). The third session was a morecomplex training paradigm using the TDS for 1 h (Fig. 1).After 1 wk, six out of 16 subjects participated in a TDScontrol experiment as experienced subjects (as they had al-ready tried the TDS in the continuous TDS 1-h session).Also, six additional and naive subjects were included ascontrols in the control experiment (Fig. 1). The naive sub-jects did not participate in sessions 1–3 and therefore did nothave any prior experience with tongue training. The controlexperiment involved 20 min of preparation time (describedin detail in the following section on the TDS) followed by2 · 5 min of active training with the TDS separated by a 30-min rest. The control experiment was performed to inves-tigate the degree of skill retention in experienced subjectsfrom the first to the second TDS session (control
experiment), and the difference in performance increasebetween the continuous 1-h TDS training session andthe control session with only 2 · 5 min of active trainingand a large proportion of the session consisting of rest(between groups and within groups, experienced andnaive). An increase in performance during a period ofrest could be considered �offline learning� and the inclusionof a resting period in this study is a control for thatphenomenon (29).The subjects were asked to report fun, pain, fatigue, and
motivation on four separate 0–10 numerical rating scalesafter every session. On the scale, �0� indicated no fun/pain/fatigue/motivation at all and �10� indicated the highest levelof fun/pain/fatigue/and motivation imaginable. Beforeevery session, subjects were encouraged to perform as wellas possible.
Simple tongue-protrusion task
The subjects performed two identical (except for the forcelevel) 1-h tongue-protrusion task sessions in the laboratory(288 repeated and identical trials). In accordance with ourprevious detailed description (14, 16, 30), the subjects wereasked to protrude the tongue 288 times onto a force trans-ducer that was affixed rigidly to a beam on the table in frontof the subject; the force plate was located in the middle,2 cm anterior to the most anterior portion of the upper lip.A horizontal beam to secure a constant distance to the forcetransducer supported the forehead. The transducer output
Sixteen healthy subjects
Session 1–3 in randomized order (Every session of 1 h)
1 N Simple 3 N Simpletongue training tongue training
Complex tongue training (TDS)
Subgroup of 6/16 subjects included as experienced controls
2×5 min of Tongue Drive System training separated by 30 min rest
Six naive subjects as naive control
One week a�er comple�on of session 1–3
Fig. 1. Experimental protocol. Sixteen healthy subjects partic-ipated in sessions 1–3 in randomized order; these sessions in-cluded two different sessions of simple tongue training withforce levels of 1 N and 3 N, and the third session was complextongue training with the Tongue Drive System (TDS). Oneweek after completion of sessions 1–3, six of 16 subjects wereincluded as an experienced control with six naive subjects in acontrol experiment. The control experiment was 2 · 5 min oftraining with the TDS separated by a 30-min rest.
Force and complexity of tongue training 47

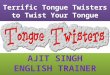
controlled the vertical position of a cursor on a computermonitor located in front of the subject (Fig. 2A). Duringeach tongue-protrusion trial, a computer-controlled base-line window appeared initially at the bottom of the com-puter screen and, after a 10-s pretrial period, it wasdisplaced to a preset target force level (1 N or 3 Ndepending on the session). During the 10-s pretrial period,the subject sat relaxed in the chair. A 0.5-s dynamic tongue-protrusion phase (ramp up) was the period where the targetwindow moved from the bottom of the screen to the targetlevel. During this phase, the subject had to exert theappropriate force to keep the tongue-controlled cursor(0.25 cm · 0.25 cm) within the target window. This wasfollowed by a 1.5-s holding phase, during which the subjectwas required to hold the target force level, and finally aramp-down phase (0.5 s) where the subjects could retractthe tongue (14, 16, 28, 30, 31). A graphic representation ofthis paradigm has been published previously (30). At alltimes, the location of the cursor relative to the movingtarget box was displayed on the computer screen so thatsubjects had constant visual feedback of the current per-formance. The performance success rate was determined foreach individual tongue-protrusion trial as the proportion oftime (percentage), in which the cursor was placed correctlyinside the target window. Each session of simple tonguetraining lasted for 60 min: 12 blocks of 5 min with 1 N and3 N were recorded.
