Embed Size (px)
Citation preview

Food Fortification in Food Fortification in Public Health PolicyPublic Health Policy
TH Tulchinsky MD MPHTH Tulchinsky MD MPH
Braun SPHBraun SPH
11 Nov 200311 Nov 2003

Essential ConsiderationsEssential Considerations Public health and medical responsibility
Food industry and regulators involved
Create demand - enriched foods, behavior changes
Monitor compliance and ID rates
National council on nutrition - academic and professional organizations and public reps
Long term program
Regulatory, monitoring and laboratory support

Public Health Nutrition StrategiesPublic Health Nutrition Strategies
• Food based strategyFood based strategy – Socio economic factors– Food supply/costs – Education
• Supplementation for target groupsSupplementation for target groups– Women and children– Elderly
• Fortification of basic foodsFortification of basic foods• Surveillance and monitoringSurveillance and monitoring

18-1918-19thth Century Breakthroughs Century Breakthroughs
• Lind and scurvy 1747
• Lemon juice in Royal Navy, 1796
• Davy isolates sodium, potassium, calcium, magnesium, sulphur, boron, 1807
• Chatin shows iodine prevents goiter, 1850
• Takaki and beriberi, Japanese Navy, 1885
• Eijkman publishes cause of beriberi, 1897

0
1
2
3
4
IronSuppl .
Iron Fort . IodineSuppl.
IodineFort .
Vit ASuppl.
Vit AFort .
US
Do
llar
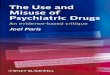
sLow Cost Solutions to Eliminate Low Cost Solutions to Eliminate
Micronutrient MalnutritionMicronutrient Malnutrition
Source: World Bank, 1994
Annual Per Capita Cost of Interventions

Productivity Gained per US$ Expended
$13.8$24.7 $28.0
$47.5
$84.1
$146.0
$0
$25
$50
$75
$100
$125
$150
Fe Suppl .( Wom).
Fe Suppl .(Preg .Wom).
IodineFort .
Vit .AFort .
Fe Fort . Vit .ASuppl .
Relative Cost Effectiveness of Relative Cost Effectiveness of Micronutrient InterventionsMicronutrient Interventions
Source: UNICEF/UNU/WHO/MI, 1999

Vital AminesVital Amines
• 1900, nutrition - calories, fats, carbohydrates proteins
• 1912, Funk defines vital amines • Rickets, scurvy, goiter, beriberi common in
industrial countries• Pellagra “epidemic” in southern US• 1914, Goldberger of USPHS investigates
pellagra• 1922, McCollum and vitamin D in cod liver oil

More on VitaminsMore on Vitamins
• 1931, Fluoride shown to prevent tooth decay• 1932, Vitamin C and riboflavin isolated• 1933, Williams - kwashiorkor as vitamin
deficiency• 1941, Prenatal diet and health of newborn• 1945, Fluoridation of water Grand Rapids• 1948, Vitamin B12 isolated• 1949, Framingham study begins

Key LandmarksKey Landmarks
• Morton’s iodized salt, 1924
• Louisiana - mandates vit B fortification of flour, 1928
• US federal mandate - enrichment of flour with vitamins B and iron, 1941
• UK and colonies same during WWII

Preventing Goiter and Iodine Deficiency Disorders
• 1917, high % US draftees rejected - goiter
• 1922-27, goiter rates fall from 39% to 9% by statewide prevention programs
• 1924, Morton’s Iodized Salt (N America)
• 1979, Iodization mandatory in Canada
• 1980s, WHO - universal iodization of salt
• Many countries achieved iodization

Iodine Fortification of Salt in the U.S.: Trend in Goiter Prevalence in
Michigan
0
10
20
30
40
50
1924 1929 1951
Year
Per
cen
t
WHO Monograph Series N. 44

Pellagra: The 4 DsPellagra: The 4 Ds
• Diarrhea, dermatitis, dementia, death
• Thought to be of infectious origin
• Common in prisons, mental institutions, sharecroppers in southern US
• Curable by dietary change (Goldberger)
• 1929, niacin found as essential factor
• 1906-1940, 3 million cases and 100,000 deaths attributed to pellagra

Figure 2

RicketsRickets
• 1921, rickets affects 75% of children in New York City schools
• Cod liver oil commonly used (middle class) • 1940s, US fortifies milk with vitamin D
dramatically reduces rickets incidence• Canada fortifies milk 1940s, then refortifies
resulting in increase in rickets in 1960s

Global Burden of Global Burden of Micronutrient DeficienciesMicronutrient Deficiencies
• Iron deficiency - all ages• Chronic undernutrition – all ages• Iodine deficiency – pregnancy• Vitamin A deficiency – young
children• PEM – young children• Folic acid deficiency – all ages
2 billion* 1 billion* 200 million** 200 million*
167 million* Unknown
•Source WHO

Iron DeficiencyIron Deficiency
• Commonest MND
• Affects survival, health and productivity
• Affects women in age of fertility
• Affects pregnancy and newborn
• Affects growth and cognitive development of infants and children
• Interaction with vitamin C deficiency

Global Burden of Iron DeficiencyGlobal Burden of Iron Deficiency
WHO RegionAnemic or Iron Deficient
Prevalence of Anemia in Pregnancy
Africa
America
Europe
E. Mediterranean
S.E. Asia
Western Pacific
206
94
27
149
616
1058
52
60
18
50
74
40
•Source WHO