Tongue Drive System
The TDS is an assistive technology originally developed forquadriplegic patients, allowing them to have control over apowered wheelchair, computer, and telephone or to controlthe user�s environment by using the tongue as a manipulator(for example, a computer mouse) (22, 24, 25, 32). In thisstudy, it was used for the first time as a device for three-dimensional complex tongue training. To perform withTDS, a small disc-shaped rare earth permanent magnet of5 mm · 1.3 mm (10800 Gauss strength) was secured on thetongue as a magnetic tracer by using a tissue adhesive(Cyanodent fast; Ellman, New York, NY, USA). A mag-netic field was generated inside and around the mouth usingthis magnet. The magnetic fields were detected by an arrayof magnetic sensors mounted on a headgear, which wasworn by the subject on the head while performing the task(22, 25) (Fig. 2B). The sensor outputs were transmittedwirelessly to a computer using a wireless USB receiver af-fixed on the computer. The USB receiver and the headgearhad a built-in wireless connection (2.4 MHz) that allowedthe tongue to act as a computer mouse (Fig. 2C). A digitalsensor signal-processing algorithm running on the computerclassified the sensor signals and converted them into usercontrol commands, which were then communicated wire-lessly to the computer. The complex tongue-training sessionlasted for 60 min. Within the 60 min, there was 20 min ofpreparation time, which included placement of headgear,calibration, attachment of the magnet to the tongue, and aset-up procedure session. To set up the TDS, subjects wererequired to define specific positions in their mouth whichthey could easily reach with the magnet attached to the tipof their tongue, and associate them to each �tongue com-mand� [i.e. the subjects were instructed to consistently placetheir tongue at three recommended positions (tooth 14 for�up� command, tooth 24 for �down� command, and tongue-resting position) 10 times in a row, so that the TDS couldcollect enough data to be able to recognize those specificcommands based on the recorded data]. Later on, when thesubjects placed their tongue at those specific positions, theTDS could correctly associate the positions to the com-mands practiced during the set-up session (23, 26). Thepreparation time was included in the training time because itinvolved active tongue movements. This set-up procedurewas then followed by 40 min of continuous training: eightblocks of 5 min, in which the subjects played a computergame �Scuba Diver� (http://www.icq.com/greetings/cards/142/). In the scuba diver game, the subjects were given threelives and were instructed to collect as many coins and asmuch wealth (number of game points achieved) as possiblewhile swimming. In addition, they had to escape fromobstacles such as fish, bottles, and rocks coming their way.The performance success rates were noted manually everytime they lost their three lives. They were instructed to playthe game several times, until the total TDS time (includingthe preparation time) reached 1 h. In the control experimentthe subjects were instructed to play the same scuba divergame for 2 · 5 min, separated by 30 min of rest, and with20 min of preparation and calibration before actualtraining.
Statistics
All data are presented as mean ± SEM. In all sessions, thetraining success rate was averaged into 5-min blocks. Beforeanalysis, normal quantile plots were used to evaluate theassumption of normal distribution. Between the two simple
A
B C
Fig. 2. (A) The subject protrudes the tongue to a force trans-ducer with application of 1 N or 3 N force. (B) Headgear of theTongue Drive System (TDS) worn by the subject who was in-structed to play a computer game and had control of thecomputer cursor wirelessly through a magnet attached to thetongue. (C) Data on the magnet position is transferred wire-lessly from magnetic sensors on a headgear to a computer,where it is further processed to indentify the subject�s tonguecommand.
48 Kothari et al.

tongue-training sessions, repeated-measurement (RM)anovas with session (1 N and 3 N) and time (12 blocks of5 min) as factors were used to analyze the performancesuccess rate. As a control for motor learning transfer be-tween the two simple sessions, comparison of the perfor-mance success rate between naive 1 N (N = 7) and naive3 N (N = 4) was analyzed by two-way RM-anova. Anal-ysis of performance success rates for the TDS session overtime (eight blocks of 5 min) was performed by RM-anova.Relative increases in success rates were compared betweenthe three sessions with RM-anova. In order to evaluate thepossible differences in dynamics of success rate over timebetween sessions, the coefficient of determination (R2) andthe slope of the fitted regression line were calculated afterfinding the relative increase in success from the first 5 min toevery time block for each subject in each session, and RM-anova was used to test for differences between sessions.Data from the experienced group in the control experi-
ment were compared with the data from the first and last5 min of the 1-h TDS session using a two-way anova
(factors: session and time). Another two-way anova in thecontrol experiment session was performed with group(experienced and naive) and time (the first 5 min and the last5 min) as factors. A third two-way anova was performed toanalyze possible differences between the naive group in thecontrol experiment and the results of the experienced groupfrom the 1-h TDS session, hence when the experiencedgroup was naive (factors: group and time). When appro-priate, Tukey Honestly Significant Difference (HSD) testswith correction for multiple comparisons were performed.As a result of the low number of subjects in the controlexperiment, non-parametric analyses were also performedbut are not presented in the results section, as they do notchange any of the conclusions.The subject-based reports of fun, pain, fatigue, and
motivation were compared between sessions with RM-anovas. Finally, Spearman correlation analyses were usedto test for associations between relative increase in successrates and subject-based reports of fun, pain, fatigue, andmotivation for all sessions. The level of significance was setat P < 0.05.
Results
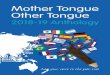
In the comparison between simple tongue-training ses-sions (1 N and 3 N) there was a main effect of session(P = 0.001) as well as of time (P < 0.001). The per-formance success rate was higher in the 3 N session thanin the 1 N session (P = 0.001; Fig. 3). Performancesuccess rates at all time-points were significantly higherthan at baseline (P < 0.001). There was no overall sig-nificant difference between groups in the post-hoc com-parison of naive 1 N (n = 7) and naive 3 N (n = 4)(P = 0.605). There was, however, a significant effect oftime (P < 0.001) and a significant interaction betweengroup and time (P = 0.009). Post-hoc tests revealed anincrease in performance over time and a significantlyhigher success in the 3 N group than in the 1 N group intime block 1 (0–5 min) (P = 0.017).There was also a significant increase in success rates
over time in the 1-h TDS session (P < 0.001). Perfor-mance success rates at all time-points were significantlyhigher than at baseline (P < 0.002). The performancesuccess rate increased from 21,487 ± 4,089 points to
72,620 ± 10,931 points during the TDS session(P < 0.001; Fig. 4A).The relative increase in performance success rate was
higher in the complex tongue-training task (285 ± 45%)than in the simple tongue-protrusion tasks with 1 N(80 ± 12%) and 3 N (52 ± 11%) (P < 0.001). Therewas no significant difference in relative increase in per-formance between 1 N and 3 N (P = 0.741).The mean coefficient of determination, R2, was
0.59 ± 0.06 in the 1 N session, 0.37 ± 0.07 in the 3 Nsession, and 0.50 ± 0.05 in the TDS session, and therewere no significant differences between sessions(P = 0.074). The mean slopes of the regression lineswere 5.93 ± 0.91 in the 1 N session, 3.56 ± 0.90 in the3 N session, and 35.24 ± 4.90 in the TDS session, with asignificant difference between sessions (P < 0.001). Post-hoc testing showed that the slope of the TDS regressionline was significantly different from 1 N and 3 N sessions(P < 0.001) with no difference between 1 N and 3 Nsessions (P = 0.832).For the six experienced subjects participating in both
the 1-h TDS session and the control experiment therewas no overall between-session difference (P = 0.082).There was a main effect of time (P < 0.001) and a sig-nificant interaction between session and time(P = 0.026). Post-hoc tests revealed that the perfor-mance success rate increased from the first 5 min to thelast 5 min (P < 0.001), and in the control experimentthe subjects had higher performance success rates in thefirst 5 min compared with the first 5 min of the 1-h TDSsession (P = 0.021; Fig. 4B).In the two-way anova between groups (experienced
and naive) and time-points (the first 5 min and the last5 min) in the control experiment session, there was amain effect of group (P = 0.019) with no effect of time(P = 0.084) (i.e. no significant increase in success after30 min of rest). The post-hoc test revealed that theexperienced group had higher performance success ratesthan the naive group (P = 0.019; Fig. 4B).The two-way anova between the naive group in the
control experiment and the experienced group in the 1-hcontinuous TDS session (when they were naive) revealed
0
10
20
30
40
50
60
0 1 2 3 4 5 6 7 8 9 10 11 12Time block (5 min)
Succ
ess
rate
(%)
**
***** **
**
Fig. 3. Simple tongue training. Mean (± SEM) performancesuccess rate (expressed as a percentage) during the two 60-min(12 blocks of 5 min) training sessions with 1 N (diamonds,lower curve) and 3 N (squares, upper curve) force. Success rateincreased over time in both groups (P < 0.001). Success ratewas higher in the 3 N session than in the 1 N session(P = 0.001). *Significant difference from baseline in bothsessions (P < 0.001) (n = 16).