Benefits of PreventingBenefits of PreventingIron DeficiencyIron Deficiency
Benefits to childrenBenefits to childrenImproved behavioral and cognitive
developmentImproved child survival (where severe
anemia is common) Benefits to adolescentsBenefits to adolescents
Improved cognitive performanceBetter iron stores for later pregnancies
(females)

Benefits to Pregnant Women and Their InfantsBenefits to Pregnant Women and Their Infants
Decreased low birth weight and perinatal mortality
Decreased maternal mortality and obstetrical complications (where severe anemia is common)
Benefits to all IndividualsBenefits to all Individuals
Improved fitness and work capacity
Improved cognition
Increased immunity
Lower morbidity from infectious disease

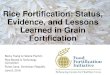
Trends in Prevalence of Anemia* in Low-Trends in Prevalence of Anemia* in Low-income U.S. Children, 12-17 Months Oldincome U.S. Children, 12-17 Months Old
0
2
4
6
8
10
12
14
73 75 77 79 81 83
Birth Year
Per
cent
Program Enrollment
Follow-up
*Hgb <10.3 g/dLYip et al., JAMA, 1987

Preschool children
School age children
and adolescents
Non-pregnant women
Pregnant women
Adult men

*Based on serum ferritin modelNHANES III (Ogden et al., 1998)
Prevalence of iron deficiency* by income and Prevalence of iron deficiency* by income and race/ethnicity, U.S., 1-4 year olds, 1988-94race/ethnicity, U.S., 1-4 year olds, 1988-94
0
2
4
6
8
10
12
white black Mexican-American
<=185% poverty
>185% poverty

US Federal PolicyUS Federal Policy• USDA extension programs
• 1921-29, US Maternal and Infancy Act - state health departments employ nutritionists
• 1930s, relief/commodity distribution
• 1941, enriched wheat flour with iron, vit B
• 1941, US establishes RDAs
• Food stamps, WIC, school lunch programs
• National nutrition surveys

Canada 1979Canada 1979
• National nutrition survey 1971
• Geographic, social and ethnic deficiencies
• Process of consultation
• 1979 federal regulations, mandatory
• Vitamin A and D in all milk products
• Iodine in salt
• Vitamins B and iron in flour

Epidemiologic Revolution Epidemiologic Revolution 1960s-1980s1960s-1980s
• Risk factors for chronic disease• Health field concept• Health for All• Declining mortality from stroke and CHD, trauma• Advances in drugs and diagnostics• Control of infectious diseases• Rapid increase in costs of care: health system
reform

Nutrition InteractionsNutrition Interactions• Iodine Deficiency – psychomotor retardation• Iron Def Anemia and infectious diseases• Iron promotes growth and development• Vitamin A and infectious diseases e.g. measles• Vitamin A promotes growth • Folic acid prevents birth defects• Folic acid with CVD, Alzheimer’s Disease• Nutrition and cancer• Nutrition and cardiovascular disease• Nutrition and diabetes• Nutrition in disease management

Folic Acid and NTDsFolic Acid and NTDs
• Pre pregnancy folic acid supplements prevent neural tube defects, 1980s
• Supplements to women in age of fertility achieves <1/3 coverage, 1990s (US)
• FDA mandates fortification of “enriched” flour, from 1998
• Canada and UK also mandate folic acid fortification of flour
• New paradigm in public health

Table
Return to top.
Figure

Figure


Folic Acid and Heart DiseaseFolic Acid and Heart Disease
• High homocysteine levels associated with excess CHD, birth defects, Alzheimer’s Disease
• Folic acid reduces high homocysteine• Flour fortification effective in raising FA
levels in population• Clinical trials of folic acid and CHD
underway• New paradigm in public health nutrition

OsteoporosisOsteoporosis
• Aging of the population
• Vit D production in skin seasonal
• Sun varies by season and latitude even in sunny countries
• Fortification of calcium popularized
• Vitamin D lacking in raw milk
• Calcium, vitamin D, fluoride co-factors
• Fortifying milk products with Vit D needed

Problems with Fortification PolicyProblems with Fortification Policy
• Antagonism to trends in North America
• European resistance e.g. EU
• Nutritionist focus on clinical approach
• WHO ambivalence/opposition
• “Green” attitudes
• Medical attitudes and lack of interest
• Resistance to “mandatory medication”
• Individual choice
• Clinical vs. population approaches
• Manufacturer’s and regulatory agency attitudes

ProgressProgress• Decreased contamination and food-borne
disease • Improved food handling methods - refrigeration• Improved nutritional value of foods and crops • Food fortification • Identifying essential micronutrients• Food-fortification programs eliminated rickets,
goiter, pellagra in the US, Canada• Folic acid and other new disease relationships• Micronutrients as functional food elements • Genetically engineered foods

ConclusionConclusion
• Nutrition a major public health issue• Affects MCH, infectious, non infectious
disease• High priority – birth defects, IDA, IDD, CHD• Fortification has low sex appeal vs. clinical • Mandatory vs. voluntary – false dilemma• Requires concern, knowledge, advocacy
and leadership• Public health role

ReferentsReferents
• World Health Organization
• UNICEF
• CDC
• American Academy of Pediatrics
• American College Obstetrics and Gynecology
• Food and Drug Administration
• Health Canada