Force and complexity of tongue training 49

a main effect of group (P = 0.002) as well as of time(P < 0.001), with a significant interaction betweengroup and time (P < 0.001). Post-hoc tests revealed thatoverall, the experienced group in the 1-h continuousTDS session had higher performance success rates thanthe naive group in the control experiment (P = 0.002)and that the performance success rates increased overtime (P < 0.001; Fig. 4B). There was no between-groupdifference in the first 5 min (P = 0.887) but significantlyhigher success rates in the last 5 min after continuoustraining compared with after 5 min of training and a 30-min rest (P < 0.001). Comparison between success in
the last 5 min obtained by the naive group in the controlexperiment and time block 2 (5–10 min) of the 1-h con-tinuous TDS session (i.e. comparing a total TDS trainingtime of 10 min between sessions) showed no significantdifference (P = 0.208).The subject-based reports revealed that training with
the TDS compared with simple tongue training (1 N and3 N) was rated as more fun (P < 0.001; Fig. 5A), in-duced less pain (P < 0.049; Fig. 5B), less fatigue(P < 0.009; Fig. 5C), and was associated with higherlevels of motivation (P < 0.003; Fig. 5D). No significantcorrelations were found between relative increase inperformance success rates and subject-based reports offun, pain, fatigue, and motivation in any session(q<0.316; P > 0.224).
Discussion
The first main finding in this study was that force levelinfluenced the tongue motor learning. The 3 N sessionhad higher performance success rates than the 1 N ses-sion, even though there was more fatigue in the 3 Nsession than in the 1 N session. A post-hoc analysis ofthe success in those subjects, who were naive in the 1 Nand 3 N sessions, also indicated a higher success in the3 N session, as a significant difference in success wasalready present in the first time block (0–5 min) oftraining. The maximum tongue-protrusive forcerecorded in other studies was 27 N with a range of 16–42 N (33). The lower overall performance success rates inthe present 1 N session may be explained by a higher riskof overshoots compared with the 3 N session. Thisfinding is consistent with a previous tongue task trainingstudy (14, 34).The second main finding was that the complexity of
tongue training influenced tongue motor learning, asmeasured by the relative increase in performance successrates. This finding can be important because it has beenproposed that increasing the complexity of the novelmotor skill task over the duration of rehabilitationtraining may encourage cognitive effort and thereby en-hance cortical plasticity (35). It was not possible to per-form a direct comparison between the two differenttraining paradigms (simple and complex tongue training)as performance success rates in the simple tongue-train-ing sessions were measured as a percentage and complextongue training was measured as the number of gamepoints achieved during training. This is, of course, amajor limitation and therefore indirect comparison (rel-ative increases) and a comparison of the coefficients ofdetermination were performed between the trainingparadigms. The relative increase in performance successrates was higher in the complex tongue-training taskthan in the simple tongue-protrusion tasks (1 N and3 N), which suggests that the three-dimensional trainingwith a computer game may prove more beneficial andkeep the subjects more motivated to improve their per-formance of the task. The comparison between sessionsof the coefficient of determination (R2) showed that datafrom all sessions were fitted equally well by a linear
0
20000
40000
60000
80000
0 1 2 3 4 5 6 7 8Time block (5 min)
Succ
ess
rate
(poi
nts)
*
*
*
* *
*
*
A
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
1 2 3 4 5 6 7 8
Time block (5 min)
Succ
ess
rate
(poi
nts)
30 min rest in control session
*
*
##§ §n = 6, Experienced control, control
session
n = 16, 1 h TDS session
n = 6, Naive control, control session
n = 6, Experienced controls in 1 h TDSsession when they were naive
B
Fig. 4. Complex tongue training. (A) Mean (± SEM) perfor-mance success rate during a 40-min (eight time blocks of 5 min)training session with the Tongue Drive System (TDS) (complextongue training) in a 1-h TDS session. The success rate in-creased over time in the 1-h TDS session (n = 16; P < 0.001).*Significant difference from baseline (P < 0.001) (n = 16). (B)Control experiment. Black bars (n = 16): mean ± SEM suc-cess rate in the 1-h TDS session in time block 1 (0–5 min), timeblock 2 (6–10 min), and time block 8 (36–40 min). *Significantincrease in success from time block 1 (P < 0.002). Striped bars:subgroup of six of 16 subjects (experienced controls in the 1-hTDS session when they were naive). Grey bars: experiencedcontrols (n = 6, a subgroup of the group of 16 subjects).#Significantly higher success rate in time block 1 in the controlsession compared with the 1-h TDS session (P = 0.021). §Theexperienced controls performed better than the naive controls(white bars) (P = 0.019). Neither group improved during rest(P = 0.995). Comparison between success in time block 8 ofthe naive group (total training time of 10 min) and time block 2of the 1-h TDS session shows no significant difference(P = 0.208).
50 Kothari et al.

regression line. The slope of the regression line fromchanges in TDS success over time was significantlysteeper than the slopes of the 1 N and 3 N regressionlines, suggesting a difference in TDS success dynamicscompared with those of 1 N and 3 N. In future studies, itwill be possible and necessary to compare the effect ofthe three training paradigms, in terms of their ability toinduce cortical plasticity, using, for example transcranialmagnetic stimulation.Skill training induces neuroplastic changes more
effectively than strength training, and motor skill train-ing coupled with strength training does not promotegreater cortical neuroplastic changes in the MI thanmotor skill training alone (35–38). In order to facilitatethe cortical neuroplastic changes, findings from the
spinal system suggest that skilled or precision tasksshould be used in association with the learning stages ofuntrained functional tasks. It can ultimately lead toimprovements in motor behavior or performance(35–38). In a previous tongue-training study (a simpletongue-protrusion task), we indeed found a gradual andsignificant improvement in the performance success ratesover the 7-d training period, which was associated withspecific and reversible plasticity of the corticomotorexcitability related to tongue muscle control (14). Theneuroplastic changes associated with the learning of theorofacial motor task appeared to be specific to the ton-gue because they were not accompanied by comparablechanges in the first dorsal interosseos muscle (the controlsite). Therefore, it was concluded that the observedchanges did not reflect a generalized neuroplasticity inthe corticomotor pathways (14). Further studies onchanges in corticomotor excitability with the new andmore complex tongue-training paradigm introduced inthis study, in comparison with the tongue-protrusiontask, are needed.The recall of experienced subjects in the TDS session
displayed similar performance success rates, achieved inthe last 5 min of the TDS 1-h continuous session, indi-cating skill retention during the time-periods between thetwo sessions. The subjects achieved no further increase inperformance success rates after 30 min of rest in thecontrol experiment. Likewise, the naive group showed nosignificant increase in performance success rates during30 min of rest (offline learning), indicating that the in-crease in performance success rates in the 1-h TDS ses-sion was a result of continuous (repetitive) training andnot just a time effect. In the experienced group, the lackof further increase in success can also be hypothesized tobe caused by a ceiling effect of behavioral learning. Thedifference in success rate between experienced and naivesubjects in the control experiment may also be influencedby the fact that the experienced subjects had participatedin three tongue-training sessions (1 N, 3 N, and theTDS) before entering into the control experiment. Itcannot be concluded that the high success rate in theTDS control experienced session was solely based onprior TDS experience. Another limitation to the controlexperiment was, of course, the low number of subjects.However, statistically significant results were found, andnon-parametric re-analysis (not presented) did notchange the conclusion.The analyses of subject-based reports showed that
subjects experienced more fun and were feeling signifi-cantly more motivated while performing the complextongue-training task compared with the simple tongue-protrusion tasks. In addition, the TDS training was lesspainful and made subjects less fatigued compared withsimple tongue-protrusion tasks. Fatigue and pain havebeen shown to negatively influence motor learning (34)and are therefore important factors. The motivationalfunction of feedback (like, for example, the number ofgame points in a computer game) is thought to energizethe task interest and encourage continued effort, persis-tence, and attention to goal accomplishment throughevidence of performance progress (39). Within the
0
2
4
6
8
10
1 N 3 N TDS
0
2
4
6
8
10
1 N 3 N TDS
0
2
4
6
8
10
1 N 3 N TDS
0
2
4
6
8
10
1 N 3 N TDS
NRS
sco
res
(0–1
0)N
RS s
core
s (0
–10)
NRS
sco
res
(0–1
0)N
RS s
core
s (0
–10)
**
**
**
**
Fun
Pain
Fatigue
Motivation
Fig. 5. Mean subject-based reports (n = 16) comparing threesessions [1 N, 3 N, and the Tongue Drive System (TDS)] withfun, pain, fatigue, and motivation, revealing that the TDS wasmore fun (P < 0.001), induced less pain (P < 0.049) and lessfatigue (P < 0.009), and had a higher level of motivation(P < 0.003) than the other sessions. *Significant differencebetween sessions (P < 0.049). NRS, numerical rating scale.
Force and complexity of tongue training 51

motor-learning literature, the role of feedback has playedan important role and garnered research attention (40).The role of feedback not only has an informationalfunction, but also has motivational properties that havean important influence on motor learning. Feedbackindicating better than average performance has beenshown to have a beneficial effect on learning (40) but inthe present study no significant correlation was foundbetween relative increases in performance success ratesand subject-based reports on level of motivation. Thepossible limitation may be the unidimensional numericalrating scale applied in the present study, as more aspectsof motivation and other feedback measures, such asobservational feedback, focus of attention, and self-controlled practice, can also play a major role inbehavioral learning and it will be valuable to take theseinto consideration for future studies (39, 40).The influence of the type of tongue training (strength
vs. skill; simple vs. complex) on the extent and durationof changes in cortical excitability and intracorticalfacilitatory and inhibitory networks is another importantfield to explore in future studies in order to use thetechnique in the development of optimal neurorehabili-tation strategies for patients suffering from tongue dys-functions such as dysphagia (14, 15, 19).In conclusion, the results of the present study provide
evidence that force level and complexity of tongue-train-ing paradigms influences behavioral measures of tonguemotor learning (i.e. performance improvement). Formerexperience with the TDS influenced baseline success,indicating a degree of skill retention. Training with theTDS was rated as more fun, less painful, less fatiguing,and more motivating compared with simple tonguetraining. However, in the present study there was no sig-nificant correlation between performance success ratesand subject-based reports. The influence of the tongue-training paradigm and the level of feedback measures,such as fun, motivation, fatigue, and pain, on corticalplasticity needs further study and may help to guide thedevelopment of optimal tongue-training strategies.
Acknowledgements– This study was funded by the Danish DentalAssociation.
Conflicts of interest– The authors report no conflict of interest.
References1. Smith A. The control of orofacial movements in speech. Crit
Rev Oral Biol Med 1992; 3: 233–267.2. Sawczuk A, Mosier KM. Neural control of tongue movement
with respect to respiration and swallowing. Crit Rev Oral BiolMed 2001; 12: 18–37.
3. Hiiemae KM, Palmer JB. Tongue movements in feeding andspeech. Crit Rev Oral Biol Med 2003; 14: 413–429.
4. Martin RE, Macintosh BJ, Smith RC, Barr AM, Stevens
TK, Gati JS, Menon RS. Cerebral areas processing swallowingand tongue movement are overlapping but distinct: a functionalmagnetic resonance imaging study. J Neurophysiol 2004; 92:2428–2443.
5. Sessle BJ, Yao D, Nishiura H, Yoshino K, Lee JC, Martin
RE, Murray GM. Properties and plasticity of the primatesomatosensory and motor cortex related to orofacial sensori-
motor function. Clin Exp Pharmacol Physiol 2005; 32: 109–114.
6. Hori K, Ono T, Iwata H, Nokubi T, Kumakura I. Tonguepressure against hard palate during swallowing in post-strokepatients. Gerodontology 2005; 22: 227–233.
7. Hori K, Ono T, Nokubi T. Coordination of tongue pressureand jaw movement in mastication. J Dent Res 2006; 85: 187–191.
8. Khedr EM, Abdel-Fadeil MR, El-Khilli F, Ibrahim MQ.Impaired corticolingual pathways in patients with or withoutdysarthria after acute monohemispheric stroke. NeurophysiolClin 2005; 35: 73–80.
9. Axelsson K, Norberg A, Asplund K, Soderberg O, Wenn-
gren BI. Training of eating after a stroke in a patient withdysphagia of pharyngeal type. Scand J Caring Sci 1988; 2:31–36.
10. Terre R, Mearin F. Oropharyngeal dysphagia after the acutephase of stroke: predictors of aspiration. NeurogastroenterolMotil 2006; 18: 200–205.
11. Dennis M. Nutrition after stroke. Br Med Bull 2000; 56: 466–475.
12. Melsen B, Attina L, Santuari M, Attina A. Relationshipsbetween swallowing pattern, mode of respiration, and devel-opment of malocclusion. Angle Orthod 1987; 57: 113–120.
13. Rogers B. Feeding method and health outcomes of childrenwith cerebral palsy. J Pediatr 2004; 145: S28–S32.
14. Svensson P, Romaniello A, Arendt-Nielsen L, Sessle BJ.Plasticity in corticomotor control of the human tongue mus-culature induced by tongue-task training. Exp Brain Res 2003;152: 42–51.
15. Baad-Hansen L, Blicher JU, Lapitskaya N, Nielsen JF,Svensson P. Intra-cortical excitability in healthy human sub-jects after tongue training. J Oral Rehabil 2009; 36: 427–434.
16. Svensson P, Romaniello A, Wang K, Arendt-Nielsen L,Sessle BJ. One hour of tongue-task training is associated withplasticity in corticomotor control of the human tongue mus-culature. Exp Brain Res 2006; 173: 165–173.
17. Pascual-Leone A, Grafman J, Hallett M. Modulation ofcortical motor output maps during development of implicit andexplicit knowledge. Science 1994; 263: 1287–1289.
18. Ernberg M, Serra E, Baad-Hansen L, Svensson P. Influenceof topical anaesthesia on the corticomotor response to tonguetraining. Arch Oral Biol 2009; 54: 696–704.
19. Boudreau S, Romaniello A, Wang K, Svensson P, Sessle BJ,Arendt-Nielsen L. The effects of intra-oral pain on motorcortex neuroplasticity associated with short-term novel tongue-protrusion training in humans. Pain 2007; 132: 169–178.
20. Gabriel DA, Kamen G, Frost G. Neural adaptations toresistive exercise: mechanisms and recommendations for train-ing practices. Sports Med 2006; 36: 133–149.
21. Seidl RO, Nusser-Muller-Busch R, Hollweg W, Westho-
fen M, Ernst A. Pilot study of a neurophysiological dysphagiatherapy for neurological patients. Clin Rehabil 2007; 21: 686–697.
22. Ghovanloo M. Tongue operated assistive technologies. ConfProc IEEE Eng Med Biol Soc 2007; 4376–4379.
23. Huo X, Wang J, Ghovanloo M. Introduction and preliminaryevaluation of the Tongue Drive System: wireless tongue-oper-ated assistive technology for people with little or no upper-limbfunction. J Rehabil Res Dev 2008; 45: 921–930.
24. Huo X, Wang J, Ghovanloo M. Wireless control of poweredwheelchairs with tongue motion using tongue drive assistivetechnology. Conf Proc IEEE Eng Med Biol Soc 2008; 4199–4202.
25. Huo X, Wang J, Ghovanloo M. A wireless tongue-computerinterface using stereo differential magnetic field measurement.Conf Proc IEEE Eng Med Biol Soc 2007: 5723–5726.
26. Huo X, Wang J, Ghovanloo M. A magneto-inductive sensorbased wireless tongue-computer interface. IEEE Trans NeuralSyst Rehabil Eng 2008; 16: 497–504.
27. Jensen JL, Marstrand PC, Nielsen JB. Motor skill trainingand strength training are associated with different plasticchanges in the central nervous system. J Appl Physiol 2005; 99:1558–1568.
52 Kothari et al.

28. Murray GM, Lin LD, Moustafa EM, Sessle BJ. Effects ofreversible inactivation by cooling of the primate face motorcortex on the performance of a trained tongue-protrusion taskand a trained biting task. J Neurophysiol 1991; 65: 511–530.
29. Robertson EM, Press DZ, Pascual-Leone A. Off-line learn-ing and the primary motor cortex. J Neurosci 2005; 25: 6372–6378.
30. Kothari M, Svensson P, Basic A, Christiansen B, Vigso M,Truc L, Baad-Hansen L. Influence of the ability to roll thetongue and tongue-training parameters on oral motor perfor-mance and learning. Arch Oral Biol 2011; 56: 1419–1423.
31. Baad-Hansen L, Arima T, Arendt-Nielsen L, Neumann-Jensen B, Svensson P. Quantitative sensory tests before and1(1/2) years after orthognathic surgery: a cross-sectional study.J Oral Rehabil 2010; 37: 313–321.
32. Huo X, Ghovanloo M. Using unconstrained tongue motion asan alternative control mechanism for wheeled mobility. IEEETrans Biomed Eng 2009; 56: 1719–1726.
33. Mortimore IL, Bennett SP, Douglas NJ. Tongue protrusionstrength and fatiguability: relationship to apnoea/hypopnoeaindex and age. J Sleep Res 2000; 9: 389–393.
34. Boudreau SA, Hennings K, Svensson P, Sessle BJ, Arendt-Nielsen L. The effects of training time, sensory loss and
pain on human motor learning. J Oral Rehabil 2010; 37: 704–718.
35. Boudreau SA, Farina D, Falla D. The role of motor learningand neuroplasticity in designing rehabilitation approaches formusculoskeletal pain disorders. Man Ther 2010; 15: 410–414.
36. Perez MA, Lungholt BK, Nyborg K, Nielsen JB. Motorskill training induces changes in the excitability of the leg cor-tical area in healthy humans. Exp Brain Res 2004; 159: 197–205.
37. Remple MS, Bruneau RM, Vandenberg PM, Goertzen C,Kleim JA. Sensitivity of cortical movement representations tomotor experience: evidence that skill learning but not strengthtraining induces cortical reorganization. Behav Brain Res 2001;123: 133–141.
38. Jull GA, Falla D, Vicenzino B, Hodges PW. The effect oftherapeutic exercise on activation of the deep cervical flexormuscles in people with chronic neck pain. Man Ther 2009; 14:696–701.
39. Lewthwaite R, Wulf G. Social-comparative feedback affectsmotor skill learning. Q J Exp Psychol (Colchester) 2010; 63:738–749.
40. Wulf G, Shea C, Lewthwaite R. Motor skill learning andperformance: a review of influential factors.Med Educ 2010; 44:75–84.
Force and complexity of tongue training 53